Ronald S. Gibbs
Premature rupture of the fetal membranes (PROM) is one of the most common problems in obstetrics, complicating approximately 5% to 10% of term pregnancies and up to 30% of preterm deliveries. Although the etiology of premature rupture of the membranes is often not clinically evident, a degree of consensus has arisen regarding management options. Indeed, the problem is intricate. Considerations in selecting management in a particular patient are gestational age and patient demographics. The clinician is confronted by a complex set of options including use of corticosteroids, tocolytics, more potent antibiotics, and innovative approaches using various tests (such as amniocentesis, ultrasound, and biophysical testing). Of major importance is the marked improvement in survival of low–birth-weight infants.
DEFINITIONS
PROM is usually defined as rupture at any time before the onset of contractions. Unfortunately, “premature” also carries the connotation of preterm pregnancy. To avoid confusion, we use the word preterm to refer to gestational age of less than 37 weeks. Thus, preterm PROM (PPROM) refers to PROM prior to 37 weeks gestation. The latent period is defined as the time from membrane rupture to onset of contractions. It is to be distinguished from a similar term, latent phase, designating the early phase of labor before the active phase. Various terms have been used to describe presumed maternal or perinatal infections related to PROM. During labor, designations have included “fever in labor,” “intrapartum fever,” “chorioamnionitis,” “amnionitis,” and “intrauterine infection.” The degree of temperature used to define “fever” has varied. After delivery, maternal infection is referred to as “endometritis” or “postpartum infection.” These diagnoses are usually based upon fever, uterine tenderness, and exclusion of other sources of fever. In neonates, the most common term used to report infection was neonatal sepsis, but this may mean strictly a positive blood culture or simply clinical signs or symptoms of sepsis.
INCIDENCE
The incidence of PROM ranges about 5% to 10% of all deliveries, and preterm PROM occurs in approximately 1% of all pregnancies. Approximately 70% of cases of PROM occur in pregnancies at term, but in referral centers, more than 50% of cases may occur in preterm pregnancies. PROM is the clinically recognized precipitating cause of about one third of all preterm births. Despite some progress in prolonging the latent period after preterm PROM and prevention of recurrence (in women with bacterial vaginosis), PPROM remains a leading contributor to the overall problem of premature birth.
ETIOLOGY
In the vast majority of cases, the etiology is not clinically evident. Earlier studies had identified selected clinical conditions such as cervical incompetence and polyhydramnios as being risk factors evident in some cases of PROM.
A scholarly review of the etiology of PPROM identified numerous potential causes in any given case. These included: a generalized decrease in tensile strength of membranes, local defects in the membranes, decreased amniotic fluid collagen and a change in collagen structure, uterine irritability, apoptosis, collagen degradation, and membrane stretch. The Maternal-Fetal Medicine (MFM) Network found that risk factors for PPROM were previous PPROM, positive fetal fibronectin at 23 weeks, and short cervix (<25 mm) at 23 weeks.
Substantial evidence is available to show that subclinical infection may be a cause of PROM, not merely its result.
Support for a role of infection is provided by studies showing an association between clinically diagnosed bacterial vaginosis (or isolation of anaerobes in the vagina) and preterm birth/preterm premature rupture of the membranes. Some genital bacteria elaborate enzymes such as proteases, phospholipases, and collagenases that may act to weaken the membranes. Positive cultures of the amniotic fluid in cases of PPROM are obtained in approximately 30%.
In a large case-control study, three factors were associated with preterm PROM in a multifactorial analysis. These were previous preterm delivery (odds ratio [OR] = 2.5; 95% confidence interval [CI] = 1.4-2.5), cigarette smoking (stopped during pregnancy, OR = 1.6; 95% CI = 0.8–3.3; continued during pregnancy, OR = 2.1; 95% CI = 1.4–3.1), and bleeding (first trimester, OR = 2.4; 95% CI = 1.5–3.9; third trimester, OR = 6.5; 95% CI = 1.9–23; more than one trimester, OR = 7.4; 95% CI = 2.2–26). This study enrolled controls at the same gestational age as cases (thus correcting for the decreasing frequency of coitus closer to term) and found no association between coitus and PROM. However, other large studies have not confirmed smoking or vaginal bleeding as risk factors. Recent coitus is probably not a cause of PROM.
Investigations into the placental histology have provided correlates with clinical outcomes in cases of preterm premature rupture of the membranes. Overall, acute inflammation was seen in 43%, vascular lesions were seen in 20%, inflammation plus vascular lesions in 20%, normal findings in 14%, and “other” findings in 3% (Fig. 11.1). When acute inflammation was seen in the placenta (either by itself or mixed with vascular lesions), birth less than 26 weeks was more common, and delivery for suspected or proved clinical infection was also more common.
|
|
|
FIG. 11.1. Placental histology in 235 cases of premature PROM. (From Sweet RL, Gibbs RS. Infectious diseases of the female genital tract, fourth ed. Philadelphia: Lippincott Williams & Wilkins, 2002; with permission.) |
COMPLICATIONS AND CONSEQUENCES OF PROM
Onset of Labor
At term, the onset of labor occurs within 24 hours after membrane rupture in 80% to 90% of patients. Among patients with PROM prior to term, latent periods occur longer. Latent periods of more than 24 hours occur in 57% to 83%, of more than 72 hours in 15% to 26%, and of 7 days or more in 19% to 41%. There is an inverse relationship between gestational age and the proportion of patients with latent periods longer than 3 days. For pregnancies between 25 and 32 weeks, 33% had latent periods longer than 3 days, whereas for pregnancies of 33 to 34 and 35 to 36 weeks, the corresponding values were 16% and 4.5%, respectively.
Effect of Tocolytic Drugs
The value of tocolytics in PPROM remains controversial. None of eight prospective trials showed a decrease in neonatal morbidity, whether tocolysis was used prophylactically (for all patients in admission regardless of uterine activity) or therapeutically (for patients who developed uterine contractions). Only three of the eight showed a prolongation of the latency period; an additional study showed a prolongation for gestation less than 28 weeks. In three studies steroids were used; in another three studies antibiotics were used.
A comparison of short-term versus long-term tocolysis in preterm PROM at 26 to 35 weeks showed adverse effect of “long-term tocolysis.” Patients with preterm PROM at 26 to 35 weeks were randomized to receive either an intravenous β-mimetic drug for less than 48 hours versus until delivery. All patients received corticosteroids, and group B streptococci (GBS) and gonococci were treated. There was no significant difference in the latent period or in neonatal infection, but there was a significant increase in both chorioamnionitis and endometritis with long-term tocolysis. Accordingly, use of tocolytics in patients with preterm PROM remains controversial, but the bulk of the evidence shows no benefit. However, if tocolytics are used, such as during transfer to a tertiary care center or obtaining benefits of corticosteroids, the course of tocolytics should be limited to less than 48 hours.
Respiratory Distress Syndrome, Infections, and Other Complications
The risks of PROM have generally been viewed as those of infection versus those of prematurity. The most common clinically evident complication among pregnancies with PROM before 37 weeks is respiratory distress syndrome (RDS), which, in general, is found in 10% to 40% of neonates. Bona fide neonatal sepsis is documented in less than 10%, and amnionitis (based always on clinical criteria) occurs in approximately 3% to 31%. Subclinical infection, based upon positive amniotic fluid culture or histologic inflammation of the cord or membranes, is seen much more often, in up to 80% at very early gestational ages with PPROM. Endometritis develops in 0% to 29%. Abruption after PROM is reported in 4.0% to 6.3% of cases, higher than the usually quoted rate of 0.5% to 1.0%. Pulmonary hypoplasia is a serious fetal complication occurring in preterm PROM. Pulmonary hypoplasia is more common when there is very early preterm PROM, especially when this occurs in the presence of prolonged PROM and with severe oligohydramnios. There is nearly a 100% probability of lethal pulmonary hypoplasia when PROM occurs before 23 weeks and when there is severe oligohydramnios. With later gestational age at the onset of preterm PROM, the likelihood of pulmonary hypoplasia decreases. Notably with preterm PROM more than 28 to 29 weeks, even with oligohydramnios, pulmonary hypoplasia is rare. When preterm PROM occurs less than 25 weeks with severe oligohydramnios lasting more than 14 days, the likelihood of lethal pulmonary hypoplasia is estimated to be 80%. At the other extreme, when preterm PROM occurs at more than 25 weeks and when there is either no severe oligohydramnios or severe oligohydramnios for less than 5 days, then the predicted probability of lethal pulmonary hypoplasia is only 2%. These data provide important information for counseling patients with mid-trimester PROM.
RECURRENCE
The reported recurrence rate for PPROM is 32% for patients who had PPROM in an index pregnancy. Based on these data, the risk of recurrence is considerable, prompting patient education and close follow-up in subsequent pregnancies.
EVALUATION
Diagnosis
The initial evaluation may reveal amniotic fluid egressing from the vagina. The differential diagnosis of rupture of membranes includes loss of mucus plug, vaginal discharge associated with infection, and urinary incontinence. If the patient is not going to be delivered immediately, then a digital examination should be deferred as examination may introduce bacteria into the uterus and shorten the latent phase. A sterile speculum exam may demonstrate pooling of fluid in the posterior vaginal vault. Direct observation of fluid leaking from the cervical os is proof of ruptured membranes. The normal pH of the vagina is between 4.0 and 4.7 in pregnancy, whereas the pH of the amniotic fluid is 7.1 to 7.3. Nitrazine paper changes to a dark blue from yellow with a pH above 6.5. Nitrazine paper to diagnose amniotic fluid in the vagina has an overall accuracy of approximately 93%, but false-positive results can result from blood, semen, alkaline urine, bacterial vaginosis, and trichomoniasis.
The diagnosis of PROM may also be confirmed by observing arborization or “ferning” of dried amniotic fluid on a slide. This method has an overall accuracy of diagnosis of PROM of approximately 96%. False positives occur with contamination by semen or cervical mucus. False negatives can result from a dry swab, contamination with blood at a 1:1 dilution, or not allowing sufficient time for the fluid to dry on the slide. Amniotic fluid arborization is unaffected by meconium at any concentration and is unaffected by pH alteration.
Ultrasound examination has been used widely, since oligohydramnios suggests PROM, but there have been no evaluations of its sensitivity and specificity. A multicenter clinical trial compared fetal fibronectin detection with standard tests for detection of rupture of membranes at term. Fetal fibronectin showed an excellent sensitivity (98.2%) but a low specificity, leading to speculation that fetal fibronectin in cervicovaginal secretions may be a marker for impending labor, even without frank rupture of the membranes.
When the diagnosis of ruptured membranes is unclear by these tests, a transabdominal dye injection is sometimes performed. A dye such as indigo carmine blue is injected into the amniotic fluid, and a sponge is placed into the vagina and later inspected for the dye. Methylene blue should not be used because of reported methemoglobinemia in the fetus. This test is invasive, and the accuracy of diagnosis is not established. After dye injection, an observation period of 30 minutes is sufficient to detect passage of dye from the vagina.
Fetal Maturity
Determination of the fetal age and maturity status is useful in developing a treatment plan. The patient's history and early milestones of the pregnancy should be used. Ultrasound examination of the fetus can be limited because of the decreased fluid surrounding the fetus, and some measurements, especially of the abdomen and head, may be altered with oligohydramnios after PROM. As part of the overall decision process as to delivery, assessment of fetal lung status may be incorporated, for example, if gestational age is 32 to 34 weeks or if there is uncertainty regarding growth restriction versus prematurity. Amniotic fluid may be collected by amniocentesis or by collection from the vaginal pool. Vaginal pool collection is less accurate for lecithin/sphingomyelin ratio (L/S R) determination. Whereas phosphatidylglycerol (PG) production by vaginal bacteria has been described, there has been an excellent correlation between PG detection in amniotic fluid obtained vaginally and transabdominally.
Cervical Status
In addition to documentation of ruptured membranes, the sterile speculum exam can evaluate the degree of cervical dilation and can exclude the possibility of a fetal extremity or umbilical cord prolapsing through the cervix. Endovaginal ultrasound may be used in patients with preterm PROM without increasing the risk of infection or shortening the latent period.
Infection
When the diagnosis of PROM is made, a rectovaginal culture should be taken for GBS and appropriate antibiotics for prevention of GBS infection should be given pending culture results.
All patients with preterm PROM should be evaluated for possible evidence of chorioamnionitis. Physical exam includes maternal or fetal tachycardia, uterine tenderness, and detection of a purulent, foul-smelling discharge. Temperature elevation is often a late sign of chorioamnionitis, especially in preterm PROM. In Table 11.1, we show the positive and negative predictive values of several tests for intrauterine infection in PPROM. Amniocentesis may be performed to evaluate for an intrauterine infection, for example, if there are equivocal clinical signs of infection. Because of the high likelihood of subclinical infection and the association of intrauterine infection with cerebral palsy, there is a growing enthusiasm for early detection of subclinical infection. Accordingly, amniocentesis may become more widely used. Analyses of amniotic fluid for possible infection include Gram stain, glucose concentration, and culture. Gram stain does not identify colonization with genital mycoplasmas. A low amniotic fluid glucose predicts a positive amniotic fluid culture. When the glucose is greater than 20 mg per dL, the likelihood of a positive culture is less than 5%; when glucose is less than 5 mg per dL, the likelihood of a positive culture approaches 90%. Although not widely available, an elevated interleukin 6 (IL-6) in amniotic fluid may be the most sensitive predictor of intrauterine infection. A biophysical profile of 6 or less has been shown in several studies to correlate with intrauterine infection. Most newborns who are delivered after clinical chorioamnionitis do not show clinical infection.
|
|
|
TABLE 11.1. Prediction of infection in PROM |
TREATMENT CONSIDERATIONS
The overall approach to management of PROM takes into consideration neonatal survival at the gestational age when rupture occurs. Management may be divided into four different phases of pregnancy. During the second trimester, neonatal survival is nil, leading numerous investigators to adopt a policy of expectant management or induction. Early in the third trimester, neonatal survival rises markedly, but there is still considerable morbidity associated with delivery at this gestational age. In the mid-third trimester, neonatal survival is high, but there is still considerable morbidity, whereas in the late third trimester (at or near term) neonatal mortality and morbidity are low. Neonatal outcome is one of the driving features in determining clinical management.
Diagnosis of Infection After PROM
Both invasive and noninvasive tests have been assessed. As shown in Table 11.1, none of these tests is ideal, particularly because of their low positive predictive values.
Use of Steroids
Clinicians remain unable to agree on the risks and benefits of steroids in preterm PROM. The first meta-analysis in 1989 concluded that the use of steroids “increases the incidence of endometritis and may increase neonatal infections.” The 1994 National Institutes of Health (NIH) Consensus Conference concluded that the risk of maternal and infant infection may be increased with corticosteroid use after PROM but that the magnitude of this risk was small. The NIH recommendations are summarized in Table 11.2. The benefits of steroids with PPROM before 28 weeks, however, have not been firmly established.
|
|
|
TABLE 11.2. Corticosteroid use in PPROMa |
Effect of Latent Period and Vaginal Examination upon Incidence of Amnionitis
In earlier studies, the incidence of amnionitis rose with increasing length of the latent period, but other investigators have found no increase in the incidence of amnionitis among preterm pregnancies with increasing latent periods. In a comparison of outcomes, women with digital examination after PROM had a significantly shorter latent period (2.1 ± 4.0 vs. 11.3 ± 13.4 days; P < .001), more maternal infection (44% vs. 33%; P = .09), and more positive amniotic fluid cultures (11/25 [44%] vs. 10/63 [16%]; P < .05). Thus, routine vaginal examination should be avoided until labor develops in patients with preterm PROM.
Use of Prophylactic Antibiotics
In patients with PROM prior to term, there are two rationales for prophylactic antibiotics. The first is a clear one; namely, for prevention of perinatal GBS infection.
A second rationale for antibiotic prophylaxis has been based upon the hypothesis that infection is either the triggering cause of preterm PROM or that infection ensuing after preterm PROM triggers the labor. Accordingly, this rationale for prophylactic antibiotics has been to delay delivery after preterm PROM rather than to prevent clinically evident infection. We believe that good evidence has been provided to favor use of broad-spectrum antibiotics in selected cases of preterm PROM. This support was provided in a meta-analysis and in prospective randomized trials. In the meta-analysis, 24 trials were identified and 13 were included, containing 1,594 women. However, only 6 of the trials were placebo-controlled, and the trials were heterogeneous with regard to antibiotics used. In addition, there was no standard use of steroids, tocolytics, or prophylaxis for GBS. Nevertheless, benefits were demonstrated in favor of women receiving antibiotics. These benefits included a significant delay in delivery within 7 days, a reduction in chorioamnionitis, and a reduction in neonatal sepsis. There were also reductions (that did not achieve statistical significance) in postpartum infection, neonatal death, neonatal pneumonia, and neonatal bacteremia.
In the large MFM trial, patients were enrolled if they had preterm PROM for less than 72 hours at 24 to 32 weeks gestation. Patients were excluded if there was chorioamnionitis, labor, or fetal distress. Patients were then randomized to a course of ampicillin plus erythromycin (each for 2 days i.v. followed by up to 7 days orally) vs. placebo. Patients with GBS were given treatment during the latent period and no tocolytics were used. However, at the time the study was designed, it was decided not to use corticosteroids in any patients. The primary end point was a prospectively defined composite of neonatal death, neonatal RDS, grade III or IV intraventricular hemorrhage, grade II or III necrotizing enterocolitis, or neonatal sepsis. Patients randomized to antibiotic therapy had a significantly greater likelihood of remaining undelivered when assessed at 2 days, 7 days, 14 days, and 21 days (Fig. 11.2). In addition, the primary composite outcome was significantly reduced in the total population and in the GBS-negative cohort. Individual adverse outcomes significantly reduced in the antibiotic group included RDS, chorioamnionitis, neonatal sepsis, and neonatal pneumonia. Table 11.3 summarizes the benefits of antibiotics in patients with preterm PROM and stratifies the results by total population versus the GBS-negative cohort.
|
|
|
FIG. 11.2. Prolongation of pregnancy in group B streptococci-negative cohort. Antibiotic group shown in open circles; placebo in solid circles. (From Sweet RL, Gibbs RS. Infectious diseases of the female genital tract, fourth ed. Philadelphia: Lippincott Williams & Wilkins, 2002; with permission.) |
|
|
|
TABLE 11.3. Maternal–Fetal Medicine network trial of antibiotics after PPROM: summary of benefits |
Subsequent to this trial, others have appeared assessing antibiotics in conjunction with antenatal corticosteroid therapy for patients with preterm premature rupture of the membranes. One study assessed 112 women with PROM from 25 to 35 weeks and randomized them to ampicillin sulbactam/amoxicillin clavulanate versus ampicillin/amoxicillin versus placebo. Tocolytics were used in this trial and betamethasone was used weekly up to 32 weeks. Patients receiving the antibiotics had less serious neonatal complications including neonatal death, RDS, and neonatal sepsis (P < .05) and they also had significantly higher mean birth weight (P = .03). Lewis and colleagues reported a randomized clinical trial of corticosteroids in patients with preterm PROM after treating these patients for a minimum of 12 hours with ampicillin/sulbactam. Antibiotics were continued for 7 days and steroids were repeated weekly. No tocolytics were used. The authors defined the primary outcome as the incidence of RDS, whereas secondary outcome measures included latency and neonatal or maternal infections. In this study of 77 patients, no statistically significant difference in latency was noted comparing the steroid versus no steroid group, and both neonatal and maternal infections were similar. However, there was a significant reduction in the incidence of RDS, 18.4% in the steroid group compared with 43.6% in the no steroid group. The authors concluded that treating preterm PROM with a broad-spectrum antibiotic before corticosteroids decreased RDS without apparent adverse effect. In 1998, a meta-analysis of five trials on antibiotic and glucocorticoid treatment reportedly did not show a significant effect on outcomes including maternal infection, neonatal sepsis, RDS, intraventricular hemorrhage, necrotizing enterocolitis, and neonatal morbidity. In contrast, the authors note “antibiotic therapy without concomitant use of glucocorticoids significantly reduced the odds of maternal infection, neonatal sepsis, and intraventricular hemorrhage substantially.” However, this meta-analysis did not include some of the more recent studies noted immediately above.
In a very large (nearly 5,000 patients) international trial (ORACLE I), patients with PPROM were randomized to one of four courses: oral erythromycin, oral amoxicillin-clavulanic acid, both antibiotics, or oral placebo. Each regimen was taken four times a day for 10 days or until delivery. The primary outcome measure used was a composite of neonatal death, chronic lung disease, or major cerebral abnormality on ultrasound. Erythromycin was associated with several benefits to the neonate (fewer cases with the composite outcome, prolongation of pregnancy, and fewer positive blood cultures). Amoxicillin-clavulanic acid—with or without erythromycin—was associated with prolongation of pregnancy, but it was also associated with a significant increase in neonatal necrotizing enterocolitis. The applicability of this study to contemporary U.S. practice is limited, however, because the authors made no provision for GBS prophylaxis. Other features of the study to emphasize are that antibiotics were used orally, enrollment was permitted up to 37 weeks (only 50% of cases were less than 32 weeks), and there was no standard approach for use of steroids or tocolytics. (Steroids were used in 75% of cases and tocolytics in <15%.)
Widespread use of antibiotics in this situation has raised concern about selection pressure toward resistant organisms, but in the MFM trial, there was no significant increase in maternal yeast infection or neonatal Candida sepsis, nor were there any cases of pseudomembranous colitis, maternal sepsis, or maternal death.
Determination of Fetal Lung Maturity
Because RDS is the single greatest threat to infants with PROM, some investigators have determined the status of fetal pulmonary maturity and proceeded with delivery when there was lung maturity. One study used amniocentesis and obtained fluid in about half of the cases. Others have attempted to collect amniotic fluid from the vagina and have had success rates of 80% to 94%. Presence of either PG or an L/S R of more than two in amniotic fluid collected vaginally has been reported to be a good predictor of pulmonary maturity.
In a larger series of patients with PROM before 36 weeks, investigators determined whether PG was present in the vaginal pool and delivered patients when there was presence of PG, spontaneous labor, or evidence of sepsis. PG in amniotic fluid from the vagina reliably predicted fetal lung maturity. However, absence of PG did not necessarily mean that RDS would develop. Of the 131 patients who did not show PG in the vaginal pool in any sample, 82 (62%) were delivered of infants who had no RDS. Thus, even with PROM, delivery of a premature infant simply because its lungs showed biochemical maturity may be questioned in view of other potential hazards of prematurity and the difficulty of the induction. Of note, some genital tract bacteria have been found to yield a false-positive test for PG.
MANAGEMENT
PROM at or Near Term (Table 11.4)
|
|
|
TABLE 11.4. Summary of management: PROM at or near term (≤ 35 wks) |
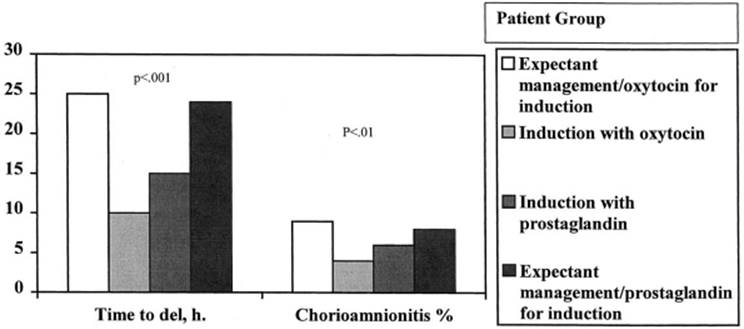
In the last few years, new studies have influenced changes in management of PROM at term. Previously, induction of labor (with oxytocin) within 12 to 24 hours after PROM at term was a practice followed by most U.S. obstetricians. Studies in the United States and in Scandinavia supported the safety of this approach and reported shorter maternal hospital stays with less clinically evident neonatal infection. Although expectant management with inpatient observation had been shown to be safe in most patient populations, this approach has become less popular because of the inconvenience and expense of the hospitalizations. Several studies have reported the safety and benefits of prostaglandins and have supported the increased popularity of induction with these preparations. In comparison to patients managed expectantly, those given intravaginal prostaglandin E2 (PGE2) shortly after admission had significantly less likelihood of a need for oxytocin and a significantly shorter time to delivery. There was no significant difference in cesarean section rate or in maternal or neonatal infection rates. In the largest trial of management of PROM at term, patients were studied in a four-arm trial with approximately 1,250 patients in each arm. These arms were as follows: Expectant management plus oxytocin for induction as needed; induction with i.v. oxytocin shortly after admission; induction with PGE2 gel in a dose of only 1 to 2 mg shortly after admission; and expectant management followed by PGE2 induction as needed. One methodological concern regarding this study is the low dose of PGE2 gel used vaginally. With most patients receiving less than 2 mg, the dose was smaller than used in most U.S. trials. As shown in Figure 11.3, patients randomized to expectant management initially had significantly longer times to delivery than patients randomized to either of the induction arms (P < .001). In addition, the rate of clinically diagnosed chorioamnionitis was less in the patients randomized to induction initially (with significance achieved at P < .01 comparing arms 1 vs. 2). The distribution of postpartum infection was similar to that of chorioamnionitis. In addition, there was no significant difference in rates of neonatal infection or cesarean section. Of note, patient satisfaction was significantly higher in the induction arms.
|
|
|
FIG. 11.3. Selected outcomes in an international term PROM trial. (From Sweet RL, Gibbs RS. Infectious diseases of the female genital tract, fourth ed. Philadelphia: Lippincott Williams & Wilkins, 2002; with permission.) |
A large meta-analysis involving 23 studies and including nearly 7,500 patients concluded that conservative management may result in more maternal infections than immediate induction with either oxytocin or prostaglandins. This meta-analysis also showed that the rate of chorioamnionitis was higher in patients induced with prostaglandin versus those induced with oxytocin. However, this meta-analysis was heavily influenced by the large international trial, and as noted previously, this trial used a very low dose of prostaglandin.
Within the last few years, intravaginal misoprostol (a PGE1 analog) has assumed marked popularity for induction because of its efficacy and low cost. Intravaginal misoprostol (50 µg every 4 hours for a maximum of 12 tablets) was compared with oxytocin in women with single pregnancies and an unfavorable cervix (<2 cm dilated and <80% effaced). The results of this trial are presented in Table 11.5. Overall, patients randomized to misoprostol had a shorter induction time, by approximately 2 hours, but they had significantly more uterine tachysystole. Of note, over 85% of patients required only one dose of misoprostol. Compared to other trials evaluating misoprostol in patients at term with intact membranes, the dose used in this trial is relatively high.
|
|
|
TABLE 11.5. Misoprostol vs. oxytocin in PROM |
A 1998 American College of Obstetricians and Gynecologists' (ACOG) Practice Bulletin concluded that with term PROM, labor may be induced at the time of admission or that patients may be observed for up to 24 to 72 hours after PROM. In sum, while a range of practices is available and supported in the literature, the decision regarding delivery after PROM at term must take into account fetal presentation, fetal status, cervical ripeness, presence of infection, and patient desires. For patients with a breech (or other malpresentation) infant or an infant with evidence of intolerance of labor, prompt cesarean delivery is most appropriate. If there is clinically evident infection and no contradiction to vaginal delivery, then immediate induction and antibiotic therapy are indicated. If the cervix is ripe, then a short period of observation is reasonable, but induction with oxytocin resolves the situation. When the cervix is unripe, induction with either prostaglandins or oxytocin shortens the time to delivery, decreases risk of infection, and does not appear to increase cesarean section rate. The epidemiologic data linking chorioamnionitis with cerebral palsy provide additional impetus to move toward delivery after PROM at term.
PROM at 32 to 34 Weeks (Table 11.6)
|
|
|
TABLE 11.6. Summary of management: PROM at 32–34 wks |
Management in this gestational age category remains controversial. When there is evidence of fetal lung maturity, two trials have reported benefits to induction versus continued expectancy. In one trial, induction had several benefits, including a shorter time to delivery (14 vs. 36 hours; P < .001), shorter maternal hospital stay (2.3 vs. 3.5 days; P < .001), and less chorioamnionitis (11 vs. 28%; P = .06). Neonatal hospital stay was also shorter (6.3 vs. 7.3 days), but this difference was not significant. Although the authors found less clinically diagnosed neonatal sepsis in the induction group (28 vs. 60%; P < .003), there was no difference in confirmed sepsis (7 cases in induction group vs. 4 in expectant). There were no significant differences in the rates for cesarean delivery, postpartum infection, or neonatal survival. The other trial also found advantages to induction versus expectancy. Despite the reasons advanced by these authors, there is not yet compelling evidence to induce all pregnancies with PROM at 32 to 34 weeks simply because there is evidence of lung maturity. There is no improvement in perinatal mortality (PNM), and in other populations, induction in the presence of an unripe cervix at 32 to 34 weeks might result in higher infection rates or cesarean delivery rates. However, the evolving concern of intrauterine infection causing cerebral palsy adds strength to arguments for induction in the presence of lung maturity.
For pregnancies with PROM at 32 to 34 weeks, we have generally used expectant management. We do not routinely perform amniocentesis, but use this selectively when we suspect infection or growth restriction. We assess fetal status during expectant management with usual testing, mainly daily nonstress tests with biophysical profiles as needed for backup. In selected pregnancies at 32 to 34 weeks, we induce labor in the presence of lung maturity. Such situations include development of a favorable cervix (noted on a speculum examination) or poor patient compliance. We, of course, proceed with delivery when there are maternal or fetal indications including evidence of infection. For pregnancies with PROM at 32 to 34 weeks, we give intrapartum prophylaxis per the Centers for Disease Control and Prevention (CDC)/ACOG guidelines. We also obtain an appropriate rectovaginal culture for GBS at the time of admission, unless delivery is imminent. We then begin empirical intravenous prophylaxis until the culture result is available and is negative. If at 33 to 34 weeks the culture is positive, we will continue intravenous penicillin for 48 hours, then stop and re-culture.
PROM at 25 to 31 Weeks (Table 11.7)
|
|
|
TABLE 11.7. Summary of management: PROM at 25–32 wks |
Management in the gestational age category also remains especially controversial. For management of PROM after viability but before 32 weeks, our practice is to generally follow expectant management and proceed with delivery where there is spontaneous onset of labor or clinical evidence of infection. We follow national guidelines for intrapartum prophylaxis for prevention of GBS neonatal sepsis. For patients in whom delivery is not imminent, we also obtain an appropriate culture for GBS from the rectovaginal area. We do administer corticosteroids in a standard regimen. We also apply broad-spectrum antibiotic therapy, usually following the ampicillin/amoxicillin plus erythromycin regimen of the MFM trial. This regimen is limited to 7 days. When the patient goes into labor, we begin GBS prophylaxis unless the GBS culture was negative on admission, as recommended by the CDC. Use of tocolytics during this gestational age in patients with preterm premature rupture of the membranes remains controversial.
PROM at Less Than 25 Weeks (Table 11.8)
|
|
|
TABLE 11.8. Summary of management: PROM <25 wks |
For PROM before viability (approximately 24 weeks), several descriptive reports have demonstrated a highly variable latent period, high maternal infection rates (but with little serious morbidity), and an appreciable survival rate, especially when delivery occurs after week 24 (Table 11.9). Outcome data with expectant management of PROM in the second trimester showed perinatal survival and “intact” neurologic survival stratified by the gestational age at the time of PROM (Fig. 11.4). In sum, when gestational age occurred from weeks 14 to 19, overall survival was only 40% whereas when PROM occurred at 20 to 25 weeks, overall survival was nearly 90%. The alternative to expectant management is induction. In the patient with PROM this early in pregnancy, we individualize the decision, involving the family fully. In the proper setting, we offer expectant management.
|
|
|
TABLE 11.9. Summary of management: PROM at ≤24 wks |
|
|
|
FIG. 11.4. Outcome with expected management of second trimester PROM. (From Sweet RL, Gibbs RS. Infectious diseases of the female genital tract, fourth ed. Philadelphia: Lippincott Williams & Wilkins, 2002; with permission.) |
Chorioamnionitis Complicating PROM at Any Gestational Age (Table 11.10)
|
|
|
TABLE 11.10. Management of clinically evident chorioamnionitis |
When clinically evident chorioamnionitis is diagnosed at any gestational age, broad-spectrum antibiotics, appropriate for the array of suspected aerobes and anaerobes, should be initiated intravenously. There is no place for expectancy when intrauterine infection becomes clinically overt and preparation should be made for delivery.
SUMMARY POINTS
Management of PROM
· At or near term (35 weeks) induction is usually preferred; GBS prophylaxis is given with a positive screening culture at 35 to 37 weeks or with rupture of membranes greater than 18 hours plus an unknown culture status.
· At 32 to 34 weeks, manage by either expectancy or by induction (especially with evidence of lung maturity). Give GBS prophylaxis. Do not use tocolytics or corticosteroids.
· At 25 to 32 weeks, manage by expectancy. Give GBS prophylaxis and give corticosteroids. We give antibiotics for 7 days to prolong pregnancy. No standard regimen is established. We use ampicillin plus erythromycin most often. Use of tocolytics is controversial.
· At less than 25 weeks, manage by induction or expectancy, depending upon gestational age and patient desires. We do not use tocolytics or corticosteroids in this situation. A course of antibiotics for 7 days may prolong pregnancy as at 25 to 32 weeks.
SUGGESTED READINGS
1. Arias F, Tomich P. Etiology and outcome of low birth weight and preterm infants. Obstet Gynecol 1982;60:277.
2. Arias F, Victoria A, Cho K, et al. Placental histology and clinical characteristics of patients with preterm premature rupture of membranes. Obstet Gynecol1997;89:265–271.
3. Descavales G, Mastrogiannis D, Papadopoulos V, et al. Eur J Obstet Gynecol Reprod Biol 1995;59:143–147.
4. Farooqi A, Holmgren PA, Engberg S, et al. Survival and 2-year outcome with expectant management of second-trimester rupture of membranes. Obstet Gynecol 1998;92:895–901.
5. Fontenot T, Lewis DF. Tocolytic therapy with preterm premature rupture of membranes. Clin Perinatol 2001;28: 787–796.
6. Hannah ME, Ohlsson A, Farine D, et al. Induction of labor compared with expectant management for prelabor rupture of the membranes at term. TERMPRO Study Group. N Engl J Med 1996;334:1005–1010.
7. Harger JH, Hsing AW, Tuomala RE, et al. Risk factors for preterm premature rupture of fetal membranes: a multicenter case-control study. Am J Obstet Gynecol 1990;163:130–137.
8. Kenyon SL, Taylor DJ, Tarnow-Mordi W, et al. Broad spectrum antibiotics for preterm, prelabor rupture of fetal membranes: the ORACLE I Randomized trial. Lancet 2001;357:979.
9. Kilbride HW, Yeast J, Thibeault DW. Defining limits of survival: lethal pulmonary hypoplasia after midtrimester premature rupture of membranes. Am J Obstet Gynecol 1996;175:675–681.
10. Lee T, Silver H. Etiology and epidemiology of preterm premature rupture of the membranes. Clin Perinatol 2001;28:721–734.
11. Leitich H, Egarter C, Reisenberger K, et al. Concomitant use of glucocorticoids: a comparison of two meta-analyses on antibiotic treatment in preterm premature rupture of membranes. Am J Obstet Gynecol 1998;178:899–908.
12. Lewis DF, Brody K, Edwards MS, et al. Preterm premature ruptured membranes: a randomized trial of steroids after treatment with antibiotics. Obstet Gynecol 1996;88:801–805.
13. Lewis DF, Major CA, Towers CV, et al. Effects of digital vaginal examinations on latency period in preterm premature rupture of membranes. Obstet Gynecol 1992;80:630–634.
14. Lovett SM, Weiss JD, Diogo MJ, et al. A prospective, double blind, randomized, controlled clinical trial of ampicillin-sulbactam for preterm premature rupture of membranes in women receiving antenatal corticosteroid therapy. Am J Obstet Gynecol 1997;176:1030–1038.
15. McGregor JA, French JI, Lawellin D, et al. Bacterial protease-induced reduction of chorioamniotic membrane strength and elasticity. Obstet Gynecol1987;69:167.
16. Mercer BM, Arhearat KL. Antimicrobial therapy in expectant management of preterm premature rupture of the membranes. Lancet 1995;346:1271–1279.
17. Mercer BM, Crocker LG, Boe NM, et al. Induction versus expectant management in premature rupture of the membranes with mature amniotic fluid at 32 to 36 weeks: a randomized trial. Am J Obstet Gynecol 1993;169:775–782.
18. Mercer BM Goldenberg RL, Meis PJ, et al. The Preterm Prediction Study: prediction of preterm premature rupture of membranes through clinical findings and ancillary testing. Am J Obstet Gynecol 2000;183:738–745.
19. Mercer BM, Miodovnik M, Thurnau GR, et al. Antibiotic therapy for reduction of infant morbidity after preterm premature rupture of membranes. A randomized controlled trial. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. JAMA 1997;278:989–995.
20. Mozurkewich EL, Wolf FM. Premature rupture of membranes at term; a meta-analyses of three management schemes. Obstet Gynecol 1997;89:1035–1043.
21. NIH Consensus Development Conference Statement. Effect of corticosteroids for fetal maturation. Feb 28–March 2, 1994; Washington, DC.
22. Ohlsson A, Wang E. An analysis of antenatal tests to detect infection in preterm premature rupture of the membranes. Am J Obstet Gynecol1990;162:809–818.
23. Parry S, Strauss JF 3rd. Premature rupture of the fetal membranes. N Engl J Med 1998;338:663–670.
24. Spinnatto JA II. Maturity testing with preterm premature rupture of the membranes. Clin Perinatol 2001;28: 819–836.
25. Tan BP, Hannah ME. Oxytocin for prelabour rupture of membranes at or near term, Cochrane Database of Systematic Reviews, 2001;issue 4.
26. Tan BP, Hannah ME. Prostaglandins versus oxytocin for prelabour rupture of membranes at or near term. Cochrane Database of Systematic Reviews, 2001;issue 4.
27. The American College of Obstetricians and Gynecologists. Premature rupture of membranes. ACOG Practice Bulletin No. 1, June 1998.
28. Vidaeff AC, Ramin SM, Gilstrap LC. Antenatal corticosteroids in women with preterm premature rupture of the membranes. Clin Perinatol 2001;28:797–806.