Melissa C. Bush, MD
Martin L. Pernoll, MD
ESSENTIALS OF DIAGNOSIS
![]() The incidence of multiple gestations has risen significantly over several decades, primarily due to increased use of fertility drugs for ovulation induction, superovulation, and assisted reproductive technologies (ART), such as in vitro fertilization (IVF).
The incidence of multiple gestations has risen significantly over several decades, primarily due to increased use of fertility drugs for ovulation induction, superovulation, and assisted reproductive technologies (ART), such as in vitro fertilization (IVF).
![]() Compared with singleton pregnancies, twin pregnancies are more likely to be complicated by hypertensive disorders, gestational diabetes mellitus, anemia, preterm birth, ante- and postpartum hemorrhage, and maternal death.
Compared with singleton pregnancies, twin pregnancies are more likely to be complicated by hypertensive disorders, gestational diabetes mellitus, anemia, preterm birth, ante- and postpartum hemorrhage, and maternal death.
![]() The perinatal mortality rate of twins is 3–4 times higher—and for triplets much higher still—than in singleton pregnancies as a result of chromosomal abnormalities, prematurity, structural anomalies, hypoxia, and trauma.
The perinatal mortality rate of twins is 3–4 times higher—and for triplets much higher still—than in singleton pregnancies as a result of chromosomal abnormalities, prematurity, structural anomalies, hypoxia, and trauma.
![]() This is particularly true of monozygotic twins, which are also uniquely susceptible to twin–twin transfusion syndrome.
This is particularly true of monozygotic twins, which are also uniquely susceptible to twin–twin transfusion syndrome.
Pathogenesis
In the United States, between 1980 and 2004, the twin rate climbed 101% with 68,339 twins born in 1980 and 137,085 twins born in 2006. Multiple gestations now comprise 3% of all pregnancies, and twins comprise 25–30% of deliveries resulting from assisted reproductive technologies (ART). Significant maternal and neonatal effects are felt from this increase in multiple births. The financial costs are also staggering, with combined costs of ART plus pregnancy care, delivery, and neonatal care reaching hundreds of thousands of dollars in some cases. Maternal morbidity and mortality rates are much higher in multiple pregnancy than in singleton pregnancy. Compared with singleton pregnancies, twin pregnancies are more likely to be complicated by hypertensive disorders, gestational diabetes mellitus, anemia, preterm birth, ante- and postpartum hemorrhage, and maternal death. Earlier and more precise sonography has revealed the incidence of multiple gestation to be 3.29–5.39% before 12 weeks. However, in over 20% of such cases, one or more of the pregnancies spontaneously disappears (“vanishing twin”). Although this event may be associated with vaginal bleeding, the prognosis remains good for the remaining twin.
Approximately two-thirds of twin pregnancies end in a singleton birth; the other embryo is lost from bleeding, is absorbed within the first 10 weeks of pregnancy, or is retained and becomes mummified (fetus papyraceous). Fetus papyraceous is a small, blighted, mummified fetus usually discovered at the delivery of a well-developed newborn. This occurs once in 17,000–20,000 pregnancies spontaneously and is also the result of multifetal reduction. The cause is thought to be death of one twin, amniotic fluid loss, or reabsorption and compression of the dead fetus by the surviving twin.
Twins can be monozygotic or dizygotic. Higher order multiples can result from either or both processes.
A. Monozygotic Multiple Gestation
Monozygotic twins (“identical twins”) are the result of the division of a single fertilized ovum that subsequently divides into 2 separate individuals. Monozygotic twinning occurs in about 4–5 of 1000 pregnancies in all races. The rate is remarkably constant in all populations and is not influenced by heredity, age of the mother, or other factors. Monozygotic twins are always of the same sex. However, the twins may develop differently depending on the time of preimplantation division. Normally, monozygotic twins share the same physical characteristics (skin, hair and eye color, body build) and the same genetic features (blood characteristics: ABO, M, N, haptoglobin, serum group; histocompatible genes), and they are often mirror images of one another (one left-handed, the other right-handed, etc). However, their fingerprints differ.
The paradox of “identical” twins is that they may be the antithesis of identical. The very earliest splits are sometimes accompanied by a simultaneous chromosomal error, resulting in heterokaryotypic monozygotes, one with Down syndrome and the other normal. Furthermore, monozygotic twins may be discordant for fetal structural malformations.
Monozygotic triplets result from repeated twinning (also called supertwinning) of a single ovum. Conversely, trizygotic triplets develop by individual fertilization of 3 simultaneously expelled ova. Triplets may also be produced by the twinning of 2 ova and the elimination of 1 of the 4 resulting embryos. Similarly, quadruplets may be monozygotic, paired dizygotic, or quadrizygotic (ie, they may arise from 1 to 4 ova).
Monoamniotic twins are the rarest form of monozygotic twins, with an incidence of about 1:10,000 pregnancies (1–5% of monozygotic gestations). The perinatal mortality is much higher than that of other monozygotic twins (23%) mostly due to cord entanglement as a result of the absence of a dividing membrane.
1. Placenta & cord—The placenta and membranes of monozygotic twins vary (Fig. 17–1), depending on the time of initial division of the embryonic disk. Variations are noted below.

Figure 17–1. Placental variations in twinning. (Reproduced, with permission, from Benson RC. Handbook of Obstetrics & Gynecology. 8th ed. Los Altos, CA: Lange; 1983.)
1. Division prior to the morula stage and differentiation of the trophoblast (day 3) results in separate or fused placentas, 2 chorions, and 2 amnions (dichorionic/diamniotic). (This process grossly resembles dizygotic twinning and accounts for almost one-third of monozygotic twinning.) This is clinically relevant since dichorionic twins have a much lower rate of complications.
2. Division after differentiation of the trophoblast but before the formation of the amnion (days 4–8) yields a single placenta, a common chorion, and 2 amnions (monochorionic/diamniotic). (This accounts for about two-thirds of monozygotic twinning.)
3. Division after differentiation of the amnion (days 8–13) results in a single placenta, 1 (common) chorion, and 1 (common) amnion (monochorionic/monoamniotic). This is rare.
4. Division later than day 15 may result in incomplete twinning. Just prior to that time (days 13–15), division may result in conjoined twins.
At delivery, the membranous T-shaped septum or dividing membrane of the placenta between the twins must be inspected and sectioned for evidence of the probable type of twinning (Fig. 17–2). Monochorionic, diamniotic twins most commonly have a transparent (<2 mm) septum made up of 2 amniotic membranes only (no chorion and no decidua). Dichorionic, diamniotic twins almost always have an opaque (thick) septum made up of 2 chorions, 2 amnions, and intervening decidua.

Figure 17–2. Chorionic and amniotic membranes of twins. (Reproduced, with permission, from Benson RC. Handbook of Obstetrics & Gynecology. 8th ed. Los Altos, CA: Lange; 1983.)
A monochorionic placenta can be identified by stripping away the amnion or amnions to reveal a single chorion over a common placenta. In virtually every case of monochorionic placenta, vascular communications between the 2 parts of the placenta can be identified by careful dissection or injection. In contrast, dichorionic placentas (of dizygotic twinning) only rarely have an anastomosis between the fetal blood vessels. All twin placentas are sent for pathologic examination to confirm chorionicity.
Placental and membrane examination is a certain indicator of zygosity in twins with monochorionic placentas because these are always monozygotic. Overall, approximately 1% of twins are monoamniotic, and these too are monozygotic. Determination of zygosity is clinically significant in case intertwin organ transplantation is needed later in life, as well as for assessing obstetrical risks. Monozygotic twins can rarely be discordant for phenotypic sex when one twin is phenotypically female due to Turner’s syndrome (45,XO) and its sibling is male (46,XY).
Monochorionic placentation is associated with more disease processes as a result of placental vascular problems. Inequities of the placental circulation in one area (marginal insertion, partial infarction, or thinning) may lead to growth discordance between the twins. Due to vascular anastomoses in monochorionic placentation, standard multifetal reduction using intrathoracic potassium chloride can only be performed with dichorionic placentation.
The most serious problem with monochorionic placentas is local shunting of blood—also called twin–twin transfusion syndrome. This problem affects approximately 15% of monochorionic twin pregnancies and occurs because of vascular anastomoses to each twin that are established early in embryonic life. The possible communications are artery to artery, vein to vein, and combinations of these. Artery-to-vein communication is by far the most serious; it is most likely to cause twin–twin transfusion. In uncompensated cases, the twins, although genetically identical, differ greatly in size and appearance. The recipient twin is plethoric, edematous, and hypertensive. Ascites and kernicterus are likely. The heart, liver, and kidneys are enlarged (glomerulotubal hypertrophy). Hydramnios follows fetal polyuria. Although ruddy and apparently healthy, the recipient twin with hypervolemia may die of heart failure during the first 24 hours after birth. The donor twin is small, pallid, and dehydrated (from growth restriction, malnutrition, and hypovolemia). Oligohydramnios may be present. Severe anemia, due to chronic blood loss to the other twin, may lead to hydrops and heart failure.
Velamentous insertion of the cord occurs in about 7% of twins but in only 1% of singletons. There is a corresponding increase in the potentially catastrophic vasa previa. The incidence of 2-vessel cord (single umbilical artery) is 4–5 times higher in monozygotic twins than in singletons.
Monochorionic, monoamniotic twins (1:100 sets of twins) have < a 90% likelihood of both surviving because of cord entanglement that compromises fetal-placental blood flow. Other common complications are congenital anomalies in 26% of monoamniotic twins and discordant birth weights, primarily due to twin–twin transfusion syndrome. Some authors advocate planned caesarean delivery at 32–34 weeks in an attempt to prevent in utero demise due to cord accidents, as well as continuous external fetal monitoring from about 27 weeks until delivery.
2. The fetus—There are several unusual fetal findings that may be seen in the setting of monozygotic twinning. Conjoined twins result from incomplete segmentation of a single fertilized ovum between the 13th and 14th days; if cleavage is further postponed, incomplete twinning (ie, 2 heads, 1 body) may occur. Lesser abnormalities are also noted, but these occur without regard to specific organ systems. Conjoined twins are described by site of union: pyopagus (at the sacrum); thoracopagus (at the chest); craniopagus (at the heads); and omphalopagus (at the abdominal wall). Curiously, conjoined twins usually are female. Numerous conjoined twins have survived separation.
An acardiac twin is a parasitic monozygotic fetus without a heart. It is thought to develop from reversed circulation, perfused by 1 arterial–arterial and 1 venous–venous anastomosis. This represents the twin reversed arterial perfusion (TRAP) syndrome. The otherwise normal donor twin is at risk for cardiac hypertrophy and failure and has a 35% mortality rate. Various methods of cord occlusion are being studied as in utero therapy.
B. Dizygotic Multiple Gestation
Dizygotic twins (“fraternal twins”) are produced from separately fertilized ova. They bear only the resemblance of brothers or sisters and may or may not have the same blood type. Significant differences usually can be identified over time. Slightly more than 30% of twins are monozygotic; nearly 70% are dizygotic. Twins of different sexes are always dizygotic (fraternal). Twins of the same sex may be monozygotic or dizygotic. Although monozygotism is random—ie, it does not fit any discernible genetic pattern—dizygotism has hereditary determinants.
In North America, dizygotic twinning occurs about once in 83 conceptions and triplets occur about once in 8000 conceptions. A traditional approximation of the incidence of spontaneous multiple pregnancies is as follows:

About 75% of dizygotic twins are the same sex. Many factors influence dizygotic twinning including age and ethnicity. Race is a factor, with multiple gestations most common in blacks, least common in Asians, and of intermediate occurrence in whites. The incidence of spontaneous dizygotic twinning varies from 1.3 in 1000 in Japan to 49 in 1000 in western Nigeria. The rate in the United States is about 12 in 1000. Spontaneous twinning increases with advancing maternal age. The widespread use of ART has increased the frequency of dizygotic twins with a minimal effect on the incidence of monozygotic twins.
Dizygotic twinning is more common among women who become pregnant soon after cessation of long-term oral contraception. This may be a reflection of high “rebound” gonadotropin secretion. Induction of ovulation in previously infertile patients has resulted in many multiple pregnancies—even the gestation of septuplets and octuplets. The estrogen analog clomiphene citrate increases the incidence of dizygotic pregnancy to about 5–10%.
Clinically, zygosity cannot be ascertained prenatally, so chorionicity seen on ultrasound is a useful surrogate marker for stratification of perinatal risk, with increased risks associated with monochorionicity.
Prevention
A. Multiple Gestations
Although ovulation induction agents result in fewer multiple pregnancies when used by experts, even in the best of hands, it is inevitable that some multiple pregnancies will occur. For example, clomiphene citrate induction of multiple ovulation increases the rate of dizygotic pregnancy above 5–10%.
With many forms of ART (eg, ovulation induction, in vitro fertilization), iatrogenic multiple pregnancies regularly occur in which the number of fetuses is so great that they may preclude any being carried to the point of viability. When this occurs, many authorities recommend multifetal pregnancy reduction by transabdominal intracardiac potassium chloride injection. Efforts are under way to recommend limiting the number of embryos transferred; legislation to this effect has been enacted in the United Kingdom. The American Society for Reproductive Medicine is now recommending single-embryo transfers in good-prognosis candidates.
Clinical Findings
With the ready availability of ultrasound, it is rare that multiple gestations go undiagnosed during pregnancy. Early diagnosis facilitates appropriate prenatal care.
A. Symptoms & Signs
All of the common annoyances of pregnancy are more troublesome in multiple gestations. The effects of multiple gestation on the patient include earlier and more severe pressure in the pelvis, nausea, backache, varicosities, constipation, hemorrhoids, abdominal distention, and difficulty in breathing. A “large pregnancy” may be indicative of twinning (distended uterus). Fetal activity is greater and more persistent in twinning than in singleton pregnancy.
Considering the possibility of multiple gestation is essential to early diagnosis. If one assumes that all pregnancies are multiple until proved otherwise, physical examination alone will identify most cases of twinning before the second trimester. Indeed, diagnosis of twinning is possible in over 75% of cases by physical examination. The following signs should alert the physician to the possibility or definite presence of multiple pregnancy:
1. Uterus larger than expected (>4 cm) for dates.
2. Excessive maternal weight gain that is not explained by edema or obesity.
3. Polyhydramnios, manifested by uterine size out of proportion to the calculated duration of gestation, is almost 10 times more common in multiple pregnancy.
4. History of assisted reproduction.
5. Elevated maternal serum α fetoprotein (MSAFP) values (see following section, Laboratory Findings).
6. Outline or ballottement of more than 1 fetus.
7. Multiplicity of small parts.
8. Simultaneous recording of different fetal heart rates, each asynchronous with the mother’s pulse and with each other and varying by at least 8 beats/min. (The fetal heart rate may be accelerated by pressure or displacement.)
9. Palpation of 1 or more fetuses in the fundus after delivery of 1 infant.
Some of the common complications in early pregnancy may also occur as a result of multiple gestation. For example, maternal bleeding in the first trimester can indicate threatened or spontaneous abortion; however, the dead fetus may be 1 of twins, as demonstrated by realtime ultrasonography (1 anechoic or hypoechoic amniotic sac and 1 normal sac). In the second and third trimester, the demise of 1 fetus in a multiple gestation may rarely trigger disseminated intravascular coagulation (DIC), just as a singleton intrauterine demise might. This theoretical complication is so rare that DIC screening is no longer performed.
B. Laboratory Findings
The majority of multiple gestations are currently identified by using MSAFP screening or routine ultrasound. Indeed, identification of multiple gestation is so important for the institution of appropriate care that many authorities recommend routine ultrasonic scanning for early confirmation of gestational age and then again at 18–20 weeks. First-trimester ultrasonography is even more helpful for determining chorionicity and is becoming standard of care, especially since many patients undergo first-trimester ultrasound for nuchal translucency (NT) screening. Interestingly, NT measurements are similar for a given crown-rump length regardless if it is a singleton, twin, or higher order multiple gestation.
The maternal hematocrit and hemoglobin values and the red cell count usually are considerably reduced, in direct relationship to the increased blood volume. Indeed, maternal hypochromic normocytic anemia is almost universal because fetal demand for iron increases beyond the mother’s ability to assimilate iron in the second trimester.
C. Ultrasound Findings
Ultrasonography is the preferred imaging modality for the diagnosis of multiple gestation and is potentially able to differentiate multiple gestation as early as 4–5 weeks (by endovaginal probe). Dichorionicity is suggested by fetuses of different genders, separate placentas, a thick (>2 mm) dividing membrane, or a “twin peak sign” in which the membrane inserts into 2 fused placentas. In the absence of these findings, monochorionicity is likely, particularly if the twins are spontaneously conceived. A first-trimester scan is highly recommended since definitive diagnosis of chorionicity may not be possible with second- and third-trimester scans. See the chapter on imaging in pregnancy (Chapter 11) for more details.
Differential Diagnosis
Multiple pregnancy must be distinguished from the following conditions.
A. Singleton Pregnancy
Inaccurate dates may give a false impression of the duration of the pregnancy, and the fetus may be larger than expected.
B. Polyhydramnios
Either single or multiple pregnancy may be associated with excessive accumulation of fluid.
C. Hydatidiform Mole
Although usually easily distinguished from multiple gestation, this complication must be considered in diagnosis early in pregnancy.
D. Abdominal Tumors Complicating Pregnancy
Fibroid tumors of the uterus, when present in great numbers, are readily identified. Ovarian tumors are generally single, discrete, and harder to diagnose. A distended bladder or full rectum may elevate the pregnant uterus.
E. Complicated Twin Pregnancy
If 1 dizygotic twin dies early in pregnancy and the other lives, the dead fetus may become flattened and mummified (fetus papyraceous; see earlier section on fetal pathologic factors). Its portion of a fused placenta will be pale and atrophic, but remnants of 2 sacs and 2 cords may be found. If 1 twin dies in late pregnancy, considerable enlargement of the uterus persists, although the findings on palpation may be unusual and only 1 fetal heartbeat will be heard. Ultrasonography can confirm the diagnosis.
Complications
A. Maternal
A gravida with a multiple pregnancy has about 5 times the likelihood of having a morbid (febrile, complicated) course as an average patient of the same parity with a single fetus.
Multiple gestations are associated with an increased incidence of maternal anemia, urinary tract infection, preeclampsia-eclampsia, hemorrhage (before, during, and after delivery), and uterine atony. Although blood volume is increased in multiple gestations, maternal anemia often develops because of greater demand for iron by the fetuses. However, prior anemia, poor diet, and malabsorption may precede or compound iron deficiency during multiple gestation. Hypochromic normocytic anemia is 2–3 times more common in multiple pregnancy than in singleton pregnancy. Urinary tract infection is at least twice as frequent in multiple pregnancy as in singleton pregnancy due to increased ureteral dilatation secondary to higher serum progesterone and uterine pressure on the ureters. Preeclampsia–eclampsia occurs about 3 times more often in multiple pregnancy than in a singleton pregnancy.
Additionally, respiratory tidal volume is increased, but the woman pregnant with twins often is “breathless” (possibly due to increased levels of progesterone). Marked uterine distention and increased pressure on the adjacent viscera and pelvic vasculature are typical of multiple gestation. Theca lutein cysts and even ascites may be seen as a result of abnormally high levels of chorionic gonadotropin in occasional multiple pregnancies. The maternal cardiovascular, respiratory, gastrointestinal, renal, and musculoskeletal systems are especially subject to stress in multiple pregnancy, combined with greater maternal–fetal nutritional requirements.
Placenta previa develops more frequently because of the large size of the placenta or placentas. Placenta previa may be responsible for antepartum bleeding, malpresentation, or unengagement of the first fetus. A large placenta (or placentas) and possibly fundal scarring or tumor may lead to low implantation of the placenta. Premature separation of the placenta may occur antepartum, perhaps in association with preeclampsia–eclampsia or with rupture of membranes of twin A and the initiation of strong uterine contractions, or after the delivery of the first twin. Careless traction on the first cord may encourage early partial separation of the placenta.
A thinned uterine wall, secondary to unusually large uterine contents, is associated with hypotonic uterine contractions and a longer latent stage of labor. However, prolonged labor is uncommon in multiple pregnancy because rupture of the membranes generally is followed by improvements in the uterine contraction pattern. Hemorrhage is about 5 times as frequent in multiple as in single pregnancies. Uterine atony often is accompanied by excessive loss of blood postpartum due to inability of the overdistended uterus to contract well and remain contracted after delivery.
Operative intervention is more likely in multiple pregnancy because of increased risk of obstetric problems such as malpresentation, prolapsed cord, and fetal distress.
Glucose tolerance tests demonstrate that rates of both gestational diabetes mellitus and gestational hypoglycemia are much higher in multiple gestation compared with findings in singleton pregnancy. This is not surprising given the placental origin of human placental lactogen, which causes insulin resistance.
B. Fetal
Perinatal mortality and morbidity rates are increased in multiple pregnancy, mainly because of preterm delivery and its complications (ie, trauma or asphyxia). The incidence of spontaneous abortion of at least 1 of several fetuses is increased in multiple pregnancy. Stillbirth occurs twice as often among twins as among singleton pregnancies. Common causes of fetal death are developmental anomalies, fetal growth restriction, cord compression, or placental disorders. In general, the higher the number of fetuses, the greater is the risk of fetal growth restriction.
Monochorionic twin pregnancies have a substantially increased risk of death as compared with their dichorionic counterparts because of the almost ever-present vascular anastomoses that may cause the twin–twin transfusion syndrome or acute feto-fetal hemorrhage after intrauterine demise of 1 twin. The greatest hazard from cord compression is cord entanglement of monozygotic twins with only 1 amniotic sac. Almost twice as many monozygotic as dizygotic twins die in the perinatal period. Attrition is even greater for triplets, quadruplets, and higher order pregnancies. Even so, preterm delivery and intrapartum complications are the most common causes of fetal loss and morbidity in multiple pregnancy.
Preterm premature rupture of the membranes and pre-term labor and delivery, often with a long prodromal phase, are common occurrences in multiple pregnancy. The average gestational age at delivery is 36–37 weeks for twins, 33 weeks for triplets, and 31 weeks for quadruplets. Efforts to reduce the incidence of prematurity have thus far been largely unsuccessful. All too frequently, preterm delivery is occasioned by premature rupture of the membranes, which occurs in about 25% of twin, 50% of triplet, and 75% of quadruplet pregnancies. Delivery before the 36th week is twice as frequent in twin pregnancies as in singleton pregnancies. Intracranial injury is more common in premature infants, even those delivered spontaneously. An increased risk of cerebral palsy is found in twins, especially very low-birthweight babies, and also in liveborn co-twins of fetuses who died in utero.
Prolapse of the cord occurs 5 times more often in multiple than in singleton pregnancy. Premature separation of the placenta before delivery of the second twin may cause death of the second twin by hypoxia. When there are 2 separate placentas, 1 of them may deliver immediately after the first twin. Although the second twin may not be compromised, it is best to proceed with its delivery, both for its protection and to conserve maternal blood.
Major fetal structural malformations are present in approximately 2% of twin infants, compared with 1% of singletons, whereas minor malformations are found in 4% of twins compared with about 2.5% of singletons. Monozygotic twins are at higher risk than dizygotic twins.
Fetal malpresentation is more common in multiple gestations. Both twins present in cephalic presentation in almost 50% of cases. Twin A will be cephalic and twin B a breech in slightly more than 33% of cases (Fig. 17–3). Both fetuses will be breech presentations in 10% of cases, and almost that many will be single (or double) transverse presentations. Approximately 70% of first twins present by the vertex. Breech presentation occurs in slightly more than 25%. Overall, noncephalic presentation occurs 10 times more often in multiple pregnancy than in singleton pregnancy.
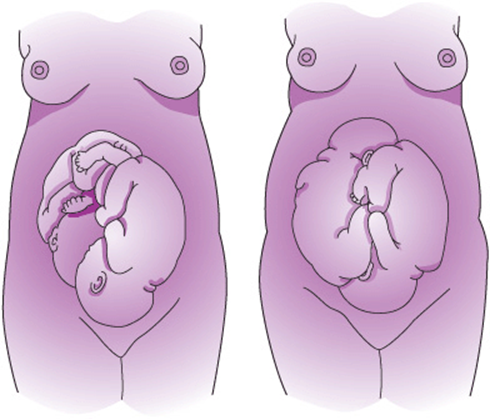
Figure 17–3. Left: Both twins presenting by the vertex. Right: One cephalic and one breech presentation. (Reproduced, with permission, from Benson RC. Handbook of Obstetrics & Gynecology. 8th ed. Los Altos, CA: Lange; 1983.)
Treatment
A. Prenatal Diagnosis
The usual indications for prenatal diagnosis and counseling in a singleton pregnancy also apply to twin and higher order gestations. Because the incidence of twin gestation increases with maternal age, women with multiple gestations are often candidates for prenatal genetic diagnosis. Because the risk of aneuploidy is increased, some centers offer invasive testing to all patients carrying multiple gestations who will be over age 33 at delivery. Now that most patients have prenatal screening with ultrasound and/or maternal serum testing, the role of age is becoming less important for stratification of risk for aneuploidy. Genetic counseling should make clear to the patient the need to obtain a sample from each fetus, the risk of a chromosomal abnormality, potential complications of the procedure, the possibility of discordant results, and the ethical and technical concerns when 1 fetus is found to be abnormal.
In twin pregnancies not accompanied by neural tube defects, the median MSAFP level will be 2.5-fold that of the median level for singleton pregnancies at 14–20 weeks’ gestation. The levels in triplets and quadruplets are 3 and 4 times as high, respectively. A value greater than 4.5 times the median is considered abnormal for twin gestations and requires a targeted ultrasound and possible amniocentesis for the determination of amniotic fluid α fetoprotein and acetylcholinesterase. Serum screening is less effective in multiple gestations, with serum screening detecting only 47% of Down syndrome pregnancies. NT screening with first-trimester serum markers can detect about 70% of Down syndrome fetuses in twin pregnancies, with some added benefit to incorporating second-trimester markers.
Both amniocentesis and chorionic villus sampling can safely be performed in multiple gestations in experienced centers. Careful documentation of the location of the fetuses and the membrane separating the sacs is important in case there is discordance for aneuploidy. Selective termination of an aneuploid fetus can be performed via ultrasound-guided intracardiac injection of potassium chloride. The pregnancy can then continue carrying the normal twin only. Multifetal reduction may be performed to decrease the risk of serious perinatal morbidity and mortality associated with preterm delivery by reducing the number of fetuses from 3 or more to twins or even a singleton.
B. Antepartum Management
To prevent the complications of multiple gestation, it is imperative to make the diagnosis as early in pregnancy as possible. Later in pregnancy, ultrasonography is useful to monitor the growth of the fetuses and to detect structural anomalies. It is recommended to perform routine growth scans on twins every 4 weeks in the third trimester, or more frequently if growth restriction is detected. Antepartum testing is routinely performed in twins with suspected intrauterine growth restriction or growth discordance but is not universally performed in normally grown uncomplicated twins.
Enhanced antenatal care assists in improving outcome. The most commonly used techniques are iron and calcium supplementation, vitamin and folic acid administration (in an attempt to avoid anemia), a high-protein diet, and more weight gain than usual (ideal weight for height plus 35–45 lb). Supplementation with magnesium, zinc, and essential fatty acids has also been recommended.
There is not enough evidence to suggest a policy of routine hospitalization for bed rest in multiple pregnancy because no reduction in the risk of preterm birth or perinatal death is evident. There is also no evidence that prophylactic cerclage improves outcome. More frequent antenatal visits are scheduled, and several authorities recommend closely following cervical length by ultrasound. Early and prompt therapy for any complications (eg, vaginal infections, pre-eclampsia–eclampsia) should be instituted, bearing in mind that preeclampsia–eclampsia is a common complication of multiple pregnancy.
Tocolytic drugs may be used to suppress premature labor and extend gestation 48 hours so that the effects of steroids may be realized. There is no evidence that long-term oral or intravenous tocolysis improves outcome; however, this is still commonly practiced to a degree. Most authorities recommend starting with intravenous magnesium sulfate. If terbutaline is used, very close monitoring for pulmonary edema must be maintained, because this complication is much more likely with administration of β-mimetic agents in multiple gestation. Also, indomethacin is a very effective tocolytic in the second and early third trimesters, but it may influence fetal ductal constriction and decreased amniotic fluid volume, complications that appear to be gestational age dependent, so it should not be used after 32 weeks’ gestation. Fetal fibronectin can be helpful, particularly when negative, to determine how aggressively to tocolyze.
Neonatal outcome is very much dependent on gestational age at delivery. In general, morbidity and mortality rates are similar for twins and singletons of equivalent gestational ages. Advances in neonatal intensive care have made survival possible even at 23 weeks’ gestation, although usually with considerable morbidity, including but not limited to intra-ventricular hemorrhage, chronic lung disease, and necrotizing enterocolitis. Because intact survival is much more likely after 32–34 weeks, it is desirable to prolong gestation at least to this point when possible. The adage “1 day in utero saves 2 days in intensive care” applies to the economic as well as the emotional costs of caring for premature infants. For the dichorionic diamniotic twin pregnancy that is otherwise uncomplicated, recent studies have found that neonatal morbidity is reduced when delivery is at about 38 weeks, so routine delivery at that time is recommended, by either induction of labor or caesarean if indicated.
Optimal treatment of twin–twin transfusion syndrome in utero remains controversial. Laser therapy for ablation of anastomotic placental vessels is available in several centers around the United States and shows improved short-term survival as compared to expectant management and serial amnioreduction. Two-year neurodevelopmental outcomes are also improved in patients treated with laser. After delivery, therapy for twin–twin transfusion syndrome includes replacing blood in the donor twin to correct fluid and electrolyte imbalance. In the recipient twin, phlebotomy may be necessary until normal venous pressure is restored. Often, other therapy for cardiac failure (eg, digitalis) is necessary.
C. Labor & Delivery
All patients carrying a multiple gestation should be delivered in a well-equipped hospital by an experienced physician who has adequate assistance. It is desirable to have a pediatrician (or neonatologist) in attendance. Delivery must be done in the operating room in case an emergent caesarean section is needed for twin B. An early epidural is recommended; in case of emergent caesarean section, anesthesia is already established and general anesthesia can usually be avoided. Prematurity, trauma of manipulative delivery, and associated asphyxia are the major preventable causes of morbidity and mortality in twins, especially the second twin.
Admit the patient to the hospital at the first sign of suspected labor or preterm labor, if there is leakage of amniotic fluid, or if significant bleeding occurs. We instruct patients to come in for >4 contractions per hour at <34 weeks’ gestation. An ultrasound evaluation should be performed to ascertain the presentation of each fetus and its estimated fetal weight. Routine, continuous electronic fetal heart rate monitoring is recommended. Labor should be conducted so that immediate caesarean section can be performed if required. A pediatric nurse team for each infant plus obstetric and anesthesiologic attendants should be present. Insert an intravenous line and send a specimen of blood for typing, antibody screening, and complete blood count.
If either twin shows signs of persistent compromise, proceed promptly to caesarean section delivery. Other indications for primary caesarean section include (but are not limited to) malpresentation, monoamniotic twins, gross disparity in fetal size, and placenta previa. In the United States, all higher order multiple gestations are delivered by caesarean delivery.
In a woman with a previous lower segment caesarean scar, limited literature suggests that delivery of twins does not mandate a repeat caesarean section in the absence of other complications. Concomitant with increasing rates of elective and nonelective caesarean section, caesarean by patient request is becoming more common. In addition, less resident training in vaginal breech delivery can decrease a clinician’s comfort with breech extraction of a second twin.
Management of twins that are candidates for vaginal delivery may proceed as outlined below. Intrapartum twin presentations may be classified as follows: (1) twin A and twin B cephalic (slightly >40% of all twins); (2) twin A vertex and twin B noncephalic (almost 40%); and (3) twin A noncephalic and twin B cephalic, breech, or transverse (about 20%).
The current intrapartum management of twins is as follows. For cephalic–cephalic presentations in labor (category 1 above), vaginal delivery of both twins may be chosen in the absence of standard indications for caesarean section delivery. Of course, if either twin develops fetal distress, caesarean section delivery should be performed. Category 2 twins, each >32 weeks and weighing more than 1500–2000 g, can usually be managed successfully by vaginal delivery of both. This is generally accomplished by total breech extraction of twin B immediately after the delivery of twin A if the patient has been consented for this procedure. External cephalic version of twin B has also been described. While external version was previously recommended for conversion of twin B from breech to cephalic, now most operators deliver vaginal second twins by complete breech extraction. When either twin A or both twins are noncephalic (category 3), primary caesarean section should be performed. This is also sometimes recommended in cases of noncephalic twin B where the estimated fetal weight is much greater than that of twin A. The ultrasound machine should be in the operating room to confirm the presentation of twin B after the delivery of twin A. The amount of time between delivery of twin A and B is still a matter of controversy. If electronic fetal monitoring suggests fetal well-being, it is not necessary to deliver twin B within a prescribed amount of time such as 30 or 60 minutes. Difficult forceps operation or rapid extraction should be avoided, but forceps to protect the aftercoming premature head may be useful. The umbilical cord should be clamped promptly to prevent the second twin of a monozygotic twin pregnancy from exsanguinating into the first born.
Perform a vaginal examination immediately after delivery of twin A to note the presentation and station of the second twin, the presence of a second sac, an occult cord prolapse, or cord entanglement.
Cut the cord as far outside the vagina as possible so that it can hang loosely to permit vaginal examination or manipulation. This eliminates inadvertent cord traction on the placenta. Tag and label the cords (twin A and B) so that they may be associated with the proper placenta or placentas.
One twin may obstruct the delivery of both fetuses in locked twins. In this circumstance, twin A is always breech and twin B cephalic presentation, and the heads become impacted in the pelvis. Locked twins can be avoided by caesarean delivery in all cases in which it is known that twin A is not cephalic. However, if the obstetrician is presented with an emergent case of locked twins (Fig. 17–4), having an assistant support the twin already partially delivered as a breech while pushing both heads upward out of the pelvis with rotation of both fetuses may accomplish delivery of the first. This may require deep anesthesia. If this cannot be done, caesarean with abdominal delivery of both fetuses may be the safest route. An alternative while caesarean preparations are under way is to elevate the partially delivered twin, establish an airway, and protect the cord.
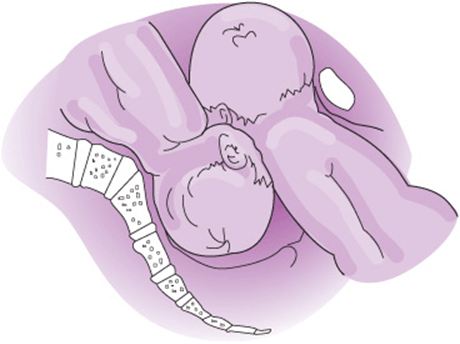
Figure 17–4. Locked twins. (Reproduced, with permission, from Benson RC. Handbook of Obstetrics & Gynecology. 4th ed. Los Altos, CA: Lange; 1971.)
Postpartum hemorrhage is common in multiple pregnancy. Increased intravenous oxytocin, elevation, and massage of the fundus and an intravenous ergot or prostaglandin product (only after the last fetus is delivered) may be required. After delivery, if separation of the placenta is delayed or bleeding is brisk, manual extraction of the placenta may be necessary. Currently, we recommend prophylactic rectal misoprostol in the operating room followed by oral misoprostol every 6 hours for 24 hours after delivery for all multiple gestations.
Preeclampsia–eclampsia and premature labor and delivery are managed as outlined elsewhere in this book.
If it is desired to determine zygosity after delivery, concordance of placental examination, clinical comparisons, and hematologic and serologic tests provides presumptive evidence of monozygotic twinning. The total probability of diagnosis of zygosity is >95% using ABO, MNSs, Rh, Kell, Kidd, Duffy, and Lewis A and B antigens and approaches 100% using chromosomal analysis.
Prognosis
The US maternal mortality rate for women carrying a multiple gestation is only slightly higher than for singletons. With diligent care, many mothers and babies will do well. A history of previous dizygotic twins increases the likelihood of multiple gestation in a future pregnancy 10-fold.
Alexander JM, Leveno KJ, Rouse D, et al. Cesarean delivery for the second twin. Obstet Gynecol 2008;112:748–752. PMID: 18827115.
American College of Obstetricians and Gynecologists. Multiple Gestation: Complicated Twin, Triplet and Higher-Order Multifetal Pregnancy. ACOG Practice Bulletin No. 56. Washington, DC: American College of Obstetricians and Gynecologists; 2004.
Berghella V, Baxter JK, Hendrix NW. Cervical assessment by ultrasound for preventing preterm delivery. Cochrane Database Syst Rev 2009;3:CD007235. PMID: 19588421.
Blickstein I. Growth aberration in multiple pregnancy. Obstet Gynecol Clin North Am 2005;32:39–54. PMID: 15644288.
Bush MC, Malone FD. Down syndrome screening in twins. Clin Perinatol. 2005;32:373–836. PMID: 15922788.
Crowther CA, Han S. Hospitalisation and bed rest for multiple pregnancy. Cochrane Database Syst Rev 2010;7:CD000110. PMID: 20614420.
Dodd JM, Crowther CA. Elective delivery of women with a twin pregnancy from 37 weeks’ gestation. Cochrane Database Syst Rev 2003;1:CD003582. PMID: 12535480.
Evans MI, Ciorica D, Britt DW, Fletcher JC. Update on selective reduction. Prenat Diagn 2005;9:807–813. PMID: 16170845.
Fox NS, Saltzman DH, Klauser CK, et al. Prediction of spontaneous preterm birth in asymptomatic twin pregnancies with the use of combined fetal fibronectin and cervical length. Am J Obstet Gynecol2009;201:313.e1–e5. PMID: 19733285.
Fox NS, Silverstein M, Bender S, et al. Active second-stage management in twin pregnancies undergoing planned vaginal delivery in a U.S. population. Obstet Gynecol 2010;115:229–333. PMID: 20093893.
Hack KE, Derks JB, Elias SG, et al. Increased perinatal mortality and morbidity in monochorionic versus dichorionic twin pregnancies: Clinical implications of a large Dutch cohort study. BJOG2008;115:58–67. PMID: 17999692.
Healy AJ, Gaddipati S. Intrapartum management of twins: Truths and controversies. Clin Perinatol 2005;32:455–473. PMID: 1592279.
Heyborne KD, Porreco RP, Garite TJ, Phair K, Abril D; Obstetrix/Pediatrix Research Study Group. Improved perinatal survival of monoamniotic twins with intensive inpatient monitoring. Am J Obstet Gynecol2005;192:96–101. PMID: 15672009.
Lewi L, Gratacos E, Ortibus E, et al. Pregnancy and infant outcome of 80 consecutive cord coagulations in complicated monochorionic multiple pregnancies. Am J Obstet Gynecol 2006;194: 782–789. PMID: 16522413.
Luke B. Nutrition and multiple gestation. Semin Perinatol 2005;29:349–354. PMID: 16360494.
Moise KJ Jr, Johnson A, Moise KY, Nickeleit V. Radiofrequency ablation for selective reduction in the complicated monochorionic gestation. Am J Obstet Gynecol 2008;198:198.e1–e5. PMID: 18226623.
Murakoshi T, Ishii K, Matsushita M, et al. Monochorionic mono-amniotic twin pregnancies with two yolk sacs may not be a rare finding: A report of two cases. Ultrasound Obstet Gynecol 2010;36:384–386. PMID: 20533442.
Oleszczuk JJ, Keith LG, Oleszczuk AK. The paradox of old maternal age in multiple pregnancies. Obstet Gynecol Clin North Am 2005;32:69–80. PMID: 15644290.
Ortibus E, Lopriore E, Deprest J, et al. The pregnancy and long-term neurodevelopmental outcome of monochorionic diamniotic twin gestations: A multicenter prospective cohort study from the first trimester onward. Am J Obstet Gynecol 2009;200:494.e1–e8. PMID: 19275567.
Peaceman AM, Kuo L, Feinglass J. Infant morbidity and mortality associated with vaginal delivery in twin gestations. Am J Obstet Gynecol 2009;200:462.e1–e6. PMID: 19318158.
Rustico MA, Baietti MG, Coviello D, Orlandi E, Nicolini U. Managing twins discordant for fetal anomaly. Prenat Diagn 2005;25:766–771. PMID: 16170860.
Shetty A, Smith AP. The sonographic diagnosis of chorionicity. Prenat Diagn 2005;25:735–739. PMID: 16170841.
Smith GC, Fleming KM, White IR. Birth order of twins and risk of perinatal death related to delivery in England, Northern Ireland, and Wales, 1994-2003: Retrospective cohort study. BMJ2007;334(7593):576. PMID: 17337456.
Spadola AC, Simpson LL. Selective termination procedures in monochorionic pregnancies. Semin Perinatol 2005;29:330–337. PMID: 16360492.
Stone J, Ferrara L, Kamrath J, et al. Contemporary outcomes with the latest 1000 cases of multifetal pregnancy reduction (MPR). Am J Obstet Gynecol 2008;199(4):406.e1–e4. PMID: 19828991.