Vincent Di Marino1 and Hubert Lepidi1
(1)
UER Médecine, Aix-Marseille Université, Marseille, France
Abstract
The formation of the clitoris, a component of the external female genital apparatus, is complex and cannot be dissociated from the organisation of the internal female genital apparatus. This organisation not only involves gonosomes (sexual chromosomes), hormonal factors and growth factors but also specific genes, the homeotic genes regulating the embryonic organisation plane.
The formation of the clitoris, a component of the external female genital apparatus, is complex and cannot be dissociated from the organisation of the internal female genital apparatus. This organisation not only involves gonosomes (sexual chromosomes), hormonal factors and growth factors but also specific genes, the homeotic genes1 regulating the embryonic organisation plane.
The first development stages of the male and female genital apparatuses are similar and the external genitals of the two sexes resemble each other until the third month of development.
In order to facilitate the reader’s understanding, we will successively study the internal phenomena and then the external phenomena before specifying what induces the said phenomena.
2.1 Internal Phenomena
The initial situation can be considered by examining the caudal end of the embryo on the 34th day of the development2 (Fig. 2.1). This end is occupied by a cavity, the cloacal cavity or cloaca, covered by an entoblastic embryonic layer.3 This cloaca is closed at its end by a didermic membrane, i.e. with double layer (endoderm lined with ectoderm), the cloacal membrane.
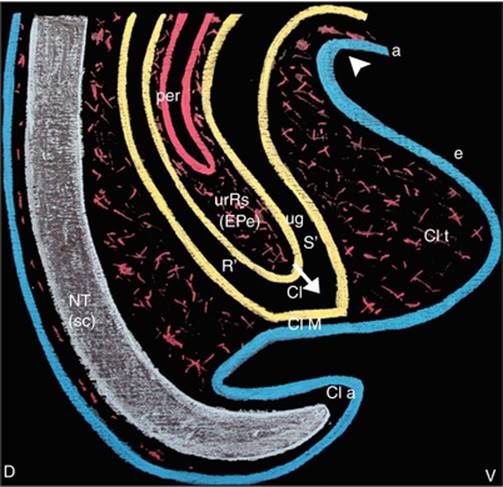
Fig. 2.1
Median sagittal section of the pelvic region (drawing of a micrograph female human fœtus; 34th day of development) (The ectoblast is drawn in blue (a amnios, e epiblast, NTneurectoblaste of the neural tube). The mesoblast is drawn in red. The entoblast is drawn in yellow). D dorsal, V ventral, Cl cloaca, Cl a cloacal appendix, Cl M cloacal membrane, Cl tcloacal tubercle, NT neural tube (scspinal cord), per peritoneum, R′ future rectum, ugS′ future urogenital sinus, urRs urorectal septum (eperon perineal of French anatomists), oblique white arrow it shows the direction of urRs′ progress towards the cloacal membrane, white arrowhead it indicates the point where the epiblast follows the amnios (which covers the umbilical cord)
On the ventral surface of the caudal end, a growth can be observed: the cloacal tubercle consisting of mesoderm covered by ectoderm.
The development in the caudal direction of the partition initially separating the primitive intestine and the allantois, the urorectal fold (which itself consists of mesenchyme coated with endoderm), will divide the cloaca, in its cranial two-third, into two ducts: a ventral duct (the urogenital sinus) and a dorsal duct (the posterior intestine). The embryologists still refer to this fold as the “fold of Tourneux”.4The cloacal tubercle is at the front of the urogenital sinus. The cranial half of this tubercle will become the infra-umbilical anterior abdominal wall (pelvic wall). As for its caudal half, it will be the site of complex phenomena leading to the formation of the urogenital sinus: it will be colonised by a budding of the ventral endodermal wall of the cloaca, the cloacal entoblastic plate, (“cloacal entoblastic lamina of Solère” for French authors). This lamina progresses towards the top of the cloacal tubercle, which it reaches around the 36th day of development (Fig. 2.2).
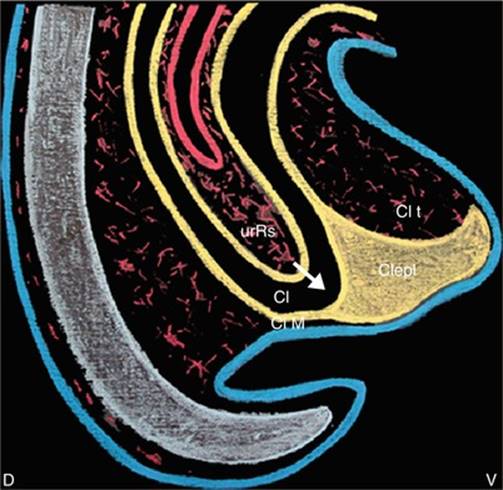
Fig. 2.2
Median sagittal section of the pelvic region (drawing of a micrograph female human fœtus; 36th day of development). Cl cloaca, Clepl cloacal entoblastic plate (lame entoblastique cloacale of French authors), Cl M cloacal membrane, Cl t cloacal tubercle, urRs urorectal septum, oblique white arrow it shows the direction of urRs′ progress towards the cloacal membrane
As of the 37th day (Fig. 2.3), apoptosis phenomena will occur within the cloacal entoblastic plate towards the top of the cloacal tubercle, with formation of vacuoles whose convergence will perform of a sort of tunnelling process. This hollowing phenomenon occurs within the cloacal entoblast, the ventral extension of the primitive urogenital sinus, which will be the phallic portion of this sinus. The urorectal fold, which has come closer to the perineum by progressing towards the cloacal tubercle, is at present referred to as the perineal urorectal septum. This septum will end up by merging with the remainder of the endodermal lamina,5 as of the 42nd day of development (Fig. 2.4), thus determining two ducts, the ventral urogenital duct and the dorsal intestinal duct, as well as two didermic membranes, i.e. a ventral membrane, the urogenital membrane and a dorsal membrane, the anal membrane. At the same time as the development of the urogenital duct, which has become the urogenital sinus, four ducts are also developing in the embryonic mesenchyme (mesoblast). They will end at this sinus and thus divide it into a cranial, urinary, vesicourethral section (future urinary bladder + future proximal urethra) and a caudal genital section: the pelvic section of the urogenital sinus. These four ducts are the two mesonephric ducts: Wolff channels and the two paramesonephric ducts (Muller channels).6
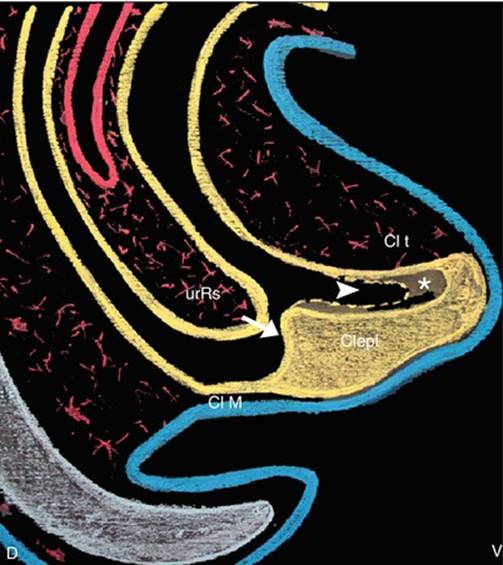
Fig. 2.3
Median sagittal section of the pelvic region (drawing of a micrograph female human fœtus; 40th day of development) (While the urRs is progressing toward the Clepl, which is digged (asterisk) toward the top of the cloacal tubercle (phenomenon explained by apoptosis and convergent vacuolisations)) Clepl cloacal entoblastic plate (lame entoblastique cloacale of French authors), Cl M cloacal membrane, Cl t cloacal tubercle, urRs urorectal septum, Oblique white arrow it shows the direction of urRs’s progress toward the Clepl (observe that the urRs is quite in contact with the Clepl), White arrowhead it shows the digging of the Clepl which will result in the formation of the phallic part of the future urogenital sinus
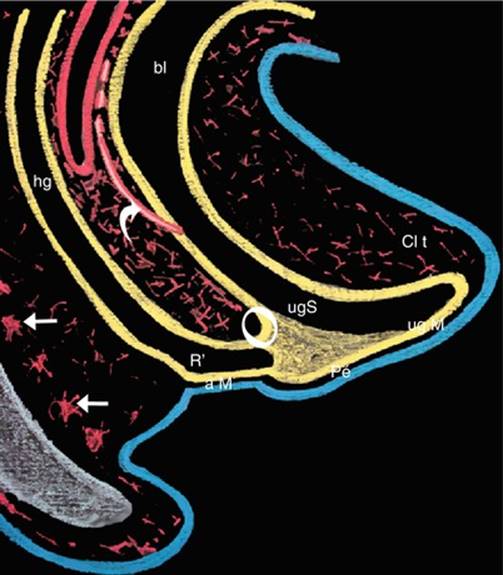
Fig. 2.4
Median sagittal section of the pelvic region (drawing of a micrograph female human fœtus; 42th day of development) (The fusion of the urRs with the Clepl (white circle), which occurred at the end of the 6th week of development, divides the primitive cloaca into two ducts: the urogenital sinus, ventral and the hindgut, dorsal. The primitive perineum separates the urogenital membrane from the anal). a M anal membrane, bl bladder, Cl t cloacal tubercle, hg hindgut, Pe perineum, ug M urogenital membrane, ug S urogenital sinus, R′ future rectum, curved white arrow it shows one of the two paramesonephric ducts opening into the urogenital sinus, white right arrows mesenchymatous condensations which will form the vertebras
On the last day of the embryonic stage, i.e. on the 56th day, at the end of the 2nd month of development (Fig. 2.5), all is ready so that the last modifications can occur. Following these modifications, it will rapidly be possible to identify the sex of the foetus. The 56-day-old embryo shows, on the median sagittal section, two endodermal ducts: a dorsal duct corresponding to the posterior intestine and its caudal expansion, the rectum, and a ventral duct corresponding to the low urinary tracts with an expansion, which is the bladder, with an extension forming the three parts of the urogenital sinus, — from top to bottom, the future urethra (Sg-u1 portion of the urogenital sinus) whose external orifice will be located just above the vaginal orifice,7 the Sg-u 2 portion (pelvic portion of the urogenital sinus) and the distal portion (phallic portion of the urogenital sinus). The two endodermal ducts are blind and closed by the anal membrane and the urogenital membrane, respectively, between which the future perineum will be positioned. The junction between the pelvic and phallic portions of the urogenital sinus comes in contact with the utero-vaginal channel of Mullerian origin, at the end of which an endodermal budding (sino-vaginal bulbs) has developed and which will grow hollow to form the distal third of the vagina.8 Between the uterine body and the rectum, the peritoneal pouch (Douglas pouch) has inserted itself between the uterine body and the rectum, thus forming the bottom of the peritoneal pouch: the utero-rectal pouch. At the same time and as of the 7th week, the top of the old perineal tubercle has been modelled so as to form a spherical end: the genital tubercle located in front of the distal end of the phallic urethra. It is also at this stage that are now distinguished, from a ventral viewpoint, the pubic bones and the pubic symphysis, which have developed from the pre-sinus mesenchyme, and, from a dorsal viewpoint, the sacral and coccygeal vertebrae, which have developed from the dorsal mesenchyme and which surround the distal part of the neural tube (distal end of the spinal cord). As from the 1st day of the 3rd month of development, the embryo becomes a foetus. It is still not possible to externally identify if the foetus is male or female.
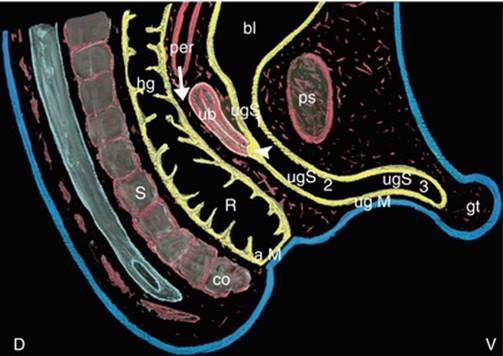
Fig. 2.5
Median sagittal section of the pelvic region (drawing of a micrograph female human fœtus; 56th day of development) (The uterus body and the superior part of the vagina are formed by the fusion of the two paramesonephric ducts (ducts of Muller) before opening into the primitive urogenital sinus. At this stage (end of the 2nd month), it is not possible to specify the embryonic sex). a M anal membrane, bl bladder, co coccyx, gt genital tubercle, hg hindgut, per peritoneum, ps pubic symphysis, R rectum, S sacrum, ub uterus body, ug Murogenital membrane, ugS1 urethral part of the urogenital sinus (future urethra), ugS2 pelvic part of the urogenital sinus, ugS3 phallic part of the urogenital sinus, right white arrow it shows the descent of the peritoneal pouch which will become the recto-uterine pouch, white arrowhead it shows the sino-vaginal bulbs which form the distal part of the vagina (the breaking down of their epithelium will connect the utero-vaginal canal with the urogenital sinus)
2.2 External Phenomena (Fig. 2.8)
At the beginning of the 6th week of development, epithelial folds have developed: they are the cloacal folds. They border the cloacal membrane on either side. Further outwards, other folds have formed: the labio-scrotal swellings.
The partitioning of the cloaca will cause the scission of the cloacal folds so that, at the end of the 6th week, two urogenital folds bordering the urogenital membrane and two anal folds bordering the anal membrane are to be observed. All these folds are ectodermal. It is to be noted that these two types of folds are separated by the superficial part of the perineal formation or primitive perineum, resulting from the posterior apposition of the urogenital folds and from the coalescence of the posterior section (dorsal) of the labio-scrotal swelling.
As observed previously, it is during the 7th week that an epithelial growth appears on the old cloacal tubercle: the genital tubercle or primitive phallus, which will become, via modelling morphogenesis phenomena, towards the end of the 2nd month, the glans clitoridis in women and penian glans in men. During the formation of the genital tubercle, in a region above the latter, the following is observed: a double cartilaginous draft of mesenchymal origin (two pubic bones connected by a pubic symphysis) and, at a higher level, the formation of the infra-umbilical ventral wall.
The perineum, which is now well represented, increases and progresses, in continuity with the mesenchymal partitions, which perfectly separate the genito-urinary and anorectal compartments.
At the start of the 9th week, the ventral growth of the genital tubercle will stretch the urogenital membrane. This membrane will break up a few days later, with the first rupture occurring at its anterior end. The anal membrane remains, but a small dip in its ectoderm appears and corresponds to the start of the formation of the future ectodermal anal canal.
From now, the anal membrane separates the ectodermal and endodermal parts of the anal canal. At the end of the 9th week, 63rd day (Figs. 2.6 and 2.7), the urogenital membrane has almost completely disappeared,9 thus exposing the endodermal ceiling of the phallic part of the urogenital sinus, in the male foetus as well as in the female foetus.10 However, major modifications will occur at the level of the external apparatus according to the sex of the individual: while in a male, the groove will secondarily close again and form the penian urethral cylinder through the fusion of the urethral folds and the bursa or scrotum will form through the fusion of the labio-scrotal swellings on the centre line,11 the groove will persist in the female sex, thus opening the vestibule onto the vulvar cleft with, on either side, the labio-scrotal swellings, which are still separate and will become the labia majora (Figs. 2.8 and 2.9). The pelvic portion of the female urogenital sinus (Su-g 2) now becomes the vestibule, into which emerges, at its cranial part, the external orifice of the urethra and directly below, the external orifice of the vagina. The genital tubercle protrudes below the ventral commissure of the labia. Inside of the labia majora, the labia minora, which are connected to the bottom surface of the genital tubercle, are hardly visible (Fig. 2.9). The epithelium which covers their medial surface comes, such as the vestibule, from the phallic portion of the urogenital sinus. It is thus of endodermal origin.

Fig. 2.6
Median sagittal section of the pelvic region (drawing of a micrograph female human fœtus; 63th day of development) (During the 9th week of development: The erectile bodies develop in the clitoral “draft”. The urogenital membrane disintegrates opening the phallic part of the urogenital sinus to the exterior and finally creating the vulvar cleft, (no secondary closure happening for the female fœtus)). a M anal membrane, bl bladder, CC corpus cavernosum clitoridis, co coccyx, gt genital tubercle, Pe perineum, per peritoneum (recto-uterine pouch), ps pubic symphysis, R rectum, S sacrum, sc spinal cord, u urethra, ub uterus body, ugS2 pelvic part of the urogenital sinus, ugS3 phallic part of the urogenital sinus, v awventral abdominal wall, va vagina, vc vertebral canal, white circle external urethral orifice
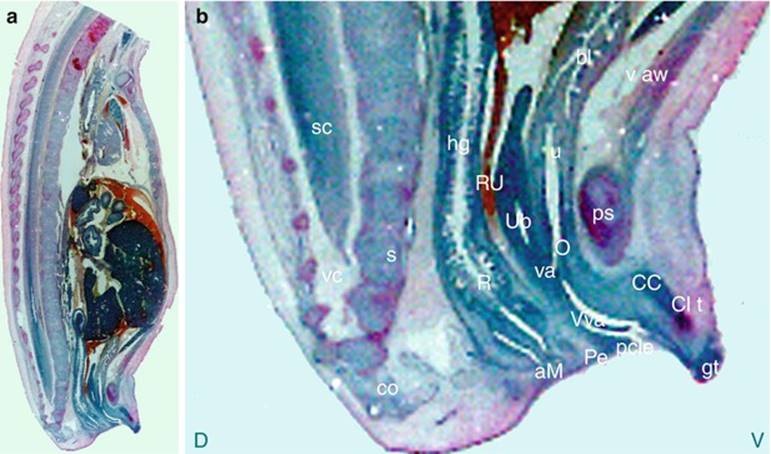
Fig. 2.7
(a) Photomicrograph of a sagittal section of a female human foetus 53 mm, (b) Photomicrograph of the pelvic region (magnification of the caudal end: x13), (Compare this sagittal section of a female human foetus with the picture of the 63th day of development). Note the remainders of the urogenital membrane, still present. As the anal membrane, it will break down at the end of the 10th week, establishing a continuity between the anal pit and the rectal part of the hindgut). D dorsal, V ventral, aM anal membrane, bl bladder, CC corpus cavernosum, Cl t cloacal tubercle, co coccyx, gt genital tubercle, hg hingut, pcle pudendal cleft, Pe perineum, ps pubic symphysis, R rectum, RU recto-uterine pouch, s sacrum, scspinal cord, u urethra, Ub uterus body, v aw ventral abdominal wall, va vagina, vc vertebral canal, Vva vestibule of the vagina, white circle around the external urethral orifice

Fig. 2.8
Differentiation of the external genitalia of the female human foetus. (a) 6th week: the cloacal membrane closes up the cloaca (caudal part of the hindgut); (b) 7th week: ventrally, the genital tubercle appears at the top of the cloacal tubercle. Dorsally, a partial fusion of the two urethral folds (creation of the genital raphe) separates the cloacal membrane into two parts, urogenital (ventral) and anal (dorsal). (c) 9th week: the urogenital membrane disintegrates, opening the phallic part of the urogenital sinus to the exterior. (d) 12th week: the urethral folds have become the labia minora, the labial swelling has become the labia majora and the hymen hides the vaginal orifice. The clitoris is in a shaping phase and the prepuce is already formed; af anal fold, aM anal membrane, as anal sphincter, Cl Mcloacal membrane, Clf cloacal fold, Cl t cloacal tubercle, dcom dorsal commissure, f frenulum, fl frenum of the labia minora, g glans, g ra genital raphe, gt genital tubercle (it appears at the 7th week, on the top of the cloacal tubercle), hy hymen, lm labium minus, lM labium majus, l sw labial swelling, pr prepuce, uf urethral fold, ug M urogenital membrane, V vestibule, vcom ventral commissure, white arrowhead perineal raphe, thick white right arrow mons pubis, fine right arrow external urethral orifice, curved white arrow hymeneal ostium, waved arrow disintegrating urogenital membrane
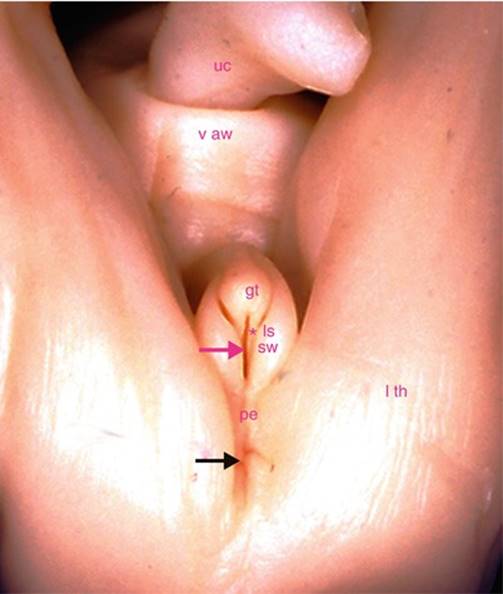
Fig. 2.9
Perineal view of the external genitalia of a female human fœtus (beginning of the 11th week of development). The fœtus is in gynaecological position. gt genital tubercle, ls sw left labio-scrotal swelling (future left greater lip), l th left thigh (posterior face), pe superficial perineum, uc umbilical cord, v aw ventral abdominal wall (infra-umbilical part), magenta asterisk left urethral fold (future left lesser lip), magenta arrow urogenital (or urethral) groove (future vulvar cleft), black arrow anus (the anal membrane is not completely disintegrated). At this stage, it is still difficult to know by a basic examination of the external genitalia, which is the sex of the foetus
The erectile bodies are already visible at this stage: They developed in the mesenchyme of the old cloacal tubercle. These are, first and foremost, the two corpora cavernosa whose attachments to each descending branch of the pubes (still cartilaginous) are quite visible (transverse sections: Fig. 2.10). These corpora cavernosa follow a development comparable to that of the male foetus. They have extended towards the genital tubercle and progress parallel to the cranial part of the genital formation (Figs. 2.7 and 2.11). At their end, they come closer in a V shape with the top pointing towards the genital tubercle (Fig. 2.12). The two spongious bodies initially develop in the mesenchyme, which surrounds the vulvar cleft and in the mesenchyme which occupies the genital tubercle (Fig. 2.10). At the level of the glans, the connections of this spongious body with the two corpora cavernosa (in preparation of the future disposition in adults) are perfectly visible. However, the development of these female spongious bodies is very particular. Due to the absence of a “penile” urethral cylinder, these spongious bodies have no periurethral future and remain separated by the vestibule, thus forming vestibular bulbs on the right and left. Moreover, while, in the male foetus, the urethral corpus spongiosum connects to that of the glans to form a single spongy flow, in the female foetus, the distal extension of the perivestibular spongy formation, despite the phallic urethra, which acts as a support stake, involutes and provides what is referred to as the “residual spongy part” without any significant erectile capacity.
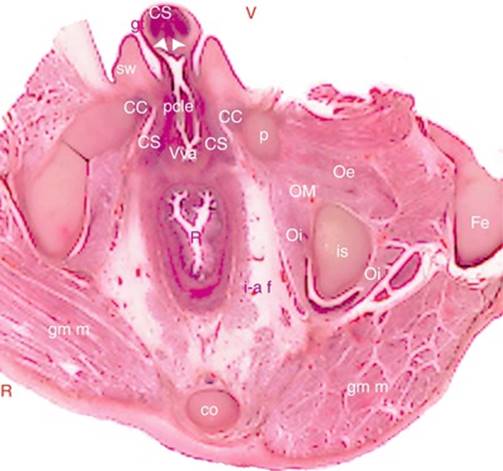
Fig. 2.10
Transverse section of the pelvic region (photomicrograph) female human fœtus; 11th week of the development. R right, V ventral, CC corpus cavernosum, CS corpus spongiosum, cococcyx, Fe femur, gm m gluteus maximus muscle, gt genital tubercle, i-a f ischio-anal fossa, is ischium, l sw labial swelling, Oe obturator externus muscle, Oi obturator internus muscle, OM obturator membrane, p pubis, pcle pudendal cleft, R rectum, Vva vestibule of vagina, white arrowheads they locate the two corpora cavernosa converging towards the future glans clitoridis, behind the corpus spongiosum. Observe: The corpora spongiosa, on either side of the vulva. They will become the bulbs. The corpora cavernosa (crura clitoridis), attached to the ischio-pubic rami
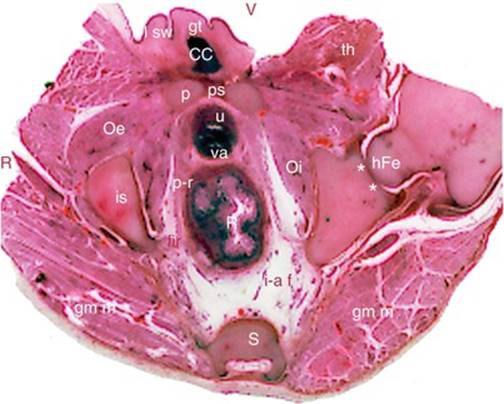
Fig. 2.11
Transverse section of the pelvic region (photomicrograph) female human fœtus; 11th week of development (section at the level of the middle third of the pubic symphysis). R right, Vventral, CCcorpora cavernosa, gm m gluteus maximus muscle, gt genital tubercle, hFe head of femur, i-a f ischio-anal fossa, is ischium, l sw labial swelling, Oe obturator externus muscle, Oi obturator internus muscle, p pubis, pr pubo-rectalis (bundle of levator ani muscle), ps pubic symphysis, R rectum, S sacrum, u urethra, th thigh, va vagina, **acetabulum. The present section, located above the previous one, is at the level of the pubic symphysis. It concerns, on the left side, the hip joint
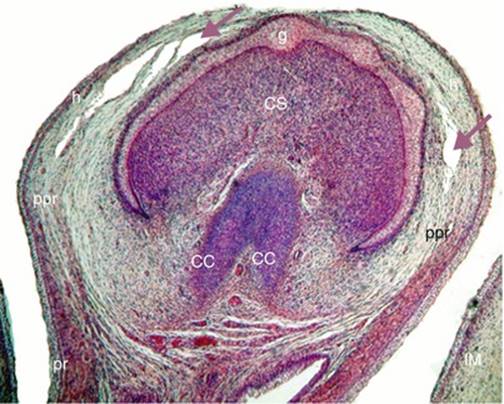
Fig. 2.12
Transverse section of the genital tubercle (photomicrograph showing the formation of the hood on a 43mm female human fœtus). CC corpus cavernosum, CS corpus spongiosum occupying the top of the genital tubercle, g top of the future glans, h future hood, lM labium majus (greater lip), ppr epithelial preputial plate (preputial lamina), pr prepuce, mauve arrows they show the vacuoles resulting from apoptosis phenomena
The following external stages will perfect the development of the external apparatus: They correspond to the formation of the preputial clitoral hood and the modelling of the clitoris.
The formation of the preputial clitoral hood is similar to that of the male penile prepuce.12 It starts as of the 8th week of development. A slight lamellar proliferation, referred to as the ectoblastic preputial plate, penetrating more or less deeply, from the surface epithelium, develops at the ectoblastic epithelial layer, which covers the genital tubercle (Fig. 2.12). Vacuoles appear in this lamina following apoptosis phenomena.13 The convergence of these vacuoles creates a space around the glans, which ends up separating, on the periphery, the glans and the portion of the prepuce which envelopes it.14 The preputial chamber of the glans clitoridis is thus created. It is bordered by the same epithelium corresponding to the internal layer of the hood and, on the other side, to the surface covering of the glans.
The clitoris will also undergo a reduction, thus modelling its shape and reducing its size (which makes us forget that at certain stages of its development, it was longer and more voluminous than the penis at same stage). Thus, in a 4-month-old female foetus (Fig. 2.13), and in relation to a normal development,15 the clitoris will have already acquired its final aspect: minuscule formation covered by the prepuce and whose end, the glans, is hidden under the hood.

Fig. 2.13
Female human fœtus at the end of the fourth month (18 weeks of amenorrhea). Macrophotography of the external genitalia Biometry of the fœtus; length vertex-coccyx: 14 cm. Weight: 220 g. All structures (greater and lesser lips, clitoris, frenula, commissures) are in place, normally developed. The genital tubercle declined, turning into clitoral glans. Compare with the genitalia of the fœtus at the 11th week
2.3 Determinism of Sexual Differentiation and Related Pathologies
We shall now examine how the sex of an embryo is determined and how it can be affected by pathological phenomena.
2.3.1 Basic Concepts
It is known that each somatic cell of each individual contains 23 pairs of chromosomes including 22 pairs of autosomes (44 autosomes) and a pair of sexual chromosomes or gonosomes (2 gonosomes). It is the latter which determine the sex that the embryo, and then the foetus, will have. If the two gonosomes are XX, the sex of the foetus will be female. If the two gonosomes are XY, the sex of the foetus will be male.16 As regards the sexual cells, i.e. the gametes (ovocytes in the ovaries and spermatozoa in the testes), there are only 23 chromosomes (one of each pair). The pairs are reformed in the egg cell (once the ovocyte has been fertilised by the spermatozoon).
2.3.2 Modern Concepts
It was necessary to wait for the second half of the twentieth century (1959) for the determinants of masculinity and femininity to be specified. Geneticists (especially P.A. Jacobs and J.A. Strong) managed to establish in an absolute manner that sexual determinism is related to gonosome Y: If this sexual chromosome is present, the foetus will be male. If it is absent, the foetus will be female.17 Seven years later, more progress (work performed by P.A. Jacobs and A. Ross) has been made and made it possible to locate the area determining the sex, in the short arm of chromosome Y. Finally, since 1987, the progress made in genetics (work performed by D.C. Page et al.) has made it possible to specify the area carrying the masculinity gene: this gene is referred to as gene SRY: the Sex-Determining Region of the Y chromosome is located in a small area of the short arm of Y, region 1 (work of M.S. Palmer et al. in 1989 and A.H. Sinclair et al. in 1990).
SRY is a trigger for genetic phenomena, which will generate, from the undifferentiated gonad, not only the formation of the testes and the secretion of the male hormone but also the secretion of the anti-Mullerian hormone, whose role is to cause the degeneration of the paramesonephric ducts of Müller. In the absence of the SRY gene, the ovaries develop and female hormones are produced.18
Later work showed that, in spite of its significance, the SRY gene is not alone and that there actually exists a gene cascade involved in sexual determinism.19
2.3.3 Pathologies of Sexual Differentiation
They can be of genetic or hormonal origin.
· Pathologies of genetic origin are the consequence of gonosome anomalies. Firstly, they include the Klinefelter and Turner syndromes (see below).
This also concerns cases of true hermaphroditism, i.e. cases in which gonads have testicular tissue and ovarian tissues (the standard case being uni- or bilateral the “ovotestis”). These cases are not very frequent. Karyotype anomalies are variable and all is visible, including “mosaic” cases with, in the same individual, cells comprising a Y chromosome and cells which do not contain this chromosome (karyotype example: 46, XX/46, XY). The phenotype is often interpreted at birth as male due to the presence of a penis.
· Pathologies of hormonal origin are due to a deficit in androgens (DHT or dihydrotestosterone20 and testosterone) or to anomalies affecting the receptors for androgens (feminising testicle), as regards male subjects. On the other hand, it is an early exposure to androgens21 which is responsible for pathologies in women. These hormonal anomalies are the cause of pseudo-hermaphroditism cases:
· Male pseudo-hermaphroditism: normal male karyotype (46, XY), normal gonads (normal testes but often ectopic testes), ambiguity of the genital tracts and external genitals (hypospadias, at a minimum, especially deficits in DHT; external female genitalia, especially in feminising testicles!)
· Female pseudo-hermaphroditism: normal female karyotype (46, XX), normal gonads (ovaries), ambiguity of the genital tracts and external genitals. All cases are possible, from the peniform clitoris associated to hypospadias and an empty scrotum to a male aspect of the external genitals but with however no testes in the bursa.22
2.3.4 The Revenge of Chromosome X
The most recent discoveries in the field of genetics have modulated the rigorous diagram referred to previously and the prominence of the SRY gene in the world of mammals (placental and marsupial mammals). Researchers (F Veyrunes, CNRS, et al., Institute of Genomics of the IRD) have discovered (December 2009), by studying the African pygmy mouse, Mus minutoides (close to the domestic mouse), that the Y chromosome does not always define the sex.
First of all, these researchers have noted, in the population of the above-mentioned mice, a majority of fertile females carrying XY gonosomes.
In order to understand, they then studied the “normal” females of this population, i.e. females carrying standard XX gonosomes. They then discovered that these two X sexual chromosomes could be differentiated morphologically and decided to call them (X) and (X*). They then turned their attention back to studying females carrying a Y chromosome and observed that the gonosomes of these females were in fact X*Y and not XY. The molecular and cytogenetic analyses, which they carried out at the same time on the Y chromosome of these females, were used to affirm that there was no mutation on the SRY gene and that there was no anomaly on this gene which could explain its non-expression. It must then be concluded that the chromosome (X*) carries a mutation, which is still unknown and which is capable of inhibiting the expression of the powerful SRY and thus cause a sex reversion. Extraordinary options are therefore now open to research and researchers are certainly in store for new surprises.
Footnotes
1
The homeotic genes are genes which determine the organisation plane of the individual: among these genes, there is the Hox gene, which determines the respective positions of the organs and the sonic hedgehog gene, which regulates morphogenesis.
2
The embryonic stages are expressed in numbers of days or weeks of development (it is necessary to add 2 weeks or 14 days to each of these figures to obtain the number of weeks of amenorrhoea: thus the 6th week of development corresponds to the 8th week of amenorrhoea).
3
The human embryo consists of 3 layers:
· The ectoblast (epiblast and neurectoblast), represented on the diagrams by a blue line
· The mesoblast, represented on the diagrams by a red line or red crosses
· The entoblast, represented on the diagrams by a yellow line.
4
F. Tourneux is the author of an Atlas of Embryology concerning genito-urinary organs, published in 1892 in Travaux et Mémoires des Facultés de Lille (Works and Memories of the Faculties of Lille).
5
Certain embryologists refer to converging paramedian folds, the Rathke folds, instead of the entoblastic lamina of Solere. These folds are linked at the Tourneux fold to partition the cloaca. We preferred the process generated by the development of the single entoblastic lamina, which is more compliant with our observations of embryos.
6
The mesonephric ducts will form, in foetuses of both sexes, the vesical trigone and the ureters. Furthermore, they will develop into spermatic ducts in male foetuses. On the other hand, the paramesonephric ducts will form, in female foetuses, the two fallopian tubes, the uterus and the top part of the vagina (utero-vaginal channel) by distal fusion on the centre line (in male foetuses, these ducts will involute following the secretion of an “anti-Mullerian” hormone, secreted by the precursors of the Sertoli cells of the male gonad).
7
In the male foetus, the pelvic portion of the urogenital sinus (Su-g 1) will become the prostatic urethra portion overlying the seminal colliculus (at the top of which ends the prostatic utricle, a Mullerian residue of the male sex!).
8
This hollowing process will be nearly complete, except for the area of junction with the urogenital sinus, where the hymeneal membrane (which will become the hymen) persists.
9
The anal membrane will only disappear during the 10th week.
10
It is not possible to specify the sex of a foetus until the 3rd month because the external genitals are similar until this date of development. This is why it is only during the second echography (morphological echography of the 2nd quarter), performed between 18th and the 24th week of amenorrhoea (16 to 22 weeks of development), that it is possible to inform a mother of the sex of the child she is carrying, if she wishes to know.
11
The closure of the penile cylinder and that of the bursa with the formation of their median raphe will only be completed during the 14th week of development.
12
In the male fœtus, the formation of the prepuce is moreover related to the development of the terminal urethra (at the level of the glans).
The preputial plate is the origin not only of the formation of the prepuce but also of that of the glandular urethral cylinder and the small navicular inside the glans: It has invaginated in the depth of the latter from its top and up to the level where the primitive penile urethra ends. The balanic (or glandular) urethra (with its small navicular), thus created, is placed in communication with the phallic urethra, resulting from the closure of Su-g3 to form the final urethra, which thus emerges at the top of the penis.
13
For other authors, the preputial chamber does not result from apoptosis phenomena but from a simple invagination of the epithelium of the glans surface.
14
The separation of the ectoblastic preputial plate is often incomplete. It then forms, for the glans, a free part and a buried, and thus hidden, part.
15
Very rare cases in which there is no clitoris have been reported in literature. It seems that, in certain young girls presenting this “agenesis”, the development of the embryonic clitoris actually did occur but that then an apoptosis gene intervened and caused its disappearance (gene comparable to the Bmp4 gene whose activation causes the disappearance of the penis in many birds including the cockerel).
16
This could be affirmed by the study of two subjects with a chromosomal anomaly: the Turner syndrome (karyotype: 45, X and female phenotype) and the Klinefelter syndrome (karyotype: 47, XXY and male phenotype).
17
Beyond this simplified diagram, it is also necessary to recall the major role of the hormones produced by the autosomes!
18
In certain relatively rare cases, it is possible for male subjects to have an XX gonosome. This is explained by an abnormal crossing over which, at the time of the meiosis, makes it possible for an X chromosome to incorporate a fragment of the short arm of the Y chromosome, bearing the region where the SRY gene is located.
19
The following have already been identified: SF-1 and WT1 expressed upstream of SRY and necessary for the development of the undifferentiated primitive gonad; DAX1 necessary for ovarian development; SOX9 necessary, with SRY, for testicular development; and SF-1 (steroidogenic factor-1) necessary for the secretion of testosterone by the Leydig cells of the testis and for the secretion of the anti-Mullerian hormone by the Sertoli cells of this testicle. Other genes are still being identified!
20
Deficiencies in DHT are generally due to a mutation of an enzyme, 5-alpha-reductase.
21
This early exposure can be due to:
· A tumour of the mother’s adrenal gland
· Foetal congenital adrenal hyperplasia
· Hormonal treatment with androgens during the pregnancy.
22
We can imagine the serious civil status mistakes resulting from the male aspect of a newborn baby!