Elisabeth L. Raab, MD, MPH
Lisa K. Kelly, MD
A full-term newborn is a baby born at 37 weeks’ or more gestation. Term newborns are evaluated in the delivery room immediately after birth to assure that they do not require respiratory or circulatory support, have no birth-related trauma or congenital anomalies requiring immediate intervention, and are transitioning as expected to extrauterine life. Approximately 97% of newborns are healthy and require only routine care in the nursery after birth. In the nursery, newborns receive a thorough evaluation to determine maturity, evaluate growth and development, and identify those with signs of acute illness or underlying congenital disease.
DELIVERY ROOM MANAGEMENT
At every delivery there should be at least 1 person whose primary responsibility is attending to the newborn. Although approximately 90% of the time no resuscitation will be required, the attendant must be able to recognize signs of distress in a newborn and carry out a skilled resuscitation.
After the umbilical cord is cut, newborns should be placed in a warm environment. They may be placed on the mother’s chest, skin-to-skin, or they may be brought to a radiant warmer. Early skin-to-skin contact increases the likelihood and duration of breastfeeding, decreases infant crying, and facilitates bonding and is therefore encouraged when possible. However, it should only be done when the newborn is crying/breathing and has good tone and when there are no risk factors that increase the likelihood that resuscitation will be required (eg, prematurity). The infant is dried with prewarmed towels to prevent heat loss and the airway is positioned and cleared to ensure patency. The airway may be cleared by suctioning the mouth and nares with a bulb syringe or a suction catheter connected to mechanical suction. If the newborn is well-appearing and not at increased risk, the airway can be cleared simply by wiping the mouth and nose with a towel.
During this initial postpartum period, the newborn’s respiratory effort, heart rate, color, and activity are evaluated to determine the need for intervention. If drying and suctioning do not provide adequate stimulus, it is appropriate to flick the soles or rub the back to stimulate breathing. It is important to note the presence of meconium in the amniotic fluid or on the newborn’s skin. Although not contraindicated, it is no longer recommended that the obstetrician routinely suction the oropharynx of an infant born with meconium-stained amniotic fluid upon delivery of the head. If a newborn is in distress or has depressed respiratory effort after delivery and there is evidence that meconium was passed in utero, it is appropriate to intubate and suction the trachea before stimulating the baby in any way. Meconium can block the airway, preventing the newborn lungs from filling with oxygen, a vital step in normal transitioning. However, if the attempted intubation is prolonged or repeatedly unsuccessful, it may be appropriate to omit tracheal suctioning in favor of initiating positive pressure ventilation (PPV) in a depressed infant. Tracheal suctioning has not been shown to decrease the incidence of meconium aspiration syndrome or mortality rates in depressed infants born through meconium-stained fluid. An active, crying, well-appearing newborn does not require endotracheal intubation, regardless of the presence of meconium staining or the thickness of the meconium.
If a newborn remains apneic despite drying, suctioning, and stimulation, or if there are signs of distress such as grunting, central cyanosis, or bradycardia, resuscitation should quickly be initiated. PPV should be initiated in response to gasping, apnea and/or a heart rate below 100 beats/min and the decision to initiate PPV should ideally be made within the first 30–60 seconds after birth.
The Assignment of Apgar Scores
The Apgar score was introduced by Virginia Apgar in 1952 to quantitatively evaluate the newborn’s condition after birth (Table 9–1). Scores between 0 and 2 in each of 5 different categories are assigned at 1 and 5 minutes of life. The score reflects the cardiorespiratory and neurologic status at those time points. If the score is <7 at 5 minutes, scores should be assigned every 5 minutes until the baby has a score of 7 or greater or has reached 20 minutes of life. The Apgar score is not what determines the need for resuscitation. Although scores are based on the same elements used to evaluate the newborn’s status, the assessment of the need for intervention with PPV should ideally already have been made by the time the 1-minute Apgar score is assigned. Studies do not show a correlation between a low 1-minute Apgar score and outcome. However, the change between the scores at 1 and 5 minutes is a meaningful measure of the effectiveness of the resuscitation efforts, and a 5-minute score of 0–3 is associated with increased mortality in both preterm and full-term infants. It is important to know that factors such as prematurity, maternal medications, and congenital disease can adversely affect scores.
Table 9–1. Apgar scoring.

The Importance of the Prenatal & Intrapartum History
Knowledge of the prenatal and intrapartum history is essential for adequate care of the newborn. The history should be reviewed before delivery (if possible), as it may alter care in the immediate postpartum period. For example, information about the use of certain anesthetic drugs during labor and delivery alerts those attending the delivery to the possibility of newborn respiratory depression and allows them to anticipate a role for the use of naloxone in the resuscitation. Other important pieces of information are the presence of chronic disease in the mother (eg, diabetes mellitus, Grave’s disease, or systemic lupus erythematosus), maternal illicit or prescription drug use, prenatal ultrasound findings, maternal screening laboratory test results, and the presence of risk factors for neonatal infection. All of these will affect how the newborn is monitored during the nursery admission and in the first few weeks of life, and adequate care is not possible without them.
A. The Initial Exam
Although a complete and detailed physical exam is delayed until the newborn is admitted to the nursery and has had time to transition to extrauterine life, a brief examination should be done shortly after delivery to rule out any problems that require immediate attention.
1. Airway—The airway should be evaluated for patency. A suction catheter may be passed through each naris if needed to remove secretions from the nasopharynx or if there is concern about the possibility of choanal atresia, but is not necessary if adequate clearance of secretions is achieved with a bulb syringe and the newborn is breathing comfortably. Although a suction catheter is an effective means of removing secretions, it should be used cautiously because it can induce bradycardia and cause trauma and edema to the mucous membranes.
2. Chest—The chest should be examined to determine the adequacy of the respiratory effort. One should assess chest wall movement, respiratory rate, and breathing pattern and look for signs of distress, such as retractions. Crackles are often audible initially, but should clear over time as fetal lung fluid is resorbed and the lungs inflate with air. Decreased or asymmetric breath sounds may result from pneumonia, atelectasis, a pneumothorax, mass, or effusion. Heart rate and rhythm should be evaluated, and the presence or absence of a murmur noted. The heart rate should be >100 beats/min.
3. Abdomen—The abdomen should be soft and nondistended. A distended, firm abdomen may indicate a bowel obstruction, pneumoperitoneum, or intraabdominal mass. A scaphoid abdomen, when accompanied by respiratory distress, should raise the examiner’s suspicion of a diaphragmatic hernia. The umbilical stump should be examined and the number of blood vessels noted. A single umbilical artery may be a clue to the presence of other anomalies, renal anomalies in particular.
4. Skin—The skin color should be evaluated. Although acrocyanosis, bluish discoloration of the hands and feet, may be seen in well newborns, central cyanosis of the trunk may be a sign that the newborn is not receiving sufficient oxygen. Cyanosis and pallor can result from a wide variety of causes such as sepsis, anemia, respiratory insufficiency with or without abnormally elevated cardiac vascular resistance, congenital heart disease, and hypoxic-ischemic injury with cardiac dysfunction; the pre- and intrapartum history is often useful in determining the etiology. Pulse oximetry is useful to help determine the oxygen saturation in the event of cyanosis. A cyanotic infant with a normal heart rate and respiratory effort may be given free-flow 100% oxygen by face mask or tubing held close to the nose and should be observed for improvement in skin coloring. If the skin does not become pink, the patient may require PPV to achieve improved oxygenation.
5. Genitalia—It is important to closely evaluate the genitalia before pronouncing the sex of the newborn. If there is ambiguity of the genitalia, the situation must be explained to the parents, and a full evaluation, including karyotyping and consultation with a pediatric endocrinologist and urologist, should be done before gender assignment.
5. General—Alertness, activity, tone, and movement of the extremities should be noted. The face and extremities should be evaluated for evidence of congenital anomalies or birth trauma. The most common birth-related injuries are nerve injuries (facial and brachial nerve palsies) and fractures (primarily clavicular). Unilateral peripheral facial nerve palsy should be suspected when the newborn has normal movement of the forehead, but difficulty closing the eye and flattening of the nasolabial folds on the affected side and an asymmetric facial expression with crying (the unaffected side will go down). Peripheral facial nerve injury is thought to result from compression of the nerve against the maternal sacrum during delivery and is not associated with the use of forceps in delivery. The risk of brachial plexus injury is increased when there is shoulder dystocia or the baby is large for gestational age (LGA). Erb’s palsy (C5–C6 injury) manifests as an inability to externally rotate or abduct the shoulder; the affected arm is held adducted and internally rotated and is extended and pronated at the elbow (“waiter-tip” position). If the C5–T1 nerve roots are all affected, the function of the hand will be affected as well.
Casey BM, McIntire DD, Leveno KJ. The continuing value of the Apgar score for the assessment of newborn infants. N Engl J Med 2001;344:467. PMID: 11172187.
Dawson JA, Kamlin COF, Vento M, et al. Defining the reference range for oxygen saturation for infants after birth. Pediatrics 2010;125;e1340–e1347. PMID: 20439604.
Ehrenstein V. Association of Apgar scores with death and neurologic disability. Clin Epidemiol 2009;1:45–53. PMID: 20865086.
Roggensack A, Jefferies AL, Farine D, et al. Management of meconium at birth. J Obstet Gynaecol Can 2009;31:353–354. PMID: 19497156.
Weiner GM, Wyckoff M, Zaichkin J. 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2010;122 (18 Suppl 3):S909–S919. PMID: 20956231.
CARE & OBSERVATION IN THE FIRST FEW HOURS OF LIFE
A single 1-mg intramuscular injection of vitamin K is recommended for all newborns to prevent bleeding as a result of vitamin K deficiency. Vitamin K prophylaxis has been standard of care since 1961, when it was first recommended by the American Academy of Pediatrics (AAP). Standard newborn care also includes applying either 0.5% erythromycin ointment, 1% silver nitrate solution, or 1% tetracycline ointment to the infant’s eyes shortly after birth to prevent infectious neonatal conjunctivitis.
The well newborn may remain with the mother after birth and attempt an initial feed. There should be continued intermittent assessment to assure that there is no cardiorespiratory distress, temperature instability, altered level of activity, or other signs of distress. It is important that care-givers are aware that babies that require resuscitation after birth are at increased risk of difficulties with transitioning and must be monitored closely.
American Academy of Pediatrics, Committee on Fetus and Newborn. Controversies concerning vitamin K and the newborn policy statement. Pediatrics 2003;112:191. PMID: 12837888.
NEWBORN NURSERY CARE
Vital Signs
Vital signs should be recorded by the nursing staff for all newborns admitted to the nursery. Body temperature is typically measured in the axilla. Fever, defined as a temperature ≥38.0° Celsius (or 100.4° Fahrenheit), is often caused by excessive environmental heat or overbundling when it occurs shortly after birth. Hypothermia may result if newborns are left in the delivery room unbundled and off the radiant warmer. A newborn with hypothermia or hyperthermia whose temperature fails to normalize in response to appropriate environmental measures should be evaluated for possible sepsis and central nervous system pathology.
A normal respiratory rate for a newborn is typically between 40 and 60 breaths per minute. A normal heart rate for a newborn is generally 100–160 beats/min, but varies considerably with sleep and activity level. If measured, pulse oximetry should be >95% in the term infant. However, it is important to realize that oxygen saturations may remain low for several minutes after birth. Data indicate that it takes approximately 8 minutes on average for pulse oxygen saturations to rise above 90%. Neonatal resuscitation guidelines published by the AAP in 2010 target a preductal saturation of >80% by 5 minutes of life and 85–95% by 10 minutes of life in both term and preterm infants. Blood pressure varies with gestation and birth weight. There is still debate regarding what constitutes an abnormal blood pressure in a neonate, but hypotension in the first 12–24 hours of life is typically defined as a mean blood pressure less than the gestational age. Hypertension in the full-term newborn is defined as a systolic blood pressure >90 mm Hg and diastolic blood pressure >60 mm Hg and a mean blood pressure >70 mm Hg. Blood pressures should be measured in all 4 extremities if there is any suspicion of cardiac disease. Coarctation of the aorta is characterized by elevated blood pressure in the upper extremities and decreased pressure in the lower extremities.
Growth and Development
Weight, length, and head circumference should be measured and plotted on curves to assess intrauterine growth (Fig. 9–1). Newborns that are small for gestational age (SGA), historically defined as less than the 10th percentile on the growth curve, may warrant evaluation for congenital infections, chromosomal syndromes, or other causes if there is no identifiable cause for the growth retardation, such as multiple pregnancy or preeclampsia or other evidence of placental insufficiency. Infants that are SGA or LGA should be treated similarly to the infants of diabetic mothers and should be monitored for hypoglycemia in the first few hours of life.


Figure 9–1. Classification of newborns based on gestational age plotted against head circumference, length, and weight. AGA, appropriate for gestational age; LGA, large for gestational age; SGA, small for gestational age.
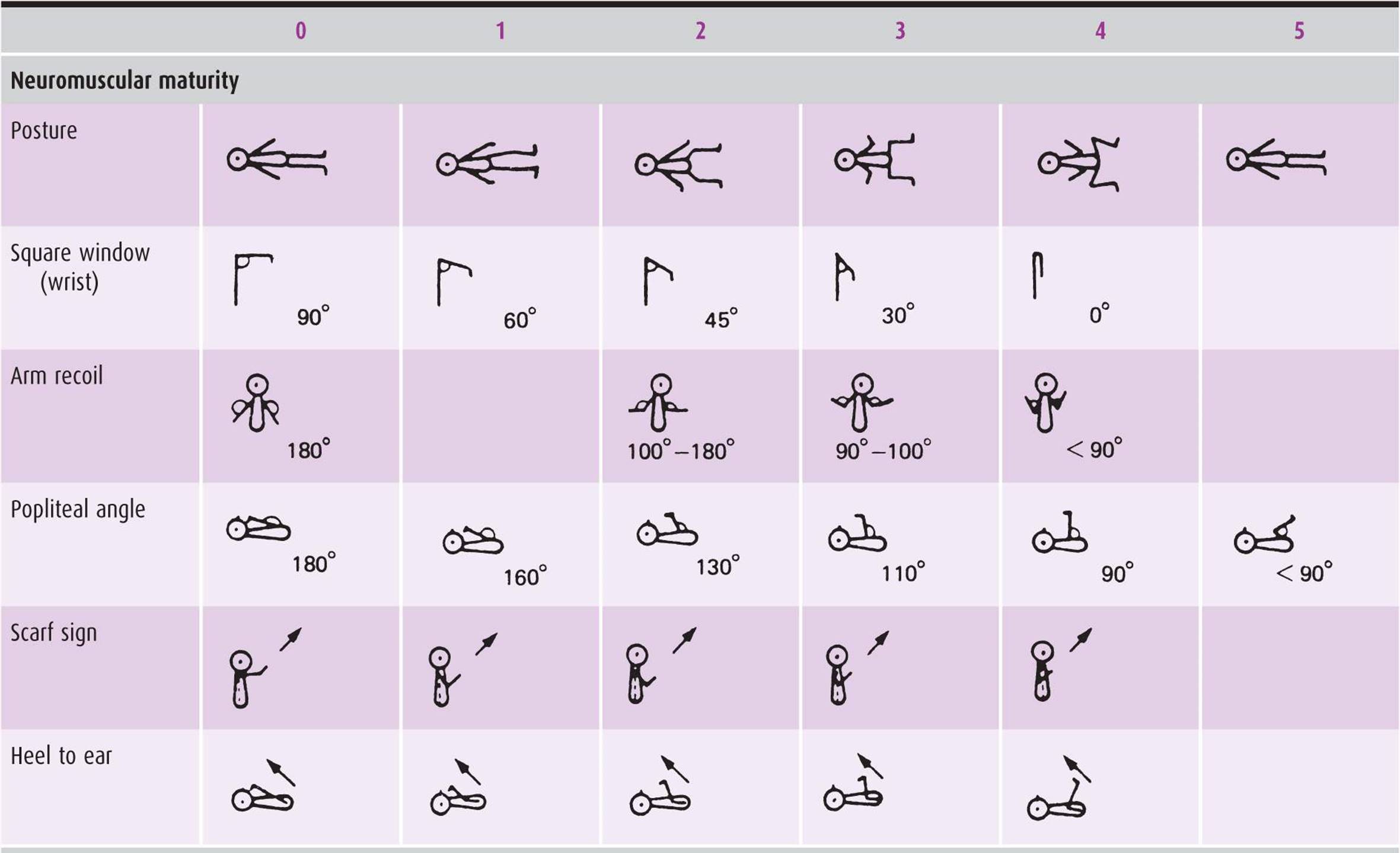
Although gestational age is usually estimated before delivery by prenatal ultrasound (preferably early on in the pregnancy) or the mother’s last menstrual period, information is sometimes unavailable or inaccurate, and maturity should be reassessed postnatally. There are measures, such as Ballard’s modified version of the Dubowitz exam (Table 9–2), that incorporate multiple elements of the physical exam and may be useful at 12–24 hours of life to help determine gestational age.
Table 9–2. Newborn maturity rating and classification.

Physical Exam
A physician should perform a complete physical exam of the newborn within the first 24 hours of life.
A. Skin
As on the initial brief examination, the color of the skin should be evaluated and the presence of cyanosis, pallor, or jaundice noted. The healthy newborn should be pink. Postterm infants often have dry, cracked skin. Clinical jaundice is rare in the first 24 hours of life and should trigger an evaluation. Plethora, often seen in infants of diabetic mothers, may indicate significant polycythemia. Practice varies, but most neonatologists consider a hematocrit >70% in an asymptomatic newborn and 65% in a symptomatic newborn grounds for a partial exchange transfusion. Symptoms of hyperviscosity include hypoxia, hypoglycemia, increased work of breathing, and seizures. Neurologic sequelae can be serious. Petechiae are often present over the face and upper torso, particularly when a nuchal cord is present. When present below the nipple line, petechiae should raise concern about the possibility of sepsis or platelet dysfunction. Bruising occurs frequently, especially with breech presentation, but should be noted because it may lead to excessive hemolysis and hyperbilirubinemia when extensive. Mongolian spots are dark purple-blue hyperpigmented areas usually over the back and buttocks that look like bruising, but are clusters of melanocytes deep within the dermis. They are present in a majority of black and Asian newborns and fade over time. Dermal sinuses, dimples, and cysts should be noted; they may indicate underlying defects or pose a risk for infection.
The most common newborn rash is erythema toxicum, which presents at 24–48 hours of life in almost half of all newborns as erythematous papular-pustular lesions that tend to spare the palms and soles. Other frequently seen benign rashes include milia, small white papules typically around the nares, and transient neonatal pustular melanosis, small vesicles or pustules present at birth that leave pigmented macules surrounded by scale when they disappear.
Hemangiomas and vascular malformations may be present at birth. Hemangiomas are benign tumors of vascular endothelium and are often not present at birth, but may be noted soon after. They eventually involute without therapy, but only after an initial period of growth, usually of 6–12 months. If present near the eyes or airways, they may require early intervention to prevent visual or airway compromise. In contrast, vascular malformations such as port-wine stains and salmon patches are always present at birth. Developmental anomalies composed of 1 or more types of vessels, they typically grow as the child grows and do not resolve spontaneously.
B. Head, Face, & Neck
The head should be evaluated for any asymmetry. The suture lines may be open or slightly overriding, but premature fusion requires intervention, as it presents a constraint to brain growth. The anterior fontanelle should be soft, not tense or bulging, when the newborn is calm. It is typically 1–4 cm in size and may be enlarged with hypothyroidism or increased intracranial pressure. The posterior fontanelle is typically <1 cm and may not be palpable.
Scalp edema (caput succedaneum) can most easily be differentiated from a cephalohematoma (a localized collection of blood under the dura mater) by noting whether or not the swelling crosses suture lines; cephalohematoma is typically confined by suture lines. A cephalohematoma should raise awareness of the possible development of hyperbilirubinemia as the collection of blood is broken down and resorbed. Skull fractures can occur, and the skull should be palpated carefully.
The face should be evaluated for dysmorphic features, malformations, and asymmetries. Micrognathia may cause significant airway compromise in the neonate and is associated with various syndromes. The palate should be palpated to ensure that it is not high-arched or clefted. A naris is patent if there is air movement through it (demonstrated by holding cotton in front of it) when the mouth and other naris are closed. Subconjunctival hemorrhages are a common finding as a result of the birth process. An absent red reflex should prompt an immediate ophthalmologic evaluation to rule out a congenital cataract, retinoblastoma, or glaucoma. Pupils should be equal and reactive. Abnormalities of the positioning or formation of the eyes, nose, or ears may suggest specific syndromes or chromosomal defects. Although preauricular tags and pits have been associated with renal malformations, there is no current evidence to suggest that their presence, when an isolated finding, is sufficient to warrant a renal ultrasound. The neck should be examined for masses, cysts, and webbing. The clavicles should be palpated for crepitus, swelling, and tenderness, which would suggest an underlying fracture. Although not usually detected until several weeks of age, torticollis may occur as a result of ischemia within, or hemorrhage into, the sternocleidomastoid muscle at birth. It manifests as a head tilt with or without a fibrous mass palpable in the muscle. Surgery is rarely necessary; the overwhelming majority of cases are managed with a home stretching regimen or physical therapy.
C. Chest
The chest should be evaluated for deformities such as widely spaced or accessory nipples and pectus excavatum. Breast buds may be present in both sexes and are normal, a product of exposure to circulating maternal hormones in utero.
The respiratory effort and rate should be evaluated, looking for signs of respiratory distress. Early on, tachypnea may be the only sign of pathologic processes as varied as pneumonia, amniotic fluid and/or meconium aspiration syndrome, sepsis, or congenital heart disease (CHD). Breath sounds are auscultated, paying attention to the quality of the breath sounds, the air entry, and any asymmetry that is present across the lung fields. Asymmetry of the breath sounds may indicate an area of consolidation from atelectasis or infection, a pneumothorax, effusion, or mass. Upper airway sounds, such as congestion or stridor, are often mistaken for abnormal breath sounds on exam. The listener can usually distinguish noises of upper airway origin from those of intrathoracic origin by listening for the presence of the sounds over the patient’s neck. Respiratory distress or an abnormal lung exam should be evaluated with a chest radiograph. In an emergency situation in which a pneumothorax is suspected, a transilluminator may be used. Transillumination is increased over the side of a pneumothorax, but it is sometimes difficult to assess accurately and should be confirmed by chest radiograph when possible before needle aspiration or chest tube placement.
A hyperdynamic precordium may indicate underlying heart disease with volume overload to one or both ventricles. The heart is auscultated to evaluate the heart rate and rhythm and characterize the heart sounds. A split-second heart sound can assure the examiner that both the aortic and pulmonary valves are present. A murmur should be described by where it is heard, what it sounds like, if it occurs in systole or diastole, and how loud it is. Murmurs are often audible in the newborn and are frequently innocent. Innocent murmurs are often attributed to a closing ductus arteriosus or foramen ovale, but the most commonly heard innocent murmur in the neonate is produced by peripheral pulmonic stenosis (PPS). PPS murmurs occur during systole and are best heard over the back or axillae.
Murmurs may or may not be present in newborns with CHD. Ventricular septal defects, the most common form of CHD, have a characteristic harsh, systolic murmur associated with them. However, the pressures in the newborn pulmonary system are still high (roughly equal to systemic pressures), and thus there is usually no flow gradient across a large ventricular defect to produce a murmur in the first few days of life. Complex CHD typically presents as cyanosis, tachypnea, or shock and will rarely present as an asymptomatic murmur. Signs may develop quickly with closure of the ductus arteriosus if the lesion has ductal-dependent pulmonary or systemic flow. The initial steps in evaluating a stable patient for suspected CHD include 4-extremity blood pressure measurements, measurement of pre- and postductal saturations, electrocardiogram, chest radiography, and a hyperoxia test. The diagnosis of CHD is usually established by echocardiogram.
D. Abdomen
The examiner should listen for bowel sounds and palpate the abdomen for masses, organomegaly, or abnormal musculature. The liver is easily palpable in the newborn and the inferior edge is usually 1–2 cm below the right costal margin. It is often possible to palpate the kidneys and spleen. Absence of the abdominal musculature may be associated with significant urinary tract abnormalities. The umbilical stump should be assessed for redness or induration that may suggest the presence of an infection. Umbilical hernias are common and typically require no intervention in infancy. Omphalocele and gastroschisis are major abdominal wall defects and require emergent surgical evaluation. Omphalocele is a midline abdominal wall defect. Bowel, and often liver, herniate through the defect, and the umbilicus is typically on the anterior aspect of the omphalocele. Unless ruptured, an omphalocele is covered by a membrane. Omphalocele is associated with aneuploidies, certain genetic syndromes such as pentalogy of Cantrell, and other congenital structural malformations. The defect in gastroschisis is typically to the right of the umbilicus on the abdominal wall, and the etiology of the defect is thought to be due to vascular interruption. The entire bowel may be externalized, but the liver typically remains internal. Unlike omphaloceles, the externalized bowel is not covered by a membrane. Other bowel abnormalities such as bowel atresias and malrotation of the bowel may be present in infants with gastroschisis. Fetuses with gastroschisis are also at increased risk of developing intrauterine growth restriction.
E. Genitalia
The penile length and clitoral size should be inspected to rule out ambiguous genitalia. The labia majora should cover the labia minora and clitoris in a term female. White mucouslike discharge from the vagina is often present and is physiologic.
The scrotum should be evaluated for hernias or masses and descent of the testicles. Transillumination of the scrotum will help to distinguish a hydrocele from an inguinal hernia. The position of the urethral meatus is important to note, as the presence of hypospadias should preclude routine circumcision to allow for optimal surgical correction of the hypospadias.
F. Anus
The rectum should be evaluated for patency and position. An anteriorly displaced rectum may be associated with a rectogenital fistula.
G. Musculoskeletal System
The extremities, spine, and hips are examined for signs of fracture, malformation, or deformation. Range of motion of the joints is assessed. Arthrogryposis, contractures of the joints, may be seen with neuromuscular disease or oligohydramnios as a result of decreased or limited movement in utero. Abnormalities of the extremities, such as polydactyly or syndactyly, are seen in different chromosomal abnormalities and syndromes and may help in making the diagnosis. Particular attention should be paid to the examination of the hips (despite the fact that a dislocation may not be detectable in the first weeks of life) because developmental dysplasia of the hip (DDH) can cause permanent damage if left undetected throughout the first year of life. Either the Barlow or Ortolani test may be used to determine whether a dislocation is present. The Barlow test involves positioning the patient on the back, bringing the knees together at midline, and then pushing down and out on the upper inner thighs. The Ortolani test involves pushing downward on the femurs while abducting the hips. With both maneuvers the dislocation is detected as a clunk as the femoral head is dislocated from the acetabulum (posteriorly with the Barlow, laterally with the Ortolani). Asymmetry of the gluteal folds and skin creases of the legs is another clue to the presence of DDH.
H. Neurologic System
Observing the activity level, alertness, and positioning of the newborn provides a tremendous amount of information about the overall state of health. A healthy, full-term newborn at rest should lie with the extremities flexed. Decreased tone may be a sign of neuromuscular or systemic illness such as sepsis. There should be spontaneous intermittent movement of all 4 limbs, and the baby should be alert during at least portions of the examination. Pupil size and symmetry should be noted. Primitive reflexes such as the Moro, grasp, suck, and tonic neck reflex should all be present at birth. To elicit the Moro reflex, the newborn is supported with a hand under the back and then rapidly dropped a few centimeters back toward the examination bed. The full Moro reflex consists of extension and then flexion and adduction of the arms (“embrace”), opening of the eyes, and a cry. Reflexes are elicited by tapping a finger over the appropriate tendon. Significant clonus may be a sign of central nervous system injury. A sacral dimple or tuft of hair over the sacral spine may indicate spina bifida occulta and should be evaluated with a spinal ultrasound; if the findings of the ultrasound are equivocal, a magnetic resonance imaging scan should be done at approximately 3 months of age.
Feeding
The benefits of breastfeeding on everything from the strength of the immune system to developmental outcomes and IQ have been well documented. Human milk is the most easily digested form of infant nutrition, and its caloric value is superior to formula. Mothers should be counseled prenatally about the benefits of breastfeeding and encouraged by their obstetric caregivers to consider breastfeeding. Contraindications to breastfeeding include HIV infection, active tuberculosis infection, and the use of certain medications. Maternal hepatitis C virus (HCV) infection is not a contraindication to breastfeeding. Transmission of HCV via breastmilk is not documented in the absence of coexisting maternal infection with HIV. Nevertheless, infected mothers should be informed that transmission via breastmilk is theoretically possible.
Breastfeeding may be difficult and frustrating for new mothers. It is important that the newborn nursery staff work to provide mothers with the support and knowledge they need to make breastfeeding a positive experience. It is also important that mothers of newborns who require bottle supplementation (eg, a dehydrated, jaundiced infant) are reassured that their efforts at breastfeeding will not be derailed by exposure to the bottle during a limited, medically necessary period, and that breastfeeding can still ultimately succeed.
Regardless of the overwhelming literature to support the value of breast milk, many mothers in the United States choose to bottle-feed their children. Selection of the formula given to the newborn is often based on what formula is available in the nursery or by the mother’s preference. Standard-term infant formula contains iron supplementation and provides 20 kcal/oz. No one formula is better than another for healthy term infants. Mothers with a family history of lactose intolerance sometimes request soy formula, and standard soy formula will provide adequate nutrition for growth and development. Formulas such as Alimentum and Nutramigen are available for infants with more significant protein allergy. Premature infant formulas contain 24 kcal/oz and provide higher amounts of protein, medium-chain triglycerides, and vitamins and minerals (eg, calcium and phosphorous) than standard formulas. The AAP currently recommends formula for the first year of life.
Voiding and Stooling
Voiding should be monitored closely in the nursery. Changes in the baby’s weight and the frequency of urination can be used to assess the hydration status and adequacy of intake in a breastfeeding baby. The time of the first void of urine and stool should be documented. Failure to void in the first 24 hours of life should prompt an evaluation of renal function and hydration status. Failure to pass stool in the first 48 hours of life should prompt an evaluation for possible bowel obstruction; 94% of normal term newborns will pass meconium in the first 24 hours of life. Obstruction can result from conditions such as bowel atresia or stenosis, Hirschsprung’s disease, and meconium ileus.
American Academy of Pediatrics and American Heart Association. Textbook of Neonatal Resuscitation. 5th ed. Dallas, TX: American Academy of Pediatrics; 2006.
NEWBORN SCREENING & PROPHYLAXIS
The initial newborn exam may be normal despite the presence of serious occult illness. Signs of complex congenital heart disease, sepsis, gastrointestinal obstruction, significant jaundice, inborn errors of metabolism, and other illnesses may not be present until the second or third day of life at the earliest: shortly before, and at times after, the baby’s discharge. Screening is done in the hopes of detecting disease before a patient becomes symptomatic and is usually reserved for processes that have a worse prognosis if not detected early and for which there is effective therapy. The maternal medical history, the obstetric and perinatal history, and state laws determine what screening is done on any given baby.
Standard newborn screening tests have traditionally screened for the following:
1. Phenylketonuria by Guthrie’s test for phenylalanine level
2. Congenital hypothyroidism by thyroid function testing
3. Congenital syphilis by either rapid plasma reagent (RPR) or Venereal Disease Research Laboratory (VDRL) test (whichever test was performed on the mother)
4. ABO incompatibility using infant blood type and direct Coombs’ test (standard if mother has O blood type, done at many institutions for all newborns)
5. Hearing loss (evaluated by auditory brainstem response or otoacoustic emissions)
Using tandem mass spectrometry, it is now possible to screen for as many as 50 congenital conditions from a single blood sample. Although it has been standard in many states for years now, expanded newborn screening was only adopted as a national standard in the United States in the spring of 2010.
Additional targeted screening often includes evaluation for infection, illicit drug exposure, hyperbilirubinemia, and hypoglycemia when there are risk factors that increase the yield of the testing. A history of rupture of amniotic membranes for >18 hours before delivery, maternal intrapartum fever, chorioamnionitis, and a positive maternal group B streptococcus culture without adequate treatment before delivery are all risk factors for newborn sepsis. A history of any of these risk factors warrants a screening evaluation of the asymptomatic newborn for laboratory evidence of infection. Screening is routinely done for hypoglycemia in infants of diabetic mothers as well as for SGA and LGA babies. At many institutions, infants of diabetic mothers are screened for polycythemia as well.
Information about maternal hepatitis B, HIV, herpes simplex virus (HSV), chlamydia, and syphilis status is essential to newborn care. Adequate prophylaxis for hepatitis B can prevent transmission in 95% of infants born to hepatitis B surface antigen–positive (HBsAg+) mothers. A baby born to a mother who is HBsAg+ should receive the hepatitis B vaccine and hepatitis B immune globulin (HBIG) within the first 12 hours of life to prevent hepatitis B virus transmission. If the mother’s status is unknown, the newborn should receive the vaccine within 12 hours of birth, and every effort should be made to determine the mother’s status. If the baby weighs more than 2 kg, HBIG can be given as late as 7 days of life if maternal status is positive or still unknown and still provide effective postexposure prophylaxis. However, a baby who weighs <2 kg at birth should receive HBIG by 12 hours of postnatal life to receive adequate prophylaxis. Appropriate screening and treatment for infants born to mothers with a history of infection with HIV, chlamydia, HSV, or syphilis are detailed in the AAP’s Red Book.
CIRCUMCISION
Routine circumcision is not currently recommended by the AAP. Although there is evidence that supports some medical benefits of circumcision (eg, decreased incidence of urinary tract infections during infancy, sexually transmitted disease, and penile cancer), the data are insufficient for the AAP to recommend the procedure for all newborn males, given concerns about the impossibility of informed consent in an infant and evidence of the pain and stress caused by the procedure. Parents should be provided with unbiased information about the procedure, and the decision to proceed should be left to them. If circumcision is performed, analgesia, either topical or by nerve block, should be given.
DISCHARGE PLANNING
The physician should complete another thorough examination on the day of discharge to reevaluate the overall health of the newborn. Anticipatory guidance should be given to parents to help them care for their newborns and recognize signs of illness and distress. Safety issues, such as the use of car seats, should be addressed. Parents should be alerted to problems such as fever, lethargy, and poor feeding that should prompt them to see a physician. They should be taught about expected newborn behavior, adequate feeding, monitoring of voiding and stooling, and umbilical cord care.
Anticipatory guidance is particularly important now that hospital stays after delivery are often only 36–48 hours. Criteria for newborn discharge at <48 hours of life are outlined in a 2004 AAP policy statement. Newborns discharged before 48 hours of life must be examined by a health care professional within 72 hours of the discharge, preferably within 48 hours. The plan for the newborn’s first visit to the physician and any necessary follow-up laboratory testing or nursing visits to the home should be clearly established at the time of discharge, and parents should be able to demonstrate skill and comfort with feeding and tending to the baby’s basic needs.
American Academy of Pediatrics. AAP 2009 Red Book: Report of the Committee on Infectious Diseases. 28th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2009.
American Academy of Pediatrics, Committee on Fetus and Newborn. Policy statement: Hospital stay for healthy term newborns. Pediatrics 2010;125:405–409. PMID: 20100744.