Jeannine Rahimian, MD, MBA
Weight at delivery once was considered evidence of prematurity (birthweight <2500 g) or postmaturity (macrosomia; birthweight >4500 g). These criteria later were revised upon the realization that birthweight can be reflective of other pathologic processes aside from prematurity. Abnormalities in fetal growth at each end of the spectrum—both large for gestational age fetuses and fetuses with suspected intrauterine growth restriction—are associated with an increased risk of adverse perinatal outcome. Normative standards applying to such ultrasound parameters as estimated fetal weight, abdominal circumference, and head circumference (HC) were developed.
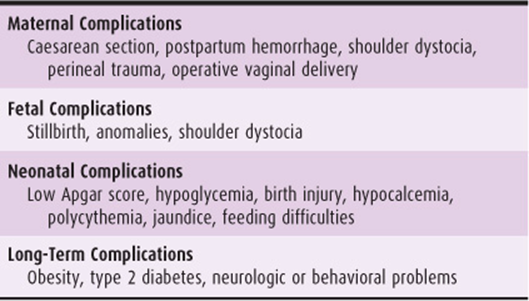
Abnormal fetal growth or fetal size is most commonly defined on the basis of estimated fetal weight. Fetuses with an estimated fetal weight ≤ the 10th percentile are classified as having intrauterine growth restriction (IUGR), and those with a weight ≥ the 90th percentile are classified as large for gestational age (LGA). Both IUGR and LGA fetuses have increased risk for perinatal morbidity and mortality (Tables 16–1 and 16–2). The pathogenesis, differential diagnosis, and treatment are different for the 2 extremes of growth.
Table 16–1. Some complications associated with intrauterine growth restriction pregnancy.
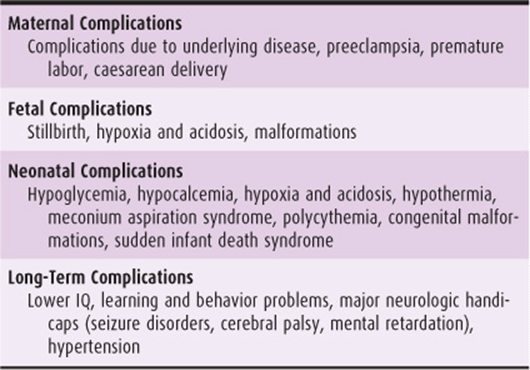
Table 16–2. Some complications of large for gestational age pregnancy.
INTRAUTERINE GROWTH RESTRICTION
ESSENTIALS OF DIAGNOSIS
![]() Estimated fetal weight less than the 10th percentile for gestational age on ultrasound
Estimated fetal weight less than the 10th percentile for gestational age on ultrasound
Many terms have been used to describe fetuses with disproportionately small growth. Intrauterine growth restriction (IUGR) is used to designate a fetus that has not met its growth potential and is defined as estimated fetal weight (EFW) at or below the 10th percentile for gestational age. Small for gestational age (SGA) is a term that applies to the infant that is less than the 10th percentile at birth.
Pathogenesis
Approximately 70% of fetuses with EFW below the 10th percentile are simply constitutionally small; thus, the term IUGR is inaccurate for many fetuses. Distinguishing between normal and pathologic growth can be difficult, but a fetus with normal anatomy, normal amniotic fluid volume, and normal growth pattern over time will generally be constitutionally small rather than IUGR. Some nonpathologic factors that affect fetal birthweight are maternal height, paternal height, parity, ethnicity, and fetal sex.
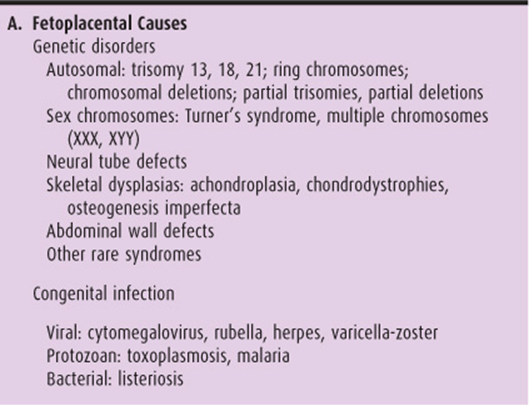
A classification of IUGR pregnancy delineated by cause is given in Table 16–3. Any inference of suboptimal growth requires, by definition, serial observations. It cannot be emphasized too strongly that a pregnancy cannot be described as IUGR unless the gestational age is known with certainty.
Table 16–3. Pathogenic classification of intrauterine growth restriction pregnancy.
Compared with an appropriate for gestational age (AGA) fetus, the IUGR fetus has altered body composition (including decreased body fat, total protein, whole body DNA and RNA, glycogen, and free fatty acids), altered distribution of weight among organs, and altered body proportions. Approximately 20% of IUGR infants are symmetrically small, with a relatively proportionate decrease in many organ weights. Eighty percent are asymmetrically small, with relative sparing of brain weight, especially when compared with that of the liver or thymus.
Numerous authors have differentiated between symmetric and asymmetric IUGR pregnancy in terms of cause and prognosis. Symmetric IUGR refers to infants in which all organs are decreased proportionally. Symmetric IUGR infants are more likely to have an endogenous defect that results in impairment of early fetal cellular hyperplasia. Symmetric IUGR infants have proportionately small brains, usually because of a decreased number of brain cells. Although this may be the result of early, severe nutritional deprivation, the cause is more often a genetic disorder, infection, or other problem. Usually the thymus is small, with an average decrease of 25%. This decrease may explain in part the decreased cellular immunity seen in IUGR infants.
Asymmetric IUGR refers to infants in which organs are decreased disproportionately (abdominal circumference is affected to a greater degree than is HC). Asymmetric IUGR more likely is caused by intrauterine deprivation that results in redistribution of flow to the brain and heart at the expense of less important organs, such as the liver and kidneys. In asymmetric IUGR infants, brain weight is decreased only slightly compared with that of AGA controls, primarily as a result of decreased brain cell size and not because of decreased brain cell numbers. Cerebral abnormalities include decreased myelination, decreased utilization of metabolic substrates other than glucose, and altered protein synthesis. In experimental animals, these changes are more likely to produce adverse effects in the brain stem and cerebellum. This differential sparing is particularly prominent when deprivation occurs in the latter half of pregnancy. Deprivation early in pregnancy is associated with less cerebral sparing and diffusely slowed brain growth.
Although this classification is helpful in establishing a differential diagnosis and framework for discussion, it is not sufficiently precise to serve as a basis for decisions regarding intervention or viability.
A number of etiologies have been shown to have an association with IUGR, either symmetric or asymmetric.
A. Fetoplacental Causes
1. Congenital abnormalities—Genetic disorders account for approximately one-third of IUGR infants. The frequency of IUGR in chromosomally abnormal infants ranges from 20 to 60%, and the risk of an IUGR infant having a major congenital anomaly is 10%. An infant with an autosomal trisomy is more likely to be IUGR. The most common trisomy is trisomy 21 (Down syndrome), with an incidence of 1.6 per 1000 live births. At term, such infants weigh an average of 350 g less than comparable normal infants and are 4 times more likely to be IUGR. This decrease is most apparent in the last 6 weeks of pregnancy. A similar decrease in birth-weight occurs in translocation Down syndrome, whereas mosaic Down syndrome is associated with an intermediate decrease in birthweight.
The second most common autosomal trisomy is trisomy 18 (Edwards’ syndrome), which occurs in 1 in 6000–8000 live births. Eighty-four percent of these infants are IUGR. Ultrasound evaluation may reveal associated anomalies. The condition is associated with an increased likelihood of breech presentation, polyhydramnios, fetal neural tube defects, and visceral anomalies. The average birthweight of infants with trisomy 18 is almost 1000 g less than that of controls. In contrast to the placental weight in infants with trisomies 13 and 21, the placental weight in infants with trisomy 18 also is markedly reduced.
Trisomy 13 occurs in 1 in 5000–10,000 live births. More than 50% of affected infants have IUGR. Birthweights average 700–800 g less than those of controls.
Other more rare autosomal chromosome abnormalities, such as ring chromosomes, deletions, and partial trisomies, are associated with an increased likelihood of IUGR. Sex chromosome abnormalities may be associated with lower birthweight. Extra X chromosomes (>2) are associated with a 200-g to 300-g decrease in birthweight for each extra X. Turner’s syndrome is associated with an average birthweight of approximately 400 g below average. Fetuses with mosaic Turner’s syndrome are intermediately affected.
Growth impairment as a result of fetal chromosome abnormalities usually occurs earlier than impairment caused by placental abnormalities. However, there is considerable clinical overlap, so gestational age at the time of diagnosis is not always of clinical value.
Fetuses with neural tube defects frequently are IUGR, weighing approximately 250 g less than controls. Anencephalic fetuses are IUGR, even considering the absent brain and skull, with average third-trimester birth-weights of approximately 1000 g less than matched controls. Certain dysmorphic syndromes are associated with an increased incidence of IUGR fetuses. Achondroplasia may be associated with low birthweight if either parent is affected but usually is associated with normal birthweight if a spontaneous mutation is the cause. Osteogenesis imperfecta consists of a spectrum of diseases, all of which result in IUGR fetuses.
Infants born with abdominal wall defects are characteristically IUGR, particularly those with gastroschisis.
Other autosomal recessive syndromes associated with IUGR include Smith-Lemli-Opitz syndrome, Meckel’s syndrome, Robert’s syndrome, Donohue’s syndrome, and Seckel’s syndrome. These conditions are rare and are most likely to be diagnosed antepartum in families with a previously affected child. Infants with renal anomalies such as renal agenesis (Potter’s syndrome) or complete urinary tract outflow obstruction often have IUGR.
Other congenital anomalies associated with an increased incidence of IUGR outcome are duodenal atresia and pancreatic agenesis.
2. Congenital infections—(See also Chapter 15, Congenital Fetal Infections, for more discussion.) Chronic intrauterine infection is responsible for 5–10% of IUGR pregnancies (Table 16–3). The most commonly identified pathogen is cytomegalovirus (CMV). Although CMV can be isolated from 0.5 to 2% of all newborns in the United States, clinically obvious infection at the time of birth affects only 0.2–2 in 1000 live births. Active fetoplacental infection is characterized by cytolysis, followed by secondary inflammation, fibrosis, and calcification. Only infants with clinically apparent infection at birth are likely to be IUGR. Signs of congenital infection are nonspecific but include central nervous system involvement (eg, microcephaly), chorioretinitis, intracranial (periventricular) calcifications, pneumonitis, hepatosplenomegaly, and thrombocytopenia.
Congenital rubella infection increases the risk of IUGR. Infection in the first trimester results in the most severely affected fetuses, primarily as a result of microvascular endothelial damage. Such infants are likely to have structural cardiovascular and central nervous system defects such as microcephaly, deafness, glaucoma, and cataracts.
Other viruses implicated in causing IUGR are herpesvirus, varicella-zoster virus, influenza virus, and poliovirus, but the number of such cases is small. As expected by virtue of their chronic, indolent nature, protozoan infections are associated with IUGR. The most common protozoan, Toxoplasma gondii, usually is acquired by ingestion of raw meat. Only women with a primary infection are at risk for having an affected infant. The average incidence is 1 in 1000 live births in the United States, but the incidence varies widely among locations and social populations. Approximately 20% of newborns with congenital toxoplasmosis will have IUGR. Malaria is another protozoan infection associated with IUGR.
Although bacterial infections occur commonly in pregnancy and frequently are implicated in premature delivery, they are not commonly associated with IUGR. Chronic infection from Listeria monocytogenes is an exception. Infants usually are critically ill at the time of delivery and often have encephalitis, pneumonitis, myocarditis, hepatosplenomegaly, jaundice, and petechiae.
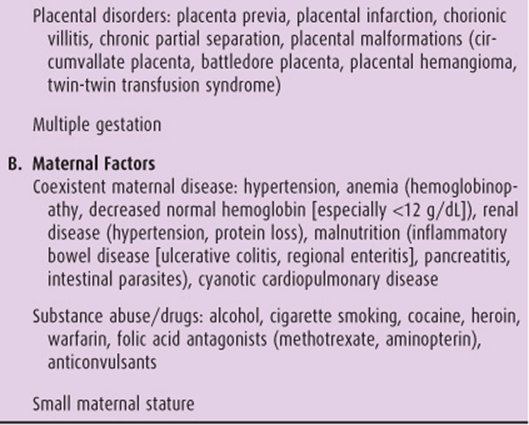
3. Placental factors—The placenta plays an important role in normal fetal growth. Placental weight has shown to be less with IUGR fetuses than with AGA fetuses, suggesting that appropriate fetal growth may depend on the size or weight of the placenta. Several placental abnormalities are associated with an increased likelihood of an IUGR fetus. Placenta previa is associated with an increased incidence of IUGR, probably because of the unfavorable site of placental implantation. Complete placenta previa is associated with a higher incidence of IUGR than is partial placenta previa. Decreased functional exchange area as a result of placental infarction also is associated with an increased incidence of IUGR fetuses. Premature placental separation or varying degrees of placental abruption may occur at any time during pregnancy, with variable effects. When not associated with fetal death or premature labor, premature placental separation may increase the risk of IUGR. Malformations of the placenta or umbilical cord, such as single umbilical artery (UA), velamentous umbilical cord insertion, circumvallate placenta, placental hemangioma, battledore placenta, and twin-twin transfusion syndrome, also are associated with an increased risk of IUGR. Chronic villitis, chronic inflammation of placental villi, is seen with increased frequency when the placentas of IUGR pregnancies are examined histologically. Finally, uterine anomalies may be associated with impaired fetal growth, primarily because of suboptimal uterine blood flow.
4. Multiple gestation—Multiple gestation has long been associated with premature delivery. However, it also is associated with a 20–30% increased incidence of IUGR fetuses, most often as a result of placental insufficiency, twin-twin transfusion syndrome, preeclampsia, or anomalies. Fetal growth has a direct relationship to the number of fetuses present and the type of placentation (monochorionic vs. dichorionic). Serial ultrasound estimates of fetal weights should be considered in a multiple gestation pregnancy.
B. Maternal Factors
Numerous maternal diseases are associated with suboptimal fetal growth. Any woman who has borne 1 IUGR fetus is at increased risk for recurrence, with a 2-fold and 4-fold increased risk for IUGR birth after 1 or 2 IUGR births, respectively.
1. Hypertension—Hypertension is the most common maternal complication causing IUGR. Systemic hypertension results in decreased blood flow through the spiral arterioles and decreased delivery of oxygen and nutrients to the placenta and fetus. Hypertension may be associated with placental infarction.
2. Drugs—Both social drugs and prescribed medications can affect fetal growth. Alcohol use has long been known to be associated with impaired fetal growth. Virtually all infants with fetal alcohol syndrome exhibit signs of growth restriction.
Cigarette smoking is much more common among women of childbearing age in the United States than is alcoholism. Smoking causes one-third of IUGR cases and is the single most preventable cause of IUGR pregnancy in the United States today. Women who smoke have a 3-fold to 4-fold increase in IUGR infants. Birthweight is reduced by approximately 200 g, with the amount of growth restriction proportional to the number of cigarettes smoked per day. Women who quit smoking at 7 months’ gestation have newborns with higher mean birthweights than do women who smoke throughout the entire pregnancy. Women who stop smoking before 16 weeks’ gestation are not at increased risk for having an IUGR fetus.
Heroin and cocaine are also associated with an increased risk of IUGR, but confounding variables make determination of a direct cause-and-effect relationship difficult. Methadone use has not been shown to be associated with an increased incidence of IUGR.
Pharmacologic agents have been associated with an increased incidence of IUGR, primarily as a result of teratogenic effects. Warfarin has been associated with an increased incidence of IUGR, primarily as a result of the sequelae of intrauterine hemorrhage. Folic acid antagonists are associated with an increased risk of spontaneous abortion stillbirth, severe malformations, and IUGR.
IUGR fetuses are more common with maternally administered immunosuppressive drugs (eg, cyclosporine, azathioprine, corticosteroids), but when controlled for the underlying maternal disease, the medications per se probably have little effect on fetal growth. Furthermore, β-blockers are also associated with an increased risk of IUGR.
3. Malnutrition and malabsorption—Maternal weight at birth, prepregnancy weight, and weight gain during pregnancy account for 10% of the variance in fetal weight and increase the risk of delivering an infant <2500 g. Studies of infants borne by women who were pregnant during the Siege of Leningrad during World War II showed that daily intake must be reduced to <1500 kcal/d before a measurable effect on birthweight becomes evident. Maternal malabsorption may predispose to IUGR pregnancy. The most common clinical situations are inflammatory bowel disease (ulcerative colitis or regional enteritis), pancreatitis, and intestinal parasites. Maternal eating disorders such as bulimia and anorexia are also associated with IUGR.
4. Vascular disease and hypoxemia—Diseases that affect maternal microvascular perfusion can be associated with IUGR. These include collagen vascular disease, insulin-dependent diabetes mellitus associated with microvasculopathy, and preeclampsia. Also, chronic maternal hypoxemia due to pulmonary disease or cyanotic heart disease is associated with growth restriction.
5. Maternal features—A small woman may have a smaller-than-normal infant because of reduced growth potential. These mothers and infants are completely normal and healthy, but they are constitutionally small because of genetic variation. The ponderal index (PI) can be used to evaluate whether an infant is simply constitutionally small or is affected by IUGR. The PI is calculated using the following formula:
PI = [Weight (in g) × 100]/[length (in cm)]3
Infants affected by asymmetric IUGR will have a low PI (ie, they will be long, lightweight infants with a PI below the 10th percentile), whereas small normal infants will have a normal PI.
Women who were SGA at birth have a 2-fold increase in risk of IUGR in their offspring.
Maternal parity exerts a modest effect on birthweight. First-born infants tend to be smaller and more often categorized as IUGR. This effect decreases with successive deliveries and is not seen beyond the third birth.
6. Sex of fetus—At term, female fetuses are an average 5% (150 g) smaller and 2% (1 cm) shorter than male fetuses. Referring to separate norms for male and female fetuses may increase the power of biometry in assessing IUGR.
Prevention
Because many causes of IUGR are not preventable, few interventions have proved effective for prevention. Interventions that have shown benefit include smoking cessation, antimalarial chemoprophylaxis, and balanced protein and energy supplementation. Smoking is the single most common preventable cause of IUGR in infants born in the United States. As discussed in Maternal Factors, women who quit smoking at 7 months’ gestation have newborns with higher mean birthweights than do women who smoke throughout the pregnancy. Women who quit smoking before 16 weeks’ gestation are not at any increased risk for an IUGR infant. Limited data suggest that balanced nutritional supplementation improves mean birthweight. As expected, such supplementation more likely will benefit those with poor nutrition or adolescent pregnancies. Pregnant women should avoid close contact with individuals known to be infected or colonized with rubella virus or CMV. Nonpregnant women of reproductive age should be tested for immunity to rubella virus and, if susceptible, should be immunized prior to conception. Currently no vaccine exists for CMV.
Women of childbearing age should be tested for immunity to T gondii if this protozoan infection is clinically suspected. If the woman is immune, her risk of having an affected infant is remote. However, if she is susceptible, she should be cautioned to avoid cat feces and uncooked meat. If the screening immunoglobulin M (IgM) for Toxoplasma is positive, no action should be taken based on this result without confirmation by a regional reference laboratory with expertise in Toxoplasma testing.
Therapeutic medications are not a major cause of IUGR pregnancy, but benefits and risks should be weighed whenever medications are prescribed. Any woman of childbearing age should be questioned about the possibility of pregnancy before receiving therapeutic or diagnostic radiation to the pelvis.
Placental factors causing IUGR pregnancies are not generally preventable. It has been postulated that low-dose aspirin and dipyridamole may increase prostacyclin production in certain patients and thus prevent idiopathic uteroplacental insufficiency. The role of these agents in preventing IUGR resulting from placental insufficiency in at-risk populations is unclear at this time.
Preventive measures for the maternal diseases listed in Table 16–3 are beyond the scope of this chapter. Treatment of many of these conditions may decrease the likelihood of IUGR pregnancy. Treatment of hypertension has a positive effect on birthweight, at least in the third trimester. However, strict bed rest and hospitalization do not seem to have any beneficial effects for patients with a history of hypertension. Although a complex issue, protein supplements for patients with significant proteinuria may increase the amount of protein available for placental transfer. Correction of maternal anemia (of whatever cause) improves oxygen delivery to the fetus, thus improving fetal growth. However, routine supplements, such as with iron, have not been shown to be associated with any altered clinical outcomes.
Treatment of malabsorption syndrome (of whatever cause) can be expected to improve nutrient absorption and subsequent nutrient transfer to the fetus. Inflammatory bowel disease should be treated if required, but if possible, pregnancy should be deferred until the disease has been quiescent for approximately 6 months. Intestinal parasites should be appropriately treated and negative cultures confirmed prior to pregnancy.
Clinical Findings
A. Ultrasound Evaluation of Estimated Fetal Weight
The diagnosis of IUGR is made when biometric parameters on ultrasound indicate that the EFW is less than the 10th percentile for gestational age. In any pregnancy at risk for IUGR, baseline ultrasound studies should be obtained early in gestation. Careful attention should always be given to gestational dating (menstrual history, serial examinations, biochemical pregnancy testing, quickening, ultrasound). An IUGR outcome, however, may develop in pregnancies without identified risk factors. For some pregnancies, the first sign of IUGR may be a lagging fundal height on clinical examination. If the fundal height varies from the assigned gestational age by more than 2 cm, ultrasound is indicated to assess the EFW and amniotic fluid volume. Careful attention to fundal height measurement is associated with 46–86% sensitivity for detecting IUGR.
Ultrasound examination early in pregnancy is accurate in establishing the estimated date of confinement (EDC) and may sometimes identify genetic or congenital causes of IUGR pregnancy. Serial ultrasound examinations are important in documenting growth and excluding anomalies. An antenatal diagnosis of IUGR is not precise given that EFW cannot be measured directly and must be calculated from a combination of directly measured parameters. Overall prediction of weight via birthweight formulas can have a 10–20% error rate. Selection of the most useful biometric parameter depends on the timing of measurements. The crown–rump length is the best parameter for dating of pregnancy in the first trimester. The biparietal diameter (BPD) and HC are most accurate in the second trimester, with a margin of error of 7–11 days for BPD and 3–5 days for HC. HC is more useful in establishing gestational age in the third trimester because BPD loses its accuracy secondary to variations in shape. Abdominal circumference measurement is the single most sensitive measurement for evaluating fetal growth restriction. The fetal abdominal circumference reflects the volume of fetal subcutaneous fat and the size of the liver, which in turn correlates with the degree of fetal nutrition. Acidemia and hypoxemia are more common when the abdominal circumference is below the 5th percentile for gestational age.
The femur length is not helpful for identifying IUGR but can identify skeletal dysplasia. Because the definition of IUGR ultimately depends on birthweight and gestational age criteria, formulas that optimally predict birthweight in a given population will be the most important contributor to ultrasonographic criteria.
Fetuses from different populations show different growth patterns. The growth curves developed by Battaglia and Lubchenco in the 1960s do not reflect the variation in birthweight for various ethnic populations. The growth curves used today also do not reflect the median birthweight increase over the last 3 decades. Racial and ethnic anthropometric variations may suggest a need for specific charts for different communities.
Differential Diagnosis
If the fundal height on clinical examination is small, other diagnoses that should be entertained are oligohydramnios or a healthy pregnancy with the wrong due date (ie, the true gestational age is earlier than assigned). Ultrasound can help to differentiate among these diagnoses.
Complications
Numerous maternal and perinatal complications have been associated with IUGR pregnancies (Table 16–1). Underlying maternal disease is more likely to be present (Table 16–3), and these women require more intensive prenatal care. Premature labor or preeclampsia is more common. IUGR fetuses at any gestational age are less likely to tolerate labor well, and the need for operative delivery is increased.
Perinatal morbidity and mortality are significantly increased in low-birthweight infants, with an inverse relationship between neonatal weight and perinatal mortality. At any given gestational age, IUGR neonates have a higher mortality than do AGA neonates. However, at any given birthweight, outcomes are similar for IUGR and AGA neonates. Perinatal morbidity and mortality are especially increased in infants born at term with birthweights at or below the 3rd percentile. Increased risk of mortality is affected by the primary etiology of growth restriction and may be modified by the severity and progression of maternal factors (eg, hypertension control). With the advent of fetal surveillance, the perinatal mortality rate associated with IUGR has decreased to 2–3 times that of the AGA population. The past decade has witnessed increased attention to minimizing the perinatal complications of surviving IUGR neonates. With continued improvements in antenatal surveillance and neonatal care, the perinatal mortality rate for IUGR pregnancies in most centers now is 1.5–2 times that of the AGA population. Unfortunately, this rate likely will not reach that of the AGA population in the near future because of the persistent occurrence of lethal anomalies and severe congenital infections.
IUGR fetuses are at risk for in utero complications, including hypoxia and metabolic acidosis, which may occur at any time but are more likely to occur during labor. Up to 50% of growth-restricted fetuses exhibit abnormal fetal heart rate patterns, most often variable decelerations. Hypoxia is the result of increasing fetal oxygen requirements during pregnancy, with a rapid increase during the third trimester. If the fetus receives inadequate oxygen, hypoxia and subsequent metabolic acidosis will ensue. If undetected or untreated, this condition will lead to decreased glycogen and fat stores, ischemic end-organ damage, meconium-stained amniotic fluid, and oligohydramnios, eventually resulting in vital organ damage and intrauterine death.
IUGR infants are at increased risk for neonatal complications, including meconium aspiration syndrome, low Apgar scores, UA pH <7.0, need for intubation in the delivery room, seizures, sepsis, polycythemia, hypoglycemia, hypocalcemia, temperature instability, apneic episodes, and neonatal death. All IUGR infants require a thorough postnatal evaluation for congenital anomalies.
Treatment
The initial evaluation of the fetus suspected to be growth restricted involves:
• Evaluation for other evidence of fetal compromise. Depending on the gestational age, this may involve performing a biophysical profile and Doppler studies of umbilical and fetal vessels (see below for more details).
• Detailed fetal anatomic survey by ultrasound.
• Detailed maternal history for any evidence of recent infection, medication or drug exposure, any maternal medical disorders that are associated with IUGR such as hypertension, or any history of IUGR in a prior pregnancy.
• Physical examination and laboratory testing for any evidence of preeclampsia.
• Maternal serum testing for viral and parasitic infections if there is a history suggestive of recent infection.
The role of maternal evaluation for inherited and acquired thrombophilia is controversial in these patients. Studies have not demonstrated a consistent link between maternal thrombophilia and IUGR. If an association exists, it is likely a weak one.
Depending on the findings, consideration may be given to fetal karyotyping via genetic amniocentesis if IUGR presents prior to the third trimester and severe growth restriction is suspected (ie, EFW <3rd percentile). Amniocentesis should also be considered for karyotyping if any structural malformations are found or if there is polyhydramnios. Amniocentesis may also be performed to assess for pulmonary maturity for selected fetuses.
Treatment of IUGR pregnancy presupposes an accurate diagnosis. Even with the history, physical examination, and ultrasound examination, an accurate diagnosis remains difficult, and some IUGR pregnancies will not be detected. Conversely, some fetuses suspected to be growth restricted may have a normal birth weight or may be found to be constitutionally small.
All pregnant women who are smoking should be advised to discontinue cigarette smoking as well as use of alcohol and all recreational drugs. Although bed rest often is recommended, no evidence shows that bed rest results in improved outcome or increased fetal birthweight for fetuses with suspected IUGR. The increased uterine blood flow that occurs when the patient is in the lateral recumbent position theoretically may result in some benefit for fetuses with asymmetric IUGR. However, data do not support this theory.
Because IUGR fetuses are at risk for antepartum or intrapartum compromise, they should be followed carefully. The goal of fetal surveillance is to identify those fetuses at greatest risk of stillbirth and neonatal morbidity related to acidosis who may benefit from preterm delivery. The best method for monitoring a fetus with suspected IUGR is not well established; however, it typically involves ultrasound for biophysical profile and Doppler studies of umbilical and fetal vessels.
• The biophysical profile (BPP) is useful for assessing fetal well-being. With a normal BPP score, the risk of fetal asphyxia in the following week is low (approximately 1 in 1000). As part of the BPP, the amniotic fluid volume is assessed. Decreased amniotic fluid volume is clinically associated with IUGR. This finding is thought to result from decreased perfusion of the fetal kidneys, which leads to decreased urine production. Oligohydramnios, defined as a maximum vertical pocket of fluid <2 cm or amniotic fluid index of <5 cm, may be seen with IUGR infants, but the presence of a normal amniotic fluid index should not preclude the diagnosis of IUGR.
• Umbilical artery (UA) Doppler velocimetry can be used to estimate the likelihood of adverse perinatal outcome and is useful in determining the intensity of fetal surveillance. Placental circulatory insufficiency is associated with increased placental resistance, which is associated with decreased maternofetal oxygen transfer. This increase in placental resistance is manifested by a fall in forward blood flow through the UA due to increased downstream impedance. During the compensated stage, diastolic flow in the UA is reduced or absent. Reversal of diastolic flow in the UA is a sign of severe hypoxemia and acidemia. Although the use of UA Doppler studies for general population screening remains unproven, it is recommended as the primary method of surveillance for already identified IUGR fetuses. Doppler flow studies, in particular the systolic-to-diastolic ratio (S/D ratio), helps reduce unnecessary interventions and improve overall fetal outcome (including reducing the risk of perinatal death) in IUGR pregnancies. A recent study showed that of fetuses with suspected IUGR evaluated by Doppler studies, none of those with normal UA Doppler flow measurements were delivered with metabolic acidemia. This finding suggests that intense antenatal surveillance may be unnecessary in a fetus with a normal UA S/D ratio and normal amniotic fluid index. Abnormal UA flow is associated with an increased risk of caesarean or operative delivery.
• In fetuses with suspected IUGR, abnormal middle cerebral artery (MCA) Doppler studies and UA S/D ratios are strongly associated with low gestational age at delivery, low birthweight, and low UA pH. Also, mean birth-weight, interval to delivery, need for emergent delivery, and occurrence of fetal distress all are related to the severity of abnormal Doppler findings after correction for gestational age. Abnormal Doppler cerebroplacental ratio (MCA pulsatile index divided by UA pulsatile index) also has been associated with a statistically significant increase in perinatal morbidity and mortality. Respiratory distress syndrome and intracranial hemorrhage are not associated with abnormal Doppler studies.
• Doppler studies of other fetal vessels such as the descending aorta, inferior vena cava, and ductus venosus have also been shown to correlate with fetal acidosis and risk of demise.
In addition to fetal kick counts, antepartum testing with BPP and UA Doppler are recommended once or twice per week for the fetus with suspected IUGR. The significance of abnormal UA Doppler results can be clarified by investigations of MCA circulation and Doppler studies of venous structures, including the ductus venosus.
Ultrasound examinations to assess adequacy of fetal growth should be performed at least every 3–4 weeks. Measurements should include BPD, HC, abdominal circumference, and femur length, especially in patients in whom an asymmetric IUGR fetus is suspected. Probably the most sensitive index of an asymmetric IUGR fetus is the abdominal circumference. The femur length/abdominal circumference ratio is a gestational age–independent ratio (normal 0.20–0.24). Asymmetric IUGR fetuses generally have a ratio >0.24.
Every IUGR pregnancy must be individually assessed for the optimal time of delivery (ie, the point at which the baby will do as well or better outside the uterus than inside). This would be whenever surveillance indicates fetal maturity, fetal compromise, or gestational age of 37–38 weeks (beyond which time there is no advantage to an IUGR fetus remaining in utero). Data are conflicting as to whether IUGR accelerates pulmonary maturity. Therefore, the current recommendation is to administer glucocorticoids to women likely to deliver before 34 weeks, as would be done with any other pregnancy.
IUGR pregnancies are at increased risk for intrapartum problems, so whenever possible, delivery should take place in a center where appropriate obstetric care, anesthesia, and neonatal care are readily available. Caesarean delivery may be necessary, and the presence of meconium-stained amniotic fluid or a compromised infant should be anticipated.
The mode of delivery must be individualized. Caesarean delivery is often indicated, especially when fetal monitoring reveals evidence of fetal compromise, malpresentation, or situations where traumatic vaginal delivery might be expected.
Continuous electronic fetal heart rate monitoring should be performed during labor in all cases, even if recent ante-partum testing has been reassuring. Arteriovenous cord blood gas determinations also are useful; as many as 50% of IUGR infants have some degree of metabolic acidosis. Minimization of anesthesia is generally preferable, but controlled epidural anesthesia usually is safe. Maternal hypotension or hypovolemia must be avoided.
Prognosis
An IUGR pregnancy per se is not considered life-threatening for the mother. However, increased maternal morbidity and mortality may result from an underlying condition (eg, hypertension or renal disease). Most women who deliver IUGR infants can be expected to have long-term prognoses equivalent to those of women delivering AGA infants.
Infants with a low birthweight have a relatively high morbidity and mortality. Short-term morbidity includes impaired thermoregulation, hypoglycemia, polycythemia, and impaired immune function. Studies have shown that the rate of neonatal death, Apgar score at 5 minutes <3, UA pH <7.0, seizures during the first day of life, and incidence of intubation are significantly increased when the fetus is at or below the 3rd percentile for birthweight.
As for long-term prognosis for the infant, reports of national survey data show that IUGR infants appear to catch up in weight in the first 6 months of life. However, IUGR infants tend to remain physically small and are shorter, lighter, and have smaller HCs than do AGA infants.
Taken as a group, IUGR infants have more neurologic and intellectual deficits than do their AGA peers. IUGR infants have lower IQs as well as a higher incidence of learning and behavioral problems. Major neurologic handicaps, such as severe mental retardation, cerebral palsy, and seizures, are more common in IUGR infants. The incidence of sudden infant death syndrome (SIDS) is increased in IUGR infants, who account for 30% of all SIDS cases. Adults who were IUGR at birth are at higher risk for developing ischemic heart disease and related disorders, including hypertension, stroke, diabetes, and hypercholesterolemia.
Alfirevic Z, Stampalija T, Gyte GM. Fetal and umbilical Doppler ultrasound in high risk pregnancies. Cochrane Database Syst Rev 2010;1:CD007529. PMID: 20091637.
American College of Obstetricians and Gynecologists. Clinical Management Guidelines: Intrauterine Growth Restriction. ACOG Practice Bulletin No. 12. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
Baschat AA, Galan HL, Bhide A, et al. Doppler and biophysical assessment in growth restricted fetuses: Distribution of test results. Ultrasound Obstet Gynecol 2006;27:41. PMID: 16323151.
Berghella V. Prevention of recurrent fetal growth restriction. Obstet Gynecol 2007;110:904. PMID: 17906027.
Lunde A, Melve KK, Gjessing HK, et al. Genetic and environmental influences on birth weight, birth length, head circumference, and gestational age by use of population based parent offspring date. Am J Epidemiol2007;165:734. PMID: 17311798.
Zhang J, Merialdi M, Platt LD, et al. Defining normal and abnormal fetal growth: Promises and challenges. Am J Obstet Gynecol 2010;202:522. PMID: 20074690.
LARGE FOR GESTATIONAL AGE PREGNANCY
ESSENTIALS OF DIAGNOSIS
![]() EFW greater than the 90th percentile for gestational age on ultrasound.
EFW greater than the 90th percentile for gestational age on ultrasound.
![]() Macrosomia represents a subset of LGA fetuses weighing >4500 g.
Macrosomia represents a subset of LGA fetuses weighing >4500 g.
Although the large for gestational age (LGA) fetus is defined according to the same concept as the IUGR fetus (LGA = heaviest 10% of newborns), LGA pregnancy has received substantially less attention since it is generally associated with fewer maternal and fetal complications than IUGR. Large for gestational age is defined as EFW above the 90th percentile for any specific gestational age. Macrosomiagenerally refers to fetuses with an EFW of at least 4500 g regardless of the gestational age; fetuses that are >4500 g are >95th percentile at any gestational age and therefore represent an extreme subset of LGA fetuses. The risk of morbidity is greater for infants born weighing between 4000 and 4500 g compared to the average population. However, the risk of infant morbidity is substantially increased at birthweights greater than 4500 g. Although there are numerous reports and studies regarding macrosomia, few data regarding LGA as defined here are available. Therefore, this section concentrates on fetal macrosomia, with additional comments regarding LGA pregnancies.
Pathogenesis
Numerous endocrinologic changes occur during pregnancy to ensure an adequate fetal glucose supply. In the second half of pregnancy, increased concentrations of human placental lactogen, free and total cortisol, and prolactin combine to produce modest maternal insulin resistance, which is countered by postprandial hyperinsulinemia. In those who are unable to mount this hyperinsulinemic response, relative hyperglycemia may develop (ie, gestational diabetes). Because glucose crosses the placenta by facilitated diffusion, fetal hyperglycemia ensues. This in turn produces fetal hyperinsulinemia with resultant intracellular transfer of glucose, leading to fetal macrosomia.
Factors that predispose to LGA pregnancy are listed in Table 16–4. As with IUGR pregnancy, diagnosis of LGA pregnancy depends on knowing with certainty the gestational age of the fetus.
Table 16–4. Factors that may predispose to fetal macrosomia or large for gestational age (LGA) pregnancy.
A. Maternal Diabetes
Maternal diabetes, whether gestational, chemical, or insulin dependent, is the condition classically associated with fetal macrosomia. The “Pedersen hypothesis” was long assumed to account for fetal macrosomia, that is, the condition was the result of inadequate management of diabetes during pregnancy. Initial reports suggested that careful control of blood glucose level in insulin-dependent diabetic women would prevent fetal macrosomia, but recent studies have suggested that the problem is not so simple and that the incidence may correlate better with cord blood concentrations of maternally acquired anti-insulin immunoglobulin G (IgG) antibodies and/or increased serum levels of free fatty acids, triglycerides, and the amino acids alanine, serine, and isoleucine. Cord serum epidermal growth factor concentrations also have been found to be higher than normal in pregnancies complicated by prepregnancy diabetes and gestational diabetes.
A significant correlation exists between plasma leptin levels and neonatal birthweight, which suggests that leptin levels are directly related to the quantity of body fat tissue in fetal macrosomia.
B. Maternal Obesity
Maternal obesity is associated with a 3- to 4-fold increased likelihood of fetal macrosomia. The increased risk of macrosomia associated with maternal obesity appears to be independent of comorbidities such as gestational or pregestational diabetes.
C. Postdatism
Prolonged pregnancy is more likely to result in a macro-somic fetus, presumably because of continued delivery of nutrients and oxygen to the fetus.
D. Genetic and Congenital Disorders
Several genetic and congenital syndromes are associated with an increased incidence of macrosomia. Beckwith-Wiedemann syndrome is frequently associated with fetal macrosomia, usually because of pancreatic islet cell hyperplasia (nesidioblastosis). Affected infants usually have hypoglycemia, macroglossia, and omphalocele. They also may have intestinal malrotation or visceromegaly. Although usually a sporadic event, other inheritance patterns have been suggested in a few families. Other rare syndromes include Weaver’s syndrome, Sotos’ syndrome, Nevo’s syndrome, Ruvalcaba-Myhre syndrome, and Marshall’s syndrome. Carpenter’s syndrome and fragile X syndrome may be associated with an increased incidence of LGA infants.
E. Constitutionally Large Fetus
Fetuses who are suspected of being LGA may simply be large secondary to constitutional factors. Large maternal stature should be considered as contributing to macrosomia because birthweight tends to correlate more closely with maternal height than maternal weight. Male fetuses are more likely to be considered LGA because male fetuses are an average of 150 g heavier than appropriately matched female fetuses at each gestational week during late pregnancy. Series addressing fetal macrosomia generally report an increased incidence of male fetuses, usually approximately 60–65%. One recent study showed that male fetuses were twice as likely to be diagnosed with macrosomia as compared with female fetuses.
F. Maternal Weight Gain
Excessive maternal weight gain in pregnancy is associated with macrosomia. A weight gain of more than 40 lb significantly increased the incidence of macrosomia by an odds ratio of 3.3.
Prevention
Prevention of macrosomia and ensuing complications requires early detection of risk factors. Risk factors for having a macrosomic infant include multiparity, advanced maternal age, and previous delivery of a macrosomic infant. When controlled for gestational age and fetal gender, the average birthweight with successive pregnancies increases by 80–120 g up to the fifth pregnancy. Multiparity is also associated with other risk factors (eg, obesity, diabetes) and therefore may be a confounding variable. Advanced maternal age also contributes to increased birthweight. However, as with multiparity, it is also associated with obesity and diabetes.
Consideration should be given to evaluating patients with the risk factors noted in Table 16–4 for possible fetal macrosomia with an ultrasound estimate of fetal size and weight.
For patients with gestational or pregestational diabetes, adequate control of maternal glucose levels is thought to prevent the development of macrosomia, although neonatal complications despite excellent metabolic control have been reported. Prepregnancy weight and degree of weight gain are strong indicators for macrosomia regardless of glycemic control. However, the rates of macrosomia and complications are reduced overall when postprandial levels are monitored. Studies have shown that the risk of macrosomia is reduced to near normal in diabetic women who monitor 1-hour postprandial glucose levels and that 1-hour postprandial glucose levels are directly related to fetal abdominal circumference values. One study showed that when postprandial glucose levels were kept below 104 mg/dL, macrosomia rates of diabetic women were similar to those of nondiabetics. Chapter 31 reviews diabetes and pregnancy in more detail.
Infants of women who participate in regular aerobic exercise programs have lower average birthweights compared with infants in the general population but no demonstrable adverse effects. To date, no studies have evaluated the potential efficacy of exercise programs as a means of decreasing birthweight in women at risk for LGA pregnancy.
Clinical Findings
The first sign of macrosomia may be detected when the fundal height measurement on clinical examination exceeds the margin of error (>3 cm) for that gestational age. A diagnosis of macrosomia is made when the EFW on ultrasound (as determined by measurements of the HC, BPD, abdominal circumference, and femur length) exceeds 4500 g. Nonetheless, EFW by ultrasound is not very accurate. More than 30 different formulas for EFW calculation have been proposed, attesting to the inadequacy of each individual method. No single formula has been consistently better than the others. Even in skillful hands, the error of fetal weight estimates by ultrasound is 10–20%. One review of ultrasonographic diagnosis of macrosomia shows sensitivity ranging from 24 to 88% and specificity from 60 to 98%. The margin of error in estimating fetal weight means that the EFW by ultrasound must be at least 4750 g in order to predict a birthweight of 4000 g with a confidence interval of 90%. The best single measurement in evaluating macrosomia in diabetic mothers is abdominal circumference. An initial abdominal circumference above the 70th percentile is significantly associated with subsequent delivery of an LGA infant. Fetal body composition and fetal shoulder width cannot be accurately assessed by ultrasound.
Differential Diagnosis
If the fundal height on clinical examination is increased, the differential diagnosis includes polyhydramnios, fetal structural abnormality (such as sacrococcygeal teratoma), and undiagnosed multiple gestation in addition to macrosomia or LGA fetus. Ultrasound can differentiate among these diagnoses.
Complications
Macrosomic pregnancies are at increased risk for many fetal and maternal complications (Table 16–2). Macrosomic pregnancies are more likely to require caesarean delivery, usually because of failure to progress. In particular, primigravidas delivering a macrosomic infant are at increased risk for complications such as prolonged labor, postpartum hemorrhage, operative vaginal delivery, and emergency caesarean section as compared to delivering a normal weight infant. Primigravidas also have a higher risk of these complications compared with multiparous women delivering a macrosomic infant. Fetal distress, as determined by electronic fetal monitoring, is not more common in macrosomic pregnancies.
Shoulder dystocia occurs in 5–24% of vaginally delivered macrosomic fetuses. The incidence of shoulder dystocia correlates not only with increasing fetal weight but also with increasing chest circumference to HC. Shoulder dystocia of macrosomic infants also is related to maternal stature, but the association is not as clear. Approximately 10–15% of infants with shoulder dystocia experience brachial plexus injury; facial nerve injury and fractures of the humerus or clavicle also may be seen.
The risk of fetal brachial plexus injury in macrosomic infants delivered vaginally is 0.3–4%. Brachial plexus injury with shoulder dystocia is approximately 7% in infants whose birthweights exceed 4000 g but is 14% for mothers with gestational diabetes. The doubled risk may be secondary to increased fetal abdominal obesity in diabetic mothers. In diabetic patients, a correlation exists between the level of fetal truncal asymmetry (abdominal circumference/BPD ratio) as measured by ultrasound and the incidence and severity of shoulder dystocia. In addition to macrosomia, risk factors for shoulder dystocia include previous shoulder dystocia and maternal diabetes (3- to 4-fold increase compared to nondiabetic mothers). Lesser risk factors that are mediated through fetal size include previous delivery of a large fetus and excessive maternal weight gain during pregnancy. The risk of shoulder dystocia is similar in primigravidas and multigravidas delivering macrosomic infants.
Perineal trauma is more likely with a macrosomic pregnancy and is related to an increased incidence of shoulder dystocia and operative vaginal delivery. Vaginal delivery of a macrosomic infant increases by 5-fold the risk of third- or fourth-degree laceration.
Although gestational diabetes and postdatism predispose to fetal macrosomia, no evidence indicates that fetal macrosomia or an LGA fetus predisposes to gestational diabetes or postdatism.
The incidence of stillbirth remains higher in macrosomic fetuses than in controls of average weight. This problem has persisted even with the availability of fetal monitoring and presumably reflects the increased incidence of maternal diabetes and postdatism. Stillbirths are known to be increased in nonanomalous diabetic mothers, but the cause is not understood. Additionally, excessive prepregnancy weight is an independent risk factor for unexplained death. In fact, large fetal macrosomia is significantly associated with unexplained fetal death even after controlling for maternal age, diabetes, and hypertension.
Many of the neonatal complications of fetal macrosomia are the result of underlying maternal diabetes or birth trauma and include low Apgar scores, hypoglycemia, hypocalcemia, polycythemia, jaundice, and feeding difficulties. LGA infants have significantly higher absolute nucleated red blood cell counts, lymphocyte counts, and packed cell volumes. These hematologic abnormalities are the same for all LGA infants regardless of whether they are infants of nondiabetic mothers, insulin-dependent diabetic mothers, or non–insulin-dependent gestational diabetics. This situation is believed to reflect a compensatory increase in erythropoiesis as a result of chronic intrauterine hypoxia resulting from increased placental oxygen consumption and decreased fetal oxygen delivery.
LGA infants of diabetic mothers have an increased incidence of cardiac septal hypertrophy.
Treatment
Labor induction for suspected macrosomia has not been shown to reduce the risk of shoulder dystocia, and caesarean delivery reducing the incidence of fetal macrosomia and intrapartum complications remains an unproven hypothesis.
Several published reviews of fetal macrosomia suggest routine caesarean delivery for fetuses with estimated weights of 5000 g or more (or estimated weights ≥4500 g in diabetic pregnancies). This suggestion is based in part on the data given in Table 16–2 and in part on anthropometric studies suggesting that very macrosomic fetuses have bisacromial circumferences in excess of HCs. Because of current limitations in the sensitivity and specificity of ultrasound-derived fetal weight calculations, decisions regarding scheduled abdominal delivery must be partially based on clinical grounds. Such considerations are particularly warranted in women who are obese or are diabetic or in postdate pregnancies. Maternal age and maternal preference also should be considered when deciding on delivery method.
Intrapartum management considerations center on close observation of the patient’s labor curve and avoidance of interventions that may be associated with an increased likelihood of traumatic vaginal delivery. Although data are conflicting, some studies have shown that patients with a protracted active phase of labor are more likely to experience shoulder dystocia. Close attention to a patient’s progress during labor may help detect this risk factor for shoulder dystocia. Furthermore, vacuum-assisted vaginal delivery increases the risk of shoulder dystocia. If the estimate of fetal weight is greater than 4000 g, the vacuum should be avoided if the second stage is prolonged, and in general, the vacuum should be used with caution. Because of these factors, women at risk for macrosomic or LGA babies should deliver in facilities where adequate obstetric care, pediatric care, and anesthesia are available. Large-bore intravenous access must be established, and blood must be available. Delivery should occur in a setting where immediate operation can be accomplished.
Prognosis
Any woman who delivers an LGA baby should be informed that the risk of her having another LGA baby is increased by 2.5- to 4-fold. Such women should be screened for previously undiagnosed chemical or insulin-dependent diabetes and, even if screening is negative, should be followed carefully in any subsequent pregnancy to rule out gestational diabetes.
Obese women should be strongly encouraged to lose weight prior to becoming pregnant. Any woman who has delivered an LGA infant should be encouraged to seek early care for any subsequent pregnancy, if for no other reason than early confirmation of the EDC, which can minimize the likelihood of subsequent postdatism. Women who deliver an LGA infant with an underlying genetic or congenital disorder should receive genetic counseling regarding recurrence risks and the feasibility of antepartum diagnosis.
In addition to the many neonatal complications previously noted, infants of mothers with gestational or pregestational diabetes are at increased risk for subsequent obesity, type 2 diabetes, or both. Infants who suffer from neonatal complications are at increased risk for subsequent neurologic or behavioral problems.
American College of Obstetricians and Gynecologists. Clinical Management Guidelines: Fetal Macrosomia. ACOG Practice Bulletin No. 22. Washington, DC: American College of Obstetricians and Gynecologists; 2010.