George K. Creatsas1 and Maria Creatsa1
(1)
2nd Department of Obstetrics and Gynecology, Aretaieio Hospital, University of Athens, 76 Vas Sofias Ave, Athens, 11528, Greece
George K. Creatsas
Email: geocre@aretaieio.uoa.gr
Menstrual disorders are a common problem in young girls. Table 1.1 presents the menstrual disorders during adolescence among 790 cases treated in our institution.
Table 1.1
Menstrual disorders during adolescence
|
Menstrual disorders |
Incidence % |
|
A. DUB |
381 (48.2 %)a |
|
B. Amenorrhea |
180 (22.8 %) |
|
C. Oligomenorrhea |
165 (20.9 %) |
|
D. Dysmenorrhea |
64 (8.1 %) |
|
Total |
790 cases |
aPersonal data
1.1 Dysfunctional Uterine Bleeding (DUB)
DUB (Table 1.1, A) is a painless endometrial bleeding that is prolonged, excessive, and irregular and not attributable to any underlying structural or systemic disease.
The etiology of DUB, during adolescence, arises out of continuing maturation of the hypothalamus [1–3]. In the USA the definition of DUB refers to anovulatory bleeding. The European Society of Human Reproduction and Embryology (ESHRE) defined DUB as excessive bleeding (excessively heavy, prolonged, or frequent) of uterine origin, which is not due to demonstrable pelvic disease, complication of pregnancy, or systemic disease. DUB can be either ovulatory or anovulatory [4].
A shift in the ratio of prostaglandins (PGs) and especially of the endometrial vasoconstrictor (PGF2a) to the vasodilator (PGE2) and an increase in total endometrial PGs have been demonstrated in ovulatory DUB patients [1, 5].
Diagnosis is made by the clinical history and the clinical examination, followed by the necessary laboratory tests, the pelvic ultrasonography, the endocrinological examination, and occasionally hysteroscopy and/or laparoscopy. DUB differential diagnosis includes pregnancy complications; neoplasms of the genital system; genital tract infections; endocrinopathies; treatment with various, several medications; trauma; coagulation disorders; and chronic systemic diseases.
The disease is classified in three groups as follows: group 1, mild hypermenorrhea (hemospherin (Hb) and hematocrit (Hct) within normal limits); group 2, moderate hypermenorrhea (Hb 9–10 g and no signs of anemia); and group 3, severe hypermenorrhea (Hb less than 8 g). The management depends on the severity of the disease and includes: the use of combined oral contraceptives (COCs,) progestogenic compounds followed by COCs, nonsteroidal anti-inflammatory drugs, transfusion, iron supplements, and reassurance [6–8].
1.2 Amenorrhea
Amenorrhea (Table 1.1, B) is classified as primary or secondary. Primary amenorrhea (PA) is the absence of menstruation in 16-year-old girls who have already developed secondary sexual characteristics or in 14-year-old girls who have no secondary sexual characteristics development. Especially for the second group, the term “late puberty” is preferable. Secondary amenorrhea (SA) is the absence of menstruation for 6 months. For adolescents with formerly regular cycles, SA is defined as the absence of menses for more than three subsequent periods [1, 5].
WHO classifies PA in three groups as follows: group I, no evidence of endogenous estrogen production, normal or low follicle stimulating hormone (FSH) levels, normal prolactin (PRL) levels, and no evidence of a lesion in the hypothalamic-pituitary region; group II, evidence of estrogen production and normal levels of PRL and FSH; and group III, which involves cases with elevated FSH serum levels indicating gonadal failure.
Table 1.2 presents the etiology of PA and SA.
Table 1.2
Etiology of PA or SA
|
1. Delayed puberty (PA) |
|
2. Congenital uterovaginal anomalies (PA or SA) |
|
3. Endocrine disorders (PA or SA) |
|
4. Premature ovarian failure (PA or SA) |
|
5. Chromosomal anomalies (PA or SA) |
|
6. Stress and psychological problems (PA or SA) |
Delayed puberty (DP) is presented as PA and is defined as the absence of onset of puberty by >2 SD later than the average age, i.e., >14 years in females [2, 8].
Congenital uterovaginal anomalies includes: obstruction of the genital tract and absence of the uterus or/and the vagina [9, 10].
Several endocrine disorders may also be the cause of PA or SA. Table 1.3 presents the causes of hypothalamic amenorrhea [2]. The pituitary causes of amenorrhea are: (a) Tumors: prolactinomas, other hormone-secreting pituitary tumors, nonfunctional tumors (craniopharyngioma) metastatic tumors. (b) Space-occupying lesions: empty sella syndrome, arterial aneurysm. (c) Pituitary necrosis: postpartum pituitary necrosis (Sheehan syndrome), panhypopituitarism, and systemic inflammatory diseases (sarcoidosis, hemochromatosis) [2, 8].
Table 1.3
Causes of hypothalamic amenorrhea
|
1. Dysfunctional |
Stress |
|
Exercise |
|
|
Nutrition and pseudocyesis |
|
|
2. Other |
Isolated gonadotropin deficiency, Kallmann syndrome, idiopathic hypogonadotropic hypogonadism |
|
Infections, chronic debilitating disease |
|
|
Tumors (craniopharyngioma, germinoma, hamartoma, Langerhans cell histiocytosis, teratoma, endodermal sinus tumor, metastatic carcinoma) |
Hyperprolactinemia is associated with decreased estradiol concentrations and amenorrhea or oligomenorrhea. In cases of persistent hyperprolactinemia, after ruling out primary hypothyroidism, a magnetic resonance imaging of the pituitary is indicated.
The premature ovarian failure (POF) is usually a cause of SA. In patients with POF who are sexually active, we would strongly consider using the combined oral contraceptives (COCs) as hormone replacement therapy. COCs may be more socially acceptable to a young woman. However, we always counsel all sexually active girls regarding the correct use of condoms to prevent sexually transmissible diseases. In adolescent women with POF, a karyotype should be also obtained to rule out sex chromosome translocations and the presence of a Y chromosome, which is associated with an increased risk of gonadal tumors.
Amenorrhea due to chromosomal anomalies may be primary of secondary. In these cases the possibility of gonadal dysgenesis, pseudohermaphroditism, and other pathologies, as mentioned above, should be ruled out.
Amenorrhea may also be due to stress, anorexia, or exercise. According to the practice committee of the American Society of Reproductive Medicine, the evaluation of PA is indicated when there has been a failure to menstruate by age 15 in the presence of normal secondary sexual development (2 SD), above the mean of 13 years or within 5 years after breast development, if that occurs before age 10 or if there is a failure of breast development by age 13 (2 SD above the mean of 10 years) [4, 11].
Further to the previous reported investigations, Table 1.4 presents the suggested flow diagram for the evaluation of amenorrhea.
Table 1.4
Suggested flow diagram aiding in the evaluation of amenorrhea [11, 12]
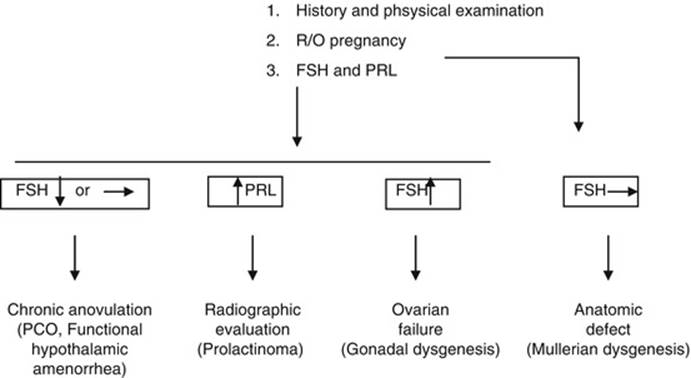
The management of amenorrhea during adolescence depends on the etiology of the symptom. In any case treatment should be started as soon as possible.
1.3 Oligomenorrhea
Oligomenorrhea during adolescence is usually due to the polycystic ovarian syndrome (PCO). Symptoms of hyperandrogenism in adolescent girls are usually due to the PCO syndrome.
The management of oligomenorrhea during adolescence is mainly related to the management of PCO syndrome using also the new generation COCs.
1.4 Dysmenorrhea
Dysmenorrhea is a common problem in adolescence. It is presented as a painful menstruation (organic disease, congenital anomalies, and endometriosis). Usually pain starts along with the start of bleeding and lasts for 48–72 h. Dysmenorrhea is characterized as primary (PD) when no organic disease is present and as secondary when a pelvic pathology is documented. PD is more frequent in adolescence and usually starts after ovulation. COCs and PG synthetase inhibitors are the most frequently used agents for the management of PD [12].
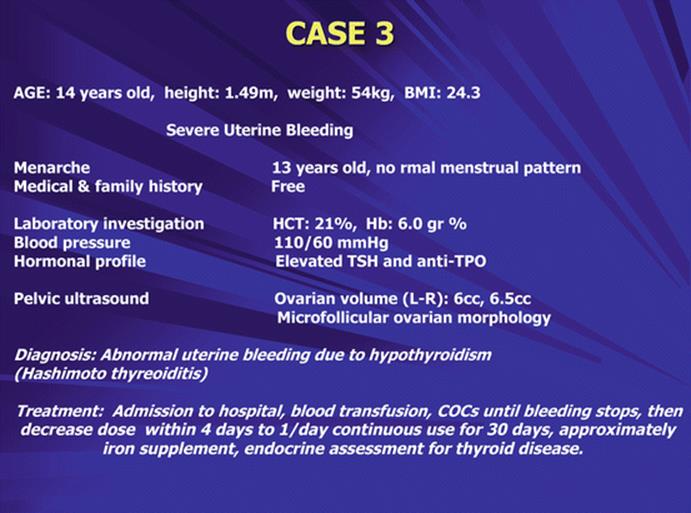
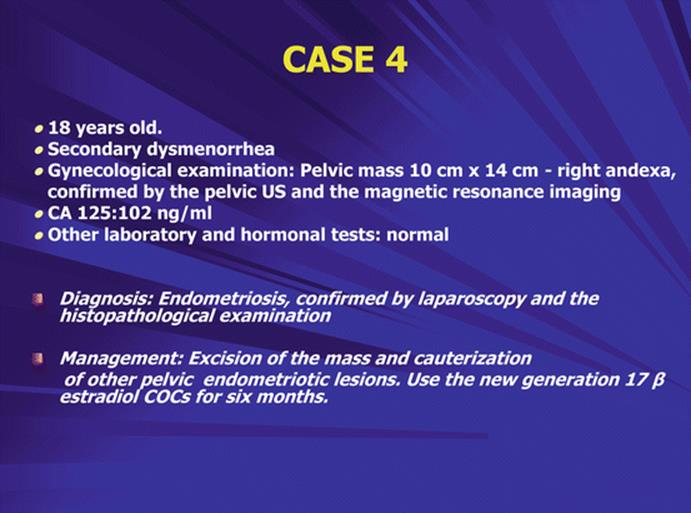
1.5 Clinical Cases


1.6 Conclusion
Menstrual disorders are a common problem during adolescence. Information and consultation should be provided to the young girl and the family about normal menstruation and menstrual disturbances. Prevention and early treatment should be provided by specialized gynecologists, preferably in pediatric and adolescent gynecological centers.
References
1.
Deligeoroglou E, Tsimaris P (2010) Menstrual disturbances in puberty. Best Pract Res Clin Obstet Gynaecol 24(2):157–171PubMedCrossRef
2.
Deligeoroglou E, Athanasopoullos N, Tsimaris P, Dimopoulos K, Vrachnis N, Creatsas G (2010) Evaluation and management of adolescent amenorrhea. Ann N Y Acad Sci 1205:23–32PubMedCrossRef
3.
The Practice Committee of the American Society for Reproductive Medicine Birmingham, Alabama (2006) Current evaluation of amenorrhea. Fertil Steril 86(5 Suppl 1):148–155
4.
Fraser IS, Sungurtekin U (2000) Defining menstrual disturbances. In: Maclean A, O’Brien PMS (eds) Study group on menstrual disorders. Royal College of Obstetricians and Gynecologist, London, pp 141–152
5.
Deligeoroglou E, Tsimaris P, Deliveliotou A, Christopoulos P, Creatsas G (2006) Menstrual disorders during adolescence. Pediatr Endocrinol Rev. (3 Suppl 1):150–9
6.
Committee on Practice Bulletins—Gynecology (2012) Practice bulletin no. 128. Diagnosis of abnormal uterine bleeding in reproductive-aged women. Obstet Gynecol 120(1):197–206CrossRef
7.
Sokkary N, Dietrich JE (2012) Management of heavy menstrual bleeding in adolescents. Curr Opin Obstet Gynecol 24(5):275–280PubMedCrossRef
8.
Deligeoroglou E, Karountzos V, Creatsas G (2013) Abnormal uterine bleeding and dysfunctional uterine bleeding in pediatric and adolescent gynecology. Gynecol Endocrinol 29(1):74–78PubMedCrossRef
9.
Creatsas G, Deligeoroglou E, Christopoulos P (2010) Creation of a neovagina after Creatsas modification of Williams vaginoplasty for the treatment of 200 patients with Mayer – Rokitansky – Kuster – Hauser syndrome. Fertil Steril 94(5):1848–1852PubMedCrossRef
10.
Creatsas G, Deligeoroglou E, Tsimaris P, Pantos K, Creatsa M (2011) Successful pregnancy in a Swyer syndrome patient with preexisting hypertension. Fertil Steril 96(2):83–85CrossRef
11.
The Practice Committee of the American Society of Reproductive Medicine (2008) Current evaluation of amenorrhea. Fertil Steril 90(Suppl):1–528
12.
Lethaby A, Duckitt K, Farquhar C (2013) Non-steroidal anti-inflammatory drugs for heavy menstrual bleeding. Cochrane Database Syst Rev (1):CD000400