Henry L. Galan
John C. Hobbins
Approximately 10% of the almost 4 million infants born each year in the United States are classified as low birth weight (LBW). Terminology used to describe the small fetus/newborn can be confusing. The term LBW is used clinically by pediatricians postnatally and is defined strictly as a birth weight less than 2500g with no regard for gestational age. The term “small for gestational age” (SGA) was originally defined by pediatricians as a newborn with a birth weight less than expected given gestational age and which can occur in a term or a preterm neonate. However, use of the term SGA subsequently expanded from the postnatal period to the antenatal period and is currently used interchangeably with intrauterine growth restriction (IUGR). For the purposes of this chapter, the use of the term SGA will be reserved for the newborn and IUGR, as implied by the name, will be restricted to the fetus. IUGR is more specifically defined later in the chapter. The fetus or newborn classified as IUGR or SGA, respectively, encompasses a group of fetuses-newborns that are small for a variety of reasons with varying prognoses, including congenital infections, congenital malformations, aneuploidy, uteroplacental insufficiency, and constitutionally small. It is important to recognize that not all fetuses or newborns that are classified as IUGR or SGA are small due to pathologic reasons (i.e., constitutionally small), but simply represent the smaller fetuses/newborns at the lower end of the bell-shaped distribution of the normal poulation. The prognosis for a given IUGR fetus is dependent on the etiology. Placental insufficiency accounts for the majority of IUGR fetuses. The scope of the problem with IUGR is quite broad, not just because it increases morbidity and mortality of the fetus, but also because it does so for the newborn and adult the fetus is destined to become. IUGR places the fetus at risk for hypoxemia, acidemia, antepartum death, and intrapartum distress. It places the neonate at risk for a number of metabolic disturbances, polycythemia, pulmonary transition difficulties, intraventricular hemorrhage, impaired cognitive function, and cerebral palsy. Several epidemiologic studies and animal studies in the early 1990s began to report on long-term sequelae of IUGR including adult hypertension, heart disease, stroke, and diabetes. The theory of fetal programming as the origin of adult disease was introduced by Barker and colleagues and is commonly referred to as the “Barker hypothesis.” The challenge in management of the IUGR fetus is to identify the condition and manage it such that adverse sequelae are minimized. The use of real-time ultrasound and Doppler velocimetry play pivotal roles in the diagnosis and management of IUGR. This chapter reviews normal placental–fetal growth, etiologies of the IUGR fetus, and practical uses of ultrasound and Doppler velocimetry in the diagnosis and management of the IUGR fetus.
DETERMINANTS OF NORMAL AND ABERRANT PLACENTAL GROWTH
Normal Placental Development
In most mammalian species, the placental and fetal mass increase exponentially for at least a portion of pregnancy. Normal growth of the fetus is in turn dependent on normal placentation and growth of the placenta. The placenta is a dynamic and multifaceted organ that serves as an interface between mother and fetus with the critical role of meeting the metabolic and circulatory demands of the growing fetus. The roles of the placenta include:
· Nutritional: Provides oxygen, glucose, amino acid, and volume (fluid) transfer.
· Immunologic: Protects the fetus from pathogens and the maternal immune system.
· Endocrinologic: Produces numerous hormones, growth factors, cytokines, and other vasoactive mediators.
· Metabolic: Serves as the respiratory and the kidney organ for the fetus and is responsible for elimination of carbon dioxide, metabolic acids, and other waste products from the fetus to maintain acid–base balance.
Placentation must be normal in order for these functions to be met.
Research has begun to provide an understanding of the complexity of the implantation and placentation processes, which requires production and coordination of numerous angiogenic growth factors (fibroblast growth factor, hepatocyte growth factor, placental growth factor, vascular endothelial growth factor), cell-adhesion molecules, cytokines, nitric oxide, extracellular matrix metalloproteinases, hormones, and transcription factors (hypoxia inducible factor). This process of coordination begins very early in pregnancy and can dictate whether the pregnancy grows in a normal or abnormal direction. During the luteal phase of the menstrual cycle, the endometrium becomes decidualized in preparation for acceptance of the products of conception. Shortly after entering the uterine cavity on day 4 postconception, the morula becomes a blastocyst with an inner cell mass at one pole that is called the embryoblast and an outer cell mass that is called the trophoblast. On day 7 postconception, the trophoblast differentiates into the cytotrophoblast, which envelops the blastocyst circumferentially. Simultaneously, the newly developed cytotrophoblast cells further differentiate into a sheet of syncytiotrophoblast cells. The syncytiotrophoblast produces proteins and steroid hormones. The cytotrophoblast, made up of nucleated cells, continues to produce the anucleate syncytiotrophoblast throughout gestation primarily by mitotic activity and loss of cytotrophoblastic cell walls. By day 13, the cytotrophoblast layer has differentiated into invasive and noninvasive cytotrophoblast. The invasive cytotrophoblast forms invasive cell columns that invade the uterine epithelium to anchor the fetus and establish blood flow to the placenta and fetus. During this process, the invasive cytotrophoblast cells (extravillous trophoblast):
· migrate through the syncytiotrophoblast and into the decidualized endometrium and myometrium
· invade the vessel walls of the maternal-based spiral arteries in these areas
· transform the spiral arteries from a high-resistance to a low-resistance vessel.
As the invasive cell columns of the cytotrophoblast penetrate the syncytiotrophoblast, spaces called lacunae are created, which subsequently fuse to form the intervillous space with intervening syncytiotrophoblast columns called trabeculae. The process of intervillous space formation and spiral artery transformation directs an increasing maternal cardiac output into the intervillous space. Loss of spiral artery vessel media is the mechanism by which the spiral arteries drop their resistance to blood flow. The syncytiotrophoblast-based trabeculae branch laterally to initiate placental villi formation on approximately day 13. The extent of vascularization of the villus architecture defines the villus as stem or primary villus, secondary villus. or tertiary villus. The stem villus is without vessels and only has trophoblast cells. The secondary villus is formed by central invasion of the primary villous core by the allantoic mesenchyme of the embryoblast. The tertiary villus forms during vasculogenesis, which is the development of de novo blood vessels from mesenchymal cells differentiating into hemangioblasts. Hemangioblasts are precursors of endothelial cells. This process begins in the 5th week of gestation.
Each cotyledon, labeled by some as a fetal unit, is characterized by a villous tree that contains three basic types of villi:
1. stem villi
2. intermediate villi
3. terminal villi.
These three villous types represent progressively smaller generations of villous branching with the terminal villi serving as the end point. The stem villi extend from the chorionic plate to the basal plate. The stem villi contain a single truncus that progressively branches into the rami chorii, which in turn branches into the ramuli chorii. It is from the ramuli chorii that the intermediate villi appear of which there are two types: The immature and mature intermediate villi. The terminal villi are the primary gas exchanging villi, which have actually been identified at all levels of branching. They account for 55% of the total number of cross-sectional villi in the peripheral villous tree. Smooth muscle staining shows that vessels coursing through the villi contain smooth muscle media down to the level of the immature villi. This distinguishes the stem and immature villi from the gas-exchanging mature and terminal villi. It has been noted that the intermediate villi, because of the smaller arterioles, venules, pre- and postcapillaries contained within, may serve a hemodynamic regulatory function (i.e., control of blood pressure and flow). The concept of blood flow control at this level is further supported by previously described sphincterlike precapillary structures.
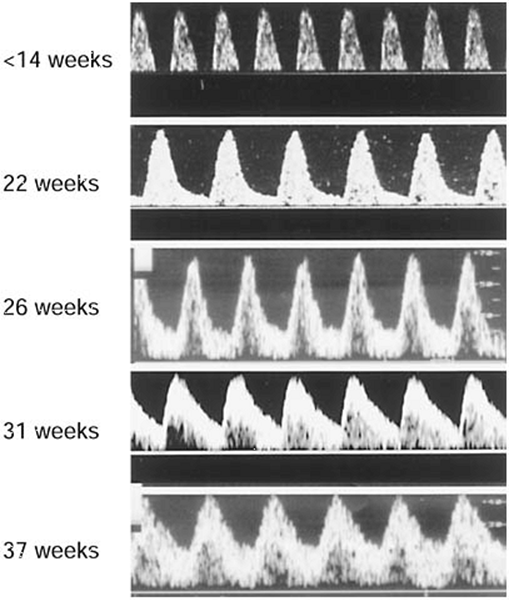
In contrast to vasculogenesis, angiogenesis represents the formation of new blood vessels from endothelial cells and is classified into branching and nonbranching angiogenesis. Branching angiogenesis occurs primarily in the first and second trimesters and leads to the formation of the immature villous tree. Branching angiogenesis continues until the end of the second trimester when there is a transition to nonbranching angiogenesis. During this process there is a dramatic increase in mature intermediate and terminal villi. The nonbranching angiogenesis forms terminal capillary loops with minimal branching and provides the network of capillaries for the intermediate and terminal villi. A dramatic decrease in vascular resistance and an increase in blood flow through the placenta are coincident with this process. The progressive decline in vascular resistance is depicted by increased end-diastolic velocities in Doppler flow velocity waveforms of the umbilical artery (Fig. 12.1).
|
|
|
FIG. 12.1. Doppler flow velocity waveform profiles in the umbilical artery across normal gestation. Note the progressive increase in end-diastolic flow. |
Abnormal Placental Development
In pregnancies complicated by preeclampsia and IUGR, trophoblast invasion is limited to the decidualized endometrium, which results in failure of the spiral arteries to become low resistance vessels. The inability of spiral arteries to transition from high to low blood flow resistance can be detected by Doppler velocimetry of the uterine artery which supplies blood to the spiral arteries. The blood flow velocity waveforms in the uterine artery obtained with pulsed-wave Doppler velocimetry are reflective of the waveforms downstream at the spiral arteries. These abnormalities are identified on a Doppler flow velocity waveform (FVW) profile by a high resistance pattern (low velocity of flow at end-diastole relative to that at systole) and by a protodiastolic (early diastolic) notch. Failure of this process to occur on the maternal side of the circulation may lead to adverse effects on both the mother and the fetus. Maternal vascular endothelial dysfunction may lead to production of a variety of vasoactive mediators, which could subsequently lead to the development of preeclampsia. Poor growth of the placental–fetal unit may also result from poor invasion and remodeling of the spiral arteries by the cytotrophoblast.
A variety of villous and vascular abnormalities have been described in the placenta of the IUGR fetus. Placentas from IUGR pregnancies have fewer gas-exchanging villi. The gas-exchanging villi are also slender, elongated, poorly branched, and poorly capillarized. Vascular abnormalities include reduced branching of stem arteries and disorganized vascular patterns including less coiling as depicted by placental vascular cast studies. There are also fewer terminal villi with smaller lumens. The reduced branching seen in the villous vasculature creates abnormal blood flow and an increase in vascular resistance to flow that can be likened to that of an electric circuit—the fewer downstream tributaries that exist from the main supply line, the higher the resistance.
DETERMINANTS OF NORMAL AND ABERRANT FETAL GROWTH
Normal Fetal Growth
In order for a fetus to grow normally, the placental developmental activities described earlier must proceed undisturbed. At 37 weeks gestation, the placenta has reached maximal surface area (11 m2) and weighs approximately 500 g. Coincident with this is maximal amniotic fluid volume and maximal human placental lactogen levels, suggesting peak placental function. Fetal growth velocity also curtails at this juncture in pregnancy. Interestingly, although the fetus grows less quickly, calorie acquisition by the fetus continues to be quite high. At this time in pregnancy, the fetus is rapidly accumulating fat which provides thermal stability for the immediate postnatal period. Fat has a high caloric content (9 calories/g) compared to carbohydrates and proteins (4 calories/g). The high metabolic demands of the fetus result in a fetal temperature that is 0.5°C above that of the mother. This difference in temperature is seen in the maternal immediate postpartum shivering, which reflects a compensatory response to the loss of fetal-derived heat.
For the fetus to achieve maximal growth potential, the uterine–placental–fetal circulation must be normal in order for the fetus to receive a variety of necessary substrates. A key feature of the uterine vascular bed in pregnancy is the lack of responsiveness to changes in blood gas tensions (PO2, PCO2). Thus, oxygen therapy for either maternal disease or for fetal benefit will not cause vasoconstriction. In contrast, the lack of responsiveness and lack of autoregulation in the uterine vascular bed renders these vessels incapable of compensating for maternal hypotension. Animal studies have shown that the volume blood flows (mL/min) in the uterine and umbilical circulations are unaffected by maternal hyperoxygenation. This is important clinically since the improvement in fetal PO2 by maternal oxygen therapy does not appear to have an adverse affect on fetal blood flow.
Glucose, oxygen, and amino acids are the major substrates needed for normal fetal growth. Glucose freely crosses the placenta by facilitated diffusion into the fetus. The maternal–fetal glucose concentration gradient that exists widens with advancing gestational age in order to accommodate the increasing metabolic demands of the fetus. Under normal circumstances, glucose is metabolized by the fetus to produce energy in the form of adenosine triphosphate (ATP) in the presence of oxygen. Oxygen passes across the placenta to the fetus by simple diffusion and is regulated by concentration gradients and uterine blood flow as described by the Fick principle. Transplacental transport of all essential and nonessential amino acids occurs by active transport. Animal and human studies have confirmed that amino acid carrier systems are present on both the maternal and fetal sides of the placenta. The placenta is quite active in amino acid metabolism contributing significantly to net umbilical–fetus uptake of certain amino acids.
Abnormal Fetal Growth
Failure of the placenta to deliver these primary substrates to the fetus will result in diminished protein production by the fetus, reduced glucose metabolism, and reduced glycogen deposition in the liver. If oxygen supply is markedly reduced either from an acute or chronic insult, the fetus will convert from an aerobic to an anaerobic metabolic state in order to meet energy (ATP) requirements. Anaerobic metabolism is far less efficient at producing ATP from a given unit of glucose compared to aerobic metabolism. Furthermore, anaerobic activity will produce “fixed” acids (lactate, urate, etc.), which diffuse slowly across the placenta thus accumulating in the fetal system. If the anaerobic process is not reversed, the accumulation of acids will consume available buffers, and the fetal blood pH will fall, leading to an acidemic and acidotic fetus.
The IUGR fetus attempts to compensate for reduced substrate delivery by different mechanisms. From a metabolic standpoint, the fetus changes the maternal–fetal glucose gradient. The normally wide glucose gradient that exists between the mother and fetus, which is needed for movement of glucose to the fetus, widens further. This compensatory mechanism enhances glucose movement across the placenta to the fetus. The smaller abdominal circumference noted in the IUGR fetus is a result of less hepatic glycogen formation in order to maximize glucose availability. In a similar fashion to the liver, fat stores, which are normally an important depot site for fat-soluble vitamins and fatty acids, are reduced. This change in body composition is reflected in the ponderal index, which neonatologists use as an index of “scrawniness.” The fetus also adjusts to reduced nutrient delivery by redistributing systemic blood flow to vital organs. The fetus will reduce flow to nonvital organs by reducing vascular resistance and increasing blood flow to the brain which normally has a relatively high vascular resistance pattern compared to other organ systems. This can be demonstrated with pulsed-wave Doppler velocimetry of the middle cerebral artery (MCA) in which the flow velocity profile shows an increase in end-diastolic velocity. Other organs being “spared” through vascular redistribution include the heart and adrenal glands. Redistribution of blood flow to vital organs in experimental animal models of hypoxemia or infusion of angiotensin II into the sheep fetus mimic the hemodynamic alterations observed in the human IUGR fetus.
DEFINITION OF IUGR
A number of definitions of IUGR have been proposed based on percentile, standard deviation, or growth rate. The most commonly used clinical definition of IUGR is an estimated fetal weight (EFW) less than the tenth percentile as determined by ultrasound. This mirrors the definition of SGA, which was originally described by Battaglia and Lubchenco in 1967 as a birth weight less than the 10th percentile for gestational age. They noted that SGA infants were at increased risk for neonatal death. The problem with the tenth percentile as a cutoff for the diagnosis of IUGR is that a number of fetuses with an EFW below that value will be normally small, otherwise referred to as “constitutionally” small and not at risk. Studies have demonstrated that if determinants of birth weight, such as maternal ethnicity, parity, maternal weight and height are considered, up to 50% of fetuses less than the tenth percentile will be constitutionally small. This has been the basis for using other definitions including less than the third or fifth percentile or less than 2 SDs from the mean. Some authors have suggested using an abdominal circumference (AC) of less than 2 SDs for gestational age. The AC measurement represents a single objective ultrasound measurement rather than combining several fetal biometric ultrasound parameters into a formula where each parameter is weighted differently.
While it seems that an EFW less than the tenth percentile is not a sufficiently strict definition of IUGR, there is also a significant problem associated with the use of more strict criteria. If a definition of less than the third percentile is used, there is a reasonable chance that one could miss some fetuses that do not meet their growth potential and could be at risk for adverse events. We believe that the fetus genetically programmed to be born at the 90th percentile that is born at the 20th percentile may be in more trouble than the baby born to a jockey and a gymnast who is at the 8th percentile. The bottom line is that no receiver operator curves have been established to assess sensitivity and specificity in order to establish a “cutoff” for the diagnosis of IUGR. This has been quite difficult to do, in part because of a wide biologic variation between patients and because of a wide variation of parameters used to diagnose IUGR (EFW, AC < 2SD, etc.). Customized growth curves, such as those envisioned and created by Gardosi that include variables that impact fetal size, may be the answer to establishing a better cutoff value for IUGR. Until such standards become published and available, the use of tools such as pulsed-Doppler velocimetry to investigate the status of the fetal circulation will help identify an IUGR pregnancy that is secondary to uteroplacental insufficiency and potentially at risk of perinatal morbidity and mortality. Doppler velocimetry is discussed in detail later in the chapter.
ETIOLOGY OF IUGR
The type and timing of insult during fetal development will dictate the subsequent development and morphology of the fetus. Fetal growth in the first trimester is characterized primarily by an increase in cell number or hyperplasia. In the second trimester, growth is a combination of hyperplasia and hypertrophy of preexisting cells. The third trimester is characterized primarily by hypertrophy. If an insult occurs in the first half of pregnancy where hyperplasia predominates, all fetal cell numbers can be reduced and lead to a small fetus that is symmetrically proportioned. That is, somatic and cerebral growth will both be similarly reduced. The underlying etiology of symmetric IUGR varies widely and includes: Karyotypic abnormalities, congenital anomalies, or congenital infections. Maternal medical illness, obstetric conditions, or primary placental pathology place the fetus at risk for uteroplacental insufficiency that may lead to a small fetus, which is asymmetrically proportioned. If these types of insults occur sufficiently early enough in pregnancy, there can be an impact on hyperplasia of cells and a symmetric growth pattern. More commonly, there is an impact upon hypertrophy that occurs late in pregnancy and primarily affects fat and hepatic glycogen deposition. The reduction in hepatic glycogen stores reduces liver size and results in an increase in the head-to-liver ratio, which defines asymmetric growth. Asymmetric growth is also characterized by a redistribution of fetal cardiac output to vital organs including the brain, heart, and adrenal glands. The redistribution of blood flow to the head allows the fetal head and brain to be preserved and maintain a normal growth velocity compared to parameters of somatic growth (abdomen and extremities). This is the basis for the common phrase, “brain-sparing”. Thus, the relative proportions of fetal dimensions can provide some insight to the etiology of IUGR based on the symmetric or asymmetric nature of the ultrasound parameters.
DIAGNOSIS OF IUGR
Dating the Pregnancy
Studies in the past decade have clarified the associations of IUGR and long-term health hazards by confirming good gestational age dating. The use of actual gestational dating rather than birth weight alone is critical since it more clearly establishes that the link of cardiovascular disease and diabetes with IUGR status at birth is not due to prematurity, but to true intrauterine growth restriction. Establishing the most accurate gestational age is probably the single most important service we provide the pregnant patient since every test or intervention performed during pregnancy is dictated by the gestational age of the patient.
The diagnosis of IUGR begins with accurate dating of the pregnancy, which in turn begins with the establishment of the estimated date of confinement (EDC) based on information gathered on the last menstrual period (LMP). Normal human gestation lasts 280 days from the LMP, and it is this time frame that “pregnancy wheels,” commonly used to determine estimated gestational age and date of confinement, are based upon. The 280-day gestation is, in turn, based upon a normal menstrual cycle length of 28 days. However, a portion of patients will have menstrual cycle lengths that vary from 21 to 35 days, which will shorten or lengthen the gestational dating, respectively. Therefore, the EDC should be adjusted accordingly. Other important questions regarding the LMP include regularity, certainty (calendar recorded, etc.), date of conception, and oral contraceptive use at the time of the LMP. It has been previously reported that the LMP is unreliable up to one-third of the time, and it is in these circumstances that ultrasound becomes a valuable resource.
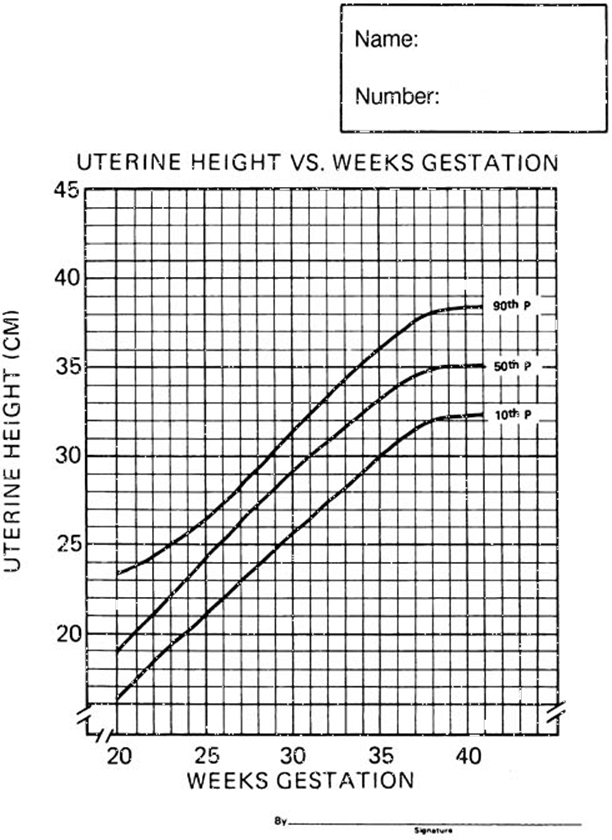
After establishment of gestational age by LMP and/or ultrasound, clinical acumen can lead to a presumptive diagnosis of IUGR. The most commonly used clinical tool for assessing growth of the pregnancy is serial measurement of uterine fundal height during regular clinic visits. Measurement of uterine fundal height (cm) from the symphysis across the uterus to the top of the fundus provides an index of growth for which a nomogram has been reported (Fig. 12.2). In general, the uterine fundus will be within 2 cm of the gestational age in weeks. This simple screening technique has been reported to be 75% accurate in diagnosing IUGR. However, the measurement may be erroneous because of several variables that impact uterine size, including interobserver variation, obesity, uterine fibroids, multiple gestation, polyhydramnios, and so forth.
|
|
|
FIG. 12.2. Uterine fundal height chart for the diagnosis of fetal growth restriction. |
Ultrasound
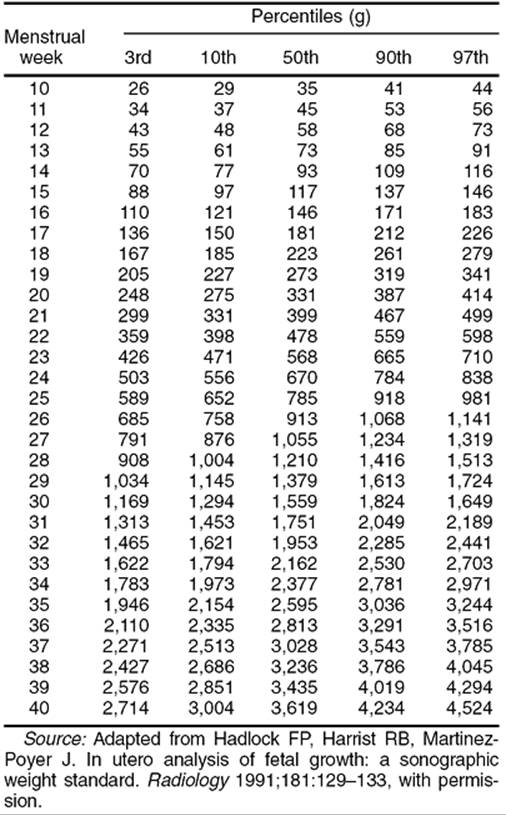
While LMP dating and clinical acumen are important in screening for IUGR, ultrasound remains the cornerstone for the diagnosis and management of this condition. The diagnosis of IUGR is made by combining ultrasound biometric measurements of the fetus into a formula that calculates the estimated fetal weight (EFW). The most commonly measured fetal biometric parameters include the biparietal diameter (BPD), the head circumference (HC), the abdominal circumference (AC), and the femur length (FL). As described earlier, IUGR is diagnosed when the EFW falls below the tenth percentile for gestational age. If available, it is important to use local standards for the diagnosis since it has been previously shown that tenth percentile for EFW can vary depending on the population studied. Goldenberg and colleagues have shown that growth charts can differ dramatically among different patient populations. For example, a fetal weight nomogram constructed by ultrasound in Colorado suggests that consistently, across gestational ages, fetuses in Denver are lighter than fetuses at sea level. The Shepard and Hadlock formulas are the most commonly used formulas for calculating EFW. Table 12.1 shows the estimated fetal weight using Hadlock's formula plotted across gestation. In general, the more parameters included, the more accurate the EFW (Hadlock: 4 parameters; Shepard: 3 parameters). However, as you increase the number of parameters in the formula above, EFW begins to lose accuracy because of the standard error of the method associated with the measuring of each parameter. Using the Shepard formula, a practitioner will obtain an EFW that will fall within 5% of the true weight 50% of the time and within 10% of the weight 80% of the time.
|
|
|
TABLE 12.1. In utero fetal weight standards at ultrasound |
A commonly encountered clinical scenario is the patient who is sent for evaluation of suspected IUGR in whom the clinical dating criteria are poor and gestational age unknown. For example, a fetus measuring 3 to 4 weeks less than expected may be the result of any of the following three possibilities:
1. The patient is 3 to 4 weeks off on clinical dating.
2. The fetus is truly 3 to 4 weeks less than clinical dating, but is genetically predisposed to be small.
3. The fetus is small, growth-restricted, and at risk.
Several ultrasound strategies are available to address this problem and to categorize the fetus into one of the categories. The ultrasound biometric parameters can be used to calculate ratios and provide some insight into the severity of the IUGR. In the 1970s, Campbell and Thoms first described the HC/AC ratio. In approximately 60% of cases with IUGR, the HC/AC ratio is in the 90th percentile for gestational age, which suggests a “brain-sparing” process. The FL/AC ratio provides information on the amount of muscle and fat mass present on the fetus providing a picture of the “scrawniness” of the fetus. This is analogous to the ponderal index used by neonatologists. Unlike the HC/AC ratio, the FL/AC ratio is gestational-age independent and may be useful when the gestational age is unknown. Other aspects of the fetus that appear to be relatively independent of the IUGR process and that remain consistent throughout gestation include the transcerebellar diameter (TCD), foot length, and epiphyseal centers. These are other strategic tools to help approximate the gestational age when dating criteria are poor.
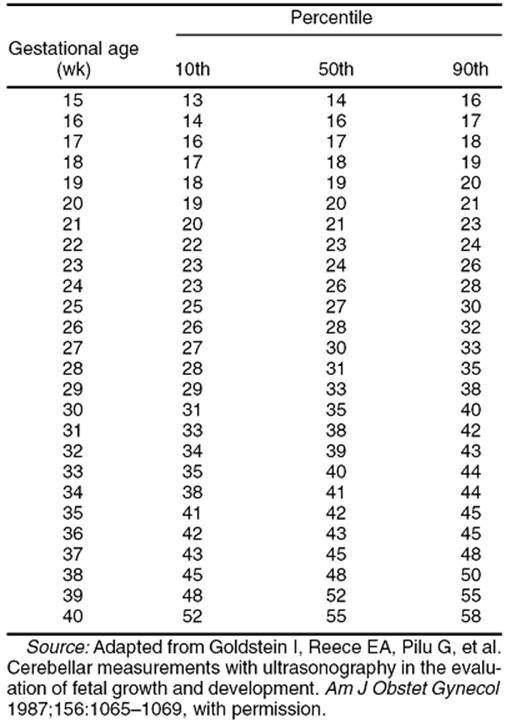
The TCD measured in centimeters mirrors the gestational age until about 22 weeks and then accelerates. Cerebellar measurements are shown in Table 12.2. While original studies by Reece and co-workers showed that the TCD is “spared” in IUGR, one study suggests that only 40% of IUGR fetuses demonstrated the sparing effect. However, the etiologies for IUGR in this study were not clearly identified. If the gestational age by TCD is greater than that suggested by other biometric parameters and is consistent with the unsure LMP dating criteria, it may be that the fetus is indeed further along and possibly growth restricted. In a similar fashion, Hadlock and colleagues showed that the foot length is gestational-age independent and may be useful in IUGR. Although not useful for estimating gestational age in the second and early third trimester, the appearance of epiphyseal centers of the long bones on ultrasound provides reassurance that the fetus is in the second half of the third trimester of gestation. In a nondiabetic population, the presence of a distal femoral epiphysis of greater than 3 mm and the presence of any proximal tibial epiphysis indicated a mature lung profile in almost all cases. The proximal tibial epiphysis is not typically present prior to 36 weeks gestation. Additionally, the proximal humeral epiphysis rarely appears prior to 38 weeks gestation. Unpublished information suggests that appearance of the epiphyseal centers in IUGR fetuses may be delayed. This should be taken in the context that it is the presence of the tibial and humeral epiphyseal centers that are useful markers of pulmonic maturity, while the absence of these centers may suggest a more immature fetus.
|
|
|
TABLE 12.2. A nomogram of the transverse cerebellar diameter (mm) |
Serial ultrasound measurements of fetal biometry and estimated fetal weight are also useful in assessing the growth-restricted fetus. The fetus that demonstrates appropriate growth, that is, continued growth along nomograms, probably represents a fetus genetically predisposed to being small and one that is likely not at immediate risk. A couple of problems of relying on growth potential alone is that it does not tell you where in gestation the fetus is or how the fetus is doing at the first evaluation. As with all these biometric tools, it is best to look at the big picture and formulate an opinion based on all information that one can obtain with the ultrasound. Another tool that can be used to categorize a small fetus is pulsed-wave Doppler velocimetry. This ultrasound modality, which has revolutionized the management of the IUGR fetus, can also be used to help delineate whether a fetus is “normal” small or “abnormal” small based on the umbilical FVW.
DOPPLER VELOCIMETRY IN THE ASSESSMENT OF IUGR
Doppler Ultrasound
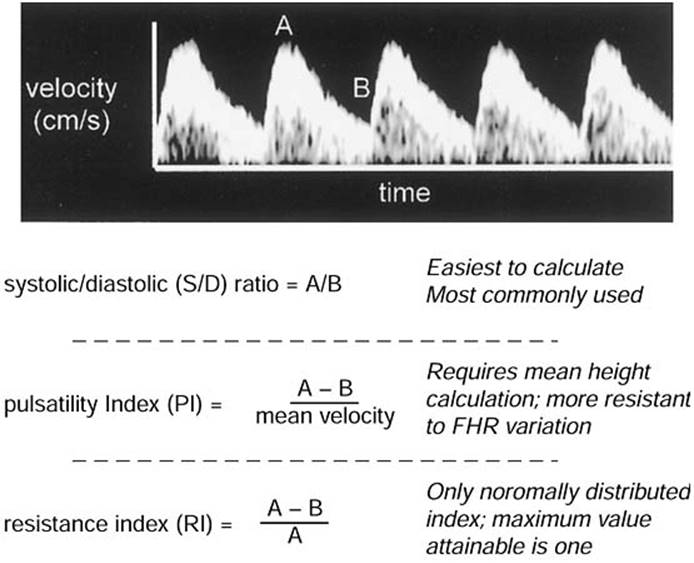
The concept of Doppler, which is used in ultrasound, is named after Johann Christian Doppler. The Doppler concept refers to energy that is reflected from a moving boundary, and how the frequency of the reflected energy varies in relation to the moving boundary. In ultrasound terms, Doppler depends on the ability of an ultrasound beam to be changed in frequency when encountering a moving object (red blood cells). After cosmetic manipulation, a waveform is generated that has a clear systolic and diastolic component. Although resistance to blood flow in a given interrogated vessel in the fetus cannot be directly measured, it is possible from the waveform to obtain an index of resistance. Figure 12.3 shows a FVW in the umbilical artery with clear systolic and diastolic cardiac components. Using the peak systolic and peak diastolic values, it is possible to generate Doppler indices of resistances. These include the systolic-to-diastolic (S/D) ratio, pulsatility index, and resistance index. Because these three indices are functions of the same variables, they are correlated highly with one another. The characteristics of these indices are also shown in Figure 12.3. The original continuous-wave Doppler technology has been replaced by pulsed-wave Doppler technology. Doppler velocimetry is useful in cases where the fetus is asymmetrically grown due to a uteroplacental etiology.
|
|
|
FIG. 12.3. Umbilical artery Doppler flow velocity waveform demonstrating peak systolic (A) and peak end-diastolic (B) velocities. Doppler indices are defined below. |
Over the past decade, numerous centers across the United States and in Europe have shed light on circulatory physiology in the normal and growth-restricted fetus. This has been approached by assessing FVWs in a number of different vessels in the fetus. While these reports provide useful information on any given vessel, reports on one or two vessels alone are not practical from the clinical standpoint since these were primarily cross-sectional studies and did not provide any information on the temporal nature of Doppler changes. After the turn of the 21st century, three reports appeared in the literature that combined longitudinal information on several different vessels with biophysical data obtained from the IUGR fetus. These studies showed that there are sequential changes in Doppler FVW-resistance measurements in different vessels of the severely growth-restricted fetus that is progressively deteriorating.
Normal Fetal Circulation
The umbilical vein leaves the placenta and enters the umbilicus with oxygen and nutrient-rich blood and volume, which are necessary for normal development of the fetus. The venous vasculature of the liver consists of the umbilical and portal veins, hepatic veins, and the ductus venosus. The umbilical vein turns acutely cephalad as it passes through the umbilicus and in the inferior portion of the falciform ligament. The hepatic portion of the umbilical vein then travels horizontally and posteriorly, and bends to the right where it joins the transverse part of the left portal vein. These then join the right portal vein, which branches anteriorly and posteriorly. As the hepatic portion of the umbilical vein bends to the right, the ductus venosus emanates, heading in a posterior and cephalad direction and joins the inferior vena cava (IVC) just below the diaphragm. The three hepatic veins (right, middle, and left) fuse and join at the juncture of the ductus venosus and IVC confluence. The ductus can be visualized easily on both axial and midline sagittal views of the fetus with the use of color velocimetry. Its detection can be enhanced by adjusting the velocity scale and looking for aliasing of the color that indicates the area of highest flow velocity. The ductus venosus plays a critical role in shunting the most oxygenated and nutrient-rich blood from the hepatic portion of the umbilical vein to the right atrium. More than half of the umbilical vein blood enters the ductus venosus. Portal blood primarily travels to the right lobe of the liver and, as a result, 98% of the blood passing through the ductus venosus comes from the umbilical vein. Some of the blood supply to the left lobe of the liver comes from branches of the umbilical vein, which increases blood oxygen levels in the left hepatic vein compared to the right. Preferential streaming is a phenomenon that occurs within precordial venous structures and the heart to ensure delivery of the most nutrient-rich blood to the left side of the heart. Briefly, nutrient-rich blood within the ductus and left hepatic vein course preferentially through the posterior and left portions of the column of blood in the thoracic IVC. Blood that is deoxygenated and contains waste products from the abdominal IVC and the right hepatic vein streams, preferentially, along the anterior and right portions of the column of blood in the thoracic IVC. Blood from the superior vena cava joins the blood traveling anteriorly and rightward, enters the right atrium across the tricuspid valve, and exits via the pulmonary artery. Only 10% of the blood from the pulmonary artery enters the pulmonary circulation with the majority crossing the ductus arteriosus into the aorta and the systemic circulation. The posterior and leftward nutrient-rich blood passes across the right atrium through the foramen ovale into the left atrium and out the left ventricle. This ensures that the heart and brain see the most oxygenated blood.
The precordial veins (ductus venosus, hepatic veins, IVC, umbilical and portal veins) have characteristic FVWs as shown by pulsed-wave Doppler velocimetry. The umbilical and portal veins have FVWs that are steady and without pulsations, while the other precordial “systemic” veins have FVWs that reflect the central venous pressures. The following information on the precordial venous FVWs is in reference to the hepatic vein, ductus venosus, and IVC, which have three characteristic phases during a single cardiac cycle. Ventricular systole induces the greatest pressure gradient between the right atrium and the precordial veins during the cardiac cycle. Thus, the blood traveling within these vessels to the heart will have the highest velocity during systole. This is referred to as the “S” component of the FVW. During early diastolic filling, the second highest velocity of blood through these venous conduits will occur and is referred to as either “D” or “e”. The lowest velocity of blood traveling through these vessels is in late diastole when the atria are contracting; this phase of the FVW is referred to as the “a”-wave. The a-wave in the ductus venosus remains in a positive direction (i.e., blood continues to move toward the heart even during the phase of lowest pressure gradient during atrial contraction). In contrast, the a-wave in the IVC and hepatic veins is in a negative direction indicating that blood is moving away from the heart. The difference in the a-waves between these vessels is important clinically because one can easily confuse reverse flow in the ductus venosus due to the close proximity of these vessels. However, the use of color Doppler and the identification of aliasing should easily distinguish the vessels.
The vast majority of fetal Doppler studies have adopted qualitative indices to describe FVW indices both for arterial flow and venous flow (i.e., S/a ratio of the venous flow of the ductus venosus). For some selected areas of investigation, quantitative parameters are calculated (i.e., peak velocity of the outflow tract of the great vessels). The arterial pipelines to almost all organs have been investigated, including the kidneys, the adrenal glands, the spleen, the lower limbs, the lungs, and the coronary arteries. While these reports provide a piece of the big picture, they do not add to information on fetal status and management gained from cardiac and precordial Doppler studies. As such they are not discussed, but are referenced at the end of the chapter (see “Suggested Readings”).
Circulation of the IUGR Fetus
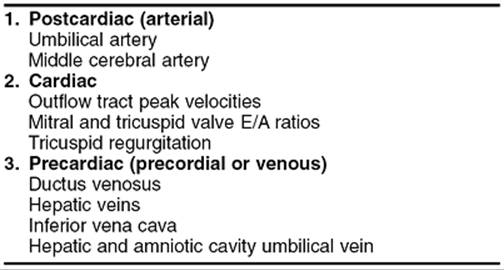
A convenient way to clinically approach the variety of fetal vessels that lend themselves to Doppler investigation is to conceptualize the progressive nature of the IUGR disease process and categorize them into three compartments related to the fetal heart:
1. Postcardiac (arterial) Dopplers
2. Cardiac Dopplers
3. Precardiac (precordial or venous) Dopplers.
The three general categories and vessels for each category are shown in Table 12.3. This organization follows the physiologic adaptations by the fetal circulation to progressive abnormalities in the placental vascular tree. Changes in the circulatory architecture of the IUGR placenta create a high-resistance vascular bed, which can be detected by Doppler velocimetry of the umbilical artery and the MCA. These represent the earliest Doppler changes in the IUGR fetus. As the IUGR fetus deteriorates, one can detect changes in peak velocities of the cardiac outflow tracts and abnormal valvular flow. Precordial or venous Dopplers also change in the IUGR fetus that is decompensating and these vessels include the ductus venosus, hepatic veins, IVC, and intrahepatic and intraamniotic umbilical veins.
|
|
|
TABLE 12.3. Categorization of fetal vessels for Doppler study |
Umbilical Artery Doppler
The first fetal vessel to be assessed by Doppler velocimetry FVW analysis was the umbilical artery in the mid-1970s. During the late 1970s and early 1980s, Gill and colleagues and Trudinger and co-workers described the umbilical artery FVW in normal and IUGR pregnancies. In 43 infants with birth weight less than the 10th percentile, Trudinger and colleagues found that the umbilical artery S/D ratio was elevated above the 95th percentile in 85% of cases. This was determined to be related to a decrease in diastolic velocity, which was in turn due to an increase in resistance to blood flow within the placenta. This was supported by work from Giles and colleagues who correlated the pathologic FVW in IUGR pregnancies with placental lesions. The key concept was that a poorly developed placental vascular bed and progressively abnormal vascularization in the face of increased fetal metabolic demands lead to an increase in placental vascular resistance. This is further supported by research work on hemodynamic bases of waveform changes as affected by increased impedance, changes in the viscosity of the blood, loss of vessel wall compliance, and decreasing inotropic function of the myocardium, all of which contribute to the increased resistance seen in abnormal arterial flow. The umbilical artery was chosen because it was the vessel that extended from the fetus to the placenta and because it reflects resistance patterns downstream within the placenta. This, in turn, could be identified clinically simply by switching a Doppler beam on the umbilical arteries and looking for an increased S/D ratio (low diastolic velocity) of the arterial waveform. During the 1990s, multiple studies on umbilical artery Doppler velocimetry in the IUGR fetus were followed by three major meta-analyses that showed a reduction in perinatal mortality by approximately one-third when umbilical artery Doppler velocimetry was used as an adjunct to other means of antenatal biophysical testing. In 1993, a European multicentered, prospective, observational trial reported by Karlsdorp and colleagues provided strong evidence suggesting that growth restricted fetuses with abnormal umbilical pulsatility index, with absent diastolic flow and with reverse diastolic flow, had progressively more severe perinatal outcomes.
Middle Cerebral Artery (MCA)
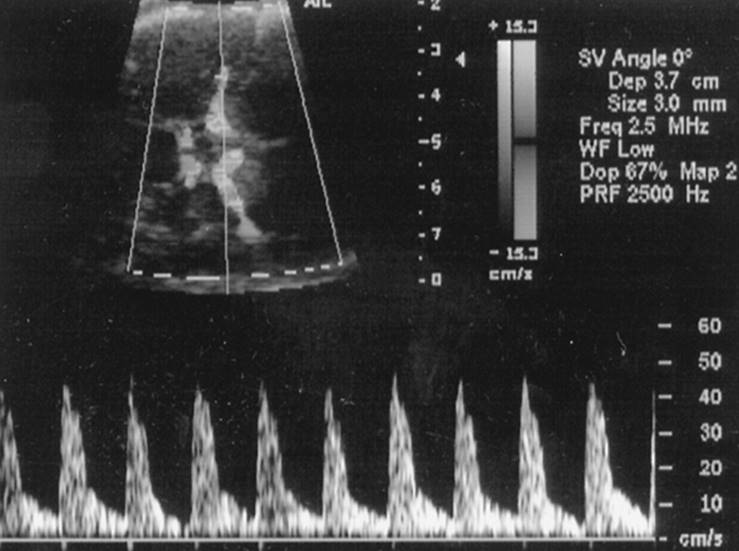
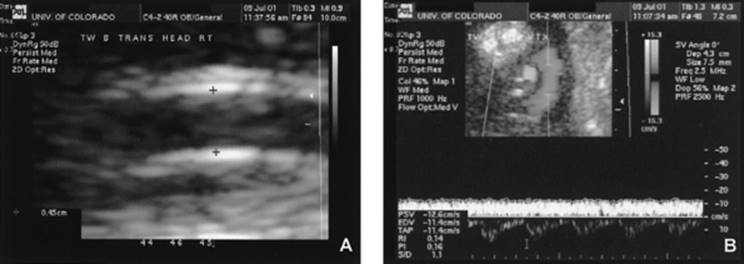
As mentioned earlier in this chapter, prolonged fetal hypoxia as a result of uteroplacental insufficiency will result in a redistribution of blood flow within the fetus in an attempt to deliver more oxygen by increasing volume blood flow to vital organs. This has been shown to be the case in some classic animal studies where prolonged hypoxia leads to blood flow redistribution that is favorable to the heart, brain, and adrenal glands. This redistribution has also been shown by pulsed-wave Doppler velocimetry to occur in human IUGR fetuses. The fetal brain normally has a high-resistance blood flow pattern, which is depicted by low flow velocity at end-diastole, relative to other organs and large vessels. During hypoxia, cerebral vascular autoregulation adjusts blood flow within the brain by decreasing the resistance to flow. The decrease in resistance can be easily detected by pulsed-wave Doppler, which provides an FVW profile that depicts an increase in end-diastolic flow velocity. This will in turn result in a calculated Doppler index of resistance that is low compared to the normally high resistance seen in the cerebral circulation. The most common cerebral artery used for Doppler assessment of the fetal brain-sparing effect is the MCA. The anatomic site and direction of the MCA is perpendicular to the cerebral midline (Fig. 12.4). This allows for the Doppler beam to be easily positioned along the midportion of the vessel with a minimal angle of insonation, thereby optimizing FVW acquisition. Incidentally, another advantage of the MCA position is that acquisition of a direct measurement of the absolute velocity in cases of fetal anemia (i.e., Rh isoimmunization and parvovirus) is easily obtained at this location.
|
|
|
FIG. 12.4. The ultrasound color Doppler image shows the circle of Willis and the middle cerebral artery branches. Also shown is the near 0-degree angle of insonation and the middle cerebral artery flow velocity waveform. See color figure 12.4. |
Both direct and indirect evidence acknowledge that hypoxia is a plausible mechanism for the decrease in MCA pulsatility index (PI) in IUGR. Direct evidence supporting this mechanism was reported by Capponi and associates in a group of IUGR fetuses with an abnormal umbilical PI. They showed that the best predictor of hypoxia at cordocentesis was the MCA PI. Baschat and co-workers provided good indirect evidence in support of hypoxia as a mechanism for the decreased MCA PI. In this study of IUGR fetuses with an abnormal umbilical artery PI, those with a decreased MCA PI had significantly higher nucleated red blood cell counts compared with those who had no Doppler evidence of MCA dilation.
The reduction in abdominal circumference typically precedes Doppler abnormalities in the umbilical artery and the MCA. Doppler studies have shown that the decrease in resistance by the fetal brain and the increase in resistance in the umbilical artery are the earliest arterial changes in Doppler flow velocities in the IUGR fetus. In our experience, they begin more than 3 weeks prior to non-reassuring fetal heart rate recordings. The primary message conveyed by Doppler investigation of the MCA vessel in IUGR fetuses is that the fetus is adapting appropriately to intrauterine hypoxia by “brain-sparing.” Loss of the “brain-sparing” adaptation is thought to be due to loss of cerebral autoregulation, and is considered to be a very late or terminal sign in the decompensating fetus. Before a loss of the “brain-sparing” is acted upon, one must be sure to avoid excessive transducer pressure because this will artificially lower the end-diastolic velocity. Furthermore, one will not see a loss of “brain-sparing” in the face of otherwise normal Doppler waveforms elsewhere, especially on the venous (precordial) side.
Precordial and Cardiac Flows
Cardiac Doppler studies in the IUGR fetus primarily include assessment of peak velocities of the outflow tracts, left and right ventricular cardiac output, and flow ratios across the valves. Variables that influence these measurements include preload, afterload, and intrinsic contractility of the left and right ventricles, as well as the valve dimensions. Significant contributions have been published on the changes in the atrioventricular filling waveform, and on the flow velocities of the outflow tract of the great vessels. Cross-sectional and longitudinal studies of IUGR fetuses with increased umbilical artery vascular resistance and decreased MCA vascular resistance show a progressive decrease in outflow tract velocity and cardiac output with advancing gestation. Valvular abnormalities tend to occur late in the course of an IUGR fetus that is rapidly decompensating. In one study of 31 IUGR fetuses and 289 normally grown fetuses, tricuspid valve regurgitation (TR) was a frequent, but in most cases, transient finding. Only 2 of the 31 IUGR fetuses showed TR. In one fetus it was only part-systolic, while the other fetus it was severely compromised with abnormal flows in both the arterial and venous system. That TR is a late sign in the course of IUGR has been confirmed elsewhere.
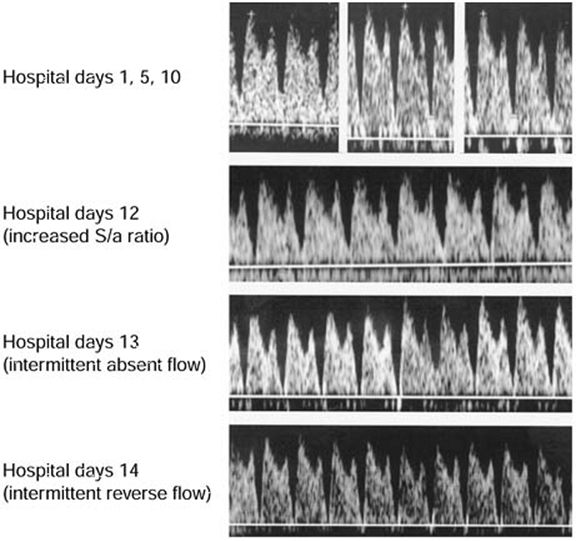
As mentioned earlier, Doppler velocimetry has been used to assess blood flow through the venous circulation of the IUGR fetus including the umbilical vein, ductus venosus, hepatic veins, and IVC. The IVC and the ductus venosus essentially represent the preload profile of the cardiovascular system. Interesting information conveyed by research on these vessels is the significant correlation between abnormal changes in the vessels and acid-base changes of the fetus. Others have correlated these Doppler indices with fetal heart monitoring patterns. Abnormalities in the ductus venosus are characterized by a decrease in velocity of the a-wave, and if the fetus continues to deteriorate, the ductus venosus may show absent or reversed flow velocity of the a-wave. The ductus venosus waveform in a severely growth restricted fetus from 20 to 22 weeks gestation of a mother with severe renal disease and hypertension is shown in Figure 12.5. The a-wave at 20 weeks showed reasonable flow velocity, but progressively deteriorated to intermittent absent and reverse flow velocity.
|
|
|
FIG. 12.5. Ductus venosus flow velocity waveform with abnormal a-waves in a severely growth restricted fetus admitted at 20 weeks gestation. Note the progressive decrease in velocity of flow in the a-wave. |
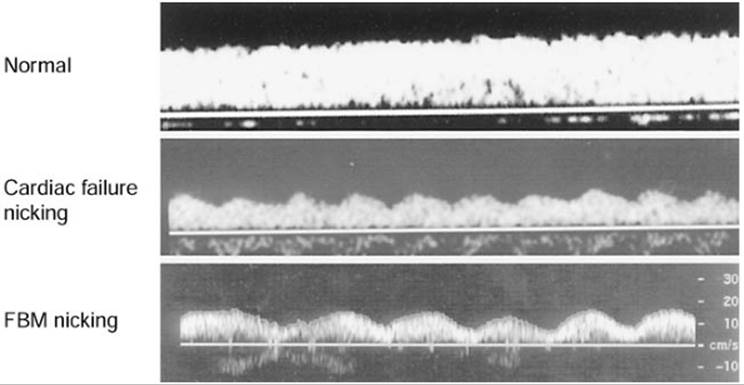
The umbilical vein normally has a steady FVW. The presence of pulsations or nicking in the umbilical vein FVW is a very late sign of the decompensating fetus and likely due to ventricular failure. These pulsations have been shown through animal studies to be initiated from atrial pressure changes and transmitted in a retrograde fashion. In early pregnancy, umbilical venous pulsations can be a normal finding. While assessing the umbilical vein with pulsed-wave Doppler, it is important to be cognizant that fetal breathing can mimic the nicking or pulsations of cardiac origin and these obviously have largely differing implications. Pulsations due to fetal breathing and due to cardiac failure can easily be distinguished by looking for fetal breathing motions or determining the rate of the pulsations seen on the FVW. A normal umbilical waveform, pulsations due to breathing, and pulsations due to cardiac failure are shown in Figure 12.6.
|
|
|
FIG. 12.6. Umbilical vein flow velocity waveform profiles demonstrating pulsations due to fetal breathing motions and cardiac failure compared to normal. |
Temporal Doppler Changes in the IUGR Fetus
While umbilical artery Doppler is useful as an adjunct in antenatal testing, it alone is not capable of distinguishing a decompensating fetus to the extent that morbidity can be reduced. Waiting until there is reverse flow nearly always results in an acidotic fetus with adverse long-term sequelae. It is here where venous Doppler studies will likely play a role in identifying earlier signs of deterioration in the IUGR. Since the late 1990s, more than 100 papers have been published both on the pathophysiology and clinical correlation of Doppler studies with traditional monitoring and with neonatal outcome. Advances in digital ultrasound technology have had a tremendous impact on the basic knowledge of fetal circulatory adaptation to placental supply deprivation. Clinically, this technology has allowed us to collect information and take a snapshot of fetal adaptation to placental dysfunction, which in turn can be interpreted as appropriate or inappropriate (i.e., decompensating) based upon the pattern of Doppler findings. The considerable knowledge gained through Doppler studies on isolated vessels or organs subsequently lead to two basic study questions regarding the “big picture”:
Is there a consistent temporally related sequence of Doppler changes within the circulation of the IUGR fetus?
If there is a progressive sequence of changes, is there a parallel increase in fetal morbidity and mortality?
These questions are just now being addressed.
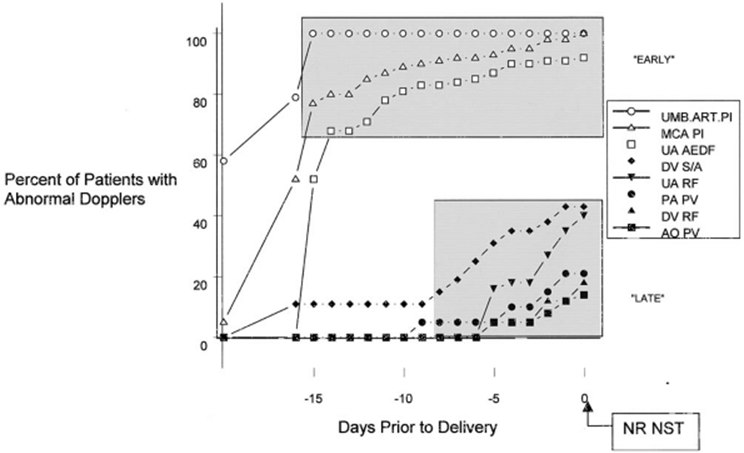
In 2001 and 2002, three studies introduced the idea that a deteriorating fetus follows a sequence of Doppler abnormalities prior to having a markedly abnormal biophysical test (nonstress test [NST], biophysical profile [BPP]) that would normally dictate delivery. It is important to understand that these studies were conducted on very preterm and severely growth-restricted fetuses. Baschat and colleagues reported that sequential deterioration of arterial and venous flows precedes BPP score abnormalities, and that perhaps adding Doppler to the BPP may enhance the performance of the BPP. Hecher and others reported that short-term variability and ductus venosus abnormalities are the important indicators for optimal timing of delivery. More recently, Ferrazzi and colleagues reported on fetal–neonatal injury and the sequential changes in Doppler velocimetry. Briefly, increased pulsatility in the umbilical artery, decreased pulsatility in the MCA (i.e., brain-sparing), and absent flow in the umbilical artery are considered “early” changes and alone were not associated with fetal injury. The next vessel to become abnormal was the ductus venosus, which was subsequently followed by other venous and cardiac Doppler abnormalities. These were considered “late” changes, frequently preceded by NST abnormalities, and were associated with a significant increase in fetal and neonatal morbidity and mortality. These “early” and “late” Doppler changes are shown in Figure 12.7. Thus, these studies suggest that waiting until the NST or the BPP become abnormal before delivery might be too late to prevent serious sequelae to the newborn and the child or adult that newborn is destined to become. They also suggest that the vessel that best determines the optimal timing for delivery is the ductus venosus.
|
|
|
FIG. 12.7. Temporal sequence of Doppler velocimetry changes in intrauterine growth restricted fetuses. (Modified from Ferrazzi E, Bozzo M, Rigano S, et al. The temporal sequence of changes in fetal velocimetry indices for growth-restricted fetuses. Ultrasound Obstet Gynecol 2002;19:140–146.) |
MANAGEMENT OF THE IUGR FETUS
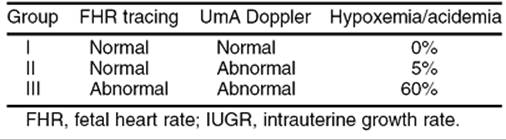
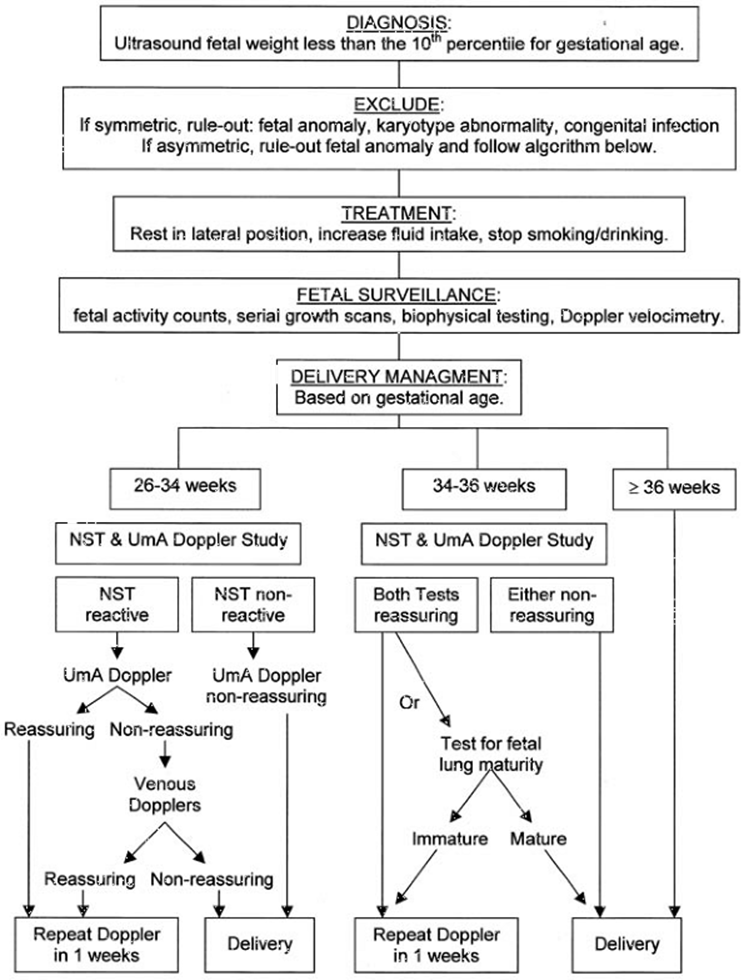
Historically, the management of the IUGR fetus was based on the fetus reaching fetal lung maturity, flattening of the growth curve, or awaiting a fetal heart rate change. In the mid-1990s, several meta-analyses demonstrated that perinatal mortality could be reduced by including umbilical artery Doppler velocimetry as part of the fetal biophysical assessment. While this was clearly a major advancement in management of the IUGR fetus, it still fell short of the goal of not only reducing perinatal mortality, but also reducing perinatal morbidity. In 1993, investigators in Milan, Italy reported a useful classification for IUGR severity. Table 12.4 shows the classification scheme that is based on fetal heart rate monitoring and umbilical artery Doppler velocimetry and the risk of fetal hypoxemia and acidemia. The study showed that waiting for the fetal heart rate to become non-reassuring would result in a hypoxic–acidemic fetus more than 60% of the time. Studies on Doppler changes in the IUGR fetus suggest that the fetus experiencing progressive compromise tends to follow a sequence of Doppler changes that may allow for better timing of delivery. These Doppler studies will likely be most useful in the management of the very preterm and severely IUGR fetus. Figure 12.8 is an algorithm for management guidelines of the IUGR fetus, which includes workup considerations for symmetric and asymmetric growth, daily routines, fetal monitoring, and gestational age based timing of delivery. Since amniotic fluid volume is a function of urine output and renal perfusion, the presence of oligohydramnios in an IUGR fetus should serve as a red flag. Oligohydramnios is not included in the algorithm. However, if it is present, delivery should be considered. If the fetus is extremely premature, hospitalization should be considered for in-house fetal monitoring.
|
|
|
TABLE 12.4. Fetal heart tracings, umbilical artery doppler, and the IUGR fetus |
|
|
|
FIG. 12.8. Algorithm for management guideline of the intrauterine growth restricted fetus. |
QUANTIFICATION OF FLOW
Until recent advancements in high-resolution digital imaging with simultaneous imaging and Doppler methodologies, the reproducibility and clinical feasibility of flow quantification have been limited. Studies show that umbilical venous flow can be measured accurately (inter- and intra-observer variability <7%) and in a timely fashion (<5 min). These flow measurements have been validated by invasive physiologic preparations in fetal lambs. Ultrasound images and formula for calculation of umbilical venous flow is shown in Figure 12.9. In a longitudinal study, not only was volume flow found to be reduced in the IUGR fetus compared to controls, but the variable responsible for this reduction was a low velocity of blood flow and not the umbilical vein diameter. Interestingly, the low umbilical flow in IUGR fetuses was identified very early in the course of IUGR before Doppler changes in other vessels became apparent. Quantitative flow measurements can even be obtained in very small vessels such as the ductus venous. Quantitative flow measurements are a potentially new-tool approach for the assessment of the growth-restricted fetus since quantification of placental flow to the fetus and its redistribution to the liver and heart is now possible.
|
|
|
FIG. 12.9. The formula for measurement of umbilical venous flow is shown. A: On ultrasound, how to obtain umbilical vein diameter (note that the calipers are placed just inside the specular reflections). B: On ultrasound, how color is used to ensure an angle of insonation at nearly 0 degrees and how Doppler velocimetry is used to obtain a steady umbilical vein waveform velocity. See color figure 12.9. |
Doppler Prediction of IUGR and Preeclampsia
The maternal side of the uteroplacental circulation has also been investigated by Doppler ultrasound and FVW analysis in hopes of identifying those pregnancies at increased risk for developing preeclampsia, abruption, and IUGR. Since the original reports on uterine artery Doppler waveform analyses, several important methodological issues have been established that include proper technology (color Doppler-guided, pulsed-wave Doppler sampling, and site of sampling), and normal reference values (S/D ratio >2.6, or resistance index >0.58). The pathophysiologic basis for abnormal uterine artery resistance is that resistance of the smaller spiral artery branches that lie downstream fail to become low-resistance vessels as a result of poor trophoblastic invasion early in pregnancy.
This test has gained a popular role in screening for preeclampsia and IUGR at 20 to 24 weeks of gestation. Scoring systems based on FVW abnormalities (increased resistance and notching) have been developed. For the most part, the highest risk for encountering an adverse pregnancy outcome goes up by having both early diastolic notching and high resistance, and if these occur bilaterally. The problem with the uterine artery Doppler test is that reported positive values vary considerably and there is a reasonably high false-positive rate. The false-positive rate can be reduced by repeating the test at 24 weeks gestation.
SUMMARY POINTS
· Proper establishment of the uterine–placental–fetal circulation early in gestation is critical to appropriate placental and fetal growth.
· Abnormal uterine artery Doppler waveforms reflect abnormal placentation and may be predictive of adverse pregnancy outcome.
· Establishment of accurate dating in pregnancy is necessary for assessment of appropriate growth and management of the pregnancy.
· Ultrasound dating of the pregnancy is most accurate in the first trimester.
· The transcerebellar diameter remains relatively unaffected in asymmetrically growth restricted fetuses.
· A distal femoral epiphysis of more than 3 mm is consistent with a pregnancy greater than 36 weeks gestation.
· In IUGR, it is important to remember to consider the possibility of a constitutionally small baby.
· In IUGR, use of umbilical artery Doppler velocimetry reduces perinatal mortality when used as an adjunct to other tests of fetal well-being.
· Doppler velocimetry studies of the venous circulation may be the best way to optimally assess the timing of delivery in the very preterm and growth-restricted fetus.
SUGGESTED READINGS
Alfirevic Z, Neilson JP. The current status of Doppler sonography in obstetrics. Curr Opin Obstet Gynecol 1996;8 (2):114–118.
Barbera A, Galan HL, Ferrazzi E, et al. The relationship of umbilical vein blood flow to growth parameters in the human fetus. Am J Obstet Gynecol1999;181:174–179.
Barker DJ, Gluckman PD, Godfrey KM, et al. Fetal nutrition and cardiovascular disease in adult life. Lancet 1993;341:938–941.
Baschat AA, Gembruch U, Reiss I, et al. Neonatal nucleated red blood cell counts in growth-restricted fetuses: relationship to arterial and venous Doppler studies. Am J Obstet Gynecol 1999;181 (1):190–195.
Baschat AA, Gembruch U, Harman CR. The sequence of changes in Doppler and biophysical parameters as severe fetal growth restriction worsens. Ultrasound Obstet Gynecol 2001;18:571–577.
Bellotti M, Pennati G, DeGasperi C, et al. Role of ductus venosus in distribution of umbilical blood flow in human fetuses during second half of pregnancy. Am J Physiol Heart Circ Physiol 2000;279:H1256–H1263.
Campbell S, Thoms A. Ultrasound measurement of the fetal head to abdomen circumference ratio in the assessment of growth retardation. Br J Obstet Gynaecol 1977;84 (3):165–174.
Capponi A, Rizzo G, Rinaldo D, et al. Effects of cordocentesis on inferior vena cava velocity waveforms: differences between normally grown and growth-retarded fetuses. Biol Neonat 1996;70 (2):84–90.
Divon MY. Umbilical artery Doppler velocimetry: clinical utility in high-risk pregnancies. Am J Obstet Gynecol 1996;174:10–14.
Dubiel M, Gudmundsson S, Thuring-Jonsson A, et al. Doppler velocimetry and nonstress test for predicting outcome of pregnancies with decreased fetal movements. Am J Perinatol 1997;14 (3):139–144.
Ferrazzi E, Bellotti M, Carconi A, et al. Peak velocity of the outflow tract of the aorta: correlations with acid base status and oxygenation of the growth-retarded fetus. Obstet Gynecol 1995;85:663–668.
Ferrazzi E, Bozzo M, Rigano S, et al. The temporal sequence of changes in fetal velocimetry indices for growth-restricted fetuses. Ultrasound Obstet Gynecol 2002;19:140–146.
Galan HL, Jozwik M, Rigano S, et al. Umbilical vein blood flow in the ovine fetus: comparison of Doppler and steady-state techniques. Am J Obstet Gynecol1999;181:1149–1153(abst).
Gembruch U, Smrcek JM. The prevalence and clinical significance of tricuspid valve regurgitation in normally grown fetuses and those with intrauterine growth retardation. Ultrasound Obstet Gynecol 1997;9:374–382.
Goldenberg RL, Cutter GR, Hoffman HJ, et al. Intrauterine growth retardation: standards for diagnosis. Am J Obstet Gynecol 1989;161:271–277.
Goldstein I, Reece EA, Pilu G, et al. Cerebellar measurements with ultrasonography in the evaluation of fetal growth and development. Am J Obstet Gynecol1987;156:1065–1106.
Hadlock FP, Harrist RB, Sharman RS, et al. Estimation of fetal weight with the use of head, body, and femur measurements—a prospective study. Am J Obstet Gynecol 1985;151:333–357.
Harrington KF, Campbell S, Bewley S, et al. Doppler velocimetry studies of the uterine artery in the early prediction of pre-eclampsia and intra-uterine growth retardation. Eur J Obstet Gynecol Reprod Biol 1991;42[Suppl]:14–20.
Hecher K, Snijders R, Campbell S, et al. Fetal venous, intracardiac, and arterial blood flow measurements in the IUGR fetus has been correlated with fetal blood gases. Am J Obstet Gynecol 1995;173 (1):10–15.
Hecher K, Hackeloer BJ. Cardiotocogram compared to Doppler investigation of the fetal circulation in the premature growth-retarded fetus: longitudinal observations. Ultrasound Obstet Gynecol 1997;9:152–161.
Hecher K, Blardo CM, Stigter RH, et al. Monitoring of fetuses with intrauterine growth restriction: a longitudinal study. Ultrasound Obstet Gynecol2001;18:564–570.
Hernandez-Andrade E, Brodszki J, Lingman G, et al. Uterine artery score and perinatal outcome. Ultrasound Obstet Gynecol 2002;19:438–442.
Hofstaetter C, Dubiel M, Gudmundsson S, et al. Uterine artery color Doppler assisted velocimetry and perinatal outcome. Acta Obstet Gynecol Scand1996;75:612–219.
Kaufmann P, Sen DK, Schweikhart G. Classification of human placental villi. Cell Tissue Res 1979;200:409–423.
Karlsdorp VHM, van Vugt JMG, van Geijn HP, et al. Clinical significance of absent or reversed end diastolic velocity waveforms in umbilical artery. Lancet1994;344:1664–1668.
Mari G, Deter RL. Middle cerebral artery flow velocity waveforms in normal and small-for-gestational-age fetuses. Am J Obstet Gynecol 1992;166:1262–1270.
Marsal K. Abnormal antenatal ultrasound findings and subsequent handicap. Baillieres Clin Obstet Gynaecol 1988;2:125–144.
Ozcan T., Sbracia M, d'Ancona RL, et al. Arterial and venous Doppler velocimetry in the severely growth-restricted fetus and associations with adverse perinatal outcome. Ultrasound Obstet Gynecol 1998;12:39–44.
Pardi G, Cetin I, Marconi AM, et al. Diagnostic value of blood sampling in fetuses with growth retardation. N Engl J Med 1993;328:692–696.
Reece EA, Goldstein I, Pilu G, et al. Fetal cerebellar growth unaffected by intrauterine growth retardation: new parameter for prenatal diagnosis. Am J Obstet Gynecol 1987;157:632–638.
Reed KL, Chaffin DG, Anderson CF. Umbilical venous Doppler velocity pulsations and inferior vena cava pressure elevations in fetal lambs. Obstet Gynecol1997;87:617–620.
Rizzo G, Arduini D, Romanini C, et al. Doppler echocardiographic assessment of atrioventricular velocity waveforms in normal and small-for-gestational-age fetuses. Br J Obstet Gynaecol 1998;95:65–69.
Soothill PW, Ajayi RA, Campbell S, et al. Prediction of morbidity in small and normally grown fetuses by fetal heart rate variability, biophysical profile score and umbilical artery Doppler studies. Br J Obstet Gynaecol 1993;100 (8):742–745.
Todros T, Sciarrone A, Piccoli E, et al. Umbilical Doppler waveforms and placental villous angiogenesis in pregnancies complicated by fetal growth restriction. Obstet Gynecol 1999;93:499–503.
Trudinger BJ, Cook CM, Giles WB, et al. Umbilical artery flow velocity waveforms in high-risk pregnancy. Randomised controlled trial. Lancet 1987;1:188–190.
Trudinger BJ, Giles WB, Cook CM. Uteroplacental blood flow velocity-time waveforms in normal and complicated pregnancy. Br J Obstet Gynaecol1985;92:39–45.
van Asselt K, Gudmundsson S, Lindqvist P, et al. Uterine and umbilical artery velocimetry in pre-eclampsia. Acta Obstet Gynecol Scand 1998;77:614–619.