Dwight P. Cruikshank
BREECH PRESENTATION
Breech presentation, the most common obstetric malpresentation, complicates approximately 4% of deliveries.
Definitions
Breech presentation is a polar alignment of the fetus in which the fetal buttocks present at the maternal pelvic inlet. Three types are recognized: frank, incomplete, and complete.
In frank breech presentation, the fetal hips are flexed and the knees extended, so that the thighs are apposed to the abdomen and the lower legs to the chest (Fig. 21.1). The buttocks are the most dependent part of the fetus. Frank breech presentation accounts for 60% to 65% of breech presentations; it is more common at term.
|
|
|
FIG. 21.1. Fetal attitude in frank, incomplete, and complete breech presentations. |
In the incomplete breech presentation, the fetus has one or both hips incompletely flexed so that some part of the fetal lower extremity, rather than the buttocks, is the most dependent part (hence the terms single footling or double footling). This presentation accounts for 25% to 35% of breech presentations and is more common among premature fetuses.
Complete breech presentation is the least common type, accounting for about 5% of breech presentations. In this situation, the fetal hips and knees are both flexed so that the thighs are apposed to the abdomen and the legs lie on the thighs. A significant proportion of these fetuses convert to incomplete breech presentations if allowed to labor.
The position of the breech fetus is described with the fetal sacrum as the reference point; thus, it is right sacrum anterior, left sacrum posterior, left sacrum transverse, and so forth.
A spontaneous breech delivery is one in which the entire infant delivers vaginally without manual aid. In the unusual circumstance of a vaginal delivery of a singleton breech the recommended form is the assisted breech delivery, also known as partial breech extraction. In this delivery the fetus is allowed to deliver by the forces of uterine contractions and maternal bearing-down efforts until the fetal umbilicus has passed over the mother's perineum. After this, delivery of the legs, trunk, and arms are assisted manually; the head may be delivered manually or with forceps. A complete breech extraction, in which manual assistance is applied by traction in the groins or on the lower extremities before delivery of the buttocks, is contraindicated in singleton breech presentations.
Incidence
The incidence of breech presentation is closely associated with birth weight. Breech presentation accounts for 4% of births overall but occurs in 15% of deliveries of low–birth-weight (<2,500 g) infants. Furthermore, the smaller the infant, the higher the incidence of breech presentation, which rises to 30% among infants weighing 1,000 g to 1,499 g and to 40% among those weighing less than 1,000 g.
Viewed from another perspective, the association between breech presentation and low birth weight is even more striking. Only 70% of infants who present as breeches weigh more than 2,500 g; 30% weigh less than 2,500 g (compared with 5% to 6% of infants who are in vertex presentation), and 12% are of very low birth weight, weighing less than 1,500 g.
Cause
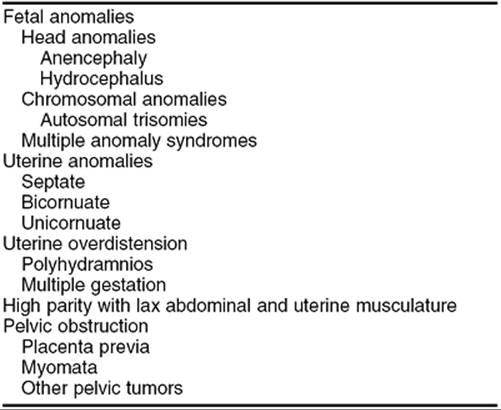
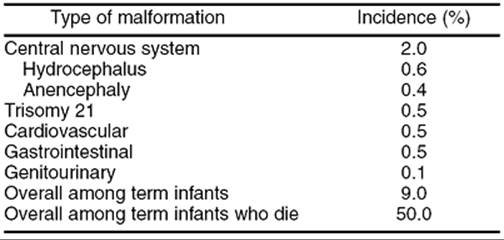
Factors that predispose to breech presentation are listed in Table 21.1. The importance of fetal anomalies cannot be overemphasized (Table 21.2). Malformations of the central nervous system complicate 1.5% to 2.0% of breech births: the incidence of hydrocephalus is ten-fold greater, and that of anencephaly two-fold to five-fold greater, than it is among infants presenting as vertex. Up to 1% of infants in breech presentation have a significant chromosomal abnormality: One in 200 has Down syndrome, and the incidence of other autosomal trisomies is increased as well. Of those infants presenting as breeches the incidence of major congenital anomalies is 17% among premature infants, 9% among term infants, and 50% among term infants who die in the perinatal period. It is prudent to keep these numbers in mind when deciding on a method of delivery for a fetus in breech presentation.
|
|
|
TABLE 21.1. Factors predisposing to breech presentation |
|
|
|
TABLE 21.2. Congenital malformations among term Infants in breech presentation |
For many years an association between cerebral palsy and breech presentation (although not vaginal breech delivery) has been assumed. As it becomes apparent that most fetal insults leading to cerebral palsy occur before term, it appears that cerebral palsy is another cause of breech presentation. In fact, among term infants, the risk of cerebral palsy is not related to presentation after correcting for fetal growth restriction.
In more than 50% of cases, no causative factor for breech presentation can be identified.
Diagnosis
On abdominal examination, the first Leopold maneuver demonstrates the fetal head in the fundus. The third maneuver reveals the softer breech over the pelvic inlet. It is useful to remember that the head narrows down to the neck before attaching to the body, whereas there is no such tapering between the buttocks and body. Auscultation of fetal heart tones usually reveals them to be most easily detected in the upper quadrants of the uterus when the fetus is in breech presentation.
The diagnosis is often made by vaginal examination. In frank or complete breech presentation, the anal orifice may be felt, with the bony prominences of the ischial tuberosities directly lateral to it. Face presentation may be difficult to distinguish from frank breech presentation, with the fetal mouth being mistaken for the anus. It is helpful to remember that the mouth is surrounded by bone, whereas the anus is not. In incomplete breech presentations palpation of the feet on vaginal examination is diagnostic. During labor, any presentation that is not clearly vertex by vaginal examination should be confirmed by ultrasound.
Perinatal Mortality
Perinatal mortality is higher in breech presentation than in vertex, being four-fold greater among term infants and two- to three-fold greater among premature infants. Much of this excess mortality is not preventable; 64% of deaths among term infants in breech presentation are due to malformations or infection. Among premature infants, malformations, infection, maternal disease, and intrauterine death before labor account for 56% of perinatal mortality, and complications of prematurity unrelated to the method of delivery account for another 11%. Thus only about one-third of perinatal deaths among breech infants are due to potentially preventable factors. These factors basically fall into two categories: Trauma and asphyxia.
Trauma to the head is a significant risk in both term and premature infants who present in the breech position, regardless of the route of delivery. Unlike the situation in vertex presentation, in which the fetal head is in the maternal pelvis for hours or days during which molding can occur, the aftercoming head of the breech fetus must come through the pelvis as is—there is no time for molding. Thus, minor variations in maternal pelvic architecture, which would be insignificant in vertex presentation, may become major risks. This problem is compounded for the infant at less than 32 weeks of gestation in whom the head is the largest part. In these circumstances the fetal body may deliver through an incompletely dilated cervix, which then entraps the head. Performance of a cesarean does not ensure a traumatic delivery of the aftercoming head. An inadequate incision or suboptimal uterine relaxation may result in head entrapment leading to significant injury to the infant and mother.
Damage to fetal muscles, soft tissue, and viscera may occur with delivery if the fetus is grasped in places other than its bony pelvis. Likewise, delivery may be associated with nerve injury if the arms are not delivered properly, especially if there are nuchal arms. Finally, trauma to the cervical spinal cord may occur with delivery of a breech fetus with hyperextension of the neck.
Asphyxia may be caused by prolapse of the umbilical cord. The incidence of cord prolapse in term fetuses in frank breech presentation is 0.4%. In complete breech presentation, the incidence is 5% to 6%, and with incomplete breech presentation the incidence may be as high as 10%. Cord prolapse in incomplete breech presentation, although an indication for prompt cesarean delivery, is often not the devastating event that it is in vertex or frank breech presentation. Because the cord is prolapsed between the fetal legs, it often is not markedly compressed during subsequent contractions.
Not all of the excess asphyxia among fetuses in breech presentation is caused by overt cord prolapse. Abnormalities of the fetal heart rate pattern during labor are four to eight times more common in fetuses in breech presentation than fetuses in vertex. An unknown percentage of this is undoubtedly due to occult cord prolapse and other forms of cord compression.
Antepartum Management
Breech presentation diagnosed before 32 weeks gestation should be managed expectantly. The fetuses of approximately two-thirds of multiparas and one-third of primigravidas who are diagnosed as being in breech presentation before 32 weeks of gestation will convert to vertex presentation spontaneously before labor. Breech presentation that persists into the late third trimester should be evaluated by an ultrasound examination for congenital anomalies.
When a breech presentation persists beyond 32 weeks of gestation, some obstetricians have recommended attempts at converting the presentation to vertex by external cephalic version (ECV). Ranney reported his experience with 860 patients managed by external version. Attempts were made to turn the fetus to vertex whenever breech presentation was found in the third trimester, and some patients had repeated versions performed. Ranney was able to lower the incidence of breech presentation at term to 0.6%, about one-sixth the expected number, and encountered no fetal trauma or death and no increase in the incidence of placental abruptions.
The results of Kasule and co-workers are less optimistic. All patients with fetuses in breech presentation after 30 weeks of gestation were prospectively randomized to either an external version group (310 patients) or a control group (330 patients). The subjects in the external version group had the procedure performed between 33 and 36 weeks of gestation. If the first attempt failed, or if the fetus reverted to breech presentation, the procedure was repeated up to three times in subsequent weekly visits. No attempts at external version were made after 36 weeks of gestation. Although their immediate success rate was 80%, 46% of fetuses spontaneously reverted to breech presentation. There were three perinatal deaths attributed to the procedure: two from abruptio placentae and one from premature labor and delivery. Most important, the incidence of breech presentation at delivery was 52% in the external version group and 51% in the control group, with 49% of fetuses in the control group converting to vertex presentation spontaneously before delivery. The authors surmised that many, if not all, of their successful external versions may have been in patients whose fetuses would have converted spontaneously had nothing been done. This hypothesis, coupled with the three perinatal deaths, led them to conclude that “there is no place for external cephalic version before 36 weeks gestation.”
The Cochrane Database of Systematic Reviews found three randomized trials of external version prior to 37 weeks of gestation. These studies showed no effect of ECV before term on the rate of breech presentation at delivery (risk ratio [RR] = 1.02; 95% confidence interval [CI] = 0.89–1.17), cesarean section (RR = 1.10; 95% CI = 0.78–1.54), low Apgar scores (RR = 0.81; 95% CI = 0.44–1.49), or perinatal mortality (RR = 1.19; 95% CI = 0.46–3.05). It was concluded that “in view of the lack of evidence of effectiveness, and reports from observational studies of unacceptably high complication rates from ECV before term, there is at present no place for ECV before term in modern obstetrics.”
If external version at term is to be attempted, it should be done in the labor and delivery suite, using monitoring of the fetal position and heart rate by ultrasound. In the past, the consensus was that no anesthesia should be used, pain being considered a reason to discontinue the attempt. As vaginal breech birth has become less of an option, however, a different approach has been proposed. This involves waiting until the pregnancy has progressed at least to 37 completed weeks of gestation, at which time epidural anesthesia is instituted. External version is attempted, and if successful, the patient has an immediate induction of labor; if unsuccessful, the patient is delivered by cesarean. In either case the epidural used for the external version attempt is used for the delivery as well. This approach seems to have merit, provided one is careful not to be overly aggressive with attempts at external version in an anesthetized patient.
Lau and associates reported a prospective case-control study of external version at term. They reported an overall success rate of 57% in nulligravidas and 84% in multiparas. They also found a rate of reversion to breech presentation of 4%. Complications included a 3.3% incidence of transient fetal bradycardia, and a 0.4% rate (one case) of what the authors called placental abruption. This particular patient had a 3-minute episode of fetal bradycardia and some vaginal spotting, although nothing suggesting abruption was found at the time of emergency cesarean. These same investigators have reported another series of 243 women who underwent attempts at external version. Regression analysis identified three independent predictors of failed version: engaged presenting part, difficulty palpating the fetal head, and nulliparity. The chance of success was 0% if all three variables were present, less than 20% if any two were present, 30% to 60% if only one was present, and 94% if none were present. Interestingly, placental location, position of the fetal spine, attitude of the fetal legs, and maternal obesity were not significant variables for predicting successful version, when the other variables were controlled.
Regarding ECV at term, the Cochrane Database of Systematic Reviews concludes that “the chance of breech birth and cesarean section may be substantially reduced by attempting ECV at term. The numbers are too small to give an accurate assessment of the risks of ECV. There is sound reason to use ECV at term, with appropriate cautions.”
It should be noted that successful external version does not necessarily reduce the cesarean rate to that found in other vertex presentations. Lau and colleagues reported a 32% cesarean rate in nulliparous patients after successful external version to vertex presentation; the rate in multiparous patients was 11%.
Active labor and ruptured membranes are contraindications to the procedure. Relative contraindications include an engaged presenting part and an estimated fetal weight of 4,000 g or more. Whether a previous cesarean contraindicates attempts at external version is uncertain, but in modern practice, delivery of breech fetus in a woman with a previous cesarean by elective repeat cesarean seems reasonable.
Management of Delivery
Term Breech Presentation
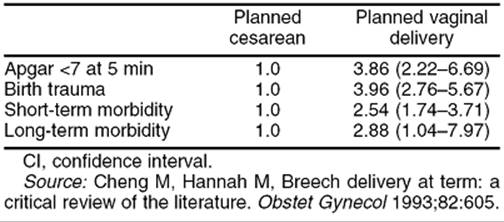
Cheng and Hannah (1993) published a critical review of the literature on singleton term breech pregnancies, reviewing all articles in the English language literature between 1966 and 1992. They found that there were only 24 studies that presented results according to the intended mode of delivery, and which presented outcome data in sufficient detail to be analyzed. Of these 24 reports, only two were randomized trials;* eight were prospective cohort studies and 14 were randomized cohort studies. Twenty-two of these studies, including both prospective trials, did not demonstrate a statistically significant difference in corrected perinatal mortality between those patients for whom a vaginal delivery was planned and those for whom a cesarean was planned. Two series did show significantly worse outcome among those for whom vaginal delivery was planned. When the authors combined all of the data, they produced a “typical odds ratio” for perinatal mortality of 3.86 (95% CI = 2.22–6.69) in the planned vaginal delivery group. Their data on low 5-minute Apgar scores, birth trauma, and short- and long-term neonatal morbidity were similar to the data on perinatal mortality, in that the majority of individual studies did not find a difference between those for whom vaginal birth was planned and those for whom cesarean was planned. When the studies were combined, however, the planned vaginal delivery group fared worse in all categories (Table 21.3). The authors of this review carefully pointed out all of the flaws in the papers they reviewed, and concluded that most of these studies were too poorly done to allow definitive conclusions. They conclude their paper by stating “the only way to obtain more definitive information regarding the effectiveness of a policy of elective cesarean versus that of a trial of labor in women with breech presentation at term is to mount an appropriately sized, randomized controlled trial. In the absence of such a trial, a policy of elective cesarean delivery appears to be a reasonable option for the woman with breech presentation at term.”
|
|
|
TABLE 21.3. Neonatal morbidity, planned vaginal delivery vs. cesarean. Typical odds ratio and 95% CI |
In order to answer the question of the optimal route of delivery of the term breech, Hannah and associates organized the Term Breech Trial, a randomized trial of planned cesarean delivery versus planned vaginal birth for term singleton frank and complete breech infants. This trial was carried out between January 1997 and April 2000 in 121 hospitals in 26 countries. Sixteen were industrialized nations with low perinatal mortality rates, and ten were underdeveloped countries with high perinatal mortality rates. The results of this trial were published in 2000, and will be presented here in considerable detail because of the uniqueness and importance of the study.
Patients were eligible for the trial if they were at 37 or more weeks of gestation with a singleton frank or complete breech. Women were excluded for clinical or radiographic evidence of pelvic inadequacy (91% of subjects in both groups had only clinical evaluation of the pelvis), if the fetus was estimated to weigh more than 4,000 g either clinically or by ultrasonography (60% of subjects had sonography, 40% had clinical evaluations of fetal weight), if hyperextension of the fetal neck was felt to be present by clinical exam (31% of subjects) or ultrasonography (69% of subjects), if there was a contraindication to labor or vaginal delivery, or if there were fetal malformations incompatible with life or predisposing to mechanical problems with vaginal delivery. The labor protocol permitted induction and augmentation of labor for usual indications, and called for either continuous electronic fetal monitoring or intermittent auscultation every 15 minutes in the first stage of labor and every 5 minutes in the second. Adequate labor progress was defined as a rate of cervical dilation of ≥0.5 cm per hour in the active phase, descent of the breech to the pelvic floor within 2 hours of the second stage, and imminent delivery within 1 hour of active pushing. The method of vaginal delivery was spontaneous or assisted; total breech extraction was not permitted. Most importantly, all vaginal deliveries were to be attended by a clinician experienced with vaginal breech delivery (self-defined with confirmation by the individual's department head).
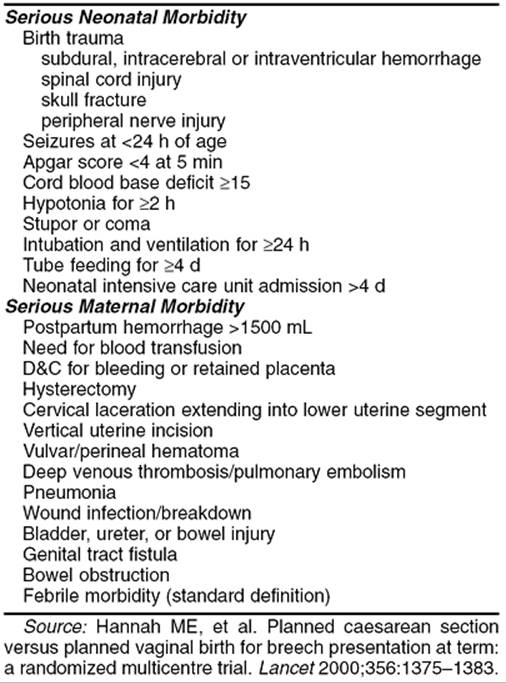
The primary outcomes measured were perinatal/neonatal morality and serious neonatal morbidity. The secondary outcomes measured were maternal mortality and serious maternal morbidity (Table 21.4). Power analysis prior to the study calculated a required randomization of 2,800 subjects. An interim analysis of the first 1,600 births revealed a clear advantage for planned cesarean, and therefore recruitment was stopped at 2,088 women (488 additional women had been enrolled while the interim analysis of the first 1,600 was in progress). In the final analysis, the rate of perinatal mortality and morbidity was 1.6% in the planned cesarean group and 5.0% in the planned vaginal delivery group (RR = 0.33; 95% CI = 0.19–0.56; P < .0001). Considering perinatal mortality alone, the respective rates for cesarean and vaginal delivery were 0.3% and 1.3% (RR = 0.23; 95% CI = 0.07–0.81; P < .01). Similar data for neonatal morbidity alone were 1.4% and 3.8% (RR = 0.36; 95% CI = 0.19–0.65; P < .0003). For every subcategory of neonatal morbidity, infants in the planned cesarean group fared significantly better than those in the planned vaginal delivery group. Most interestingly, the improvement in neonatal outcome with planned cesarean was better in the countries with already low perinatal mortality rates. The authors determined that in industrialized nations, one case of neonatal mortality or serious morbidity could be avoided for every seven additional cesareans, whereas in underdeveloped countries, as many as 39 additional cesareans might be needed to avoid one dead or compromised baby. For the entire population studied, the number of additional cesareans needed to avoid one dead or seriously injured baby was 14. The authors' finding of a significant advantage for planned cesarean birth was maintained even after excluding labors which were prolonged, induced, or augmented and after correcting for whether or not epidural anesthesia was used. Finally, and of equal importance, the authors found no differences between the groups in terms of maternal mortality or serious morbidity; there were no differences in maternal morbidity whether the various morbid conditions were totaled or considered separately.
|
|
|
TABLE 21.4. Primary and secondary outcomes in the Term Breech Trial |
The Cochrane Database of Systematic Reviews includes a systematic review of the three randomized, controlled trials of planned cesarean versus planned vaginal delivery for breech presentation (Collea and colleagues, 1980; Gimovsky and colleagues, 1983; Hannah and colleagues, 2000) and concludes “policy of planned cesarean section for term breech presentation is associated with a large decrease in perinatal/neonatal mortality, and neonatal morbidity, and a modest increase in maternal morbidity (RR = 1.29; 95% CI = 1.03–1.61). Overall the results clearly favor a policy of planned cesarean section.”
Based on this information the American College of Obstetricians and Gynecologists' Committee on Obstetric Practice issued Committee Opinion #265 in December 2001, concluding, “patients with a persistent breech presentation at term in a singleton gestation should undergo a planned cesarean delivery.” It is important to point out that they further stated “a planned cesarean delivery does not apply to patients presenting in advanced labor with a fetus in breech presentation in which delivery is likely to be imminent, or to patients whose second twin is in a nonvertex presentation” (see Chapter 14).
There are many points on which one can criticize the Term Breech Trial. It is not a perfect study, but it is a good study. It brings real evidence to bear on the question of breech delivery, and given today's medicolegal and social climate, it may be the best evidence we are ever going to have. Two other points are pertinent. First, almost no obstetrician completing residency in the past 10 years has the training or experience to be skillful at vaginal breech delivery, and the cadre of obstetricians capable of imparting these skills is retiring or giving up obstetrics. Second, the argument that vaginal delivery is significantly safer than cesarean for the mother is becoming more and more difficult to prove. A growing number of studies, including the Term Breech Trial, have shown that maternal morbidity and mortality is as good or better with planned cesarean delivery as with vaginal birth. On the other hand, emergency cesarean or cesarean after a trial of labor is clearly more morbid than either elective cesarean or vaginal delivery. In nearly all recent series, including those in the Cochrane Database, 40% to 45% of women given a trial of labor for breech presentation eventually were delivered by cesarean, which greatly increases the overall risk of morbidity and mortality in the total group for whom vaginal breech delivery is planned.
Two fairly large retrospective studies of term breech delivery from Sweden confirm the findings of the Term Breech Trial. Herbst and Thorngren-Jerneck published a series of 1,050 term singleton breeches delivered at a single institution between 1988 and 2000. A planned vaginal delivery group of 699 women was compared to a planned cesarean group of 327. Acidemia at birth, low 5-minute Apgar scores, neonatal intensive care unit admissions, and the rate of neonatal neurologic morbidity were all significantly greater among infants in the planned vaginal delivery group.
Roman and associates studied 15,818 term singleton breeches delivered in Sweden between 1987 and 1993. A summary of their neonatal data is shown in Table 21.5 and demonstrates a clear advantage for cesarean delivery. Of significant importance, the authors found the same rates of maternal morbidity for elective cesarean (1.7%) and vaginal delivery (1.8%). The maternal morbidity rate for emergency cesarean was 2.8%.
|
|
|
TABLE 21.5. Neonatal outcome, cesarean vs. vaginal breech delivery (OR and 95% CI) |
Given the data from these studies I believe it is time to consider the matter settled. Unless and until another large, randomized, controlled trial reveals different findings from what is known from these studies, the route of delivery for the term singleton breech should be cesarean.
Premature Breech Presentation
Almost no randomized prospective data are published regarding delivery of the premature infant in breech presentation. Penn and co-workers attempted a multicenter, randomized, controlled trial in 26 hospitals in England, in an effort to determine the optimal mode of delivery for breech infants at gestational ages between 26 and 32 weeks. After 17 months of attempting to enroll patients the study was abandoned because only 13 women from 6 hospitals had been recruited. The authors stated, “The low accrual rate was due to clinicians' reluctance to randomize eligible women.” Eller and VanDorsten polled the Maternal-Fetal Medicine Units network and found 7 of 11 centers willing to do a randomized controlled trial comparing cesarean to vaginal birth for breech infants between 24 to 28 weeks of gestation; because of small numbers they calculated this study would require at least 10 years. No center in the network was even willing to study breech birth in pregnancies greater than 28 weeks of gestation. Therefore, management decisions regarding the premature breech must be made based on retrospective data, which suffer from serious shortcomings. These data, however, all indicate that cesarean delivery is preferable for the premature breech.
The Effect of Parity
To separate primigravidas whose fetuses are in breech presentation as a group needing cesarean delivery is fallacious for two reasons: First, there are no data to suggest that primigravidas are at more risk than parous women for fetal injury, cord prolapse, difficult vaginal delivery, or perinatal death. Second, this philosophy implies that a parous woman in labor with a fetus in breech presentation is not at very high risk. The parous woman is at no less risk than the multiparous woman because a subsequent fetus may be larger than previous infants delivered, and because the pelvis may be adequate for vertex presentation but not for the unmolded head of a breech fetus.
Extension of the Fetal Neck
Ballas and Toaff demonstrated that when the fetal neck is hyperextended to an angle of greater than 90 degrees (Fig. 21.2), vaginal delivery is associated with a 70% incidence of fetal spinal cord transections. This complication is avoided by cesarean delivery if generous abdominal and uterine incisions are employed, and the head is delivered slowly while attempts are made to flex the neck.
|
|
|
FIG. 21.2. Hyperextension of the fetal neck. |
Management of Vaginal Delivery
Occasionally a patient will arrive at the hospital in the process of delivering a breech infant. In such circumstances, a vaginal delivery is probably less traumatic to both infant and mother than a rushed cesarean under suboptimal emergency conditions. The Cochrane Review anticipates this problem without providing a solution, stating “one problem with a policy of routine cesarean section for breech presentation at term is that in time the skills of breech delivery will be lost, placing women who deliver before cesarean section can be carried out at increased risk.” To prepare as much as possible for such circumstances, given the paucity of actual experience with vaginal breech delivery, all obstetricians should frequently review the principles of vaginal breech delivery.
Vaginal delivery of a fetus in breech presentation requires the attendance of at least an obstetrician and an anesthesiologist. It is preferable to have a pediatrician in attendance as well.
The fetal monitor should be taken to the delivery room, and monitoring should be continued until one is committed to a vaginal delivery. Such a commitment occurs when the fetal umbilicus passes over the mother's perineum, at which time the fetal head is in the maternal pelvis. Traction on the fetus before that point constitutes a total breech extraction and should be avoided.
Once the fetal umbilicus passes over the maternal perineum, a loop of cord 4 to 6 inches in length should be brought down to prevent subsequent excessive traction on the cord. The legs may then be delivered by flexing the knees and sweeping the legs out from in front of the fetus. A towel is placed around the fetal pelvis, which is then grasped, and downward traction is applied until the fetal scapulae pass under the maternal symphysis. Then the fetal body is rotated so that the shoulders are in an anteroposterior position, and the anterior arm is flexed and swept out under the symphysis. The fetus is then rotated 180 degrees in the direction that will keep the fetal back toward the maternal symphysis, and the other arm is swept out in a similar manner. It is important during delivery of a breech that the fetus not be allowed to assume a position with the fetal face or abdomen toward the maternal symphysis.
If the breech infant is delivering so rapidly that cesarean birth is not feasible, the aftercoming head usually delivers spontaneously. Should this not occur, delivery of the fetal head with Piper forceps will be necessary. An assistant must support the fetal body during application of these forceps (Fig. 21.3). The temptation to elevate the fetal body to provide better visualization must be resisted, because this maneuver hyperextends the neck. Rather, the fetal body should be supported parallel to the floor, and the operator should drop to the knee for application of the forceps. The application is pelvic rather than cephalic, with the forceps being applied to the lateral aspects of the maternal pelvis, not wandered around from the posterior using landmarks on the fetal head, as one would do in vertex presentation. Controlled delivery of the fetal head is then accomplished, with suctioning of the fetal airway as soon as the mouth passes over the perineum.
|
|
|
FIG. 21.3. Breech delivery with Piper forceps to the aftercoming head. Note that the infant's body is being supported parallel to the floor. |
A generous episiotomy is necessary for any vaginal breech birth. For the term-sized infant, a mediolateral episiotomy is appropriate.
Management of Cesarean Delivery
Abdominal delivery does not guarantee a traumatic birth of the fetus in breech presentation. Just as in vaginal delivery, it is important to grasp the fetal bony pelvis rather than soft tissue during extraction. The most serious complication is head entrapment by the uterus contracting down around the neck after delivery of the body. Some physicians have advocated a vertical uterine incision so that it may be extended should this occur. This may be the best choice for the premature fetus accompanied by a poorly developed lower uterine segment. Because such an incision compromises future childbearing, the obstetrician should perform a low transverse cervical incision for the term fetus or the premature fetus when labor has resulted in a well-developed lower segment. Such an incision can be extended in a J-shaped (rather than a T-shaped) manner, if necessary. A technique that may obviate the need for this in the face of head entrapment is general anesthesia with an agent that rapidly relaxes the uterus. The anesthesiologist should be alerted that this might become necessary even if the cesarean is begun under regional anesthesia.
FACE PRESENTATION
In face presentation, the fetal neck is hyperextended so that the occiput touches the back. The presenting part is that part of the fetal face between the orbital ridges and the chin (Fig. 21.4). The incidence is approximately one in 550 births.
|
|
|
FIG. 21.4. Face presentation. |
Cause
Proposed causative factors include anencephaly, high parity, contracted pelvis, large infant, small infant, and nuchal cord. It is interesting to note that, in the majority of studies, one of the larger categories is that in which no causative factor can be identified; this varies from 2% to 97%, with an average frequency of 38%.
Anencephalic fetuses frequently present by the face if the fetal presentation is cephalic. However, because the course and mechanism of labor, management of delivery, and perinatal outcome are entirely different in this situation, these cases should be excluded from consideration of face presentation. The association between face presentation and anencephaly is important to remember, however, because when face presentation is suspected clinically, ultrasound studies are indicated to rule out this anomaly.
Most series demonstrate an association between high parity and face presentation; whether this relation is causal is not clear. The average reported incidence of contracted pelves in series of face presentations is 15%. In reality, the incidence is probably much lower, because in most series only those patients with arrested labor were studied radiographically. Contracted pelvis or cephalopelvic disproportion is probably diagnosed clinically with excessive frequency in face presentation, because the extended head feels larger on abdominal palpation and because the head is often floating at the onset of labor.
However, if large series of radiographically diagnosed pelvic contraction are examined, it is rare to find a case of face presentation, none being reported in three series of radiographically diagnosed pelvic contraction totaling more than 700 patients. The weight of evidence seems to indicate that pelvic contraction is not of causative significance in face presentation.
Some authors associate face presentation with large infants, on the assumption that cephalopelvic disproportion may result from excessive fetal size in spite of a normal pelvis. The argument that large infants cause cephalopelvic disproportion, and thus face presentation, is weakened by the high proportion of vaginal deliveries in most series of face presentations. Furthermore, the average incidence of large infants (variously defined) in series of face presentations is 12%, not significantly different from that in the general obstetric population.
Many series have demonstrated an increased proportion of low-birth-weight infants among face presentations and ascribed causative significance to prematurity, although other studies have found no excess of low–birth-weight infants. Part of the discrepancy results from the inclusion of anencephalic fetuses in many series—fetuses that usually are small for gestational age. The average incidence of low birth weight is 11% in those series of face presentation in which it is possible to exclude anencephalics; this is not significantly different from the incidence of low birth weight in the general population. Thus it is difficult to conclude that low birth weight or prematurity are causative factors in face presentation.
Nuchal cord occurs in approximately 25% of cephalic deliveries. The average incidence of nuchal cord in face presentation is 10%. Nuchal cord is not a cause of face presentation.
Of all the proposed causative factors in face presentation, there is no unanimity of opinion regarding their significance, and as reported by Cruikshank and Cruikshank, none can withstand careful scrutiny. There does seem to be an association between face presentation and high parity, but 34% of face presentations occur in primigravidas. All of the postulated causes presume that face presentation develops after the onset of labor. Cases of face presentation that occur before labor are called primary and are thought to be due to increased tone in the extensor muscles of the fetal neck. The usual attitude of the fetal neck is flexion caused by greater tone in the flexor muscles, but occasionally infants are seen in whom the extensors predominate. In addition to face presentation, hyperextension of the neck occurs in transverse lie (i.e., “flying fetus”) and in breech presentation; in fact, up to 5% of breech fetuses have hyperextended necks.
To ascertain the true incidence of primary face presentation, it is necessary to examine large series of x-ray films obtained before labor. In three such series, seven primary face presentations were found among 1,762 patients, an incidence of one face presentation in 251 cases, which is more than twice the reported incidence of face presentation at delivery. These data, coupled with the uncertainties surrounding the proposed causative factors, make it most likely that all face presentations are primary and intrinsic to the fetus and that there are no significant causative factors. The preponderance of multiparas in series of face presentation is compatible with this theory. Increased extensor muscle tone cannot cause extension of the neck if the head is fixed in the pelvis; thus, face presentation is less likely to occur during the last 1 to 2 weeks of pregnancy in a primigravida with an engaged presenting part than in a multipara in whom the head often is not engaged until after the onset of labor.
Diagnosis
The diagnosis usually is made by vaginal examination during labor followed by ultrasound studies. Face presentation is rarely diagnosed prior to the onset of labor, with 35% of cases being diagnosed in the first stage, 27% in the second stage, and 35% at the time of delivery. At the time of diagnosis, 60% of face presentations are mentum (chin) anterior (MA), 15% are mentum transverse (MT), and 25% are mentum posterior (MP).
Mechanism and Course of Labor
In face presentation, the presenting diameter is the tracheloparietal (trachelobregmatic), which is 0.7 cm longer than the presenting diameter in vertex presentation (the suboccipitobregmatic). Internal rotation in face presentation occurs between the ischial spines and the ischial tuberosities, lower than in vertex presentation. After internal rotation to MA has placed the fetal chin under the maternal symphysis, delivery occurs by flexion of the fetal neck. It is important to remember that in face presentation, the distance from the leading edge to the largest presenting diameter is greater than that in vertex presentation. Thus, engagement of the presenting part probably has not occurred until the face is at a +2 station.
Safe vaginal delivery of a term-sized, persistent MP is impossible for two reasons: the short fetal neck cannot span the full length of the maternal sacrum so the fetal head and shoulders must enter the maternal pelvis at the same time, and even if this should occur, the persistent MP would have to deliver under the symphysis by extension, but the neck is already maximally extended. Many MPs will spontaneously rotate and convert to MA; the average reported rate being 35%. This may be an artificially low value because, as pointed out earlier, rotation does not occur until the head is well down in the pelvis. Surgical intervention before that point would make the incidence of spontaneous rotation seem lower. In fact, some series report spontaneous rotation rates of 50% to 65%. When the face is MT at the time of diagnosis during labor, spontaneous rotation to MA usually occurs.
Most patients with face presentations have durations of the first stage of labor similar to those of patients with vertex presentations, although there may be some prolongation in MP presentations. Likewise, the length of the second stage is similar to, or only slightly longer than, that in vertex presentation.
Management
The average reported incidence of spontaneous or elective low forceps delivery in face presentation is 72% (range, 40% to 90%). The average rate of cesarean delivery is 15%, and in only two series was it greater than 29%. In older series, up to 12% of face presentations were delivered by various operative vaginal procedures, including midforceps rotation, version and extraction, and manual conversion of face to vertex (Thorn maneuver). These procedures are associated with high perinatal mortality and maternal morbidity, and there is no place for them in the modern management of face presentation.
Face presentation alone is not a contraindication to oxytocin stimulation of labor, and it can be done for the same reasons and with the same precautions as in vertex presentation. Likewise, outlet forceps delivery in MA presentation can be accomplished using the same criteria one would use in vertex presentation, but midforceps delivery in face presentation should be abandoned. Because of the altered diameters of the presenting part, if the face is not bulging the perineum, any forceps delivery is probably a midforceps operation and should not be attempted.
The old adage “if a face is progressing, leave it alone” is still valid. This applies to MT and MP presentations as well as to MA, because of the likelihood that these presentations will convert to MA. Rotation may not occur, however, until the presenting part is on the pelvic floor. In any face presentation, as in vertex presentation, if progress in dilation and descent ceases despite adequate contractions, delivery should be accomplished by cesarean. Conversely, as long as dilation and descent continue, management should be expectant.
The only series using fetal monitoring extensively in the management of face presentation reported variable decelerations in 59% of 29 infants, severe variables in 29%, and late decelerations in 24%. Only 14% of patients in the study (4 of 29) had no fetal heart rate abnormality. It seems plausible that the increased incidence of fetal heart rate abnormalities is due in part to abnormal pressure on the extended head, neck, or eyes, similar to the mechanism of heart rate abnormalities described in occiput posterior presentations. Therefore, face presentation is an indication for electronic fetal monitoring.
BROW PRESENTATION
In brow presentation, the fetal neck is midway between flexion and hyperextension, and the presenting part is that portion of the head between the orbital ridges and the anterior fontanelle. Brow presentation is less common than face; the reported incidence is approximately one in 1,400 births.
Cause
As in face presentation, numerous factors have been proposed as causative in brow presentation. Most series report a few cases of brow presentation associated with placenta previa, polyhydramnios, uterine anomalies, and fetal malformations, but these are no longer seriously proposed as causes of brow presentation. Likewise, the reported incidence of nuchal cord in brow presentation is lower than that in the general obstetric population, and nuchal cord seems to be related to brow presentation only by coincidence. The average incidence of low birth weight among brow presentations is 13%; this does not seem to be etiologically significant. Most data suggest however that cephalopelvic disproportion is more commonly associated with brow presentation than with face presentation.
Many authors believe that brow presentation, like face presentation, is nearly always primary (i.e., caused solely by factors intrinsic to the fetus). Others believe that brow is an unstable or transitional presentation, representing a head in the process of converting from vertex to face presentation or vice versa. If this is true, and if, as proposed, all face presentations are primary, then all brow presentations must likewise be primary. If so, how can the apparent association between brow presentation and cephalopelvic disproportion be explained? Two factors seem relevant:
1. “Relative” cephalopelvic disproportion is more likely to occur in brow presentation because the presenting diameters of the fetal head are greater than in face or vertex presentation (see “Mechanism and Course of Labor” below).
2. Persistent brow presentation probably selects for patients with smaller pelves, because in patients with larger pelves, the brow may convert to face or to vertex before being recognized.
Diagnosis
The diagnosis is nearly always made by vaginal examination or sonographic studies, or both. Most cases are diagnosed in labor, with approximately one-half diagnosed during the second stage. If labor is progressing, the diagnosis is often missed until late in the second stage of labor.
Mechanism and Course of Labor
When the fetal head engages as a brow presentation, there are three possible mechanisms of labor, depending on whether the brow converts to a face, converts to a vertex, or persists as a brow. Spontaneous conversion to face or vertex occurs in approximately 50% of cases, with 30% converting to face and 20% to vertex. However, in those series in which the brow presentation was diagnosed early in labor, spontaneous conversion rates of 67% to 75% are reported. In fact, many occiput posterior presentations probably enter the pelvis as brows but are never diagnosed as such.
Regardless of the eventual outcome, the brow usually engages transversely at the pelvic brim. The engaging diameter is the mentoparietal, which is about 1.5 cm longer than the engaging diameter in vertex presentation and 0.8 cm longer than that in face presentation.
Most would agree that there is no mechanism of labor for a term-sized, persistent brow under most circumstances, and therefore vaginal delivery is impossible. Vaginal delivery however can occur if the fetus is quite small or the pelvis very large.
Most series report a definite prolongation of labor with brow presentation, but the duration of labor in those patients who eventually convert to face or vertex is no different from the duration of labor with vertex presentation. It would seem that those cases destined to convert to face or vertex and deliver spontaneously have normal to slightly prolonged labor, whereas those destined to persist as brows often have very prolonged labors unless timely intervention is undertaken.
Management
The best recommendation for management of brow presentations is the same as that for face presentations. If dilation and descent are progressing normally, expectant management is best. If progress ceases, delivery should be by cesarean. The association of cephalopelvic disproportion with brow presentation may contraindicate the use of oxytocin to stimulate labor. Forceps deliveries are acceptable if the brow converts to MA face or vertex. Persistent brow presentations, once progress in labor has ceased, require delivery by cesarean, and all forceps operations are contraindicated.
In assessing whether progress in labor has stopped, it is important to remember that if the fetus becomes arrested at the pelvic brim, tremendous caput succedaneum may form over the brow, giving a false impression of descent of the head.
SHOULDER PRESENTATION (TRANSVERSE LIE)
When the long axis of the fetus lies perpendicular to that of the mother, the condition is termed a shoulder presentation or transverse lie. This malpresentation complicates one in 300 births.
Definitions
In transverse lie, the fetal head lies in one maternal iliac fossa and the buttocks in the other. A better term for this would be transverse presentation, but this term is avoided because it is often confused with transverse position of vertex presentation. Because the fetal shoulder usually lies over the pelvic inlet, the formal term is shoulder presentation, which should be considered synonymous with transverse lie. The fetal position is described with the fetal acromion used as a reference point and is termed left or right acromion, according to which side of the mother the fetal shoulder is directed. Because the fetal back may be directed anteriorly, posteriorly, superiorly, or inferiorly, the additional qualifying terms dorsum superior, dorsum anterior, and so on are used as well. Thus, a fetus with its head on the mother's left and its back toward the mother's head would be described as left acromion dorsum superior.
If one fetal pole lies in a maternal iliac fossa and the other pole lies in the opposite upper quadrant of the uterus, the lie is said to be oblique or unstable.
Cause
The most common causative factors are high parity with lax abdominal wall and uterine musculature, and conditions in which the fetus is small in relation to the volume of the uterus (i.e., prematurity and polyhydramnios). Shoulder presentation may also be caused by anything that prevents descent of a fetal pole into the maternal pelvis, such as pelvic contraction, placenta previa, lower uterine segment myoma, or an ovarian tumor in the cul-de-sac. These conditions should be kept in mind for any patient who presents with a transverse lie, but especially in the patient of low parity who has this malpresentation at or near term.
Diagnosis
The diagnosis usually can be made by physical examination of the maternal abdomen, with the fetal head and buttocks palpable in the iliac fossae and no fetal pole at the pelvic inlet. A very high or unreachable presenting part on vaginal examination suggests transverse lie. All such findings should be confirmed by ultrasound.
Mechanism of Labor
The tiny fetus in transverse lie may deliver by the mechanism of conduplicato corpore, in which the fetal body doubles up on itself and the fetal head and buttocks enter the maternal pelvis simultaneously. This is often associated with rupture of fetal abdominal viscera.
If the fetal weight is greater than about 800 g, there is no mechanism of labor. Uterine contractions will wedge the fetal shoulder into the maternal pelvis, and eventually the membranes will rupture and the fetal arm will prolapse into the vagina. Such a condition is termed a neglected transverse lie. If labor is permitted to continue, there will be progressive thinning of the lower uterine segment, a Bandl retraction ring will form, the uterus will rupture, and eventually both the fetus and the mother will die.
Management
Shoulder presentations diagnosed before term should be managed expectantly, because most will convert to polar presentations before labor. If the patient is not at term but the cervix is significantly dilated (> 3 cm), hospitalization and bed rest should be considered as the incidence of cord prolapse in such a patient is 10% to 15% should rupture of membranes occur.
If the patient is at term (37 or more completed weeks gestation), external version may be attempted with the same techniques and precautions as described for breech presentation. Induction of labor may be undertaken immediately if the version is successful and the cervix favorable. External version may also be attempted in early labor; provided the membranes are intact and no fetal part has entered the pelvis. Before any version attempt, ultrasound should be used to rule out placenta previa and pelvic masses.
If the patient is in active labor or has ruptured membranes, and the fetus is of a gestational age to be considered viable, delivery must be by cesarean. Because of exceedingly high morbidity and mortality for both mother and fetus, there is no role for internal version and extraction in the management of transverse lie in singleton gestation. Because the lower uterine segment may be poorly developed, vertical uterine incisions are often necessary. If, however, the fetus can be manipulated to a polar presentation after opening the abdomen but before entering the uterus, a low transverse incision may be performed. This usually is possible only if the membranes are still intact.
The patient with a neglected transverse lie is an obstetric emergency. Usually she is septic, and often the fetus is dead. If the uterus is still intact, it is exceedingly thin. Some patients will be completely dilated on arrival at the hospital, but the temptation to try vaginal maneuvers such as internal version must be resisted as this will often result in uterine rupture and may lead to maternal death. Such patients should have basic laboratory studies, coagulation indices, and blood cultures obtained. Rapid intravenous hydration and antibiotic therapy should be instituted, type-specific blood should be available, and the patient should be taken promptly to the operating room for cesarean delivery. Cesarean hysterectomy is often the best procedure for such patients, especially if the uterus has ruptured or is grossly infected. In the past, various vaginal fetal destructive procedures were described for treating the neglected transverse lie with a dead fetus. Given that obstetricians today have almost no training in such procedures, they should be abandoned in favor of cesarean delivery, even in the face of a dead fetus.
COMPOUND PRESENTATION
A compound presentation occurs whenever some part of a fetal extremity is prolapsed alongside the presenting part. By far the most common type is vertex/hand or vertex/arm, in which some part of the upper extremity is alongside the head. Much less common types are breech/arm and vertex/foot. The reported incidences range between one in 400 and one in 1200 births.
Cause
Situations in which the presenting part fills the pelvis poorly predispose to compound presentation. The most obvious of these is prematurity, which is associated with most compound presentations. In fact, the incidence of this complication among infants who weigh more than 1,500 g is only one in 1,600 births.
Diagnosis
The diagnosis almost invariably is made by vaginal examination and generally is made late in labor. At least 50% of these malpresentations are diagnosed in the second stage of labor. Whenever a fetal hand or arm is palpated on vaginal examination, the examiner must be certain that the fetal head is in the pelvis as well, before concluding that the presentation is compound. If the head is not easily palpated in the pelvis in such circumstances, most likely the diagnosis is shoulder presentation with a prolapsed arm, a much more serious and urgent obstetric condition.
Management
Management of vertex/arm and vertex/hand presentations should be expectant. One of three outcomes will occur:
· the prolapsed part will withdraw back up into the uterus as labor progresses
· the baby will deliver with the arm or hand alongside the head
· progress in labor will cease, in which case cesarean delivery is indicated.
The reported incidence of cord prolapse in compound presentation is 10% to 20%, but many of these are related to attempts to replace the prolapsed arm into the uterus, which often necessitates upward displacement of the fetal head. For this reason, attempts at replacement of the prolapsed part in compound presentation should be avoided.
Because of the increased incidence of cord prolapse, electronic fetal monitoring should be used in these situations. Vertex/arm and vertex/hand presentations are not indications for cesarean delivery in and of themselves. Indications for cesarean delivery in such circumstances include failure to progress in labor, cord prolapse, and fetal distress.
Cases of breech/arm presentation should be managed as any other breech presentation would be managed. Cases of vertex/foot presentation are rare, but those few reported cases have a perinatal mortality two to three times that of other compound presentations, and are best managed by cesarean delivery. In essence, these are variants of shoulder presentation.
There is no role for internal version and extraction in the modern management of compound presentation, although this was commonly done in the past.
UMBILICAL CORD COMPLICATIONS
The mean length of the umbilical cord at term is 55 to 60 cm, and the normal range (5th to 95th percentile) is 35 to 80 cm. The longest umbilical cord reported measured 129 cm. The length of the cord is related to fetal activity in the first two trimesters; there is little change in the length of the cord after 28 weeks of gestation. At term, mean cord length is slightly (1.6 cm) but significantly longer in male fetuses compared with females, and is 4.5 cm greater in vertex infants compared with breech. There is no correlation between cord length and either fetal or placental weight.
Cord Prolapse
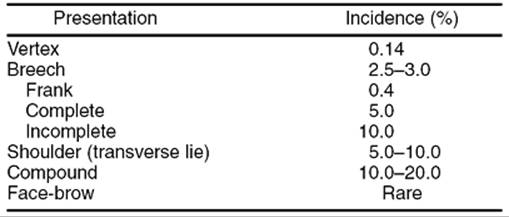
The reported incidence of prolapse of the umbilical cord varies between 0.2% and 0.6% of births. Cord prolapse almost never occurs with cords shorter than 35 cm; the incidence is 0.4% with normal-length cords (35–80 cm) and 4% to 6% with cords longer than 80 cm. Besides excessive cord length, other causative factors include malpresentation in approximately 50% of cases, low birth weight (<2,500 g) in 30% to 50% of cases, grand multiparity (more than five pregnancies) in 10% of cases, multiple gestation in 10% and obstetric manipulation, including artificial rupture of membranes, in 10% to 15%. Table 21.6shows the association between cord prolapse and malpresentation, especially with nonfrank breech, compound, and shoulder presentations. Nearly 50% of cord prolapses occur during the second stage of labor.
|
|
|
TABLE 21.6. Incidence of cord prolapse |
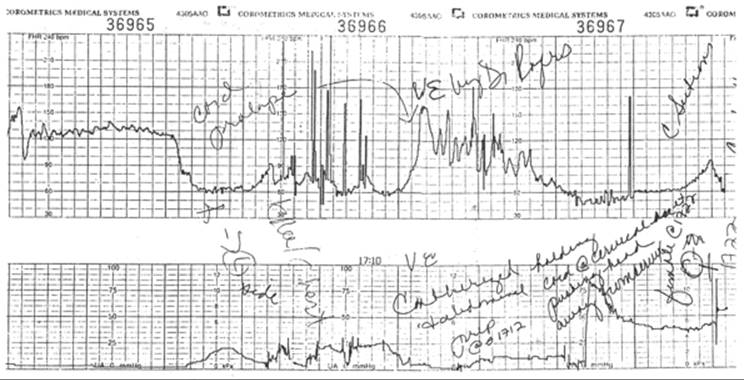
The diagnosis of cord prolapse should be suspected in any patient who develops fetal heart rate abnormalities after rupture of the membranes, either spontaneous or artificial. The heart rate abnormalities usually observed are sustained bradycardia and, less frequently, profound variable decelerations (Fig. 21.5). All such patients should be promptly examined or reexamined and the diagnosis confirmed by palpation of the cord alongside the presenting part or in the cervix or vagina.
|
|
|
FIG. 21.5. Fetal monitor tracing associated with umbilical cord prolapse. |
When cord prolapse is diagnosed, every effort should be made to prevent compression of the cord by the presenting part. The patient should be placed in steep Trendelenburg or the knee–chest position, and the presenting part should be manually elevated as far out of the pelvis as possible and held there until delivery is accomplished. Once the diagnosis is made, further palpation of the cord must be avoided, because this causes spasm of the umbilical arteries and may further compromise the fetus. Confirmation of fetal cardiac activity should be by ultrasound rather than by cord palpation. In fact, ultrasound is the only certain way to confirm fetal viability. There are at least two reported cases in which nonpulsatile cords were palpated and no fetal heart tones were heard with Doppler or stethoscope but ultrasound revealed fetal heart rates of 50 to 80 beats per minute. In both cases, prompt delivery resulted in surviving infants.
Cesarean delivery is the treatment of choice in almost all cases if there is fetal cardiac activity. Even at complete dilation, the perinatal outcome is better with cesarean delivery than with such maneuvers as breech extraction or high forceps. If the fetus is dead with no fetal cardiac activity present by ultrasound, and the fetal lie is polar, the mother usually is better served by allowing continued labor and vaginal delivery.
In most series of cord prolapse, perinatal mortality is approximately 15%. Among term infants and among all infants delivered by cesarean within 10 minutes of cord prolapse, mortality is less than 5%. Murphy and Mackenzie reported a retrospective study of 132 consecutive cases of cord prolapse in a single hospital. The overall perinatal mortality was 9% (12 of 132 infants). However, all but one death was due to either extreme prematurity or congenital malformations; the perinatal mortality rate attributable to asphyxia was 0.8% (one case). Of the 120 survivors they reported, only one infant had a major neurologic handicap.
True Knots
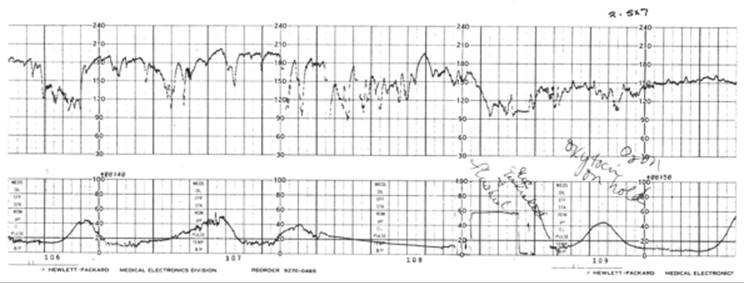
The reported incidence of true knots in the cord is 0.3% to 2.1% of births, the mean being about 1.0%. As is true of all cord accidents, true knots are more common if the cord is abnormally long. Ten percent of true knots occur in cords greater than 80 cm in length, and 3% of cords longer than 80 cm have true knots. However, many true knots must form early in pregnancy, for the incidence in aborted fetuses is 0.9%. True knots can be diagnosed only after delivery in the vast majority of cases, because unless the knot is pulled tight, there is no reduction of flow or increase in perfusion pressure, and thus no abnormality of the fetal heart rate or Doppler velocimetry. The patient with a tight knot will demonstrate a typical cord pattern of variable decelerations (Fig. 21.6) and will, of necessity, be managed like any other patient with fetal heart rate abnormalities.
|
|
|
FIG. 21.6. Monitor tracing of a fetus with a tight true knot in the umbilical cord. |
The Collaborative Study of Cerebral Palsy found no difference in 5-minute Apgar scores or neurologic abnormalities at 1 year of age between controls and infants born with true knots in the cord. There is an association however between true knots and antepartum stillbirths. About 4% to 5% of stillborns have true knots in the cord, compared with 1% of live-born infants.
Nuchal Cord
The incidence of loops of umbilical cord around the fetal neck is 25% of live-born infants, with 21% having one loop around the neck and 4% having two or more. In fact, 0.1% of fetuses have four or more loops of nuchal cord; the maximum reported number is nine. The incidence is 14% with short cords (<35 cm), 23% with normal length cords, and 53% with cords longer than 80 cm. There is no evidence that nuchal cords cause fetal death or significant degrees of fetal distress. The Collaborative Study of Cerebral Palsy found no increase in the incidence of depressed 5-minute Apgar scores, perinatal mortality, or abnormal neonatal development among infants with nuchal cords. It did demonstrate reduced 1-minute Apgar scores in these infants, however. Although nuchal cords are at times diagnosed by ultrasound, the excellent outcome of these infants demonstrates that no alteration in management is indicated unless the fetus develops bona fide distress during labor.
Body Coils of Cord
The incidence of coils of umbilical cord around various parts of the fetal body other than the neck is 0.5% to 2.0%, and is more frequent with long cords. As with nuchal cords, body coils are not associated with any increase in low Apgar scores, perinatal mortality, or neonatal morbidity.
SUMMARY POINTS
· The singleton breech fetus at term should be delivered by cesarean. This is a level A recommendation based on type I evidence.
· The preterm singleton breech at 28 weeks of gestation and beyond should be delivered by cesarean. This is a level A recommendation based on type II-2 evidence. There is no real evidence about the optimal mode of delivery of the singleton breech at 24 to 27 weeks of gestation.
· In the absence of contraindications, external cephalic version (ECV) should be attempted at term in singleton breech fetuses. At present there is no role for ECV before term.
· Fetal anomalies and chromosome abnormalities are important causes of breech presentation. Likewise, fetuses that have sustained neurologic insults leading to cerebral palsy often present as breeches.
· Nearly all cases of face presentation and compound presentation should be managed expectantly and vaginal delivery anticipated. Persistent mentum posterior (MP) face, persistent brow, and essentially all cases of shoulder presentation should be delivered by cesarean.
SUGGESTED READINGS
Albrechtsen S, Rasmussen S, Reigstad H, et al. Evaluation of a protocol for selecting fetuses in breech presentation for vaginal delivery or cesarean section. Am J Obstet Gynecol 1997;177:586–592.
Ballas S, Toaff R. Hyperextension of the fetal head in breech presentation: radiological evaluation and significance. Br J Obstet Gynaecol 1976;83:201.
Cheng M, Hannah M. Breech delivery at term: a critical review of the literature. Obstet Gynecol 1993;82:605.
Collea JV, Chein C, Quilligan EJ. The randomized management of term frank breech: a study of 208 cases. Am J Obstet Gynecol 1980;137:235.
Cruikshank DP, Cruikshank JE. Face and brow presentation: a review. Clin Obstet Gynecol 1981;24:333.
Eller D, VanDorsten JP. Route of delivery for the breech presentation: a conundrum. Am J Obstet Gynecol 1995;173:393–398.
Gimovsky ML, Wallace RL, Schifrin BS, et al. Randomized management of the nonfrank breech presentation at term: a preliminary report. Am J Obstet Gynecol 1983;146:34.
Hannah ME, Hannah WJ, Hewson SA, et al. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Lancet 2000;356:1375–1383.
Herbst A, Thorngren-Jerneck K. Mode of delivery in breech presentation at term. Increased neonatal morbidity with vaginal delivery. Acta Obstet Gynecol Scand 2001;80:731–737.
Kasule J, Chimbira THK, Brown IM. Controlled trial of external cephalic version. Br J Obstet Gynaecol 1985;92:14.
Lau TK, Lo KWK, Rogers M. Pregnancy outcome after successful external cephalic version for breech presentation at term. Am J Obstet Gynecol1997;176:218.
Lau TK, Lo KWK, Wan D, Rogers MS. Predictors of successful external cephalic version at term: a prospective study. Br J Obstet Gynaecol 1997;104:798.
Lee KS, Khoshnood B, Sriram S, et al. Relationship of cesarean delivery to lower birth weight-specific neonatal mortality in singleton breech infants in the United States. Obstet Gynecol 1998;92:769–774.
Murphy DJ, Mackenzie IZ. The mortality and morbidity associated with umbilical cord prolapse. Br J Obstet Gynaecol 1995;102:826.
Penn ZJ, Steer PJ, Grant A. A multicentre randomised controlled trial comparing elective and selective caesarean section for the delivery of the preterm breech infant. Br J Obstet Gynaecol 1996;103:684.
Ranney B. The gentle act of external cephalic version. Am J Obstet Gynecol 1973;116:239.
Roman J, Bakos O, Cnattingius S. Pregnancy outcomes in mode of delivery among term breech births: Swedish experience 1987–1993. Obstet Gynecol1998;92:945–950.
Sornes T. Umbilical cord knots. Acta Obstet Gynecol Scand 2000;79:157–159.
Footnote
*The papers of Collea and colleagues (1980) and Gimovsky and colleagues (1983) deserve special mention as “classic papers.” They are the only two published randomized trials of term breech delivery in all obstetric history prior to the year 2000.