Dwight J. Rouse
Elaine St. John
LABOR
Labor is defined as regular uterine contractions that lead to effacement and dilation of the cervix. If the estimated gestational age is accurate, labor usually begins within 2 weeks of the estimated date of confinement (EDC), which is 280 days (i.e., 40 weeks after the first day of the last menstrual period). However, because only 3% to 5% of patients actually deliver on their EDC, it has been suggested that EDCs be framed in terms of a range (e.g., from 38 to 42 weeks). Conceptualizing EDCs in this manner, it has been argued, might lessen the pressure for date-predicated interventions such as induction of labor.
Prior to the onset of true labor, there is a general softening and stretching of pelvic ligaments and the soft tissues of the vagina. There is also shortening and dilation (ripening) of the cervix. Braxton Hicks contractions (weak, irregular, regional contractions) usually occur for weeks before the onset of actual labor. The normal stimulus for the biochemical cascade that finally results in labor is unknown. Corticotropin-releasing factor (CRF) plays a role. It is released into the maternal circulation early in the second trimester, and its concentration rises exponentially as pregnancy advances. CRF regulates the secretion of adrenal cortisol, which can increase the strength of uterine contractions. CRF also stimulates production of oxytocin by the fetus and prostaglandins by the placenta.
Other factors probably play a role. For instance, progesterone inhibits and estrogen stimulates uterine contractility. Like CRF, estrogen also stimulates the production of oxytocin receptors in the uterus. Thus, as progesterone levels decline near term, estrogen may stimulate myometrial contractility. Mechanical stretch can also increase uterine contractility, as occurs with twin gestations and pregnancies complicated by polyhydramnios. Once labor is initiated, the process is thought to involve multiple positive feedback loops. For instance, contractions stretch the cervix. Stretching of the cervix elicits a reflex contraction by the uterus, pushing the fetal head against the cervix to stretch it more, and so on.
Labor Progress
Clinically recognizable labor is typically divided into three stages, each with statistically derived normative rates and durations. Many normative labor values were derived from the investigations of Emanuel Friedman, who studied thousands of normal and abnormal labors and plotted cervical dilation and fetal descent against time. The resulting graphic labor curve can be used to recognize individual labor patterns which deviate from normal and to guide the nature and timing of interventions. In a World Health Organization study of 35,484 women, use of a partogram (Fig. 2.1) and an agreed upon labor management protocol was associated with a reduction in the percentage of prolonged labors, the proportion of labors requiring augmentation, and postpartum sepsis.
|
|
|
FIG. 2.1. Flow sheet for following labor progress. (From Chua S, Arulkumaran S. Poor prognosis in labor, including augmentation, malpositions and malpresentations. In: James DK, Steer PJ, Weiner CP, Gonik B, eds. High risk pregnancy, second ed. London: Harcourt Brace, 1999:1105; with permission.) |
The first stage of labor begins with the onset of regular uterine contractions and ends with complete cervical dilation. This stage is further divided into three phases: latent, active, and deceleration, although the existence of the last phase has been questioned. During the latent phase, contractions become progressively stronger, longer, more frequent, and better coordinated. The mother's discomfort may be minimal or it may be severe. The latent phase is considered prolonged if it lasts longer than 20 hours in a nullipara, or 14 hours in a parous woman. The active phase commences when the slope of cervical dilation reaches its maximum. Typically, and especially in the nullipara, this occurs at 3 to 4 cm of dilation. During the active phase, contractions are usually strong and regular, occurring every 2 to 3 minutes. The active phase ends with complete (10 cm) cervical dilation. This phase of labor is generally quite painful. The length of the active phase is more predictable than the latent, lasting, on average, about 5 hours in nulliparas, and 2 hours in multiparas. Without labor epidural analgesia, respective minimum (fifth percentile) rates of dilation are 1.2 cm per hour and 1.5 cm per hour. With epidural, the rates are slower. Progressive descent of the fetal head into the maternal pelvis occurs to a variable degree during the active phase.
The second stage is defined as the period from complete cervical dilation to complete delivery of the baby. During the second stage, contractions are strong and regular, with a frequency of every 1 to 3 minutes. The baby's head descends more deeply into the pelvis, and in women without regional anesthesia, each contraction stimulates a strong urge to push. In combination, uterine contractions and maternal expulsive efforts effect delivery of the baby. The second stage typically lasts about 50 minutes in nulliparas and 20 minutes in multiparas, but is often longer in women with regional anesthesia. The third stage of labor is defined as the period from delivery of the baby to delivery of the placenta. Regardless of parity, the third stage of labor is usually brief (under 10 minutes). The third stage of labor is prolonged if it persists beyond 30 minutes.
The three classic determinants of the progress of labor are:
· Power—uterine contractions and, in the second stage, maternal expulsive efforts
· Pelvis—the bony pelvis and the overlying maternal soft tissues
· Passenger—the fetus and its lie, presentation, and position.
The power of labor can be assessed clinically by uterine palpation or with the use of an intrauterine pressure catheter. Assessment of the pelvis involves manual evaluation of the pelvic inlet, midpelvis, and outlet.
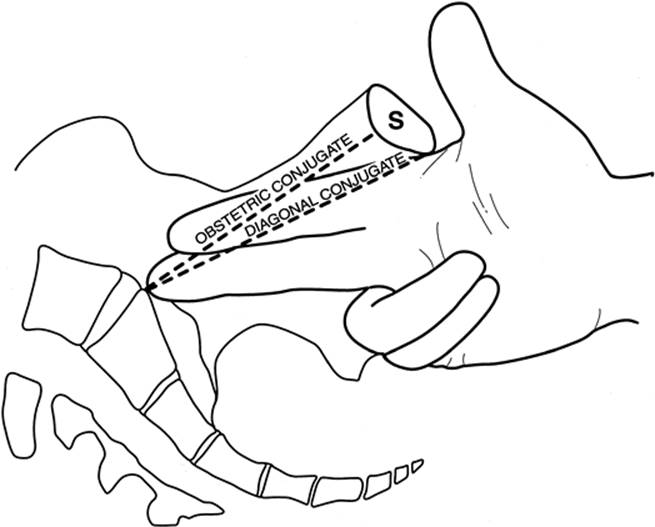
· Pelvic inlet—The transverse diameter of the pelvic inlet averages 13 cm. It cannot be measured clinically, but a narrow transverse inlet is a very rare cause of abnormal labor progress. The anteroposterior (AP) diameter of the inlet is more important. It is estimated clinically by determining the distance between the lower margin of the symphysis pubis and the sacral promontory (Fig. 2.2). This value is known as the diagonal conjugate. The obstetric conjugate—or true AP diameter—is 1.5 to 2.0 cm shorter. The pelvic inlet is an adequate size for a normal fetus if the diagonal conjugate is 12 cm or greater.
|
|
|
FIG. 2.2. The pelvic inlet anteroposterior diameter is estimated from the diagonal conjugate. |
· Midpelvis—The specific diameters of the midpelvis cannot be measured clinically. Contraction of the midpelvis is suspected if the ischial spines are quite prominent (or the sacrosciatic notch is less than two fingerbreadths wide), the pubic arch is narrow, the pelvic side walls converge, or the sacral concavity is quite shallow (Fig. 2.3).
|
|
|
FIG. 2.3. The transverse diameter of the midpelvis is estimated by evaluating the distance between the ischial spines. |
· Pelvic outlet—The transverse diameter of the pelvic outlet should be greater than 8 cm. This diameter can be estimated by placing a fist on the perineum to measure the distance between the ischial tuberosities.
The AP diameter is estimated by noting the angle made by the pubic rami. A contracted outlet is rarely the sole cause of dystocia; however, it is often associated with midpelvis contraction.
Consideration of these measurements allows assignment to one of the various pelvic types, and thus an appreciation of how and where labor may be stalled if the pelvis is not favorable for childbirth (Fig. 2.4). Careful evaluation of the midpelvis is most important, as those women found to have a contracted midpelvis are poor candidates for forceps-assisted vaginal delivery. However, because the fetal skull has the ability to mold, borderline pelvimetry is not a contraindication to a trial of labor.
|
|
|
FIG. 2.4. Pelvic types. A: Gynecoid pelvis—most common, round to oval inlet, ischial spines not prominent, curved sacrum, wide pubic arch; best suited for childbearing. B: Android pelvis—heart-shaped inlet, narrow midpelvis with anterior sacrum, prominent ischial spines, convergent side walls, narrow pubic arch. C: Platypelloid pelvis—least common, decreased anteroposterior dimensions at all levels with wide transverse dimensions. D: Anthropoid pelvis—narrow inlet, midpelvis, and pubic arch. |
From the perspective of the passenger (fetus), labor involves movement progressively downward through the pelvis by the following cardinal movements (Fig. 2.5).
|
|
|
FIG. 2.5. Cardinal movements of labor. A: Engagement. B: Flexion. C: Descent and internal rotation. D, E: Extension. F: External rotation. |
· Engagement occurs days to weeks prior to labor for primigravidas and at the onset of labor for multigravidas.
· Flexion of the neck allows the occiput to lead, thus the smallest possible diameter of the fetal head travels downward through the pelvis.
· Descent is progressive as the cervix thins, and the lower uterine segment lengthens.
· Internal rotation occurs during descent. The vertex rotates from transverse to either a posterior or anterior position to pass the ischial spines.
· Extension occurs as the fetal head distends the perineum and the occiput passes beneath the symphysis.
· External rotation of the head after delivery to a transverse position allows the shoulders to rotate internally to an AP position.
MANAGEMENT OF LABOR AND DELIVERY
Antepartum Instructions
All women should be advised of the circumstances that should prompt them to seek evaluation for labor. These include (a) possible rupture of the membranes, (b) regular uterine contractions, (c) bleeding per vagina, and (d) back, pelvic, or abdominal pain greater than they are anticipating. Nulliparas are more likely to confuse false labor or Braxton Hicks contractions with true labor. Although distinguishing the two can be problematic, the contractions of false labor tend to be irregular both in intensity and in interval, and the associated discomfort, if any, is typically limited to the lower abdomen and groin. The contractions of false labor usually abate with time, analgesia, or sedation. With true labor, the contractions progressively increase in intensity. They occur every 2 to 4 minutes and cause discomfort in the abdomen and back with the associated sensation of increasing pelvic pressure. For many women labor will be preceded, by several hours or even days, by the passage of bloody show (a small amount of bloody mucous discharge from the cervix). In 10% of pregnancies, chorioamnion rupture precedes the onset of labor, and amniotic fluid leaks through the cervix and out of the vagina. Optimal management for such women has recently been clarified. A randomized trial of over 5000 women with prelabor rupture of membranes at term demonstrated that induction of labor with oxytocin (as opposed to expectant management, or induction with prostaglandins) resulted in the lowest rate of neonatal infection and maternal postpartum fever, and did not increase the cesarean delivery rate. In many cases, the only way to confirm the diagnosis of true labor is observation over several hours and examination of the cervix for change.
Admission
If the woman is having contractions, their time of onset and frequency should be recorded. Questions should focus on spontaneous rupture of the membranes, presence or absence of bleeding, and fetal activity. A review of the patient's prenatal record should take specific note of her EDC and its reliability, as well as her past medical and surgical history, and details of previous pregnancies: number, gestation, fetal size, duration of labor, and any complications (e.g., shoulder dystocia). Prenatal laboratory data should be reviewed, including blood type, hematocrit, Rh0(D) immune globulin requirements, VDRL test, rubella immunity, and hepatitis and human immunodeficiency virus (HIV) status.
The admission physical examination should include vital signs (temperature, pulse, blood pressure), auscultation of the heart and lungs, and a brief neurologic examination. Leopold maneuvers should be performed to assess fetal position (Fig. 2.6), and the uterus should be palpated, or a tocodynamometer employed, to determine the frequency, intensity, and duration of uterine contractions. Fundal height should be evaluated and a clinical assessment of fetal weight should be performed. Fetal heart tones should be assessed, either by auscultation or via electronic monitoring, with specific attention to the response of the fetal heart rate (FHR) to the uterine contractions.
|
|
|
FIG. 2.6. Leopold maneuvers. First maneuver: The uterine contour is outlined; the fundus is palpated, allowing identification of the fetal parts. Second maneuver: By palpation of the sides of the maternal abdomen, the location of the fetal back is determined. Third maneuver: The presenting part is grasped, identified, and evaluated for engagement. Fourth maneuver: With palpation toward the pelvis, the identity of the presenting part is confirmed, and flexion or extension of the fetal head is evaluated. |
The vulva should be examined for herpetic lesions. If membrane rupture is suspected, it should be confirmed (or ruled out). Several signs support rupture, including pooling of amniotic fluid in the vagina (observed by sterile speculum examination) or direct visualization of fluid leakage through the cervix. The pH of the pooled fluid can be checked with nitrazine paper, which turns blue in the presence of amniotic fluid (but also in the presence of blood), and an air-dried sample (on a slide) of the fluid can be examined under a microscope for the characteristic “fern” pattern that confirms the presence of amniotic fluid (Fig. 2.7). Since cervical mucus and maternal serum can demonstrate a fern pattern, care must be taken in collection of this sample. Palpation of the cervix includes attention to the following:
|
|
|
FIG. 2.7. Typical ferning pattern of dried amniotic fluid (400×). (Original photo, courtesy of Dr. Dwight Rouse.) |
· assessment of consistency (soft or firm)
· degree of effacement (Fig. 2.8)
|
|
|
FIG. 2.8. Degree of cervical effacement. A: No effacement. B: 75% effacement. C: 100% effacement. |
· dilation of the cervical os
· location of the cervical os with respect to the vaginal axis (posterior, midplane, or anterior).
The presenting part should be identified by palpation. Station is determined by noting the position of the fetal presenting (bony) part relative to the ischial spines (Fig. 2.9). The fetal position is determined by noting the orientation of occiput relative to the maternal pelvis (Fig. 2.10).
The attitude of the fetal head is the position of the fetal head relative to the fetal chest and any lateral flexion of the head (Fig. 2.11, Fig. 2.12 and Fig. 2.13). Pelvimetry should be performed as previously described.
|
|
|
FIG. 2.9. Stations of the fetal head. At the 0 station, the fetal head is at the bony ischial spines and fills the maternal sacrum. Positions above the ischial spines are referred to as -1 through -5, referring to the number of centimeters that the head is positioned above the spines. As the head descends past the ischial spines, the stations are referred to as +1 through +5 (head visible at the introitus). |
|
|
|
FIG. 2.10. Fetal position. The orientation of the presenting vertex within the maternal pelvis. |
|
|
|
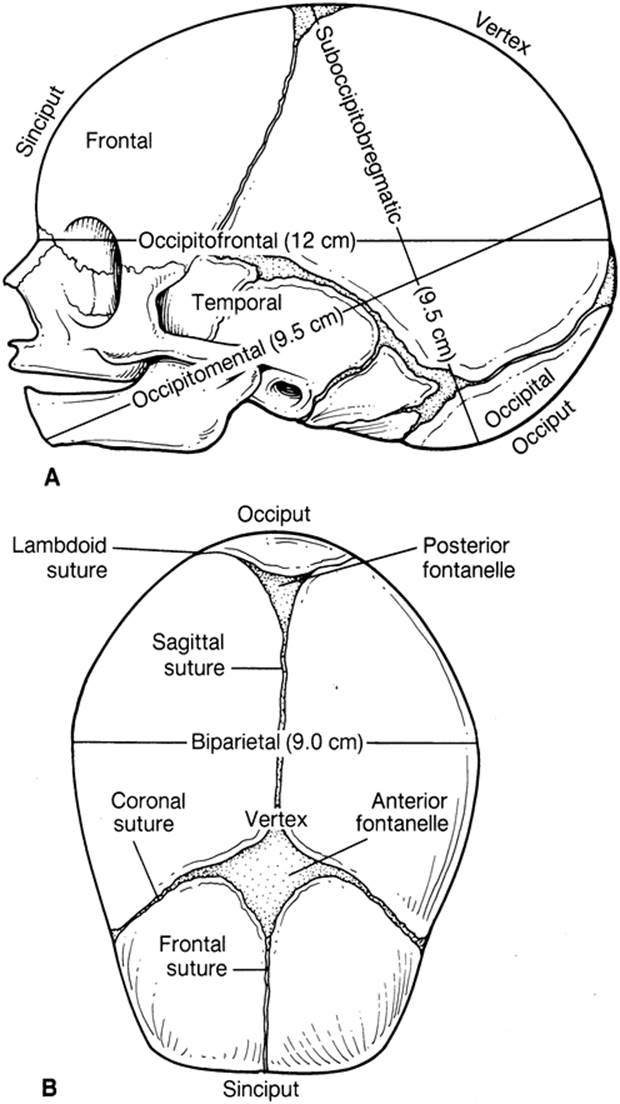
FIG. 2.11. A, B: The bones, sutures, fontanelles, and clinically important diameters of the fetal head. |
|
|
|
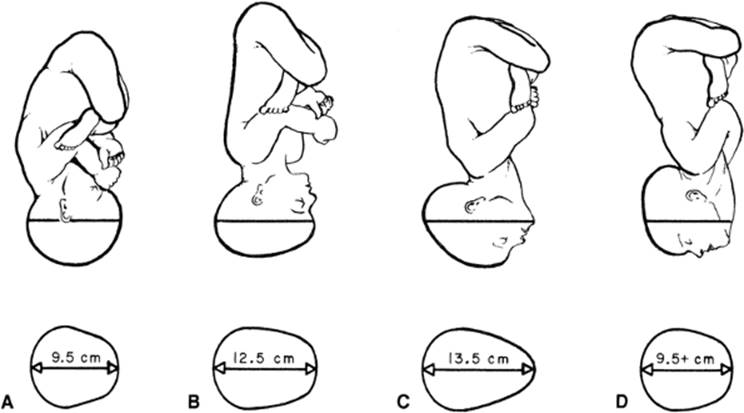
FIG. 2.12. Fetal attitude and dimensions of a term-size fetus. A: Full flexion presents the smallest circumference of the fetal head to the narrower planes of the pelvis. B: Military attitude usually changes to full flexion with descent into the pelvis. C: Brow presentation usually converts to full flexion or a face presentation, as the occipitomental diameter is too large for all except the largest pelves to accommodate. D: Face presentation shows dimensions that allow descent through the pelvis, unless the chin is posterior. Persistent mentum posterior must be delivered by cesarean section. |
|
|
|
FIG. 2.13. Fetal attitude and lateral flexion of the fetal head. A: Synclitism—The plane of the biparietal diameter is parallel to the plane of the inlet. B:Asynclitism—Lateral flexion of the fetal head leads to anterior parietal or posterior parietal presentation. |
In women at term with rupture of the membranes prior to the onset of labor, it is appropriate to defer digital examination of the cervix until they are in active labor, to decrease the risk of chorioamnionitis. It is important, however, to confirm the baby's presentation, and an ultrasound examination should be performed if the presentation is not clear.
Management of the First Stage of Labor
A variety of management approaches to the first stage of labor have been employed and evaluated, and no single approach is clearly superior. The primary management goals are to monitor fetal well-being, support the woman through what can be a lengthy, uncomfortable period, and offer intervention as it may become appropriate. Support of the woman through labor includes allowing her to assume whatever position is most comfortable (or least uncomfortable) for her. All forms of monitoring, be it intermittent auscultation, external fetal monitoring, or internal monitoring, can be accomplished in a lying, sitting, or upright position. In most normal labors, the only time a healthy woman's movements must be limited is after she has received analgesia and would not be steady on her feet. Uterine blood flow is maximal in the lateral recumbent position, and this should be the initial position adopted if there is concern over fetal well-being. Because of impaired venous return and reduced maternal cardiac output, the supine position is usually best avoided. With these considerations in mind, women should be free to position themselves as they like.
Vital signs should be monitored at least every 4 hours, or more frequently as clinically indicated. By consensus of the Centers for Disease Control and Prevention and the American College of Obstetricians and Gynecologists (ACOG), all women whose 35-37 week rectovaginal group B streptococcus (GBS) culture was positive should receive intrapartum antibiotic prophylaxis for the prevention of early onset neonatal GBS disease. Acceptable prophylactic antibiotic regimens include intravenous penicillin G 5 million units initially, and then 2.5 million units every four hours until delivery, or intravenous ampicillin 2 gm initially, followed by 1 gm every 4 hours until delivery. For women allergic to penicillin, clindamycin, erythromycin, vancomycin, or, in women without a urticarial or anaphylactoid response to penicillin, a first generation cephalosporin may be substituted.
Irrespective of rectovaginal culture results, women with GBS bacteriuria during the pregnancy and those who have previously delivered an infant with early onset GBS disease should also receive antibiotic prophylaxis. If an appropriate rectovaginal GBS culture was not performed or is not available, prophylaxis should be based on the following risk factors: threatened pre-term delivery (< 37 weeks), GBS bacteriuria at any time in the current pregnancy, fever (≥ 38.0°C), rupture of membranes for at least 18 hours, or delivery of a prior infant with early onset GBS disease. Separate from the issue of GBS prophylaxis, if a woman develops an intrapartum fever, defined by some authorities as a temperature of at least 37.8°C (100.0°F) and by others as at least 38.0°C (100.4°F), evaluation and treatment for chorioamnionitis may be indicated.
Placement of an intravenous line is not necessary for all women in labor. However, women who are dehydrated may benefit from intravenous hydration. It seems prudent to establish intravenous access for administration of fluids and medication, should they be necessary, in women at increased risk of postpartum hemorrhage (i.e., those with prior postpartum hemorrhage, prolonged labor, or overdistended uterus).
In most women, laboratory evaluation upon presentation in labor can be minimized. Although in many units it is customary to perform routine admission blood type and antibody screen, hemoglobin and hematocrit, and syphilis serology, the necessity and cost-effectiveness of repeating these tests in healthy women who have received adequate prenatal care is debatable. Certainly, if a woman has hypertension on admission, she should be evaluated for possible preeclampsia. In women who have not had any prenatal care, it is advisable to order a hemoglobin and hematocrit, blood type, and Rh status, an antibody screen, a rubella titer, and syphilis, hepatitis, and HIV screens.
The benefits of continuous caregiver support (by nurses, midwives, or laypeople) throughout labor have been established by multiple randomized trials. Salutary effects of such support include reduced pain medication requirements, lowered rates of operative vaginal and cesarean delivery, and a diminution in the frequency of 5-minute Apgar scores below 7. Thus, to the extent possible, all women should have access to continuous caregiver support throughout labor.
No evidence-based criteria are available to direct how often the cervix should be examined during the first stage of labor. In general, frequent examinations in the latent phase of labor serve little purpose. They may unrealistically increase a woman's expectation for progress in labor and in addition, are uncomfortable and increase risk for infectious morbidity. However, during observation, if the membranes rupture, the cervix should be examined and the FHR evaluated if the presenting part was not well applied to the cervix on previous examination. These measures should enhance the detection of umbilical cord prolapse. In the active phase of labor, monitoring the progress of labor with cervical examinations every 2 hours allows identification of those women who are not making normal progress and who should therefore be evaluated for oxytocin augmentation.
During labor, the FHR should be monitored. For most women, both intermittent auscultation and intermittent or continuous electronic monitoring are acceptable (see Chapter 9). While artificial rupture of membranes (amniotomy) may shorten the duration of labor by 1 to 2 hours and reduce the use of oxytocin, it may also increase the risk of cesarean delivery by 25%. Thus, in most women, amniotomy should be reserved for such indications as placement of internal fetal monitoring devices for better assessment of the FHR pattern, or for abnormal labor progress. To avoid umbilical cord prolapse, amniotomy is best performed when the presenting part is well applied to the cervix, and preferably during a contraction (or with fundal pressure) to minimize the chance for dislodging the fetal head. Although typically performed with a thin, plastic, hook-ended tool designed specifically for the purpose, amniotomy may be achieved simply by placing a fetal scalp electrode. In cases of excess amniotic fluid, or when the vertex is not well applied, a spinal or pudendal block needle may be used to create a small opening in the membranes to allow the gradual egress of amniotic fluid, thereby avoiding umbilical cord prolapse or the rapid decompression of the uterus and the associated risk of placental abruption.
Meconium staining of the amniotic fluid occurs in up to one-fifth of deliveries. Meta-analysis of randomized trials performed in settings of standard perinatal surveillance demonstrates that with moderate or severe meconium staining, amnioinfusion of 500 to 1000 mL (or more, depending on the protocol) of sterile saline into the uterus (through an intrauterine catheter) will reduce variable heart rate decelerations and may lower the risk of cesarean delivery. In settings of limited perinatal surveillance, amnioinfusion reduces the risk of meconium aspiration syndrome, neonatal hypoxic ischemic encephalopathy, neonatal ventilation or intensive care unit admission, and perhaps perinatal mortality.
Management of the Second Stage of Labor
The onset of the second stage of labor with complete dilation of the cervix is usually noted by the woman as the presenting part descends into the vagina and she experiences the urge to push with contractions. However, regional anesthesia may partially or completely blunt this urge. The cervix should be examined at this time to confirm complete dilation, and the position and station of the presenting part should be ascertained. Whether nulliparous women with regional anesthesia should begin expulsive efforts in the absence of an urge to push was the subject of a multicenter, randomized clinical trial. In the trial, women allocated to immediate pushing were less likely to have intrapartum fever (4.5% vs. 8.5%). Moreover, their second stages were one hour shorter. However, difficult deliveries (defined as midpelvic operative vaginal deliveries, low-pelvic rotational deliveries, or second stage cesarean delivery) were less common (18% vs. 23%) in the delayed pushing group, who were instructed to not push until the urge was irresistible or the head was on the perineum. Neonatal outcomes were equivalent between the groups. This trial thus supports individualization in the timing of maternal expulsive efforts.
Support of a woman in the second stage involves allowing her to find the most comfortable and effective position for pushing, as well as encouraging her efforts. Preparations for delivery should be made when the presenting part begins to distend the perineum and often sooner for multigravidas. Local or pudendal anesthesia, if necessary, should be administered at this time.
An episiotomy is an incision in the perineum used to facilitate vaginal delivery. It is useful for patients in whom the perineum does not readily stretch and when delivery must be expedited. In the past, routine episiotomy was advocated to prevent subsequent pelvic relaxation; however, there is no evidence that it does so. Meta-analysis of randomized episiotomy trials, in which restrictive episiotomy use (~ 30% of women underwent episiotomy) was compared to liberal use (~70% episiotomy rate), reveals the following. Restrictive use of episiotomy lowers the risk of posterior perineal trauma, lessens the need for suturing, and is associated with fewer healing complications. However, restrictive use of episiotomy increases the risk of anterior perineal trauma. There is no difference between the two policies in severe vaginal or perineal trauma, or subsequent dyspareunia, urinary incontinence, or perineal pain.
There are two basic types of episiotomy: midline and mediolateral. The benefits of a midline episiotomy include anatomic end results, easy repair, and lower incidence of postpartum pain or dyspareunia. A mediolateral episiotomy is less likely to extend into the anal sphincter or rectal mucosa, but is generally believed to result in more pain, dyspareunia, and excessive blood loss. Episiotomy should not be performed until delivery is imminent. A midline incision is made with scissors from the midpoint of the posterior fourchette directly backward toward the rectum (Fig. 2.14). The midline episiotomy is subdivided as follows:
|
|
|
FIG. 2.14. Midline episiotomy. A: As the fetal head distends, with the perineum under adequate anesthesia, the episiotomy is cut through the perineal body and the tissues of the vagina and the rectovaginal septum. B: The episiotomy is repaired by reapproximating the vaginal mucosa in a running fashion with a delayed absorbable suture. C: The submucosal tissue of the vagina and the subcutaneous tissue and fascia of the perineal body are then closed. D:The skin is then reapproximated with a running subcuticular suture. |
· first degree—through the mucosa only
· second degree—through the mucosa and subcutaneous tissues, including the muscles of the perineal body
· third degree—into or through the anal sphincter
· fourth degree—through the rectal mucosa.
A mediolateral incision is made with scissors from the midpoint of the posterior fourchette at a 45-degree angle laterally on either side.
Regardless of use of an episiotomy, tears and extensions into the rectum are best prevented by keeping the baby's head well flexed until the occiput passes beyond the subpubic arch. As the vertex appears beneath the symphysis, the perineum is supported by direct pressure from a draped hand over the coccygeal region. As the head delivers, it will rotate to a transverse position; the mother should be encouraged to continue to push to achieve delivery of the anterior shoulder. A quick evaluation for the presence of the umbilical cord around the baby's neck (nuchal cord) should be carried out. A nuchal cord can usually be slipped around the baby's head. Occasionally, it must be double-clamped and cut if it is too tight to reduce. Maternal pushing efforts can be assisted by placing gentle downward traction on the baby's head. With delivery of the anterior shoulder, a moment can be taken to bulb suction the baby's nose and mouth. Renewed pushing by the mother in combination with gentle upward traction by the obstetrician will achieve delivery of the posterior shoulder. The baby's body generally delivers easily following the shoulders. Care must be taken to support the baby's head and ensure that the baby does not slip from one's grip. After confirmation of good respiration and normal heart rate (easily checked at the cord insertion at the umbilicus), the baby may be given to the mother to cradle. The cord is then double-clamped and cut, and cord blood collected. The baby should be dried and wrapped soon following delivery to maintain its body temperature.
Management of the Third Stage of Labor
The third stage of labor begins following the delivery of the baby and ends with the delivery of the placenta. Signs of spontaneous placental separation include an apparent lengthening of the umbilical cord, a gush of vaginal bleeding, and a change in shape of the uterus from discoid to globular along with a rise in fundal height. Active management of the third stage of labor, which involves prompt umbilical cord clamping and cutting, administration of an oxytocic agent, and gentle umbilical cord traction, reduces maternal blood loss and the frequency of postpartum hemorrhage, and lessens the risk that the third stage will be prolonged. Cord traction should be used only against fundally applied counter-traction (Fig. 2.15) to lessen the potential for uterine inversion and catastrophic hemorrhage. If at any time heavy bleeding occurs during the third stage of labor or if the placenta is not delivered within 30 minutes of the birth, the placenta should be manually removed. The anesthesiologist should be alerted at this time, as general anesthesia may be required for women who have no regional anesthesia, and curettage may be necessary if the placenta does not readily separate from the uterine wall. Manual removal is accomplished by developing a cleavage plane with the intrauterine hand between the maternal surface of the placenta and the uterine wall, while simultaneously fixing the uterus with the abdominal hand, and progressively peeling the placenta free. To ensure complete placental removal, a 4-inch by 4-inch gauze may be wrapped around the hand and used to abrade the uterine wall. The placenta should then be carefully inspected for cord insertion, confirmation of a three-vessel cord (infants with only two cord vessels have a higher rate of malformations and warrant closer evaluation by the newborn caregiver), and completeness of the placenta and membranes. If any portion of the placenta or the membranes is missing, the uterine cavity should be manually explored. Some advocate routine exploration of the uterine cavity to reduce the risk of infection and bleeding from retained placental fragments. In most women, especially those without regional anesthesia, the benefit of manual exploration is outweighed by the discomfort it causes, as well as the increased risk for uterine infection.
|
|
|
FIG. 2.15. Stage three of labor: delivery of the placenta. A: Spontaneous separation of the placenta is confirmed. B: With gentle traction on the umbilical cord and suprapubic palpation of the fundus, the placenta and membranes are delivered. C: If spontaneous separation of the placenta does not occur or bleeding ensues, the placenta is manually separated from the wall of the uterus and removed. |
The uterus should be frequently palpated following delivery of the placenta to ensure that it remains well contracted. Oxytocin, 10 to 20 U administered intramuscularly or as a dilute intravenous solution, has been demonstrated to decrease the incidence of postpartum hemorrhage secondary to uterine atony. The birth canal, including the cervix, vagina, and perineum should be inspected for lacerations requiring repair. During this time, under most circumstances and after drying and swaddling, the baby should be kept with the family and, for women planning to breast-feed, placed to the breast to nurse within the first 10 to 20 minutes after birth. This first suckling not only stimulates endogenous oxytocin release but also begins the process of milk production and successful breast-feeding.
Management of the “Fourth Stage” of Labor
Because many complications of birth occur or become evident during the first hour after delivery, this time has been referred to as the “fourth stage” of labor, though it is not officially defined as a labor stage. The new mother should be seen at least every 15 minutes by a trained labor and delivery nurse to assess vital signs and look for evidence of uterine atony or postpartum hemorrhage. The perineum should be inspected for any signs of hematoma formation, which may be signaled by inordinate vulvar or rectal pain. The newborn should undergo its initial assessment at this time and be observed closely for any signs of compromise.
Postpartum Care
After the first 24 hours, postpartum recovery is rapid. A regular diet can be offered to most women as soon as they request food, sometimes shortly after delivery. Because of their risk to require general anesthesia, it is prudent to delay feeding women who have experienced, or are at risk for, significant postpartum hemorrhage. Full ambulation is encouraged as soon as possible. Exercises to improve tone and strengthen abdominal muscles may be started after 1 day. The perineum should be cleansed with warm water two or three times daily after voiding or bowel movements. Both showers and baths may be taken, but vaginal douching is prohibited during the early puerperium to avoid the risk of introducing infection into the uterus. Pain from an uncomfortable perineal laceration or episiotomy can be relieved with warm sitz baths and an analgesic (e.g., acetaminophen, 650 mg, with or without codeine or ibuprofen, 600 to 800 mg) (Table 2.1).
|
|
|
TABLE 2.1. Examples of orders after routine vaginal delivery: immediately postpartum |
When regional anesthesia is used, care must be taken to avoid problems with urinary retention and bladder overdistention. Women should be encouraged to void every 2 to 3 hours, even if they are not aware of any sensation of bladder fullness, as rapid diuresis may occur following delivery, especially when oxytocin is discontinued.
Prior to discharge, a hemoglobin or hematocrit should be checked if there is any concern that a woman has experienced heavier than normal postpartum bleeding, or if she entered labor significantly anemic. In addition, seronegative women should be immunized against rubella on the day of discharge. If the mother is Rh-negative, is not sensitized, and has an Rh-positive infant, she should be given Rh0(D) immune globulin to prevent sensitization from occurring. As discharge from the hospital now occurs anywhere from 12 to 48 hours following an uncomplicated birth, most women have not begun milk production prior to their discharge. To support breast-feeding, it is critical to advise women of the availability of assistance, should they experience any difficulty with nursing. Binding and avoiding any stimulation of the breasts are advised if the mother does not plan to breast-feed. She should also take aspirin, acetaminophen, or ibuprofen if engorgement becomes uncomfortable.
The length of inpatient hospitalization following childbirth has changed remarkably over the past two decades, reflecting the decreasing risk of postpartum complications and changing medical and societal attitudes toward birth, as well as pressures from third-party payors. Numerous reports, including three randomized, controlled trials have shown early discharge, 12 to 24 hours postdelivery, with appropriate follow-up in the home results in a low and acceptable rate of readmission of mothers and babies. Several studies show that longer hospital stays improve maternal postpartum adjustment and breast-feeding success. Stays of 12- to 24-hours are only acceptable when patients have adequate help in the home and the community has a home care nursing program with 24-hour coverage, 7 days a week. Home care services, while not always necessary, can be very helpful and appear to increase the safety of early discharge. All women and their babies discharged within 24 hours of birth should be offered a minimum of one home visit or an appointment for outpatient follow-up in the first few days following discharge.
PUERPERIUM
The puerperium is the 6 to 8 weeks following delivery of the placenta, in which the uterus returns to its normal state. Following delivery of the placenta, the uterus rapidly contracts to half of its predelivery size. The involution that then occurs over the next several weeks is most rapid in women who breast-feed their newborns. Postpartum vaginal discharge, or lochia, changes as the uterus involutes. Initially, the discharge is grossly bloody (lochia rubra), persisting for 3 to 4 days. It then decreases in volume and changes to pale brown and becomes thinner (lochia serosa), persisting for 10 to 12 days. Finally, the discharge becomes yellowish white, occasionally tinged with blood (lochia alba), and may persist for several weeks. The total volume of lochia is about 250 mL, and women are usually encouraged to use external pads to absorb it, rather than intravaginal tampons, in order to minimize the risk of infection. When followed closely, a woman's hematocrit may actually rise due to diuresis following delivery and autotransfusion occurring as the uterus involutes. After 1 week, the uterus is firm and nontender and extends to about midway between the symphysis and the umbilicus. By 2 weeks postpartum, the uterus should no longer be palpable abdominally. The contractions of the involuting uterus may be painful, especially during the first few days following delivery. These “after pains” are usually relieved with acetaminophen or ibuprofen.
Prior to discharge, women should receive instructions regarding what they can expect during the puerperium and recommendations for activity. In general, women should be encouraged to rest as they feel necessary and gradually increase their activity following delivery. They do not need to be restricted in terms of ambulation, but should be cautioned that driving in the early postpartum may not be advisable if perineal discomfort is distracting, or would cause a delay in reaction in case of an emergency. Women can resume a regular diet, and, if nursing, should be encouraged to keep well hydrated. Perineal pain should gradually diminish. If it does not, or it worsens, women should be instructed to seek evaluation for possible infection or hematoma. Normal bladder function should resume, but women should be cautioned that they may experience some difficulty with stress and urge incontinence, which can be expected to gradually improve in the months following delivery.
Parents should receive information regarding lochia, expected volume, changes, and duration; activities; care of the breasts, perineum, and bladder; and dietary and, specifically, fluid requirements. The specific signs of complications should be stressed, including fever, chills, leg pain or swelling, episiotomy pain or drainage, and abnormal duration or amount of bleeding.
Couples should be advised that they can safely resume coitus when desired and comfortable; however, abstaining for at least 2 weeks following the birth is often recommended. They should be forewarned of potential discomfort of the perineum and problems with vaginal dryness due to atrophic vaginitis, as well as the potential for transient changes in libido related to pregnancy and delivery.
For women who are breast-feeding, ACOG has summarized hormonal contraceptive options (Table 2.2).
Women who are not nursing and desire a combination oral contraceptive can safely have this method initiated 1 to 2 weeks following delivery. Long-acting progestin contraception such as medroxyprogesterone acetate (Depo-Provera) injections or levonorgestrel implants (Norplant System) can be started or placed anytime following delivery. A diaphragm should be fitted only after complete involution of the uterus at 6 to 8 weeks postpartum. In the meantime, condoms and spermicidal foam or jelly should be used. Intrauterine devices can be placed immediately following delivery of the placenta; however, insertion at this time is associated with an increased risk of expulsion. Thus, waiting until 6 to 8 weeks postpartum may be preferable.
|
|
|
TABLE 2.2. ACOG recommendations for hormonal contraception if used by breast-feeding women |
In nonlactating women, ovulation usually occurs about 6 weeks postpartum. The first menses following delivery is often an anovulatory cycle; however, conception has been reported as early as 2 weeks postpartum, so contraception must be advised even in the early postpartum period. While women who exclusively breast-feed their babies usually do not ovulate for at least 3 months following delivery, an occasional nursing mother will ovulate early, and thus contraception use should be advised. Women who receive rubella immunization, which is a live vaccine, are advised to delay pregnancy for at least a month. Women should be cautioned about postpartum depression. Instructions from the pediatrician regarding care of the neonate should be reinforced, as well as encouraging follow-up should any problems occur.
Although its value is open to question, it is customary to schedule an office visit 4 to 6 weeks postpartum. At this visit, inquiries should be made regarding breast-feeding, continued bleeding, resumption of sexual intercourse, use of appropriate contraception, and any difficulty with regard to voiding or bowel movements. A focused physical examination can be performed, and a Pap smear obtained, if indicated. Women should be counseled regarding emotional lability in the postpartum period and reassured that intervention is available should she experience clinically significant depression.
Complications of the Puerperium
Puerperal Infection
Fever (a temperature of at least 38°C or 100.4°F) is the most commonly observed sign of puerperal infection. The differential diagnosis includes infections of the perineum, vagina, uterus, parametrium, bladder, kidneys, or breast. Noninfectious causes of fever such as thrombophlebitis and breast engorgement must also be considered. After vaginal delivery, endometritis is infrequent but may be presaged by chorioamnionitis. Various obstetric factors increase the risk of endometritis; two of the most consistent are prolonged rupture of the membranes and prolonged labor, both of which are often associated with multiple intrapartum cervical examinations, which also add to the risk. Endometritis is usually caused by normal vaginal flora, including Escherichia coli, β-hemolytic streptococci, facultative organisms such as Streptococcus faecalis, and anaerobes such as Peptostreptoccus, Bacteroides, and Prevotella species. Most infections involve mixed flora, but progression to an anaerobic infection is a particular risk following cesarean delivery.
Women suffering with serious puerperal infection of the reproductive tract frequently complain of chills, headache, malaise, and anorexia. Physical examination usually reveals tachycardia and often pallor. If the uterus is involved, it is usually tender and may be large and boggy. Lochia may be diminished if the cervix is blocked, or it may be profuse and malodorous. Parametrial involvement, peritonitis, and pelvic thrombophlebitis may complicate the illness. Endotoxic shock or a virulent puerperal sepsis may develop in a relatively short time and can be fatal. Prompt and aggressive management with broad-spectrum antibiotics—and potentially surgery—is mandatory (see Chapter 19).
Postpartum Hemorrhage
Postpartum hemorrhage has been defined as a blood loss of greater than 500 mL during or after the third stage of labor. This definition is somewhat paradoxical, as careful measures of blood loss following delivery indicate that the average is approximately 500 mL. After hypertensive disorders and embolism, postpartum hemorrhage is the major cause of maternal mortality for women who reach the second trimester. The major cause of postpartum hemorrhage is uterine atony, or failure of the uterus to contract sufficiently after delivery. This failure inhibits the major hemostatic mechanism of the postpartum uterus—myometrial contraction with constriction of placental bed arteries and veins. Risk factors for uterine atony include prolonged or oxytocin-augmented labor, uterine overdistension (as with polyhydramnios, fetal macrosomia, or multiple gestation), chorioamnionitis, grand multiparity, and a history of postpartum hemorrhage. Halogenated anesthetic agents also inhibit uterine contractility, and very rapid labors have been associated with failure of the uterus to contract adequately after delivery. Additional causes of postpartum hemorrhage are vaginal or cervical lacerations, and retained products of conception. Most serious hemorrhages occur within the first 24 hours after delivery but may occur even weeks after delivery.
If hemorrhage occurs, and uterine atony is the presumptive cause, bimanual uterine compression (using a fist in the anterior vaginal fornix and the other hand on the abdomen, open and compressing the posterior uterine wall) should be performed and dilute intravenous oxytocin (40 to 80 units per L) administered. Large bore intravenous access should be secured. If bleeding persists, the vagina and cervix should be inspected for bleeding lacerations, and these should be sutured if found. The uterus should be manually explored for retained placental fragments or membranes. Intramuscular injection of methylergonovine maleate (0.2 mg) or prostaglandin F2 (0.25 mg) can aid in stimulating contraction of the atonic uterus. Both may exacerbate or provoke hypertension. Preparation should be made to replace blood and blood products as necessary to prevent the development of a consumptive coagulopathy. If contractions cannot be stimulated in a refractory atonic uterus, laparotomy with uterine artery ligation, hypogastric artery ligation (if a skilled, experienced surgeon is available and the woman is hemodynamically stable) or hysterectomy may be required. If bleeding from a vaginal wall laceration is persistent, packing, angiography, and selective embolization may be helpful.
Depression
Many mothers (at least half) feel an emotional letdown during the first few days after delivery. These “maternity blues” are characterized by bouts of sadness, crying, and lability of mood. This state is usually, but not always, short-lived and seldom persists beyond 2 weeks. No specific therapy other than emotional support is indicated. More seriously, up to 20% of women may experience a major postpartum depression, characterized by such symptoms as insomnia, pessimism, lethargy, feelings of inadequacy, inability to cope, and fatigue. In women with these symptoms, it is important to rule out postpartum hypothyroidism. Both counseling and medication (usually with a selective serotonin reuptake inhibitor) may be indicated. Profound, persistent depression or that associated with lack of interest in the infant, suicidal or homicidal thoughts, hallucinations, or psychotic behavior should prompt psychiatric consultation. The recurrence risk for postpartum depression is high, and prophylactic therapy beginning 2 to 3 weeks before delivery may be indicated. An earlier postpartum visit should be considered for women at risk of postpartum depression including those with a prior history of depression not associated with pregnancy. Puerperal psychosis (hallucinations, suicidal impulses) is unusual but may complicate as many as 1 in 500 pregnancies. It is an emergency which should be immediately attended to by a psychiatrist to prevent the mother from harming herself or her infant.
Breast-feeding
Breast-feeding has undergone somewhat of a renaissance in the United States over the past 30 years: in 1971 only one-fourth of mothers breast-fed at hospital discharge, versus almost two thirds in 1998. In 1997, the AAP summarized the manifest benefits of breast-feeding for the infant (Table 2.3).
|
|
|
TABLE 2.3. Research on established and potential protective effects of human milk and breast-feeding on infants |
Breast-feeding mothers benefit as well. Suckling-triggered oxytocin release promotes uterine contractions and leads to diminished blood loss. Oxytocin and prolactin levels are elevated in breast-feeding mothers, enhancing feelings of attachment and relaxation. Women who breast-feed face lower risks of ovarian and premenopausal breast cancer, and are less subject to pregnancy-induced obesity. By delaying ovulation, breast-feeding contributes to longer interpregnancy intervals.
Almost all women may breast-feed. However, some women should not. According to the ACOG, these include women who:
· take street drugs or do not control alcohol use
· have an infant with galactosemia
· are infected with HIV
· have active, untreated tuberculosis
· take certain medications
· are undergoing treatment for breast cancer.
Additionally, women with active varicella infections, herpes simplex virus infections of the breast, and active hepatitis A and B (until the infant has been passively and actively vaccinated) should refrain from breast-feeding. The list of medications contraindicated in breast-feeding is not extensive. It includes bromocriptine, cocaine, cyclophosphamide, cyclosporine, doxorubicin, ergotamine, lithium, methotrexate, phencyclidine, phenindione, and radioactive iodine and other radiolabeled elements. Women who want to breast-feed but who receive radioactive elements on a one-time or short-term basis (as for a diagnostic study) can pump and discard their milk until the radioactivity has cleared their bodies.
Premature infants can be breast-fed, but may have special nutritional requirements, especially those born very prematurely. Consultation is necessary to ensure adequate nutrition for such babies. Mothers whose babies are temporarily unable to breast feed may pump their breasts (which is most efficiently done with an electric pump) and the milk may be administered to the baby or stored for later use (frozen unless use is planned within 2 days).
Lack of education and knowledge, both on the part of caregivers and mothers, is the biggest barrier to breast-feeding. To redress this deficiency, ACOG has compiled two lists of resources (Table 2.4, Table 2.5). It is incumbent upon obstetric and pediatric care providers to provide education, support, and assistance to allow women to begin and maintain successful breast-feeding. These activities should begin at the first prenatal visit (or even sooner, e.g., routine gynecologic health visits) and continue throughout the pregnancy and postpartum period. Hospital protocols and care delivery should be conducive to breast-feeding, and specific practices to support breast-feeding have been enumerated (Table 2.6). Since most women are discharged before their milk comes in, most questions and problems with breast-feeding are handled on an outpatient basis. Therefore, to achieve successful, sustained breast-feeding among their patients, physicians and their office staff must have the ability to field questions and promptly correct problems with nursing.
|
|
|
TABLE 2.4. Patient breast-feeding education materials |
|
|
|
TABLE 2.5. References for health care workers and patients seeking in-depth information about breast-feeding |
|
|
|
TABLE 2.6. Ten hospital practices to encourage and support breast-feedinga |
Women who make an informed decision not to breast-feed should be reassured that milk production will gradually diminish over the first few days after delivery. During this time, a properly fitted bra, ice packs, and oral analgesics should minimize the discomfort of breast engorgement. Medical therapies to hasten this process are no longer advised.
Other than encouraging breast-feeding women to follow a well-balanced, varied diet, and to keep adequately hydrated, no specific dietary modifications are necessary. It is reasonable to recommend a multivitamin with iron supplementation to all nursing women, especially strict vegetarians and those who do not eat dairy products.
Nursing women have a greater delay in resumption of intercourse, compared to those who bottle-feed. In some women, this is clearly attributable to discomfort due to relative vaginal atrophy and decreased lubrication from low estrogen levels. If lubrication during intercourse does not provide relief, women with a well-established milk supply may benefit from vaginal estrogen cream.
Not working, or working part-time, is associated with a longer period of breast-feeding. However, working is rarely the reason given by women for not breast-feeding. The barriers to breast-feeding while working include lack of a flexible or part-time work schedule, inadequate maternity leave and job security, lack of on-site day care, and lack of an appropriate place to pump or breast-feed. Often, the most significant problem facing a mother trying to work and breast-feed is the people around her who do not understand her choice to nurse. Increasingly, however, societal attitudes, and social policies and laws have become more favorable to, and supportive of, breast-feeding.
Nursing Problems
Evaluating problems with nursing requires the observation of the mother and baby while nursing, to which the office setting may not be conducive—and thus the advantage of lay assistance and lactation specialists. Adequate rest is important, and encouragement to rest should accompany almost all calls about problems with nursing.
Concerns about Insufficient Milk Supply
The most common reason women give for discontinuing breast-feeding is a concern over insufficient milk supply. Milk letdown can be inhibited by cold, pain, and emotional stress and is sometimes difficult to achieve using a breast pump. A quiet, private setting and pictures of the baby to look at may help. Thus simple supportive measures and environmental modification may be all that is required. If the problem proves refractory, oxytocin in nasal-spray form may be helpful. The spray contains 40 USP units (IU) per milliliter, which is administered into one or both nostrils 2 to 3 minutes prior to nursing or pumping.
Painful Nipples
Painful nipples are usually caused by problems with positioning and latching on. For some women, comfort will be gained by leaving their nipples exposed and using either a lamp or hair dryer to dry their nipples after feedings. Additionally, breast shields and purified lanolin cream may help provide relief.
Mastitis
One to two percent of breast-feeding women will develop mastitis, which can occur any time, but is most frequent in the first through fifth week of breast-feeding. Typical symptoms are unilateral breast pain, chills, and malaise. Signs include fever, and an erythematous, indurated segment of breast. Staphylococcus aureus is the most common agent, although a broad- spectrum of bacteria may be causative. In women not allergic or sensitive to penicillin, a 7- to 10-day course of oral dicloxacillin, 500 mg q.i.d., is usually curative. Oral hydration is advised and antipyretics may lessen discomfort and fever. For penicillin-intolerant women, erythromycin may be substituted. Breast-feeding should continue, as drainage of the breast has therapeutic value. Neglected or recurrent infections and infections with resistant organisms can lead to a breast abscess. Treatment of an abscess usually involves intravenous antibiotics and aspiration or surgical drainage.
NEWBORN CARE
Immediate Assessment and Resuscitation
The transition from fetus to newborn infant is the most dramatic physiologic change that occurs in the human life span. The fetus that received all of its oxygen and nutritional needs via the placenta must now use two entirely different, essentially dormant organ systems to meet these needs. The circulation is rerouted and the pulmonary bypass paths (ductus arteriosus, foramen ovale, and umbilical circulation) are no longer used. The lungs and left side of the heart that once handled about 15% of the circulation must now deal with 100% of the circulation in series with the right heart and remainder of the body. The fluid-filled, unexpanded lungs must be inflated and cleared of fluid to allow gas exchange, as they are now the sole source of oxygen for the infant.
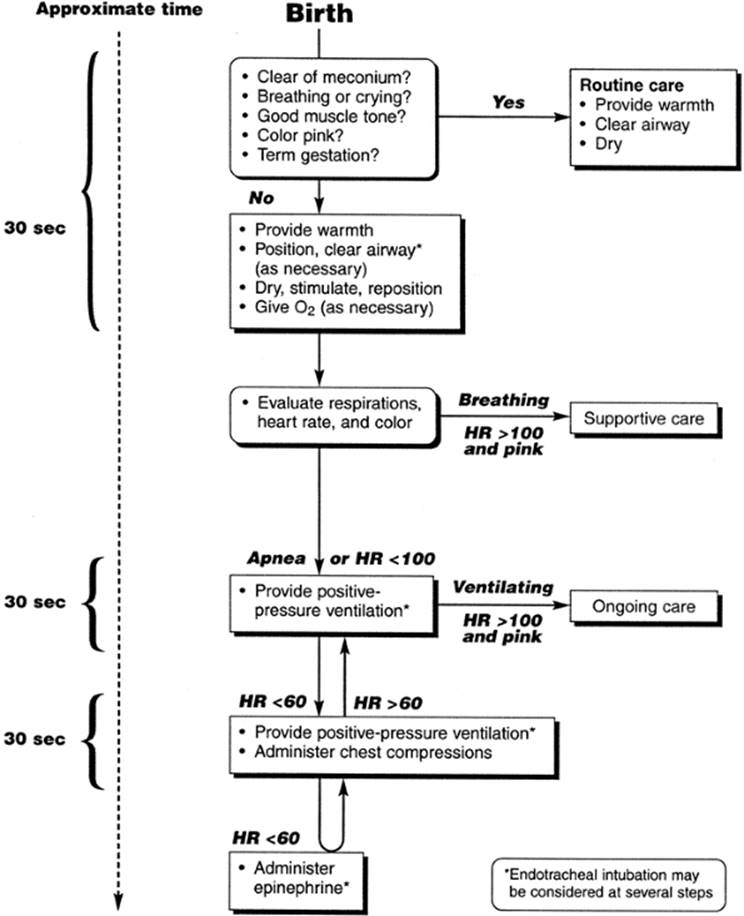
Resuscitation in the delivery room is geared toward helping the infant accomplish this transition. The AAP Neonatal Resuscitation Program (NRP) is a training course that all those specializing in pediatrics complete and is strongly encouraged for all individuals who deliver infants or attend deliveries; in fact, many institutions now require current certification for delivery room personnel. The resuscitation algorithm from the current NRP is shown in Figure 2.16.
|
|
|
FIG. 2.16. Algorithm for resuscitation of the newly born infant. (From American Academy of Pediatrics © 2000; with permission.) |
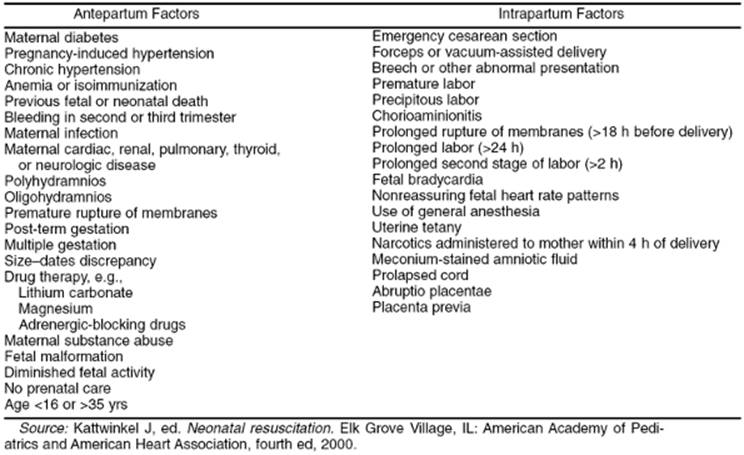
While every delivery should be attended by personnel trained in newborn resuscitation, the presence of personnel experienced in resuscitation is most desirable for deliveries where the need for resuscitation is more likely.
Examples of these situations are summarized in Table 2.7.
|
|
|
TABLE 2.7. Antepartum factors and intrapartum factors |
Meconium
Meconium passage prior to birth occurs in up to 20% of term deliveries and is a common reason for neonatal resuscitation. In the 1970s it was recognized that early suctioning by the obstetrician or pediatrician decreased the incidence of meconium aspiration syndrome (MAS). In the 1980s, routine suctioning of the oropharynx at the perineum or endotracheal suctioning were standard practice; however, it became clear that not all cases of MAS could be prevented and that aspiration in utero could occur. In the 1990s, many neonatologists were concerned that vigorous babies with thin meconium had a very low risk of MAS, and might actually do better if not intubated for tracheal suctioning. Unfortunately, the majority of studies pertinent to this issue have not been prospective, randomized, or controlled. The most recent Cochrane Library review concluded that until further evidence is available, endotracheal suctioning for meconium should be reserved for those infants who are depressed or have respiratory difficulties.
The Apgar Score
In 1952, Dr. Virginia Apgar devised a 0 to 10 scale scoring system intended to focus attention on the newborn and allow the systematic assessment of its condition and immediate needs (Table 2.8). Since that time, Apgar scores have become a mainstay in immediate newborn assessment. The Apgar score is a useful tool to guide those charged with assessment and care of the newborn. It provides an overall picture of infant status, and has been used in clinical research to correlate later outcomes with initial appearance. It cannot be used to predict neurologic outcome without other tests or examinations, nor is it a validated tool for determining asphyxia. Moreover, it was never intended for use in premature infants. Scores are assigned at 1 minute of age, and every 5 minutes thereafter until the score is over 7, or until 20 minutes of age. Clearly, resuscitation should begin if necessary prior to the 1-minute score.
|
|
|
TABLE 2.8. Apgar mnemonic |
General Evaluation and Treatment
Every newborn infant should have a thorough physical examination. The newborn exam is focused on identification of congenital abnormalities, birth trauma, and signs of transitional difficulties (Table 2.9). Although infants of 35 or more weeks and over 2 kg will generally be able to maintain their temperature and feed successfully, all infants born prior to 37 weeks may require more frequent monitoring of temperature and blood glucose. Infants who are large or small for their delivery dates are at higher risk for hypoglycemia. If dates are uncertain, a Dubowitz or Ballard examination may be performed, ideally between 24 to 48 hours of age. In addition to monitoring blood sugar prior to established feeding, routine laboratory work often includes blood type, Coombs test, and hematocrit. A positive Coombs test can be caused by Rh or ABO incompatibility. Hematocrit levels between 40% to 65% are acceptable. Most states screen for phenylketonuria (PKU) and congenital hypothyroidism. Other tests used by some states include screens for congenital adrenal hyperplasia, cystic fibrosis, and other inborn errors of metabolism. These tests may be initiated prior to discharge according to state mandates. Infants born in U.S. hospitals are given either dilute silver nitrate drops or erythromycin ophthalmic ointment to prevent Neisseria gonorrhoeae conjunctivitis, which was once the most common cause of congenital blindness. Vitamin K is administered intramuscularly to prevent vitamin K deficiency bleeding (VKDB). Factors that can contribute to this deficiency include low vitamin K stores at birth, poor placental transfer of vitamin K, low levels of vitamin K in breast milk, and sterility of the gut. Because standard commercial infant formulas contain supplemental vitamin K, VKDB is almost exclusively a problem of breast-fed infants. The most common sites of bleeding are the umbilicus, mucous membranes, gastrointestinal tract, the penis after circumcision, and skin (from venipuncture). Intracranial bleeding can occur and is the main cause of mortality and long-term morbidity. In the United States, all infants are actively immunized against hepatitis B, the initial dose of which is generally given on the day of birth. If the mother is positive for hepatitis B surface antigen or if her status cannot be determined within a few days, the infant should also receive passive immunization within 7 days in the form of hepatitis B immune globulin.
|
|
|
TABLE 2.9. Examination of the newborn |
Early Onset Sepsis
One of the most serious problems encountered in the immediate newborn period is early onset sepsis, defined as occurring in the first 5 days after birth. The current estimated rate in the United States is 1 to 2 per 1000 live births. Group B streptococci (GBS) remain the most common causal organisms, but with the routine use of intrapartum antibiotic prophylaxis for GBS, Escherichia coli now constitutes a larger proportion of causative organisms. The symptoms of neonatal sepsis include respiratory distress, lethargy, poor feeding, hypotonia, seizures, and shock. The management of infants with symptoms of sepsis includes blood and, if indicated, cerebrospinal fluid cultures, followed by the administration of broad-spectrum intravenous antibiotics, generally a penicillin in combination with an aminoglycoside. The management of asymptomatic infants of mothers with risk factors for neonatal sepsis is less clear and has become a topic of considerable debate since the routine use of intrapartum GBS chemoprophylaxis. Based on expert opinion and limited data the following general approach has been recommended. Because of an increased risk for early-onset GBS septicemia and greater difficulty in assessing symptoms, asymptomatic infants born prior to 35 weeks gestation should be evaluated with a complete blood count and blood culture, and observed in the hospital without empirical antimicrobial therapy for at least 48 hours. In infants born at and beyond 35 weeks, clinical assessment is more dependable. Routine laboratory evaluation is not recommended in these infants. They should, however, be observed in-hospital for at least 48 hours.
Hyperbilirubinemia and Discharge Planning
Timing of newborn discharge has been a topic of controversy for nearly 20 years. Prior to and during much of this time, the traditional stay was 3 days for a vaginally delivered baby and 5 days for those delivered by cesarean (due to the mother's extended stay). This minimum of 3 days allowed detection of the most common serious problems of the newborn, such as ductal-dependant congenital heart disease, early onset sepsis, hyperbilirubinemia, and failure to establish adequate breast-feeding. Discharges at 24 hours (or less) became popular in the late 1980s, a practice driven largely by third-party payors. While numerous small studies were performed to assess the safety of early discharge, most suffered from insufficient numbers to rule out an increase in adverse outcomes that, individually, are relatively uncommon. Bilirubin encephalopathy, a disorder rarely seen for the past 30 to 40 years, has recently been reported to be on the rise. Bilirubin peaks at 5 days in formula-fed infants but may peak as late as 7 to 10 days in breast-fed infants. Breast milk production is minimal in the first 48 hours after delivery and does not reach 80% of full volume until 4 days postpartum. Because of this time frame, it is not easy to predict at 3 days of age which breast-fed infants with a negative Coombs test will be at risk of dangerously high bilirubin levels (>25 mg/dL), and it is nearly impossible to do so at less than 48 hours. In recognition of these issues, the pendulum appears to be swinging back to a 3-day stay for most breast-fed infants. Infants readmitted after discharge prior to 48 hours are most likely breast-fed and jaundice is the most common reason for admission. In addition to insufficient breast milk intake, hyperbilirubinemia can result from relative polycythemia, bruising, cephalohematoma, or be idiopathic. The current AAP guidelines for management of term infants with nonhemolytic jaundice are given in Table 2.10.
|
|
|
TABLE 2.10. American Academy of Pediatrics hyperbilirubinemia treatment guidelines: total serum bilirubin (mg/dL) |
SUMMARY POINTS
· Labor is defined as regular uterine contractions that lead to effacement and dilation of the cervix.
· Labor can be conceptualized as depending on the Power, the Passage, and the Passenger.
· A variety of management approaches to labor have been employed and evaluated, and no single approach is clearly superior.
· Both infection and hemorrhage can complicate normal labor and delivery, and caregivers must be vigilant for these complications and competent in their management.
· Encouraging and providing support for breast-feeding has significant benefits for both infants and mothers.
· Every delivery should be attended by personnel trained in newborn resuscitation.
· Newborn hospital stays shorter than 3 days may compromise the detection of hyperbilirubinemia in breast-fed infants.
SUGGESTED READINGS
American Academy of Pediatrics Provisional Committee for Quality Improvement Hyperbilirubinemia Subcommittee. Practice parameter: management of hyperbilirubinemia in the healthy term newborn. Pediatrics 1994;94:558–565.
American College of Obstetricians and Gynecologists. Breastfeeding: maternal and infant aspects. ACOG Educational Bulletin No. 258, July 2000.
American College of Obstetricians and Gynecologists. Prevention of early-onset Group B streptococcal disease in newborns. ACOG Committee Opinion #279, December 2002.
Carroli G, Belizan J. Episiotomy for vaginal birth. Cochrane Database of Systematic Reviews 2001;issue 3.
Chua S, Arulkumaran S. Poor prognosis in labor, including augmentation, malpositions and malpresentations. In: James DK, Steer PJ, Weiner CP, Gonik B, eds. High risk pregnancy, second ed. London: Harcourt Brace, 1999:1105.
Fraser WD, Turcot L, Krauss I, Brisson-Carrol G. Amniotomy for shortening spontaneous labour. Cochrane Database of Systematic Reviews 2001;issue 2.
Fraser WD, Marcoux S, Krauss I, et al. Multicenter, randomized, controlled trial of delayed pushing for nulliparous women in the second stage of labor with continuous epidural analgesia. Am J Obstet Gynecol 2000;182:1165–1172.
Halliday HL. Endotracheal intubation at birth for preventing morbidity and mortality in vigorous, meconium-stained infants born at term. Cochrane Database of Systematic Reviews 2002;issue 1.
Hannah ME, Ohlsson A, Farine D, et al. Induction of labor compared with expectant management for prelabor rupture of the membranes at term. N Engl J Med 1996;334:1005–1010.
Hodnett ED. Caregiver support for women during childbirth. Cochrane Database of Systematic Reviews 2001;issue 2.
Hofmeyr GJ. Amnioinfusion for meconium-stained liquor in labour. Cochrane Database of Systematic Reviews 2001;issue 2.
Kattwinkel J, ed. Neonatal resuscitation, fourth ed. Elk Grove Village, IL: American Academy of Pediatrics and American Heart Association, 2000.
Prendiville WJ, Elbourne D, McDonald S. Active versus expectant management in the third stage of labour. Cochrane Database of Systematic Reviews2001;issue 2.
Radmacher P, Massey C, Adamkin D. Hidden morbidity with “successful” early discharge. J Perinatol 2002;22:15–20.
World Health Organization Maternal Health and Safe Motherhood Programme. World Health Organization partograph in management of labour. Lancet1994;343:1399–1404.