T. Flint Porter
Morgan Peltier
D. Ware Branch
REPRODUCTIVE IMMUNOLOGY
The physiologic mechanisms that protect the fetus and its placenta from attack by the maternal immune system are complex, and many remain poorly understood. Nevertheless, the practicing obstetrician should be familiar with the immunologic aspects of the maternal–fetal relationship, as well as the profound impact that aberrations in immunologic function have on pregnancy outcome.
Fundamental Immunobiology
The primary function of the immune system is to protect against foreign pathogens, primarily by distinguishing biologic “self” from “nonself” (the clonal selection model of immunity). In the early stages of development, immune cell precursors are educated to recognize self. T cells that recognize self-antigens are killed or rendered inactive while T cells with specific receptor types against foreign pathogens continue to develop.
The immune system has two primary effector mechanisms classified as either innate or adaptive. Although they function through different mechanisms, they work together to defend the body from foreign pathogens. The innate immune response, also known as cellular immunity, is a continuous, nonspecific process that recognizes all foreign material as nonself. Components of the innate system include physical and biochemical barriers, primary effector cells such as mononuclear phagocytes, natural killer (NK) cells, and polymorphonuclear leukocytes, and circulating biochemical factors such as the complement system. Recognition of foreign pathogens by membrane receptors on effector cells is followed by phagocytic destruction and induction of apoptosis by NK cells (Fig. 18.1). One family of pathogen recognition receptors, called Toll-like receptors (Tlr), appears to play an important role in mediating the inflammatory responses in the reproductive tract. As membrane receptors on inflammatory cells, they initiate a nonspecific response to bacterial antigens and may also function to facilitate adhesion of immune cells on endothelium.
|
|
|
FIG. 18.1. Schematic view of innate and adaptive immune systems. Phagocytic cells of the innate immune system recognize foreign antigen. The foreign antigen can be a microbial pathogen, viral antigen, or tumor antigen. Innate immune responses result in direct cytotoxicity or destruction of the pathogen. Activation of the adaptive immune system depends on interaction with processed antigen provided by cells of the innate immune system. T-cell and B-cell activation results in T-cell clonal proliferation and B-cell antibody production, respectively. IL, interleukin; NK, natural killer. (From Dudley DJ. The immune system in health and disease. Balliere's Clin Obstet Gynaecol 1992;6:393.) |
As proliferating T cells mature, they differentiate into an array of subtypes that have diverse functions. CD4+ helper cells help other cells proliferate and help B cells produce antibodies. CD4+ inducer cells control the subsequent development of other T cells. CD8+ cytotoxic cells lyse foreign or virus-infected cells, and CD8+ suppressor cells prevent uncontrolled proliferation. T-cell subsets destroy and remove foreign tissues and organisms by direct binding and secretion of cytokines that recruit and activate macrophages. Cytokines are a means of communication between immune cells. Interleukin (IL)-1 is produced by macrophages and monocytes and promotes multiplication and activation of lymphocytes. IL-2, produced in response to lymphocyte activation, is the major T-cell growth factor for the proliferation of activated T cells.
The hallmark of adaptive immunity is precise specificity of antigen recognition and memory so that repeated exposures to a specific antigen elicit an enhanced immune response. The adaptive response includes several stepwise processes that occur in the lymphatic system (see Fig. 18.1). The primary adaptive effector cells are B cells, precursors of plasma cells that secrete specific antibodies that circulate through the bloodstream and destroy target cells in concert with complement or antibody-dependent cellular cytotoxic cells. Antibodies are heterogeneous proteins produced by gene rearrangement, a process that creates myriad possible immunoglobulin antigen-recognition sites. The first antibody to respond is immunoglobulin M (IgM), which is soon superseded by a predominantly immunoglobulin G (IgG) response.
Cells of the innate immune system act as secondary effector cells in the adaptive response through T-cell recognition of HLA antigens, which are products of the major histocompatibility complex (MHC) located on the short arm of chromosome 6 (Fig. 18.2). Class I MHC antigens are expressed by nearly all nucleated cells and are identified by cytotoxic T cells. Class II MHC antigen expression is restricted to B cells, monocytes, macrophages, and activated T cells but is important for presenting antigen to helper T cells.
|
|
|
FIG. 18.2. Chromosomal location of the major histocompatibility complex. Within the complex are genes that encode as follows: for class I antigens (HLA-A, HLA-B, and HLA-C); for several components of the complement cascade, including complement components 2 and 4 and factor B, some of which are located at position C; and for class II antigens. (From Scott JR, Rote NS, eds. Immunology in obstetrics and gynecology. Norwalk, CT: Appleton-Century-Crofts, 1985:35.) |
Embryologic Development of the Immune System
The development of the immune system begins at conception and continues throughout pregnancy and into the newborn period. During weeks 2 and 3 of gestation, pluripotential yolk sac stem cells form the precursors for all the blood cell series. The thymus develops in the human embryo at 6 weeks gestation, and lymphocyte differentiation proceeds in the absence of foreign antigens. Small lymphocytes appear in the peripheral blood at week 7 and around lymphocyte plexuses by week 8. As early as 13 weeks gestation, T cells that can respond to mitogens and recognize histoincompatible cells begin to appear. By 20 weeks gestation, the human fetus has the ability to respond to congenital infections by producing plasma cells and antibodies.
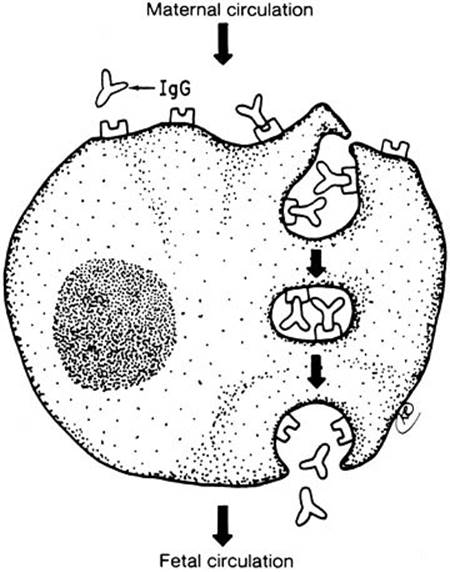
The presence of an intact trophoblastic cellular barrier prevents the movement of large numbers of immunocompetent cells into or out of the fetus during pregnancy. In contrast, maternal IgG, by virtue of its Fc fragment, is specifically selected for placental transfer (Fig. 18.3). Fetal IgG concentrations are about 10% of adult levels by the middle of the first trimester (Fig. 18.4). Adequate humoral immunity in the neonatal period depends on the circulating immunoglobulins that have crossed the placenta, and fetal blood levels of IgG reflect maternal levels. The specific antibody protection depends on the mother's own antigenic experience. The primary role of maternal antibodies is to protect the neonate from infections. However, several maternal autoimmune disorders are characterized by production of IgG antibodies and can be harmful to the infant.
|
|
|
FIG. 18.3. The transport of maternal immunoglobulin G (IgG) across the trophoblast and into the fetal circulation is an active process. Maternal IgG binds to Fc receptors on the surface of the trophoblast and is internalized into vacuoles. These receptors are specific for the Fc portion of IgG and do not bind other classes of immunoglobulins. The interaction of IgG with the receptors probably protects the antibody from digestion during the transport of the vacuole across the cell. On the fetal side, IgG is released into the fetal circulation. (From Scott JR, Rote NS, eds. Immunology in obstetrics and gynecology. Norwalk, CT: Appleton-Century-Crofts, 1985:70.) |
|
|
|
FIG. 18.4. Levels of antibody in the cord blood and neonatal circulation. Early in gestation, maternal immunoglobulin G (IgG) crosses the placenta and enters the fetal circulation. At the time of birth, the fetal circulation normally contains a near-adult level of IgG, which is almost exclusively maternal, and small amounts of fetal immunoglobulin M and immunoglobulin A. After delivery of the child, maternal IgG is rapidly catabolized, whereas neonatal IgG production increases. (From Scott JR, Rote NS, eds. Immunology in obstetrics and gynecology. Norwalk, CT: Appleton-Century-Crofts, 1985:69.) |
Pathogenesis of Autoimmune Disease
The immune system is normally regulated so that cells capable of producing an immune response to self-antigens are suppressed. Activation of innate immunity requires two separate signals from a presenting antigen to T cells. The first signal is produced through the recognition of the MHC antigen on presenting cells. The second signal is through CD28 expressed on the T cell and CD80 or CD86, which are expressed on the activated antigen-presenting cell. If only one signal is received, the T cell is rendered anergic or unresponsive to further activation even if both signals are given at a later time.
Autoimmune diseases result from a breakdown in normal regulatory mechanisms that lead to an inability to discriminate between self and nonself. Autoimmunity is characterized by persistent activation of immunologic mechanisms that affect the function and integrity of certain cells and organs. The process may be initiated by environmental agents but is probably sustained by persistent T-cell activation that overrides normal tolerance of self-antigens. Autoimmune diseases have a predilection for women of reproductive age and are often encountered during pregnancy. The effects of pregnancy on autoimmunity appear to depend on whether the autoimmune disease is innate (cellular) or adaptive (humoral) in nature. Diseases with strong cellular pathophysiology, such as rheumatoid arthritis and multiple sclerosis, are associated with remission during pregnancy whereas diseases characterized by autoantibody production, such as lupus and Graves disease, are more severe in pregnancy.
Maternal–Fetal Immunology
Maternal immunologic reaction to the genetically dissimilar cells of the conceptus begins at fertilization and continues throughout pregnancy as differentiated fetal trophoblast cells interact with maternal uterine tissue and blood. The normal relationship between mother and fetus appears to be healthy and growth-promoting rather than the usual allogeneic model of destruction.
Several mechanisms likely play a role in protection of the fetus from immunologic damage. Circulating blocking factors have been theorized to attenuate maternal immunologic reaction. One progesterone-induced blocking factor suppresses production of lymphocytes and pro-inflammatory cytokines. In addition, so-called blocking antibodies may prevent lymphocytic destruction by binding to receptors on fetoplacental tissues. Alternatively, blocking antibodies may be directed against antigen-specific combining sites (idiotypes) on maternally produced antibodies that prevent them from assisting lymphocytes in targeting cells on the conceptus. While the concept is appealing, the relevance of blocking antibodies and other alleged circulating pregnancy-maintaining factors remains unsettled. Not only do agammaglobulinemic women without antibody production have normal pregnancies, antibodies do not frequently appear until late in the first or second trimester of the first pregnancy.
Immunotolerance during pregnancy probably results from interactions at the local maternal–fetal interface rather than from generalized maternal immunosuppression. Before conception, endometrial stromal cells transform into decidual cells that contain T-cell subtypes with immunosuppressive activity. One T-helper cell subset secretes cytokines that are beneficial or neutral to the presence of the fetus. Another is thought to prevent colonization with microbial pathogens. Additional evidence suggests that some subsets of the decidual T cells promote growth of the placenta through the secretion of cytokines that suppress inflammation. Hormones, enzymes, growth factors, and endometrial proteins within maternal decidual tissue also have potent immunomodulatory properties that promote a favorable interaction between the conceptus and the mother.
The presence of large granular lymphocytes in luteal phase and early to mid-pregnancy deciduas has generated considerable interest among reproductive immunologists. Under normal circumstances, these nonspecific innate immune effector cells, similar to NK cells, kill standard NK cell targets with the notable exception of trophoblastic cells. Their absence or alteration has been associated with pregnancy loss.
The placenta also plays an active role in protection of the fetus from maternal immune responses. Villous cytotrophoblasts and syncytiotrophoblasts escape destruction because both express nonclassic MHC antigens that prevent trophoblast destruction through inhibition of lysis by activated NK cells, limitation of leukocyte cytotoxic activity, suppression of pro-inflammatory cytokine production, and induction of T-cell death. Nonclassic MHC antigens also promote trophoblast proliferation and invasion. Altered expression of nonclassic MHC antigens has been linked to recurrent miscarriage and preeclampsia.
Placental expression of a protein known as the Fas ligand may also play a role in pregnancy success through selective deletion of antifetal T-cell clones. In animal studies, binding to the Fas ligand causes death and removal of autoreactive T cells.
The placenta may also inhibit T-cell proliferation by sequestering nutrients. Placental indolamine 2,3-dioxidase (IDO) inactivates the amino acid tryptophan that is essential for the proliferation of T cells. The role of IDO in recurrent pregnancy loss in humans has not yet been widely investigated.
ERYTHROBLASTOSIS FETALIS
Though the first description of erythroblastosis fetalis (hemolytic disease of the newborn) dates back to the 1609, it was not until the early 1900s that the role of alloimmunization in the pathogenesis of erythroblastosis was established. The early investigators determined that an Rh–negative mother becomes alloimmunized by exposure to Rh–positive fetal erythrocytes during pregnancy or delivery. Maternally produced anti-erythrocyte antibodies pass through the placenta to the fetus where they react with the Rh–positive fetal erythrocytes, causing their destruction. In the past, Rh alloimmunization has also been referred to as sensitization and immunization. The terms alloimmunization and sensitization will be used interchangeable in this text.
Many other erythrocyte antigens have been described since the discovery of the Rh antigen but only a few are clinically important causes of maternal alloimmunization. However, with the widespread use of Rh–immunoglobulin prophylaxis and the decline in Rh-D alloimmunization, the overall importance of the “minor antigens” in red cell alloimmunization has increased.
Genetics of the Rh Antigen
The Rh blood group was so named because rabbits immunized with rhesus monkey erythrocytes produced an antibody that agglutinated erythrocytes from 85% of whites. The so-called Rh factor is actually an antibody directed against an erythrocyte surface antigen of the rhesus blood group system. The Rh blood group system has a high degree of polymorphism, with five major antigens and many variant minor antigens. While three systems of nomenclature have been suggested, the Fisher-Race system is probably best suited to understanding the inheritance of the Rh antigen and the clinical management of Rh alloimmunization. It assumes the presence of three genetic loci, each with two major alleles, lettered C, c, D, E, and e. No antiserum specific for a ″d″ antigen has been found.
The Rh gene complex is described by the three appropriate letters with eight possible combinations (listed in decreasing order of frequency among whites): CDe, cde, cDE, cDe, Cde, cdE, CDE, and CdE. Genotypes are indicated as pairs of gene complexes, such as CDe/cde. Certain genotypes, and thus certain phenotypes, are more prevalent than others. Although the alleles are always written in the order C(c), D, E (e), the actual order on chromosome one is of the genes coding for the antigens D, C(c), E (e). Anti–C, anti–c, anti–D, anti–E, and anti–e designate specific antibodies directed against the respective antigens. Because the majority of Rh alloimmunization resulting in overt clinical disease results from incompatibility with respect to the D antigen, common convention holds that Rh-positiveindicates the presence of the D antigen and Rh-negative indicates the absence of D antigen on erythrocytes.
Unique Rh antibodies have been used to identify more than 30 antigenic variants in the Rh blood group system, the most common of which is the Du antigen, now commonly referred to as weak D. This heterogeneous group of clinically important D-antigen variants is most often found in blacks. At least some weak D–positive patients are capable of producing anti–D, which could presumably result in a weak D–positive mother becoming sensitized to her D–positive fetus, but such an occurrence is exceedingly rare.
The Rh-D antigen appears very early in embryonic life and has been demonstrated on the red blood cells of a 38-day-old fetus. Its precise function is unknown, though it may play a role in maintaining red cell membrane integrity or regulate the asymmetric distribution of different phospholipids through the red cell membrane.
Pathophysiology of Rh Alloimmunization
Rh alloimmunization can only occur in the presence of three conditions:
1. The fetus must have Rh–positive erythrocytes, and the mother must have Rh–negative erythrocytes.
2. The mother must have the immunogenic capacity to produce antibody directed against the D antigen.
3. A sufficient number of fetal erythrocytes must gain access to the maternal circulation.
Incidence of Rh-D Incompatibility and Subsequent Alloimmunization
About 15% of whites, 5% to 8% of blacks, and 1% to 2% of Asians and Native Americans are Rh-D–negative. In terms of risk, an Rh–negative woman has about an 85% chance of mating with an Rh–positive man, 60% of whom are heterozygous and 40% of whom are homozygous at the D locus. Assuming that one-half of the conceptions of heterozygous men will be Rh-D–positive, the chance of an Rh–positive man producing an Rh–positive fetus is about 70%. An Rh–negative woman has about a 60% chance of bearing an Rh–positive fetus (0.85 × 0.70). About 10% of pregnancies are Rh-incompatible (0.15 × 0.60). However, fewer than 20% of Rh–incompatible pregnancies result in alloimmunization because fetomaternal hemorrhage sufficient to trigger a maternal antibody response does not occur in every case. About 16% of untreated Rh–negative women become alloimmunized in their first Rh–incompatible (ABO–compatible) pregnancy. Half produce detectable anti–D antibody within 6 months of delivery while the rest have undetectable amounts until early in the next incompatible pregnancy. Overall, even before the introduction of Rh–immunoglobulin prophylaxis, only about 1% of pregnant women had anti–D antibody.
Maternal Immunologic Response
The probability and severity of Rh-D alloimmunization varies depending on individual patient characteristics. As many as 30% of Rh–negative individuals appear to be immunologic “nonresponders” who will not become sensitized. In addition, ABO incompatibility diminishes the risk of alloimmunization to about 1.5% to 2.0% after the delivery of an Rh–positive fetus. This is possibly due to rapid clearance of ABO–incompatible fetal cells from the maternal circulation or alteration or damage to the fetal Rh antigen so that it is no longer immunogenic. The effect is most pronounced if the mother is type O and the father is type A, B, or AB.
Fetomaternal Hemorrhage
Fetal red cells may gain access to the maternal circulation during pregnancy, delivery, and the immediate postpartum period. Fetomaternal hemorrhage in a volume sufficient to cause alloimmunization is most common at delivery, occurring in 15% to 50% of births. The amount of fetal blood entering the maternal circulation is usually less than 0.1 mL but may be greater than 30 mL in 0.2% to 1% of cases. Risk factors for excessive postpartum fetomaternal hemorrhage include cesarean delivery, multiple gestations, bleeding placenta previa or abruption, manual removal of the placenta, and intrauterine manipulation. However, the majority of cases of excessive fetomaternal hemorrhage occur after uncomplicated vaginal delivery.
Antepartum events can also result fetomaternal hemorrhage in sufficient volume to cause in alloimmunization in 1% to 2% of cases, even without obvious disruption of the choriodecidual junction (Table 18.1). Fortunately, asymptomatic antepartum sensitization rarely occurs before the third trimester.
|
|
|
TABLE 18.1. Antepartum events associated with fetomaternal hemorrhage |
Rh-D Immunoglobulin
The prevention of alloimmunization to a specific antigen by the passive administration of antibody is termed antibody-mediated immune suppression. In the case of Rh-D alloimmunization, a high degree of protection was first achieved by administering anti–D immunoglobulin (Rh-D immunoglobulin) to Rh–negative male volunteers who had been infused with Rh–positive red cells. It was later established that the amount of Rh-D immunoglobulin necessary to prevent alloimmunization varies according to the size of fetomaternal hemorrhage:
· 300 g of Rh-D immunoglobulin for exposure to 10 mL of fetal blood
· 20 g of Rh-D immunoglobulin for exposure to 1 mL of fetal erythrocytes
· 10 g of Rh-D immunoglobulin for 1 mL of whole fetal blood.
Postpartum Alloimmunization Prophylaxis
The early Rh-D alloimmunization prevention trials found that administration of Rh-D immunoglobulin within 72 hours of delivery reduced alloimmunization to less than 1.5% in Rh–negative women, a seven- to ten-fold decrease in alloimmunization compared with untreated controls. Although 300 g of Rh immunoglobulin was used (and continues to be the standard in the United States), it has subsequently been shown that a dose of 100 g to 150 g is probably adequate for routine use.
Rh-D immunoglobulin must be given as soon as possible after exposure to Rh-D–positive blood (delivery or other event associated with fetomaternal hemorrhage) before the primary immune response is established. While 72 hours is the standard recommendation, it is an artifact from the early studies performed using inmates, during which prison officials would allow visits only at 3-day intervals. Prophylaxis beyond 3 days has never been extensively studied but if for some reason Rh–immune prophylaxis does not occur within 72 hours after exposure, susceptible Rh-D–negative women should be treated up to 14 to 28 days. Further, if the neonatal Rh status is unknown 3 days after delivery, Rh immunoglobulin should be given rather than waiting for the neonatal results.
Antepartum Alloimmunization Prophylaxis
One to two percent of susceptible Rh-D–negative women become sensitized during pregnancy in spite of postpartum Rh-D–immune prophylaxis. Most failures can be attributed to antepartum fetomaternal hemorrhage that is often not clinically apparent. Prophylactic administration of Rh-D immunoglobulin at 28 weeks gestation reduces the incidence of alloimmunization from 1.8% to 0.1%. Initial concerns about potential adverse effects of antenatal Rh-D–immune prophylaxis have been refuted by decades of experience with Rh-D immunoglobulin without reports of maternal or fetal complications. Further, routine antepartum prophylaxis is much less expensive than the neonatal intensive care required for severely anemic infants.
Management of the Unsensitized Rh–Negative Pregnant Woman
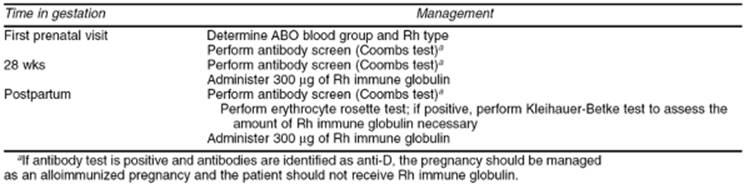
Prenatal care for Rh-D–negative women, without evidence of alloimmunization is straightforward (Table 18.2). Every woman should have her ABO blood group, Rh type, and antibody screen checked at the first prenatal visit of all pregnancies. If she is Rh-negative or weak D–negative and has no demonstrable antibody, she is a candidate for 300 g Rh–immunoglobulin prophylaxis at around 28 weeks gestation and again immediately postpartum. The American Association of Blood Banks recommends obtaining another antibody screen before administration of Rh immunoglobulin, including antepartum prophylaxis.
|
|
|
TABLE 18.2. Evaluation and management of an unsensitized Rh-negative, pregnant woman |
After delivery, another antibody screen is routinely performed. If negative and the newborn is Rh-D–positive or weak D–positive, alloimmunized women should be given 300 g of Rh-D immunoglobulin. In addition, because up to 1% of deliveries result in a fetomaternal hemorrhage greater than 30 mL (the largest volume of fetal blood adequately covered by a standard 300-g dose of Rh immunoglobulin), a screen for “excessive” fetomaternal hemorrhage should be performed. Most laboratories use the erythrocyte rosette test, a simple and sensitive method for detecting fetomaternal bleeding. If the rosette test is positive, the volume of fetal red cells in the maternal circulation can be calculated using the Kleihauer-Betke test. If the volume of fetomaternal hemorrhage is greater than 30 mL whole blood, an additional 10g of Rh immunoglobulin should be administered for each additional milliliter of fetal blood.
A weak D–positive mother who delivers an Rh–positive infant is not at significant risk of Rh sensitization, probably because the weak D antigen is actually an incompletely expressed D antigen. Therefore, weak D–positive mothers usually do not require Rh immunoglobulin. Occasionally a woman previously typed as Rh-negative is unexpectedly found to be weak D–positive during pregnancy or after delivery. In this situation, the clinician should be suspicious that the patient's “new” weak D–positive status is actually due to a large number of Rh–positive fetal cells in the maternal circulation. Appropriate diagnostic studies should be performed, and if fetomaternal hemorrhage is found, the mother should be treated with Rh immunoglobulin.
Several antepartum complications and procedures may also result in fetomaternal hemorrhage (see Table 18.1). First trimester complications, including spontaneous miscarriage, elective abortion, and ectopic abortion, may result in fetomaternal hemorrhage sufficient to result in alloimmunization.
Fetomaternal hemorrhage has also been demonstrated in up to half of women with threatened first trimester miscarriage but is only occasionally associated with alloimmunization. Management is controversial with no clear consensus or evidence-based recommendation on use of Rh immunoglobulin.
An Rh–negative, unsensitized patient who has antepartum bleeding or suffers an unexplained second or third trimester fetal death should receive Rh–immunoglobulin prophylaxis and be evaluated for the possibility of massive fetomaternal hemorrhage. Several procedures may also result in fetomaternal hemorrhage sufficient to cause alloimmunization including chorionic villus sampling, amniocentesis, and external cephalic version.
For first trimester pregnancy complications and procedures, 50 g of Rh immunoglobulin is protective. Beyond 12 weeks, a full 300-g dose is indicated even if in the absence of detectable hemorrhage. In addition, because excessive fetomaternal hemorrhage may occur with any complication or procedures performed in the second and third trimester, an assessment of the volume of fetal whole blood should be performed and the appropriate amount of Rh-D immunoglobulin should be given.
Failure to administer Rh immunoglobulin when indicated is responsible for one-fourth of new cases of alloimmunization. This inexcusable oversight may be due to:
· failure to type the patient's blood at the first prenatal visit or to order Rh-D immunoglobulin when indicated
· error in transmitting the proper blood type to the mother's chart and to the physician
· error in typing the mother's, father's, or baby's blood
· failure to administer Rh-D immunoglobulin when ordered
· unrecognized fetomaternal hemorrhage during pregnancy
· inadequate Rh-D-immunoglobulin for the volume of fetomaternal hemorrhage
· patient refusal.
Management of the Rh-D–Alloimmunized Pregnancy
Obstetric History
A well-documented obstetric history is essential to guide management of alloimmunized pregnancy. Fetal hemolytic disease tends to become more severe in subsequent pregnancies. If hydrops occurred in a previous pregnancy, the next Rh–incompatible fetus has an 80% to 90% chance of becoming hydropic as well. With this in mind, patients are grouped into one of three categories:
· mildly affected fetuses, which can be allowed to remain in utero until they have achieved pulmonary maturation
· moderately affected fetuses, which may need to be delivered before pulmonary maturity but who do not need fetal treatment
· severely affected fetuses, which require active intervention to reach a gestational age at which the risks of delivery and neonatal intensive care are less than the risks of in utero therapy.
In general, hemolysis and hydrops develop at about the same time or somewhat earlier in subsequent pregnancies; this can be used as a rough guide for timing initial fetal studies and transfusions. Fetal hydrops seldom develops in a first sensitized pregnancy.
Maternal Antibody Titers
Severe erythroblastosis or perinatal death does not occur if antibody levels remain below 1:16. Some centers use an anti–D titer of 1:8 because of variations in reliability and methods of titration. In general, women with anti–D titers of 1:8 or less, and no history of a previously affected infant, can be safely followed with anti–D titers every 2 to 4 weeks and serial fetal ultrasound assessment. Those with anti–D titers of 1:16 or greater should be referred for amniocentesis.
Once the critical anti–D antibody titer has been reached in a sensitized pregnancy, more antibody titers are not useful in the current pregnancy or subsequent pregnancies. Titers may remain stable in up to 80% of severely affected pregnancies. Variability between maternal antibody levels and severity of fetal disease is explained by the fact that antibody concentration is only one factor influencing the degree of anemia. Other factors include antibody subclass and degree of glycosylation, placental transfer of antibody, antigen expression on fetal erythrocytes, functional maturity of the fetal reticuloendothelial system, and the presence of HLA-related antibodies that inhibit fetal erythrocyte destruction.
Determination of the Fetal Antigen Status
The possibility that the fetus is Rh-negative (not at risk) should always be considered. A reasonable first step in this process is to determine paternal Rh–antigen status and zygosity:
· If the father is Rh-negative, the fetus must also be Rh-negative and no further testing is necessary.
· If the father is Rh-positive, but has previously fathered Rh–negative children, he is heterozygous and the probability that this fetus is Rh-negative is 50%.
· If the father is Rh-positive without other Rh–negative children, zygosity can be established using either DNA analysis or Rh antisera. If the father is homozygous, this fetus is Rh-positive and no other testing is necessary.
In the past, determination of fetal blood type required direct analysis of fetal blood obtained by umbilical cord blood sampling with its attendant risks of fetal loss and fetomaternal hemorrhage. The development of DNA tests that use polymerase chain reaction (PCR) has made it possible to determine fetal Rh status from uncultured amniocytes obtained from as little as 2 mL of amniotic fluid or 5 mg of chorionic villi. Though highly accurate, DNA testing for fetal Rh status is equivocal in about 1% of cases, probably because of the presence of gene rearrangements near the Rh-D locus that can be missed by standard DNA primers used for PCR. Most laboratories recommend simultaneous testing of paternal blood and amniotic fluid.
Fetal antigen testing from amniocytes has become routine at most centers in the United States. Most alloimmunized women have fetal antigen typing at the time of the first amniocentesis for amniotic fluid bilirubin analysis. Alloimmunized women having chorionic villus sampling (CVS) or second trimester amniocentesis for other unrelated conditions can have fetal antigen typing earlier. However, except for patients with severe Rh sensitization who would consider termination of an Rh–positive pregnancy, CVS and amniocentesis are not usually offered for detection of Rh-D fetal antigen status alone. If the DNA test indicates an Rh–negative fetus, the small likelihood of misdiagnosis should be discussed and the patients offered standard antenatal surveillance. In the future, fetal Rh–antigen status will likely be performed on fetal cells obtained from the maternal circulation or by preimplantation genetics.
Amniotic Fluid Optical Density Analysis
Assessment of amniotic fluid in Rh alloimmunization is based on the original observations that spectrophotometric determinations of amniotic fluid bilirubin correlated with the severity of fetal hemolysis. A by-product of fetal hemolysis, bilirubin is excreted into the amniotic fluid through fetal pulmonary and tracheal secretions and by diffusion across the fetal membranes and the umbilical cord. Using a semilogarithmic plot, the curve of optical density of normal amniotic fluid is approximately linear between wavelengths of 525 and 375 nm. Bilirubin causes a shift in the spectrophotometric density with a peak at a wavelength of 450 nm. The amount of shift in optical density from linearity at 450 nm (the ΔOD450) is used to estimate the degree of fetal red cell hemolysis (Fig. 18.5).
|
|
|
FIG. 18.5. Spectrophotometric scan of amniotic fluid containing bilirubin. An arbitrary line (thick line) has been drawn to show where the scan would have been traced if there had been no increase in bilirubin. The peak absorption of bilirubin occurs at 450 µm. The difference between the peak and the arbitrary line equals 0.204. |
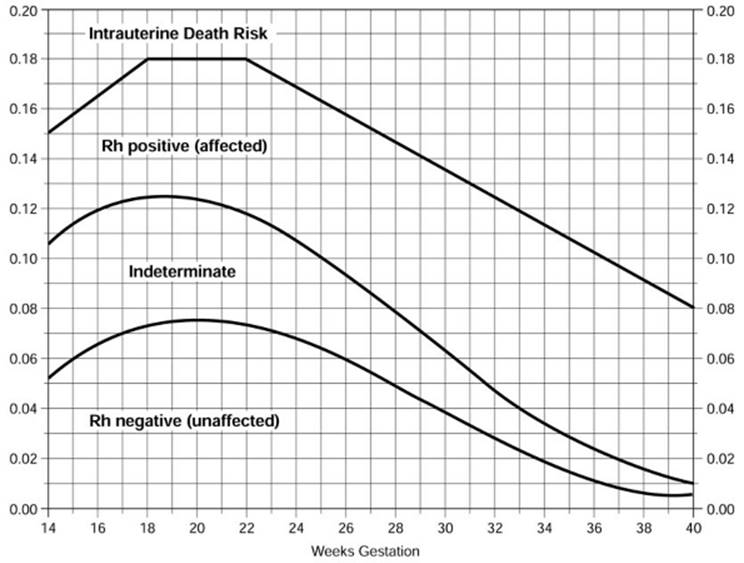
Liley was the first to correlate amniotic fluid ΔOD450 values with newborn outcome by dividing a semilogarithmic graph of gestational age versus ΔOD450 into three zones (Fig. 18.6). Unaffected fetuses and those with mild anemia had ΔOD450 values in zone I (the lowest zone), while severely affected fetuses had ΔOD450 values in zone III (the highest zone). Fetuses with zone II values (the middle zone) had disease ranging from mild to severe, indicated primarily by the trend of the determinations of amniotic fluid bilirubin. Because there is a tendency for amniotic fluid bilirubin to decrease as pregnancy advances, the boundaries of the zones slope downward as gestational age increases. Implementation of Liley's method reduced perinatal mortality from 22% to 9% over a 5-year period.
|
|
|
FIG. 18.6. This form is used to record serial data on each Rh-immunized patient. The modified Liley graph is divided into three zones to predict the outcome of the pregnancy in terms of umbilical cord blood hemoglobin, intrauterine deaths, or unaffected fetuses. |
A single ΔOD450 measurement is seldom helpful in the management of alloimmunized pregnancies unless it is very high or very low. Instead, serial amniocenteses should be performed to determine the trend of ΔOD450 values over time. Amniotic fluid ΔOD450 values trend downward in unaffected and mildly affected infants while values from severely affected fetuses show a mixed pattern of higher values. A horizontal or rising trend is ominous and indicates the need for intervention either by intrauterine transfusion (IUT) or delivery.
The usefulness of third trimester measurements of amniotic fluid bilirubin using ΔOD450 determinations has been confirmed by decades of clinical experience. There have also been attempts to extrapolate Liley's original graph backward to assess fetal status before 27 weeks gestation. However, ΔOD450 measurements in the second trimester tend to be less reliable predictors of true fetal anemia because of wide physiologic variation in concentrations of amniotic fluid bilirubin. Laboratory techniques, including chloroform extraction to remove blood and meconium from amniotic fluid, appear to improve the accuracy of second trimester ΔOD450 measurements. Still, umbilical cord blood sampling remains the most accurate method of fetal assessment during the second trimester in severely alloimmunized pregnancies. Unfortunately, it is often impractical because of the technical expertise and clinical support required to avoid an unacceptably high rate of pregnancy loss.
Enthusiasm for second trimester measurement of concentrations of amniotic fluid bilirubin has grown in recent years. One approach uses a curve developed by Queenan (Fig. 18.7), which, like Liley's original curve, plots ΔOD450 measurements against gestational age. The Queenan curve has four outcome zones which predict the degree of fetal anemia and guide management. Alternatively, others have simply extended Liley's original zones backward with some success. Recognizing that this issue is not completely settled, one reasonable approach is to use the standard semilogarithmic Liley curve for amniotic fluid assessment, extrapolated linearly back to 24 weeks gestational age (see Fig. 18.6). Clinical management is then based on trends rather than single ΔOD450 values, taking history and gestational age into consideration.
|
|
|
FIG. 18.7. The Queenan curve plots ΔOD450 measurements against gestational age, dividing them into four zones of fetal risk. This curve allows prediction of the degree of fetal hemolysis from 14 weeks gestation until term. (Adapted from Queenan JT, Tomai TP, Ural SH, et al. Am J Obstet Gynecol1993;168:1370–1376.) |
Fetal Blood Analysis
Ultrasound-guided umbilical cord sampling (cordocentesis) should be performed to assess the degree of fetal anemia in severely alloimmunized pregnancies. The procedure is successful in greater than 95% of cases with fetal loss rates between 0.5% and 2% per procedure. Fetomaternal bleeding may occur at the time of cordocentesis resulting in worsened maternal alloimmunization. Traversing an anterior placenta with the sampling needle is thought to result in increased sensitization in as many as 50% of cases. Other complications have also been described including acute refractory fetal distress, umbilical cord hematoma, amnionitis with maternal adult respiratory distress syndrome, and placental abruption.
The role of cordocentesis in the management of alloimmunization is limited to assessment of those fetuses already known to be antigen-positive and who are suspected of having moderate to severe anemia. Because of the technical difficulty and increased hazard (both immediate and remote) associated with the procedure, umbilical cord blood sampling should be used with caution and performed only by properly trained personnel.
Ultrasound and Doppler Studies
Ultrasonographic examination of the fetus has become an extremely important adjunct in the management of the Rh–alloimmunized pregnancy, primarily as a guide for amniocentesis, cordocentesis, and IUT. Sonographic fetal findings have also been studied in an effort to identify those with severe anemia and reduce the need for invasive procedures. However, other than identifying frank hydrops, ultrasound is not sufficiently reliable in distinguishing mild from severe hemolytic disease.
Doppler flow velocity waveforms of fetal cardiac output and red cell flow in numerous fetal blood vessels have been extensively investigated as noninvasive predictors of fetal anemia. Doppler flow waveforms of the fetal middle cerebral artery (MCA) have shown the most promise in the management of Rh–alloimmunized pregnancies. Several investigators have reported that fetal MCA peak systolic velocity waveforms consistently identify fetuses with moderate or severe anemia when velocities are greater than 1.5 times the median of values derived from normal controls (Fig. 18.8). New protocols are emerging at many centers that use fetal MCA peak systolic velocity values to guide management of alloimmunized pregnancies in a manner similar to traditional amniotic fluid protocols using amniotic fluid ΔOD450 values. As more clinical experience is gained, it seems likely that this noninvasive tool may become routinely employed to direct fetal management.
|
|
|
FIG. 18.8. Peak velocity of systolic blood flow in the middle cerebral artery in 111 fetuses at risk for anemia due to maternal red-cell alloimmunization. Open circles indicate fetuses with either no anemia or mild anemia (0.65 multiples of the median hemoglobin concentration). Triangles indicate fetuses with moderate or severe anemia (<0.65 multiples of the median hemoglobin concentration). The solid circles indicate the fetuses with hydrops. The solid curve indicates the median peak systolic velocity in the middle cerebral artery, and the dotted curve indicates 1.5 multiples of the median. (From Mari G, Deter RL, Carpenter RL, et al. N Engl J Med 2000;342:9–14.) |
Intrauterine Transfusion in Rh–Alloimmunized Pregnancies
Determining the Need for Transfusion
The goals of IUT are to correct fetal anemia in an effort to improve fetal oxygenation and to reduce extramedullary hematopoietic demand which, in turn, should result in a fall in portal venous pressure and improved hepatic function. The need for cordocentesis and IUT should be determined by obstetric history, clinical findings, and the experience and expertise of the management team.
About one-half of susceptible infants of Rh–immunized pregnancies have mild to moderate hemolytic disease and do not require IUT or extensive extrauterine therapy. Reasonable management for these patients includes serial ultrasound examinations of the fetus every 2 to 4 weeks from 20 weeks gestation until delivery and serial amniotic fluid ΔOD450 determinations, with the first amniocentesis at 24 to 28 weeks gestation. The timing of the next amniocenteses or need for IUT or delivery depends on the trend in ΔOD450 values (Fig. 18.9). If ΔOD450 values fall within the low zone or the lower half of the middle zone on the Liley graph, amniocentesis is repeated every 2 to 4 weeks. Severe anemia is suspected when the ΔOD450 values rise into the upper fourth of the middle zone or into zone III, especially before 30 weeks gestation. Depending on the clinical situation, a single ΔOD450 value in zone III may also be an indication of severe anemia. If ultrasound reveals any evidence of fetal hydrops, severe fetal anemia (hematocrit <15%) can be assumed and cordocentesis and IUT should be arranged immediately.
|
|
|
FIG. 18.9. Relative risks of pregnancy loss in women with antiphospholipid syndrome after treatment. Closed circles represent the relative risk of pregnancy loss after treatment with heparin and low-dose aspirin. Horizontal lines represent range of 95% confidence interval. |
A history of severe alloimmunization with early hemolysis and fetal hydrops is predictive of a similarly bad outcome in the current pregnancy. Fetal survival may depend on identifying severe anemia earlier than 24 weeks gestation. Either the Queenan curve or extrapolation of the Liley curve can be used to guide management, understanding that single ΔOD450 values between 18 and 24 weeks are difficult to interpret and that trends in ΔOD450 determinations are more accurate indicators of fetal anemia. In general, ΔOD450 values below 0.09 suggest an unaffected or mildly affected fetus while those greater than 0.15 suggest fetal anemia. In the occasional patient with a particularly ominous history of early second trimester disease or previous severe disease with misleading ΔOD450 values, cordocentesis to determine the fetal hematocrit is a reasonable first step. At any gestational age, fetal hydrops should be considered evidence of severe fetal anemia and cordocentesis with immediate intravascular transfusion is indicated.
Intraperitoneal Intrauterine Transfusion
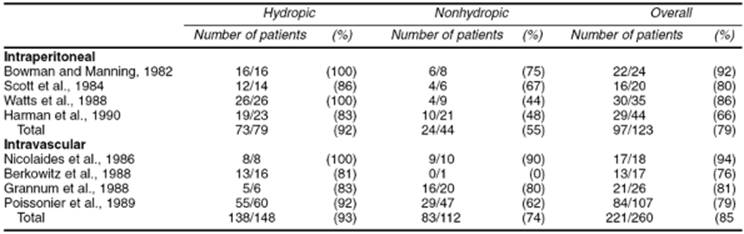
Intraperitoneal transfusions were the mainstay of IUT therapy until the mid-1980s. Placement of erythrocytes in the fetal peritoneal cavity was found to reduce fetal anemia by gradual uptake of transfused red cells into the fetal circulatory system via subdiaphragmatic lymphatics. Success depended on the gestational age and the severity of fetal disease, particularly with regard to fetal hydrops (Table 18.3).
|
|
|
TABLE 18.3. Neonatal survival of infants with severe Rh alloimmunization treated with intrauterine transfusions |
The routine use of ultrasound for needle guidance has dramatically reduced the procedure-related morbidity and mortality associated with intraperitoneal transfusion. Confirmation of appropriate needle placement is usually straightforward, but inadvertent transfusion into the bowel, liver, abdominal wall, and retroperitoneum may occur. Infection, premature rupture of the membranes, refractory preterm labor, and fetal distress necessitating immediate delivery are potential hazards of intraperitoneal IUT. The procedure should be performed only in well-equipped centers with appropriately trained personnel.
Intrauterine Intravascular Transfusion
Direct access to the fetal circulation for transfusion offers several advantages over the intraperitoneal approach. The initial fetal hematocrit can be measured, allowing a more precise calculation of the volume of blood required for transfusion. In some cases, the fetus will have a higher hematocrit than expected and transfusion can be delayed. A post-transfusion hematocrit can also be obtained to determine whether the transfusion was adequate and when the next one should be scheduled. Further, transfusion into the fetal vascular system ensures complete uptake with a more rapid correction of fetal anemia, especially important for hydropic fetuses that often do not adequately absorb intraperitoneally transfused erythrocytes.
Disadvantages of intravascular fetal transfusion include the rare possibility of volume overload in the compromised fetus, procedure-related complications, and the risk of increasing the severity of maternal sensitization due to fetomaternal hemorrhage. The perinatal survival of nonhydropic fetuses exceeds 90%, and approximately 75% of hydropic fetuses survive with intravascular transfusion (see Table 18.3).
Several different methods of estimating the volume of blood needed for transfusion have been reported with a goal of keeping the post-transfusion hematocrit at 40% to 45%. Following intravascular transfusion, the decline in the donor hematocrit is most dependent on the life span of the donor erythrocytes, the rate of fetal growth (and increased vascular volume), and the ratio of fetal to donor erythrocytes (since the fetal erythrocytes are subject to continued hemolysis). The latter is most influential between the first and second intravascular transfusions, when the ratio of fetal cells to donor cells is greatest. On average, the decline in the fetal hematocrit following the first transfusion is about 1.5% per day; following subsequent transfusions, the decline in fetal hematocrit is about 1% to 2% per day. Follow-up intravascular transfusions are scheduled to keep the fetal hematocrit above 20% to 25%.
Morbidity and mortality associated with intravascular transfusion are related to the technique of vascular access and transfusion. Fetal bradycardia is the most common problem, occurring in 8% to 12% of cases, though only rarely requires immediate delivery. Postprocedure infection and premature rupture of the membranes have also been reported. Overall, it appears that intravascular transfusion in experienced hands seems to have a procedure-related complication rate of around 10% to 15% and a perinatal mortality rate of 1% to 5%.
Other Therapies
A number of noninvasive alternatives to IUT have been investigated for the treatment of fetal hemolysis. Most have been aimed at modifying the maternal immune response. High-dose intravenous immunoglobulin (IVIG) has been used to treat women with severe Rh alloimmunization refractory to traditional treatment. Experience is limited to case reports and small case series, all with different dosing regimens. The mechanism of action is uncertain, but is most likely at the maternal or placental level since direct fetal administration is not effective. Plasmapheresis has also been tried in refractory Rh alloimmunization and has been associated with a transient reduction in the anti–D titer during or immediately after treatment. However, no long-term, clinically significant reduction in antibody titer has been achieved.
Timing of Delivery
The timing of delivery should be based on individual case circumstances, including obstetric history and severity of Rh-D alloimmunization. In mildly affected pregnancies, induction of labor at 37 to 38 weeks gestation is reasonable, unless fetal pulmonary maturity is documented earlier by amniocentesis. In severely sensitized pregnancies, the risks of continued cord blood sampling and transfusions must be weighed against the potential neonatal morbidity and mortality associated with preterm delivery. This has traditionally led to scheduling the last procedures around 30 to 32 weeks gestation, with delivery between 32 to 34 weeks after maternal steroid administration to enhance fetal pulmonary maturity. In an effort to limit neonatal morbidity, IUT can be continued up to 36 weeks gestation with delivery between 37 and 38 weeks. At the University of Utah, we generally time the last procedure so that delivery can be carried out at about 34 to 36 weeks. Using this approach, neonatal survival in our nursery approaches 100% and long-term morbidity from prematurity is exceedingly low.
Alloimmunization Caused by Minor Antigens
The reduction in Rh disease brought about by Rh–immunoglobulin prophylaxis has led to a relative increase in the number of cases of alloimmunization caused by other red blood cell surface antigens, known as “minor,” “atypical,” or “irregular” antigens (Table 18.4).
Overall, alloimmunization due to minor antigens occurs in about 1.5% to 2.5% of obstetric patients though the frequency depends on ethnicity of the population under study. Most cases result from incompatible blood transfusion because blood banks do not routinely assess donor–recipient compatibility for antigens other than ABO and Rh-D. Some of the most common antibodies (i.e., anti–Lea, anti–Leb, and anti–I), do not cause fetal or neonatal hemolysis. However, other commonly encountered atypical antibodies (i.e., anti–E, anti–Kell, anti–c, anti-c + E, and anti–Fya [Duffy A]) may cause erythroblastosis fetalis and hydrops.
|
|
|
TABLE 18.4. Minor (atypical) red blood cell antigens, their risk of hemolytic disease, and proposed management |
In general, management of pregnancies complicated by alloimmunization to one of the minor red cell antigens is similar to management of pregnancies complicated by Rh-D alloimmunization. An exception to this rule is alloimmunization to the Kell antigen, which requires special vigilance because of its unpredictability and potential for severe fetal anemia, hydrops, and death. Its virulence may be related to its ability to suppress fetal erythropoiesis and activate the complement cascade in addition to hemolysis. Fortunately, only 9% of whites are positive for the Kell antigen and only 0.2% of pregnancies are complicated by Kell alloimmunization.
Compared to Rh alloimmunization, maternal antibody titers and amniotic fluid ΔOD450 values and trends do not predict the degree of fetal hemolysis in cases of Kell alloimmunization. Severe anemia seems to occur with lower antibody titers and in zones of the Liley curve rather than with Rh-D alloimmunization. Because of this, some authorities suggest routine umbilical cord blood sampling as early as 20 weeks gestation if the father is Kell-positive or of uncertain status. An alternative approach with less likelihood of perinatal morbidity and mortality is to perform early amniocentesis (20 weeks or less) and have a lower threshold to proceed with cordocentesis and IUT. In addition, noninvasive diagnostic modalities that detect fetal anemia, such as Doppler and ultrasound, may be well suited to management of pregnancies complicated by Kell alloimmunization.
ABO INCOMPATIBILITY
A comparison of Rh and ABO incompatibility is important because they are the most frequent causes of immune hemolytic disease in the neonatal period. In about 20% to 25% of pregnancies, ABO incompatibility exists between mother and infant, but a clinically recognizable hemolytic process in the infant occurs in only 10%. ABO hemolytic disease affects the firstborn child in about 50% of cases, and it is not uncommon for multiple siblings to be affected with comparable severity.
The pathophysiology involves the transplacental passage of maternal antibody and its interaction with fetal or neonatal red blood cell antigens, yielding erythrocyte destruction, variable anemia, and hyperbilirubinemia. Clinically, ABO hemolytic problems are confined almost exclusively to the A (specifically A1 rather than A2) or B infants of group O mothers. Anti–A and anti–B “natural” antibodies produced early in life by group A or B individuals are predominantly IgM. In contrast, group O individuals produce anti–A or anti–B that is predominantly IgG and capable of crossing the placenta. Yet, for reasons not completely understood, these antibodies seldom cause harm during pregnancy. There is no relationship between the antibody titer and the severity of hemolytic disease. The discordance between the high frequency of ABO–incompatible pregnancies and the low frequency of hemolytic disease as well as the broad spectrum of the severity has been attributed to such factors as immature, weak, nonspecific, or altered antigens on the fetal red blood cell; absorption of the antibodies by ABO antigens present in all body tissues; and the presence of soluble blood group substances in fetal plasma and tissue fluids that can neutralize maternal antibody. No single test exists that can forewarn the physician of impending ABO hemolytic disease.
Because this problem does not occur until after birth, amniocentesis and preterm induction of labor are not justified. The most common manifestations of ABO incompatibility in the neonate are early-onset jaundice (i.e., within 24 hours) and a variable elevation of the indirect bilirubin fraction. In contrast to Rh disease, kernicterus and anemia are rare. The cornerstones of management of ABO incompatibility are bilirubin surveillance, phototherapy (required in about 10% of infants), and, occasionally, exchange transfusion.
PLATELET ALLOIMMUNIZATION
Like erythrocytes, platelets have specific surface antigens that occasionally result in maternal alloimmunization when there is an incompatibility between fetus and mother. In a situation analogous to Rh disease, fetal or neonatal alloimmune thrombocytopenia (NAIT) results from maternal production of antiplatelet antibodies followed by placental transfer of antiplatelet antibodies and subsequent platelet destruction. The maternal platelet count is normal but fetal/neonatal thrombocytopenia is often profound.
Several different bi-allelic antigen systems may cause platelet alloimmunization, but most cases (75%) are due to sensitization to the HPA-1a (PlA1) antigen. Approximately 2% of whites, 0.4% of blacks, and less than 0.1% Asians are negative for HPA-1a and thus at risk for NAIT. Though fetomaternal incompatibility to platelet antigens is relatively common, only about 1:1,000 to 1:2,000 births are complicated by NAIT, probably because maternal HLA-antigen class II type influences susceptibility. Clinically, about 90% of affected newborns have diffuse petechiae and 9% to 12% suffer intracranial bleeding with a neonatal mortality of 5% to 13%. Fetal thrombocytopenia has been detected as early as 20 weeks gestation with 50% of intracranial hemorrhages diagnosed at the time of prenatal ultrasound.
Unlike erythrocyte alloimmunization, platelet alloimmunization often occurs during the first pregnancy with diagnosis after delivery of severely affected firstborn children. Maternal platelet antibody titers are not beneficial in predicting the severity of NAIT. Routine testing for HPA-1a antibody status during pregnancy has been proposed but is probably not justified because of the wide variation in the clinical expression of maternal–fetal platelet incompatibility and because 25% of cases of NAIT are due to antigens other than HPA-1a. The incidence of recurrent NAIT following delivery of an affected newborn is approximately 90% to 95% and thrombocytopenia is generally equal or worse in severity.
Obstetric Management of Platelet Alloimmunization
Umbilical cord blood sampling and direct measurement of fetal platelet count is the only method that accurately predicts disease severity. However, serial cordocentesis and IUT are not recommended because of the high risk of procedure-related fetal loss. Based on the effectiveness of IVIG treatment for neonates with NAIT, antenatal protocols using maternally administered high-dose IVIG have been developed and widely accepted. Some centers also add dexamethasone if the response to IVIG treatment is not adequate. The mechanism of IVIG treatment probably involves Fc–receptor saturation in the placenta and blockage of antibody transfer to the fetus. Direct fetal administration has not been successful. The use of high-dose IVIG in pregnancies at risk for NAIT is not without risk. Treatment with IVIG is expensive (over $1,000 per weekly infusion), occasional shortages have occurred, and there have been sporadic reports of acute hepatitis C associated with IVIG use.
The management of pregnancies at risk for NAIT is directed at prevention of hemorrhage in the fetus and newborn. As in erythrocyte alloimmunization, the paternal antigen status can be determined using DNA diagnostic techniques. If the father is homozygous, the fetus is at risk and pregnancy management should proceed accordingly. If the father is heterozygous for the particular antigen, amniocentesis at 16 to 20 weeks can be performed to assess fetal antigen status. If the fetus is antigen-negative, there is no significant risk of thrombocytopenia or intracranial hemorrhage and no fetal blood sampling is performed. If the fetus is antigen-positive, a protocol involving a combination of cordocentesis and IVIG treatments should be offered. In all cases at risk for NAIT, maternal platelets should be available for transfusion after delivery, regardless of the antenatal treatment or previously obtained fetal platelet counts.
MATERNAL THROMBOCYTOPENIA
Maternal thrombocytopenia is one of the most common hematologic disorders in pregnancy. Most cases of maternal thrombocytopenia are immunologically mediated, though thrombocytopenia may also be part of other systemic illnesses as well (Table 18.5). Normal values for platelets are unchanged during pregnancy; the mean platelet count for healthy pregnant women is 246,000 per mL. Platelet counts less than 150,000 per mm3 occur in up to 7.6% of pregnant women and counts less than 100,000 per mm3 occur in less than 1%. Thrombocytopenia may be categorized into mild (100,000–150,000/mL), moderate (50,000–100,000/mL), and severe (<50,000/mL). Clinically significant bleeding does not usually occur until platelet counts drop below 10,000 per mL. Excessive bleeding associated with trauma or surgery is uncommon unless the patient's platelet count is less than 50,000 per mL.
|
|
|
TABLE 18.5. Causes of thrombocytopenia in pregnancy |
Gestational Thrombocytopenia
Gestational thrombocytopenia, also known as essential thrombocytopenia or incidental thrombocytopenia is the most common type of mild thrombocytopenia in pregnancy. It is often diagnosed at the time of routine prenatal screening. Characteristics of gestational thrombocytopenia include the following:
· Thrombocytopenia is mild, usually greater than 70,000 per mL.
· Women with thrombocytopenia are asymptomatic with no history of bleeding diathesis.
· There is no history of thrombocytopenia, except in prior pregnancies.
· Platelet counts return to normal 1 to 2 weeks following delivery.
· There are no serious maternal or fetal consequences.
The mechanism of gestational thrombocytopenia is unknown but may involve accelerated platelet consumption. Many women with gestational thrombocytopenia have antiplatelet antibodies but their presence is probably meaningless. Except for the addition of serial platelets counts, no change in prenatal care is necessary.
Autoimmune Thrombocytopenia
Autoimmune thrombocytopenia (ATP) is the most common autoimmune bleeding disorder encountered during pregnancy, affecting between 1 in 1,000 to 10,000 pregnancies. While acute ATP is a self-limited disorder of childhood, chronic ATP typically presents in the second or third decade of life with a female-to-male ratio of 3:1. Autoimmune thrombocytopenia is characterized by production of IgG antibodies directed against platelet membrane glycoproteins. The IgG antiplatelet antibodies bind to platelets, rendering them more susceptible to sequestration and premature destruction in the reticuloendothelial system. Thrombocytopenia occurs when the rate of destruction exceeds the ability of the bone marrow to produce new platelets. Though other sites are also involved, most antibody production and platelet destruction occur in the spleen.
The diagnosis of ATP should be based on clinical findings, after other causes of thrombocytopenia have been excluded. Characteristics include:
· Thrombocytopenia (platelet count <100,000/mL) is present before and after pregnancy with or without megathrombocytes on the peripheral smear.
· Bone marrow aspirates reveal normal or increased numbers of megakaryocytes.
· Patients usually, but not uniformly, have a history of bleeding, easy bruising, petechiae, menorrhagia, or other bleeding problems.
· Splenomegaly is absent.
The course of ATP is not substantially influenced by pregnancy. However, ATP may lead to complications in pregnancy, the most serious of which is maternal hemorrhage around the time of delivery. No maternal deaths from ATP in pregnancy have been recorded since the early 1980s, but peripartum bleeding may result in serious morbidity. Because the placenta selectively transports maternal IgG antiplatelet antibodies into the fetal circulation, fetal thrombocytopenia may also occur, sometimes leading to purpura, ecchymosis, or melena. Intracranial hemorrhage is only rarely reported and appears to be unrelated to the mode of delivery.
Many women with ATP have elevated levels of platelet-associated antibodies and sometimes circulating antiplatelet antibodies. Assays for these antibodies are commercially available but should not be routinely performed because they are nonspecific, poorly standardized, and subject to a large degree of interlaboratory variation. Furthermore, levels of antiplatelet antibodies do not correlate well with the degree of fetal thrombocytopenia.
Treatment
Treatment of pregnant women with ATP are aimed at preventing bleeding by maintenance of the platelet count above 20,000 per mm3 in the antepartum period and over 50,000 per mm3 for delivery.
Glucocorticoids
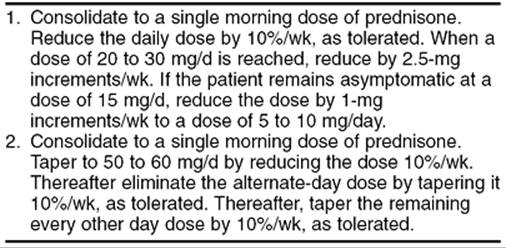
Glucocorticoid drugs are the cornerstones of therapy for ATP in pregnancy. Prednisone (1–2 mg/kg/d in divided doses) for 2 to 3 weeks is the most typical regimen. An increase in platelet count to more than 50,000 per mL, accompanied by a decrease in clinical bleeding, is usually achieved within 21 days. More than 70% of patients have some response and complete remission occurs in up to 25%. The prednisone dose is tapered by 10% to 20% decrements at 2-week intervals to a dose that maintains the platelet count above 50,000 per mm3. Dexamethasone and betamethasone also cause an increase in platelet count but both readily cross the placenta and have harmful fetal effects. The side effects of glucocorticoids in pregnancy include steroid-induced moon facies, gestational diabetes mellitus, psychosis, adrenocortical insufficiency, osteoporosis, aseptic necrosis, hypertension, and uteroplacental insufficiency.
Intravenous Immunoglobulin
Given at high doses (i.e., 400 mg/kg/d for 5 days), IVIG usually induces a peak in platelet count within 7 to 9 days. More than 80% of patients achieve a platelet count greater than 50,000 per mm3, and the response lasts for more than 30 days in 30% of patients. Only 2 to 3 days of IVIG therapy may be needed in some patients, and doses greater than 800 mg or 1 g per kg may suffice as a single or double infusion. Although expensive, IVIG therapy initiated 1 to 2 weeks before delivery or surgery may be useful in some obstetric patients who must undergo operative procedures or who develop bleeding problems and require emergency treatment. The exact mechanism of action of IVIG is unclear, but may be related to decreased antiplatelet antibody production, interference with antibody attachment to platelets, inhibition of macrophage receptor-mediated immune complex clearance, or interference with platelet receptor mechanisms in the reticuloendothelial system.
IgG is selectively transported across the placenta and the amount transferred increases with gestational age and dose so that after 32 weeks of gestation, maternally infused IgG sometimes has a beneficial effect on the fetal platelet count. No cases of human immunodeficiency virus (HIV) transmission have been reported with the use of IVIG, but adverse effects include thrombosis, alopecia, liver function disturbances, transient neutropenia, chills, nausea, flushing, tightness of the chest, wheezing, and anaphylactic reactions in patients with immunoglobulin A (IgA) antibodies.
Splenectomy
Splenectomy serves to remove the site of destruction of damaged platelets as well as the major source of antibody production. During pregnancy, it is used only for patients with ATP who are refractory to or cannot tolerate glucocorticoids and IVIG. A complete remission is obtained in 80% of patients. The postsplenectomy platelet count increases rapidly and often is normal within 1 to 2 weeks. The surgery is associated with a modest risk of spontaneous abortion or preterm labor and is technically more difficult late in gestation. If splenectomy is unavoidable, it is best performed in the second trimester; it has also been combined safely with cesarean section at term. Splenectomy does not always protect the fetus from thrombocytopenia because antibodies to platelets are also produced in other lymphoid tissues.
Platelet Transfusions
Platelet transfusions are used only as a temporizing measure to control life-threatening hemorrhage or to prepare a patient for splenectomy or cesarean section. The survival of transfused platelets is decreased in patients with ATP because antiplatelet antibodies also bind to donor platelets. In addition, patients with ATP do not respond as well as normal individuals to platelet transfusions but 6 to 10 U is usually sufficient to temporarily control hemostasis.
Other Treatments
Other agents have been used with some success in patients who are refractory to glucocorticoids, IVIG, and splenectomy. Those most commonly used, such as azathioprine, cyclophosphamide, Vinca alkaloids, and danazol, are to be avoided in pregnancy because of their toxicity and potential adverse effects on the fetus. Plasmapheresis has also been tried, but the results of this treatment are variable.
Obstetric Management of Autoimmune Thrombocytopenia
Management of pregnancies complicated by ATP is controversial largely because of uncertainties regarding the actual risk of fetal thrombocytopenia. In the past, cesarean delivery was advocated in all women with ATP because of anecdotal reports of intracranial hemorrhage associated with vaginal delivery. Prompted by the fact that clinically significant bleeding is extremely unlikely in fetuses with platelet counts more than 50,000 per mL, some authorities recommended cesarean delivery only if the fetal platelet count was less than 50,000 per mL. However, this required measurement of the fetal platelet count. Fetal scalp sampling during labor was the first and most commonly performed method of obtaining the fetal platelet count, allowing 80% of fetuses with acceptable platelet counts to be safely delivered vaginally. Unfortunately, the procedure is technically difficult to perform in early labor and falsely low platelets were sometimes obtained. Cordocentesis often replaced fetal scalp sampling because platelet counts were extremely accurate and the procedure could be performed before the onset of labor. However, cordocentesis is expensive and unavailable in centers without appropriate expertise and equipment. It also has several potentially serious complications including fetal bradycardia, hemorrhage at the puncture site, and cord hematoma.
Both fetal scalp sampling and cordocentesis might be useful if there was any evidence that cesarean delivery reliably prevents intracranial hemorrhage in thrombocytopenic fetuses. However, it appears that early reports of ATP in pregnancy overestimated the risk of severe fetal thrombocytopenia and intracranial hemorrhage associated with vaginal delivery. In a recent, large, population-based study of almost 16,000 pregnancies, no infant born to a mother with ATP suffered intracranial hemorrhage, regardless of the route of delivery.
Because it appears that fetal scalp sampling, cordocentesis, and cesarean delivery contribute to cost and morbidity without preventing intracranial hemorrhage, many obstetricians have abandoned antenatal measurement of fetal platelet counts and reserved cesarean delivery for the usual obstetric indications.
Mothers with ATP do not require substantial alterations in prenatal care. Serial platelet counts should be obtained during the pregnancy. If the platelet count is less than 50,000 per mL in the weeks preceding delivery, patients with ATP should be treated with glucocorticoids or IVIG. Women requiring chronic glucocorticoid therapy during pregnancy should be carefully monitored for the development of gestational diabetes and should have serial ultrasounds to assess fetal growth. Women with prior splenectomy should be monitored for the development of infection. Delivery is best accomplished in a setting in which platelets, fresh frozen plasma, and IVIG are available. A neonatologist or pediatrician familiar with the disorder should be present to promptly treat any hemorrhagic complications in the neonate. In the puerperium, salicylates and nonsteroidal antiinflammatory drugs (NSAIDs) should be avoided. Though breast-feeding may theoretically induce neonatal thrombocytopenia because of the passage of antiplatelet antibodies in the colostrum, it is considered safe and reasonable by most pediatricians.
Other Causes of Thrombocytopenia in Pregnancy
Other than ATP, the most common serious condition associated with maternal thrombocytopenia late in pregnancy is preeclampsia or HELLP syndrome (hemolysis, elevated liver enzymes, and low platelet count). Other conditions that can result in maternal thrombocytopenia at any gestational age include acute HIV infection, systemic lupus erythematosus, antiphospholipid syndrome (APS), sepsis, cocaine abuse, thrombotic thrombocytopenic purpura, transfusion reaction, blood dyscrasias, or certain medications (see Table 18.5).
Pseudothrombocytopenia can result from laboratory artifacts such as platelet clumping induced by ethylenediaminetetraacetic acid (EDTA) in the collection tube, blood clotting related to techniques of blood withdrawal, and an inadequate amount of anticoagulant. These factors can be confirmed by examining a stained peripheral maternal blood smear. Once the diagnosis of pseudothrombocytopenia is established, no further treatment is needed for mother or infant.
SYSTEMIC LUPUS ERYTHEMATOSUS
Systemic lupus erythematosus (SLE) is a chronic inflammatory condition affecting virtually every organ system of the body. With a predilection for women of reproductive age, it is the autoimmune disease most commonly encountered during pregnancy. No specific gene mutation for SLE has been identified. However, 5% to 12% of affected individuals have another relative with SLE and 25% to 50% of affected monozygotic twins are concordant for the disease. Several alterations in the HLA-antigen system have been linked to the development of SLE and homozygous carriers of inherited complement deficiency disorders also appear to be predisposed to development of the disease. With an increased awareness of the disease, more sophisticated diagnostic methods, and improved drug therapy, the 10-year survival rate now exceeds 90%.
Diagnosis of Lupus
Lupus may easily be overlooked because it often begins with mild and vague symptoms such as fatigue and is characterized by periods of exacerbation and remission. The presence of autoantibodies, characteristically against nuclear components, is a hallmark of the disorder. The American Rheumatism Association has set criteria for the diagnosis of SLE that incorporate immunologic abnormalities and improve disease classification for purposes of clinical studies (Table 18.6). The most common clinical manifestations include arthralgia or arthritis (90%), dermatologic involvement (70%–80%), renal disease (46%), hematologic abnormalities (50%), and cardiovascular disease (30%–50%). The most frequent laboratory findings are thrombocytopenia, leukopenia, and the presence of autoantibodies.
|
|
|
TABLE 18.6. Diagnostic criteria for systemic lupus erythematosusa |
Lupus should be suspected when a woman in her reproductive years presents with glomerulonephritis, nephrotic syndrome, hemolytic anemia, leukopenia, or thrombocytopenia. A positive antinuclear antibody (ANA) test is confirmatory in virtually all (98%) patients. However, this test does not have high specificity for SLE and many healthy women may test positive for low levels of ANA antibodies. High titers of antibodies to double-stranded DNA and antibodies to the Smith (Sm) antigen are most specific for SLE.
Systemic Lupus Erythematosus and Pregnancy
Lupus Flare During Pregnancy
Considerable debate surrounds the incidence and severity of SLE flare during pregnancy. Studying SLE flare in pregnancy is difficult because many of the signs and symptoms typically associated with SLE flare are considered routine during pregnancy. In addition, studies have not consistently used the same criteria for flare or disease severity. Nevertheless, it appears that SLE flare occurs in 35% to 65% of pregnant women with well-controlled SLE. Most flares are mild-to-moderate in nature and easily treated with glucocorticoids. Flares occur with equal frequency in all three trimesters and the puerperium.
Women at greatest risk for complications of SLE during pregnancy are undoubtedly those with preexisting lupus nephritis (LN). Approximately half of all SLE patients eventually develop LN as a result of immune complex deposition in the kidney with subsequent complement activation and inflammatory tissue damage. Patients typically present with proteinuria, hematuria, aseptic pyuria, and urinary sediment. Renal biopsy is necessary to confirm the diagnosis. Pregnancy places women with LN at risk for deterioration of renal function and increased proteinuria, especially if active nephritis or renal insufficiency is present at the time of conception. However, the risks of pregnancy may not be so serious for women with stable LN. About one-third of women with LN experience flare during pregnancy, fewer than 25% have worsening renal function, and 10% of have permanent deterioration. The incidence of maternal death attributed to renal failure during pregnancy is less than 2%.
Obstetric Complications in Women with Lupus
Women with SLE are at risk for several obstetric complications. Between 20% to 30% of women with SLE have pregnancies complicated by preeclampsia. Women with secondary APS, underlying renal disease, chronic hypertension, or chronic steroid use are at particular risk. Uteroplacental insufficiency resulting in intrauterine growth restriction (IUGR) or neonates who are small for gestational age has been reported in 12% to 40% of pregnancies complicated by SLE. Renal insufficiency or hypertension increases the risk of IUGR.
The risk of pregnancy loss for women with SLE is uncertain with reported rates ranging from 10% to 50%. There appears to be a predilection for the second and third trimester. Renal insufficiency increases the risk of fetal loss; live births occur in only 50% of pregnancies complicated by moderate to severe renal insufficiency (serum creatinine >1.5 mg/dL) and in 40% with preexisting proteinuria (>300 mg/24 h or creatinine clearance <100 mL/min). Coexisting APS poses the greatest risk for pregnancy loss in women with SLE. Only 50% of women with SLE and APS have live births; if they have previously experienced a fetal loss, 85% have recurrent loss in subsequent pregnancies.
Lupus Disease Activity and Risks of Pregnancy
The degree of disease activity at conception dramatically affects the risk of SLE flare and other complications during pregnancy. The rate of SLE flare is lower for women with SLE in remission prior to conception. Renal deterioration is also less likely and less severe in women with inactive LN in the 6 months prior to conception. Furthermore, nearly 90% of women with inactive SLE at conception have live births compared to 64% of those with active disease. Women with SLE who plan their pregnancies after disease remission have outcomes similar to those of the general population.
Neonatal Lupus Erythematosus
Neonatal lupus erythematosus (NLE) is a rare condition of the fetus and neonate, occurring in 1 of 20,000 of all live births and in fewer than 5% of all women with SLE. Dermatologic NLE is most common with lesions described as erythematosus, scaling annular or elliptical plaques occurring on the face or scalp, analogous to the subacute cutaneous lesions in adults. Lesions appear in the first weeks of life, probably induced by exposure of the skin to ultraviolet light, and may last for up to 6 months. Hypopigmentation may persist for up to 2 years. Hematologic NLE is manifest as autoimmune hemolytic anemia, leukopenia, thrombocytopenia, and hepatosplenomegaly.
The most well-known form of SLE is congenital complete heart block (CCHB) caused by endomyocardial fibrosis of the conduction system in the area of the atrioventricular node. The diagnosis is usually made in the second trimester when a fixed bradycardia, in the range of 60 to 80 beats per minute, is detected during a routine prenatal visit. Fetal echocardiography confirms complete atrioventricular dissociation with a structurally normal heart. There is no known treatment for prenatally diagnosed CCHB though glucocorticoids, plasmapheresis, intravenous immune globulin, digoxin, or some combination thereof, have been tried. Maternally administered glucocorticoids appear to reduce the risk of recurrence of CCHB in another pregnancy. The prognosis for fetuses with CCHB varies but hydrops fetalis may develop in the most severe cases. Because the endomyocardial damage is permanent, a pacemaker may be necessary for neonatal survival.
The manifestations of NLE are probably caused by maternal autoantibodies that cross the placenta and bind to fetal tissue. Anti–Ro/SSA antibodies are found in 75% to 95% mothers who deliver babies with NLE. A smaller percentage of mothers have anti–La/SSB, and some have both. About 15% of infants born to mothers with anti–Ro/SSA antibodies have dermatologic SLE; the incidence of CCHB is much smaller. However, with a previously affected infant, the risk of recurrence increases two- to three-fold. Occasionally, women with no history of SLE give birth to babies with NLE. More than half eventually develop lupus.
Obstetric Management for Women with Lupus
Immunosuppressive Medications
Glucocorticoids
Glucocorticoid preparations are the group of drugs most commonly given to pregnant women with SLE, both as maintenance therapy and in “bursts” to treat suspected SLE flares. Dosing regimens in pregnant women are the same as those in nonpregnant patients. Prophylactic treatment with glucocorticoids is not necessary or prudent in women with inactive disease. Maternal side effects of chronic glucocorticoid therapy include weight gain, striae, acne, hirsutism, immunosuppression, osteonecrosis, and gastrointestinal ulceration. Pregnant women are also at risk for preeclampsia, uteroplacental insufficiency, and glucose intolerance. Prednisolone or methylprednisolone should be used as maintenance therapy because of their conversion to relatively inactive forms in the human placenta. Glucocorticoids with fluorine at the 9a position (dexamethasone, betamethasone) are considerably less well metabolized by the placenta and chronic use may lead to undesirable fetal effects.
Antimalarials
An accumulating body of evidence suggests that antimalarial drugs may be used safely for the treatment of SLE during pregnancy. Past concerns about teratogenicity including ototoxicity and eye damage appear to be unfounded. In randomized controlled trials, hydroxychloroquine appears to be more efficacious than glucocorticoids for prevention of flare during pregnancy.
Cytotoxic Agents
Azathioprine, methotrexate, and cyclophosphamide are used to treat only the most severely affected patients with SLE. Azathioprine, a derivative of 6-mercaptopurine, is not a human teratogen but has been associated with fetal growth impairment and impaired neonatal immunity. Cyclophosphamide is a known teratogen and should be avoided during the first trimester. Thereafter, its use should be limited to women with severe, progressive proliferative glomerulonephritis or SLE-related central nervous system (CNS) disease. Methotrexate is well known to kill chorionic villi and cause fetal death and its use should be scrupulously avoided.
Nonsteroidal Medications
The most common types of analgesics used by women with SLE are NSAIDs. Unfortunately, they readily cross the placenta and should be avoided after the first trimester. Although short-term tocolytic therapy with indomethacin appears to be safe, long-term use of any NSAID has been associated with decreased fetal urinary output and oligohydramnios as well as neonatal renal insufficiency.
Other Treatments
Several new treatment regimens including cyclosporine, high-dose IVIG, mycophenolate mofetil, and thalidomide have been studied in the treatment of nonpregnant patients with SLE. Only IVIG has been used during pregnancy without reports of adverse fetal effects. Obviously, thalidomide is absolutely contraindicated during pregnancy.
Detection of SLE Exacerbation (Flare)
Thorough and frequent clinical assessment remains essential for the timely and accurate detection of SLE flare. The most common presenting symptom in both flare and new-onset disease is extreme fatigue (see Table 18.6). In pregnancy, skin rashes are more frequent than musculoskeletal manifestations. Patients with LN exhibit worsening proteinuria along with pyuria, hematuria, and urinary casts, which can sometimes be confused with the onset of preeclampsia.
Laboratory evaluation of SLE activity should be used to confirm flare in confusing cases. Serial evaluation of complement levels has been suggested as a method of predicting SLE flare during pregnancy. However, the predictive value of complement activation has been inconsistent and never been proven to be superior to thorough and frequent clinical assessment. The most specific laboratory test for disease activity is an elevation in the anti–double-stranded DNA (anti–dsDNA) titer that precedes lupus flare in more than 80% of patients and has been shown to correlate with the need for preterm delivery. In combination with anticardiolipin (aCL) antibodies, elevated levels of anti–dsDNA have been shown to predict fetal loss.
Treatment of SLE Flare during Pregnancy
Mild to moderate symptomatic exacerbations of SLE without CNS or renal involvement may be treated with initiation or increased dose of glucocorticoids. Relatively small doses of prednisone (e.g., 15–30 mg/d) result in improvement in most cases. For severe exacerbations without CNS or renal involvement, 1.0 to 1.5 mg per kg per day of prednisone in divided doses should be used, and a good clinical response can be expected in 5 to 10 days. Thereafter, glucocorticoids may be tapered by several different approaches (Table 18.7).
|
|
|
TABLE 18.7. Suggested methods for tapering prednisone |
Severe exacerbations, especially those involving the CNS or kidneys, are treated more aggressively. Intravenous-pulse glucocorticoid therapy should be given, usually in a dose of methylprednisolone at 10 to 30 mg per kg (about 500–1,000 mg) for 3 to 6 days. Thereafter, the patient is treated with 1.0 to 1.5 mg per kg per day of prednisone in divided doses and rapidly tapered over the course of 1 month. One can expect that 75% of patients will respond favorably to this approach. This regimen may be repeated every 1 to 3 months in severe cases as an alternative to cytotoxic drugs.
The use of cytotoxic agents, plasmapheresis, and IVIG should be reserved for severe SLE exacerbations that do not respond to glucocorticoid therapy. Severe proliferative lupus nephritis is often responsive only to cyclophosphamide.
Obstetric Care for Women with Systemic Lupus Erythematosus
Clinical precautions in pregnancies associated with SLE are similar to those required for other high-risk pregnancies. Recommended laboratory studies in addition to routine prenatal tests are listed in Table 18.8. The gestational age should be firmly established early in pregnancy. Serial sonography should be performed to assess fetal growth. Antenatal surveillance (e.g., nonstress tests, biophysical profiles, etc.) should be initiated in the third trimester to confirm fetal well-being. Lupus per se is not an indication for cesarean delivery. Instead, the route of delivery should be based on appropriate obstetric indications.
|
|
|
TABLE 18.8. Management of systemic lupus erythematosus during pregnancy |
ANTIPHOSPHOLIPID SYNDROME IN PREGNANCY
The diagnosis of APS is based on the presence of one or more characteristic thrombotic or obstetric features of the condition in combination with positive serologic testing for antiphospholipid antibodies (aPL). Patients with bona fide APS must manifest at least one of two clinical criteria (vascular thrombosis or pregnancy morbidity) and at least one of two laboratory criteria (positive lupus anticoagulant [LA] or medium to high titers of β2-glycoprotein I-dependent IgG or IgM isotype aCL antibodies, confirmed on two separate occasions at least 6 weeks apart (Table 18.9). APS may exist as an isolated immunologic derangement (primary APS) or in combination with other autoimmune diseases (secondary APS), most commonly SLE.
|
|
|
TABLE 18.9. Clinical and laboratory criteria for antiphospholipid syndrome (APS)a |
Clinical Features of Antiphospholipid Syndrome during Pregnancy
In the original description of APS, the sole obstetric criterion for diagnosis was fetal loss (>10 menstrual weeks of gestation). At least 40% of pregnancy losses reported by women with LA or medium to high positive IgG aCL occur in the fetal period. More recently, APS-related pregnancy loss has been extended to include women with early recurrent pregnancy loss (RPL) including those occurring in the preembryonic (<6 menstrual weeks of gestation) and embryonic periods (6–9 menstrual weeks of gestation). In addition, APS is associated with other pregnancy complications including gestational hypertension or preeclampsia and uteroplacental insufficiency as manifested by fetal growth restriction, oligohydramnios, and non-reassuring fetal surveillance. Obstetric complications other than pregnancy loss appear to persist in spite of treatment. There have been some attempts to link infertility and failure of in vitro fertilization (IVF) to the presence of aPL antibodies. However, there is no evidence to support such a relationship. Indeed, multiple studies have refuted any association between aPL antibodies and infertility and failed IVF.
Treatment of Antiphospholipid Syndrome during Pregnancy
The goals of APS treatment during pregnancy are two-fold:
1. Improve maternal and fetal–neonatal outcome by preventing pregnancy loss.
2. Reduce or eliminate risk of thromboembolism.
Initial attempts at treating women with APS during pregnancy involved immunosuppression with a glucocorticoid preparation, usually prednisone. Early enthusiasm for treatment of APS with glucocorticoids waned after publication of a small, randomized trial found maternally administered heparin to be as effective as prednisone, without all of the risks associated with chronic glucocorticoid use during pregnancy. At present, maternally administered heparin is considered the treatment of choice, usually initiated in the early first trimester after ultrasonographic demonstration of a live embryo. Daily low-dose aspirin is usually included as well. Live-birth rates among women with APS are generally greater than 70% with regimens including both heparin and aspirin (see Fig. 18.9). However, rates of other obstetric complications associated with APS are not improved, regardless of therapy.
The safe and effective dose of heparin for pregnant women with APS is debated but should probably depend on individual patient history. Women with APS and a history of thromboembolism should receive adjusted-dose anticoagulation with unfractionated heparin or low–molecular-weight heparin during pregnancy (Table 18.10). For women with APS without a history of thromboembolic disease, the choice of anticoagulation is less clear. Low-dose heparin prophylaxis may be sufficient for women with recurrent first trimester loss and no history of fetal loss. However, women with a history of fetal death (>10 weeks gestation) may be at higher risk for thromboembolism during pregnancy and should probably receive higher doses of heparin prophylaxis. We treat such women with generous thromboprophylaxis (e.g., 15,000 to 20,000 units of standard heparin or 60 mg of enoxaparin in daily divided doses). Recommendations for postpartum therapy vary but most authorities recommend at least 6 weeks of some regimen of anticoagulation with unfractionated heparin, low–molecular-weight heparin, or warfarin.
|
|
|
TABLE 18.10. Regimens for anticoagulation during pregnancy |
Healthy women with recurrent embryonic and preembryonic loss who have low or negative aPL titers do not require anticoagulation.
Women with APS should be counseled about the potential risks of heparin therapy during pregnancy including heparin-induced osteoporosis (1%–2%) and heparin-induced thrombocytopenia (HIT). Women treated with heparin should be encouraged to take daily supplemental calcium and vitamin D (e.g., prenatal vitamins) and perform daily axial skeleton weight-bearing exercise (e.g., walking). Immune-mediated HIT is much less common but potentially more serious. Most cases have their onset 3 to 21 days after heparin initiation and are relatively mild in nature. A more severe form of HIT paradoxically involves venous and arterial thromboses resulting in limb schemia, cerebrovascular accidents, and myocardial infarctions, as well as venous thromboses. We obtain serial platelet counts for 2 weeks and discontinue heparin if a significant decrease in platelet count occurs.
Postpartum and Catastrophic Antiphospholipid Syndrome
Catastrophic APS is a rare but devastating syndrome characterized by multiple simultaneous vascular occlusions throughout the body, often resulting in death. The diagnosis should be suspected if at least three organ systems are affected and confirmed if there is histopathologic evidence of acute thrombotic microangiopathy affecting small vessels. Renal involvement occurs in 78% of patients. Most patients have hypertension and 25% eventually require dialysis. Other common manifestations include adult respiratory distress syndrome (66%), cerebral microthrombi and microinfarctions (56%), myocardial microthrombi (50%), dermatologic abnormalities (50%), and disseminated intravascular coagulation (25%). Death from multiorgan failure occurs in 50% of patients. The pathophysiology of catastrophic APS is poorly understood. However, the onset may be presaged by several factors including infection, surgical procedures, discontinuation of anticoagulant therapy, and the use of drugs such as oral contraceptives.
Early and aggressive treatment of catastrophic APS is necessary to avoid death. Patients should be transferred to an intensive care unit where supportive care can be provided. Hypertension should be aggressively treated with appropriate antihypertensive medication. While no one treatment has been shown to be superior to another, a combination of anticoagulants (usually heparin) and steroids plus either plasmapheresis or IVIG has been successful in some patients. Streptokinase and urokinase have also been used to treat acute vascular thrombosis. Women suspected of catastrophic APS during pregnancy should probably be delivered.
RHEUMATOID ARTHRITIS
Rheumatoid arthritis (RA) is a chronic inflammatory process that primarily involves synovial-lined joints resulting in swelling and pain. The following criteria must be met to establish the diagnosis of RA (i.e., seven criteria for classic RA, five criteria for definite RA, three criteria for probable RA, two criteria for possible RA):
· morning stiffness
· pain and tenderness in at least one joint
· swelling of at least one joint
· swelling of at least one other joint
· symmetric joint swelling
· subcutaneous nodules
· x-ray changes typical of RA
· positive test result for rheumatoid factor
· poor mucin precipitate of synovial fluid
· characteristic histologic changes of synovium
· characteristic histologic changes of nodules.
Most cases are mild and require little or no medical treatment. In others, the disease is characterized by intermittent exacerbations with ultimate progression over many years to typical joint deformities.
Pregnancy is associated with clinical improvement in at least 50% of patients, a phenomenon that may be related to elevated blood levels of free cortisol or to enhanced phagocytosis of immune complexes. The rheumatoid factors (i.e., IgM antibodies against autologous IgG) do not cross the placenta, and there is no fetal or neonatal involvement.
Management of RA during pregnancy should include an appropriate balance of medication, rest and exercise, heat, and physical therapy. The basic reliance on large doses of salicylates, NSAIDs, and analgesics must be modified during pregnancy. Low-dose steroids (e.g., prednisone, 5 mg/d) and low-dose aspirin are recommended. Though gold compounds cross the placenta, no fetal adverse effects or teratogenicity have been reported. Gold therapy can be continued in selected pregnant patients with RA who are unresponsive to glucocorticoids. Other NSAIDs and penicillamine are not recommended because of potential detrimental fetal effects. As in SLE, antimalarials (hydroxychloroquine) appear to be another safe option during pregnancy.
Specialized antenatal surveillance is unnecessary for women with RA. Serial ultrasounds and antenatal surveillance should be reserved for the usual obstetric indications. Joint deformities rarely preclude vaginal delivery but mechanical obstacles may occur in women with hip deformities. Cesarean delivery can usually be reserved for standard obstetric indications. The type of anesthesia (regional vs. general) chosen depends on the presence of skeletal deformities or special problems such as atlantoaxial subluxation.
Other Rheumatic (Collagen Vascular) Diseases
Most disorders of undetermined origin, which are characterized by inflammation of various tissues, have been termed systemic rheumatic or collagen vascular diseases. More recently, many have been classified as autoimmune disorders because of their association with the production of autoantibodies and other immunologic aberrations. This group includes:
· mixed connective tissue disorder
· Sjögren syndrome
· polyarteritis nodosa
· dermatomyositis
· scleroderma.
The risk of both maternal and perinatal death is particularly high in patients with polyarteritis nodosa, mixed connective tissue disorder, and scleroderma complicated by renal disease or cardiopulmonary disease. Scleroderma worsens in at least 10% of women during pregnancy. At least 5% have life-threatening complications, usually related to renal or cardiopulmonary disease.
MYASTHENIA GRAVIS
Myasthenia gravis (MG) is a chronic neuromuscular autoimmune disease characterized by fatigue and weakness, usually involving the extraocular, facial, pharyngeal, and respiratory muscles. It is worsened by exertion and relieved by rest and anticholinesterase drugs. Antibodies to human acetylcholine receptors (AChR) are detectable in up to 90% of patients with MG. The anti–AChR antibodies are involved in complement-dependent destruction of the postsynaptic membrane of the myoneural junction, resulting in decreased nerve impulse transmission. Thymoma, thymic hyperplasia, and other autoimmune diseases often accompany MG. The functional abnormalities associated with the disease are similar to those induced by curare. The course during pregnancy is variable, although there is a tendency for relapse during the puerperium.
The cholinesterase inhibitors and their equivalent doses most commonly used to alleviate symptoms are 0.5 mg of intravenous neostigmine, 1.5 mg of subcutaneous neostigmine, 15 mg of oral neostigmine, 60 mg of oral pyridostigmine, and 5 mg of oral ambenonium. Drugs are adjusted to the dose at which the patient's muscle strength is optimal with a minimum of cholinergic adverse effects. Oral pyridostigmine, or a sustained-release preparation of pyridostigmine, is the most commonly used medication for MG. Overmedication results in unpleasant effects such as abdominal cramps, flatulence, diarrhea, nausea, vomiting, and excessive secretion of saliva and tears. Toxic levels of pyridostigmine lead to a myasthenic crisis-like syndrome involving profound muscle weakness and eventually respiratory failure. Treatment with high-dose glucocorticosteroids has also been used successfully in some patients. Regular rest periods with limited physical activity should be prescribed for the pregnant patient with MG. Infections should be treated aggressively because of their propensity to exacerbate MG.
Careful plans should be made for drug therapy during pregnancy, labor, delivery, and the postpartum period. Some antibiotics such as the aminoglycosides may produce a myasthenic crisis and should be avoided. Other medications may also be harmful in women with MG (Table 18.11). Many patients with MG are sensitive to sedatives, analgesics, tranquilizers, and especially narcotics. Muscle relaxants should be avoided. Local or regional anesthetics are preferable. Magnesium sulfate is contraindicated because the drug diminishes the acetylcholine effect and has been known to induce a myasthenic crisis.
|
|
|
TABLE 18.11. Medications that may exacerbate or cause muscle weakness in patients with myasthenia gravis |
Labor typically progresses normally and sometimes more rapidly than usual because smooth muscle is unaffected. Cesarean delivery should be reserved for obstetric reasons. Assisted ventilation should be available in the event of respiratory difficulty. During labor, the patient's oral dose of anticholinesterase should be discontinued and replaced with an intramuscular equivalent.
About 12% to 20% of infants born to women with MG exhibit neonatal MG, which lasts from a few hours to several days. The manifestations are caused by the transplacental transfer of acetylcholine-blocking factor. Interestingly, neonatal MG does not occur in all infants born to mothers with MG. The classic features of neonatal MG differ from those seen in adults. The symptoms usually do not develop until day 1 or 2 of life, probably because of some protection to the infant from the maternal blood levels of anticholinesterase agents. A high index of suspicion is necessary to recognize this phenomenon because an infant who appears healthy at birth may later develop respiratory failure with asphyxia. The involved infant shows generalized muscle weakness and hypotonic limbs and is limp and motionless. The Moro reflex often is weak or absent, and there may be a feeble cry, inability to suck, and associated difficulty in swallowing and breathing. Arthrogryposis (i.e., joint contractures), which may develop as a result of reduced intrauterine movement, has been reported in several infants born to mothers with MG.
SUMMARY POINTS
ERYTHROBLASTOSIS FETALIS
· Rh immunoglobulin should be given to Rh–negative, unsensitized women at 28 weeks gestation, within 72 hours after delivery, and in the event of antenatal procedures and complications associated with fetomaternal hemorrhage.
· Rh–alloimmunized women with anti–D titers 1:16 or greater should be referred for measurements of amniotic fluid bilirubin.
· Serial measurements of amniotic fluid bilirubin are used to identify fetuses at risk for significant fetal anemia.
· Intravascular intrauterine transfusion is most efficacious for the treatment of severely anemic fetuses with hydrops.
PLATELET ALLOIMMUNIZATION
· Platelet alloimmunization results in severe fetal and neonatal thrombocytopenia, which may be ameliorated with maternal administration of intravenous immunoglobulin.
MATERNAL THROMBOCYTOPENIA
· Gestational thrombocytopenia is a benign disorder characterized by mild thrombocytopenia (>70,000/mL), no history of excessive bleeding, no history of thrombocytopenia, resolution of thrombocytopenia 1 to 2 weeks after delivery, and no serious risk to mother or fetus.
· Autoimmune thrombocytopenia is characterized by thrombocytopenia before and after pregnancy, megathrombocytes on peripheral smears, bone marrow aspirate with normal or increased numbers of megakaryocytes, history of excessive bleeding, and absence of splenomegaly.
· Antiplatelet antibodies are not useful in differentiating between gestational thrombocytopenia and autoimmune thrombocytopenia.
· Autoimmune thrombocytopenia is not associated with a significant risk of fetal thrombocytopenia leading to intracranial hemorrhage.
SYSTEMIC LUPUS ERYTHEMATOSUS
· The diagnosis of lupus is based on specific clinical criteria.
· A positive antinuclear antibody (ANA) test is confirmatory in 98% of patients but elevated levels of antibodies to double-stranded DNA are most specific for disease activity.
· Most lupus flares during pregnancy are easily treated with glucocorticoids.
· Prophylaxis with glucocorticoid medication is not indicated to prevent flare during pregnancy.
· Lupus flare during pregnancy is best detected by frequent and thorough clinical assessment.
· Congenital cardiac heart block associated with neonatal lupus is characterized by fetal bradycardia diagnosed in the second trimester in a fetus with a structurally normal heart.
ANTIPHOSPHOLIPID SYNDROME
· The diagnosis of antiphospholipid syndrome (APS) should be based on the presence of thromboembolism or pregnancy loss in combination with medium to high titers of anticardiolipin antibodies or the lupus anticoagulant.
· A regimen of heparin and low-dose aspirin reduces the risk of thromboembolism and pregnancy loss in women with APS.
RHEUMATOID ARTHRITIS
· Pregnancy is associated with clinical improvement in at least 50% of patients with rheumatoid arthritis.
MYASTHENIA GRAVIS
· Myasthenia gravis (MG) is a chronic neuromuscular autoimmune disease characterized by fatigue and weakness, usually involving the extraocular, facial, pharyngeal, and respiratory muscles.
· Women with MG should avoid magnesium sulfate and aminoglycoside preparations, narcotics, and muscle relaxants.
· Neonatal MG occurs in 12% to 20% of infants born to mothers affected with MG.
SUGGESTED READINGS
Reproductive Immunology
Silver RM, Branch DW. The immunology of pregnancy. In: Creasy R, Resnik R, eds. Maternal fetal medicine, 3rd ed. Philadelphia: WB Saunders, 1998:115.
Erythroblastosis Fetalis
American College of Obstetricians and Gynecologists. Management of isoimmunization in pregnancy. Technical Bulletin No. 227, Aug 1996.
American College of Obstetricians and Gynecologists. Prevention of Rh D alloimmunization. Practice Bulletin No. 4, May 1999.
Mari G. Noninvasive diagnosis by Doppler ultrasonography of fetal anemia due to maternal red-cell alloimmunization. N Engl J Med 2000;342:9.
Standards Committee, American Association of Blood Banks. Standards for blood banks and transfusion services, 19th ed. Washington, DC: American Association of Blood Banks, 1999.
Platelet Alloimmunization
Bussel JB, Zabusky MR, Berkowitz RL, et al. Fetal alloimmune thrombocytopenia. N Engl J Med 1997;337:22.
Silver RM, Porter TF, Branch DW, et al: Neonatal alloimmune thrombocytopenia: antenatal management. Am J Obstet Gynecol 2000;182:1233.
Autoimmune Thrombocytopenia
American College of Obstetricians and Gynecologists. Thrombocytopenia in pregnancy. Practice Bulletin No. 6, Sept 1999.
Cines DB, Blanchette VS. Immune thrombocytopenic purpura. N Engl J Med 2002;346:995–1008.
Systemic Lupus Erythematosus
Buyon JP, Hiebert R, Copel J, et al. Autoimmune-associated congenital heart block: demographics, mortality, morbidity and recurrence rates obtained from a national neonatal lupus registry. J Am Coll Cardiol 1998;31:1658–1666.
Julkunen H, Kaaja R, Palosuo T, et al. Pregnancy in lupus nephropathy. Acta Obstet Gynecol Scand 1993;72:258–263.
Le Huong D, Wechsler B, Vauthier-Brouzes D, et al. Outcome of planned pregnancies in systemic lupus erythematosus: a prospective study on 62 pregnancies. Br J Rheumatol 199;36:772–777.
Levy RA, Vilela VS, Cataldo MJ, et al. Hydroxychloroquine (HCQ) in lupus pregnancy: double-blind and placebo-controlled study. Lupus 2001;10:401–404.
Antiphospholipid Syndrome
American College of Obstetricians and Gynecologists. Thromboembolism in pregnancy. ACOG Practice Bulletin No. 19, 2000.
Backos M, Rai R, Baxter N, et al. Pregnancy complications in women with recurrent miscarriage associated with antiphospholipid antibodies treated with low dose aspirin and heparin. Br J Obstet Gynaecol 1999;106:102–107.
Empson M, Lassere M, Craig JC, et al. Recurrent pregnancy loss with antiphospholipid antibody: a systematic review of therapeutic trials. Obstet Gynecol2002;99:135–144.
Levine J, Branch DW, Rauch J. The antiphospholipid syndrome. N Engl J Med 2002;346:752–763.
Rheumatoid Arthritis
Kanik KS, Wilder RL. Hormonal alterations in rheumatoid arthritis, including the effects of pregnancy. Rheum Dis Clin North Am 2000; 26:805–823.
Myasthenia Gravis
Mitchell PJ, Bebbington M. Myasthenia gravis in pregnancy. Obstet Gynecol 1992;80:178.