Stuart Ralston1
(1)
Bone and Rheumatology Research Group, University of Edinburgh, Edinburgh, EH4 2XU, UK
Stuart Ralston
Email: stuart.ralston@ed.ac.uk
Introduction
Bisphosphonates are amongst the most widely used medicines in the pharmacopoeia and are indicated for the treatment of various bone diseases associated with osteoclast over-activity including osteoporosis, cancer-associated bone disease and Paget’s disease of bone (Russell 2011). Prescription of bisphosphonates has increased over recent years, largely due to increased awareness of osteoporosis which us by far the most common indication for bisphosphonate therapy. Osteoporosis is a common disease but predominantly affects post-menopausal women. Reflecting this fact it has been estimated that about 30 % of women suffer an osteoporosis–related fracture at some point in life (Sambrook and Cooper 2006). This chapter reviews the beneficial effects and adverse effects of bisphosphonates used in the treatment of osteoporosis.
Historical Aspects
Bisphosphonates were first synthesised in the nineteenth century and initially used as chelating compounds in various industrial applications. An application which eventually led to studies of their use in bone disease was as water softening agents in detergents. The initial studies of bisphosphonates in bone focused on the hypothesis that they might be useful for the treatment of ectopic calcification based on the fact that that bisphosphonates are powerful inhibitors of mineralisation (Francis et al. 1969). However clinical studies have not shown beneficial effects of bisphosphonates on ectopic calcification and the clinical application of these drugs has focused on their inhibitory effects on bone resorption (Russell et al. 1970).
It was originally considered that bisphosphonates inhibit bone resorption by preventing dissolution of hydroxyapatite crystals (Fleisch et al. 1969) but it is now known that the inhibitory effects of bisphosphonates on bone resorption are not due to a physicochemical mechanism but rather, to a cellular mechanisms (Russell 2011). Nonetheless, the physiochemical interaction between bisphosphonates and hydroxyapatite plays a crucial role in targeting bisphosphonates to the bone surface and is an important determinant of potency (Nancollas et al. 2006). This activity continues to be exploited diagnostically through by the use of 99Tm-labelled bisphosphonates as reagents for radionuclide bone scanning. However, in this chapter I will focus on the clinical use of bisphosphonates as treatments for bone disease rather than as imaging agents.
Chemical Structure
Bisphosphonates share in common a core structure of phosphate-carbon-phosphate atoms (Fig. 12.1) which is responsible for the bisphosphonates’ ability to bind calcium and hydroxyapatite crystals.
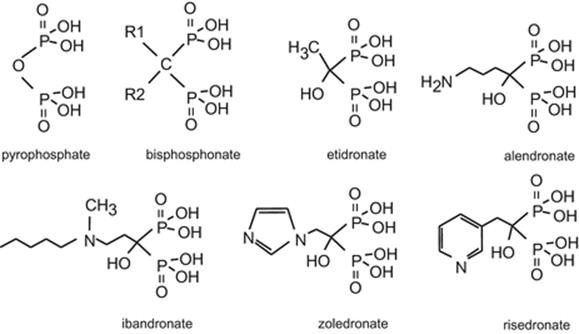
Fig. 12.1
Bisphosphonate structure
Bisphosphonates are chemically related to pyrophosphate and have a common core structure in which a central (geminal) carbon links two phosphonate groups. The phosphonate groups bind calcium and are responsible for the ability of bisphosphonates to bind hydroxyapatite crystals in bone. Different bisphosphonates have different side chains attached to the carbon atom at the R1 and R2 position and these influence both potency and affinity for mineral binding (see text for more details)
Bisphosphonates have a similar core structure to pyrophosphate which is a naturally occurring inhibitor of mineralisation. The central (or geminal) carbon atom of bisphosphonates render them chemically stable and resistant to hydrolysis, unlike pyrophosphate which is broken down rapidly by alkaline phosphatase. Chemical substitutions at the central (geminal) carbon atom of the bisphosphonates alter both the affinity for calcium binding and the mechanisms of action. For example the presence of a hydroxyl group at the R1 position tends to increase calcium binding affinity. Substitutions of nitrogen containing side chains at the R2 position not only alter the calcium binding properties of bisphosphonates but also increase potency considerably (Ebetino et al. 2011).
Pharmacology
Following administration, bisphosphonates are widely distributed in the extracellular fluid. About half of the administered dose is excreted by the kidney without further metabolism and the remainder is bound to the skeleton particularly at sites of high bone turnover (Russell 2011; Sato et al. 1991). When bone containing the bisphosphonate undergoes resorption, the drug is released within the osteoclast causing cell death and inhibition of bone resorption (Fig. 12.2).
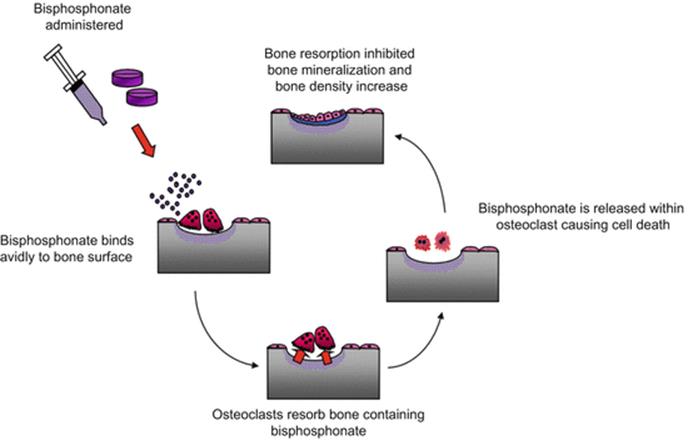
Fig. 12.2
Mechanism of action of bisphosphonates
It should be noted that the mechanisms of osteoclast inhibition differ for nitrogen-containing and simple bisphosphonates, as discussed in more detail below (Ebetino et al. 2011). Bisphosphonates also inhibit bone formation, but it is unclear to what extent this is due to the close coupling that exists between bone resorption and formation or a direct inhibitory effect on the osteoblast (Idris et al. 2008). Bisphosphonate that has become bound to bone which is not immediately resorbed by osteoclasts can remain within the skeleton for prolonged periods. It is thought that slow release of bound bisphosphonate from the bone occurs subsequently over a period of months or years as the result of two processes; passive diffusion into the extracellular space and release during cycles of bone resorption (Russell 2011). The half-life of bisphosphonates in the skeleton is very long indeed such that inhibitory effects on biochemical markers of remodelling may be observed for one or more years after treatment has stopped. This is most relevant for bisphosphonates that have a high affinity for hydroxyapatite binding such as zoledronic acid and alendronic acid (Nancollas et al. 2006).
Bisphosphonates are poorly absorbed from the gastro-intestinal tract (<5 %) and absorption is further inhibited with food (Porras et al. 1999; Sansom et al. 1995), probably due to binding of the phosphonate moiety with dietary calcium (Janner et al. 1991). This, coupled with the tendency of some bisphosphonates to cause upper gastrointestinal (GI) upset, has led some pharmaceutical companies to develop intravenous formulations of bisphosphonates. All bisphosphonates have the potential to cause inhibition of bone mineralisation, but this is of most clinical relevance in the case of etidronate where the concentration required to inhibit bone resorption is close to that required to inhibit bone mineralisation (Flora et al. 1981).
Bisphosphonates inhibit osteoclastic bone resorption and this is accompanied by an increase in bone mineral density (BMD) (Ebetino et al. 2011). Although the increases in BMD observed during bisphosphonate therapy were originally thought to be due to infilling of the remodelling space (suppression of bone resorption with continued bone formation) it is now known that the increased BMD that occurs in response to bisphosphonate treatment mainly occurs through increased mineralisation of existing bone, rather than a gain in bone mass (Boivin et al. 2000).
Mechanism of Action
Bisphosphonates can be divided into two broad classes in terms of the mechanism by which they inhibit osteoclast activity (Rogers et al. 1999). Simple bisphosphonates such as etidronate, become incorporated into non-hydrolysable analogues of adenosine triphosphate (ATP) that result in cytotoxicity and cell death by depleting levels of ATP which plays an essential role in storing energy within osteoclasts and other cells (Frith et al. 1997, 2001). On the other hand, nitrogen containing bisphosphonates such as alendronic acid, risedronate, ibandronate and zoledronic acid inhibit the enzyme farnesyl pyrophosphonate synthase (FPPS) which is responsible for the addition of lipid chains (prenylation) to small GTPases such as Ras, Rac and Rho. This prevents the GTPases localising to cell membranes properly, resulting in osteoclast inhibition and loss of resorptive function (Coxon et al. 2000; Luckman et al. 1998).
Nitrogen-containing bisphosphonates (also known as aminobisphosphonates) are much more powerful inhibitors of osteoclast activity than simple bisphosphonates. There are also major differences between aminobisphosphonates in the potency with which they inhibit FPPS. The inhibitory effect of aminobisphosphonates on bone resorption in man is correlated with the potency with which they inhibit FPPS, but also depends on factors such as their affinity for hydroxyapatite binding (Russell et al. 2008).
Bisphosphonates for the Prevention and Treatment of Osteoporosis
The bisphosphonates discussed below have been licensed in many countries for the prevention and treatment of osteoporosis although not all drugs are available in all countries. Whilst bisphosphonates share many properties in common, differences also exist in terms of chemical structure, mechanism of action and pharmacological profile which makes each bisphosphonate subtly different (Russell 2011). Because of this, the therapeutic and adverse effects of different bisphosphonates will be considered separately in the sections that follow.
Etidronate
Etidronate is licensed for the treatment of osteoporosis but is now seldom used due to the availability of more potent bisphosphonates. Indeed in the UK etidronate is no longer marketed for the treatment of osteoporosis even though the drug still has marketing approval for this indication.
Etidronate is administered orally and should be taken on an empty stomach and the patient advised to fast for at least 1 h after administration to ensure adequate intestinal absorption. Like other bisphosphonates, etidronate should be used with caution in renal impairment and is contraindicated in patients with a glomerular filtration rate (GFR) below 30. In osteoporosis, etidronate is given cyclically in a dose of 400 mg daily orally for a period of 10 days every 3 months, alternating with calcium supplements between the cycles of etidronate.
Efficacy
Cyclical etidronate was first marketed by Proctor and Gamble as Didronel PMO™ for the treatment of osteoporosis. The studies of etidronate in osteoporosis were small by today’s standards. In one study 429 postmenopausal women were randomise to receive cyclical etidronate or placebo along with calcium supplementation or phosphate supplements over a 2 year period (Watts et al. 1990). Each treatment group consisted of about 100 patients. Bone density at the spine increased by about 5 % in the etidronate treated groups but did not change significantly in the placebo groups. Phosphate had no additional effect. Fewer patients in the etidronate treated groups suffered vertebral fractures (29.5/1,000 patient years vs. 62.9/1,000 patient years), a result which was just significant (p = 0.043) but there was no reduction in non-vertebral fractures.
Another smaller study with 33 patients per group showed similar effects on BMD over a 3 year period but, not surprisingly given the small numbers, there was no significant reduction in fractures (Storm et al. 1990). An observational study in the UK General Practice Research Database (GPRD) which compared fracture rates in etidronate treated patients with matched controls who had a diagnosis of osteoporosis but who were not treated with etidronate reported a reduced risk of fracture in the etidronate treated group (relative risk 0.80, 95 % CI 0.70–0.92). However it was not possible in this study to control for various confounding factors such as the severity of osteoporosis and selection bias so the results have to be treated with caution (van Staa et al. 1998).
Cyclical etidronate is also licensed for the treatment of glucocorticoid induced osteoporosis (GIOP). The largest randomised trial of etidronate in GIOP involved 67 etidronate and 74 placebo treated patients followed over a 12 month period. About 60 % of patients were women, the majority of whom were postmenopausal. Spine bone density increased by about 4 % in the etidronate group but fell in the placebo group – a result that was significant (p = 0.02). Vertebral fractures were less common in the etidronate group but the relative risk reduction was not significant (0.6, 95 % CI 0.2–1.6) (Adachi et al. 1997). A subsequent pooled analysis of etidronate from five randomised trials in GIOP confirmed that the drug increased BMD by about 5 % at the spine but reported no overall reduction in fracture risk (RR = 0.50, 95 % CI = 0.21–1.19).
Adverse Effects
The randomised trials placebo-controlled trials of etidronate, while limited in sample size, showed that the drug was well tolerated with an adverse effect profile that was not different from placebo. Adverse effects mentioned in the summary of product characteristics include diarrhoea, upper GI upset and leg cramps. Mineralisation defects and pathological fractures have been reported in patients with Paget’s disease treated with etidronate (Boyce et al. 1984) but this does not seem to be a problem with the cyclical regimen used for osteoporosis (Storm et al. 1990). Renal impairment has rarely been reported in patients with hypercalcaemia given high doses of intravenous etidronate (Bounameaux et al. 1983), but this is not relevant in the osteoporosis setting.
Alendronic Acid
Alendronic acid is an aminobisphosphonates that is about 50 times more potent than etidronate at inhibiting bone resorption (Fleisch 1993). It also has a high affinity for binding hydroxyapatite (Nancollas et al. 2006) and this is thought to be responsible for its long duration of action. Alendronic acid, like other bisphosphonates, is poorly absorbed from the GI tract and must be taken on an empty stomach with a large glass of water and the patient should be advised to remain upright for 30 min to minimise the risk of the tablet sticking in the oesophagus. This prompted Merck, the manufacturer of branded alendronate (Fosamax®) to introduce a film – coated tablet to ease passage through the oesophagus, although multiple generic brands of alendronic acid are now available that do not have any special coating. Following administration patients should be advised to wait for at least 30 min before taking other medication or food to ensure adequate absorption. This can prove inconvenient or impractical for some patients. Alendronic acid should be used with caution in renal impairment since it is primarily eliminated by renal excretion. Alendronic acid is contra-indicated in patients with a GFR below 35 ml/min.
Efficacy
Several large-scale randomised trials of alendronic acid have been performed in women with postmenopausal osteoporosis with the entry criteria of low BMD and/or pre-existing vertebral fractures (Liberman et al. 1995; Black et al. 1996; Pols et al. 1999). Meta-analyses have shown that alendronic acid reduces the risk of vertebral, non-vertebral and hip fractures in postmenopausal women as compared with calcium and vitamin D supplemented supplemented placebo. For vertebral fractures, data are available from six studies involving 7,361 postmenopausal women in which the relative risk was 0.55 (95 % CI 0.45–0.67) for alendronic acid as compared with placebo. For non-vertebral, non hip fractures, data from 9,625 women in six studies showed a relative risk of 0.84 (95 % CI 0.74–0.94) compared with placebo. For hip fractures data from 9,952 women showed a relative risk of 0.61 (95 % CI 0.40–0.92) compared with placebo (Wells et al. 2008a).
Alendronic acid is also effective at increasing BMD and reducing vertebral fracture risk in GIOP (Saag et al. 1998; Adachi et al. 2001). The studies in GIOP are much smaller than in postmenopausal osteoporosis and were designed with BMD as a primary endpoint rather than fracture. A key study was that of Saag and colleagues who compared the effects of two doses of alendronate (5 and 10 mg daily) with calcium supplemented placebo in 447 patients with GIOP over a 48 week period (Saag et al. 1998). About 70 % of the study group were women and two thirds were postmenopausal. Bone density in the alendronic acid treated patients increased by about 3 % but fell in the placebo group, a difference that was highly significant (p < 0.01). An extension of this study to 2 years in 66 men and 142 women (Adachi et al. 2001) showed that vertebral fractures were less frequent in the alendronic acid group versus the placebo group (0.7 % versus 6.8 %; p = 0.026). There was no significant difference in the frequency of non vertebral fractures. The only substantial experience of alendronic acid in premenopausal women is in the patients who were enrolled into GIOP studies. Subgroup analysis of these studies showed that the response of BMD in premenopausal women was similar to that in postmenopausal women.
Whilst the pivotal fracture trials of alendronic acid were performed with 10 mg alendronic acid daily, subsequent studies showed that 70 mg weekly was bioequivalent in terms of inhibiting bone turnover markers and increasing BMD (Schnitzer et al. 2000). Since the once weekly dosing is much more convenient, alendronic acid is now almost always given in a dose of 70 mg once weekly in the treatment of osteoporosis. In routine clinical practice it is also usual to prescribe alendronic acid in combination with calcium and vitamin D supplements since these supplements were used routinely in the randomised trials. A combination product containing alendronic acid 70 mg and cholecalciferol 5,600 units once a week is also available (Fosavance™).
Duration of Treatment
The optimal duration of alendronic acid for the treatment of osteoporosis remains a subject of debate. The effect of duration of therapy has been investigated in one randomised placebo controlled trial in women with postmenopausal osteoporosis who participated in the Fracture Intervention Trial (FIT) (Black et al. 1996). Patients who had already been treated for at least 3 years with alendronic acid in the FIT trial were invited to take part in an extension study in which they were randomised to receive therapy with placebo (n = 437) or to continue alendronic acid 5 mg daily (n = 329) or 10 mg daily (n = 333) for a further 5 years (Black et al. 2006). All patients received calcium and vitamin D supplements. The average duration of alendronic acid on entry to the study was 5 years. Patients with a total hip T-score of <−3.5 and those with a T-score below the baseline value in FIT were excluded. The proportion of patients who completed follow up according to protocol was close to 90 % and did not differ between the groups.
At the end of the study, patients who continued alendronic acid for 10 years maintained the increase in total hip BMD observed during the initial 5 years therapy, whereas those randomised to placebo experienced a fall in total hip BMD between years 5 and 10 of about 2 %. At the lumbar spine, BMD increased by about 4 % between years 5 and 10 in both alendronic acid groups but remained stable in the placebo group. The bone resorption marker N-telopeptide of type I collagen cross-links (NTX) remained suppressed in alendronic acid treated patients during the 10-years of study, but increased by about 60 % between years 5 and 10 in the patients assigned to placebo. At the end of the study, there were no differences in the rate of non-vertebral fractures or morphometric vertebral fractures between the groups, but clinical vertebral fractures were less common in the patents that had received 10 years therapy (5.3 % for placebo and 2.4 % for alendronate; relative risk, 0.45; 95 % CI, 0.24–0.85). Adverse effects were similar in the two treatment groups.
The long term effects of alendronic acid have also been documented in an observational study of postmenopausal women who were treated over a 10-year period with alendronic acid (Bone et al. 2004). This represented an extension study of two randomised placebo controlled trials which together enrolled 994 women with postmenopausal osteoporosis. Of 804 women who entered the extension, 322 were randomised to receive continued alendronic acid 5 or 10 mg daily and 164 (50 %) completed 10 years therapy. The original trial included a cohort of 160 women who received 5 years of alendronic acid (20 mg daily for years 1–2 and 5 mg daily for years 3–5). These were reassigned to receive placebo for 5 years and 83 (51.9 %) completed 10 years follow up. The initial gains in BMD and reduction in bone turnover markers observed during the first 3 years of therapy of alendronic acid were maintained for 10 years in those allocated to 5 and 10 mg alendronic acid, with no difference between the groups. Those allocated to placebo following 5 years alendronic acid showed a ~20 % rise in NTX and a 2 % fall in femoral neck BMD but no change in lumbar spine BMD. The proportion of patients with fracture in women assigned to 10-years alendronic acid (5 and 10 mg combined) were similar to those who discontinued alendronic acid after 5 years. Adverse effect profile was also similar between the groups.
Taken together these studies suggest that increases in BMD and reductions in bone turnover are maintained in postmenopausal women who continued therapy with alendronic acid for up to 10 years. While the studies suggest that fracture risk reduction is also maintained with alendronic acid for up to 10 years without an obvious increase in adverse reactions, they had limited powered to detect differences in adverse events or fractures between the treatment groups.
Adverse Effects
The adverse event profile of alendronic acid was reported to be similar to that of placebo in randomised trials (Liberman et al. 1995; Black et al. 1996; Pols et al. 1999). However in routine clinical practice, upper gastrointestinal symptoms such as dyspepsia and epigastric pain have emerged as a common adverse effect occurring in about 5 % of patients (Mackay et al. 1998). Oesophageal ulceration and perforations have been reported in isolated patients but it is difficult to estimate the exact frequency with which they occur. They are thought to be due to the tablet sticking in the oesophagus (Mackay et al. 1998). Other rare adverse events which have emerged from post-marketing surveillance studies include uveitis, osteonecrosis of the jaw (Khosla et al. 2007), atypical subtrochanteric fractures (Schilcher et al. 2011) and bone, joint or muscle pain (Wysowski and Chang 2005; Bock et al. 2007).
Osteonecrosis of the jaw is a very rare adverse effect of oral alendronate. It is characterised by the occurrence of necrotic bone in the mandible or maxilla following tooth extraction although some cases occur spontaneously (Novince et al. 2009). In one series, based in the South East of Scotland, the incidence was estimated as less than 0.004 % per treated patient per year for alendronic acid prescribed for postmenopausal osteoporosis, but this increased to 0.1 % for patients treated for GIOP. The condition was first reported during the mid 1980s in patients receiving high dose intravenous bisphosphonate therapy for metastatic bone cancer (Woo et al. 2006) and for this indication it remains a significant problem occurring in up to 2 % of patients (Stopeck et al. 2010). The pathogenesis is incompletely understood but it is thought to be related to over-suppression of bone turnover (Allen and Burr 2009) since it is rare in patients treated with the doses of bisphosphonates used in osteoporosis but is common in cancer associated bone disease where the dose of bisphosphonate is an order of magnitude greater (Woo et al. 2006). Emphasising this fact, osteonecrosis of the jaw has also been associated with denosumab treatment, another powerful antiresorptive drug (Stopeck et al. 2010).
Atypical subtrochanteric fractures are an uncommon adverse effect of alendronic acid with an estimated incidence of 5 cases per 10,000 patient years of treatment (Schilcher et al. 2011). Patients are at risk of developing these fractures within 1 year of starting alendronic acid but the risk increases progressively with duration of exposure (Schilcher et al. 2011). Following cessation of alendronic acid the risk falls rapidly. The clinical presentation is with a transverse fracture line in the lateral cortex with a medial spike (Fig. 12.3). Focal cortical thickening with a periosteal reaction may be seen in proximity to the transverse fracture line.

Fig. 12.3
Bisphosphonate associated atypical subtrochanteric fracture
Radiograph from a 74 year old women who suffered a spontaneous fracture of the right femoral shaft showing the typical transverse fracture line through the lateral cortex and medial spike. She had been on oral alendronate for 8 years
These fractures occur with minimal or no trauma and may be preceded by thigh pain localised to the affected side. Atypical subtrochanteric fractures are thought to be due to over-suppression of bone resorption with the development of stress fractures in the lateral cortex of the femoral shaft in susceptible individuals (Shane et al. 2014). It has been speculated that certain patients may be genetically predisposed to develop these fractures but the mechanisms that underlie susceptibility remain poorly understood (Shane et al. 2014). Risk factors that have been identified as being associated with atypical subtrochanteric fractures in one or more epidemiological studies include; duration of bisphosphonate treatment; being of Asian ethnicity; glucocorticoid use; active rheumatoid arthritis; prior fragility fracture and low serum 25(OH)D levels (as reviewed by Shane and colleagues (2014)).
Although the risk-benefit balance is overwhelmingly favourable in the vast majority of osteoporotic patients who receive treatment with alendronic acid and other bisphosphonates, the occurrence of this complication emphasises the importance of only giving bisphosphonates to patients with a substantially increased fracture risk (Shane et al. 2014; Abrahamsen 2010).
Risedronate
Risedronate is an aminobisphosphonate which is more potent than alendronate at inhibiting osteoclast activity in vitro but which has lower affinity than alendronate for binding hydroxyapatite (Nancollas et al. 2006). Despite its greater potency, risedronate inhibits bone turnover to a lesser extent than alendronic acid at the dose used clinically, resulting in less marked reductions in bone turnover and smaller increases in BMD (Rosen et al. 2005). Similarly the inhibitory effects of risedronate on bone turnover are of relatively short duration and are lost within about 12 months of stopping therapy (Mortensen et al. 1998). Risedronate is primarily used in the treatment of osteoporosis but is also licensed in several countries for the treatment of Paget’s disease of bone. Risedronate is poorly absorbed from the GI tract and must be taken on an empty stomach as described for alendronic acid. Risedronate is mainly excreted by the kidney and should be used with caution in renal impairment. It is contra-indicated in patients with a GFR below 30 ml/min.
Efficacy
Large-scale randomised trials in women with postmenopausal osteoporosis have shown that oral risedronate 5 mg daily reduces the risk of vertebral, non-vertebral and hip fractures as compared with calcium and vitamin D supplemented placebo in postmenopausal osteoporosis. A meta-analysis of five randomised placebo controlled trials involving 2,620 postmenopausal women with pre-existing vertebral fractures or low BMD on dual energy X-ray absorptiometry (DEXA), showed that the relative risk of vertebral fractures in risedronate treated patients was 0.64 (95 % CI 0.52–0.78) as compared with placebo (Wells et al. 2008b). A further meta-analysis of six trials including 12,309 postmenopausal women showed a relative risk of 0.80 (95 % CI 0.72–0.90) for non-vertebral, non-hip fractures in risedronate-treated patients as compared with placebo. Four studies included in the above meta-analysis had data on hip fractures and in these subjects, the relative risk of hip fracture was 0.74 (95 % CI 0.59–0.94) in risedronate treated patients (Wells et al. 2008b).
A further study was specifically designed to examine the effects of risedronate on hip fracture, in 9,331 elderly postmenopausal women. In this trial, 5,445 subjects were enrolled on the basis that they were aged 70–79 years and had low hip BMD on DXA (T-score <−3.0) whereas the remaining 3,886 subjects were enrolled on the basis that they were aged over 80 years with at least one clinical risk factor for hip fracture. This study showed a significant reduction in hip fracture risk overall (relative risk 0.70 95 % CI 0.60–0.90) but subgroup analysis showed that the risk of hip fracture was statistically significant in patients with low BMD (relative risk 0.60, 95 % CI 0.40–0.90) but not significant in those with clinical risk factors alone (relative risk 0.80, 95 % CI 0.60–1.20).
Risedronate has also been found to be effective at increasing BMD and preventing vertebral fractures in GIOP (Wallach et al. 2000). The effects of risedronate at doses of 2.5 or 5 mg daily in combination with calcium supplements versus placebo were investigated in two parallel trials of similar design involving 518 patients receiving glucocorticoid therapy. About 50 % of participants were female and of these, about 86 % were postmenopausal. One study sought to investigate the effects of risedronate in preventing GIOP (Cohen et al. 1999). In this trial participants had been on 7.5 mg prednisolone daily or more for less than 3 months.
Another study sought to investigate the effects of risedronate in the treatment of GIOP and here, prednisolone had been given in a dose of 7.5 mg daily or more for at least 6 months (Reid et al. 2000). Analysis of pooled data from both trials showed that risedronate was effective at increasing BMD as compared with calcium and vitamin D supplemented placebo in reducing vertebral fractures (relative risk 0.33, 95 % CI 0.13–0.81) but there was no significant reduction in the frequency of non-vertebral fractures (relative risk 1.08, 95 % CI 0.45–2.59) (Wallach et al. 2000). Trials of oral risedronate acid have also been conducted in children with osteogenesis imperfecta. These studies have shown increases in BMD as compared with placebo (Rauch et al. 2009; Bishop et al. 2013), and one study showed a reduction in fracture incidence compared with placebo (Bishop et al. 2013).
Adverse Effects
The adverse event profile of risedronate has been reported to be similar to that of placebo in randomised placebo-controlled trials (Reginster et al. 2000; McClung et al. 2001; Fogelman et al. 2000; Harris et al. 1999; Taggart et al. 2002). However in routine clinical practice, upper gastrointestinal symptoms such as dyspepsia and epigastric pain have emerged as a common adverse effects of risedronate. There are no published data on the frequency with which these adverse effects occur, but the author’s impression is that the incidence is similar to that in alendronic acid treated patients. Having said that, some patients who develop upper GI side effects with alendronate can tolerate risedronate perfectly well. Like other oral bisphosphonates, risedronate should be avoided in patients with dysphagia and other oesophageal disorders that might result in the tablet sticking in the oesophagus.
Other rare adverse events which are thought to be a class effect of bisphosphonates that have emerged from post-marketing surveillance studies include uveitis, osteonecrosis of the jaw (Khosla et al. 2007), atypical subtrochanteric fractures (Schilcher et al. 2011) and bone, joint or muscle pain (Wysowski and Chang 2005; Bock et al. 2007). There is much less information on the relative risk of these events with risedronate as compared with alendronic acid. However in the study of Schilcher, the relative risk of atypical subtrochanteric fractures with risedronate was similar to that of alendronate (Schilcher et al. 2011).
Observational studies have suggested that risedronate may be less likely to cause upper GI adverse effects than alendronate (Ralston et al. 2010) but randomised comparative studies of these two drugs showed no difference in GI side effects (Rosen et al. 2005). There have been fewer reports of ONJ and atypical subtrochanteric fractures in risedronate treated patients as opposed to alendronate treated patents. It has been speculated that this might be due to the fact that at the doses used clinically, risedronate is a less potent inhibitor of bone resorption than alendronate. However another possibility, given that these are rare adverse effects, is that this is simply because risedronate is much less widely used than alendronate.
Ibandronate
Ibandronate is a nitrogen containing bisphosphonate. It is a more potent inhibitor of osteoclast activity in vitro than alendronic acid, but is less potent than risedronate. Its binding affinity for hydroxyapatite is greater than risedronate but less than alendronate. Ibandronate is primarily used in the treatment of osteoporosis but is also licensed in the UK and Europe for the treatment of cancer-associated hypercalcaemia and for the prevention and treatment of metastatic bone disease. Administration instructions for oral ibandronate are similar to those described for alendronic acid. The medication must be taken on an empty stomach and 30 min should be allowed to elapse before taking other medication or food. Like other bisphosphonates ibandronate should be used in caution in patient with renal impairment and it is contraindicated if the GFR is less than 30.
Ibandronate is usually given in a dose of 150 mg once monthly in combination with calcium and vitamin D supplements in the treatment of osteoporosis (Reginster et al. 2005a) but can also be given intravenously in a dose of 3 mg every 3 months (Adami et al. 2004). The intravenous preparation is usually reserved for patients who have difficulty in swallowing tablets or those that experience GI upset with oral bisphosphonates. Most clinicians choose intravenous zoledronic acid over intravenous ibandronate if a parenteral bisphosphonate is required in view of the similar adverse effect profile and more robust data on anti-fracture efficacy (Black et al. 2007).
Efficacy
The pivotal fracture trials with ibandronate were performed with a 2.5 mg daily dose and a rather complicated intermittent dose regimen in which 20 mg was given on alternate days for 12 days every 3 months (Delmas et al. 2004). The study involved 2,946 postmenopausal women with osteoporosis and was placebo controlled. All participants received calcium and vitamin D supplements. Both ibandronate regimens increased BMD, and reduced biochemical markers of bone turnover compared with placebo. The relative risk of vertebral fractures was 0.62 (0.41–0.75) with the 2.5 mg daily regimen and 0.50 (0.26–0.66) with the 20 mg intermittent regimen but there was no significant preventative effect of non-vertebral or hip fractures with either regimen.
A subsequent post hoc analysis of randomised trials of oral and intravenous ibandronate suggested that treated patients may experience a 24 % reduction in the rate of non-vertebral fractures in subjects treated with an annual cumulative ibandronate exposure of ≥10.8 mg (Harris et al. 2008). Although these data raise the possibility that ibandronate might have efficacy for non vertebral fractures, the results have to be treated with caution given the limitations of this type of analysis.
Adverse Effects
Randomised controlled trials of oral ibandronate showed no difference in adverse events compared with placebo (Delmas et al. 2004). The adverse events of oral ibandronate are much less well documented as compared with alendronic acid and risedronate probably because it is used relatively infrequently. However the author’s personal experience with monthly ibandronate indicates that the adverse effects are very similar to those of alendronic acid and risedronate.
Like other amino bisphosphonates, intravenous ibandronate treatment can cause an acute phase response (APR) which presents as a transient flu-like illness, characterised by fever, arthralgia, bone pain and general malaise, lasting for 1–2 days after administration. Experience with other intravenous bisphosphonates such as pamidronate and zoledronic acid indicates that the APR does not recur or is much less prominent after second and subsequent infusions but there is little published data on ibandronate with regard to this issue. Similarly, hypocalcaemia is a potential adverse effect with intravenous ibandronate particularly in patients with vitamin D deficiency but there is little published data on the frequency with which this occurs. In clinical practice it is important to ensure that patients treated with ibandronate have normal vitamin D levels or are on vitamin D supplements at the time of infusion.
There have been few reports of BRONJ and atypical subtrochanteric fractures in osteoporosis patients treated with ibandronate but this may simply be a reflection of the fact that ibandronate is less widely used than alendronic acid and is licensed in fewer countries.
Zoledronic Acid
Zoledronic acid is the most potent licensed bisphosphonate. It is a nitrogen-containing bisphosphonate with high binding affinity for hydroxyapatite. As a result of this it has very powerful inhibitory effects on bone resorption and a long duration of action. Zoledronic acid is licensed for the treatment of osteoporosis, cancer-associated hypercalcaemia, metastatic bone disease and Paget’s disease of bone. It is administered intravenously for all indications. In osteoporosis the dose is 5 mg given intravenously over 15 min every 12 months. In most countries zoledronic acid is given in a day patient setting but it can be given by primary care physicians. Like other bisphosphonates zoledronic acid is excreted by the kidney and should be used in caution in patient with renal impairment. It is contraindicated if the GFR is less than 35.
Efficacy
The pivotal fracture trial (Black et al. 2007) showed that zoledronic acid 5 mg annually for 3 years combined with calcium and vitamin D supplements reduced the risk of vertebral, fractures non-vertebral fractures and hip fractures in patients with osteoporosis as compared with calcium and vitamin D supplemented placebo in women with postmenopausal osteoporosis. This study involved 7,765 postmenopausal women with DEXA proven osteoporosis who were randomised to receive intravenous zoledronic acid or placebo infusions 5 mg every 12 months for 3 years. Both groups received calcium and vitamin D supplements.
When compared with placebo, bone density increased at the spine by about 7 % and at the femoral neck by about 5 % in zoledronic acid treated patients over the 3 year treatment period (p < 0.0001). The relative risk of clinical vertebral fractures was 0.23 (95 % CI 0.14–0.37) in zoledronic acid treated patients when compared with placebo. Corresponding values for non vertebral, non hip fractures were 0.75 (0.64–0.87) and for hip fractures were 0.59 (0.42–0.83) (Black et al. 2007).
While there have been no comparative trials of zoledronic acid with oral bisphosphonates, it is of interest to note that the relative risk reduction of non-vertebral and hip fractures with zoledronic acid is very similar to that observed with alendronic acid and risedronate, whereas the relative risk reduction of vertebral fractures is numerically greater with zoledronic acid. Zoledronic acid is unique in that it has been shown to exert a favourable effect on recurrent fracture and mortality following hip fracture (Lyles et al. 2007). In this study 1,065 patients who had suffered a low trauma hip fracture, who were unable or unwilling to take oral bisphosphonates, were randomised to receive zoledronic acid or placebo infusions. About 75 % of patients were postmenopausal women. Both groups were given vitamin D supplements prior to the first infusion and were subsequently supplemented with calcium and vitamin D during the study. The relative risk of recurrent fractures in the zoledronic acid treated group was 0.65 (0.50–0.84) and the relative risk of death was 0.72 (0.56–0.93) (Lyles et al. 2007).
Subsequent studies showed that the prevention of recurrent fractures explained only 8 % of the effect on mortality and also showed that adjusting for acute medical events eliminated the survival benefit (Colon-Emeric et al. 2010). Zoledronic acid-treated subjects were less likely to die from pneumonia and arrhythmias than placebo treated patients, although the mechanism by which these effects occurred remain unclear since at baseline the treatment groups were well matched for co-morbidities.
Duration of treatment
The duration of action of zoledronic acid on bone density and fractures was investigated in a 3 year extension to the pivotal fracture trial. In this study 1,223 postmenopausal women who had completed 3 years zoledronic acid treatment in the HORIZON study (Black et al. 2007) were randomised to receive a further three infusions resulting in a total duration of 6 years treatment (Z6) (n = 616) or to have placebo infusions (n = 617) for 3 years (Z3P3) (Black et al. 2012).
Bone mineral density values remained relatively stable between years 3 and 6 in the Z6 group but fell by about 1.3 % at the femoral neck and 2 % at the lumbar spine between year 3 and year 6 in the in the Z3P3 group, differences that were significant (p < 0.001). There was no difference in the occurrence of clinical fractures between the groups, but morphometric vertebral fractures were less common in the Z6 group (relative risk 0.51, 95 % CI 0.26–0.95). However, stroke was more common in the Z6 group (3.1 % vs. 1.5 %, p = 0.06). Because of this, and concerns about over suppression of bone turnover with long term zoledronic acid use, many clinicians favour a zoledronic acid regimen of 3 years on and 3 years off therapy.
There is evidence that single infusions of zoledronic acid can exert prolonged inhibitory effects on bone turnover (Grey et al. 2010) and favourably influence the risk of fracture in osteoporosis. Evidence of this comes from a post-hoc analysis of the pivotal fracture trials described previously (Black et al. 2007; Lyles et al. 2007) in which 746 patients who received a single infusion of zoledronic acid were found to have a 32 % reduction in fracture risk (95 % CI 2–53 %) compared with 610 patients who received a placebo infusion. The relative risk reduction with a single infusion was similar to the 34 % reduction (23–43 %) observed in the same studies in patients who had three infusions (Reid et al. 2013). These interesting observations suggest that one zoledronic acid infusion might be enough to reduce the risk of fracture in many patients with osteoporosis in routine clinical practice.
Adverse Effects
The adverse effects of intravenous zoledronic acid are similar to those of other intravenous ibandronate but have been documented in much more detail. The incidence of an APR (transient flu like illness) with zoledronic acid in osteoporosis is about 42 % after the first infusion, falling to 11 % and 7 % after the second and third infusions (Reid et al. 2010). These reactions are more common in younger people, and NSAID users, but less common in smokers and those who have previously received oral bisphosphonates.
Osteonecrosis of the jaw has been extensively studied in relation to the high doses of zoledronic acid used in the treatment of metastatic bone disease. In this situation zoledronic acid is typically given in doses of 4 mg intravenously every 3–4 weeks, resulting in an annual exposure about 10 times higher than in patients with osteoporosis. In the AZURE study of women with breast cancer the incidence of ONJ was 2.7 % (Rathbone et al. 2013) whereas in the MRC XI myeloma study the incidence was somewhat higher at 3.7 % with zoledronic acid as compared with 0.5 % with clodronate (Jackson et al. 2014). In osteoporosis ONJ associated with zoledronic acid treatment is thought to be very rare and in one study the incidence was estimated as less than 1 in 14,200 patient years (Grbic et al. 2010).
There is little information on the risk of atypical subtrochanteric fractures with zoledronic acid but they appear to be rare in that there was no excess of these fractures in the randomised trials of zoledronic acid as compared with placebo (Adachi et al. 2011; Black et al. 2010). Intravenous zoledronic acid has been associated with an increased risk of atrial fibrillation in the pivotal fracture trial discussed previously (Black et al. 2007). In this study, which involved 7,765 postmenopausal women serious atrial fibrillation resulting in admission to hospital was observed in 1.3 % of the zoledronic acid group compared with 0.5 % of the placebo group (p < 0.001). However the overall incidence of atrial fibrillation was similar in both treatment groups (2.4 % vs. 1.9 %) (Black et al. 2007). This adverse effect was not seen in other studies and the mechanism remains unclear.
Role of Bisphosphonates in the Prevention and Treatment of Osteoporosis
Over the past 10 years bisphosphonates have become established as the principle treatment of osteoporosis, due to their relatively low cost, robust anti-fracture efficacy and generally good tolerability and adverse event profile. In contrast, and as discussed elsewhere in this book, the use of hormone replacement therapy (HRT) as a treatment for osteoporosis has declined due to concerns about the increased risk of cardiovascular disease and breast cancer with long term therapy in postmenopausal women (Rossouw et al. 2002).
Comparative studies of bisphosphonates with other agents used in the treatment of osteoporosis are limited in number. Randomised controlled trials have shown that teriparatide (TPTD) is superior to alendronic acid at increasing BMD and reducing the risk of vertebral fractures in GIOP (Saag et al. 2009) and is superior to risedronate in reducing the risk of vertebral fractures in postmenopausal osteoporosis (Hadji et al. 2012). Whilst superiority of teriparatide over bisphosphonates in preventing vertebral fractures has also been observed in observational studies (Oswald et al. 2014), treatment with teriparatide is usually reserved for patients with severe spinal osteoporosis or those in whom the response to bisphosphonates has been inadequate, due to the much greater cost of TPTD and need for daily injections.
There have been no comparative studies of bisphosphonates with other anti-osteoporosis treatments in which fractures have been an endpoint. However, the relative risk reduction in non-vertebral fractures that has been observed with bisphosphonates in placebo controlled randomised trials (~20–25 %) is numerically superior to that observed with strontium ranelate (Reginster et al. 2005b) (~16 %) and is similar to that observed with HRT (~24 %) (Rossouw et al. 2002) and denosumab (~20 %) (Cummings et al. 2009).
Bisphosphonates in Pregnancy and Lactation
Bisphosphonates are contraindicated during pregnancy. Preclinical studies have shown that bisphosphonates cross the placenta and adversely effect development of the fetal skeleton. There are several case reports of patients receiving bisphosphonate therapy during pregnancy however and these have shown no obvious adverse effects on the foetus (Shenker et al. 2010; Levy et al. 2009; Djokanovic et al. 2008; Hellmeyer et al. 2007; O’Sullivan et al. 2006; Ornoy et al. 2006). In one case series, 51 patients were treated with various bisphosphonates before or during pregnancy and this did not seem to affect outcome of the pregnancy or the fetal skeleton (Djokanovic et al. 2008). Similar observations were reported in another case series of 21 patients (Levy et al. 2009).
There is very little information on the use of bisphosphonate therapy during lactation, but one case report of a patient with pregnancy-associated osteoporosis reported no adverse effects on mother or child (Shenker et al. 2010). These observations suggest that there is no major reason for concern if a woman is exposed to bisphosphonate therapy during pregnancy.
Bisphosphonates and Aromatase Inhibitor Induced Bone Loss
The aromatase enzyme is responsible for conversion of adrenal androgens to oestrogen in various tissues including bone (Morishima et al. 1995). Oestrogen produced by this pathway protects against bone loss particularly in postmenopausal women. With the increasing use of aromatase inhibitors such as anastrozole and letrozole as adjuvants treatment for breast cancer, aromatase inhibitor-induced osteoporosis has become an important issue in clinical practice (Reid et al. 2008).
Aromatase inhibitors are now widely used in preference to tamoxifen as an adjuvant treatment of breast cancer following large scale trials which showed advantages in progression free survival (Baum et al. 2002, 2003). Aromatase inhibitor therapy is associated with accelerated bone loss as compared with tamoxifen however, and an increased risk of fractures (Baum et al. 2002; Coleman et al. 2007; Eastell et al. 2006).
The bone loss associated with aromatase inhibitor therapy can be prevented by antiresorptive drugs and the bisphosphonates zoledronic acid and risedronate have both been found to be effective in this situation in randomised placebo controlled studies (Safra et al. 2011; Van Poznak et al. 2010).
On the basis of this, current guidance in the UK suggests that women who are to commence aromatase inhibitor therapy should undergo DEXA scanning and that bisphosphonates and calcium plus vitamin D supplements should be prescribed in those with T-score values of less than −2.0 (Reid et al. 2008). Although there is good evidence to suggest that this approach will prevent bone loss, there is no evidence as yet that it will prevent fractures.
Bisphosphonates and Corticosteroid-Induced Osteoporosis
Bisphosphonates are widely used for the prevention and treatment of corticosteroid induced osteoporosis as discussed previously in this chapter. Randomised controlled trials have shown that alendronic acid (Saag et al. 1998; Adachi et al. 2001), risedronate (Wallach et al. 2000) and etidronate (Adachi et al. 1997) increase BMD and reduce the risk of vertebral fractures when compared with placebo. Zoledronic acid has been shown to be superior to risedronate at increasing BMD in corticosteroid induced osteoporosis, although no difference was seen in fracture occurrence (Reid et al. 2009). The trials of bisphosphonates in corticosteroid-induced osteoporosis have been much smaller than those in postmenopausal osteoporosis and have been designed with changes in BMD as the primary endpoint rather than fracture. Perhaps reflecting this fact, there is no evidence as yet to show that bisphosphonates reduce the risk of non-vertebral fractures in corticosteroid induced osteoporosis.
The indications for treatment in GIOP differ somewhat from postmenopausal osteoporosis. In clinical practice, prophylactic bisphosphonate therapy is usually initiated in patients who are expected to be on corticosteroids in a dose of 7.5 mg daily or more for more than 3 months where BMD T-score values are less than −1.5 at either the spine or hip (Eastell et al. 1998). Although bisphosphonates have positive effects in this situation, comparative studies with alendronic have shown that the bone anabolic agent teriparatide gives a better outcome in terms of BMD and vertebral fractures (Saag et al. 2009). This probably reflects the fact that corticosteroids cause bone loss principally by inhibiting bone formation rather than increasing bone resorption (van Staa 2006). Despite this, bisphosphonates remain the mainstay of prevention and treatment, principally because of the fact that the mode of administration is simpler and they have a much lower acquisition cost.
Conclusions
Bisphosphonates are among the most widely used medicines for the treatment of bone diseases. They share a common core structure but are functionally divided into two groups, based on the presence or absence of nitrogen containing side chains. Nitrogen containing bisphosphonates are highly potent inhibitors of bone resorption and are of clinical value in the treatment of many bone diseases associated with osteoclast activation including osteoporosis, Paget’s disease and cancer-associated bone disease.
Bisphosphonates are generally well tolerated and serious adverse events are rare. Accordingly the overall risk-benefit risk profile for bisphosphonates in the treatment of postmenopausal women with osteoporosis is overwhelmingly favourable. Numerous randomised placebo controlled studies have shown that in patients with low BMD and/or pre-existing vertebral fractures, bisphosphonates reduce the risk of new vertebral fractures by about 50 %; of non vertebral fractures by 20–25 % and of hip fractures by 40 %.
For some patients, the requirement to take oral bisphosphonates on an empty stomach is a limiting factor as are upper gastro-intestinal side effects, but these problems can be circumvented by the use of intravenous bisphosphonates. The emergence of atypical subtrochanteric fractures as an adverse effect of bisphosphonates, emphasises the fact that treatment should be reserved for patients with low BMD who are at increased fracture risk where the benefits are considerable (Shane et al. 2014). However initiation of bisphosphonate therapy as a preventative measure in younger women with osteopenia who are at low risk of fracture now seems inadvisable and in this situation, HRT may prove to be a more favourable option, at least in terms of bone health.
Take Home Messages
· Bisphosphonates are small molecule inhibitors of bone resorption which are of clinical value in the treatment of many diseases associated with increased osteoclast activity
· Bisphosphonates preferentially target to bone and have a prolonged skeletal half life, exerting inhibitory effects on bone resorption for months or years after therapy is stopped.
· Oral bisphosphonates are poorly absorbed from the gastrointestinal tract and they need to be taken on an empty stomach to ensure adequate absorption.
· When administered to patients with osteoporosis, bisphosphonates reduce the risk of non-vertebral and hip fractures by 20–40 % and of vertebral fractures by 50–70 %.
· Upper gastro-intestinal upset is the most common adverse effect with oral bisphosphonates
· With intravenous bisphosphonates the most common adverse event is a transient flu-like illness which is self limiting.
· Other less frequent, but more serious adverse effects include adverse skeletal effects related to over-suppression of bone remodelling, resulting in osteonecrosis of the jaw and atypical subtrochanteric fractures in some patients.
· The benefit risk ratio of bisphosphonates is positive in the vast majority of patients.
References
Abrahamsen B (2010) Adverse effects of bisphosphonates. Calcif Tissue Int 86:421–435PubMedCrossRef
Adachi JD, Bensen WG, Brown J, Hanley D, Hodsman A, Josse R, Kendler DL, Lentle B, Olszynski W, Ste-Marie LG, Tenenhouse A, Chines AA (1997) Intermittent etidronate therapy to prevent corticosteroid- induced osteoporosis. N Engl J Med 337:382–387PubMedCrossRef
Adachi JD, Saag KG, Delmas PD, Liberman UA, Emkey RD, Seeman E, Lane NE, Kaufman JM, Poubelle PE, Hawkins F, Correa-Rotter R, Menkes CJ, Rodriguez-Portales JA, Schnitzer TJ, Block JA, Wing J, McIlwain HH, Westhovens R, Brown J, Melo-Gomes JA, Gruber BL, Yanover MJ, Leite MO, Siminoski KG, Nevitt MC, Sharp JT, Malice MP, Dumortier T, Czachur M, Carofano W, Daifotis A (2001) Two-year effects of alendronate on bone mineral density and vertebral fracture in patients receiving glucocorticoids: a randomized, double-blind, placebo-controlled extension trial. Arthritis Rheum 44:202–211PubMedCrossRef
Adachi JD, Lyles K, Boonen S, Colon-Emeric C, Hyldstrup L, Nordsletten L, Pieper C, Recknor C, Su G, Bucci-Rechtweg C, Magaziner J (2011) Subtrochanteric fractures in bisphosphonate-naive patients: results from the HORIZON-recurrent fracture trial. Calcif Tissue Int 89:427–433PubMedCentralPubMedCrossRef
Adami S, Felsenberg D, Christiansen C, Robinson J, Lorenc RS, Mahoney P, Coutant K, Schimmer RC, Delmas PD (2004) Efficacy and safety of ibandronate given by intravenous injection once every 3 months. Bone 34:881–889PubMedCrossRef
Allen MR, Burr DB (2009) The pathogenesis of bisphosphonate-related osteonecrosis of the jaw: so many hypotheses, so few data. J Oral Maxillofac Surg 67:61–70PubMedCrossRef
Baum M, Budzar AU, Cuzick J, Forbes J, Houghton JH, Klijn JG, Sahmoud T (2002) Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early breast cancer: first results of the ATAC randomised trial. Lancet 359:2131–2139PubMedCrossRef
Baum M, Buzdar A, Cuzick J, Forbes J, Houghton J, Howell A, Sahmoud T (2003) Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of postmenopausal women with early-stage breast cancer: results of the ATAC (Arimidex, Tamoxifen Alone or in Combination) trial efficacy and safety update analyses. Cancer 98:1802–1810PubMedCrossRef
Bishop N, Adami S, Ahmed SF, Anton J, Arundel P, Burren CP, Devogelaer JP, Hangartner T, Hosszu E, Lane JM, Lorenc R, Makitie O, Munns CF, Paredes A, Pavlov H, Plotkin H, Raggio CL, Reyes ML, Schoenau E, Semler O, Sillence DO, Steiner RD (2013) Risedronate in children with osteogenesis imperfecta: a randomised, double-blind, placebo-controlled trial. Lancet 382:1424–1432PubMedCrossRef
Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, Bauer DC, Genant HK, Haskell WL, Marcus R, Ott SM, Torner JC, Quandt SA, Reiss TF, Ensrud KE (1996) Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 348:1535–1541PubMedCrossRef
Black DM, Schwartz AV, Ensrud KE, Cauley JA, Levis S, Quandt SA, Satterfield S, Wallace RB, Bauer DC, Palermo L, Wehren LE, Lombardi A, Santora AC, Cummings SR (2006) Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. JAMA 296:2927–2938PubMedCrossRef
Black DM, Delmas PD, Eastell R, Reid IR, Boonen S, Cauley JA, Cosman F, Lakatos P, Leung PC, Man Z, Mautalen C, Mesenbrink P, Hu H, Caminis J, Tong K, Rosario-Jansen T, Krasnow J, Hue TF, Sellmeyer D, Eriksen EF, Cummings SR (2007) Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med 356:1809–1822PubMedCrossRef
Black DM, Kelly MP, Genant HK, Palermo L, Eastell R, Bucci-Rechtweg C, Cauley J, Leung PC, Boonen S, Santora A, de Papp A, Bauer DC (2010) Bisphosphonates and fractures of the subtrochanteric or diaphyseal femur. N Engl J Med 362:1761–1771PubMedCrossRef
Black DM, Reid IR, Boonen S, Bucci-Rechtweg C, Cauley JA, Cosman F, Cummings SR, Hue TF, Lippuner K, Lakatos P, Leung PC, Man Z, Martinez RL, Tan M, Ruzycky ME, Su G, Eastell R (2012) The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal Fracture Trial (PFT). J Bone Miner Res 27:243–254PubMedCentralPubMedCrossRef
Bock O, Boerst H, Thomasius FE, Degner C, Stephan-Oelkers M, Valentine SM, Felsenberg D (2007) Common musculoskeletal adverse effects of oral treatment with once weekly alendronate and risedronate in patients with osteoporosis and ways for their prevention. J Musculoskelet Neuronal Interact 7:144–148PubMed
Boivin GY, Chavassieux PM, Santora AC, Yates J, Meunier PJ (2000) Alendronate increases bone strength by increasing the mean degree of mineralization of bone tissue in osteoporotic women. Bone 27:687–694PubMedCrossRef
Bone HG, Hosking D, Devogelaer JP, Tucci JR, Emkey RD, Tonino RP, Rodriguez-Portales JA, Downs RW, Gupta J, Santora AC, Liberman UA (2004) Ten years’ experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med 350:1189–1199PubMedCrossRef
Bounameaux HM, Schifferli J, Montani J-P, Jung A, Chatelanat F (1983) Renal failure associated with intravenous diphosphonates. Lancet i:471CrossRef
Boyce BF, Smith L, Fogelman I, Johnston E, Ralston SH, Boyle IT (1984) Focal osteomalacia due to low-dose diphosphonate therapy in Paget’s disease. Lancet 1:821–824PubMedCrossRef
Cohen S, Levy RM, Keller M, Boling E, Emkey RD, Greenwald M, Zizic TM, Wallach S, Sewell KL, Lukert BP, Axelrod DW, Chines AA (1999) Risedronate therapy prevents corticosteroid-induced bone loss: a twelve- month, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum 42:2309–2318PubMedCrossRef
Coleman RE, Banks LM, Girgis SI, Kilburn LS, Vrdoljak E, Fox J, Cawthorn SJ, Patel A, Snowdon CF, Hall E, Bliss JM, Coombes RC (2007) Skeletal effects of exemestane on bone-mineral density, bone biomarkers, and fracture incidence in postmenopausal women with early breast cancer participating in the Intergroup Exemestane Study (IES): a randomised controlled study. Lancet Oncol 8:119–127PubMedCrossRef
Colon-Emeric CS, Mesenbrink P, Lyles KW, Pieper CF, Boonen S, Delmas P, Eriksen EF, Magaziner J (2010) Potential mediators of the mortality reduction with zoledronic acid after hip fracture. J Bone Miner Res 25:91–97PubMedCrossRef
Coxon FP, Helfrich MH, Van’t Hof RJ, Sebti S, Ralston SH, Hamilton A, Rogers MJ (2000) Protein geranylgeranylation is required for osteoclast formation, function, and survival: inhibition by bisphosphonates and GGTI-298. J Bone Miner Res 15:1467–1476PubMedCrossRef
Cummings SR, San Martin J, McClung MR, Siris ES, Eastell R, Reid IR, Delmas P, Zoog HB, Austin M, Wang A, Kutilek S, Adami S, Zanchetta J, Libanati C, Siddhanti S, Christiansen C (2009) Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med 361:756–765PubMedCrossRef
Delmas PD, Recker RR, Chesnut CH III, Skag A, Stakkestad JA, Emkey R, Gilbride J, Schimmer RC, Christiansen C (2004) Daily and intermittent oral ibandronate normalize bone turnover and provide significant reduction in vertebral fracture risk: results from the BONE study. Osteoporos Int 15:792–798PubMedCrossRef
Djokanovic N, Klieger-Grossmann C, Koren G (2008) Does treatment with bisphosphonates endanger the human pregnancy? J Obstet Gynaecol Can 30:1146–1148PubMed
Eastell R, Reid DM, Compston J, Cooper C, Fogelman I, Francis RM, Hosking DJ, Purdie DW, Ralston SH, Reeve J, Russell RG, Stevenson JC, Torgerson DJ (1998) A UK Consensus Group on management of glucocorticoid-induced osteoporosis: an update. J Intern Med 244:271–292PubMedCrossRef
Eastell R, Hannon RA, Cuzick J, Dowsett M, Clack G, Adams JE (2006) Effect of an aromatase inhibitor on bmd and bone turnover markers: 2-year results of the Anastrozole, Tamoxifen, Alone or in Combination (ATAC) trial (18233230). J Bone Miner Res 21:1215–1223PubMedCrossRef
Ebetino FH, Hogan AM, Sun S, Tsoumpra MK, Duan X, Triffitt JT, Kwaasi AA, Dunford JE, Barnett BL, Oppermann U, Lundy MW, Boyde A, Kashemirov BA, McKenna CE, Russell RG (2011) The relationship between the chemistry and biological activity of the bisphosphonates. Bone 49:20–33PubMedCrossRef
Fleisch HA (2000) Bisphosphonates in bone disease: from laboratory to the patient, 4th edn. Academic Press, San Diego
Fleisch H, Russell RGG, Francis MD (1969) Diphosphonates inhibit hydroxyapatite dissolution in vitro and bone resorption in tissue culture and in vivo. Science 165:1262–1264PubMedCrossRef
Flora L, Hassing GS, Cloyd GG, Bevan JA, Parfitt AM, Villanueva AR (1981) The long-term skeletal effects of EHDP in dogs. Metab Bone Dis Relat Res 3:289–300PubMedCrossRef
Fogelman I, Ribot C, Smith R, Ethgen D, Sod E, Reginster JY (2000) Risedronate reverses bone loss in postmenopausal women with low bone mass: results from a multinational, double-blind, placebo-controlled trial. BMD-MN Study Group. J Clin Endocrinol Metab 85:1895–1900PubMed
Francis MD, Russell RGG, Fleisch H (1969) Diphosphonates inhibit formation of calcium phosphate crystals in vitro and pathological calcification in vivo. Science 165:1264–1266PubMedCrossRef
Frith JC, Monkkonen J, Blackburn GM, Russell RG, Rogers MJ (1997) Clodronate and liposome-encapsulated clodronate are metabolized to a toxic ATP analog, adenosine 5′-(beta, gamma-dichloromethylene) triphosphate, by mammalian cells in vitro. J Bone Miner Res 12:1358–1367PubMedCrossRef
Frith JC, Monkkonen J, Auriola S, Monkkonen H, Rogers MJ (2001) The molecular mechanism of action of the antiresorptive and antiinflammatory drug clodronate: evidence for the formation in vivo of a metabolite that inhibits bone resorption and causes osteoclast and macrophage apoptosis. Arthritis Rheum 44:2201–2210PubMedCrossRef
Grbic JT, Black DM, Lyles KW, Reid DM, Orwoll E, McClung M, Bucci-Rechtweg C, Su G (2010) The incidence of osteonecrosis of the jaw in patients receiving 5 milligrams of zoledronic acid: data from the health outcomes and reduced incidence with zoledronic acid once yearly clinical trials program. J Am Dent Assoc 141:1365–1370PubMedCrossRef
Grey A, Bolland M, Wattie D, Horne A, Gamble G, Reid IR (2010) Prolonged antiresorptive activity of zoledronate: a randomized, controlled trial. J Bone Miner Res 25:2251–2255PubMedCrossRef
Hadji P, Zanchetta JR, Russo L, Recknor CP, Saag KG, McKiernan FE, Silverman SL, Alam J, Burge RT, Krege JH, Lakshmanan MC, Masica DN, Mitlak BH, Stock JL (2012) The effect of teriparatide compared with risedronate on reduction of back pain in postmenopausal women with osteoporotic vertebral fractures. Osteoporos Int 23:2141–2150PubMedCrossRef
Harris ST, Watts NB, Genant HK, McKeever CD, Hangartner T, Keller M, Chesnut CH III, Brown J, Eriksen EF, Hoseyni MS, Axelrod DW, Miller PD (1999) Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA 282:1344–1352PubMedCrossRef
Harris ST, Blumentals WA, Miller PD (2008) Ibandronate and the risk of non-vertebral and clinical fractures in women with postmenopausal osteoporosis: results of a meta-analysis of phase III studies. Curr Med Res Opin 24:237–245PubMedCrossRef
Hellmeyer L, Kuhnert M, Ziller V, Schmidt S, Hadji P (2007) The use of i. v. bisphosphonate in pregnancy-associated osteoporosis–case study. Exp Clin Endocrinol Diabetes 115:139–142PubMedCrossRef
Idris AI, Rojas J, Greig IR, van’t Hof RJ, Ralston SH (2008) Aminobisphosphonates cause osteoblast apoptosis and inhibit bone nodule formation in vitro. Calcif Tissue Int 82:191–201PubMedCrossRef
Jackson GH, Morgan GJ, Davies FE, Wu P, Gregory WM, Bell SE, Szubert AJ, Navarro CN, Drayson MT, Owen RG, Feyler S, Ashcroft AJ, Ross FM, Byrne J, Roddie H, Rudin C, Boyd KD, Osborne WL, Cook G, Child JA (2014) Osteonecrosis of the jaw and renal safety in patients with newly diagnosed multiple myeloma: Medical Research Council Myeloma IX Study results. Br J Haematol 166:109–117PubMedCrossRef
Janner M, Muhlbauer RC, Fleisch H (1991) Sodium EDTA enhances intestinal absorption of two bisphosphonates. Calcif Tissue Int 49:280–283PubMedCrossRef
Khosla S, Burr D, Cauley J, Dempster DW, Ebeling PR, Felsenberg D, Gagel RF, Gilsanz V, Guise T, Koka S, McCauley LK, McGowan J, McKee MD, Mohla S, Pendrys DG, Raisz LG, Ruggiero SL, Shafer DM, Shum L, Silverman SL, Van Poznak CH, Watts N, Woo SB, Shane E (2007) Bisphosphonate-associated osteonecrosis of the jaw: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 22:1479–1491PubMedCrossRef
Levy S, Fayez I, Taguchi N, Han JY, Aiello J, Matsui D, Moretti M, Koren G, Ito S (2009) Pregnancy outcome following in utero exposure to bisphosphonates. Bone 44:428–430PubMedCrossRef
Liberman UA, Weiss SR, Broll J, Minne HW, Quan H, Bell NH, Rodriguez-Portales J, Downs RW Jr, Dequeker J, Favus M et al (1995) Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. The Alendronate Phase III Osteoporosis Treatment Study Group. N Engl J Med 333:1437–1443PubMedCrossRef
Luckman SP, Hughes DE, Coxon FP, Graham R, Russell G, Rogers MJ (1998) Nitrogen-containing bisphosphonates inhibit the mevalonate pathway and prevent post-translational prenylation of GTP-binding proteins, including Ras. J Bone Miner Res 13:581–589PubMedCrossRef
Lyles KW, Colon-Emeric CS, Magaziner JS, Adachi JD, Pieper CF, Mautalen C, Hyldstrup L, Recknor C, Nordsletten L, Moore KA, Lavecchia C, Zhang J, Mesenbrink P, Hodgson PK, Abrams K, Orloff JJ, Horowitz Z, Eriksen EF, Boonen S (2007) Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med 357:1799–1809PubMedCrossRef
Mackay FJ, Wilton LV, Pearce GL, Freemantle SN, Mann RD (1998) United Kingdom experience with alendronate and oesophageal reactions. Br J Gen Pract 48:1161–1162PubMedCentralPubMed
McClung MR, Guesens P, Miller PD, Zippel H, Roux C, Roux C, Adami S, Fogelman I, Diamond T, Meunier PJ, Wasnich RD, Greenwald M, Kaufman JM, Chestnut CH III, Reginster JY (2001) Effect of risedronate on the risk of hip fracture in elderly women. N Engl J Med 344:333–340PubMedCrossRef
Morishima A, Grumbach MM, Simpson ER, Fisher C, Qin K (1995) Aromatase deficiency in male and female siblings caused by a novel mutation and the physiological role of estrogens. J Clin Endocrinol Metab 80:3689–3698PubMed
Mortensen L, Charles P, Bekker PJ, Digennaro J, Johnston CC Jr (1998) Risedronate increases bone mass in an early postmenopausal population: two years of treatment plus one year of follow-up. J Clin Endocrinol Metab 83:396–402PubMed
Nancollas GH, Tang R, Phipps RJ, Henneman Z, Gulde S, Wu W, Mangood A, Russell RG, Ebetino FH (2006) Novel insights into actions of bisphosphonates on bone: differences in interactions with hydroxyapatite. Bone 38:617–627PubMedCrossRef
Novince CM, Ward BB, McCauley LK (2009) Osteonecrosis of the jaw: an update and review of recommendations. Cells Tissues Organs 189:275–283PubMedCrossRef
Ornoy A, Wajnberg R, Diav-Citrin O (2006) The outcome of pregnancy following pre-pregnancy or early pregnancy alendronate treatment. Reprod Toxicol 22:578–579PubMedCrossRef
O’Sullivan SM, Grey AB, Singh R, Reid IR (2006) Bisphosphonates in pregnancy and lactation-associated osteoporosis. Osteoporos Int 17:1008–1012PubMedCrossRef
Oswald AJ, Berg J, Milne G, Ralston SH (2014) Teriparatide treatment of severe osteoporosis reduces the risk of vertebral fractures compared with standard care in routine clinical practice. Calcif Tissue Int 94:176–182PubMedCrossRef
Pols HA, Felsenberg D, Hanley DA, Stepan J, Munoz-Torres M, Wilkin TJ, Qin-sheng G, Galich AM, Vandormael K, Yates AJ, Stych B (1999) Multinational, placebo-controlled, randomized trial of the effects of alendronate on bone density and fracture risk in postmenopausal women with low bone mass: results of the FOSIT study. Foxamax International Trial Study Group. Osteoporos Int 9:461–468PubMedCrossRef
Porras AG, Holland SD, Gertz BJ (1999) Pharmacokinetics of alendronate. Clin Pharmacokinet 36:315–328PubMedCrossRef
Ralston SH, Kou TD, Wick-Urban B, Steinbuch M, Masud T (2010) Risk of upper gastrointestinal tract events in risedronate users switched to alendronate. Calcif Tissue Int 87:298–304PubMedCrossRef
Rathbone EJ, Brown JE, Marshall HC, Collinson M, Liversedge V, Murden GA, Cameron D, Bell R, Spensley S, Agrawal R, Jyothirmayi R, Chakraborti P, Yuille F, Coleman RE (2013) Osteonecrosis of the jaw and oral health-related quality of life after adjuvant zoledronic acid: an adjuvant zoledronic acid to reduce recurrence trial subprotocol (BIG01/04). J Clin Oncol 31:2685–2691PubMedCrossRef
Rauch F, Munns CF, Land C, Cheung M, Glorieux FH (2009) Risedronate in the treatment of mild pediatric osteogenesis imperfecta: a randomized placebo-controlled study. J Bone Miner Res 24:1282–1289PubMedCrossRef
Reginster J, Minne HW, Sorensen OH, Hooper M, Roux C, Brandi ML, Lund B, Ethgen D, Pack S, Roumagnac I, Eastell R (2000) Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos Int 11:83–91PubMedCrossRef
Reginster JY, Adami S, Lakatos P, Grennwald M, Stepan JJ, Silverman SL, Christiansen C, Rowell L, Mairon N, Bonvoisin B, Drezner MK, Emkey R, Felsenberg D, Cooper C, Delmas PD, Miller PD (2005a) Efficacy and tolerability of once-monthly oral ibandronate in postmenopausal osteoporosis: 2-year results from the MOBILE study. Ann Rheum Dis 65(5):654–661PubMedCrossRef
Reginster JY, Seeman E, de Vernejoul MC, Adami S, Compston J, Phenekos C, Devogelaer JP, Diaz CM, Sawicki A, Goemaere S, Sorensen OH, Felsenberg D, Meunier PJ (2005b) Strontium ranelate reduces the risk of nonvertebral fractures in postmenopausal women with osteoporosis: TROPOS study. J Clin Endocrinol Metab 90:2816–2822PubMedCrossRef
Reid DM, Hughes RA, Laan RF, Sacco-Gibson NA, Wenderoth DH, Adami S, Eusebio RA, Devogelaer JP (2000) Efficacy and safety of daily risedronate in the treatment of corticosteroid-induced osteoporosis in men and women: a randomized trial. European Corticosteroid-Induced Osteoporosis Treatment Study. J Bone Miner Res 15:1006–1013PubMedCrossRef
Reid DM, Doughty J, Eastell R, Heys SD, Howell A, McCloskey EV, Powles T, Selby P, Coleman RE (2008) Guidance for the management of breast cancer treatment-induced bone loss: a consensus position statement from a UK Expert Group. Cancer Treat Rev 34(Suppl 1):S3–S18PubMedCrossRef
Reid DM, Devogelaer JP, Saag K, Roux C, Lau CS, Reginster JY, Papanastasiou P, Ferreira A, Hartl F, Fashola T, Mesenbrink P, Sambrook PN (2009) Zoledronic acid and risedronate in the prevention and treatment of glucocorticoid-induced osteoporosis (HORIZON): a multicentre, double-blind, double-dummy, randomised controlled trial. Lancet 373:1253–1263PubMedCrossRef
Reid IR, Gamble GD, Mesenbrink P, Lakatos P, Black DM (2010) Characterization of and risk factors for the acute-phase response after zoledronic acid. J Clin Endocrinol Metab 95:4380–4387PubMedCrossRef
Reid IR, Black DM, Eastell R, Bucci-Rechtweg C, Su G, Hue TF, Mesenbrink P, Lyles KW, Boonen S (2013) Reduction in the risk of clinical fractures after a single dose of zoledronic Acid 5 milligrams. J Clin Endocrinol Metab 98:557–563PubMedCrossRef
Rogers MJ, Frith JC, Luckman SP, Coxon FP, Benford HL, Monkkonen J, Auriola S, Chilton KM, Russell RG (1999) Molecular mechanisms of action of bisphosphonates. Bone 24:73S–79SPubMedCrossRef
Rosen CJ, Hochberg MC, Bonnick SL, McClung M, Miller P, Broy S, Kagan R, Chen E, Petruschke RA, Thompson DE, de Papp AE (2005) Treatment with once-weekly alendronate 70 mg compared with once-weekly risedronate 35 mg in women with postmenopausal osteoporosis: a randomized double-blind study. J Bone Miner Res 20:141–151PubMedCrossRef
Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, Jackson RD, Beresford SA, Howard BV, Johnson KC, Kotchen JM, Ockene J; Writing Group for the Women’s Health Initiative Investigators (2002) Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 288:321–333
Russell RG (2011) Bisphosphonates: the first 40 years. Bone 49:2–19PubMedCrossRef
Russell RGG, Muhlbauer RC, Bisaz S, Williams DA, Fleisch H (1970) The influence of pyrophosphate, condensed phosphates, phosphonates and other phosphate compounds on the dissolution of hydroxyapatite in vitro and on bone resorption induced by parathyroid hormone in tissue culture and in thyroparathyroidectomised rats. Calcif Tissue Res 6:183–196PubMedCrossRef
Russell RG, Watts NB, Ebetino FH, Rogers MJ (2008) Mechanisms of action of bisphosphonates: similarities and differences and their potential influence on clinical efficacy. Osteoporos Int 19:733–759PubMedCrossRef
Saag KG, Emkey R, Schnitzer TJ, Brown JP, Hawkins F, Goemaere S, Thamsborg G, Liberman UA, Delmas PD, Malice MP, Czachur M, Daifotis AG (1998) Alendronate for the prevention and treatment of glucocorticoid-induced osteoporosis. Glucocorticoid-Induced Osteoporosis Intervention Study Group. N Engl J Med 339:292–299PubMedCrossRef
Saag KG, Zanchetta JR, Devogelaer JP, Adler RA, Eastell R, See K, Krege JH, Krohn K, Warner MR (2009) Effects of teriparatide versus alendronate for treating glucocorticoid-induced osteoporosis: thirty-six-month results of a randomized, double-blind, controlled trial. Arthritis Rheum 60:3346–3355PubMedCrossRef
Safra T, Bernstein-Molho R, Greenberg J, Pelles-Avraham S, Stephansky I, Sarid D, Inbar MJ, Stemmer SM, Geffen DB (2011) The protective effect of zoledronic acid on bone loss in postmenopausal women with early breast cancer treated with sequential tamoxifen and letrozole: a prospective, randomized, phase II trial. Oncology 81:298–305PubMedCrossRef
Sambrook P, Cooper C (2006) Osteoporosis. Lancet 367:2010–2018PubMedCrossRef
Sansom LN, Necciari J, Thiercelin JF (1995) Human pharmacokinetics of tiludronate. Bone 17:479S–483SPubMedCrossRef
Sato M, Grasser W, Endo N, Akins R, Simmons H, Thompson DD, Golub E, Rodan GA (1991) Bisphosphonate action. Alendronate localization in rat bone and effects on osteoclast ultrastructure. J Clin Invest 88:2095–2105PubMedCentralPubMedCrossRef
Schilcher J, Michaelsson K, Aspenberg P (2011) Bisphosphonate use and atypical fractures of the femoral shaft. N Engl J Med 364:1728–1737PubMedCrossRef
Schnitzer T, Bone HG, Crepaldi G, Adami S, McClung M, Kiel D, Felsenberg D, Recker RR, Tonino RP, Roux C, Pinchera A, Foldes AJ, Greenspan SL, Levine MA, Emkey R, Santora AC, Kaur A, Thompson DE, Yates J, Orloff JJ (2000) Therapeutic equivalence of alendronate 70 mg once-weekly and alendronate 10 mg daily in the treatment of osteoporosis. Alendronate Once-Weekly Study Group. Aging (Milano) 12:1–12
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O’Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP (2014) Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 29:1–23PubMedCrossRef
Shenker NG, Shaikh MF, Jawad AS (2010) Transient osteoporosis associated with pregnancy: use of bisphosphonate in treating a lactating mother. BMJ Case Rep doi:10.1136/bcr.07.2009.2112
Stopeck AT, Lipton A, Body JJ, Steger GG, Tonkin K, de Boer RH, Lichinitser M, Fujiwara Y, Yardley DA, Viniegra M, Fan M, Jiang Q, Dansey R, Jun S, Braun A (2010) Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol 28:5132–5139PubMedCrossRef
Storm T, Thamsborg G, Steiniche T, Genant HK, Sorensen OH (1990) Effect of intermittent cyclical etidronate therapy on bone mass and fracture rate in women with postmenopausal osteoporosis [see comments]. N Engl J Med 322:1265–1271PubMedCrossRef
Taggart H, Bolognese MA, Lindsay R, Ettinger MP, Mulder H, Josse RG, Roberts A, Zippel H, Adami S, Ernst TF, Stevens KP (2002) Upper gastrointestinal tract safety of risedronate: a pooled analysis of 9 clinical trials. Mayo Clin Proc 77:262–270PubMedCrossRef
Van Poznak C, Hannon RA, Mackey JR, Campone M, Apffelstaedt JP, Clack G, Barlow D, Makris A, Eastell R (2010) Prevention of aromatase inhibitor-induced bone loss using risedronate: the SABRE trial. J Clin Oncol 28:967–975PubMedCrossRef
van Staa TP (2006) The pathogenesis, epidemiology and management of glucocorticoid-induced osteoporosis. Calcif Tissue Int 79:129–137PubMedCrossRef
van Staa TP, Abenhaim L, Cooper C (1998) Use of cyclical etidronate and prevention of non-vertebral fractures. Br J Rheumatol 37:87–94PubMedCrossRef
Wallach S, Cohen S, Reid DM, Hughes RA, Hosking DJ, Laan RF, Doherty SM, Maricic M, Rosen C, Brown J, Barton I, Chines AA (2000) Effects of risedronate treatment on bone density and vertebral fracture in patients on corticosteroid therapy. Calcif Tissue Int 67:277–285PubMedCrossRef
Watts NB, Harris ST, Genant HK, Wasnich RD, Miller PD, Jackson RD, Licata AA, Ross P, Woodson GC 3rd, Yanover MJ et al (1990) Intermittent cyclical etidronate treatment of postmenopausal osteoporosis. N Engl J Med 323:73–79PubMedCrossRef
Wells GA, Cranney A, Peterson J, Boucher M, Shea B, Robinson V, Coyle D, Tugwell P (2008a) Alendronate for the primary and secondary prevention of osteoporotic fractures in postmenopausal women. Cochrane Database Syst Rev doi:10.1002/14651858.CD001155.pub2
Wells G, Cranney A, Peterson J, Boucher M, Shea B, Robinson V, Coyle D, Tugwell P (2008b) Risedronate for the primary and secondary prevention of osteoporotic fractures in postmenopausal women. Cochrane Database Syst Rev doi:10.1002/14651858.CD004523.pub3.
Woo SB, Hellstein JW, Kalmar JR (2006) Narrative [corrected] review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med 144:753–761PubMedCrossRef
Wysowski DK, Chang JT (2005) Alendronate and risedronate: reports of severe bone, joint, and muscle pain. Arch Intern Med 165:346–347PubMedCrossRef