Joy L. Hawkins
The purpose of this chapter is to acquaint the obstetrician with the various techniques of obstetric analgesia (pain relief) and anesthesia (for surgical procedures) and to describe their indications, advantages, disadvantages, and complications. The technical aspects, including the methods of administration, will not be described in detail. Readers seeking specific information on how to perform the various obstetric anesthetic techniques are referred to one of the basic obstetric anesthesia textbooks (1).
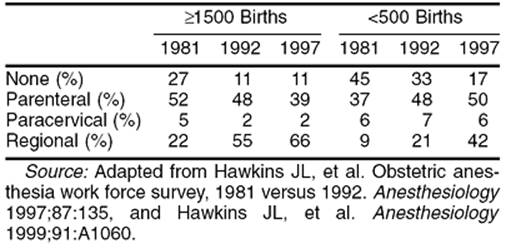
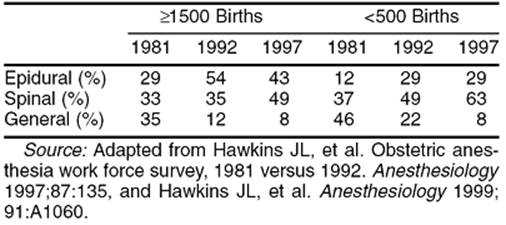
Obstetric analgesia or anesthesia refers to the multiple techniques useful for the alleviation of the pain associated with labor, delivery, or surgery. The choice of an appropriate analgesic technique must be made by the patient, the obstetrician, and the anesthesiologist and should take into consideration the patient's anatomy and physiology, the status of her fetus, the obstetric plan for delivery, and the pharmacology of the drugs to be employed (2). Most women now request some form of analgesia during childbirth (Table 3.1).
|
|
|
TABLE 3.1. Types of labor analgesia provided by size of hospital in three time periods |
PAIN OF PARTURITION
Increasing dilation of the cervix, contraction and distention of the uterus, and distention or tearing of the vagina, vulva, and perineum causes the pain that occurs during labor and delivery. Pain may be generated through stretching or application of pressure to adjacent pelvic organs.
The pain that occurs in the first stage of labor increases in severity as the cervix becomes more dilated. The onset of pain lags approximately 15 to 30 seconds behind the onset of the uterine contraction and is first perceived when the intraamniotic pressure reaches 15 mm Hg above that of resting tonus. In the second stage of labor, sharp pain occurs as the tissues of the vagina and perineum are stretched. Stretching stimulates the second, third, and fourth sacral nerve roots, which carry nociceptive information to the spinal cord through the sensory fibers of the pudendal nerve. Adnexal pressure and traction on the bladder, urethra, rectum, and peritoneum also contribute to the pain of parturition. Compression of the lumbosacral plexus by the fetal head, particularly in the occiput posterior position, may cause pain even before the onset of labor.
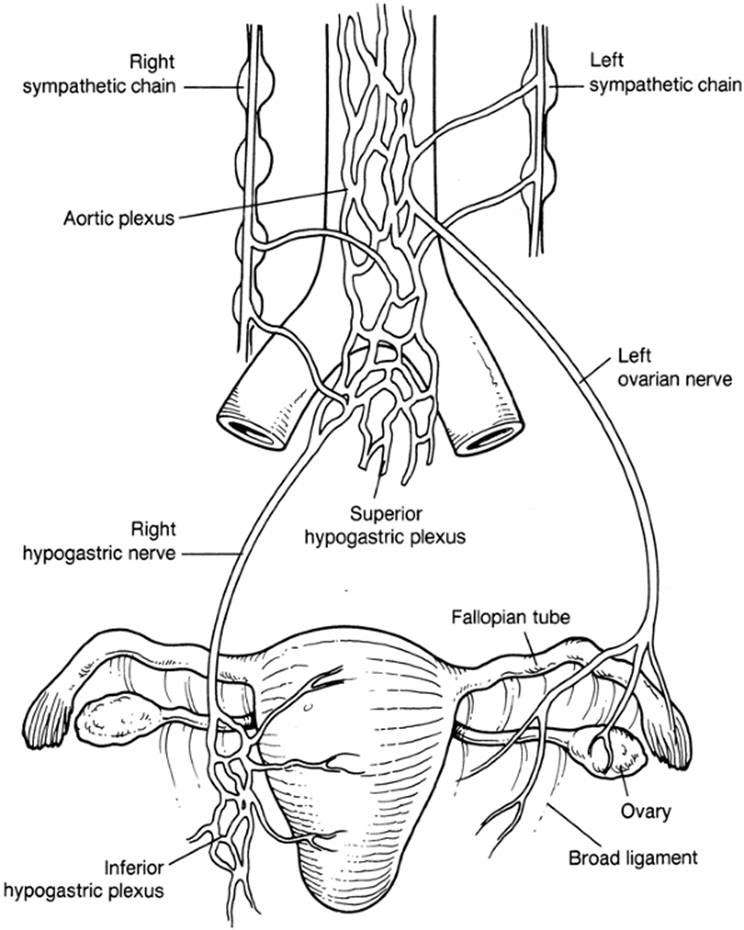
The pain of uterine contractions is conducted through small sensory nerve fibers of the paracervical and inferior hypogastric plexuses to join the sympathetic nerve chain at L2-3. The ascending fibers enter the spinal cord through the nerve roots of T-10 to T-12, with a variable contribution from L-1 (Fig. 3.1). Because the cutaneous branches of the lower thoracic and upper lumbar nerves migrate caudally for a considerable distance before they innervate the skin, the pain of uterine contractions is often referred to the area over the upper sacrum and the lower lumbar spine.
|
|
|
FIG. 3.1. Sympathetic nerve supply of the uterus from the pelvic and abdominal distribution. The uterine nerves arise from the upper part of the uterus (i.e., upper uterine segment), the contraction of which contributes to pain; from the lower part of the uterus (i.e., lower uterine segment), the distention of which contributes to pain; and from the cervix, the dilation of which contributes to pain. The ovarian nerve supplies the ovary, fallopian tube, broad ligament, round ligament, and the side of the uterus, and it communicates with the uterine plexus. The sympathetic efferent and afferent fibers are shown together. (Adapted from Abouleish E. Pain control in obstetrics. Philadelphia: JB Lippincott Co, 1977.) |
Pain from the uterus and cervix is transmitted through the small-diameter myelinated δ-A fibers and unmyelinated C fibers. Because there are relatively fewer nociceptive afferent nerves from visceral structures than from somatic structures, visceral pain is perceived as being diffuse and difficult to localize. These visceral afferents also synapse on and excite the same dorsal horn neurons as afferents from somatic structures. This arrangement is responsible for the phenomenon of referred pain.
The gate theory of Melzack and Wall holds that stimulation of the large cutaneous β-A nerve fibers closes a “gate” in the substantia gelatinosa of the spinal cord, preventing pain impulses from being carried rostrally by the δ-A and C nerve fibers. This theory forms the basis for the use of acupuncture, transcutaneous electrical nerve stimulation, and intracutaneous nerve stimulation with sterile water injections for the relief of pain associated with parturition.
Pregnancy appears to reduce anesthetic requirements. It has been postulated that high progesterone levels lead to increased quantities of endogenous endorphins, which may increase the maternal threshold to pain. One study correlated pain intensity during labor and plasma levels of β-endorphin. The lowest endorphin levels were found after abolition of labor pain by epidural analgesia. The highest concentrations were observed in the first few minutes after delivery, immediately after cessation of the severe pain of expulsive labor.
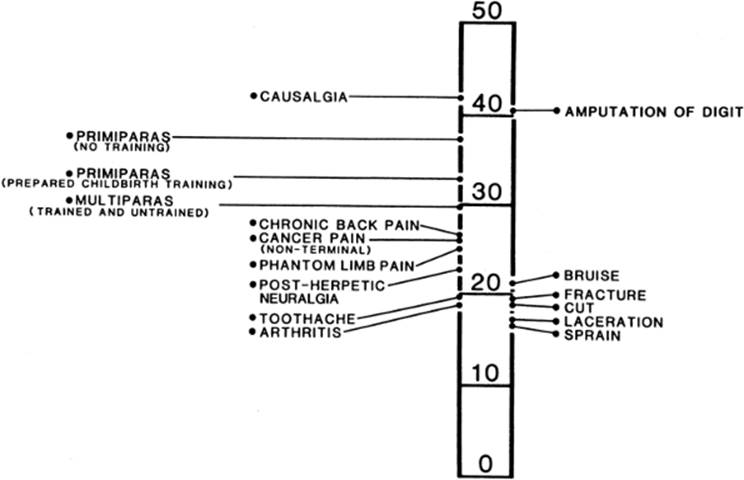
The nature of the pain of labor varies in intensity with the stages of labor. The intensity of pain is related to physical factors such as the strength and duration of uterine contractions, the rapidity of cervical dilation, the degree of distention of the vaginal and perineal tissues, the requirement for operative delivery, and the size, presentation, and position of the infant. Augmentation of labor with oxytocin increases the strength and pain of uterine contractions. The primiparous woman may perceive greater pain than the multipara who enters labor with more advanced cervical dilation and who may also be more psychologically prepared (Fig. 3.2). Exhaustion, psychological factors, and protracted nausea and vomiting may also increase the parturient's perception of labor pain.
|
|
|
FIG. 3.2. Comparison of pain scores obtained from women during labor and from patients in a general hospital pain clinic or emergency department using the McGill pain questionnaire. (From Melzack R. The myth of painless childbirth. Pain 1984;19:321–37.) |
Pain management is an important part of modern obstetric care. The obstetrician should appreciate the importance of providing pain relief during labor through the use of nonpharmacologic techniques, systemic analgesics, or regional block analgesia. During the second stage of labor, additional analgesia may also be needed through perineal extension of a segmental epidural or through the use of pudendal or spinal blocks.
SYSTEMIC ANALGESIA AND SEDATION
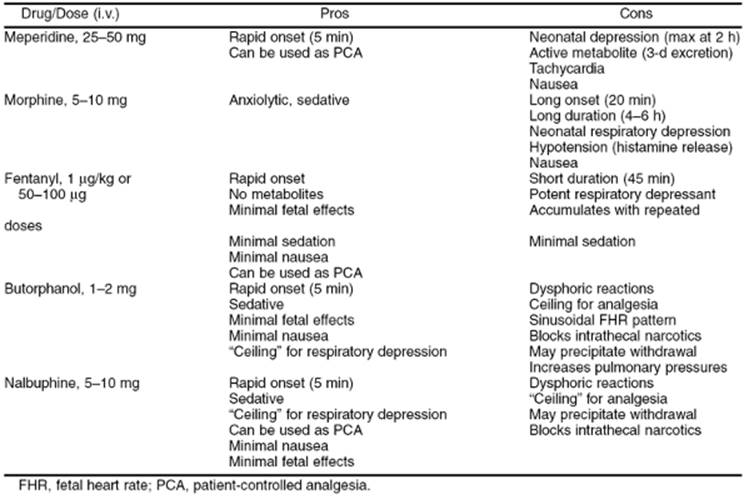
In the management of labor pain, systemic narcotics are usually considered to be the first step beyond the less invasive or “natural” methods such as massage, water baths, and birth attendants (doulas). They may also be necessary for patients who are not candidates for regional analgesia. Research indicates the analgesic effects of parenteral agents used in labor is limited and the primary mechanism of action is heavy sedation (3). Although narcotics may be effective for some patients in relieving the pain of labor, their side effects prohibit the use of large doses. The physician must balance maternal and neonatal respiratory depression with effective relief of the pain of labor. Because the pain of labor occurs intermittently with contractions, maternal hyperventilation during a contraction leads to hypoventilation for the 2 to 3 minutes between contractions, especially when narcotics have depressed the carbon dioxide response curve. There are advantages and disadvantages of all available narcotics, and a drug should be chosen with knowledge of its side effects and pharmacokinetics (Table 3.2).
|
|
|
TABLE 3.2. Parenteral medications for labor analgesia |
Use of Systemic Medications
Because the use of systemic narcotics and tranquilizers does not require special training or the availability of anesthesia personnel, they are used extensively in the United States to provide labor analgesia (see Table 3.1). These compounds do not induce fetal heart rate (FHR) abnormalities other than changes in variability and rarely sinusoidal heart rate patterns, nor do they cause fetal acidosis. The drug-related adverse maternal effects of narcotics can include nausea, vomiting, pruritus, sedation, decreased gastric motility, loss of protective airway reflexes, and hypoxia due to respiratory depression. The adverse neonatal effects of these agents include central nervous system (CNS) depression, respiratory depression, impaired early breast-feeding, altered neuroadaptive behavior, and decreased ability to regulate body temperature. To minimize these side effects, the lowest effective dosage should be employed, and the timing with respect to delivery must be carefully considered. Resuscitation equipment should be kept at hand, and naloxone, used to antagonize opioids, should be readily available. Benzodiazepine effects may be reversed with flumazenil (Romazicon).
Systemic Narcotics
Meperidine
Meperidine (Demerol) has achieved wide popularity for systemic analgesia during labor. It is preferred over morphine because it produces less emesis and does not depress the newborn carbon dioxide response curve as much as morphine. It can be administered intravenously or intramuscularly during labor. Current usage most often consists of small, incremental intravenous doses of 25 to 50 mg. Small doses can also be used to treat shivering. Placental transfer of meperidine occurs rapidly. Maximal depression of the infant occurs when delivery takes place 2 to 4 hours after maternal intravenous or intramuscular administration. Delivery of the infant within 1 hour of administration produces little evidence of newborn depression. A study using meperidine for labor analgesia by a patient-controlled infusion device found 5% of infants required naloxone at delivery (4).
Meperidine has as its principal metabolite the compound normeperidine, which is equipotent with meperidine in its ability to produce respiratory depression and can also cause seizures. Repeated intravenous administration of small doses of meperidine leads to increasing maternal and fetal levels of normeperidine. Meperidine has an elimination half-life in neonatal blood of 22.7 hours, and that of normeperidine is measured in days, reflected in abnormal neurobehavioral scores for up to 3 days.
Morphine
Morphine is pharmacologically more potent than meperidine by a factor of approximately 10. Morphine depresses the newborn carbon dioxide response curve more than meperidine, perhaps due to greater permeability of the infant brain to morphine. Because of this reputation, morphine has virtually disappeared from the armamentarium of analgesic drugs used by the obstetrician for the management of labor.
Fentanyl
Fentanyl (Sublimaze) is a potent synthetic narcotic with analgesic activity approximately 100 times that of morphine. Its onset of action is rapid, and its duration of activity is short (i.e., 20–30 minutes) because of its rapid distribution from plasma. The terminal drug elimination half-life after a single small dose is 1 to 2 hours. Fentanyl is highly bound to protein, which may limit its placental transfer. It has no active metabolites. Fetal–maternal blood concentration ratios average 0.31 over the first 10 minutes after intravenous administration. Fentanyl produces moderate analgesia and mild sedation. There may be a brief period of decreased FHR variability, but no other disturbing FHR patterns have been reported. Comparative studies with meperidine indicate that the need for newborn naloxone (Narcan) administration is greater after use of meperidine than after administration of fentanyl.
Nalbuphine
Nalbuphine (Nubain) is a potent narcotic agonist–antagonist agent which, at equianalgesic doses, produces respiratory depression equivalent to that of morphine. The advantage and disadvantage of nalbuphine is that as the dosage is increased, a ceiling effect is seen for respiratory depression, and unfortunately also for analgesia. Maximal respiratory depression occurs with a dose of 30 mg in a 70-kg adult. Sedation and dysphoric reactions may also occur. Reversal of other opioid effects may precipitate withdrawal in a susceptible patient. A possible transient depressive effect of nalbuphine on the fetal CNS has been identified.
Butorphanol
Butorphanol (Stadol) is another synthetic narcotic with agonist–antagonist properties. It is five times more potent than morphine and 40 times more potent than meperidine. It has achieved moderate popularity in the United States in the management of the pain of the first stage of labor. It is usually administered intravenously in doses of 1 to 2 mg. Butorphanol exhibits the same ceiling effect for analgesia and respiratory depression as nalbuphine. Maternal side effects may include sedation, dysphoric reactions, and reversal of other opioid effects.
Newer Opioids
Sufentanil and remifentanil, the newer synthetic opioids, have not been studied extensively for systemic analgesia during labor.
Patient-controlled Intravenous Analgesia
Intravenous patient-controlled analgesia (PCA) is widely available and provides pain relief through self-administration of intravenous opioids. Fentanyl, remifentanil, and meperidine are the analgesics most commonly employed with this technique. The infusion pump is programmed so that the patient receives an incremental dose when she pushes the button, followed by a lockout interval when additional requests by the patient will not be administered. An hourly maximum may also be programmed. A basal infusion is rarely used in labor because of the risk of respiratory depression between contractions. The actual settings are dictated by the pharmacokinetics of the narcotic chosen. The main advantage of PCA is improved patient satisfaction due to a feeling of control and not having to wait for a nurse to bring pain medication. Use of PCA may also decrease nursing staffing requirements.
In a study by Rosenblatt and colleagues (5), metoclopramide (Reglan) was used as an analgesic adjunct to PCA for patients undergoing prostaglandin induction of labor for second-trimester termination of pregnancy. Patients were given intravenous metoclopramide, 10 mg, or saline placebo followed by PCA-administered morphine. Those receiving metoclopramide used 54% less morphine and had lower pain scores.
Narcotic Antagonists
Naloxone
Because all narcotics cross the placenta and can produce respiratory depression in the neonate, availability of an effective antagonist is essential. Naloxone reverses opioid-induced respiratory depression without producing side effects of its own. Because it also reverses analgesia, its prophylactic use is not advised. Naloxone may be administered to the parturient as an intravenous bolus of 0.1 to 0.4 mg to treat maternal respiratory depression. Care must be taken to titrate naloxone to the desired effect, since large doses have been implicated in the causation of myocardial infarction, pulmonary edema, and severe hypertension. Naloxone, 0.01 mg per kg, may also be administered intravenously, intramuscularly, or through the endotracheal tube to the newborn to reverse the respiratory depressant effects of placentally transferred narcotics. The effect is usually apparent within a few minutes and persists for as long as 2 hours. The neonate must be carefully observed for evidence of renarcotization, because the half-life of naloxone is less than that of most narcotics.
Sedative Drugs
Benzodiazepines
The principal benzodiazepine drugs are diazepam (Valium) and midazolam (Versed). Diazepam has been used extensively in other parts of the world for seizure prophylaxis in patients with severe preeclampsia. However, because of its side effects on the newborn, it has found little favor in the United States. Newborns exposed to diazepam characteristically exhibit hypotonicity, hypoactivity, and impaired temperature regulation and metabolic response to cold stress.
Midazolam is a newer benzodiazepine anxiolytic, a sedative drug with significant amnestic properties. It is five times more potent than diazepam and is soluble in water, a property that reduces pain associated with intravenous administration. Midazolam crosses the sheep placenta, achieving a fetal–maternal concentration ratio of 0.15. Its metabolites are inactive, and the drug is excreted more rapidly than diazepam. Midazolam has been used as an induction agent for cesarean delivery, but because of its ability to cross the placenta, it has produced neonatal respiratory depression and decreased body tone and temperature. Midazolam has not been recommended for use as a tranquilizer-sedative in labor, because its amnestic properties are unacceptable to most parturients.
Barbiturates
Barbiturates may be used in the latent phase of labor. Although they cause maternal sedation and decreased anxiety, barbiturates lack analgesic properties and may increase the perception of pain when given without concomitant administration of a narcotic. Most barbiturates have long elimination half-lives and readily cross the placenta. Prolonged neonatal effects have led to the virtual elimination of these drugs from use during labor.
Other Sedatives
Phenothiazine derivatives, such as promethazine (Phenergan), have been used in obstetrics and provide sedation and decrease nausea. Hydroxyzine, although not a phenothiazine, has similar properties when used in combination with narcotics. Maternal sedation is achieved without significant maternal or newborn side effects. It is important to remember that none of these drugs provide analgesia, and some parturients may object to the heavy sedation they cause. In addition, both medications are very painful intramuscular injections. They should have little place in the management of labor analgesia.
Ketamine (Ketalar), when administered intermittently at low doses (10–15 mg), can produce analgesia in parturients without causing maternal loss of consciousness or neonatal respiratory depression. An improvement on this technique using low-dose ketamine infusion has been described by Maroof and associates (6). In this study, patients were given an intravenous bolus of ketamine, 0.5 mg per kg, upon achieving 4 cm of cervical dilation. This was followed by an infusion of ketamine at 0.25 mg per kg per hour. Patients served as their own controls, evaluating labor with and without the benefit of ketamine. Pain scores were significantly better with ketamine. The authors concluded that ketamine infusion produced acceptable analgesia throughout labor and was not associated with delirium or loss of consciousness in any patient. In addition, neonatal respiratory depression was not noted. The profound amnesia and potential for dysphoria or other psychomimetic effects when using ketamine limit its general use for labor analgesia. It is most useful for short painful procedures such as urgent forceps delivery or manual removal of the placenta.
Inhalational Agents
Nitrous oxide can be inhaled periodically with contractions in a 50% mixture with oxygen. During a painful contraction, the mother breathes from a mask connected to the regulator valve of a breathing circuit. A scavenging system is required by the Occupational Safety and Health Administration (OSHA) to eliminate exhaled waste anesthetic gases. Unfortunately, when it is breathed at the onset of a contraction, maximal analgesia is achieved only after the contraction has ended. When nitrous oxide is used in conjunction with narcotics, maternal oxygen saturation may decrease. Use of a pulse oximeter to ensure adequate maternal oxygenation is recommended. In practical terms, since almost all deliveries in the United States now take place outside the operating room, an anesthesia machine will probably not be available to safely administer inhalational agents.
REGIONAL ANALGESIA
Local Anesthetic Agents
Most local anesthetic agents share a common structure consisting of a hydrophilic amino group connected by an intermediate chain to a lipophilic aromatic residue. Their presumed mechanism of action is to block exchange of sodium and potassium ions across the cell membrane, probably through mechanical interruption of ion flow through cell wall channels.
Local anesthetic drugs are manufactured as chloride salts. The nonionized base is able to diffuse across tissues, while the ionized form is actually the active component. The amounts of nonionized (mobile) and ionized (active) drug depend on the pKa of the local anesthetic and tissue pH.
After injection of lidocaine (Xylocaine), the sensory nerve action potential decreases more sharply in pregnant women than in nonpregnant women. This implies that pregnant women have an increased susceptibility to the effects of local anesthetic agents (7).
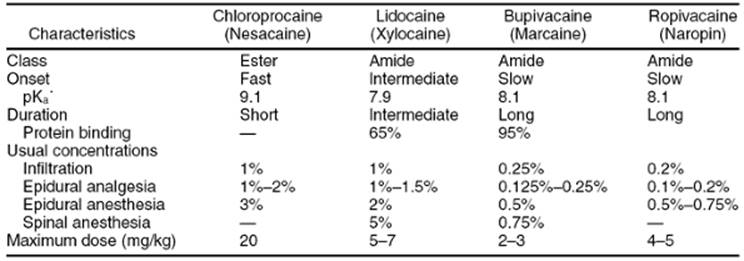
Local anesthetics belong principally to two groups, those of ester and amide configurations. Ester drugs are generally characterized by their rapid onset of action, short duration, and low toxicity. Chloroprocaine (Nesacaine) is a representative of this group. It is rapidly metabolized by serum pseudocholinesterase, forming paraaminobenzoic acid. Lidocaine, bupivacaine, ropivacaine, and levobupivacaine are representatives of the amide group. These drugs are more highly bound to protein and have a slower onset and a longer duration of action. They are metabolized in the liver. Toxicity is usually greater for amides than for drugs of the ester group (Table 3.3).
|
|
|
TABLE 3.3. Characteristics of local anesthetics commonly used in obstetric anesthesia |
Local anesthetic drugs are absorbed systemically. Distribution to the fetus depends on maternal tissue uptake, maternal blood concentration, uterine blood flow, and maternal and fetal metabolism and excretion. Fetal-tissue drug distribution is also affected by asphyxia. Fetal asphyxia leads to increased PaCO2, which results in cerebral and coronary vessel dilation and increased brain and myocardial blood flow. The increased perfusion of these organs with anesthetic drug leads to greater toxicity. The decrease in pH seen with fetal asphyxia results in increased ionized (active) drug in the fetal circulation and tissues, a phenomenon referred to as ion trapping. The clinical significance of this is unclear.
Side Effects of Local Anesthetic Drugs
Systemic Toxicity
Systemic complications involving the use of local anesthetics include toxic blood levels of the drug and allergic reactions, as well as reactions due to epinephrine that is often added to local anesthetic solutions to retard systemic absorption and prolong duration of action.
Maximal safe doses for healthy young adults are 7 mg per kg (300 mg) of lidocaine, 2 to 3 mg per kg (175 mg) of bupivacaine, and 20 mg per kg (1000 mg) of chloroprocaine (see Table 3.3).
The most common reason for high blood levels of local anesthetic drugs is accidental intravascular injection. This most commonly occurs when an epidural catheter has been placed or migrated into a vein. To minimize accidental intravenous injection, gentle aspiration should be undertaken before each injection. Injection should be done slowly and incrementally with only 2 to 5 mL of local anesthetic drug to reduce the chance of a sudden increase in plasma levels. A marker such as epinephrine may be added to the local anesthetic solution so that intravascular injection will manifest as tachycardia.
The infiltration of a local anesthetic agent into an area rich in vessels, such as the region of the uterine artery (e.g., paracervical block), pudendal vessels, or the epidural space may be associated with absorption of the drug through blood vessel walls. The serum levels tend to rise slowly, and toxic manifestations usually occur only after multiple injections.
Repeated injections of slowly metabolized local anesthetic drugs, such as the amides, may lead to accumulation in the serum such that toxic levels are achieved. This phenomenon does not occur readily with esters such as chloroprocaine, which are rapidly metabolized (maternal serum half-life of 21 seconds and fetal serum half-life of 43 seconds for chloroprocaine). To minimize the likelihood of producing high serum levels, care should be taken to record the amount and concentration of local anesthetic solution and to limit use to approximately 25% less than the maximal safe dose.
Signs and symptoms of local anesthetic drug toxicity include, in order of their appearance, a relaxed feeling, drowsiness, lightheadedness, tinnitus, circumoral paresthesias, metallic taste, slurred speech, blurred vision, unconsciousness, convulsions, and cardiac dysrhythmias and arrest. In 1983, the U.S. Food and Drug Administration issued an advisory, warning that 0.75% bupivacaine should no longer be used in obstetrics because of reports of bupivacaine-induced cardiac arrest occurring at blood levels of only 3 to 5 µg per mL. The advisory stated that the resuscitation in these cases had been “difficult or impossible despite apparently adequate preparation and appropriate management.” Inadvertent intravascular injection causes high serum levels, which produce cardiac arrest through blockade of the cardiac sodium channels, inhibiting repolarization of the nerve cell membranes of the conduction system of the heart. Bupivacaine has been found to bind avidly to nonspecific cardiac protein–binding sites, slowing the conduction of impulses arising in pacemaker cells and causing a dose-dependent reduction in the strength of myocardial contractility, leading to cardiac arrest.
Management is best accomplished through prevention, as described previously. Therapy is symptomatic. Initial treatment includes the use of mask oxygen, a reliable intravenous line, and measures to ensure and protect the airway. These include use of cricoid pressure to occlude the esophagus, the availability of adequate suction, and the capability to perform endotracheal intubation, if needed.
Adequacy of respirations must be ensured, if necessary by means of positive pressure ventilation with 100% inspired oxygen. The patient should be hyperventilated to help correct metabolic acidosis caused by seizure activity and decreased cardiac output. CNS hyperreactivity and convulsions are treated with thiopental (Pentothal) in small, incremental doses of 25 to 50 mg given intravenously, or with 1 to 5 mg of midazolam given intravenously. In the event of cardiovascular depression, elevate the lower extremities and verify left uterine displacement. Vasoactive drugs such as ephedrine, phenylephrine, epinephrine, and calcium may be employed to support the circulation. If cardiopulmonary resuscitation is indicated, the fetus should be delivered within 5 minutes to relieve maternal central venous compression and advanced cardiac life support (ACLS) protocols should be followed.
Use of Regional Anesthetic Blocks
Local Infiltration of the Perineum
Local infiltration of the perineum is commonly performed when an episiotomy is needed and time or fetal head position does not allow a pudendal block to be administered. An average of 10 to 20 mL of local anesthetic solution is employed. The preferred drugs are lidocaine 1% or chloroprocaine 2%.
Pudendal Block
The pudendal block provides analgesia of the vaginal introitus and perineum. There are several advantages of this analgesic technique. Because the elapsed time between administration and delivery is short, there is relatively little systemic absorption and therefore little opportunity for the drug to directly affect the fetus. The block is easy to accomplish and provides analgesia of the perineum only. The disadvantages include the need for large drug doses (i.e., 10 mL on each side) and the potential for local anesthetic toxicity, hematoma, and the possibility of infection leading to retropsoas or subgluteal abscess.
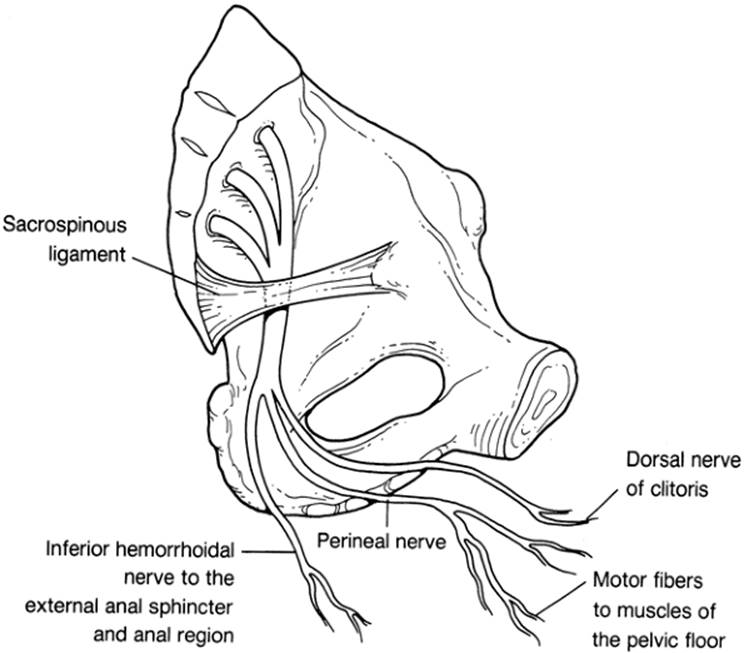
With the transvaginal approach, the ischial spine must first be identified. Through a guide, a needle is inserted into the vagina and directed laterally and posteriorly to the ischial spine. A submucosal wheal is made, and the needle is advanced into the sacrospinous ligament, where resistance is felt. As the needle passes the ligament, a loss of resistance is felt. The needle has now entered the pudendal canal, which contains the pudendal nerve and associated vessels (Fig. 3.3). After aspirating the needle for blood, 3 to 5 mL of local anesthetic solution (usually lidocaine 1%) is injected, and the needle is advanced another 0.5 to 1 cm. If aspiration is again negative, 5 to 7 mL of solution is injected. A total of 10 mL is injected on each side. Approximately 10 minutes are required for anesthesia to occur. Chloroprocaine 1% to 2% may also be used for this block. Analgesia with chloroprocaine lasts less than 1 hour, but lidocaine analgesia is more prolonged.
|
|
|
FIG. 3.3. The pudendal nerve and its branches. The inferior hemorrhoidal nerve can arise higher up from the pudendal nerve or separately from the sacral plexus. (Adapted from Abouleish E. Pain control in obstetrics. Philadelphia: JB Lippincott Co, 1977.) |
Paracervical Block
Paracervical block (PCB) anesthesia may be used when the active phase of labor begins, and it can be employed until approximately 8 cm of dilation has been achieved. Although formerly popular, this block has fallen into relative disuse since the description of bradycardia after PCB and its proven association with fetal acidosis. The PCB is useful when anesthesia personnel are unavailable and parenteral narcotics are inadequate.
The PCB relieves the pain associated with uterine contractions, but it is not effective for pain associated with distention of the pelvic floor. The two drugs of choice are chloroprocaine and lidocaine in 1% concentrations. Typically, 6 mL of drug is administered superficially, just under the vaginal mucosa, at the 4- and 8-o'clock positions (Fig. 3.4). In this way, bradycardia, which occurs in 10% to 30% of cases, is less likely to appear. The landmark study by Baxi and colleagues (8), using a transcutaneous oxygen electrode attached to the fetal scalp, demonstrated that bradycardia is related to decreasing fetal oxygenation, which becomes marginal approximately 10 minutes after injection. This research has been corroborated by the study of isolated human uterine artery segments and by work in animals, indicating that direct uterine artery vasoconstriction and uterine hypertonus in response to the injection of a local anesthetic drug diminish uterine blood flow and fetal oxygenation.
|
|
|
FIG. 3.4. Technique of paracervical block. Notice the position of the hand and fingers in relation to the cervix and fetal head and the shallow depth of the needle insertion. No undue pressure is applied at the vaginal fornix by the fingers or needle guide. (Adapted from Abouleish E. Pain control in obstetrics.Philadelphia: JB Lippincott Co, 1977.) |
Lumbar Epidural Analgesia
Standard Technique
Lumbar epidural analgesia was first performed in 1884 by Corning, who recognized that analgesia could still occur when attempted spinal analgesia failed. In 1921, Pages applied the technique to surgery. Obstetric applications were made by Graffagnino and Seyler in 1935.
The most commonly used anesthetic agents for lumbar epidural analgesia for labor are bupivacaine 0.0625% to 0.25% and ropivacaine 0.1% to 0.2%.
The technique of lumbar epidural analgesia involves the insertion of a 17- or 18-gauge hollow-bore needle through the ligamentum flavum into the epidural space at the L4-5, L3-4, or L2-3 interspace. Although the hanging-drop technique for identification of the epidural space is generally effective, most physicians prefer the loss-of-resistance technique as the one that affords the least risk of penetration of the dura. Use of air or saline may be used to identify the epidural space. A 20-gauge catheter is passed through the epidural needle for a distance of 3 to 5 cm within the epidural space. This catheter is securely taped in place and serves as an avenue for intermittent or continuous infusion of local anesthetic agents or opioids.
Combined Spinal–Epidural Analgesia
The combined spinal–epidural (CSE) technique adds a subarachnoid injection of an opioid with or without a small dose of local anesthetic in a needle-through-needle technique to provide a faster onset with a smaller dose of medication than is possible using epidural medications alone (9). The epidural catheter is still available for additional analgesia. A prospective, double-blinded, randomized study compared CSE analgesia with standard epidural analgesia in spontaneously laboring nulliparous parturients. There was no difference in the rate of progress of labor, the amount of epidural local anesthetic required, and the incidence of instrumental deliveries between the CSE and the standard epidural analgesia groups. However, analgesia was more complete and there was higher patient satisfaction in the CSE group than in the epidural analgesia group.
Patient-controlled Epidural Analgesia
Patient-controlled epidural analgesia (PCEA) is a technique by which the patient self-administers on-demand doses of an analgesic mixture via an epidural catheter, whenever she perceives discomfort. To avoid overdosage, a lockout period follows each self-administration. This technique is associated with a decreased use of local anesthetic solution and less demand on staff time compared to continuous epidural infusion (CEI). Most studies have found patients will self-administer less local anesthetic solution than continuous infusions provide and that anesthesia workforce needs are reduced by about 40% (10). Quality of analgesia, complications, and amount of motor block are similar between the two techniques.
Epidural Medications in Labor
Epidural injection of opioids alone has been shown to be of limited value for the relief of labor pain. High doses of morphine (7.5 mg) have provided satisfactory analgesia, but only during the first stage of labor. Because of its slow onset of action (often 1 hour or more) and high incidence of side effects (nausea and pruritus), morphine is not a satisfactory agent for this use. Fentanyl and sufentanil used alone can provide analgesia for early labor, but require high doses—100 µg fentanyl or 30 µg sufentanil. In contrast, spinal injection of opioids alone provides excellent, although time-limited analgesia for labor in small doses—10 to 25 µg fentanyl or 5 to 10 µg sufentanil.
Fortunately, the addition of opioids to dilute concentrations of epidural local anesthetics has been proven to be quite effective in the relief of labor pain. The combination is a rational one because local anesthetic solutions relieve somatic pain preferentially, whereas opioids are more effective in relieving visceral pain. By combining a lipid-soluble opioid such as fentanyl or sufentanil to bupivacaine or ropivacaine, the concentration of local anesthetic can be dramatically decreased and motor block can be minimized. The addition of fentanyl or sufentanil approximately doubles the analgesic efficacy of any concentration of bupivacaine or ropivacaine, while shortening the time to complete analgesia.
Opioid and Chloroprocaine Mixtures. Mixtures of morphine with chloroprocaine have not been shown to be useful, as chloroprocaine appears to antagonize the analgesic effects of the opioid, while increasing its side effects, particularly nausea and pruritus. The mechanism of this unfavorable interaction is unknown. Chloroprocaine may also prolong the onset of morphine analgesia and decrease the effectiveness of bupivacaine if used before these agents. The most satisfactory analgesia appears to be produced when opioids are combined with amide local anesthetics.
The beneficial effects of epidural opioids in labor appear to be the following:
· reduction in motor block, allowing improved mobility of the patient
· reduction in shivering
· decreased incidence of hypotension
· use of lower doses of local anesthetic agents
· greater maternal satisfaction with the analgesia that they provide.
Effects of Epidural Analgesia on Uterine Blood Flow
Studies investigating changes in intervillous blood flow and mean arterial pressure with lumbar epidural analgesia in adequately preloaded patients have demonstrated only a negligible reduction in these parameters with the onset of effective analgesia. Well-hydrated patients with preeclampsia have experienced improvement in intervillous blood flow along with a slight decrease in blood pressure.
Advantages and Disadvantages of Lumbar Epidural Analgesia
There are three principal advantages of lumbar epidural analgesia:
· the parturient remains awake and cooperative.
· the incidence of complications is very low when the technique is used correctly.
· once an epidural catheter is in place, it can be used to provide analgesia or anesthesia for a vaginal or cesarean delivery.
The disadvantages of lumbar epidural analgesia include:
· the possibility of poor perineal analgesia
· the presence of “hot spots”, where analgesia is insufficient
· delayed onset of action
· technical difficulty
· intravascular injection
· accidental dural puncture
· hypotension.
Technical failure occurs in approximately 4% of cases.
Indications and Contraindications for Lumbar Epidural Analgesia
Indications for lumbar epidural analgesia include pain in labor, management of the patient with preeclampsia who does not have a coagulation abnormality, management of labor in patients with certain cardiac lesions, and management of breech delivery.
A joint statement by the American College of Obstetricians and Gynecologists (ACOG) and the American Society of Anesthesiologists (ASA) (11) notes that: “Labor results in severe pain for many women. There is no other circumstance in which it is considered acceptable for a person to experience untreated severe pain, amenable to safe intervention, while under a physician's care. In the absence of a medical contraindication, maternal request is a sufficient medical indication for pain relief during labor. Of the various pharmacologic methods of pain relief used in labor and delivery, regional analgesia techniques—spinal, epidural and combined spinal epidural (CSE) are the most flexible, effective, and least depressing to the CNS, allowing for an alert, participating mother and an alert neonate.”
There are absolute and relative contraindications to the induction of lumbar epidural analgesia. Absolute contraindications include the following: patient refusal, hemodynamic instability, infection at the anticipated site of puncture, and absence of resuscitation equipment. Relative contraindications may include fever, preexisting CNS disease, hypovolemia, hypotension, lack of experience by the anesthetist, and blood coagulation defects.
Although an arbitrary platelet count of 100,000 per mm3 has been advocated as the lower limit for safe lumbar epidural analgesia, successful blocks without epidural bleeding complications have been obtained with platelet counts as low as 50,000 per mm3. In one report, Beilin and colleagues (12) described a study of 80 women who presented for labor and delivery and had platelet counts less than 100,000 per mm3 during the peripartum period. Of these 80, 30 were given an epidural anesthetic. The range of platelet counts was 69,000 to 98,000 per mm3. No patient had any documented neurologic complication. These authors concluded that regional anesthesia should not necessarily be withheld when the platelet count is less than 100,000 per mm3. However, given that the risk of epidural hematoma is extremely rare, a study this small would be unlikely to reveal a problem. The underlying cause of the thrombocytopenia is also important and must be considered along with any absolute number. For example, the patient with idiopathic thrombocytopenic purpura or gestational thrombocytopenia is much less likely to bleed at a low platelet count than the patient with HELLP (hemolysis, elevated liver enzymes, low platelet count) syndrome. The best indicator of potential bleeding is a patient history of bruises, contusions, petechiae, bleeding from the gums, and so on.
Subarachnoid Analgesia
Subarachnoid or spinal analgesia for labor has become increasingly popular. The major advantages of spinal analgesia include (a) use of a very low dose of local anesthetic or narcotic analgesic drug and (b) the excellent analgesia provided. Onset of action is rapid, and uterine activity is not affected. The disadvantages include (a) the possibility of postdural puncture headache (PDPH) which is increasingly rare with the use of pencil-point needles and (b) the time-limited nature of a single-shot technique. For this reason spinal analgesia is commonly combined with an epidural catheter as a CSE technique. Indications and contraindications are similar to epidural analgesia.
Morphine and fentanyl can provided analgesia during labor when administered intrathecally in small doses. Labor analgesia usually lasts for 4 to 8 hours and is not accompanied by motor block. The major disadvantages include pruritus and nausea. Pruritus can be antagonized with small doses of intravenous naloxone or oral naltrexone. PDPH can be minimized through the use of 22- to 27-gauge Whitacre, Sprotte, or other pencil-point needles.
A 28-gauge microcatheter can be passed through 22-gauge spinal needles, permitting the use of continuous spinal analgesia in labor and surgery. These catheters were withdrawn from the market because of associated cauda equina syndrome, probably related to local anesthetic neurotoxicity.
Complications of Regional Block Analgesia
Hypotension
Hypotension is common, occurring in 10% to 20% of patients undergoing epidural analgesia for labor and 50% to 80% for cesarean delivery. It often occurs despite left uterine displacement and administration of an adequate vascular preload. Treatment should consist of the following steps:
1. Ensure or verify left uterine displacement.
2. Increase intravenous fluid infusion to the maximal available rate.
3. Administer oxygen by facemask.
4. If hypotension does not immediately resolve, administer ephedrine intravenously in 5- to 10-mg increments until hypotension resolves.
Phenylephrine, an α-agonist, has been avoided in the past because of concerns about compromising uterine blood flow, but more recent work has shown no adverse clinical effects and higher fetal pH values than ephedrine alone (13).
Postdural Puncture Headache
When a large-bore epidural needle (e.g., 18-gauge Tuohy) penetrates the dura and arachnoid membranes, the incidence of PDPH is greater than 50%. Other factors governing the incidence of PDPH include the number of times the dura has been punctured, the direction of the bevel, and the type of needle used.
PDPH occurs because a decrease in cerebrospinal fluid (CSF) volume causes compensatory cerebral vasodilation and traction on the pain-sensitive blood vessels and meninges. Assumption of the erect position increases traction on these structures and aggravates the pain. Therefore, the main diagnostic criterion of PDPH is that it is postural. Ocular and auditory symptoms, such as vertigo, ataxia, and sixth cranial nerve palsy may be associated with PDPH.
Many different treatment regimens have been employed for this condition, including administration of saline through the epidural catheter, the use of abdominal binders, the administration of intravenous or oral caffeine (as a cerebral vasoconstrictor), bed rest, analgesics, and epidural blood patches. The most effective of these is the epidural blood patch.
Evidence suggests that prophylactic epidural blood patch can substantially reduce the incidence and severity of PDPH. In a study by Lowinwirt and associates (14), patients with accidental dural puncture with 16- or 17-gauge needles were randomized and allocated to two treatment groups. In one group, patients received 15 to 20 mL of autologous blood through the indwelling epidural catheter at least 5 hours following the last dose of local anesthetic and just before catheter removal. Patients in the control group were managed conservatively with intravenous hydration, bed rest, theophylline, or caffeine. Eighty-three percent of patients receiving the prophylactic epidural blood patch avoided PDPH. Only 4% of patients treated conservatively avoided PDPH. Use of a prophylactic epidural blood patch was not associated with any complications.
Chronic Back Pain
Low-back pain is a common complaint in the postpartum period. A controversy exists as to the role that epidural analgesia for labor and delivery might play in the subsequent development of low-back pain. Whereas several retrospective studies have demonstrated an association, other prospective studies have shown no increased risk of acute low-back pain after epidural use. A study by Loughnan and colleagues (15) examined the risk of low-back pain 6 months after delivery in patients who received epidural analgesia, as compared with those who did not. This prospective follow-up study showed no difference in the prevalence of low-back pain at 6 months after delivery. Therefore, it seems unlikely that epidural analgesia makes any significant contribution to the 19% to 33% prevalence of low-back pain among postpartum women.
Neurologic Complications
Neurologic complications of epidural and spinal analgesia are rare, occurring in about 1 per 10,000 blocks. Many postpartum neurologic sequelae are related to intraoperative positioning problems. An example is foot drop associated with pressure on the lateral popliteal nerve and caused by an improperly placed stirrup. In the lithotomy position, pressure applied on the femoral cutaneous nerve by the inguinal ligament may cause pain and numbness in the lateral thigh. Pain and numbness in the distribution of the sciatic nerve may result from forceps delivery or passage of the baby's head through the pelvis.
Spinal nerve root neuropathy may be caused by traumatic insertion of a spinal needle or an epidural needle or catheter. In this case, pain and paresthesias along the distribution of the nerve are perceived immediately, but they tend to disappear when the needle or catheter is removed. Rarely, symptoms may appear as long as 2 days after the procedure. Recovery usually occurs in 1 to 2 weeks, but injury can be permanent.
Accidental injection of an irritant solution (e.g., thiopental) or a prep solution into the CSF may produce adhesive arachnoiditis, which can cause permanent loss of spinal cord function. Epidural abscess usually is caused by hematogenous spread and not by injection of contaminated anesthetic solutions.
Epidural hematoma is a serious complication that, although rare, may occur in conjunction with coagulopathy. A hematoma should be suspected if recovery from the block is slow or absent or if neurologic function worsens after a period of initial recovery. The primary symptoms are pain and weakness, which may progress rapidly to paralysis. Early surgical drainage provides the only chance for recovery of neurologic function.
Effects of Epidural Analgesia on Progress of Labor
Whether use of regional analgesic techniques is associated with an increased risk of cesarean delivery remains controversial, but that concern is mainly based on results from small retrospective studies. There is definitely an association between use of epidural analgesia for labor and cesarean delivery, but the problem is that nulliparous women with longer and more painful labors are the patients more likely to choose epidural analgesia, and they are also those who are at higher risk to have a cesarean delivery regardless of their choice of labor analgesia. The presence of severe pain during early labor signals an increased risk for prolonged labor and operative delivery (16). Also, regional analgesia is often recommended to women in whom operative or instrumental delivery is thought to be likely. Designing a study to remove that bias or association has proven difficult, both for the ethical reason you cannot refuse a treatment available to a patient if requested (i.e., if a patient is randomized to receive “no epidural” but she later requests it because of inadequate pain relief she must be allowed to cross over) and because there is no other form of pain relief to offer that provides equivalent analgesia (i.e., a “control group”). For this reason, many studies done prior to the last decade were methodologically flawed.
More recent studies have attempted to control for the fact that women already at increased risk for an operative delivery are more likely to choose epidural analgesia, and have not found regional analgesia to be associated with cesarean delivery (17). There are different methodological ways to accomplish this. Several retrospective, population-based studies have found that the introduction of an epidural analgesia service or the increased use of epidural analgesia did not increase the cesarean delivery rate. In a “natural” experiment, a military hospital went from a 1% to 84% epidural analgesia rate in one year while other conditions remained unchanged (18). A review of singleton, nulliparous, term patients in spontaneous labor before and after the change found no differences in rates of cesarean delivery overall and for dystocia, no change in instrumental delivery rates, no change in duration of first and active stages of labor, but an increase in the second stage of labor by about 25 minutes. At the National Maternity Hospital in Dublin, the epidural rate increased from 10% to 57% over 3 years with no effect on cesarean delivery rates (19). These clinicians suggested use of active management of labor and use of oxytocin in the second stage of labor to overcome increases in instrumental vaginal delivery rates.
Other studies have used generous doses of narcotics in the control group to prevent crossover to the epidural analgesia group. A review of 802 nulliparous patients randomized to epidural analgesia or intramuscular meperidine using standardized labor management found similar cesarean delivery rates in an intent-to-treat analysis (20). The spontaneous vaginal delivery rate was also similar between groups. A randomized trial of 715 women who received epidural analgesia or patient-controlled meperidine found no difference in cesarean delivery rates and lower pain scores in the epidural group (4). Pain relief is a worthy goal unto itself!
Obstetric management must also influence the cesarean delivery rate. Even randomized trials cannot blind the obstetrician to the type of analgesia being used, and the obstetrician makes the decision regarding the need for cesarean delivery. If epidural analgesia has an influence on the risk of cesarean delivery, then those obstetricians with a higher use should have a higher cesarean delivery rate. In contrast, a review of 110 obstetricians in a single hospital practice found no relationship between frequency of epidural analgesia use and rate of cesarean section for dystocia across practitioners (R2 = 0.019) (21). They concluded that after accounting for a number of known patient risk factors, obstetric practice style appears to be a major determinant of rates of cesarean delivery.
As noted earlier, the intensity of labor pain may be predictive of an increased risk of cesarean delivery for dystocia. A secondary analysis of women randomized to receive patient-controlled intravenous meperidine analgesia for labor found that those who required higher doses of narcotic had higher pain scores initially, longer labors (9 vs. 5 hours), and more cesarean deliveries for dystocia (14% vs. 1.4%) (22).
Thus, it would appear that there are many variables with the potential to affect the risk of cesarean delivery besides choice of analgesia during labor. These would include patient-related factors such as parity, induction, level of pain, labor pattern, and oxytocin use, as well as obstetrician-related factors such as active or passive management. An editorial suggested that “Perhaps the time has now come to look at the problem in a different way and to ask why labor is prolonged and spontaneous delivery less likely in some units than in others. The realization that labor with regional analgesia is not the same as that without and that management must be modified will hopefully result in improvements in outcome” (23).
Chestnut (24) has made some astute comments on the current state of affairs regarding anesthesia in labor:
1. Use of dilute solutions of local anesthetics in labor may be less likely to have an effect on progress of labor.
2. Administration of epidural analgesia should be delayed until labor is well established; however, it is unnecessary to wait until an arbitrary cervical dilation, such as 5 cm.
3. Studies on patients attempting vaginal birth after cesarean delivery have not shown an increase in cesarean delivery rates when epidural analgesia is used, and good analgesia may encourage some women to attempt vaginal delivery.
4. Use of epidural analgesia during labor may decrease the use of general anesthesia with its attendant risks if emergency cesarean delivery is required.
5. Maternal administration of high doses of narcotics may result in substantial neonatal effects such as respiratory depression (25).
6. Maternal–fetal factors and obstetric management, not epidural analgesia, are the most important determinants of the cesarean delivery rate.
OTHER METHODS OF PAIN RELIEF
Prepared Childbirth
Prepared childbirth techniques are based on the belief that pain can be eliminated or reduced by conditioned reflexes of controlled relaxation and that education about the birth process can diminish the pain resulting from fear of the unknown. Parturients and significant others are offered a series of five to ten weekly lectures and are educated about pregnancy, labor, and the delivery process. The parturient is taught how to relax and engages in exercises to strengthen her back and abdominal muscles. She also learns specific breathing patterns to be used while she experiences the discomfort of uterine contractions. All parturients should have access to emotional support, whether by her husband, a family member, a birth attendant (doula), or professional hospital staff. Insurance companies are beginning to pay for doulas as the literature has supported the beneficial effect on decreasing interventions (26). Effective courses also teach pregnant women that additional methods of pain relief are available and that these do not cause harm to the fetus. The pregnant woman should be advised that to ask for these other methods does not imply that she is a failure.
Hypnosis
Hypnosis is a state of altered consciousness that requires deep concentration. The patient is not asleep, but she initiates a trance as labor begins and continues it until delivery is completed. The patient must undergo a time-consuming series of training sessions with a hypnotist, and this technique is not always successful (27).
Acupuncture
Acupuncture has been used to help control labor pain in China and the Far East for many years. Since the early 1970s, mixed reports of its efficacy have been published in the West. Some studies indicate that acupuncture can significantly lower pain scores and may decrease the duration of the first stage of labor. Although enthusiasm for the technique varies in Western countries, the Chinese continue to report 99% rates of excellent and good success. When acupuncture is used for cesarean section in conjunction with intravenous meperidine and local anesthetic infiltration, blood pressure, pulse rate, and respirations are stable, and the degree of patient acceptance is reported to be high.
Biofeedback
Biofeedback is provided by a portable electromyographic device through an audible sound and visual monitor. Electrodes placed over the maternal abdomen monitor tension of the abdominal musculature. This technique may be helpful during the first stage of labor and may reduce its duration.
Transcutaneous Electrical Nerve Stimulation
Transcutaneous electrical nerve stimulation (TENS) analgesia is based on the observation that application of a mild electric current to the skin can result in reduction of pain. Activation based on the gate theory and release of enkephalins are possible modes of action. Studies evaluating the effectiveness of TENS suggested that, although the method does no harm, it probably does little good and should not be advocated for widespread use for labor analgesia (28).
Intracutaneous Nerve Stimulation
Trolle and colleagues (29) evaluated the analgesic effect of intradermal sterile water blocks in women complaining of severe low-back pain during labor. Saline solution was used as a control. Sterile water or saline (0.1 mL) was injected at four different spots in the low-back area, approximately corresponding to the borders of the sacrum. Eighty-nine percent of women in the sterile water group reported an analgesic effect, compared with 45% in the saline group. However, meperidine use in the two groups was similar, as were the rates for oxytocin use and dystocia. The cesarean section rate in the sterile water group was significantly lower due to more cephalopelvic disproportion and malposition of the occiput in the saline group. This technique is free of adverse effects and enjoys a high degree of patient acceptance although the mechanism is unclear.
ANESTHESIA FOR CESAREAN DELIVERY
There are three anesthetic choices for cesarean delivery. Selection of one over the others depends on the patient's desires, medical status, and the urgency of the operation. Regional anesthesia is strongly preferred in the United States (Table 3.4).
|
|
|
TABLE 3.4. Types of cesarean anesthesia provided by size of hospital in three time periods |
Epidural Anesthesia
Epidural anesthesia accounts for approximately 40% of anesthetics used for cesarean section. It offers the advantages of unlimited duration, minimizing the risks of airway management, and providing a route for postoperative pain management.
To carry out a cesarean delivery, a sensory dermatome level of at least T-4 is required. Anesthesia to this level eliminates proprioception from the respiratory muscles of the chest wall, and the parturient may experience a subjective sensation of dyspnea. Reassurance will usually allay this fear. The patient should be placed on the operating table with the uterus displaced laterally through elevation of the right hip or by tilting of the operating table, to prevent aortocaval compression.
A vascular preload of 1000 to 1500 mL of a non–glucose-containing crystalloid solution should be administered before dosing of the epidural needle or catheter with the anesthetizing solution. A surgical concentration of a local anesthetic (often 2% lidocaine) with or without added opioid is administered through the catheter in 3- to 5-mL increments. The patient should be given oxygen by nasal cannula or by mask. One study failed to reveal any differences in the clinical condition of neonates, as assessed by Apgar scores and blood gas analyses, when oxygen administration by these two modalities was compared.
Epidural opioids have been useful for relieving pain of visceral origin, which affects as many as one-third of the women who have cesarean sections under epidural anesthesia. Visceral pain occurs primarily during bladder retraction, exteriorization of the uterus, and suturing of the peritoneum. The addition of fentanyl or sufentanil to the local anesthetic reduces the time of onset of analgesia, decreases the incidence of nausea, and increases the quality of analgesia without depressing the neurobehavioral status of the newborn.
Studies of fentanyl concentrations in neonates demonstrate that fentanyl crosses the placenta. Even high maternal doses (e.g., 100 µg) of fentanyl yield safe levels in the newborn. Morphine 2 to 4 mg is often administered through the epidural catheter after delivery to provide 12 to 24 hours of postoperative analgesia, although the incidence of associated pruritus and nausea can be high. Use of epidural morphine may reactivate herpetic labialis (herpes simplex virus-1) infections (30).
There are several advantages to using epidural analgesia for cesarean section delivery:
· if an epidural catheter is already in place, it can be used expeditiously for the cesarean section delivery.
· maternal hypotension may be less pronounced and slower in onset with epidural than with spinal anesthesia.
· headache is usually avoided, unless the patient sustains an accidental dural puncture.
· the length of anesthesia is controllable in case surgery is prolonged.
· the technique is adaptable for postoperative pain relief.
The disadvantages include:
· the slower onset of analgesia
· the requirement for a larger amount of anesthetic solution with its attendant increased risk of systemic toxicity
· the lower success rate than that experienced with subarachnoid block.
An unexpectedly high level of anesthetic block may be achieved with epidural or spinal anesthesia and, as a result, this should be monitored. The likelihood of inadvertent spinal anesthesia while attempting epidural block can be minimized through gentle aspiration of the catheter combined with using a test dose of sufficiently small volume that it is unlikely to produce a high block. A total spinal block generally occurs within 90 seconds after injection, but it may be delayed for as long as 20 minutes. Dyspnea, hypotension, unconsciousness, and apnea are signs and symptoms of total spinal block. Treatment includes ventilation through an endotracheal tube and, if needed, circulatory support.
Subarachnoid or Spinal Anesthesia
A subarachnoid block provides excellent anesthesia for cesarean section delivery. Over 50% of cesarean deliveries are performed using this technique (see Table 3.4). Prehydration is administered with 1500 to 2000 mL of a non–glucose-containing crystalloid solution. A 22- to 27-gauge pencil-point spinal needle is inserted into the subarachnoid space, which is identified by the characteristic feel of the needle penetrating the dura and observing CSF in the needle. Bupivacaine 0.75%, 10 to 12 mg, with dextrose, is most commonly used. Analgesia of shorter duration is obtained with the use of lidocaine 5% in 7.5% dextrose.
Opioids may also be administered intrathecally to improve quality of analgesia, decrease nausea, and improve cardiovascular stability by allowing a lower dose of local anesthetic. Spinal (as well as epidural) narcotics are associated with a high incidence of pruritus, as well as the rare but real potential for delayed respiratory depression. Fentanyl may be administered to improve intraoperative analgesia while the addition of morphine can provide postoperative analgesia that may last for 18 to 24 hours.
Contraindications to spinal anesthesia are the same as for epidural anesthesia and include patient refusal, septicemia, infection of the puncture site, acute or chronic hypovolemia, and abnormal clotting parameters. Spinal anesthesia is usually avoided in pregnant women with acute CNS disease.
The most common complication of spinal anesthesia is hypotension. This should be treated promptly with fluid administration and intravenous ephedrine (5- to 10-mg bolus). Oxygen should be given, and the parturient's oxygen saturation should be monitored with a pulse oximeter. In the event of a high spinal block which compromises ventilation or airway control, cricoid pressure should be applied and endotracheal intubation performed to prevent aspiration of gastric contents.
With the increasing use of spinal and epidural narcotics, pruritus is becoming a commonplace adverse effect. Its incidence approaches 60% when spinal or epidural morphine is employed. The cause seems to be related to stimulation of opioid receptors rather than to release of histamine. Naloxone can be used to control pruritus, but the dose must be titrated carefully to avoid antagonism of analgesia. Nalbuphine may also be used and is less likely to antagonize analgesia.
Approximately 23% of women experience shivering during normal labor and delivery, and the rate increases to approximately 68% with epidural analgesia. Shivering can be diminished or abolished through epidural injection of opioids (e.g., fentanyl 100 µg) or small intravenous doses of meperidine (e.g., 12.5 mg).
General Anesthesia
General anesthesia is used for cesarean delivery when the patient refuses regional analgesia or has a contraindication to regional analgesia, or when a need exists for rapid delivery because of fetal distress, cord prolapse, shoulder dystocia, or maternal hemorrhage.
The American College of Obstetricians and Gynecologists in the fifth edition of Guidelines for Perinatal Care, cites the risk factors for failed intubation and urges obstetricians to be alert to the presence of the factors that place parturients at increased risk for complications from emergency general anesthesia. Among these are marked obesity, severe facial and neck edema, extremely short stature, short neck, difficulty opening the mouth, a small mandible, protuberant teeth, arthritis of the neck, anatomic abnormalities of the face or mouth, a large thyroid gland, asthma, serious medical or obstetric complications, and a history of problems with anesthetics. If any of these factors is identified, a member of the anesthesia team should be consulted to prepare for the unexpected need to induce general anesthesia. If the anesthesiologist has concerns about his or her ability to intubate the patient, early placement of a regional anesthetic should be planned or arrangements for an awake intubation should be made.
Pneumonitis resulting from aspiration of gastric contents has long been feared as a complication of general anesthesia for obstetrics, but is extremely rare. One review compared the incidence of aspiration in obstetric and gynecological patients (31). The incidence of clinically significant aspiration was 0.11% in women undergoing cesarean delivery compared to 0.01% in gynecology inpatients. No patient died, but morbidity was significant. The prudent anesthetist administers a nonparticulate oral antacid, such as sodium citrate, given prophylactically to increase the gastric pH. If time allows, an H2-blocker (e.g., ranitidine 50 mg intravenously) should be administered. Intravenous metoclopramide, 10 mg, hastens gastric emptying, increases gastroesophageal sphincter tone, and may decrease nausea.
Before induction of anesthesia, the patient should be preoxygenated with 100% oxygen by mask for at least 3 minutes. Induction is commonly carried out using thiopental (3–4 mg per kg i.v.). Propofol (Diprivan) has also been used. Propofol is associated with a blunted hypertensive response to endotracheal intubation and has yielded similar and satisfactory Apgar scores, neurologic and adaptive capacity scores, and umbilical cord blood gas analyses. If propofol infusion is used for maintenance of anesthesia for a prolonged time before delivery, neonatal blood levels are high, and neurologic and adaptive capacity scores may be impaired. If the patient is hemodynamically unstable, ketamine 1 mg per kg or etomidate 0.3 mg per kg may be used.
Intubation is facilitated by use of succinylcholine. Cricoid pressure is maintained during induction of anesthesia until the endotracheal tube is in place, the cuff has been inflated, respirations have been auscultated, and end-tidal carbon dioxide has been seen. After successful intubation, a mixture of equal parts of nitrous oxide and oxygen may be administered, and a low dose of an inhalational agent, such as desflurane 3%, sevoflurane 1% or isoflurane 0.75%, is administered to optimize maternal analgesia and amnesia. These low concentrations have minimal effects on uterine contractility and are not associated with postpartum hemorrhage. After delivery of the infant, the nitrous oxide concentration may be increased to 70%, and narcotics may be given intravenously to supplement the anesthesia. Midazolam may be used to decrease the risk of maternal recall.
The advantages of general anesthesia include:
· reliability of the technique
· rapidity of induction of anesthesia
· avoidance of sympathetic blockade and hypotension.
The disadvantages include:
· the risks of maternal aspiration of gastric contents
· failed intubation
· maternal awareness
· hypertension during manipulation of the larynx.
If the cords are poorly visualized during laryngoscopy, no more than three attempts at endotracheal intubation should be made before beginning a failed intubation drill (32). The initial maneuver in the failed intubation drill depends on the obstetric indication for cesarean section. If the operation is not emergent, the patient should be awakened and an epidural or spinal block performed. If a regional anesthetic cannot be accomplished, an awake fiberoptic intubation should be considered. In an obstetric emergency where surgery must proceed, the patient must be ventilated with bag and mask or laryngeal mask airway, and anesthesia may be maintained with inhalational or intravenous agents throughout the remainder of the cesarean section. The continuation of cricoid pressure is important to reduce the maternal risk of aspiration. If it should prove impossible to ventilate the patient with bag and mask, an emergency maneuver such as cricothyroidotomy must be performed. Use of an esophageal gastric tube airway (Combitube) or laryngeal mask may enable adequate ventilation.
Inability to intubate has been estimated to occur seven times more commonly in the obstetric patient than in the general operating room, and continues to contribute significantly to anesthetic causes of maternal mortality (33). Anticipation of a difficult intubation allows the anesthesia team to be prepared to avoid general anesthesia or plan an awake intubation.
Analgesia after Cesarean Section
Considerable advances have been made in the management of pain after cesarean section. The availability of spinal and epidural narcotics has enabled the anesthesia team to provide the postsurgical patient with effective, long-term analgesia. Morphine is the most commonly used neuraxial opioid because of its long duration and lack of motor block compared to local anesthetic infusions. The most feared complication is respiratory depression. The rate of analgesia-related respiratory depression is approximately 0.09%. Because this complication is rare, patients receiving postoperative neuraxial opioid analgesia may be safely nursed on the general ward, if the nurses are appropriately educated in monitoring the degree of somnolence and the respiratory rates of their patients. Patients who did not receive regional anesthesia may receive intravenous PCA. Combining narcotics and nonsteroidal antiinflammatory medications such as ketorolac or ibuprofen improves the quality of analgesia and allows reduced doses of narcotics. Naloxone should be readily available to antagonize respiratory depression.
SUMMARY POINTS
· Pain management is an important part of modern obstetric care. Most women will request some form of analgesia during childbirth.
· Parenteral narcotics for labor analgesia may be administered by intermittent injection or patient-controlled intravenous infusion. There are advantages and disadvantages of all opioids.
· High systemic blood levels of local anesthetic caused by intravascular injection or excessive absorption may lead to convulsions and cardiac arrest. Resuscitation equipment must be immediately available whenever regional blocks are used.
· Modern techniques of regional analgesia for labor (dilute concentrations of epidural local anesthetics, combined spinal–epidural analgesia and patient-controlled epidural infusions) emphasize pain relief with minimal motor block. Studies indicate these techniques do not impact progress of labor.
· Although modern anesthetic care for cesarean delivery is extremely safe (anesthesia-related maternal mortality = 1.1 per million live births), general anesthesia complications are more common than regional anesthetic complications because of difficulties with airway management.
REFERENCES
1. Rosen MA, Hughes SC, Levinson G. Regional anesthesia for labor and delivery. In: Hughes SC, Levinson G, Rosen MA, eds. Anesthesia for obstetrics, fourth ed. Philadelphia: Lippincott Williams & Wilkins, 2002:123–148.
2. Hawkins JL, et al. ASA Practice Guidelines for Obstetrical Anesthesia. Anesthesiology 1999;90:600–611.
3. Olofsson CH, Ekblom A, Edman-Ordeberg G, et al. Lack of analgesic effect systemically administered morphine or pethidine in labour. Br J Obstet Gynaecol 1996;103:968–972.
4. Sharma SK, Sidawi JE, Ramin SM, et al. A randomized trial of epidural versus patient-controlled meperidine analgesia during labor. Anesthesiology1997;87:487–494.
5. Rosenblatt WH, Cioffi AM, Sinatra R, et al. Metoclopramide: an analgesic adjunct to patient-controlled analgesia. Anesth Analg 1991;73:553–558.
6. Maroof M, Hakin S, Khan RM, et al. Low-dose ketamine infusion if effective in relieving labor pain. Anesth Analg 1998;86:S380(abst).
7. Butterworth JF IV, Walker FO, Lysak SZ. Pregnancy increases median nerve susceptibility to lidocaine. Anesthesiology 1990;72:962–965.
7a. Weinberg GL. Current concepts in resuscitation of patients with local anesthetic cardiac toxicity. Reg Anes Pain Med 2002;27:568–575.
8. Baxi LV, Petrie RH, James LS. Human fetal oxygenation following paracervical block. Am J Obstet Gynecol 1979;135:1109–1113.
9. Shennan AH. Effect of low-dose mobile versus traditional epidural techniques on mode of delivery: a randomized controlled trial. Lancet 2001;358:19–23.
10. Viscomi C, Eisenach JC. Patient-controlled epidural analgesia during labor. Obstet Gynecol 1991;77:348–351.
11. American College of Obstetricians and Gynecologists. Pain relief during labor. ACOG Committee Opinion No. 231, 2000.
12. Beilin Y, Zahn J, Comerford M. Safe epidural analgesia in thirty parturients with platelet counts between 69,000 and 98,000 mm-3. Anesth Analg1997;85:385–391.
13. Lee A, Kee WDN, Gin T. A quantitative, systematic review of randomized controlled trials of ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery. Anesth Analg 2002;94:920–926.
14. Lowenwirt I, Cohen S, Zephyr J, et al. Can prophylactic epidural blood patch reduce the incidence and severity of postpartum dural puncture headache in obstetrics? Anesth Analg 1998;86:S378(abst).
15. Loughnan BA, Carli F, Romney M, et al. Epidural analgesia and backache: a randomized controlled comparison with intramuscular meperidine for analgesia during labour. Br J Anaesth 2002;88:466–442.
16. Wuitchik M, Bakal D, Lipshitz J. The clinical significance of pain and cognitive activity in latent labor. Obstet Gynecol 1989;73:35–42.
17. Sharma SK, Leveno KJ. Update: epidural analgesia during labor does not increase cesarean births. Curr Anesth Rep 2000;2:18–24.
18. Zhang J, Yancey MK, Klebanoff MA, et al. Does epidural analgesia prolong labor and increase risk of cesarean delivery? A natural experiment. Am J Obstet Gynecol 2001;185:128–134.
19. Impey L, MacQuillan K, Robson M. Epidural analgesia need not increase operative delivery rates. Am J Obstet Gynecol 2000;182:358–363.
20. Loughnan BA, Carli F, Romney M, et al. Randomized controlled comparison of epidural bupivacaine versus pethidine for analgesia in labour. Br J Anaesth2000;84:715–719.
21. Segal S, Blatman R, Doble M, et al. The influence of the obstetrician in the relationship between epidural analgesia and cesarean section for dystocia. Anesthesiology 1999;91:90–96.
22. Alexander JM, Sharma SK, McIntire DD, et al. Intensity of labor pain and cesarean delivery. Anesth Analg 2001;92:1524–1528.
23. Russell R. The effects of regional analgesia on the progress of labour and delivery. Br J Anaesth 2000;85:709–712.
24. Chestnut DH. Epidural analgesia and the incidence of cesarean section. Anesthesiology 1997;87:472–476.
25. Halpern SH, Leighton BL, Ohlsson A, et al. Effect of epidural vs parenteral opioid analgesia on the progress of labor. JAMA 1998;280:2105–2110.
26. Kennell J, Klaus M, McGrath S, et al. Continuous emotional support during labor in a US hospital: a randomized controlled trial. JAMA 1991;265:2197–2201.
27. Freeman RM, Macaulay AJ, Eve L, et al. Randomized trial of self hypnosis for analgesia in labour. Br Med J 1986;292:657–658.
28. Carroll D, Tramer M, McQuay H, et al. Transcutaneous electrical nerve stimulation in labour pain: a systematic review. Br J Obstet Gynaecol1997;104:169–175.
29. Trolle B, Moller M, Kronborg H, et al. The effect of sterile water blocks on low back labor pain. Am J Obstet Gynecol 1991;164:1277–1281.
30. Crone LA, Conly JM, Clark KM, et al. Recurrent herpes simplex virus labialis and the use of epidural morphine in obstetric patients. Anesth Analg1988;67:318–323.
31. Soreide E, Bjornestad E, Steen PA. An audit of perioperative aspiration pneumonitis in gynaecological and obstetric patients. Acta Anaesth Scand1996;40:14–19.
32. Caplan RA, Benumof JL, Berry FA, et al. Practice guidelines for management of the difficult airway. Anesthesiology 1993;78:597–602.
33. Hawkins JL, Koonin LM, Palmer SK, et al. Anesthesia-related deaths during obstetric delivery in the United States, 1979–1990. Anesthesiology1997;86:277–284.