Helen H. Kay
All bleeding during pregnancy should be investigated by examination and by imaging studies. There are many etiologies for bleeding in pregnancy but the most clinically significant are placental previa and placental abruption since these conditions can lead to serious fetal compromise. Other causes of bleeding that should be excluded are cervical lesions such as carcinoma or polyps, vaginal lacerations from trauma or carcinoma, other uterine bleeding such as dehiscence of a prior cesarean section scar, and premature cervical dilation, although these usually do not involve large amounts of blood loss. The presence of either placenta previa or abruption places the patient in a high-risk situation that warrants close monitoring. A definitive diagnosis is extremely important since either placenta previa or abruption, in many cases, commits the patient to a period of prolonged bed rest and hospitalization.
PLACENTA PREVIA
Incidence
Placenta previa is encountered in approximately 0.5% to 1% of all pregnancies but its incidence may be higher now than in the past due to the increased diagnosis by widespread use of ultrasound scanning. It is fatal in 0.03% of cases (1). Formerly, the diagnosis of milder degrees of placenta previa without hemorrhage may have gone unnoticed by clinical exam. It is more common in multiparous than nulliparous women, occurring in only one in 1,500 nulliparas and as many as 1 in 20 grand multiparas. The incidence in the United States is declining, probably in part due to the declining number of grand multiparous women.
Definition
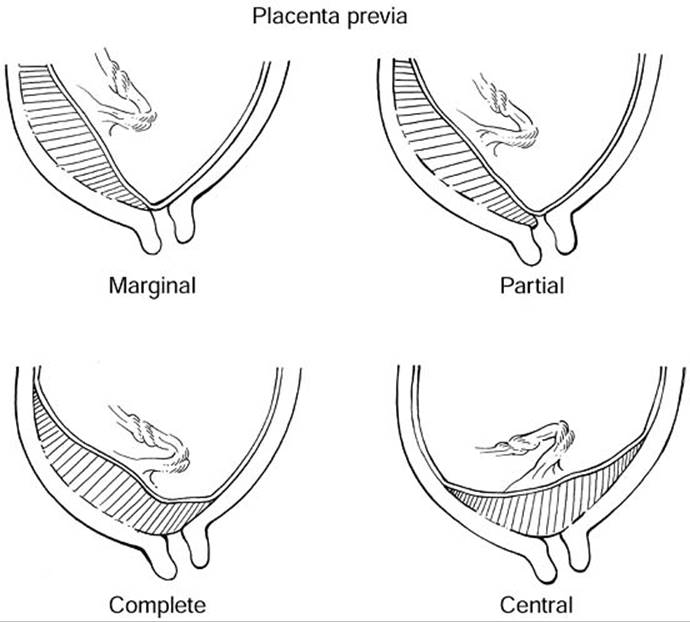
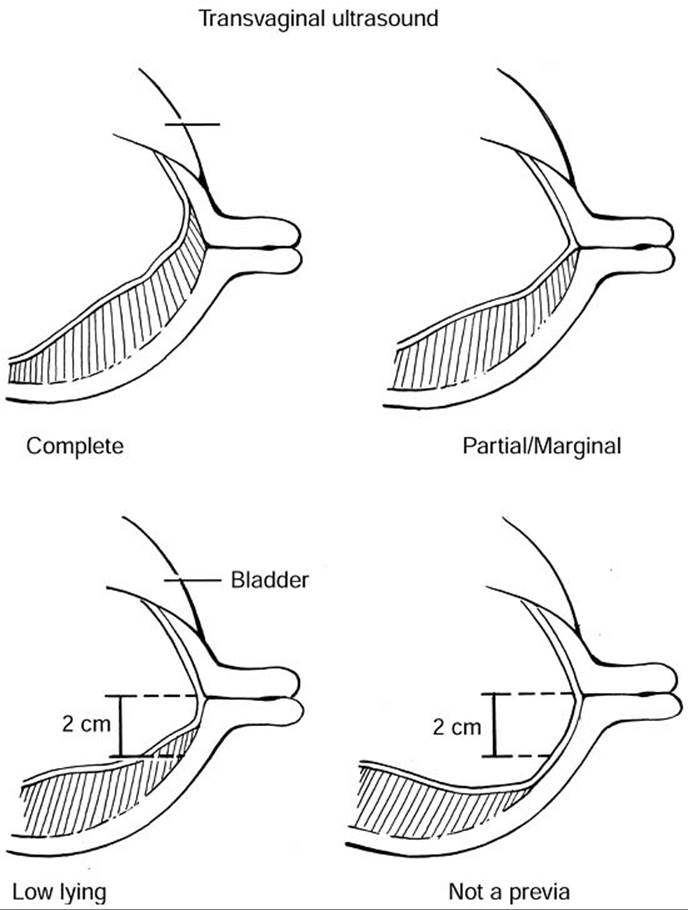
The definition of placenta previa has been complicated because the original descriptions referred to the location of the placenta in relation to a dilated cervix (i.e., one in labor) determined by digital exam. In this definition of a complete previa, the placenta extends over and beyond the internal os. A partial previa refers to a placenta with its edge partially over the dilated cervix, meaning that if we were to visualize the cervix with a speculum, we would see placental tissue over some part of the dilated cervical area, but not all. The last type of previa, the marginal previa, refers to a placenta where the edge lies very close to and up to the edge of the os but does not cover any of it. In those original descriptions, the distance between the placental edge and the internal os was never defined in terms of centimeters (Fig. 20.1). However, with the advent of transvaginal ultrasound imaging, the cervix can be routinely imaged, even when not dilated, and the internal os is seen as a point, hence the confusion over the terminology. In today's practice, any suspected low-lying placenta seen by transabdominal scan should be further evaluated by a transvaginal scan to determine the distance between the edge of the placenta and the internal os (Fig. 20.2). Those cases where the placental edge completely covers the cervical os will be labeled as a complete previa. Those with the placental edge at the cervical os should be labeled as partial or marginal (partial/marginal) since it is impossible to determine whether those placentas will remain covering the dilated cervix during labor or whether they will remain at the edge of the dilated cervix. The cases in which the placental edge is located within 1 to 2 cm of the internal os are the most confusing. Studies that have evaluated this report that patients with a placenta edge less than 1 cm from the cervical os tend to have cesarean sections because they are most like placenta previa patients (i.e., with bleeding and these are delivered by cesarean section) (2). Patients with the edge between 1 to 2 cm of the internal os, however, remain in the gray zone. These patients will benefit most with either a double setup at the time of labor or with close observation in labor and an attempt for a vaginal delivery if there is no bleeding. Patients with a placental edge greater than 2 cm from the cervical os are considered to have normal placentas and not a previa.
|
|
|
FIG. 20.1. Diagrammatic illustration of the three classic types of previa: Marginal, partial, and complete. These relate to diagnosis by digital or visual examination when the patient is in labor with a partially dilated cervix. The term central previa refers to a previa in which the central portion of the placenta lies directly over the cervical os. |
|
|
|
FIG. 20.2. Diagrammatic illustration of the classes of placenta previa diagnosed by transvaginal ultrasound. In the nonlaboring, patient the internal os is seen as a point, and the distance between this and the lower edge of the placenta becomes the more critical reference. |
Pathophysiology
Placenta previa is a condition of abnormal implantation (i.e., into the lower uterine segment rather than the corpus or fundal region). The exact pathophysiology is unknown but because it is seen more frequently in patients who tend to be older, multiparous, and had prior cesarean sections or prior uterine curettage, it is thought to result from scarring in the endometrium. This leads to abnormal endometrial tissue, poor vascularization, thinner myometrium, and a less favorable location for implantation. Presumably, the embryo is attracted to healthier tissue which would be the untampered endometrium of the lower uterine segment. Interestingly, it would appear that the anterior uterine segment after cesarean section would be an unfavorable site for implantation but, for uncertain reasons, the uterine trauma from cesarean sections actually increases the risk of previa by as much as six-fold.
Risk Factors
Several risk factors have been found in association with placenta previa (Table 20.1). The most significant is a prior cesarean section (approximately 1 in 200 deliveries; the incidence is higher if a woman has undergone two or more C-sections). Black or minority patients seem to be at higher risk as are women older than 35 years. Other risks include increased gravidity and parity, and cigarette smoking, with a 2.6- to 4.4-fold increase (3,4 and 5). Interestingly, meta-analyses have shown a preponderance of male gender among the fetuses with placenta previa (6). The mechanism for this is unknown. Previous abortion has not been consistently shown to be associated with an increase in risk for previa.
|
|
|
TABLE 20.1. Risk factors associated with placenta previa |
Diagnosis
The diagnosis of placenta previa can be made by transabdominal ultrasound. With the advent of the curvilinear probe, the cervical and lower uterine segment is much better imaged and the relationship of the lower placental edge to the internal cervical os can be routinely visualized. However, the most common pitfalls include a full, distended bladder and a lower uterine segment contraction that can lead to misdiagnosis. Of those diagnosed in the second trimester, 90% to 95% resolve by the third trimester due to further development of the lower uterine segment, also referred to as migration of the placenta. However, if the placenta covers the internal os by 20 mm or more, meaning that it crosses the os by 20 mm, there is a 100% sensitivity rate for detection of previa at delivery requiring cesarean section (2). Three-dimensional scanning may further increase prenatal detection but remains a new investigational technique for previa at this time. Therefore, it is imperative that follow-up scanning be performed to determine if there is resolution of what appears to be a placenta previa. Marginal and partial placenta previa are significantly less likely to persist into the third trimester (i.e., <5% chance).
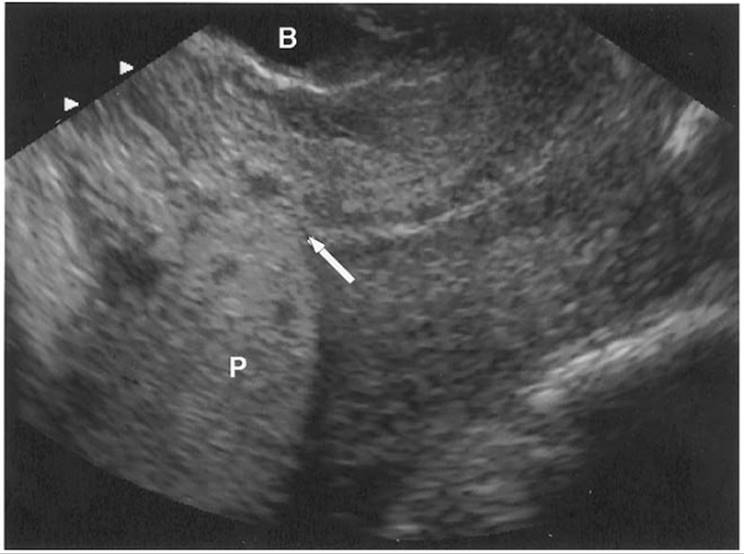
Although initially thought to be contraindicated in patients with suspected placenta previa, transvaginal scanning can be safely performed with caution. In many cases, the relationship between the placental edge and the internal os can be difficult to assess and only a close-up view with a transvaginal approach can make a definitive diagnosis (Fig. 20.3). This approach to scanning has been studied carefully and it does not appear to lead to increased vaginal bleeding, in part because it is technically impossible to introduce the probe through the cervix. Another alternative approach is with translabial scanning which has been reported to be 100% sensitive for detection of a previa. However, on occasion, bowel gas can interfere. When a clear diagnosis of placenta previa is made by a transabdominal or translabial scan, there is no need to perform a transvaginal scan. However, when a partial/marginal placenta previa or low-lying placenta is suspected, a transvaginal scan should be performed to confirm the diagnosis and the distance between the internal os and lower placental edge should be determined. Both types of scanning have greatly reduced the false-positive rate by transabdominal scanning alone which is reported to be as high as 25%.
|
|
|
FIG. 20.3. A transvaginal ultrasound image of a complete placenta previa. The arrow points to the internal os. P, placenta; B, bladder. |
It is debatable whether transvaginal scanning has made the double setup examination obsolete because the relationship between the placenta and cervix can be identified well by experienced scanners. However, there is probably still a place for this exam, particularly in those patients with a placental edge between 1 to 2 cm from the internal os, and with no bleeding. This type of exam can be used in labor to determine the relationship between the placental edge and the cervix by carefully introducing the examining finger into the cervix with the patient prepped and draped in the operating room so that if placenta is encountered at the internal os, an immediate cesarean section can be performed, particularly in the event of acute hemorrhage. If the cervix is dilated, a finger can be passed through the cervical canal to the internal os and placental tissue can be palpated as gritty, fibrous tissue in contrast to the fetal membranes that are smooth to touch, particularly with amniotic fluid behind them. If placental tissue is palpated to cover the os or is located easily within reach, it is considered to be a previa. In this case, the distance relationship (i.e., whether it is 1 or 2 cm from the os) is insignificant since that is an ultrasound imaging determination. At that point, the patient would be managed by proceeding with a cesarean delivery. However, if the cervix is dilated, the membranes are ruptured to allow the fetal vertex to be better applied to the cervix, tamponading what bleeding may develop and enabling the patient to continue laboring to achieve a vaginal delivery or to augment labor with Pitocin.
Clinical Features
Patients with placenta previa typically remain asymptomatic until they have vaginal bleeding. Many are now detected during second trimester ultrasound screening although they remain asymptomatic. It is becoming increasingly rare to have a patient present late in the third trimester with new diagnosis. There are no means to predict which patients will bleed and when they will bleed. Approximately one-fourth of patients do not bleed prior to 36 weeks (7). Usually the first episode of painless vaginal bleeding occurs without any precipitating event, although intercourse and excessive activity by the patient may be inciting factors. Complete previas are more likely to bleed earlier than partial or marginal previas. The thinning lower uterine segment most likely tears into the intervillous space of the placenta. The blood can bring about uterine irritability and occasionally preterm contractions. The amount of blood in this first bleed tends to be variable, from slight to heavy, although it is usually unlikely to be heavy enough to prompt delivery. However, the amount of subsequent bleeds tends to be increasingly heavier as the cervix and lower uterine segment changes. Blood seen on a patient's feet is usually a good indication of a heavy bleed.
Most patients stop bleeding with bed rest, particularly those in the second trimester. Many patients are placed at bed rest either at home or in the hospital until resolution of bleeding. The bright red blood usually converts to a brownish discharge. In the third trimester, though, the amount of bleeding increases and often, delivery is prompted by one massive bleed after multiple earlier bleeds. The blood is typically of maternal origin and therefore the fetus is usually not in jeopardy. In cases with massive bleeding, the fetal heart rate tracing may show signs of distress, usually with repetitive late decelerations.
Patients with placenta previa are at increased risk for abruptio placentae (rate ratio 13.8), cesarean delivery (rate ratio 3.9), fetal malpresentation (rate ratio 2.8), and postpartum hemorrhage (rate ratio 1.7) (1). Although fetal growth restriction was formerly thought to be an outcome of placenta previa, more recent studies do not show an association when comparisons were made between a study group and a well-matched control group and when gestational age at delivery was controlled (8). Although it is impossible to predict which patients will bleed and when, one report suggests that patients with elevated maternal serum alpha-fetoprotein (MSAFP) levels greater than 2.0 multiples of the median (MoM) have a 50% chance of requiring hospitalization for bleeding before 30 weeks gestation, to be delivered preterm before 34 weeks, and to be delivered for pregnancy-associated hypertension before 34 weeks (9). MSAFP elevations did not predict those with placenta accreta or emergent cesarean hysterectomy. Careful note of the MSAFP levels in the second trimester may help us target those patients who need to be cautioned more specifically about adverse outcomes due to the presence of the previa.
Management
Patients diagnosed in the second trimester should be cautioned about the possibility of bleeding. Intercourse should be avoided unless a follow-up scan reveals further migration of the placenta. Otherwise patients may be allowed their usual activities without excess exertion. A repeat scan approximately every 4 weeks should be performed to determine the persistence or resolution of the previa. If further scans reveal resolution, no further evaluation is necessary. However, if follow-up shows persistent previa into the third trimester, the patient should be further counseled regarding her chances of bleeding. Decreased physical activity would be advisable and travel away from home should be discouraged.
Every patient who bleeds needs to be evaluated. Fetal status should be documented. Depending on the amount of bleeding, intravenous fluids should be started and blood should be cross-matched or, at a minimum, typed and screened. Subsequently, continuous availability of cross-matched blood does not appear to be necessary, as few antepartum patients require emergent transfusion. Rh status should be checked and RhoGam should be administered if patients are Rh-negative and unsensitized. A baseline blood count with hemoglobin and hematocrit should be determined to assess degree of bleeding. These blood counts should be interpreted carefully in the context of normal reserve in these pregnant patients as well as the hemodilution with intravenous hydration. Because pregnant women have such reserve, their vital signs and laboratory values may not directly reflect their vascular compromise until they have had a very large amount of bleeding. Their status may be deceptively stable until they get close to serious decompensation. If signs of hypovolemia are present, such as hypotension and tachycardia, the patient more than likely has had severe hemorrhage—more than might be clinically observed. Since it is rare to develop a coagulopathy with a bleed from a previa, a coagulation profile is not necessary at the onset. A Kleihauer-Betke test for fetal blood is also not necessary since it is rare to find an abnormal test result.
If the fetus is clearly previable, continued monitoring and stabilization of maternal hemodynamics is appropriate. Blood can be transfused as needed to maintain the maternal blood count in a normal range (hematocrit >30) until fetal viability is reached. In patients who decline transfusions, erythropoietin may be a good option. In addition, the use of autologous blood donation in these patients may be a safer therapy in some parts of the world. If bleeding ceases, the patient may be a candidate for continued outpatient bed rest. Outpatient expectant management has been analyzed and the cost–benefit ratio was favorable with no outcome difference between those managed as outpatients versus those managed as inpatients (10). Antenatal steroids for fetal lung maturity should be administered between 24 and 34 weeks gestation.
In the third trimester, the threshold for discharging the patient should be higher. A period of prolonged bed rest and observation is warranted and it is not unreasonable to consider hospitalization until delivery. If it appears that immediate delivery is not necessary, patients should be given a course of antenatal steroids, from 24 to 34 weeks with intact membranes. Continuous fetal monitoring should be carried out until the bleeding is stable and then daily fetal assessment is appropriate. Additional episodes of bleeding, despite full bed rest, are not uncommon. Approximately 70% of patients treated expectantly will have a second episode of bleeding and 10% will have a third bleed. Unless acute bleeding mandates preterm delivery, the patient can undergo semi-elective amniocentesis after 36 weeks and delivery if fetal lung maturity can be documented. Approximately 25% to 30% of patients will achieve 36 weeks gestation. If significant bleeding occurs after 34 weeks gestation, a decision to proceed directly to delivery without amniocentesis is justified.
In the event of severe hemorrhage on admission, the medical team should prepare for immediate delivery if the fetus has reached a viable gestation. The anesthesiologist and neonatologist should be notified immediately. Two large-bore intravenous lines should be established and blood should be cross-matched immediately. A Foley catheter should be inserted to monitor urine output. A coagulation panel should also be sent. Continuous fetal monitoring should be performed while preparing for delivery and any decompensation should hasten the delivery process.
In about 20% of the cases with bleeding, the uterus contracts and the additional problem of managing preterm labor needs to be confronted. A transvaginal or translabial ultrasound scan can be performed to assess the cervix if bleeding is not too heavy. If fetal lung maturity is not documented or unlikely, efforts to arrest the labor should be attempted, if only to try to get a course of antenatal steroids on board. However, use of tocolytics is considered controversial and no studies have confirmed their benefit in these patients. The choice of tocolytics should be carefully weighed. Beta-mimetics produce maternal tachycardia and hypotension and are generally contraindicated unless the bleeding appears to be stable. Calcium channel blockers can also cause hypotension. Indomethacin is generally not recommended after 32 weeks because of possible premature closure of the fetal ductus arteriosus. Magnesium sulfate is a popular choice and is the most widely used.
Delivery is by cesarean section for all categories of placenta previa when documented by transvaginal scan with an undilated cervix in the third trimester regardless of whether it is a complete, partial, or marginal previa. However, if the diagnosis cannot be established definitively, such as when vaginal scanning is unavailable, or there is a suspected marginal or partial previa between 1 to 2 cm from the os and without any bleeding, a double setup may be considered when in labor or before labor. If no placenta tissue can be palpated, the membranes should be ruptured and the patient may be allowed to labor. Rupturing the membranes and allowing labor to continue could bring the fetal vertex down, and tamponade any placental bleeding.
In the majority of cases, a low transverse uterine incision can be successfully achieved, particularly with a posterior placenta and with a well-developed lower uterine segment. A transverse incision can still be accomplished in skilled hands even when an anterior placenta is encountered by cutting quickly through the uterus and placenta and delivering the fetus as quickly as possible before there is significant fetal exsanguination. In a good percentage of cases, the placenta previa leads to fetal malpresentation such as transverse lie. In those cases, the best uterine incision would be a vertical, or classical one.
Regional anesthesia may be successfully used for patients with placenta previa. It has been reported that the management of blood pressure for hemorrhage is not a problem and may be the preferred choice due to the lowered amounts of intraoperative blood loss compared to general anesthesia. With heavy bleeding preceding delivery, however, many anesthetists would still opt to use general anesthesia because regional anesthesia in the presence of major hemorrhage may exacerbate hypotension and block the normal sympathetic response to hypovolemia.
Complications
Complications from placenta previa include a longer hospital stay, cesarean delivery (risk ratio [RR] = 3.9), abruptio placenta (RR = 13.8), postpartum hemorrhage (RR = 1.7), fetal malpresentation (RR = 2.8), and maternal death from uterine bleeding (50%) and disseminated intravascular coagulation (DIC) (15.9%) (1).
Placenta Accreta
One significant complication of placenta previa is placenta accreta, increta, and percreta, particularly with a prior history of a cesarean section. Placenta accreta refers to the placenta being attached to the myometrium but does not invade the muscle; increta is seen with the villi invading the myometrium; and percreta is seen when the villi penetrate through the entire uterine wall and into the bladder or rectum. The presence of placenta previa in a patient with a prior cesarean section is associated with accreta in 10% to 35% of cases. With multiple cesarean sections, the risk may be as high as 60% to 65% (11).
During antenatal ultrasound scans, the lower uterine segment should be scrutinized for any evidence of a disruption in the demarcation between the placental fibrinoid base known as the Nitabuch layer and the uterine decidua basalis. Color Doppler assessment can be very helpful by demonstrating marked or turbulent blood flow within the placenta and extending into the surrounding tissues, which is also described as lacunar flow. Similar, and perhaps better, scrutiny can be offered by magnetic resonance imaging (MRI) that can demonstrate placental tissue extension through the uterus (Fig. 20.4). MRI diagnosis for placenta percreta may be quite accurate but diagnosis for placenta accreta, a lesser degree of myometrial invasion, is much lower with sensitivity in the 30% to 40% range. The imaging features include a loss of the decreased signal intensity demarcation between myometrium and decidua basalis. However, one report showed a sensitivity of only 38% for the detection of accreta by MRI. There are some reports of gadolinium-enhanced MRI that can more clearly distinguish a placenta accreta from a percreta. There is not enough data thus far to determine whether MRI is superior to ultrasound for diagnosing placental accreta and percreta.
|
|
|
FIG. 20.4. A sagittal T2-weighted magnetic resonance imaged case of placenta percreta. The percreta is low anterior (arrow). (Courtesy Dr. Mark Kliewer.) |
In the presence of placental accreta, increta, and percreta, the risk of hemorrhage is extremely high. Careful attention should be paid to the lower uterine segment after delivery of the placenta. If bleeding persists despite the usual postpartum uterotonic agents and uterine or hypogastric artery ligation, hysterectomy must be considered. Complications are more likely to arise from delay in making the decision to proceed with hysterectomy. It may be a worthwhile exercise to attempt other methods to control the bleeding before hysterectomy such as oversewing the lower uterine segment, uterine artery ligation, ovarian artery ligation, and uterine packing, but all are associated with mixed results. If definitive hysterectomy is not performed, bilateral arterial embolization of the uterine arteries should be the next option of choice although more experience is needed to determine the success rate of such a procedure for placenta percreta. Precautions to control hemorrhage in general should include intravenous access, blood products, and anesthesiology assistance. If these conditions are suspected by imaging studies prior to delivery, a planned cesarean section after uterine artery catheters are placed for possible embolization may be useful to avoid a hysterectomy. Plans should also be made to deliver in an operating room where there would be access to extra assistance and equipment should a hysterectomy be performed. The interventional radiologists should be notified of the possibility for embolization and the proper equipment should be made available.
Other types of management have included methotrexate for placenta accreta tissue left in situ from bladder wall invasion, subendothelial vasopressin to control bleeding, and balloon occlusion in the hypogastric arteries before hysterectomy. Some of these have been reported with mixed results. Ongoing improvements in the management, once hemorrhage is recognized, will decrease overall morbidity to the patient.
Other complications in the presence of significant hemorrhage from placenta previa could include complications from hypotension such as acute tubular necrosis and Sheehan syndrome of pituitary infarction. Although maternal mortality is low, less than 1%, and perinatal mortality is less than 5%, there can be significant morbidity for both. Lesser complications include risk for hysterectomy (RR = 33.26), antepartum bleeding (RR = 9.81), intrapartum and postpartum hemorrhages (RR = 1.86), blood transfusion (RR = 10.05), septicemia (RR = 5.55), and thrombophlebitis (RR = 4.85) (12). Cases of spontaneous uterine rupture attributable to placenta percreta without prior cesarean delivery have also been reported.
Outcomes
Many reports have suggested a causative effect between placenta previa and low birth weight. The association between placenta previa and fetal growth restriction has been assumed to a large extent. However, more recent studies that have controlled for the gestational age at delivery have found no significant association between previa and growth restriction and the previously seen association is most likely due to preterm birth. Other neonatal outcomes of significance also include an increased risk of congenital anomaly, respiratory distress syndrome, and anemia. The mechanism for the increase in congenital anomalies is not known but the increase in respiratory distress syndrome and anemia can be explained by the increased perinatal bleeding. Mortality, intraventricular hemorrhage, and low Apgar scores are not different, reflecting advances in obstetrics and neonatal treatments.
Recurrence risks for placenta previa are 2% to 3% or six- to eight-fold higher than the normal population. Cigarette smoking further increases these recurrence risks.
Prevention
There are no means to prevent placenta previa. However, some studies have suggested that a cervical cerclage placed between 24 and 30 weeks gestation may decrease the chance of bleeding and blood transfusion while prolonging the pregnancy, increasing the birth weight, and decreasing the hospital stay and costs and admission to the neonatal intensive unit. The mechanism is thought to be due to stabilization of the lower uterine segment. This practice, however, is not established and there have been no large randomized trials to test this intervention (10). Other trials found some benefits in a prolongation of pregnancy by 1 week, fewer readmissions for bleeding, fewer hospitalization days, and higher birth weights, although none of these were statistically significant.
VASA PREVIA
A vasa previa occurs in approximately 1 in 1,000 to 1 in 5,000 pregnancies and refers to a condition associated with a very high fetal mortality in the range of 33% to 100%. It is seen when a fetal vessel crosses and covers the internal os (Fig. 20.5). Patients at risk include those with bi-lobed placentas, succenturiate-lobed placentas, low-lying placentas, pregnancies from in vitro fertilization, and multiple pregnancies. These conditions all increase the likelihood that fetal vessels in the membrane will rest over the cervical os. It is technically only possible in two conditions. One is in the presence of a velamentous cord insertion and the other is a placenta with a succenturiate lobe. In both cases, unprotected fetal vessels within the membranes can go undiagnosed and at the time of artificial rupture of the membranes or with advanced labor, these fetal vessels can be ruptured leading to fetal exsanguinations.
|
|
|
FIG. 20.5. A transvaginal color Doppler ultrasound image of a suspected vasa previa. Markers indicate the distance between the internal os and the cord insertion into the membranes away from the placental edge, a distance less than 1 cm. See color figure 20.5. |
When fetal blood is suspected, it may be confirmed quickly by doing a test for fetal hemoglobin. Because fetal hemoglobin is resistant to alkaline pH, several alkaline denaturation tests have been developed such as the Apt, Ogita, and Loendersloot tests. These tests differ only in the duration of the test but all are less than 10 minutes. Therefore, they are all suitable for an acute situation prior to grossly obvious fetal deterioration. Fetal distress can be represented by a sinusoidal pattern on the fetal heart monitor.
It is prudent to identify the location of the cord insertion into the placenta and to look for the presence of a secondary placental lobe at the time of a routine second trimester scan to avoid a disastrous outcome. Color Doppler scanning dramatically simplifies this diagnosis and when combined with either transvaginal or translabial scanning, can distinguish a funic presentation (i.e., cord presenting ahead of the vertex) from a vasa previa. Reports have also suggested that three-dimensional ultrasonography and MRI may help in the diagnosis of vasa previa but further experience with these techniques needs to be demonstrated. Transvaginal scanning with color Doppler is currently the most effective means available.
Early recognition has been reported to be associated with decreased fetal mortality. It can assist in planning delivery and preventing iatrogenic harm such as from artificial rupture of the membranes. Elective cesarean delivery decreases the perinatal mortality. In undiagnosed cases, a heightened sense of suspicion and aggressive intrapartum and neonatal management are the only means to achieve successful neonatal outcomes.
PLACENTAl ABRUPTION
Placental abruption is a pathologic condition in which some part of the placenta prematurely separates from the uterus. It is one of the leading causes of fetal and neonatal mortality.
Incidence
Many factors lead to placental abruption and its incidence seems to be increasing. The incidence is 0.5% to 1.0%. It is a leading cause of perinatal mortality accounting for 10% to 15% of all perinatal deaths, although this rate may be decreasing with improved neonatal care.
Definition
Three types of placental abruption are:
1. Retroplacental—between the placenta and myometrium; severe is 30% to 40% of the surface area, 50% fetal mortality if greater than 60 mL of blood.
2. Marginal, subchorionic—between the placenta and membranes.
3. Preplacental, subamniotic—between the placenta and the amniotic fluid. These are of no clinical significance.
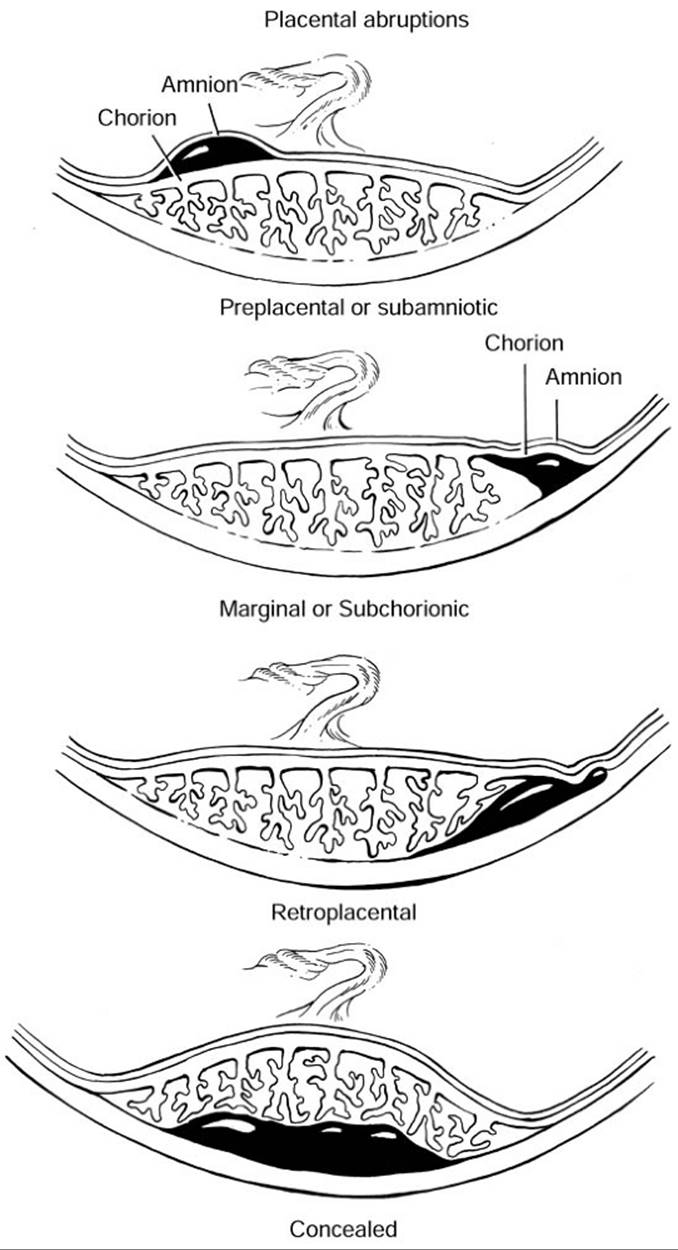
There are several categories of abruptions, some more dangerous than others (Fig. 20.6). The most significant abruption is a retroplacental abruption that can compromise fetal oxygenation and perfusion. These can derive from a marginal abruption, which refers to those located at the edge of the placenta and is seen as a simple lifting of the placental edge away from the uterus. These can be serious when the abruption extends from the margin to the rest of the placenta. A concealed abruption is a retroplacental abruption in which there is no obvious discernible external bleeding.
|
|
|
FIG. 20.6. Diagrammatic representation of various degrees of placental abruption: preplacental or subamniotic (between amnion and chorion), marginal or subchorionic (between placenta and membranes), and retroplacental (between placenta and myometrium). |
Pathophysiology
The pathophysiology of an abruption depends on the etiology. An abruption is the clinically recognized end result when villi separate from the underlying decidua basalis. In blunt trauma, the cause is clearly a forceful shearing effect. In the majority of other cases, bleeding results from cell death (apoptosis) induced through ischemia and hypoxia. In patients with thrombophilia, the tendency to clotting leads to a thrombotic event in the decidua basalis resulting in ischemia and hypoxia. In patients with chorioamnionitis, lipopolysaccharides and other endotoxins generated from the infectious agents induce the accumulation of cytokines, eicosanoids, and reactive oxygen species such as superoxide. All have cytotoxic potential that promotes ischemia and hypoxia. One of the cytotoxic actions of endotoxin is the induction of nitric oxide synthase (NOS) activity that produces nitric oxide (NO), a potent vasodilator and inhibitor of platelet aggregation. As NO is metabolized, peroxynitrite is generated which is a longer lasting oxidant capable of causing ischemia and hypoxia through actions on vascular endothelial cells. As the beneficial effects of NO are outweighed by the overwhelming inflammation, ischemia and hypoxia result leading to cell death and bleeding. The specific mechanisms involved in this final step are under active investigation (13).
Risk Factors
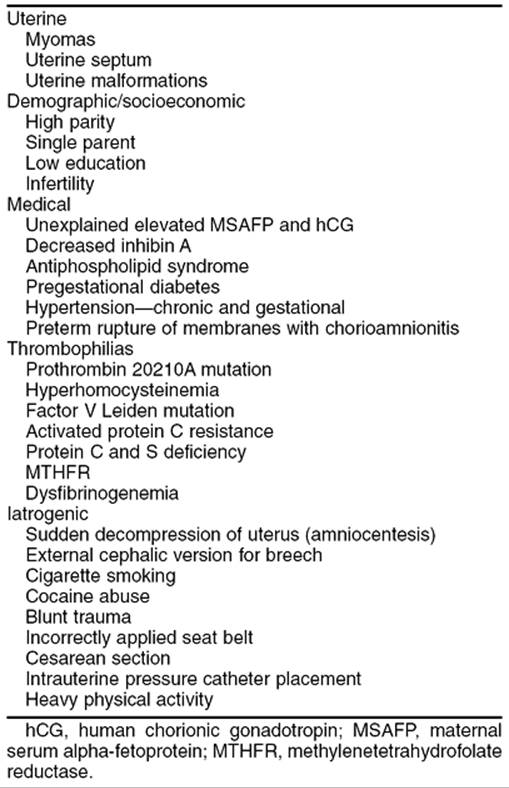
Many risk factors for placental abruptions have been studied extensively (14) (Table 20.2). These factors may be categorized. The first is socioeconomic factors with young age, primiparity, single parenthood, and low education being associated with abruption. Also included in this category would be a prior abruption with a recurrence risk ten times higher than those without a prior history. Another category includes physical factors such as blunt abdominal trauma from domestic abuse or a motor vehicle accident. A third category includes uterine defects including myomas and septums. Multiple studies have shown higher incidence of abruptions in patients with a retroplacental myoma, particularly if the myoma volume exceeded 200 cm3 and was submucosal in location (15). The fourth category is the largest and most significant and includes maternal illnesses such as thrombophilias and hypertensive diseases. Finally, a fifth category of iatrogenic causes should be included.
|
|
|
TABLE 20.2. Risk factors associated with placental abruption |
Maternal disease such as hypertension has been associated with increased risks for abruption. In many studies and in a large epidemiologic study of hypertensive women in Nova Scotia, only women with chronic hypertension with superimposed severe preeclampsia were at increased risk for abruption compared to women with chronic hypertension alone, a RR of 3.8 for parous women and 1.6 for nulliparous women. Not surprisingly, the effects of smoking and hypertension appeared to be additive, if not even higher (16).
Maternal illness due to premature rupture of the membranes leading to chorioamnionitis has been strongly correlated with the incidence of abruptions from epidemiologic studies, microbiologic, and histopathologic studies of the placentas (17). Pathologic evidence to support this includes observations that lipopolysaccharides and bacterial endotoxins are elevated in the amniotic fluid of patients with chorioamnionitis. These agents, in turn, induce the formation of superoxide or free oxygen radicals as evidenced by an increase in the nitrites and nitrates in maternal serum. These are metabolites of NO, an antioxidant that appears to be increased under these infectious conditions. Immunohistochemical studies have demonstrated increased expression of NOS and nitrotyrosine, which are markers for NO metabolism, in placentas from patients with chorioamnionitis and abruptions. Additionally, evidence for apoptotic cell death has been identified in placentas from both conditions (13). This evidence supports a strong link between chorioamnionitis and placental abruption.
Over the past decade, new risk factors have been identified in association with placental abruptions. These factors are encompassed under the umbrella of thrombophilia defects and include anticardiolipin antibodies, presence of the lupus anticoagulant, protein C, S and antithrombin III deficiencies, and the mutations such as factor V Leiden (also know as activated protein C resistance), methylenetetrahydrofolate reductase mutation, and prothrombin 20210A gene mutation, as well as the more rare congenital dysfibrinogenemia. The autoimmune antibodies, anticardiolipin antibodies, and lupus anticoagulant have been shown for many years to be associated with adverse pregnancy outcomes including placental abruption. Because these are nonspecific antibodies, it is difficult to understand their pathophysiologic role in bleeding. Protein C and protein S deficiency are genetic disorders seen with an increased risk for thrombosis. They have been implicated in preeclampsia and abruption. However, their levels may normally be decreased during pregnancy making it difficult to fully understand their role in the pathophysiology of abruption. More recently, research has focused on specific gene defects that predispose patients to coagulopathy.
Activated protein C resistance (APCR) is the most common genetic factor predisposing to thrombosis and appears to be the most common identifiable cause. This resistance is most often caused by the factor V Leiden mutation and in many cases is used synonymously, although patients can have APCR without the Leiden mutation. In this mutation, there is a nucleotide substitution of adenine for guanine that results in an amino acid substitution of arginine for glutamine. Patients who are heterozygous for this mutation have fewer manifestations of clinical disease than those who are homozygous. Because patients with this mutation have an increased tendency to form clots, they also have a higher risk for abruption due to clotting in the placenta, primarily thought to be in the decidua basalis either early in pregnancy resulting in spontaneous abortions or in the latter half of pregnancy resulting in bleeding and abruption. Furthermore, women with a hypofibrinolytic 4G/4G mutation of the plasminogen activator inhibitor 1 (PAI-1) gene, which is frequently associated with the thrombophilic factor V Leiden mutation, also have a predisposition to thrombosis. A study of women with adverse obstetric complications found that women with placental abruption were more often associated with homozygous and heterozygous factor V Leiden mutation, heterozygous G20210A prothrombin gene mutation, homocystinemia, APCR, or anticardiolipin immunoglobulin G (IgG) antibodies. However, other studies have found a weaker link and it is cautioned that these tests should not become standard and routine until larger studies further substantiate their relationship to placental abruption and other pregnancy complications. A concomitant search for therapeutic measures would further justify this type of testing of a beneficial treatment if one can be found (18).
One etiologic factor that has been widely studied in association with placental abruption is the condition known as hyperhomocysteinemia. Homocysteine is metabolized from methionine and then remethylated by an enzyme known as methylenetetrahydrofolate reductase (MTHFR) to methionine, with folate and vitamin B12 as cofactors. Mutations in the MTHFR gene, two known as C677T and A1298C, prevent this normal remethylation leading to increased levels of homocysteine. These elevated levels of homocysteine can damage vascular endothelium leading to thrombosis formation when they occur in veins or to placental abruption when they cause damage in the spiral arteries supplying flow to the placenta (19). Increased levels of homocysteine have been identified in the fasting state in patients with placental abruption and infarction (20). Hyperhomocysteinemia was found in 24% of Danish women with a history of placental abruption, intrauterine fetal demise, and fetal growth restriction (21). Increasing folate and pyridoxine intake successfully reduced the levels of homocysteine. Pathologic evaluation of the placentas from patients with hyperhomocysteinemia have identified an increase in pathologic features including acute atherosis, infarction, retroplacental hematomas, accelerated villous maturity, and vascular thrombosis (22). These abnormalities further support the fact that hyperhomocysteinemia is an etiologic factor in placental abruption. Future randomized trials with folate, vitamin B6, and vitamin B12 supplementation will be informative. For the present, patients with placental abruptions with no obvious etiology should be considered for hyperhomocysteinemia screening.
A final category of risks includes iatrogenic causes. Iatrogenic agents such as nicotine from cigarette smoking and cocaine can both cause vasoconstriction that leads to ischemia and abruption. This alteration in uteroplacental blood flow most likely causes placental lesions (i.e., infarction, oxidative stress, apoptosis, and necrosis) that can bring about disruptions in the placental–uterine interface leading to the abruption. Cigarette smoking was associated with an adjusted odds ratio for abruption ranging from 1.7 in all patients to 3.5 for African Americans, or an approximate two-fold relative risk (23). It has also been reported that smoking a pack of cigarettes per day increases the risk by approximately 40% (24). In another analysis, approximately 15% to 25% of abruptions can be attributed to smoking (23).
Other etiologic factors that are less well studied or less frequent include the iatrogenic risks from cesarean section, extramembranous placement of intrauterine pressure catheters, external version, amniocentesis, incorrect placement of the seat belt, and possibly maternal physical activity. No large case-control study has been performed to settle these associations satisfactorily.
Circumvallate Placenta
One final risk for placental abruption is the abnormal placentation known as a circumvallate placenta. It is an abnormality in placental development leading to a thickened placenta with an overall decreased surface area over the uterine wall. In this condition, the membranes of the chorion laéve do not insert at the edge of the placenta but some distance closer toward the center. This leaves a rim of fibrin and blood in various stages of clotting at the membrane and placental junction. The unprotected villi beyond the rim tend to bleed. In addition to hemorrhage, this abnormal placentation can lead to placental abruption, fetal growth restriction, preterm labor, and preterm rupture of the membranes. Typically, a second trimester ultrasound identifies such a placenta by its unusual shape with a raised placental margin that does not lay flat against the uterine wall. However, clinically observed bleeding is usually not seen until the end of the second trimester and beginning of the third trimester. Therefore, when suspicions are raised, the patient will need to be warned of the potential for bleeding and other complications and will need to be followed closely.
In summary, many risk factors have now been identified in association with placental abruption. Many are preventable, thus justifying programs that can assess an individual's risk in order to attempt modification of behaviors preconceptually or during pregnancy.
Diagnosis
The diagnosis of a suspected abruption can be made clinically. The symptoms include vaginal bleeding, uterine pain, a tetanic contraction of the uterus, and fetal heart rate abnormalities including a sinusoidal pattern in severe abruption. Bleeding occurs in approximately 80% of cases but the remaining symptoms may be present in less than 20% of cases. A definitive diagnosis can only be made retrospectively after delivery and inspection of the placenta because even ultrasound diagnosis is at best 50% sensitive because hemorrhage can be difficult to visualize. MRI can detect blood through detection of methemoglobin but it is not a practical modality for an acute problem as with an abruption.
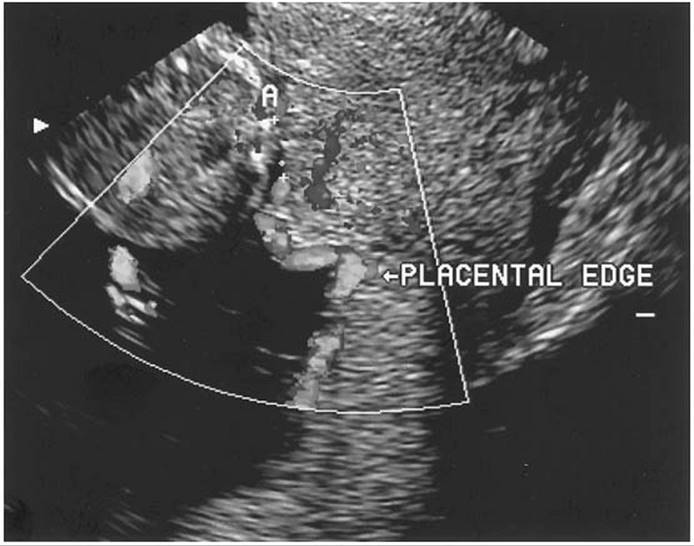
Ultrasound diagnosis is usually performed transabdominally but may be supplemented with transvaginal scanning if the bleeding placental edge is low (Fig. 20.7). Careful examination of the retroplacental area is required. False-positive identification of the normal retroplacental complex, the normal vascular complex of uterine vessels, decidua and myometrium, as an abruption has been reported. This complex appears hypoechoic on ultrasound. Acute bleeding may take on a variety of appearances from hypoechoic to isoechoic to hyperechoic and diagnosis of an abruption may be confused by this complex. The hyperechoic retroplacental complex, which is usually no more than 2 cm in thickness, demonstrates very high amounts of blood flow by color Doppler imaging that excludes its likelihood of being a clot that should demonstrate no active flow. Other hypoechoic areas such as a myoma or a uterine contraction can be mistaken for an abruption but again color Doppler can assist in the distinction because contractions demonstrate a large amount of blood flow within them and myomas demonstrate blood flow around most of their periphery and less within them. A repeat scan of a fresh bleed is often helpful since the ultrasound appearance of a clot will change with time, becoming more echogenic at 48 hours and then hypoechogenic within 1 to 2 weeks. Aside from this retroplacental complex, an abruption is also difficult to distinguish from the placenta itself. Acute hemorrhage tends to be difficult to distinguish from the placenta but with time, the clot becomes hypoechoic compared to the placenta.
|
|
|
FIG. 20.7. Transvaginal ultrasound image of a retroplacental abruption. The markers indicate the size of the clot, 3.5 × 1.0 cm. |
Pulsed-wave Doppler is not a useful tool for abruption diagnosis because the results have been inconsistent. Some studies evaluating the use of umbilical artery Doppler velocimetry have shown no abnormalities despite the presence of large retroplacental clots while others have shown elevated resistive indices and waveforms in both the umbilical and uterine arteries in patients with third trimester hemorrhage. These inconsistent findings probably reflect the heterogeneity of patients who presented with an abruption in the published studies. It also reflects the fact that none of the studies to date have had sufficiently high numbers of patients with isolated abruptions. The majority of these studies have evaluated these markers in a heterogeneous group of patients with a wide number of pregnancy complications in addition to abruptions. Uterine artery Doppler studies between 22 to 24 weeks gestation are better for predicting subsequent preeclampsia and fetal growth restriction. Therefore, undertaking the use of either of these tests to predict subsequent abruption would not be a valued undertaking at this time. However, use of these tests to detect patients at higher risk for pregnancy outcome complications would be a meaningful exercise.
Other means to diagnose or detect placental abruptions include serum biochemical tests. Two markers that have been studied are MSAFP and maternal serum human chorionic gonadotropin (hCG). Presumably, these proteins leak across the placenta when there is an abnormality in its physiologic and anatomic integrity. These markers are elevated in low-risk women with fetal or neonatal death, pregnancy-induced hypertension, placenta previa, preterm delivery, growth restriction, and perinatal complications but who did not have an a priori risk for a neural tube defect or a chromosomal abnormality. The risk of an unexplained elevated MSAFP has been associated with as high as a ten-fold increase of placental abruptions. Among women with third trimester preterm labor, elevated levels of MSAFP at an MoM of 2.0 was observed when an abruption was present with a sensitivity of 67% without bleeding and 100% with bleeding. The negative predictive value can be as high as 94% and 100%, respectively (25).
The latest serum marker to be studied in this context is inhibin A, a placental protein that is currently part of a quadruple–serum-marker screen for detection of Down syndrome in which it tends to be increased. Although preliminary, some studies suggest that inhibin A is decreased in patients with systemic lupus erythematosus who also had placental abruptions.
One other marker worth discussion is a test for fetal hemoglobin in maternal blood such as the Kleihauer-Betke test which is a stain for fetal hemoglobin. This test is routinely ordered for Rh-negative patients with a positive blood-screening test to determine how much RhoGam to administer to protect against sensitization. Studies, however, have shown that it is not a useful test to detect suspected placental abruption. This may be explained by the fact that most abruptions consist of maternal blood and most originate in the retroplacental space where there is no overlap of the fetal and maternal blood compartments as would be encountered with an intraplacental bleed where the fetal blood within villous vessels is in close proximity to maternal blood within the intervillous spaces.
Clinical Features
A patient with an abruption will typically present with painless or painful vaginal bleeding. Approximately 20% will have no external bleeding. Typical symptoms include uterine tenderness and irritability. Uterine tone may be increased and may be difficult to distinguish from uterine contractions. Patients with abruptions can have quite significant coagulopathy that develops over a very short time.
Management
The majority of abruptions are marginal abruptions and patients tend to be quite stable. Large retroplacental abruptions are usually quite symptomatic and more easily diagnosed. They also require more acute and aggressive management to prevent disastrous adverse consequences. The chance of a marginal abruption extending to a large retroplacental hematoma is unknown. The decision to hospitalize a patient with any bleeding or with a diagnosed abruption in the latter half of the second trimester or in the third trimester after fetal viability is established is an easy one. On admission, the patient should have blood drawn for a complete blood count and a type and cross or type and screen depending on the amount of bleeding. With large bleeds, 4 units of packed red blood cells should be made available. A coagulation panel consisting of a prothrombin time (PT), partial thromboplastin time (PTT), fibrin degradation product, and fibrinogen level should be drawn if there is a large amount of bleeding. When the fibrinogen level is less than 150 mg per dL, blood in a red top tube may not clot within 6 minutes or forms and lyses within 30 minutes. With mild bleeding, fetal monitoring and observation is appropriate. If significantly previable, intermittent transfusions may be necessary to maintain the hematocrit above 30.
When there is a large amount of bleeding, fetal well-being should be documented by continuous fetal monitoring, a Foley catheter should be inserted to monitor urine output, frequent maternal vital signs should be performed, and a neonatologist and anesthesiologist should be notified of a potential emergent cesarean delivery. An ultrasound should be obtained to ascertain the amount and location of bleeding. Antenatal steroid treatment should be considered if membranes are intact and the fetus is between 24 and 34 weeks gestation. For any patient with bleeding, consideration for treatment with 1 mg folic acid and vitamin B12 and B6 should be undertaken for the possible link between abruptions and hyperhomocysteinemia.
With mild bleeding, the patient will likely resolve her symptoms and should be able to be discharged once an acceptable time interval without any further bleeding has been established, usually 2 to 5 days. However, the decision on when to discharge patients who have had a large bleed is a more difficult one and there are no strict guidelines. Clearly, no decision on discharge should even be considered if the patient is symptomatic either with pain or contractions. Much of the decision will also rest on the patient's home support, whether she will be able to comply with bed rest, and it would not be unreasonable to keep a patient in the hospital until delivery if she is noncompliant or if the home environment will not allow her to undertake bed rest. Whether the patient is an inpatient or an outpatient, some fetal monitoring program should be established.
The issue of tocolytic use in a patient with a known or suspected abruption who has uterine contractions is a debatable one. Although it was formerly taught that no tocolytics should be used in patients with undiagnosed bleeding, it has now become acceptable to consider a short course of tocolytic therapy for patients with bleeding and contractions provided that the patient is stable, the abruption appears to be limited, fetal well-being is established, gestational age is preterm, and there is a controlled environment (26). Tocolytics can also be justified if they can prevent labor until a full course of antenatal steroids can be administered and 48 hours posttreatment can be achieved. Because β-mimetics can mask or blunt the patient's cardiovascular responses to volume depletion, terbutaline and ritodrine should be avoided. Calcium channel blockers may further reduce the blood pressure and nifedipine should be used with caution. The most accepted agent at the present time is magnesium sulfate. As with patients with preterm labor, these agents should be used in the acute setting and efforts should be made to discontinue them when there is a persistent period of quiescence.
Delivery can be by either vaginal delivery or cesarean section depending on the degree of bleeding, the presence or absence of active labor, and the presence or absence of fetal distress. Operative deliveries have been used liberally, in excess of 50% of cases.
When abruption leads to fetal demise, there is a very high rate of DIC. The best marker of severity is the fibrinogen level. Blood products should be administered as needed to correct the coagulopathy and then plans for delivery should be made. Induction of labor and successful vaginal delivery has been reported. Cesarean section may seriously jeopardize the mother's health in the face of a coagulopathy and should be reserved for those cases where there is fetal distress or when it appears that labor and delivery will not be successfully achieved within a reasonable amount of time, between 12 to 18 hours.
Complications
One complication of placental abruption is uteroplacental apoplexy, also known as a Couvelaire uterus. It occurs rarely but is seen with severe placental abruption in which blood extravasates from the clot into the myometrium. The appearance is that of a blue-tinted uterus. This is a very obvious visual diagnosis but biopsies have confirmed the presence of heme throughout the myometrium. This heme can lead to a very hypotonic uterus and on occasion a hysterectomy is needed in order to control the bleeding. Uterine artery embolization is likely not to be effective, although it has not been reported in the literature.
Another complication is disseminated intravascular coagulopathy marked by a fibrinogen level less than 300 mg per dL, a prolonged PT and PTT. If this occurs, large-bore intravenous lines should be placed and crystalloid and blood products should be given as quickly as possible in the form of packed red cells, fresh frozen plasma, cryoprecipitate, and platelets. A Foley catheter should be placed to monitor urine output and a central venous pressure catheter should be considered if urine output drops below 30 mL per minute.
Outcomes
Several significant adverse outcomes have been seen in association with placental abruptions. In a large epidemiologic study of placental abruption in the United States from 1995 and 1996 that incorporated over 7 millions births, the perinatal mortality rate was reported to be 119 per 1,000 births with abruption compared with 8.2 per 1,000 in all other births (27). Although there was significant mortality attributed to prematurity and growth restriction, the high perinatal death rate persisted. Term babies of normal size had a 25-fold higher mortality with an abruption than those without abruption. The pathophysiology regulating this outcome remains to be determined. In another similar epidemiologic study, abruption was also found to be associated with a very high risk for stillbirth (8.9-fold), preterm birth (39.6%), and growth restriction (14.3%). These investigators also evaluated outcomes related to the degree of abruption and found that all abruptions had a significant risk for stillbirth (RR of 31.5 for 75% abruption vs. RR of 5.5% for 25% abruption) (28).
Patients with an abruption should be counseled that there is a recurrence risk with an adjusted odds ratio of 6.4 and possibly as high as 25%. Efforts should be made to identify risk factors and to modify them. Fetal surveillance in subsequent pregnancies should be monitored starting at least two weeks before the gestational age at which the previous abruption was diagnosed in order to reduce the recurrence risk. Surveillance could consist of serial ultrasound scans for fetal growth restriction and placental bleeds in combination with fetal biophysical profiles depending on when the gestational age surveillance is initiated.
Other outcome measures such as intraventricular hemorrhage, cystic periventricular leukomalacia, and cerebral palsy have been evaluated. All are seen in higher frequency among infants delivered because of an abruption. However, many of these infants were also growth- restricted, making it difficult to discern whether these adverse outcomes were attributed to the early gestational age, the abruption, or the growth restriction. Many of these studies were also plagued by small numbers of infants studied.
Prevention
There is no established protocol for the prevention of primary or recurrent abruption. Based on the risk factors that have been identified to date, a protocol could be established to educate patients on the signs and symptoms of an abruption, on how to avoid and report domestic abuse, on how to properly use their seat belts, and on the health-related effects of cigarette smoking. A nutritional educational program can focus on how to increase the patient's folic acid and iron intake. A social service contact can be established for those at risk because of a poor home situation and those engaged in hard physical activity. Ultrasound scanning should be used to scrutinize the integrity of the uterine wall in patients with a prior cesarean section and to identify other uterine or placental abnormalities, such as the presence of a myoma or septum and the placental location in relation to it. Finally, patients with medical illnesses such as hypertension should be seen frequently to optimize their medical well-being.
SUMMARY POINTS
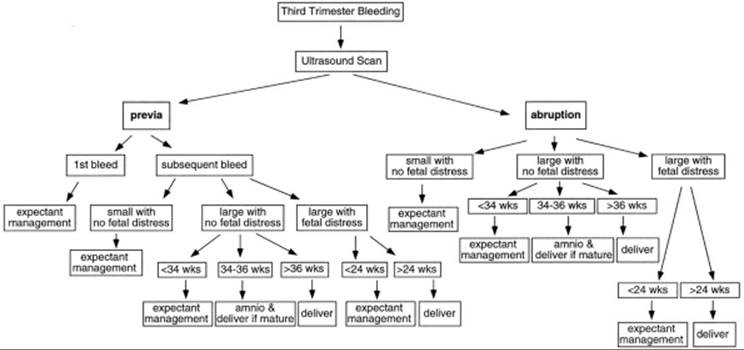
· The workup of a patient who presents with third trimester bleeding should be methodical and thorough in order to optimize the neonatal outcome. The two major etiologies, placenta previa and placental abruption, are better diagnosed today by state-of-the art imaging. Best outcomes can be obtained by following a systematic approach. The risk factors for each should be identified in order to prevent similar future events (Fig. 20.8).
|
|
|
FIG. 20.8. Flow diagram summarizing recommended clinical management for bleeding in the third trimester. Individualization is warranted and the entire clinical picture must be factored into the management plan. |
· There are two ways to classify a placenta previa: (a) By visual inspection or digital exam—marginal, partial, or complete; and (b) by transvaginal ultrasound—less than 1 cm, between 1 and 2 cm, or greater than 2 cm from the undilated internal cervical os.
· New imaging modalities including color Doppler ultrasound and MRI can improve on making the diagnosis of placenta previa, accreta, and abruption. This has minimized the need for a double setup exam in the case of a previa.
· Arterial embolization is becoming a standard means to decrease the need for a hysterectomy due to postdelivery bleeding from a previa.
· There are many risk factors for placental abruptions and the clinician should know them. When possible, the risks (i.e., cigarette smoking) should be modified to decrease the chance for abruption.
· Placenta previa and placental abruption can both lead to serious bleeding. However, placental abruption is more likely to lead to significant maternal coagulopathy.
· Expectant management is an acceptable plan for placenta previa and abruptions when the gestational age is preterm, there is no fetal distress, and the patient is stable.
· Amniocentesis should be routinely used in patients with placenta previa and abruption to document fetal lung maturity and plan delivery as soon as possible in these potentially unstable situations.
REFERENCES
1. Iyasu S, Saftlas AK, Rowley DL, et al. The epidemiology of placenta previa in the United States, 1979 through 1987. Am J Obstet Gynecol1993;168:1424–1429.
2. Oppenheimer L, Holmes P, Simpson N, et al. Diagnosis of low-lying placenta: can migration in the third trimester predict outcome? Ultrasound Obstet Gynecol 2001;18:100–102.
3. Hershkowitz R, Fraser D, Mazor M, et al. One or multiple previous cesarean sections are associated with similar increased frequency of placenta previa. Eur J Obstet Gynecol Reprod Biol 1995;62:185–188.
4. Chelmow D, Andrew DE, Baker ER. Maternal cigarette smoking and placenta previa. Obstet Gynecol 1996;87:703–706.
5. Ananth CV, Savitz DA, Bowes WA, et al. Influence of hypertensive disorders and cigarette smoking on placental abruption and uterine bleeding during pregnancy. Br J Obstet Gynaecol 1997;104:572–578.
6. Demissie K, Breckenridge MB, Joseph L, et al. Placenta previa: preponderance of male sex at birth. Am J Epidemiol 2000:152:195–196.
7. Wing DA, Paul RH, Miller LK. Management of the symptomatic placenta previa: a randomized, controlled trial of inpatient versus outpatient expectant management. Am J Obstet Gynecol 1996;175:806.
8. Crane JM, van den Hof MC, Dodds L, et al. Neonatal outcomes with placenta previa. Obstet Gynecol 1999;93:541–544.
9. Butler EL, Dashe JS, Ramus RM. Association between maternal serum alpha-fetoprotein and adverse outcomes in pregnancies with placenta previa. Obstet Gynecol 2001;97:35–38.
10. Neilson JP. Intervention for suspected placenta praevia. Cochrane Database of Systematic Reviews 2002; issue 1.
11. Chattopadhyay S, Kharif H, Sherbeeni J. Placenta previa and accreta after previous cesarean section. Eur J Obstet Gynecol Reprod Biol 1993;52:151.
12. Crane JM, van den Hof MC, Dodds L, et al. Maternal complications with placenta previa. Am J Perinatol 2000;17:101–105.
13. Nakatsuka M, Asagiri K, Kimura Y, et al. Generation of peroxynitrite and apoptosis in placenta of patients with chorioamnionitis: possible implications in placental abruption. Hum Reprod 1999;14(4):1101–1106.
14. Kyrklund-Blomberg NB, Gennser G, Cnattingius S. Placental abruption and perinatal death. Paediatr Perinat Epidemiol 2001;15:290–297.
15. Exacoustos C, Rosati P. Ultrasound diagnosis of uterine myomas and complications in pregnancy. Obstet Gynecol 1993;82:881–882.
16. Ananth CV, Savitz DA, Luther ER. Maternal cigarette smoking as a risk factor for placental abruption, placenta previa, and uterine bleeding in pregnancy. Am J Epidemiol 1996;144:881–889.
17. Ananth CV, Savitz DA, Williams MA. Placental abruption and its association with hypertension and prolonged rupture of membranes: a methodologic review and meta-analysis. Obstet Gynecol 1996;88:309–318.
18. Alfirevic Z, Roberts D, Martlew V. How strong is the association between maternal thrombophilia and adverse pregnancy outcome? A systematic review. Eur J Obstet Gynecol Reprod Biol 2002;101:6–14.
19. Eskes TK. Homocysteine and human reproduction. Clin Exp Obstet Gynencol 2000;27:157–167.
20. Goddijn-Wessel TA, Wouters MG, van de Molen EF, et al. Hyperhomocysteinemia: a risk factor for placental abruption or infarction. Eur J Obstet Gynecol Reprod Biol 1996;66:23–29.
21. De Vries JL, Dekker GA, Huijgens PC, et al. Hyperhomocysteinaemia and protein S deficiency in complicated pregnancies. Br J Obstet Gynaecol1997;104:1248–1254.
22. Khong TY, Hague WM. The placenta in maternal hyperhomocysteinaemia. Br J Obstet Gynaecol 1999;106:273–278.
23. Ananth CV, Smulian JC, Vintzileos AM. Incidence of placental abruption in relation to cigarette smoking and hypertensive disorders during pregnancy: a meta-analysis of observational studies. Obstet Gynecol 1999;93:622–628.
24. Raymond EG, Mills JL. Placental abruption. Maternal risk factors and associated fetal conditions. Acta Obstet Gynecol Scand 1993;72:633–639.
25. Bartha JL, Comino-Delgado R, Arce F. Maternal serum alpha-fetoprotein in placental abruption associated with preterm labor. Int J Gynaecol Obstet1997;56:231–236.
26. Towers CV, Pircon RA, Heppard M. Is tocolysis safe in the management of third-trimester bleeding? Am J Obstet Gynecol 1999;180:1572–1578.
27. Ananth CV and Wilcox AJ. Placental abruption and perinatal mortality in the United States. Am J Epidemiol 2001;153:332–337.
28. Ananth CV, Berkowitz GS, Savitz DA, et al. Placental abruption and adverse perinatal outcomes. JAMA 1999;282:1646–1651.