Christine H. Holschneider, MD
CERVICAL INTRAEPITHELIAL NEOPLASIA
ESSENTIALS OF DIAGNOSIS
![]() The cervix often appears grossly normal.
The cervix often appears grossly normal.
![]() Infection with the human papillomavirus is present.
Infection with the human papillomavirus is present.
![]() Dysplastic or carcinoma in situ cells are noted in a cytologic smear preparation (traditional Pap smear or liquid-based cytology).
Dysplastic or carcinoma in situ cells are noted in a cytologic smear preparation (traditional Pap smear or liquid-based cytology).
![]() Colposcopic examination reveals an atypical transformation zone with thickened epithelium, coarse punctate, or mosaic patterns of surface capillaries.
Colposcopic examination reveals an atypical transformation zone with thickened epithelium, coarse punctate, or mosaic patterns of surface capillaries.
![]() Iodine-nonstaining (Schiller-positive) area of squamous epithelium is typical.
Iodine-nonstaining (Schiller-positive) area of squamous epithelium is typical.
![]() Biopsy diagnosis of cervical intraepithelial neoplasia (dysplasia or carcinoma in situ).
Biopsy diagnosis of cervical intraepithelial neoplasia (dysplasia or carcinoma in situ).
General Considerations
Lower genital tract squamous intraepithelial neoplasia is often multicentric (ie, affecting multiple anatomic sites that embryologically are derived from the same anogenital epithelium): cervical intraepithelial neoplasia (CIN), vaginal intraepithelial neoplasia (VAIN, see Chapter 47), vulvar intraepithelial neoplasia (VIN, see Chapter 47), and perianal intraepithelial neoplasia (PAIN). Approximately 10% of women with CIN have concomitant preinvasive neoplasia of the vulva, vagina, or anus. Conversely, 40–60% of patients with VIN or VAIN have synchronous or meta-chronous CIN.
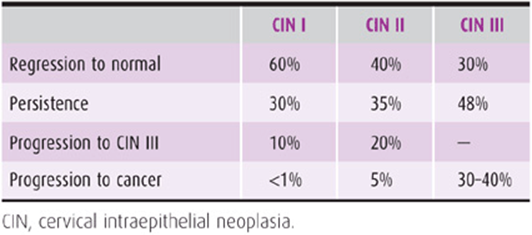
CIN, formerly called dysplasia, means disordered growth and development of the epithelial lining of the cervix. There are various degrees of CIN. Mild dysplasia, or CIN I, is defined as disordered growth of the lower third of the epithelial lining. Abnormal maturation of the lower two-thirds of the lining is called moderate dysplasia, or CIN II. Severe dysplasia, CIN III, encompasses more than two-thirds of the epithelial thickness with carcinoma in situ (CIS) representing full-thickness dysmaturity. While histologically evaluated lesions are characterized using the CIN nomenclature, cytologic smears are classified according to the Bethesda system, which was most recently revised in 2001. Briefly, atypical squamous cells are divided into those of undetermined significance (ASC-US) and those in which a high-grade lesion cannot be excluded (ASC-H). Low-grade squamous intraepithelial lesion (LSIL) encompasses cytologic changes consistent with koilocytic atypia or CIN I. High-grade squamous intraepithelial lesion (HSIL) denotes the cytologic findings corresponding to CIN II and CIN III. CIN may be suspected because of an abnormal cytologic smear, but the diagnosis is established by cervical biopsy. Spontaneous regression, especially of CIN I, occurs in a significant number of patients, allowing for expectant management with serial cytologic smears in the reliable patient. A certain percentage of high-grade lesions will progress to an invasive cancer if left untreated. Because it is not presently possible to predict which lesions will progress, it is recommended that all patients with CIN II and CIN III be treated when diagnosed. The only 2 exceptions to this recommendation concern adolescents, in whom CIN II may be followed, as spontaneous regression is substantial and the risk of cancer almost nil, as well as pregnant women, in whom treatment should be deferred to the postpartum period.
Pathogenesis
Prevalence figures for CIN vary according to the socioeconomic characteristics and geographic area of the population studied, from as low as 1.05% in some family planning clinics to as high as 13.7% in women attending sexually transmitted disease (STD) clinics. CIN is most commonly detected in women in their 20s; the peak incidence of CIS is in women ages 25–35 years, whereas the incidence of cervical cancer rises most significantly after the age of 40 years.
The epidemiologic risk factors for CIN are similar to those for cervical cancer and include multiple sexual partners, early onset of sexual activity, a high-risk sexual partner (history of multiple sexual partners, human papillomavirus [HPV] infection, lower genital tract neoplasia, or prior sexual exposure to someone with cervical neoplasia), a history of sexually transmitted infections (STIs), cigarette smoking, human immunodeficiency virus (HIV) infection, acquired immunodeficiency syndrome (AIDS), other forms of immunosuppression, multiparity, and long-term oral contraceptive pill use.
HPVs are a prime etiologic factor in the development of CIN and cervical cancer. In fact, most of the above behavioral and sexual risk factors for cervical neoplasia become statistically insignificant as independent variables after adjusting for HPV infection. Analyses of cervical neoplasia lesions show the presence of HPV in more than 80% of all CIN lesions and in 99.7% of all invasive cervical cancers. The 2 most common high-risk HPV types are HPV-16, found in 50–70% of cervical cancers, and HPV-18, found in 7–20% of cases.
Infection with HPV is extremely common and varies with the patient’s age. In the United States, the prevalence of detectable HPV infection rises from 1% in newborns, to 20% in teenagers, to 40% in women 20–29 years of age, with a slow decline thereafter to a plateau of 5% in women age 50 years and older. A women’s lifetime risk for infection with HPV is approximately 50–80%. Condoms are not as protective against HPV as they are against other STDs because transmission can occur from labial-scrotal contact. Regular and consistent condom use is necessary to achieve a 60% protection against infection.
There are about 130 HPV types, about 30–40 of which infect the anogenital epithelium. Based on their malignant potential, HPV subtypes are categorized into low-risk and high-risk types. Low-risk HPV types (eg, types 6, 11, 42, 43, and 44) are associated with condylomata and low-grade lesions (CIN I), whereas high-risk HPV types (eg, types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68) are associated with invasive cancer in addition to high-grade lesions (CIN II and CIN III),
More than 90% of immunocompetent women will have a spontaneous resolution of their HPV infection over a 2-year period, and only approximately 5% will have cytologically detectable CIN. About 10% of women will have a persistent high-risk HPV infection, which places them at increased risk for developing CIN II/III and cervical cancer.
The vast majority of women infected with HPV do not develop CIN or cervical cancer. This suggests that infection with HPV alone is insufficient for the development of CIN or cervical cancer and underscores the importance of other cofactors, such as cigarette smoking or immunosuppression.
Cigarette smoking and HPV infection have synergistic effects on the development of CIN, and cigarette smoking is associated with a 2- to 4-fold increase in the relative risk for developing cervical cancer. Cigarette smoke carcinogens have been found to accumulate locally in the cervical mucus, and the cumulative exposure as measured by pack-years smoked is related to the risk of developing CIN or CIS. However, the mechanisms by which cigarette smoking contributes to cervical carcinogenesis are poorly understood.
The incidence of cervical neoplasia is increased in HIV-infected women, who, in some studies, have a 20–30% incidence of colposcopically confirmed CIN. With increasing immunosuppression, there is an increased risk of de novo HPV infection, persistent HPV infection, and progressive cervical neoplasia. Since 1993, invasive cervical cancer has been included as an AIDS-defining illness.
Prevention
A. HPV Vaccination
Two HPV vaccines are currently approved by the Food and Drug Administration (FDA), a quadrivalent vaccine (Gardasil) against HPV-16, -18, -6, and -11 and a bivalent vaccine (Cervarix) against HPV-16 and -18. In clinical trials, the efficacy of these vaccines for preventing CIN II or worse due to HPV types included in the vaccine was 93–100% in the HPV-naïve study population. In the entire study cohorts (those with or without prior HPV infection), the efficacy of either vaccine for preventing CIN II or worse was only 30–44%. Among HPV-naive populations, these vaccines also provided approximately 20–50% protection against CIN II or worse due to nonvaccine HPV types. The Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices (ACIP) recommends that all girls 11–12 years of age should be routinely offered HPV vaccination, as well as girls and women age 13–26 who have not yet been vaccinated (catch-up population) and girls as young as 9 years, if indicated. In 2009, the FDA approved the use of the quadrivalent vaccine in males, and ACIP states that the quadrivalent vaccine may be given to males age 9–26 years to reduce their likelihood of acquiring genital warts and prevent the development of anal intraepithelial neoplasia and anal cancer.
These HPV vaccines are prophylactic and not therapeutic. Thus, immunization with HPV vaccine is most effective in female or male individuals who have not been infected with HPV (eg, before sexual debut). These recommendations are not altered if a girl or woman in the qualifying age group is found to have an abnormal Pap or a positive HPV test for the following reason: By their mid-20s, approximately 25% of women test positive for 1 of the 4 HPV types in the quadrivalent vaccine, but only 1% test positive for HPV-16 and -18, and only 0.1% test positive for all 4 HPV types. Thus, the bivalent or quadrivalent HPV vaccine should offer benefit to almost all individuals in the indicated age range. There is no evidence that HPV vaccine is harmful during pregnancy. However, HPV vaccination is not recommended during pregnancy due to limited safety data. Women who have started the vaccination series but became pregnant before completion or women who received the vaccination before knowing they were pregnant should be reassured and advised to resume the vaccination series postpartum. It is safe to offer HPV vaccination during lactation.
B. Screening for CIN & Cervical Cancer
Following the implementation of population-based screening programs and treatment of preinvasive and early invasive disease, there has been a 75% reduction in the incidence and mortality of cervical cancer in developed countries. In the United States, more than half of women who develop cervical cancer either have never had cervical cytology, have been screened only sporadically, or have not been screened within the previous 5 years. It is critical that women, whether vaccinated or not, follow current cervical cancer screening guidelines.
1. Cervical cytology screening—In 2012 new and generally consistent cervical cancer screening recommendations for the general population, HPV vaccinated and unvaccinated, were released by two separate groups: the U.S. Preventive Services Task Force (USPSTF) and the multidisciplinary partnership of the American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology (ACS/ASCCP/ASCP).
A. ONSET OF SCREENING—Cervical cytology screening should not begin before age 21 regardless of the age at onset of sexual intercourse. This recommendation is based on the fact that invasive cervical cancer is very rare in women younger than 21 years of age; yet there is significant potential for adverse effects associated with the follow-up of abnormal cervical cytology including anxiety, cost, morbidity and long-term consequences of overuse of follow-up procedures. In young women, there is a high prevalence of HPV infection shortly after the onset of intercourse, commonly associated with abnormal cervical cytology and followed by a very high subsequent spontaneous clearance rate of both HPV infection and dysplasia.
B. FREQUENCY OF SCREENING—Cervical cytology screening is recommended every 3 years for women 21–29 years of age. HPV testing should not be performed in this age group. Women age 30 or older should be screened with cytology and HPV co-testing every 5 years or cytology alone every 3 years.
C. DISCONTINUATION OF SCREENING—Screening should be discontinued in women older than 65 years with negative consecutive screening in the preceding 10 years. Screening should not be resumed for any reason. However, women who have completed their post-treatment surveillance for CIN 2/3 or worse, should continue routine screening for at least 20 years, even if that extends screening past age 65. Cytology testing should be discontinued in women who have had a total hysterectomy and do not have a prior history of CIN 2/3 or worse. Evidence of adequate negative prior screening is not required.
D. SPECIAL POPULATIONS—Based on 2009 ACOG guidelines, women who are HIV positive should be screened twice in the first year after diagnosis and annually thereafter. Women who are immunosuppressed for other reasons or had in utero DES exposure should be screened annually.
As previously discussed, the Pap test results are reported using the 2001 Bethesda nomenclature.
2. HPV testing—Currently, there are 2 US FDA-approved HPV tests in clinical practice. They test for the presence of 1 or more of 13 or 14 high-risk HPV types. High-risk HPV testing is currently being used in the United States for cervical cancer screening in the following scenarios:
• As a triage test for ASC-US cervical cytology in women 21 years of age or older with reflex-HPV testing on the residual preservative of the liquid-based cytology.
• As a triage test for LSIL in postmenopausal women.
• As a follow-up test after CIN I or negative colposcopy in women with ASC-US, ASC-H, LSIL, or atypical glandular cells (AGCs).
• In follow-up after treatment for CIN II/III.
• As an adjunct to cytology for the primary screening in women older than 30 years. HPV testing combined with a cervical cytology smear has been approved as a primary screening approach in the patient age 30 years and older, who still has her uterus and has no immunosuppression. If both results are negative, combined screening should not be repeated for 5 years. If cytology and HPV testing are positive, triaging to colposcopy is as outlined earlier. If cytology is normal, but HPV test is positive, repeat cytology and HPV testing in 6–12 months is recommended, with colposcopy at that point if either test is abnormal. Type-specific testing for HPV-16 and HPV-18 has recently been FDA approved and can be used as an adjunct for women with negative cytology results but positive high-risk HPV test.
3. Visual screening in low-resource settings—Visual inspection of the cervix is being used as a screening tool in low-resource settings with no access to HPV testing or cytology screening. It has limited specificity but is economical and provides immediate results. Visual inspection can be performed by direct visual inspection or by performing cervicoscopy using acetic acid, toluidine blue, or Lugol’s iodine as an adjunct.
Clinical Findings
A. Symptoms & Signs
There are usually no symptoms or signs of CIN, and the diagnosis is most often based on biopsy findings following an abnormal routine cervical cytology smear. Because high-grade dysplasia is a transitional phase in the pathogenesis of many cervical cancers, early detection by following the previously described screening guidelines is extremely important. If during pelvic examination, a cervical lesion is visualized, it should be promptly biopsied.
B. Pathology
On cytologic examination, the dysplastic cell is characterized by anaplasia, an increased nuclear-to-cytoplasmic ratio (ie, the nucleus is larger), hyperchromatism with changes in the nuclear chromatin, multinucleation, and abnormalities in differentiation.
Histologically, involvement of varying degrees of thickness of the stratified squamous epithelium is typical of dysplasia. The cells are anaplastic and hyperchromatic and show a loss of polarity in the deeper layers as well as abnormal mitotic figures in increased numbers. Benign epithelial alterations, particularly those of an inflammatory nature, the cytopathic effects of HPV, and technical artifacts may be mistaken for CIN I and CIN II.
The columnar epithelium of the mucus-secreting endocervical glands can also undergo neoplastic transformation. Adenocarcinoma in situ (ACIS) is defined as the presence of endocervical glands lined by atypical columnar epithelium that cytologically resembles the cells of endocervical adenocarcinoma, but that occur in the absence of stromal invasion. The diagnosis of ACIS can be made only by cone biopsy.
C. Special Examinations
All abnormal cervical cytology tests require further evaluation, such as visual inspection of the cervix, repeat cytology, HPV testing, staining with Lugol’s solution (Schiller test) or toluidine blue, colposcopy, directed biopsy, endocervical sampling, or diagnostic conization (see Treatment section) (Fig. 48–1). The objective is to exclude the presence of invasive carcinoma and to determine the degree and extent of any CIN.
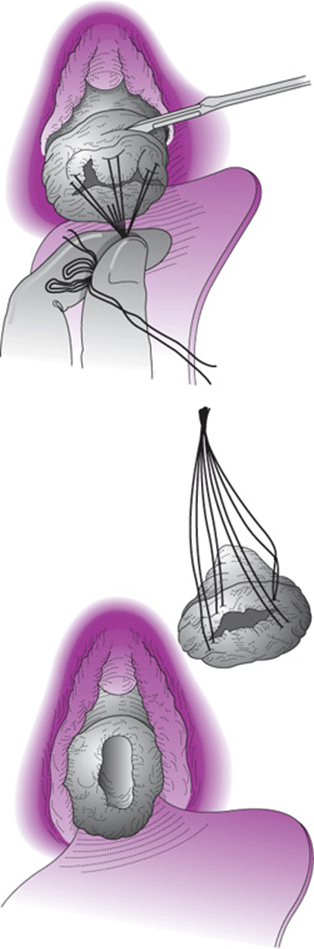
Figure 48–1. Conization of the cervix.
1. Repeat cervical cytology—There are 3 acceptable initial evaluation steps for patients with minimally abnormal cervical cytology smears (eg, ASC-US, postmenopausal LSIL): accelerated serial cytology smears, triage to colposcopy based on a positive HPV testing result, or immediate referral to colposcopy. All patients with ASC-H, premenopausal LSILs, HSILs, AGCs, or smears suspicious for cancer should be referred for immediate colposcopy.
Prior to performing a repeat smear for a patient with ASC-US, she should be evaluated and treated for potential underlying conditions that might contribute to an atypical smear, such as antimicrobials for infections or hormones for atrophic vaginitis. The cervical cytology smear should be repeated every 6 months until there are 2 consecutive normal smears. The use of serial cytologic smears is important, as the false-negative rate of a single repeat smear following an ASC-US diagnosis is as high as 33% for biopsy-proven HSILs (CIN II/III). A second abnormal smear (atypical squamous cell [ASC] or worse) should be evaluated by colposcopy.
2. HPV testing—Testing for low-risk HPV types has no role in cervical cancer prevention. Testing for high-risk HPV types has become an integral part of the management of some abnormal cervical cytology smears (ie, ASC-US, post-menopausal LSIL). For patients with ASC-US, reflex HPV testing is the preferred approach, with triage of women who test positive for high-risk HPV to colposcopy. Reflex HPV testing refers to the concurrent collection of a specimen for cervical cytology and HPV testing, with the HPV testing being performed only in case of an abnormal cytologic screen. For ASC-US, this approach is the most cost-effective and has an equal or higher sensitivity for CIN II/III at the lowest referral rate to colposcopy compared to the 2 alternate approaches (accelerated serial cytology or immediate colpos-copy). Women with an ASC-US smear and a negative HPV test are followed with a cervical cytology smear at 1 year. The value of HPV testing for the triage of premenopausal patients with LSIL is limited because nearly 85% of the lesions are HPV positive.
3. Schiller test—The Schiller test is based on the principle that normal mature squamous epithelium of the cervix contains glycogen, which combines with iodine to produce a deep mahogany-brown color. Nonstaining, therefore, indicates abnormal squamous (or columnar) epithelium, scarring, cyst formation, or immature metaplastic epithelium, and constitutes a positive Schiller test. Lugol’s solution is an aqueous iodine preparation and is commonly used for the Schiller test.
4. Colposcopic examination—Colposcopy is the primary technique for the evaluation of an abnormal cervical cytology smear. The colposcope is an instrument that uses illuminated low-power magnification (5–15×) to inspect the cervix, vagina, vulva, or anal epithelium. Abnormalities in the appearance of the epithelium and its capillary blood supply often are invisible to the naked eye but can be identified by colposcopy, particularly after the application of 3–5% aqueous acetic acid solution. CIN produces recognizable abnormalities of the cervical epithelium in the majority of patients.
Indications for colposcopy are:
1. Abnormal cervical cytology smear or HPV testing;
2. Clinically abnormal or suspicious-looking cervix;
3. Unexplained intermenstrual or postcoital bleeding;
4. Vulvar or vaginal neoplasia; or
5. History of in utero DES exposure.
Details of the colposcopy technique are described in Chapter 40.
Normal colposcopic findings are those of:
1. The original squamous epithelium, which extends from the mucocutaneous vulvovaginal junction to the original squamocolumnar junction.
2. The transformation zone, which is the metaplastic squamous epithelium between the original squamocolumnar junction and the active squamocolumnar junction. The original squamocolumnar junction is the junction between the stratified squamous epithelium of the vagina and ectocervix and the columnar epithelium of the endocervical canal. In two-thirds of female infants, this original squamocolumnar junction is located on the ectocervix, in close to a third in the endocervical canal, and in a very small subset out in the vaginal fornices. During a woman’s life cycle, the squamocolumnar junction “migrates” as a consequence of various hormonal and environmental influences that alter the cervical volume and cause squamous metaplasia of everted endocervical columnar cells. Following menarche, the squamocolumnar junction is generally found on the ectocervix, with further eversion during pregnancy. In the postmenopausal patient, the squamocolumnar junction is frequently within the endocervical canal. This squamous metaplasia is a dynamic process, and cervical neoplasia almost invariably originates within the transformation zone. If the new squamocolumnar junction is visualized in its entirety, the colposcopic examination is called satisfactory; if it cannot be fully visualized, the examination is called unsatisfactory.
3. The columnar epithelium of the endocervical canal.
Abnormal findings indicative of dysplasia and CIS are those of:
1. Leukoplakia or hyperkeratosis, which is an area of white, thickened epithelium that is appreciated prior to the application of acetic acid and may indicate underlying neoplasia.
2. Acetowhite epithelium, which is epithelium that stains white after the application of acetic acid.
3. Mosaicism or punctation reflecting abnormal vascular patterns of the surface capillaries. As a general rule, capillary thickness and intercapillary distances correlate with the severity of the lesion and thus tend to be larger and coarser in higher grade lesions.
4. Atypical vessels with bizarre capillaries with so-called corkscrew, comma-shaped, or spaghetti-like configurations suggest early stromal invasion (Figs. 48–2 through 48–4).
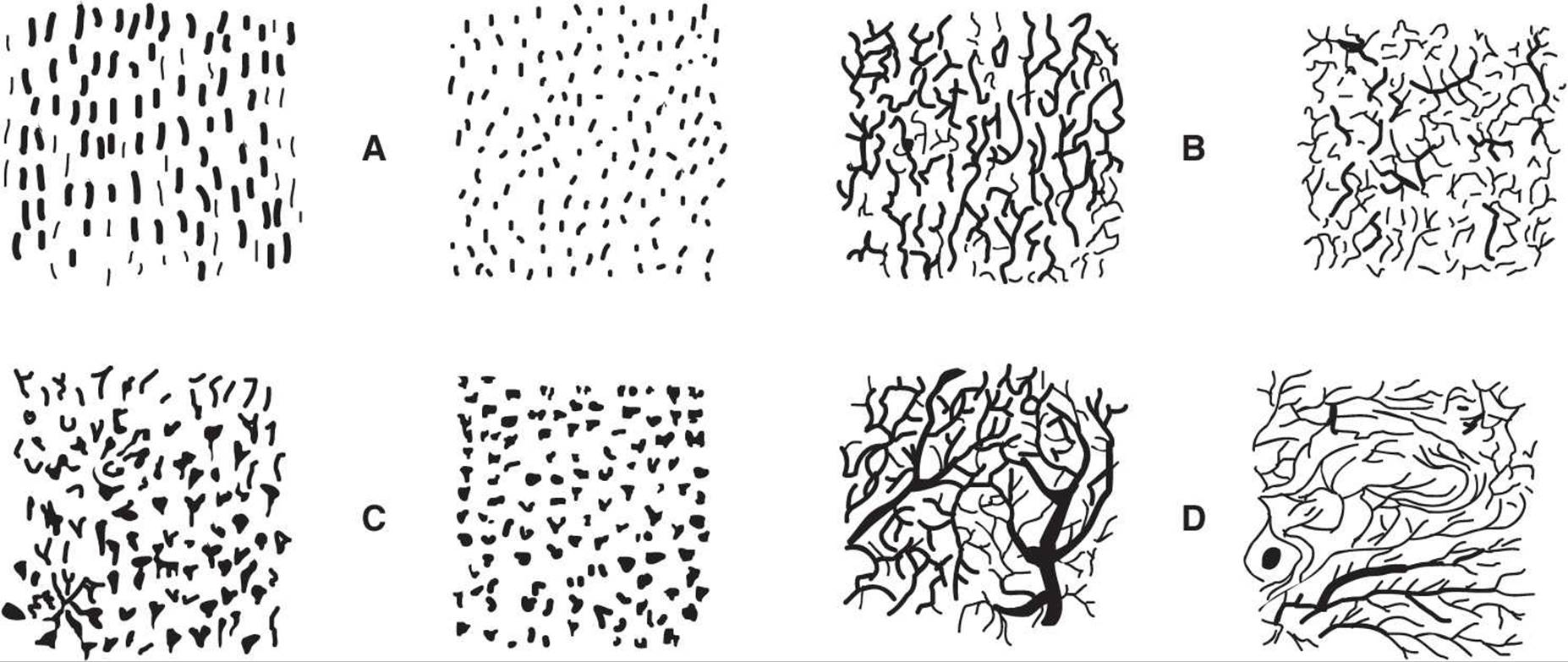
Figure 48–2. Schematic of different types of terminal vessels as observed in the normal squamous epithelium: hairpin capillaries (A), network capillaries (B) both found in normal states, double capillaries (C) seen in Trichomonasinflammation, and branching vessels (D) seen in the transformation zone. (Reproduced, with permission, from Johannisson E, Kolstat P, Soderberg G. Cytologic, vascular, and histologic patterns of dysplasia, carcinoma in situ and early invasive carcinoma of the cervix. Acta Radiol Suppl [Stockh] 1966;258:1.)
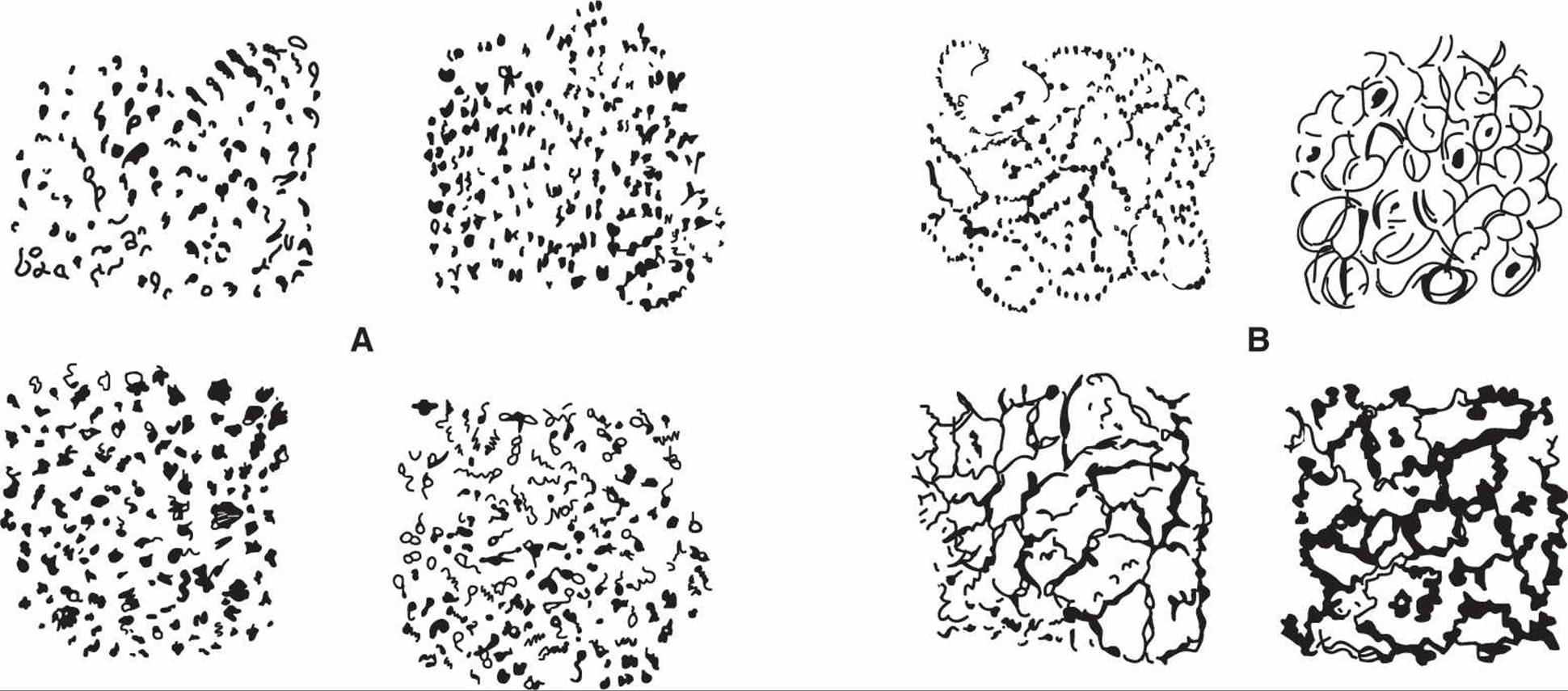
Figure 48–3. Schematic of punctation terminal vessels (A) and mosaic terminal vessels (B). (Reproduced, with permission, from Johannisson E, Kolstat P, Soderberg G. Cytologic, vascular, and histologic patterns of dysplasia, carcinoma in situ and early invasive carcinoma of the cervix. Acta Radiol Suppl [Stockh] 1966;258:1.)
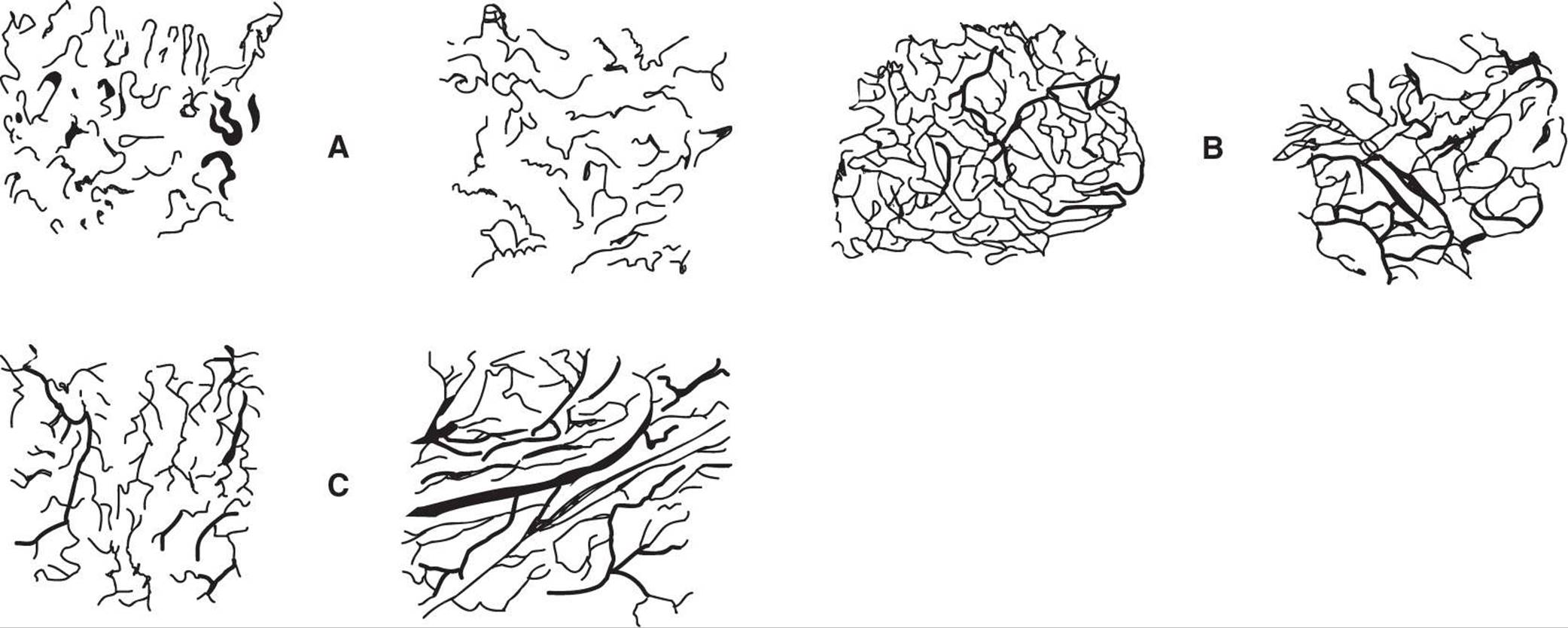
Figure 48–4. Schematic of atypical vessels: hairpinlike (A); networklike (B); and branching type (C). (Reproduced, with permission, from Johannisson E, Kolstat P, Soderberg G. Cytologic, vascular, and histologic patterns of dysplasia, carcinoma in situ and early invasive carcinoma of the cervix. Acta Radiol Suppl [Stockh] 1966;258:1.)
Colposcopically directed punch biopsy of the abnormal areas should be done. The transformation zone extends into the endocervical canal beyond the field of vision in 12–15% of premenopausal women and in a significantly higher percentage of postmenopausal women. Evaluation of the nonvisualized portion of the endocervical canal by endocervical sampling should be performed using a brush or curette, at a minimum, in every case in which colposcopy is unsatisfactory, where the lesion is extending into the endocervical canal, where the colposcopic impression does not explain the cervical cytology findings, or where ablative therapy is contemplated. Endocervical sampling is not indicated in pregnancy. In up to 20% of patients with CIN, the endocervical sampling is positive for dysplasia.
5. Diagnostic conization—Following expert colposcopic evaluation, diagnostic conization of the cervix (Fig. 48–1) is indicated if colposcopy is unsatisfactory, if the lesion extends into the cervical canal beyond the view afforded by the colposcope, if there is dysplasia on the endocervical sampling, if there is a significant discrepancy between the histologic diagnosis of the directed biopsy specimen and the cytologic examination, if ACIS is suspected, or if microinvasive carcinoma is suspected.
Differential Diagnosis
As CIN is generally asymptomatic, it is suspected based on an abnormal cervical cytology test, and diagnosis is confirmed by colposcopy-directed cervical biopsy or endocervical sampling. Abnormal cells on a cervical cytology smear may at times arise from locations other than the uterine cervix, including the vulva, vagina, and, especially in case of abnormal glandular cells, the endometrium and adnexae.
Complications
Understanding the natural history of the various degrees of CIN is central to the appropriate clinical management of these patients. In addition to the degree of dysplasia, it is likely that the course of a specific lesion is also influenced by a number of other factors, such as the patient’s age, the inciting HPV type, the patient’s immune competence, and smoking habits. For individuals who do not clear an HPV infection, longitudinal natural history studies suggest that the time from detection of an infection with high-risk HPV to development of CIN II/III is about 3–5 years and that another 10–20 years pass before the progression to cancer. It is estimated that 30–40% of CIN III actually progresses to cancer.
As summarized in Table 48–1, the majority of CIN I lesions will spontaneously regress without treatment. However, 9–16% of patients with untreated CIN I are diagnosed with CIN II/III over a 2-year follow-up. Spontaneous regression rates of CIN I overall are 60%; in young women, the rates are as high as 91%. Therefore, it is generally reasonable to expectantly follow the compliant patient with CIN I using enhanced surveillance to allow for spontaneous resolution (see following Treatment section). The majority of high-grade lesions will persist or progress (Table 48–1), so immediate treatment is generally warranted.
Table 48–1. Approximate rates of spontaneous regression, persistence, and progression of CIN.
Treatment
Patient management is based on the results of the cervical cytology smear, findings at colposcopy, biopsy and endocervical sampling results, and individual patient characteristics, such as age, wishes regarding future pregnancies, HIV infection, and the likelihood of compliance with management recommendations. Consensus guidelines for the management of women with CIN have been developed and can be found online at the American Society for Colposcopy and Cervical Pathology Web site (www.asccp.org). Management options fall into 2 general categories: expectant management or treatment. Expectant management is appropriate for CIN I when preceded by a cervical cytology smear suggestive of a low-grade lesion (ASC-US, LSIL, or ASC-H). These women have a high chance of spontaneous regression. About 12–13% will be diagnosed with CIN II/III or worse in the subsequent 2 years. Thus, expectant management of these patients entails enhanced surveillance with either 2 cervical cytology specimens every 6 months or 1 HPV test at 12 months and a referral to repeat colposcopy if cytology reveals ASC or worse or the HPV test is positive. If the 2 cervical cytology specimens are normal and/or the HPV test is negative, routine screening may be resumed. Follow-up of women with CIN I beyond 24 months has shown that spontaneous regression or progression continues to occur. There are no data to suggest that it is unsafe to continue close clinical follow-up of a compliant patient with persistent CIN I.
Because we currently lack the means to identify individuals at risk for progressive disease, immediate treatment might be appropriate for high-risk patients likely to be lost to follow-up. On the other hand, CIN I preceded by HSIL or AGC–not otherwise specified has a high prevalence of underlying CIN II/III or worse and is thus managed more aggressively. Acceptable options include a diagnostic excisional procedure, review of all findings, or for patients who desire future childbearing, observation with cytology and colposcopy at 6-month intervals for 1 year. If colposcopy is unsatisfactory or endocervical sampling is positive, a diagnostic excisional procedure should be performed. In this setting, immediate excisional procedure is also the preferred approach for any patients who are beyond childbearing. CIN II and III are high-grade lesions, and prompt treatment is generally recommended except in adolescent and pregnant patients (see later Special Situations section).
Treatment options fall into 1 of 2 main categories: procedures that ablate the abnormal tissue and do not produce a tissue specimen for additional histologic evaluation and procedures that excise the area of abnormality, allowing for further histologic study. Prior to any therapeutic intervention, an assessment has to be made as to whether a patient qualifies for ablative therapy (eg, satisfactory diagnostic evaluation has excluded invasive disease) or if she requires an excisional procedure (conization) for further diagnostic workup. In most cases, conization is also the appropriate therapeutic intervention. If the intraepithelial lesion is confined to the ectocervix, treatment with cryotherapy, laser ablation, or a superficial excision by the loop electro-surgical excision procedure (LEEP) is appropriate. If the lesion extends into the endocervical canal, the endocervical curettage contains dysplastic epithelium, or the colposcopic examination is otherwise unsatisfactory, the endocervical canal must be included in the treatment by a deeper LEEP or cone biopsy (Fig. 48–5). A conization procedure is also indicated in cases of a significant discrepancy between cervical cytology and colposcopy/biopsy results, in cases of suspected microinvasive carcinoma or adenocarcinoma in situ.
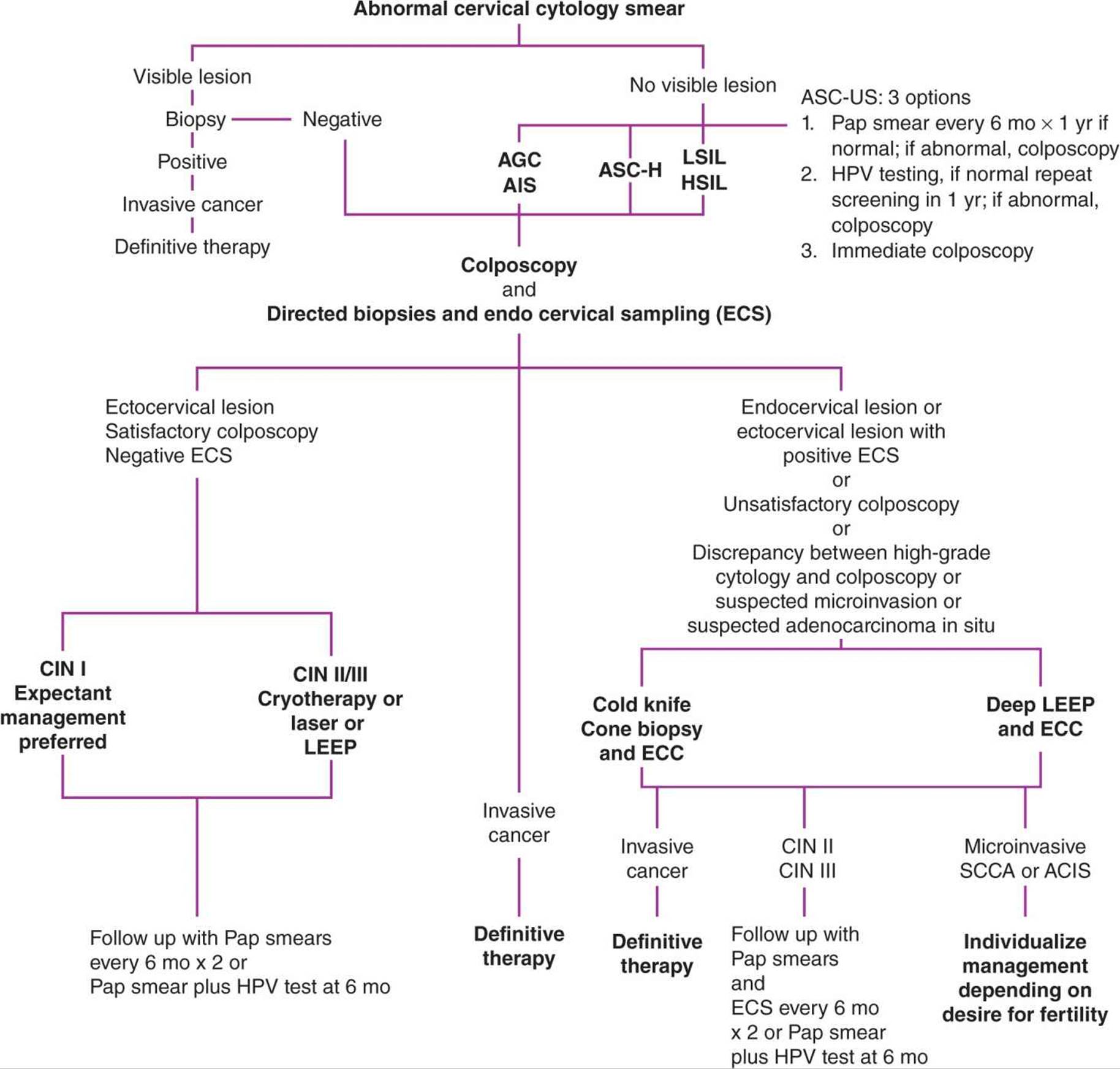
Figure 48–5. Plan for management of the abnormal cytologic smear with visible or no visible cervical lesion. SCCA, squamous cell carcinoma.
The 5 most common techniques for the treatment of CIN include 2 ablative techniques—cryotherapy and laser ablation—and 3 excisional procedures—cold knife conization, laser cone excision, and LEEP. Evidence from controlled trials shows that these techniques are of equal efficacy, averaging 80–90% success rates in the treatment of CIN. Cure depends on the size of the lesion, endocervical gland involvement, margin status of any excisional specimen, and endocervical curettage results.
A. Cryotherapy
In cryotherapy, an office procedure not requiring anesthesia, nitrous oxide or carbon dioxide is used as the refrigerant for a supercooled probe. The cryoprobe is positioned on the ectocervix where it must cover the entire lesion, which at times is not easily achieved. It is then activated until blanching of the cervix extends at least 7 mm beyond the probe in all directions in order to assure that freezing extends beyond the depth of the crypts of the glands into which the dysplasia might be extending. Introduction of a 2-cycle freeze–thaw–freeze technique has improved efficacy. The advantages of cryotherapy include ease of use, low cost, widespread availability, and a low complication rate. Side effects include mild uterine cramping and a copious watery vaginal discharge for several weeks. Infection and cervical stenosis are rare. Follow-up colposcopic examinations can be unsatisfactory because of the inability to visualize the squamocolumnar junction.
B. Carbon Dioxide Laser
Carbon dioxide (CO2) laser can be used either to ablate the transformation zone or as a tool for cone biopsies. The laser destroys tissue with a very narrow zone of injury around the treated tissue and is therefore both precise and flexible. The tissue is vaporized to a depth of at least 7 mm to assure that the bases of the deepest glands are destroyed. Posttreatment vaginal discharge may last 1–2 weeks, and bleeding that requires reexamination can occur in a small percentage of patients. The technique is expensive and requires significant training and attention to safety, as well as local or general anesthesia.
C. Loop Electrosurgical Excision Procedure
LEEP is frequently used for treating CIN II and CIN III because of its ease of use, low cost, and provision of additional tissue for histologic evaluation. LEEP uses a small, fine, wire loop attached to an electrosurgical generator to excise the tissue of interest. Various sizes of wire loop are available. Following LEEP excision of the transformation zone, frequently an additional narrow endocervical specimen (“top hat”) is removed to allow for histologic evaluation while avoiding excessive damage to the cervical stroma. Fulguration with a roller ball electrode is then used to achieve complete hemostasis in the excision bed. LEEP can be performed as an office procedure under local anesthesia. An insulated speculum to prevent conduction of electricity, a grounding pad, and a vacuum to remove the smoke are necessary. Complications are less frequent than with cold knife conization and include bleeding, infection, and cervical stenosis.
D. Cold Knife Conization
Cold knife conization of the cervix refers to the excision of a cone-shaped portion of the cervix using a scalpel. This technique can be individualized to accommodate the cervical anatomy and the size and shape of the lesion. For example, a wide, shallow cone specimen can be obtained from a young patient whose squamocolumnar junction is on the ectocervix. In an older patient, in whom the squamocolumnar junction tends to move more cephalad into the endocervical canal, a narrower, deeper cone is preferable. An endocervical sampling is performed after the conization to assess the remaining endocervical canal. Cervical cone biopsy is generally done in the operating room under local or general anesthesia. Complications include bleeding, infection, cervical stenosis, and cervical insufficiency. The need to perform the procedure in the operating room and a higher complication rate are distinct disadvantages of cold knife conization. However, it results in a specimen devoid of any thermal artifact that may complicate the histologic diagnosis and margin assessment seen with LEEP and laser conization. This becomes particularly important with suspected micro-invasive carcinoma and adenocarcinoma in situ.
Prognosis
Controlled trials show 80–90% success rates in the treatment of CIN, regardless of treatment modality used. Patients with larger lesions, endocervical gland involvement, positive margins, or positive endocervical curettage after an excisional procedure are at higher risk for persistent/recurrent disease than are women with negative margins. Most treatment failures are diagnosed within the first 1–2 years after therapy. A number of follow-up protocols have been advocated including HPV testing, serial cytology, endocervical sampling, colposcopy, or various combinations thereof. HPV testing at 6–12 months posttreatment is highly sensitive at detecting persistent/recurrent CIN and is more sensitive than cytology alone. A recent long-term multicohort study of 435 women treated for CIN II/III demonstrated the value of combined cervical cytology and high-risk HPV testing at 6 and 24 months postprocedure at a referral threshold for further evaluation and treatment if either the cytology test showed ASC or worse or the HPV test was positive: If both tests were negative at 6 months, the risk of persistent or recurrent CIN II/III was 4.6%; if both tests were negative at 6 and 24 months, the risk was 1.8%. In contrast, if either test was positive at 6 months, the risk of persistent CIN II/III or worse was 45–60%, indicating the need for immediate evaluation and treatment for these patients.
Outpatient therapy for CIN can reduce the risk of cervical cancer by 95%. However, the risk of invasive cancer among these patients remains increased for at least 20–25 years, necessitating long-term annual surveillance.
Management of recurrent dysplasia follows the same guidelines outlined in Figure 48–5. If a woman has completed childbearing, recurrent dysplasia can be treated by a simple hysterectomy after invasion has been ruled out. Women with a history of cervical dysplasia have a higher incidence of vaginal dysplasia. These women continue to need Pap tests after hysterectomy.
Impact of Treatment of CIN on Subsequent Fertility & Pregnancy
For women with CIN who desire future childbearing, management priorities are to diagnose and treat preinvasive disease and prevent cervical cancer while minimizing the impact on future fertility and pregnancy. Potential treatment-associated effects on future reproductive outcome include cervical stenosis, alteration of the cervical mucus, and removal or destruction of the collagen matrix of the cervical stroma. It appears that the cervix is better preserved following ablation compared with excision.
One of the main concerns for future pregnancy is the potential for treatment-associated preterm delivery with its associated neonatal morbidity and mortality from prematurity. These risks appear to vary by the type of treatment procedure, and many experts believe the risks are largely related to the amount and depth of tissue removed. Cold knife conization increases the risk of second-trimester pregnancy loss, preterm delivery, and perinatal mortality approximately 3-fold. The risk of preterm delivery increases further with the number of procedures performed. The data on LEEP are more conflicting. While in some studies, LEEP did not increase the risk of preterm delivery and perinatal mortality, others found that LEEP nearly doubles the risk of preterm premature rupture of membranes and preterm delivery. Cryotherapy does not appear to have such strong association with preterm delivery. Thus, strong consideration should be given to offer cryotherapy treatment to women who desire future pregnancy and are candidates for ablative therapy (as discussed earlier).
Special Situations
A. Adolescents & Young Women
Adherence to the ACOG/USPSTF/ACS/ASCCP cervical cancer screening guidelines, which recommend initiation of screening at 21 years of age, should largely obviate the need for the special management algorithms for adolescents and young women found at the American Society for Colposcopy and Cervical Pathology Web site (www.asccp.org), which rest on the guiding principle that expectant management is preferred in females age 20 years old or younger.
B. Pregnancy
Pregnant women routinely undergo cervical cytology screening at their first prenatal visit. As a result, it is not uncommon that an abnormal cervical cytology smear is first discovered during pregnancy. Colposcopy is generally performed for the same indications as in the nonpregnant patient. However, biopsies are limited unless there are colposcopic signs suggestive of high-grade dysplasia, CIS, or invasive disease. Endocervical curettage is not performed in pregnancy because of the potential risk of abortion and infection. The physiologic changes of pregnancy render the transformation zone easily accessible for satisfactory colposcopy by 20 weeks’ gestation in almost all women. Colposcopy during pregnancy can be challenging because pregnancy may produce changes in the cervical epithelium that mimic those of cervical dysplasia. Although the gravid cervix is more vascular, directed ectocervical biopsies can be performed safely with minimal increase in the risk of significant bleeding. After the diagnosis of CIN II/III has been established, the patient can be carefully followed with colposcopic examinations and cervical cytology smears each trimester. Repeat biopsies are only performed for progressive lesions. Treatment is deferred into the postpartum period. Even high-grade lesions discovered during pregnancy have a high rate of regression in the postpartum period. Conization during pregnancy is indicated only if early invasive disease is suspected and the timing and extent of the procedure during pregnancy are individualized. Complications of a cone biopsy in pregnancy include abortion, hemorrhage, infection, and incompetent cervix.
C. HIV Infection
HIV-infected women are more likely to have persistent HPV infection, and CIN is common in HIV-infected women. Based on ACOG guidelines, women who are infected with HIV should undergo cervical cytology screening twice in the first year after diagnosis of HIV infection and then annually. Women with advanced HIV appear to be more likely to have persistent HPV and CIN than those with early HIV infections. Use of highly active antiretroviral therapy (HAART) has been suggested to reduce the risk of CIN and cervical cancer. However, data are conflicting.
Cytologic abnormalities in HIV-infected women should be evaluated in the same manner as in uninfected women. Management of CIN in the HIV-infected patient presents a great challenge. Primary treatment of CIN in HIV-infected women is generally similar to the approach used in HIV-negative women. Generally, expectant management of CIN I is acceptable in HIV-infected women. LEEP excision of the cervix appears to be most appropriate for patients with CIN II/III, and topical 5-fluorouracil cream is recommended by some experts as adjunctive therapy in this setting. Following treatment, the risk of recurrent CIN is high, especially in the immunocompromised patient with low CD4 counts and high viral loads. Recurrence rates may reach 80% within 3 years in markedly immunocompromised women. Thus, surveillance with cervical cytology and colposcopy is recommended by some experts as frequently as every 3 months.
D. Atypical Glandular Cells on Cervical Cytology Smear
Patients with AGCs on a cervical cytology smear have up to a 50% risk of having significant underlying pathology. Nine to 38% of women with AGC have significant neoplasia (CIN II/III, ACIS), and 3–17% have invasive cancer.
The 2001 Bethesda System divides glandular cell abnormalities into AGCs, AGC–favor neoplasia, endocervical ACIS, and adenocarcinoma. Given the high risk for significant pathology, any patient with glandular cell abnormalities on a cervical cytology smear requires immediate evaluation, which includes, at a minimum, colposcopy with careful endocervical sampling. Assessment of the endometrium is recommended in all patients older than age 35 years, in patients at any age with conditions associated with chronic anovulation, in those at increased risk for endometrial cancer, in any women with abnormal bleeding, in women with AGC–endometrial cells, and in women with AGC–nonspecified cell type. Diagnostic conization is indicated in all cases of AGC–favor neoplasia, ACIS, or suspected adenocarcinoma as well as persistent AGC–not otherwise specified, unless a definitive diagnosis has been made on the colposcopy-directed biopsy or endometrial sampling.
E. Adenocarcinoma In Situ
ACIS of the cervix is a precursor of adenocarcinoma of the cervix, which comprises about 25% of cervical cancers in the United States. The incidence of both in situ and invasive disease is rising, especially in young women, with up to 30% of cases occurring in women younger than 35 years of age. As with squamous intraepithelial neoplasia, HPV infection is almost universally found. ACIS has no pathognomonic clinical, cytologic, or colposcopic features. The lesion is not grossly visible on examination. Management is difficult. The lesion is usually at the transformation zone but may be located high in the endocervical canal, involve the deeper portions of the endocervical clefts, or be multifocal with skip lesions. Ten to 13% of ACIS is multifocal, defined as foci of ACIS separated by at least 2 mm of normal mucosa. Nearly half of women with ACIS have concomitant squamous CIN or cancer. Conization with negative margins is required to make the diagnosis of ACIS.
Follow-up surveillance after conization is difficult, as cervical cytology, endocervical curettage, or endocervical cyto-brush sampling each have a sensitivity of only approximately 50%. This is of particular concern because the incidence of residual ACIS or invasive adenocarcinoma following conization for ACIS is as high as 45% with positive conization margins and 27% with negative conization margins. Therefore, conservative management should be undertaken only in the young patient with a negative conization margin and negative endocervical sampling who is fully counseled and desires to maintain her fertility. After completion of childbearing, hysterectomy is generally recommended. In all other patients, hysterectomy should be performed as a definitive therapeutic intervention. Approximately 7% of patients with positive and 2% of patients with negative conization margins will have invasive disease on the hysterectomy specimen. Thus, extra-fascial hysterectomy can be recommended for those patients with negative conization margins. If conization margins are positive, prehysterectomy repeat conization is recommended or consideration can be given to the performance of a modified radical hysterectomy, especially if there is significantly altered anatomy following prior conization procedures or extensive disease and positive margins were found on the preceding conization specimen.
Ahdieh L, Muñoz A, Vlahov D, et al. Cervical neoplasia and repeated positivity of human papillomavirus infection in human immunodeficiency virus-seropositive and -seronegative women. Am J Epidemiol2000;151:1148–1157. PMID: 10905527.
American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Gynecology. ACOG Practice Bulletin no. 109: cervical cytology screening. Obstet Gynecol 2009;114: 1409–1420. PMID: 20134296.
Arbyn M, Buntinx F, Van Ranst M, et al. Virologic versus cytologic triage of women with equivocal Pap smears: a meta-analysis of the accuracy to detect high-grade intraepithelial neoplasia. J Natl Cancer Inst2004;96:280–293. PMID: 14970277.
Arbyn M, Kyrgiou M, Simoens C, et al. Perinatal mortality and other severe adverse pregnancy outcomes associated with treatment of cervical intraepithelial neoplasia: meta-analysis. BMJ 2008;337:a1284. doi: 10.1136/bmj.a1284. PMID: 18808168.
Arends MJ, Buckley CH, Wells M. Etiology, pathogenesis, and pathology of cervical neoplasia. J Clin Pathol 1998;51:96–103. PMID: 9602680.
Atypical Squamous Cell of Undetermined Significance/Low-Grade Squamous Intraepithelial Lesions Triage Study (ALTS) Group. Human papillomavirus testing for triage of women with cytologic evidence of low-grade squamous intraepithelial lesions: baseline data from a randomized trial. J Natl Cancer Inst 2000;92:397–402. PMID: 10700419.
Atypical Squamous Cell of Undetermined Significance/Low-Grade Squamous Intraepithelial Lesions Triage Study (ALTS) Group. Results of a randomized trial on the management of cytology interpretations of atypical squamous cells of undetermined significance. Am J Obstet Gynecol 2003;188:1383–1392. PMID: 12824967.
Centers for Disease Control and Prevention (CDC). FDA licensure of bivalent human papillomavirus vaccine (HPV2, Cervarix) for use in females and updated HPV vaccination recommendations from the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep 2010;59:626–629. PMID: 20508593.
Denehy TR, Gregori CA, Breen JL. Endocervical curettage, cone margins, and residual adenocarcinoma in situ of the cervix. Obstet Gynecol 1997;90:1–6. PMID: 9207802.
FUTURE II Study Group. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions. N Engl J Med 2007;356:1915–1927. PMID: 17492945.
Gage JC, Hanson VW, Abbey K, et al. Number of cervical biopsies and sensitivity of colposcopy. Obstet Gynecol 2006;108:264–272. PMID: 16880294.
Harper DM, Franco EL, Wheeler C, et al. Efficacy of a bivalent L1 virus-like particle vaccine in prevention of infection with human papillomavirus types 16 and 18 in young women: a randomised controlled trial. Lancet2004;364:1757–1765. PMID: 15541448.
Ho GY, Bierman R, Beardsley L, et al. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med 1998;338:423–428. PMID: 9459645.
Holowaty P, Miller AB, Rohan T, To T. Natural history of dysplasia of the uterine cervix. J Natl Cancer Inst 1999;91:252–258. PMID: 10037103.
Im DD, Duska LR, Rosenshein NB. Adequacy of conization margins in adenocarcinoma in situ of the cervix as a predictor of residual disease. Gynecol Oncol 1995;59:179–182. PMID: 7590468.
Kocken M, Helmerhorst TJ, Berkhof J, et al. Risk of recurrent high-grade cervical intraepithelial neoplasia after successful treatment: a long-term multi-cohort study. Lancet Oncol 2011;12:441–450. PMID: 21530398.
Koutsky LA, Ault KA, Wheeler CM, et al. A controlled trial of a human papillomavirus type 16 vaccine. N Engl J Med 2002; 347:1645–1651. PMID: 12444178.
Kyrgiou M, Koliopoulos G, Martin-Hirsch P, et al. Obstetric outcomes after conservative treatment for intraepithelial or early invasive cervical lesions: systematic review and meta-analysis. Lancet2006;367:489–498. PMID: 16473126.
Lea JS, Shin CH, Sheets EE, et al. Endocervical curettage at conization to predict residual cervical adenocarcinoma in situ. Gynecol Oncol 2002;87:129–132. PMID: 12468353.
Martin-Hirsch PL, Paraskevaidis E, Kitchener H. Surgery for cervical intraepithelial neoplasia. Cochrane Database Syst Rev 2000;2:CD001318. PMID: 10796771.
McCredie MR, Sharples KJ, Paul C, et al. Natural history of cervical neoplasia and risk of invasive cancer in women with cervical intraepithelial neoplasia 3: a retrospective cohort study. Lancet Oncol2008;9:425–434. PMID: 18407790.
McIndoe WA, McLean MR, Jones RW, et al. The invasive potential of carcinoma in situ of the cervix. Obstet Gynecol 1984;64:451–458. PMID: 6483293.
Melnikow J, Nuovo J, Willan AR, et al. Natural history of cervical squamous intraepithelial lesions: a meta-analysis. Obstet Gynecol 1998;92:727–735. PMID: 9764690.
Moscicki AB, Shiboski S, Hills NK, et al. Regression of low-grade squamous intraepithelial lesions in young women. Lancet 2004;364:1678–1683. PMID: 15530628.
Moyer VA, on behalf of the U.S. Preventive Services Task Force. Ann Int Med 2012 Mar 14 [Epub ahead of print].
Munoz N, Bosch FX, de Sanjosé S, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med 2003;348:518–527. PMID: 12571259.
Noehr B, Frederiksen K, Tabor A, et al. Loop electrosurgical excision of the cervix and subsequent risk for spontaneous preterm delivery: a population-based study of singleton deliveries during a 9-year period. Am J Obstet Gynecol 2009;114:511–515. PMID: 19701028.
Olsen AO, Dillner J, Skrondal A, Magnus P. Combined effect of smoking and human papillomavirus type 16 infection in cervical carcinogenesis. Epidemiology 1998;9:346–349. PMID: 9583429.
Paavonen J, Naud P, Salmerón J, et al. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): final analysis of a double-blind, randomised study in young women. Lancet 2009;374:301–314. PMID: 19586656.
Poynor EA, Barakat RR, Hoskins WJ. Management and follow-up of patients with adenocarcinoma in situ of the uterine cervix. Gynecol Oncol 1995;57:158–164. PMID: 7729727.
Prokopczyk B, Cox JE, Hoffmann D, et al. Identification of tobacco-specific carcinogen in the cervical mucus of smokers and non-smokers. J Natl Cancer Inst 1997;89:868–873. PMID: 9196253.
Saslow D, Runowicz CD, Solomon D, et al. American Cancer Society guideline for the early detection of cervical neoplasia and cancer. CA Cancer J Clin 2002;52:342–362. PMID: 12469763.
Saslow D, Solomon, Lawson HW et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology Screening Guidelines for the Prevention and Early Detection of Cervical Cancer. CA Cancer J Clin 2012;62:147–172. PMID: 22422631.
Solomon D, Davey D, Kurman R, et al. The 2001 Bethesda system terminology for reporting results of cervical cytology. JAMA 2002;287:2114–2119. PMID: 11966386.
Solomon D, Schiffman M, Tarone R. Comparison of three management strategies for patients with atypical squamous cells of undetermined significance: baseline results from a randomized trial. J Natl Cancer Inst2001;93:293–299. PMID: 11181776.
Soutter WP, de Barros Lopes A, Fletcher A, et al. Invasive cervical cancer after conservative therapy for cervical intraepithelial neoplasia. Lancet 1997;349: 978–980. PMID: 9100623.
Stanley M. Pathology and epidemiology of HPV infection in females. Gynecol Oncol 2010;117(2 suppl):S5–S10. PMID: 20304221.
Wallin KL, Wiklund F, Angström T, et al. Type-specific persistence of human papillomavirus DNA before the development of invasive cervical cancer. N Engl J Med 1999;341:1633–1670. PMID: 10572150.
Wolf JK, Levenback C, Malpica A, et al. Adenocarcinoma in situ of the cervix: significance of cone biopsy margins. Obstet Gynecol 1996;88:82–86. PMID: 8684768.
Wright TC Jr, Massad LS, Dunton CJ, et al. 2006 consensus guidelines for the management of women with abnormal cervical cancer screening tests. Am J Obstet Gynecol 2007;197:346–355. PMID: 17904957.
Wright TC Jr, Massad LS, Dunton CJ, et al. 2006 consensus guidelines for the management of women with cervical intraepithelial neoplasia or adenocarcinoma in situ. Am J Obstet Gynecol 2007;197:340–345. PMID: 17904956.
Ylitalo N, Sørensen P, Josefsson AM, et al. Consistent high viral load of human papillomavirus 16 and risk of cervical carcinoma in situ: a nested case-control study. Lancet 2000;355:2194–2198. PMID: 10881892.
Yost NP, Santoso JT, McIntire DD, et al. Postpartum regression rates of antepartum cervical intraepithelial neoplasia II and III lesions. Obstet Gynecol 1999;93:359–362. PMID: 10097949.
CANCER OF THE CERVIX
ESSENTIALS OF DIAGNOSIS
![]() Early disease is frequently asymptomatic, underscoring the importance of cervical cytology screening.
Early disease is frequently asymptomatic, underscoring the importance of cervical cytology screening.
![]() Abnormal uterine bleeding and vaginal discharge are the most common symptoms.
Abnormal uterine bleeding and vaginal discharge are the most common symptoms.
![]() A cervical lesion may be visible on inspection as a tumor or ulceration; cancer within the cervical canal may be occult.
A cervical lesion may be visible on inspection as a tumor or ulceration; cancer within the cervical canal may be occult.
![]() Diagnosis must be confirmed by biopsy.
Diagnosis must be confirmed by biopsy.
General Considerations
In the United States, an estimated 12,710 new cases of invasive cervical cancer are diagnosed annually, and there are 4290 deaths from the disease. In contrast, with more than 529,000 new cases diagnosed annually and a >50% mortality rate, cervical cancer is the second most common cause of cancer-related morbidity and mortality among women in developing countries. This dichotomy is largely the result of a 75% decrease in the incidence of cervical cancer in developed countries following the implementation of population-based screening programs and treatment of preinvasive disease. The average age at diagnosis of patients with cervical cancer is 51 years. However, the disease can occur in the second decade of life and during pregnancy, and nearly 20% of cervical cancers are diagnosed in women age 65 or older. More than 95% of patients with early cancer of the cervix can be cured.
Pathogenesis
The major epidemiologic risk factors for cervical cancer are the same as those for CIN and were discussed earlier. HPV is central to the development of cervical neoplasia. HPV DNA is found in 99.7% of all cervical carcinomas. HPV-16 is the most prevalent HPV type in squamous cell carcinoma and adenocarcinoma, followed by HPV-18 and HPV-45. Other associated risk factors are tobacco use, immunosuppression, infection with HIV or a history of other STIs, high parity, and oral contraceptive use.
HPV is epitheliotropic. Once the epithelium is acutely infected with HPV, 1 of 3 clinical scenarios ensues:
1. Asymptomatic latent infection;
2. Active infection in which HPV undergoes vegetative replication but not integration into the genome (eg, leading to condyloma or CIN I); or
3. Neoplastic transformation following integration of oncogenic HPV DNA into the human genome.
The virus infects a subset of primitive basal cells in the epithelium where it will undergo replication. The infected cell then enters the proliferating epithelial component. Active infection, in which HPV undergoes replication but remains episomal, is characterized by minimal viral oncogene expression. However, integration of HPV into the human genome is associated with cell immortalization, allowing for malignant transformation. This involves an upregulation of the viral oncogenes E6 and E7. These oncoproteins interfere with cell-cycle control in the human host cell. E6 and E7 have the ability to complex with the tumor suppressor genes p53 and Rb, respectively. The disabling of these 2 major tumor suppressor genes is thought to be central to host cell immortalization and transformation induced by HPV and the observed increased genetic instability.
Incipient cancer of the cervix is generally a slowly developing process. Most cervical cancers probably begin as a high-grade dysplastic change (see previous section) or CIS with gradual progression over a period of several years. At least 90% of carcinomas of the cervix develop from the intraepithelial layers, almost always within 1 cm of the squamocolumnar junction of the cervix either on the portio vaginalis of the cervix or slightly higher in the endocervical canal.
Early stromal invasion (stage IA1) up to a depth of 3 mm below the basement membrane is a localized process, provided there is no pathologic evidence of lymphovascular space involvement. Penetration of the stroma beyond this point carries an increased risk of lymphatic metastasis (Table 48–2). When the lymphatics are involved, tumor cells are carried to the regional pelvic lymph nodes (parametrial, hypogastric, obturator, external iliac, and sacral) (Fig. 48–6). The more pleomorphic or extensive the local disease, the greater is the likelihood of lymph node involvement. As the tumor grows, it also spreads by direct extension to the parametria.
Table 48–2. Risk of any lymph node metastasis for patients with microscopic squamous cell carcinoma of the cervix.
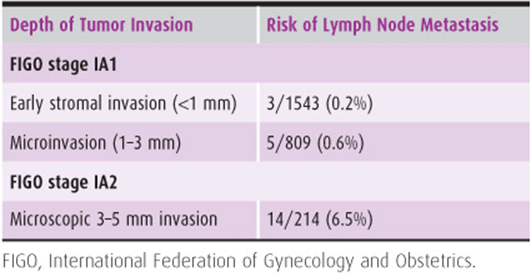

Figure 48–6. Lymphatic spread of carcinoma of the cervix.
Squamous cell carcinoma clinically confined to the cervix involves the regional pelvic lymph nodes in 15–20% of cases. When the cancer involves the parametrium (stage IIB), tumor cells can be found in the pelvic lymph nodes in 30–40% of cases and in the para-aortic nodes in approximately 15–30% of cases. The more advanced the local disease, the greater is the likelihood of distant metastases. The para-aortic nodes are involved in approximately 45% of patients with stage IVA disease.
Ovarian involvement is rare, occurring in approximately 0.5% of squamous cell carcinomas and 1.7% of adenocarcinomas. The liver and lungs are the most common sites of blood-borne metastasis, but the tumor may involve the brain, bones, bowels, adrenal glands, spleen, or pancreas.
When cancer of the cervix is untreated or fails to respond to treatment, death occurs in 95% of patients within 2 years after the onset of symptoms. Death can occur from uremia, pulmonary embolism, or hemorrhage from direct extension of tumor into blood vessels. Life-threatening sepsis from complications of pyelonephritis or vesicovaginal and rectovaginal fistulas is possible. Large bowel obstruction from direct extension of tumor into the rectosigmoid can be the terminal event. Pain from perineural extension is a significant management problem of advanced disease.
Pathology
Approximately 70–75% of cervical carcinomas are squamous cell; the remainder are composed of various types of adenocarcinomas (20–25%), adenosquamous carcinomas (3–5%), and undifferentiated carcinomas.
A. Squamous Cell Carcinomas
Cervical squamous cell carcinomas have been classified according to the predominant cell type: large cell nonkeratinizing, large cell keratinizing, and small cell carcinomas. The large cell nonkeratinizing variety accounts for the majority of tumors.
B. Verrucous Squamous Carcinoma
Verrucous squamous carcinoma, which has been associated with HPV-6, is a rare subtype of well-differentiated squamous carcinoma. It is a slow-growing, locally invasive neoplasm. Histologically, this tumor is composed of well-differentiated squamous cells with frondlike papillae and little apparent stromal invasion, but it is potentially lethal. Radical resection is the mainstay of therapy.
C. Papillary Squamous Carcinoma
Papillary squamous carcinoma of the cervix is characterized by highly dysplastic squamous cells forming papillary fronds with thin fibrovascular cores. The gross appearance of this lesion may be warty or fungating.
D. Adenocarcinoma
Adenocarcinoma of the cervix is derived from the glandular elements of the cervix. The incidence of adenocarcinomas, including the mucinous, endometrioid, clear cell, and serous types, has been rising over the last several decades, especially in women younger than 35 years of age. Part of this increase may be a result of an increasing prevalence of HPV infection, and part may be a result of improvements in screening and prevention of squamous preinvasive disease, thus leading to a histologic shift toward adenocarcinoma. When the initial growth of adenocarcinoma of the cervix is within the endocervical canal and the ectocervix appears normal, this lesion might not be diagnosed until it is advanced and ulcerative. Cervical adenocarcinoma is subdivided into endocervical type (usual type; minimal deviation adenocarcinoma [adenoma malignum] and well-differentiated villoglandular adenocarcinoma), endometrioid type, clear cell type, papillary serous type, intestinal type, mesonephric type, and mixed type. The clear cell type may be related to in utero exposure to DES. It has a prognosis comparable to that of other adenocarcinomas of the cervix.
E. Minimal Deviation Adenocarcinoma (Adenoma Malignum)
Adenoma malignum, or minimal deviation adenocarcinoma, is an extremely well-differentiated adenocarcinoma that may be difficult to recognize as a malignant process. It represents approximately 1% of adenocarcinomas of the cervix and has been associated with Peutz-Jeghers syndrome. It occurs mainly in the fifth and sixth decades of life. Diagnosis is often delayed because of frequently normal cervical cytology smears. Punch biopsies are often nondiagnostic, requiring conization for further evaluation.
F. Adenoid Cystic Carcinoma
Another uncommon variant of adenocarcinoma is adenoid cystic carcinoma. This lesion is considered more aggressive than most cervical adenocarcinomas and occurs more commonly in black women of high parity in their sixth and seventh decades of life. It should not be confused with adenoid basal carcinomas, which have an indolent growth pattern.
G. Adenosquamous Carcinoma
Adenosquamous carcinomas contain an admixture of malignant squamous and glandular cells; subtypes include the mature type, signetring type (mucoepidermoid carcinoma), and glassy cell type. Glassy cell carcinoma is a poorly differentiated form of adenosquamous carcinoma and is considered to have an extremely aggressive course. It accounts for approximately 1–2% of cervical cancers. Synchronous adenocarcinomas and squamous cell carcinomas that invade each other are called collision tumors.
H. Neuroendocrine Carcinomas
Approximately one-third of small cell carcinomas of the cervix stain positive for neuroendocrine markers (neuron-specific enolase, chromogranin, synaptophysin). These tumors need to be distinguished from small cell type of squamous tumors. They have a high frequency of lymphovascular space invasion, lymph node metastases, recurrence, and poor survival. Neuroendocrine carcinomas are not limited to the small-sized tumor cells. Poorly differentiated large cell carcinomas may express neuroendocrine differentiation by immunohistochemistry. Carcinoid tumors, arising from the argyrophil cells of the endocervical epithelium, are malignant but have rarely been associated with the carcinoid syndrome. Because of their propensity for early systemic spread, systemic chemotherapy is an integral part of the treatment of neuroendocrine tumors of the cervix.
I. Other Malignant Tumors
Direct extension of metastatic tumors to the cervix includes those originating from the endometrium, rectum, and bladder. Lymphatic or vascular metastases occur less often but are associated with endometrial, ovarian, gastric, breast, colon, kidney, and pancreas carcinomas. Sarcomas, lymphomas, choriocarcinomas, and melanomas are encountered rarely in the cervix.
Prevention
Until now, prevention of morbidity and death from cervical cancer largely involved recognition and treatment of preinvasive and early invasive disease. Over 60% of women who develop cervical cancer in developed countries either never have been screened or have not been screened in the preceding 5 years. Risk factors must be recognized, and screening, treatment intervention, and patient education must be modified.
Universal cytologic screening of all women age 21 years or older must be continued on a regular basis until better, more sensitive and specific means of screening are found and outreach into underserved areas is improved. Women with preinvasive cervical neoplasia should be treated and followed up closely (Fig. 48–5). It is important to remember that cervical cytology smears are of limited value in detecting frankly invasive disease, with some studies finding false-negative rates up to 50%. Sexual abstinence is an effective but impractical prophylactic measure. Education of young women and men about risk factors and the necessity for regular screening, as well as information about the association of HIV infection and smoking with the development of cervical cancers, is crucial.
The role of HPV vaccination has been discussed earlier.
Clinical Findings
A. Symptoms & Signs
Abnormal vaginal bleeding is the most common symptom of invasive cancer and may take the form of a blood-stained leukorrheal discharge, scant spotting, or frank bleeding. Leukorrhea, usually sanguineous or purulent, odorous, and nonpruritic, is frequently present. A history of postcoital bleeding may be elicited on specific questioning.
Pelvic pain, often unilateral and radiating to the hip or thigh, is a manifestation of advanced disease, as is the involuntary loss of urine or feces through the vagina, a sign of fistula formation. Weakness, weight loss, and anemia are characteristic of the late stages of the disease, although acute blood loss and anemia may occur in a bulky or ulcerating stage I lesion.
Physical examination findings include a grossly normal-appearing cervix with preclinical disease. As the local disease progresses, physical signs appear. Infiltrative cancer produces enlargement, irregularity, and a firm consistency of the cervix and eventually of the adjacent parametria. The growth pattern can be endophytic, leading to a barrel-shaped enlargement of the cervix, or exophytic, where the lesion generally appears as a friable, bleeding, cauliflowerlike lesion of the portio vaginalis. Ulceration may be the primary manifestation of invasive carcinoma; in the early stages, the change often is superficial, so that it may resemble an ectropion or chronic cervicitis. With further progression of the disease, the ulcer becomes deeper and necrotic, with indurated edges and a friable, bleeding surface. The adjacent vaginal fornices may become involved next. Eventually, extensive parametrial involvement by the infiltrative process may produce a nodular thickening of the uterosacral and cardinal ligaments with resultant loss of mobility and fixation of the cervix.
B. Biopsy
Because of the failure of malignant cells to desquamate and the obscuring effect of inflammatory cells, it is not uncommon for an invasive carcinoma of the cervix to exist despite a negative cytologic smear. Any suspicious lesion of the cervix should be sampled by adequate biopsy, regardless of cytologic examination result. Biopsy of any Schiller-positive areas or of any ulcerative, granular, nodular, or papillary lesion provides the diagnosis in most cases. Colposcopically directed biopsies with endocervical sampling or conization of the cervix may be required when reports of suspicious or probable exfoliated carcinoma cells are made by the pathologist and a visible or palpable lesion of the cervix is not evident. Colposcopic warning signs of early invasive cancer in a field of CIN include capillaries that are markedly irregular, appearing as commas, corkscrews, and spaghetti-shaped vessels with great variation in caliber and abrupt changes in direction, often causing acute angles. Ulcerations or a markedly irregular appearance of the cervix with a waxy, yellowish surface and numerous bizarre, atypical blood vessels are common. Bleeding may occur also after slight irritation.
C. Conization
In the setting of a biopsy revealing CIS, where invasion cannot be ruled out, or in the setting of a negative colposcopy in the face of a significantly abnormal cervical cytology smear, conization of the cervix should be performed to determine the presence or absence of invasion. If a cervical biopsy shows microinvasive cancer (<3 mm of invasion), a cone biopsy is necessary to rule out deeper invasion. The conization specimen should be properly marked for the pathologist (eg, with a pin or small suture), so that the area of involvement can be specifically localized in relation to the circumference and margins of the cervix. Conization for a lesion grossly suggestive of invasive cancer is not indicated, as it only delays the initiation of appropriate therapy and predisposes the patient to serious pelvic infections and bleeding. The diagnosis of such a lesion can almost always be confirmed by simple cervical biopsy.
D. Radiologic Findings
Chest radiographs are indicated in all patients with cervical cancer and an intravenous pyelogram (IVP) or computed tomography (CT) urogram should be performed to determine if there is any ureteral obstruction producing hydroureter and hydronephrosis. Magnetic resonance imaging (MRI), CT scan, lymphangiography, or positron emission tomography (PET) scanning may demonstrate involvement of the pelvic or periaortic lymph nodes or other sites of metastases. The sensitivities of CT, MRI, and PET for lymph node metastases in cervical cancer are approximately 45%, 60%, and 80%, respectively. Integrated PET CT appears to have a slightly higher sensitivity for detecting nodal metastases than PET alone. Although the latter imaging studies are not used to assign disease stage in the International Federation of Gynecology and Obstetrics (FIGO) classification, they may be of value for planning treatment, particularly the extent of the radiation therapy field or scope of surgery.
Clinical Staging
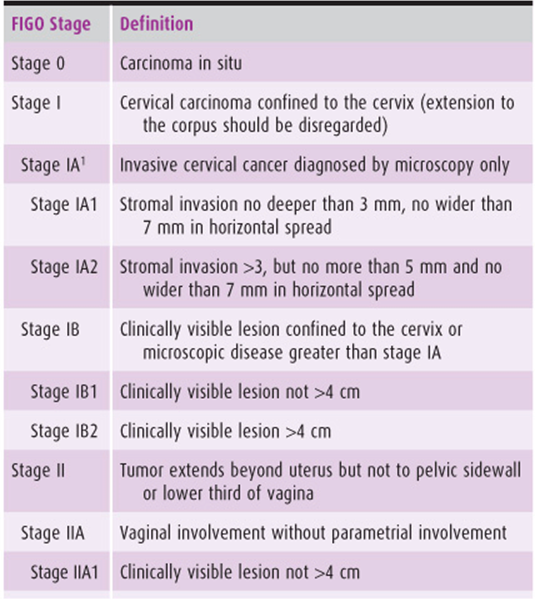
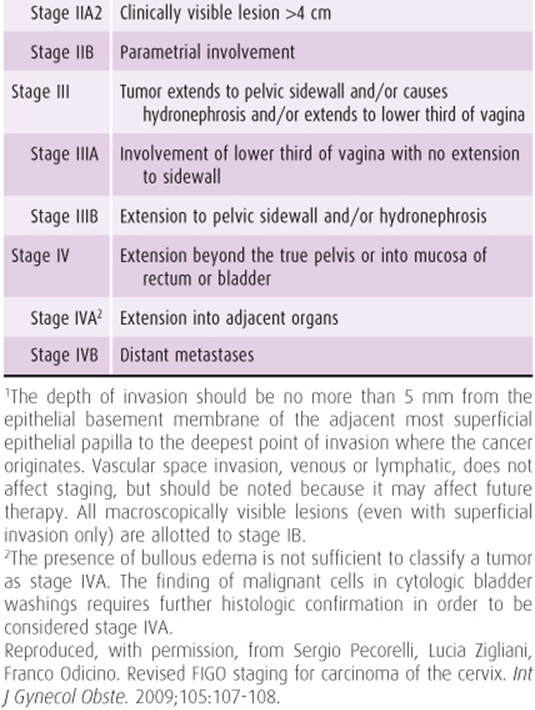
It is important to estimate the extent of the disease not only for prognostic purposes, but also for treatment planning. Clinical staging also affords a means of comparing methods of therapy for various stages of the disease worldwide. The classification adopted by FIGO is the most widely used staging system (Table 48–3). Cervical cancer is staged by clinical examination and evaluation of the bladder, ureters, and rectum. If the lesion is clearly confined to the cervix by office examination, only chest radiography and evaluation of the ureters by IVP or CT scan with intravenous contrast are necessary to assign the stage. If it is not possible to evaluate the extent of local disease in the office, examination under anesthesia with cystoscopy and proctoscopy may be necessary. Although CT scan, MRI, lymphangiography, and PET scan may offer information helpful for treatment planning, these findings do not change the FIGO stage of disease. The FIGO stage of disease is also not changed by surgicopathologic findings of metastatic disease at the time of radical hysterectomy or lymphadenectomy.
Table 48–3. 2009 International Federation of Gynecology and Obstetrics (FIGO) staging of cervical cancer.
Differential Diagnosis
A variety of lesions of the cervix can be confused with cancer. Entities that must sometimes be ruled out include cervical ectropion, acute or chronic cervicitis, condyloma acuminata, cervical tuberculosis, ulceration secondary to STD (syphilis, granuloma inguinale, lymphogranuloma venereum, chancroid), abortion of a cervical pregnancy, metastatic choriocarcinoma or other cancers, and rare lesions such as those of actinomycosis or schistosomiasis. Histopathologic examination is usually definitive.
Complications
The complications of cervical cancer, for the most part, are those related to tumor size or invasion, necrosis of the tumor, infection, and metastatic disease. The natural history of the disease was outlined earlier. There are also problems pertaining to treatment of the disease (eg, radical surgery or radiation therapy; see next section, Treatment).
Treatment
Invasive carcinoma of the cervix spreads primarily by direct extension and lymphatic dissemination. The therapy of patients with cervical cancer needs to address not only the primary tumor site, but also the adjacent tissues and lymph nodes. This is generally accomplished by either radical hysterectomy and pelvic lymphadenectomy, radiation with concomitant chemotherapy, or a combination thereof.
A. Treatment of Early-Stage Disease (Stage IA2 to IIA2)
Patients with early-stage cervical cancer may be treated either with radical hysterectomy and pelvic lymphadenectomy or with primary radiation with concomitant chemotherapy. The overall 5-year cure rates for surgery and for radiation therapy in operable patients are approximately equal. The advantages of surgery are that the ovaries may be left intact and be transposed out of the radiation field if adjuvant postoperative therapy appears necessary, that the extent of disease can be determined surgicopathologically, and that grossly metastatic lymph nodes can be resected. Furthermore, surgery may be more appropriate in sexually active women with early-stage disease as radiation causes vaginal stenosis and atrophy. Adjuvant radiation with or without concomitant chemotherapy is administered to selected patients at increased risk for recurrence following radical hysterectomy.
1. Radical hysterectomy & therapeutic lymphadenectomy—Radical hysterectomy (techniques initially described by Wertheim, Meigs, and Okabayashi) with pelvic lymphadenectomy is the surgical procedure for invasive cancer limited to the cervix and upper vagina (stages I and II). The operation is technically difficult and should be performed only by those experienced in radical pelvic surgery. Surgery involves dissection of the ureters from the paracervical structures so that the ligaments supporting the uterus and upper vagina can be removed. When the operation is done vaginally, a deep Schuchardt (paravaginal) incision is required for exposure. Five different types of hysterectomy have been described based on the extent of parametrial dissection and vaginal tissue removed (Table 48–4). Typically, a type I hysterectomy is indicated for patients with stage IA1 disease. An alternative treatment is cervical conization in the young patient wishing to preserve fertility. Stage IA2 to IIA2 can be treated with a type II (modified radical) or type III (radical) hysterectomy. It is rarely necessary to remove as much vaginal tissue as was initially recommended. As long as complete tumor clearance can be provided, a modified radical hysterectomy appears to provide therapeutic outcomes comparable to a radical hysterectomy for stage IB and IIA disease, but with shorter operating time and lower urologic morbidity. Full pelvic lymphadenectomy is indicated at the time of radical hysterectomy, followed by para-aortic lymphadenectomy for tumors larger than 2 cm or those with suspicious pelvic lymph nodes. Resection of all grossly involved lymph nodes provides a distinct survival advantage. Microscopic evaluation of the lymph nodes allows for tailoring of the postoperative radiation field, if indicated.
Table 48–4. Types of hysterectomy based on radicality.
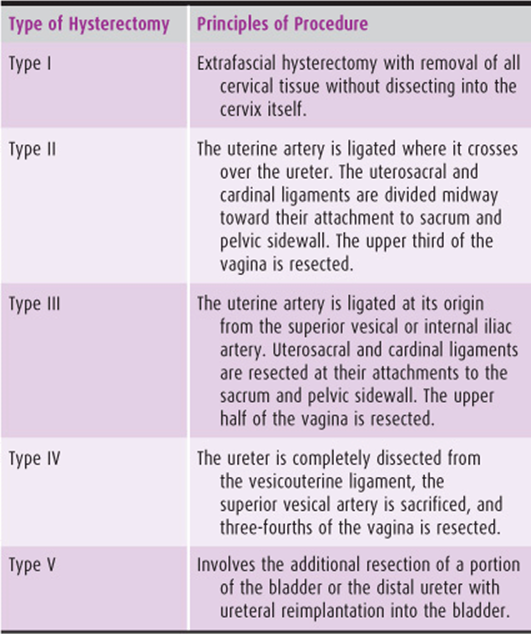
2. Adjuvant postoperative radiation with or without concomitant chemotherapy—Postoperative adjuvant radiation therapy with concomitant chemotherapy is indicated in women with localized cervical cancer at high risk for recurrent disease, such as positive lymph nodes, positive or close resection margins, or microscopic parametrial involvement. In this setting, adjuvant radiation with platinum-based chemotherapy is superior to adjuvant radiation alone, with an improvement in the 4-year progression-free interval from 63% to 80%. Women with intermediate-risk factors for recurrent disease, such as large tumor size, deep cervical stromal invasion, and lymphovascular space invasion, also benefit from postoperative adjuvant radiation. These patients have an improved 2-year recurrence-free survival of 88% with adjuvant radiation versus 79% without adjuvant therapy. Whether the addition of chemotherapy to the adjuvant radiation further improves outcomes for women with intermediate-risk factors is currently under investigation.
3. Primary radiation with concomitant chemotherapy—For the treatment of early cervical cancer (stages IA to IIA), primary therapy with definitive radiation or radical surgery followed by tailored radiation if indicated by the surgical findings produces comparable outcomes. The choice of treatment depends on the tumor size, the general condition of the patient, and patient preferences. Surgery is often preferred for young patients in the hope of preserving ovarian function. If it is likely that the patient will need postoperative radiation therapy, transposition of the ovaries to a location outside the radiation field can be performed. The main argument for primary chemoradiation exists in patients with larger tumors, due to the added morbidity of triple-modality therapy (see later section Special Situations; bulky stage IB2 and IIA2 cervical cancer). For primary radiation of cervical cancer, external-beam radiation is used in combination with intracavitary irradiation (see Chapter 52). At least 5 controlled trials have demonstrated the superiority of radiation with concomitant platinum-based chemotherapy over radiation alone. This has led to the adoption of radiation plus concomitant chemotherapy as the standard of care whenever radiation therapy is given for the treatment of cervical cancer over a broad spectrum of disease stages.
B. Treatment of Locally Advanced Disease (Stage IIB to IVA)
Patients with locally advanced cervical cancer are best treated with primary radiation (external beam plus brachy-therapy; see Chapter 52) with concomitant chemotherapy. Extended-field radiation should be considered in the presence of para-aortic lymph node metastases documented at surgical staging or by imaging, especially when biopsy confirmed and in the absence of other systemic metastases. The benefit of cisplatin-based combined-modality therapy over radiation alone for advanced disease has been demonstrated in at least 3 randomized controlled trials, which found a 30–50% reduction in the risk of death from cervical cancer for patients treated with chemoradiation compared to those treated with radiation alone. This difference is most significant for patients with stage II disease (and bulky IB disease) in whom, in 1 study, chemoradiation, compared to radiation alone, improved 5-year survival rates from 58% to 77%. For patients with more advanced disease, there is still significant benefit, but it appears to be less pronounced. The optimal drug regimen is not known. Many experts recommend weekly cisplatin concomitantly with radiation. A recent study suggested the superiority of weekly combination cisplatin/gemcitabine during chemoradiation. However, the experimental group also received 2 additional cycles of adjuvant cisplatin/gemcitabine after brachytherapy and toxicity was significant. It is unclear what proportion of the improvement in outcome can be attributed to the multiagent chemoradiotherapy versus the adjuvant chemotherapy. This question is currently being investigated by the Gynecologic Cancer Intergroup.
C. Treatment of Disseminated Primary (Stage IVB) & Persistent or Recurrent Disease
The use of chemotherapeutic agents in the treatment of cervical carcinoma has been discouraging. This is partly because most patients who may be candidates for this type of treatment either present with disseminated disease or have cancer that has already failed to respond to radical surgery or radiation therapy. In this setting, chemotherapy is generally palliative and not curative. Modest activity in recurrent or disseminated cervical cancer has been observed with single-agent cisplatin, ifosfamide, paclitaxel, and vinorelbine. If the patient can tolerate it, multiagent chemotherapy is preferred as it is associated with significantly higher response rates and longer progression-free survival. There is also a small overall survival advantage to multiagent chemotherapy with cisplatin and topotecan. Combination therapy using paclitaxel and platinum offers very similar outcomes, with response rate and median survival time of 36% and 9.7 months, compared to 27% and 9.6 months, respectively, for cisplatin and topotecan. Other acceptable combination regimens include cisplatin/vinorelbine and cisplatin/gemcitabine. Surgical resection of lung metastases is an alternative to palliative chemotherapy for highly selected patients with isolated, potentially resectable pulmonary metastases. Palliative radiation therapy may be indicated, especially for the control of symptoms, such as pain or hemorrhage. If a patient develops a palpable mass in the left supraclavicular region, it can be palliated with radiation therapy with concomitant chemotherapy, with or without resection.
D. Total Pelvic Exenteration for Isolated Central Pelvic Recurrence of Disease
Patients who develop a central recurrence of cervical cancer after primary therapy with radiation or after surgery followed by radiation may be candidates for this extensive, potentially curative surgical procedure if a complete evaluation fails to reveal evidence of metastatic disease. In a small proportion of patients with cancer of the cervix treated initially with radiation, a small recurrence of the cancer may be noted centrally within the cervix. A radical hysterectomy may be an alternative to total pelvic exenteration in this selected subgroup of patients. Surgery is the only potentially curative method of treating cancers that persist or recur centrally following adequate radiation therapy. In such instances, pelvic exenteration is often necessary to make certain that all of the cancer has been removed.
Pelvic exenteration is one of the most formidable of all gynecologic operations and requires removal of the bladder, rectum, and vagina, along with the uterus if hysterectomy has not yet been performed. This is followed by the reconstructive phase of the procedure. Urinary diversion needs to be provided, necessitating the creation of either a continent ileocolonic pouch or a noncontinent ileal conduit. In either case, a stoma is created in the anterior abdominal wall. If extensive rectal resection was required, a sigmoid colostomy serves for the passage of feces. If a low rectal anastomosis could be accomplished, a temporary diverting colostomy is recommended for all patients who have received prior radiation. The vagina can be reconstructed using various myocutaneous flaps, such as vertical rectus abdominis or gracilis myocutaneous flaps. Depending on the location of the lesion, an anterior (preservation of the rectosigmoid) or posterior (preservation of the bladder) exenteration is at times an alternative.
Because of the high surgical morbidity and mortality rates, stringent criteria are necessary to justify these procedures. Pelvic exenteration should be reserved primarily for problems that cannot be effectively managed in any other manner. In essence, this means (1) a biopsy-proven persistence or recurrence of cervical cancer following an adequate course of radiation therapy or radical surgery in which the recurrent or persistent tumor occupies the central portion of the pelvis (without metastases) and is completely removable; and (2) a patient who is able to cope with the urinary and fecal stomas in the abdomen created by the operation. Both psychological and physical preparation of the patient for this operation and its aftermath are of vital importance. Because of the extreme difficulties encountered in making an accurate assessment preoperatively, only about half of the patients explored for a total pelvic exenteration will intraoperatively be confirmed to have resectable, nonmetastatic disease. Favorable prognostic factors in addition to an isolated central pelvic recurrence with no side wall fixation are a long disease-free interval and size of the recurrence < 3 cm in diameter. The 5-year survival rate following pelvic exenteration for recurrent cervical cancer averages 30–40%.
E. Palliative Care
Comprehensive care of a patient with cancer involves, in addition to antitumor therapy, good symptom relief and personal and family support. The palliative care for patients with progressive cervical cancer poses many challenges. The emphasis should be to facilitate comfort, dignity, autonomy, and personal rehabilitation and development, especially in the face of an incurable disease.
Most patients with progressive cervical cancer eventually develop symptoms related principally to the site and extent of the malignant disease. Ulceration of the cervix and adjacent vagina produces a foul-smelling discharge. Tissue necrosis and slough may initiate life-threatening hemorrhage. If the bladder or rectum is involved in the tissue breakdown, fistulas result in incontinence of urine and feces. Pain caused by involvement of the lumbosacral plexus, soft tissues of the pelvis, or bone is frequently encountered in advanced disease. Ureteral compression leading to hydronephrosis and, if bilateral, to renal failure and uremia is a common terminal event. The comfort and well-being of the patient can be considerably enhanced even though cure cannot be effected. A foul, purulent discharge may be ameliorated by astringent douches and antimicrobial vaginal creams or suppositories. Hemorrhage from the vagina often can be controlled by packing the area with gauze impregnated with a hemostatic agent; occasionally, emergent radiation or hypogastric artery embolization is indicated.
Current management of severe pain combines the use of a long-acting narcotic such as morphine or a transdermal fentanyl patch with short-acting narcotics for breakthrough pain and nonsteroidal anti-inflammatory agents. Anxiolytics and antidepressants may be of considerable value. For patients with significant pain who are no longer responding to oral medications, a subcutaneous or intravenous morphine drip can be started. In patients with lower back or extremity pain, a peridural catheter can be placed and connected to a subcutaneous pump with a reservoir for continuous morphine instillation. This method gives pain relief without the sedating effects of oral and parenteral narcotics.
Radiation therapy may be very helpful in the relief of pain caused by bony metastases and in the treatment of lesions that recur following primary surgical treatment of cervical cancer. In general, if initial therapy was accomplished by adequate radiation therapy, retreatment is contraindicated because it does little good and carries the potential of massive radiation necrosis.
Special Situations
A. Stage IA1 Disease
The definitive diagnosis of microinvasive carcinoma of the cervix can only be made by conization. These patients may be treated by simple abdominal or vaginal hysterectomy. For a young woman desiring to maintain fertility, conization only is an acceptable treatment modality for microinvasive carcinoma with a depth of invasion of 3 mm or less, if the conization margins are negative, and if there is no evidence of lymphovascular space invasion. If conization margin and endocervical sampling are positive, the risk of residual disease is as high as 33%. In this case, repeat conization should be performed if uterine preservation is the goal. FIGO staging is not influenced by the presence of lymphovascular space invasion, which occurs in close to 10% of patients with stage IA1 disease. These patients have a small but significant risk for lymph node metastases to parametrial and pelvic lymph nodes. This subgroup of patients should therefore be treated like patients with stage IA2 disease.
B. Radical Trachelectomy
Over the past 2 decades, radical trachelectomy has evolved as an alternative to radical hysterectomy in carefully selected young women with early-stage (IA2 or small IB1) cervical cancer and no evidence of lymph node metastases who wish to preserve fertility. A preoperative MRI is critical for treatment planning as it allows for measurement of the distance between the upper margin of the lesion and the isthmus. The radical trachelectomy can be performed transvaginally or abdominally via open or robotic approach; ideally the cervix is amputated 1 cm above the tumor to optimize oncologic outcome and 1 cm below the isthmus to maintain some cervical function for future pregnancies. An open or minimally invasive therapeutic lymphadenectomy is performed, and following radical resection of the cervix, a cerclage is placed. Experience with this technique is growing, and the oncologic outcome, with recurrence rates <5% and mortality rates of 2–3%, is comparable in carefully selected patients to radical hysterectomy. A review of pregnancy outcomes in women who underwent radical trachelectomy revealed that 40% of women conceived following radical trachelectomy. Of those women who do conceive, 16–20% have a first-trimester abortion, close to 10% have a second-trimester pregnancy loss, 25% have a preterm delivery, and 42% deliver a live born infant at term. The majority of successful pregnancy outcomes have occurred with a cerclage in place.
C. Bulky Cervical Cancer
The management of patients with stage IB2 and bulky IIA2 disease is a matter of considerable debate. Proposed management strategies include the following.
1. Primary radiation therapy with concomitant chemotherapy & the option of a subsequent adjuvant extrafascial hysterectomy—Radiation therapy is usually recommended for patients with bulky cervical cancers with the addition of concomitant chemotherapy. Many of these tumors, however, contain hypoxic central areas that do not respond well to radiation, as is reflected in a 15–35% pelvic failure rate. This provides the rationale for the performance of an adjuvant hysterectomy following radiation, which is associated with a significant reduction in pelvic recurrences to 2–5%. However, the impact of adjuvant hysterectomy on extrapelvic recurrences and survival is less well established.
2. Primary radical hysterectomy & therapeutic lymphadenectomy, followed by tailored radiation with concomitant chemotherapy when indicated by pathologic findings—The potential benefits of this approach include the removal of the large primary tumor, complete surgical staging with the opportunity to resect any grossly involved lymph nodes, and the preservation of ovarian function as ovarian transposition can be performed if adjuvant radiation therapy is likely. If postoperative radiation becomes necessary, the radiation field can be tailored to the surgicopathologic findings. The resection of macroscopically involved lymph nodes has a therapeutic benefit because it improves survival to that of patients with microscopic lymph node metastases only. A primary surgical approach should be taken in patients with acute or chronic pelvic inflammatory disease, an undiagnosed coexistent adnexal mass, or anatomic alterations that make radiation therapy difficult.
3. Neoadjuvant chemotherapy followed by radical hysterectomy and lymphadenectomy & subsequent chemoradiation when indicated by pathologic findings—Neoadjuvant chemotherapy, frequently 3 cycles of platinum-based combination therapy followed by radical hysterectomy and lymphadenectomy, has been proposed as a treatment strategy for these patients. Neoadjuvant chemotherapy is reported to improve the resectability of bulky lesions, pelvic disease control, and possibly long-term survival. Although this is a provocative treatment strategy, in most studies, patients ultimately received multimodality treatment with chemotherapy, radical surgery, and radiation, and it remains unclear whether the use of neoadjuvant chemotherapy followed by surgery gives superior long-term results in the era of modern chemoradiotherapy. This question is currently being studied in phase III trials by the European Organization for the Research and Treatment of Cancer.
D. Carcinoma of the Cervix during Pregnancy
Invasive carcinoma of the cervix in pregnancy is found more frequently in areas where routine prenatal cytologic examination is done. Abnormal cervical cytology in pregnancy calls for immediate colposcopic evaluation and any other diagnostic modalities necessary to exclude invasive cancer (see section on preinvasive disease).
Invasive cervical cancer complicates approximately 0.05% of pregnancies. As is the case with nonpregnant patients, the principal symptom is bleeding, but the diagnosis is frequently missed because the bleeding is assumed to be related to the pregnancy rather than to cancer. The possibility of cancer must be kept in mind. The diagnosis and management of invasive cervical cancer during pregnancy present the patient and the physician with many challenges. Pregnancy does not appear to affect the prognosis for women with cervical cancer, and the fetus is not affected by the maternal disease, but may suffer morbidity from its treatment (eg, preterm delivery).
If the pregnancy is early and the disease is stage I to IIA, radical hysterectomy and therapeutic lymphadenectomy can be performed with the fetus left in situ, unless the patient is unwilling to terminate the pregnancy. Women at a gestational age closer to fetal viability or who are unwilling to lose the baby may decide to continue the pregnancy after careful discussion regarding the maternal risks. With early-stage disease (≤stage IB1/IIA1), the literature supports expectant management with careful serial examinations to exclude disease progression as a reasonable choice. With more advanced disease (≥ stage IB2/IIA2), neoadjuvant chemotherapy may offer an opportunity to delay definitive therapy until fetal maturity while reducing maternal risks potentially associated with treatment delay. Delivery in patients with cervical dysplasia and CIS may be via the vaginal route. Patients with invasive cervical cancer should be delivered by caesarean section to avoid potential cervical hemorrhage and dissemination of tumor cells during vaginal delivery. A caesarean radical hysterectomy with therapeutic lymphadenectomy is the procedure of choice for patients with stages IA2–IIA disease as soon as fetal maturity is established.
As in the nonpregnant patient, radiation with concomitant chemotherapy is used for the treatment of more advanced disease. Irradiation may be carried out with the expectation of spontaneous abortion. In selected cases with locally advanced disease in which the patient declines pregnancy termination, consideration may be given to neoadjuvant chemotherapy in an effort to prevent disease progression during the time needed to achieve fetal maturity. Delivery should be by caesarean section. A lymphadenectomy can be performed at the same time. Postpartum the patient should receive chemoradiation following guidelines established for the nonpregnant patient.
E. Carcinoma of the Cervical Stump
About 2% of all cervical cancers occur in the cervical stump. Early-stage cervical cancer noted on a cervical stump (left in situ following supracervical hysterectomy for an unrelated indication) should be treated with radical trachelectomy and therapeutic lymphadenectomy in the medically fit patient. Surgery is preferred over chemoradiation in this setting as the delivery of an adequate radiation dose may be difficult in a patient with a short cervical stump. However, radiation with concomitant chemotherapy is the preferred treatment modality for patients with more advanced disease.
F. Cervical Cancer Incidentally Diagnosed after Simple Hysterectomy
Women who are found to have microinvasive disease after a simple hysterectomy do not require any additional therapy. Patients with invasive disease who do not have gross parametrial disease are candidates for a radical parametrectomy, upper vaginectomy, and lymphadenectomy. This approach may be particularly desirable for young women in whom ovarian function can be preserved or for any surgically fit women with enlarged lymph nodes that should be resected prior to chemoradiation. Indications for chemoradiation follow the same guidelines as outlined earlier. Chemoradiation may be associated with less morbidity and comparable onco-logic outcomes.
Complications of Therapy
A. Radical Surgery
The operative mortality rate in radical hysterectomy with lymphadenectomy has been reduced to <1%. The most common complication is prolonged bladder dysfunction. Approximately 75% of patients have adequate recovery of bladder function within 1–2 weeks after radical hysterectomy, and most patients will have satisfactory voiding function by 3 weeks. Serious complications include fistula formation; ureterovaginal fistula is the most common type (1–2%), followed by vesicovaginal and rectovaginal fistulas. Modified radical hysterectomy, as compared to radical hysterectomy, is associated with a shorter operating time, a more rapid return of bladder function, and fewer fistulas. Other complications are urinary tract infections, lympho-cysts and lymphedema, wound sepsis, dehiscence, thromboembolic disease, ileus, postoperative hemorrhage, and intestinal obstruction.
The surgical mortality rate from pelvic exenteration has been reduced from approximately 25% to <5%, but as many as 50% of patients experience major morbidity. Complications include intraoperative and postoperative hemorrhage, infectious morbidity, urinary fistulas or obstruction, urinary pouch dysfunction, pyelonephritis, bowel obstruction or intestinal leaks and fistulas, stomal retraction, electrolyte disturbances, and other less common occurrences.
B. Radiation Therapy with Concomitant Chemotherapy
See Chapter 52.
Posttreatment Follow-Up
Approximately 35% of patients with invasive cervical cancer will have recurrent or persistent disease following therapy. Approximately 50% of deaths from cervical cancer occur in the first year after treatment, another 25% in the second year, and 15% in the third year. This explains the generally accepted schedule of posttreatment surveillance in asymptomatic patients with more frequent visits initially. Symptomatic patients should be evaluated with appropriate examinations immediately when symptoms occur. The most common signs and symptoms of recurrent malignant disease are a palpable tumor in the pelvis or abdomen, ulceration of the cervix or vagina, pain in the pelvis, back, groin, and lower extremity, unilateral lower extremity edema, vaginal bleeding or discharge, supraclavicular lymphadenopathy, ascites, unexplained weight loss, progressive ureteral obstruction, and cough (especially with hemoptysis or chest pain).
The Society of Gynecologic Oncologists has recently developed risk-stratified recommendations for the posttreatment follow-up of patients with cervical cancer. These are summarized in Table 48–5.
Table 48–5. Cervical cancer surveillance recommendations.
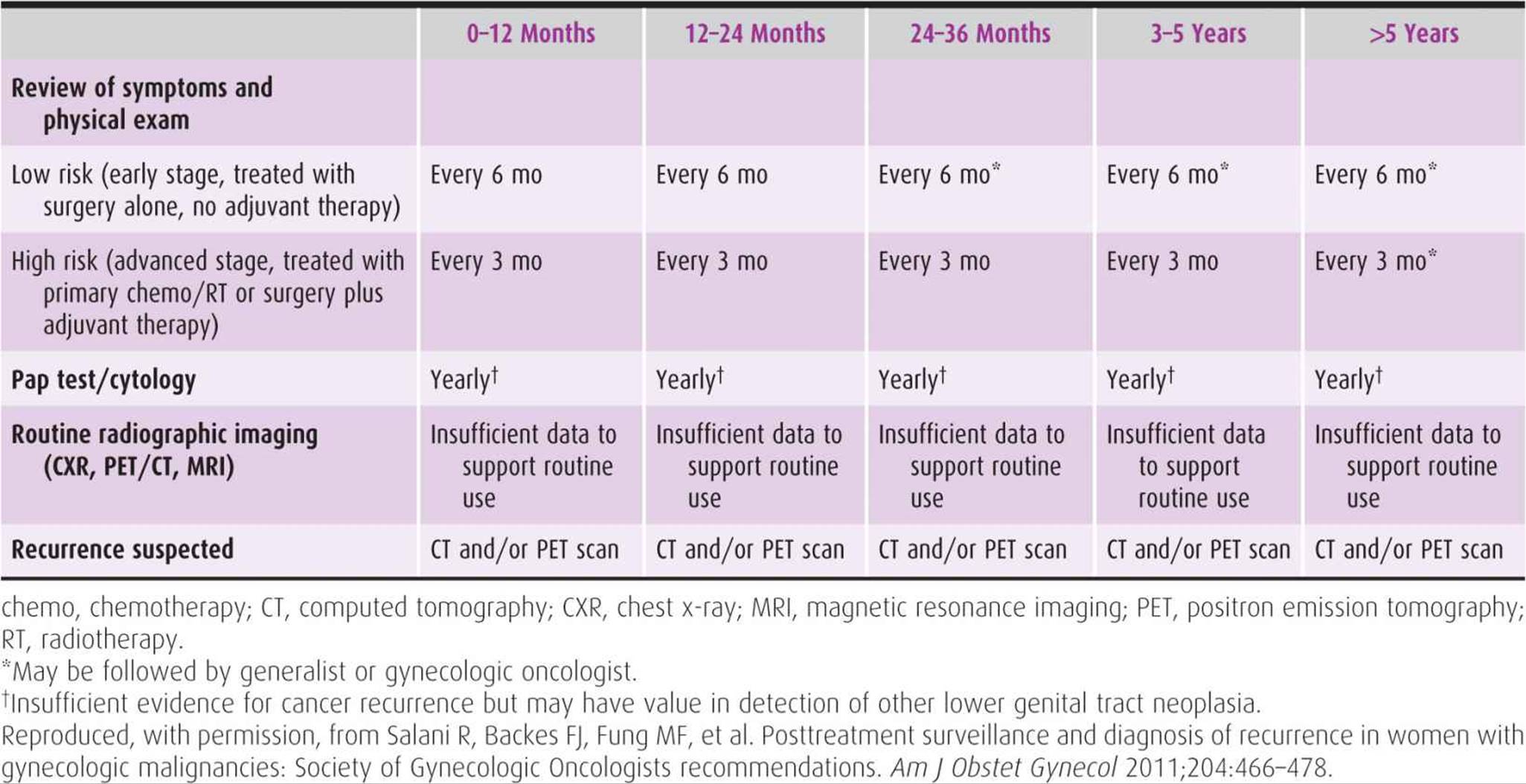
Prognosis
The major prognostic factors affecting survival are stage, lymph node status, tumor volume, depth of cervical stromal invasion, lymphovascular space invasion, and to a lesser extent, histologic type and grade. After stage of disease, lymph node status is the most important prognostic factor. For example, following radical surgery, patients with stage IB or IIA disease have a 5-year survival of 88–96% with negative lymph nodes, compared to 64–73% in the presence of lymph node metastases.
Table 48–6 summarizes survival rates by stage of disease. These are based on the FIGO Annual Report on the Results of Treatment in Gynecological Cancer, in which results of treatment for each stage of cervical cancer are reported by more than 100 participating institutions worldwide. The results are equated in terms of 5-year cure rates, or those patients who are living and show no evidence of cervical cancer 5 years after beginning therapy. Recurrences following radiation therapy are not often centrally located and thus amenable to exenteration procedures. Only approximately 25% of recurrences are localized to the central portion of the pelvis. The most common site of recurrence is the pelvic side wall.
Table 48–6. Survival of patients with cervical cancer based on International Federation of Gynecology and Obstetrics (FIGO) stage.
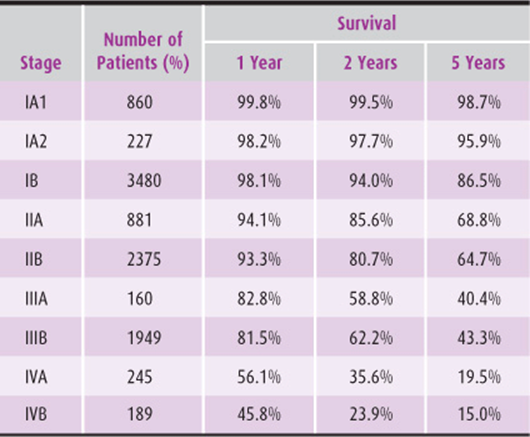
American Cancer Society. Cancer Facts and Figures 2011. Available at: http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/cancer-facts-figures-2011. Accessed September 10, 2011.
Anderson B, LaPolla J, Turner D, et al. Ovarian transposition in cervical cancer. Gynecol Oncol 1993;49:206–214. PMID: 8504989.
Ault KA. Vaccines for the prevention of human papillomavirus and associated gynecologic diseases: a review. Obstet Gynecol Surv 2006;61(6 Suppl 1):S26–S31. PMID: 16729901.
Averette HE, Nguyen HN, Donato DM, et al. Radical hysterectomy for invasive cervical cancer: a 25-year prospective experience with the Miami technique. Cancer 1993;71:1422–1437. PMID: 8431876.
Benedet JL, Bender H, Jones H 3rd, et al. FIGO staging classifications and clinical practice guidelines in the management of gynecologic cancers. FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet2000;70:209–216. PMID: 11041682.
Benedet JL, Odicino F, Maisonneuve P, et al. FIGO annual report: carcinoma of the cervix uteri. Int J Gynaecol Obstet 2003; 83(Suppl 1):41–47. PMID: 14763169.
Chemoradiotherapy for Cervical Cancer Meta-analysis Collaboration (CCCMAC). Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: individual patient data meta-analysis. Cochrane Database Syst Rev 2010;1:CD008285. PMID: 20091664.
Cosin JA, Fowler JM, Chen MD, et al. Pretreatment surgical staging of patients with cervical carcinoma: the case for lymph node debulking. Cancer 1998;82:2241–2248. PMID: 9610715.
Dargent D, Martin X, Sacchetoni A, et al. Laparoscopic vaginal radical trachelectomy: a treatment to preserve the fertility of cervical carcinoma patients. Cancer 2000;88:1877–1882. PMID: 107607665.
Dueñas-González A, Zarbá JJ, Patel F, et al. Phase III, open-label, randomized study comparing concurrent gemcitabine plus cisplatin and radiation followed by adjuvant gemcitabine and cisplatin versus concurrent cisplatin and radiation in patients with stage IIB to IVA carcinoma of the cervix. J Clin Oncol 2011;29:1678–1685. PMID: 21444871.
Eifel PJ, Thoms WW Jr, Smith TL, et al. The relationship between brachytherapy dose and outcome in patients with bulky endocervical tumors treated with radiation alone. Int J Radiat Oncol Biol Phys1994;28:113–118. PMID: 8270431.
Feeney DD, Moore DH, Look KY, et al. The fate of the ovaries after radical hysterectomy and ovarian transposition. Gynecol Oncol 1995;56:3–7. PMID: 7821844.
FIGO Committee on Gynecologic Oncology. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynecol Obstet 2009;105:103–104. PMID: 19367689.
Gallion HH, van Nagell JR Jr, Donaldson ES, et al. Combined radiation therapy and extrafascial hysterectomy in the treatment of stage IB barrel-shaped cervical cancer. Cancer 1985; 56:262–265. PMID: 4005798.
Hacker NF, Wain GV, Nicklin JL. Resection of bulky positive lymph nodes in patients with cervical carcinoma. Int J Gynaecol Cancer 1995;5:250–256. PMID: 11578485.
Hellström AC, Hellman K, Pettersson BF, et al. Carcinoma of the cervical stump: fifty years of experience. Oncol Rep 2011; 25:1651–1654. PMID: 21431283.
Hopkins MP, Lavin JP. Cervical cancer in pregnancy. Gynecol Oncol 1996;63:293. PMID: 8946860.
Hricak H, Gatsonis C, Chi DS, et al. Role of imaging in pretreatment evaluation of early invasive cervical cancer: results of the intergroup study American College of Radiology Imaging Network 6651-Gynecologic Oncology Group 183. J Clin Oncol 2005;23:9329–9337. PMID: 16361632.
Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011;61:69–90. PMID: 21296855.
Jolley JA, Battista L, Wing DA. Management of pregnancy after radical trachelectomy: case reports and systematic review of the literature. Am J Perinatol 2007;24:531–539. PMID: 17899494.
Keys HM, Bundy BN, Stehman FB, et al. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N Engl J Med1999;340:1154–1161. PMID: 10202166.
Landoni F, Maneo A, Cormio G, et al. Class II versus class III radical hysterectomy in stage IB–IIA cervical cancer: a prospective randomized study. Gynecol Oncol 2001;80:3–12. PMID: 11136561.
Landoni F, Maneo A, Colombo A, et al. Randomised study of radical surgery versus radiotherapy for stage IB–IIA cervical cancer. Lancet 1997;350:535–540. PMID: 9284774.
Lazo PA. The molecular genetics of cervical carcinoma. Br J Cancer 1999;80:2008–2018. PMID: 10471054.
Lee YN, Wang KL, Lin MH, et al. Radical hysterectomy with pelvic lymph node dissection for treatment of cervical cancer: a clinical review of 954 cases. Gynecol Oncol 1989;32:135–142. PMID: 2910773.
Long HJ 3rd, Bundy BN, Grendys EC Jr, et al. Randomized phase III trial of cisplatin with or without topotecan in carcinoma of the uterine cervix: a Gynecologic Oncology Group study. J Clin Oncol2005;23:4626–4631. PMID: 15911865.
Metcalf KS, Johnson N, Calvert S, Peel KR. Site specific lymph node metastasis in carcinoma of the cervix: is there a sentinel node? Int J Gynecol Cancer 2000;10:411–414. PMID: 11240707.
Monk BJ, Sill MW, McMeekin DS, et al. Phase III trial of four cisplatin-containing doublet combinations in stage IVB, recurrent, or persistent cervical carcinoma: a Gynecologic Oncology Group study. J Clin Oncol2009;27:4649–4655. PMID: 17920909.
Moore DH, Blessing JA, McQuellon RP, et al. Phase III study of cisplatin with or without paclitaxel in stage IVB, recurrent, or persistent squamous cell carcinoma of the cervix: a Gynecologic Oncology Group study. J Clin Oncol 2004;22:3113–3119. PMID: 15284282.
Morris M, Eifel PJ, Lu J, et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N Engl J Med 1999;340:1137–1143. PMID: 10202164.
Omura GA. Chemotherapy for stage IVB or recurrent cancer of the uterine cervix. J Natl Cancer Inst Monogr 1996;21:123–126. PMID: 9023841.
Omura GA, Blessing JA, Vaccarello L, et al. Randomized trial of cisplatin versus cisplatin plus mitolactol versus cisplatin plus ifosfamide in advanced squamous carcinoma of the cervix: a Gynecologic Oncology Group study. J Clin Oncol 1997;15: 165–171. PMID: 8991638.
Parkin DM, Pisani P, Ferlay J. Global cancer statistics. CA Cancer J Clin 1999;49:33–64. PMID: 10200776.
Perez CA, Grigsby PW, Camel HM, et al. Irradiation alone or combined with surgery in stage IB, IIA, and IIB carcinoma of uterine cervix: update of a nonrandomized comparison. Int J Radiat Oncol Biol Phys1995;31:703–716. PMID: 7860381.
Peters WA III, Liu PY, Barrett RJ 2nd, et al. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J Clin Oncol 2000;18: 1606–1613. PMID: 10764420.
Piver MS, Rutledge F, Smith JP. Five classes of extended hysterectomy for women with cervical cancer. Obstet Gynecol 1974;44:265–272. PMID: 4417035.
Plante M, Renaud MC, François H, et al. Vaginal radical trachelectomy: An oncologically safe fertility-preserving surgery. An updated series of 72 cases and review of the literature. Gynecol Oncol2004;94:614–623. PMID: 15350349.
Plante M, Renaud MC, Hoskins IA, et al. Vaginal radical trachelectomy: a valuable fertility-preserving option in the management of early-stage cervical cancer. A series of 50 pregnancies and review of the literature. Gynecol Oncol 2005;98:3–10. PMID: 15936061.
Roman LD, Felix JC, Muderspach LI, et al. Risk of residual invasive disease in women with microinvasive squamous cancer in a conization specimen. Obstet Gynecol 1997;90:759–764. PMID: 9351760.
Rose PG, Bundy BN, Watkins EB, et al. Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. N Engl J Med 1999;340:1144–1153. PMID: 10202165.
Rotman M, Sedlis A, Piedmonte MR, et al. A phase III randomized trial of postoperative pelvic irradiation in stage IB cervical carcinoma with poor prognostic features: follow-up of a gynecologic oncology group study. Int J Radiat Oncol Biol Phys 2006;65:169–174. PMID: 16427212.
Salani R, Backes FJ, Fung MF, et al. Posttreatment surveillance and diagnosis of recurrence in women with gynecologic malignancies: Society of Gynecologic Oncologists recommendations. Am J Obstet Gynecol2011;204:466–478. PMID: 21752752.
Sardi JE, Giaroli A, Sananes C, et al. Long-term follow-up of the first randomized trial using neoadjuvant chemotherapy in stage IB squamous carcinoma of the cervix: the final results. Gynecol Oncol1997;67:61–69. PMID: 9345358.
Sasieni PD, Cuzick J, Lynch-Farmery E. Estimating the efficacy of screening by auditing smear histories of women with and without cervical cancer. The National Coordinating Network for Cervical Screening Working Group. Br J Cancer 1996;73: 1001–1005. PMID: 8611418.
Sedlis A, Bundy BN, Rotman MZ, et al. A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: a Gynecologic Oncology Group study. Gynecol Oncol 1999;73:177–183. PMID: 10329031.
Sood AK, Sorosky JI, Mayr N, et al. Cervical cancer diagnosed shortly after pregnancy: prognostic variables and delivery routes. Obstet Gynecol 2000;95:832–838. PMID: 10831976.
Sutton GP, Bundy BN, Delgado G, et al. Ovarian metastases in stage IB carcinoma of the cervix: a Gynecologic Oncology Group study. Am J Obstet Gynecol 1992;166:50–53. PMID: 1733218.
Tewari K, Cappuccini F, Gambino A, et al. Neoadjuvant chemotherapy in the treatment of locally advanced cervical carcinoma in pregnancy: a report of two cases and review of issues specific to the management of cervical carcinoma in pregnancy including planned delay of therapy. Cancer 1998;82:1529–1543. PMID: 9554531.
Vizcaino AP, Moreno V, Bosch FX, et al. International trends in the incidence of cervical cancer: I. Adenocarcinoma and adenosquamous cell carcinomas. Int J Cancer 1998;75:536–545. PMID: 9466653.
Walboomers JM, Jacobs MV, Manos MM, et al. Human papilloma-virus is a necessary cause of invasive cervical cancer worldwide. J Pathol 1999;189:12–19. PMID: 10451482.
Whitney CW, Sause W, Bundy BN, et al. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stage IIB–IVA carcinoma of the cervix with negative para-aortic lymph nodes: a Gynecologic Oncology Group and Southwest Oncology Group study. J Clin Oncol 1999;17:1339–1348. PMID: 10334517.
Wright JD, NathavithArana R, Lewin SN, et al. Fertility-conserving surgery for young women with stage IA1 cervical cancer: safety and access. Obstet Gynecol 2010;115:585–590. PMID: 20177290.