Deborah Manzi-Smith
Charles C. Coddington III
As all medical specialties evolve, so has obstetrics and gynecology. Procedures that were once exclusively performed in the hospital setting are now exclusively performed in the office setting. Some office procedures (i.e., endometrial biopsy, transvaginal ultrasound/saline infusion sonography) have decreased the number of hospital surgical procedures a physician needs to perform to make a diagnosis. Additionally, medical therapies are now used that routinely replace surgical therapies (i.e., methotrexate for ectopic pregnancies). All these changes have resulted in shifting care from the hospital setting to the medical office. These changes in the specialty of obstetrics and gynecology coupled with the recent demands placed on the medical community for cost control has helped spark the trend in the development of more outpatient-oriented care and office surgical suites. Although the technology to perform minor gynecologic surgical procedures in an office setting has been available for years, most “simple” gynecologic procedures are still typically performed in the hospital setting. This chapter will discuss the preparation and briefly review a number of minor procedures which can be performed in an office surgical suite.
PREPARING THE FACILITY
Although many procedures can be performed in an office setting, the particular layout, room sizes, equipment availability, and staffing issues may make it difficult for the practitioner to perform certain office surgical procedures. The facility should, at a minimum, allow for easy access of wheelchairs and stretchers. Additionally, the basic medical supplies needed would include pulse oximeters, basic airway management equipment, electrocardiogram monitoring, intubation supplies, rooms equipped with call alarm buttons, intravenous line stands, a crash cart, and waste containers for sharps. An electronic table capable of placing patients in the Trendelenburg position, with cushioned knee stirrups, is preferred for procedures that last over 10 minutes or use anesthesia. It is important to keep in mind that in some states there are regulations for specific facility requirements when conscious sedation is used. Before developing an office surgical suite physicians should check with local regulatory committees so they will be able to meet any local standards and needs assessments.
PREPARING THE PATIENT
For procedures that are performed in the office setting, a clinician should prepare the patient the same way as they would for the similar in-hospital procedure. Important attention should be paid to the medical history and past medical history to make sure the patient is a good candidate for an in-office procedure and is of low anesthetic risk. Patients with multiple medical problems, cardiovascular disease, or neurologic disease may be better served in the hospital setting. Consents similar to what one would obtain for a day-surgery hospital procedure should be signed. It is important to remember that consent will be required not only for the surgical procedure but also for the anesthesia used. Basic preparatory instructions for the individual procedure should be given as well as postprocedure instructions in case discharge planning is needed. Fasting is recommended when conscious sedation is required, which is abstinence from food for 8 hours and clear liquids for 2 hours.
ANESTHESIA
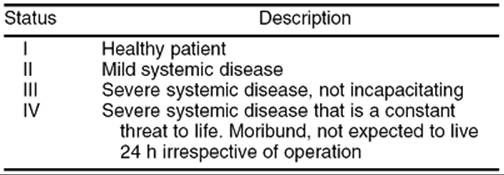
Although some office procedures can be performed without anesthesia, some will require oral or intravenous sedation. The term conscious sedation implies a state in which patients can tolerate procedures with adequate cardiopulmonary function and respond to verbal commands. The American Society of Anesthesiologists (ASA) has published guidelines for sedation and analgesia performed by medical staff not trained in the practice of anesthesia. In the office setting nonanesthesia residency–trained physicians should limit patients to ASA classification I or II (Table 27.1). The clinician should avoid procedures on patients with significant cardiac, respiratory, or neurologic disease in the office setting.
|
|
|
TABLE 27.1. American Society of Anesthesiologists (ASA) patient classification |
Per hospital policy, anesthesia records should be maintained on the patient's ventilatory and oxygenation status. Hemodynamic variables should be recorded frequently and at a minimum it should be recorded:
· prior to the administration of anesthetic agents
· following the administration of sedation
· upon completion of the procedure
· upon recovery
· at the time of discharge.
A designated medical professional (nurse, physician's assistant, or physician) other than those performing the procedure should be present to monitor the patient's vital signs throughout the procedure. A staff member trained in advanced cardiac life support (ACLS) should be immediately available. The patient should have intravenous access. Naloxone and flumazenil should be available when opioids and benzodiazepines are used.
Anesthesia techniques will vary upon the physicians training and facility requirements. Most obstetrician-gynecologists performing office surgical procedures should be versed in conscious sedation, administration of local analgesia, and paracervical blocks. Ideally patients undergoing diagnostic and therapeutic procedures receive moderate sedation. The definitions within the continuum of sedation are described in Table 27.2.
|
|
|
TABLE 27.2. Explanations of various levels of anesthetic sedation |
Local Anesthesia
Local anesthesia can be a safe and effective means of providing analgesia for office procedures. Local anesthesia is defined as the elimination of sensations, especially pain in one part of the body using topical or regional injections of medications. Most obstetrician-gynecologists are educated in the use of local anesthetics during residency training. The secrets of success with local anesthetic use is injecting slowly, using a sufficient amount of medication and waiting for the medication to take effect. Several agents may be used and include benzocaine, mepivacaine, bupivacaine, and lidocaine. It is important to remember that local anesthetics have cardiac and central nervous system toxicity, particularly with intravasation into the venous system. Local anesthetics are frequently mixed with epinephrine. Symptoms of epinephrine overdose include tachycardia and hypertension, and one should watch for these signs when using local anesthetics containing epinephrine.
Paracervical Block
Most gynecologists should be proficient in performing a paracervical block. Paracervical blocks are useful not only for cervical biopsies, cervical conization, and loop electro-excisory procedures but also for office dilation and curettage (D&C) procedures and office hysteroscopy. In performing a paracervical block, in addition to the supplies needed for the local infiltration, it is useful to have available a needle extender or long spinal needles. The application of 1% benzocaine spray or lidocaine ointment prior to insertion of the needle may relieve some of the discomfort from inserting the needle. For the paracervical block, injecting 10 mL of anesthetic (usually 1% lidocaine) at the 4 and 8 o'clock positions and waiting 10 minutes gives excellent results. This is believed to limit sensation from the uterosacral nerve bundles from S2, S3, and S4. With this technique the only area of tenderness appears to be the fundus of the uterus and providing local anesthesia to this area is difficult as it is supplied by the tenth thoracic nerve (Fig. 27.1).
|
|
|
FIG. 27.1. Injection sites for paracervical block at 4 and 8 o'clock positions. |
Conscious Sedation
Conscious sedation is defined as a minimally depressed level of consciousness whereby a patient can maintain their own airway independently and respond to verbal commands. The medications used for conscious sedation procedures include local anesthetics, sedatives, and anxiolytic and opioid analgesics. The ideal drugs to use in an office setting would have a quick onset and quick clearance rate. The medications used should have a predictable onset of action and minimal side effects. Anxiolytics and opioids are more commonly used by nonanesthesiologist practitioners for conscious sedation. The window of safety between effect and oversedation is narrow for sedatives and therefore limits their use in the outpatient setting for most physicians. It is important that the surgeon avoids turning a conscious sedation case into general anesthesia, especially in the office setting. There is an approximately a 0.2% mortality rate with conscious sedation, mostly due to oversedation and inadequate monitoring.
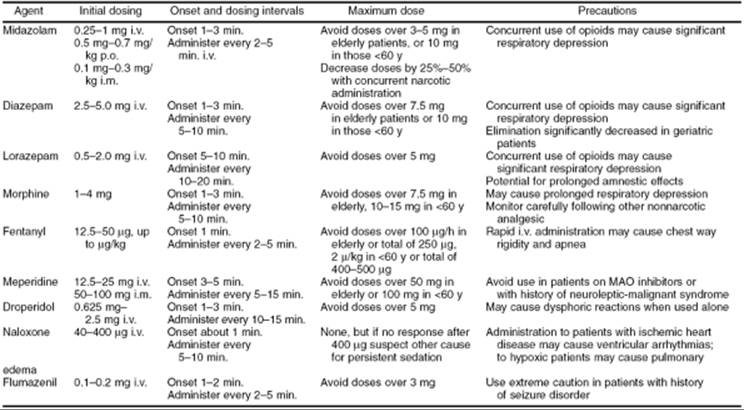
Diazepam (Valium) is the most popular of the anxiolytics used; however, midazolam (Versed) has also been used. Diazepam is popular because it can be given both intravenously and orally. The usual dose is 2.5 mg intravenously every 10 minutes to a maximum dose of 0.15 mg per kg or 10 mg. The drawback to diazepam is its long duration of action, which is why some physicians prefer midazolam. Midazolam can also be administered orally, intravenously, or intramuscularly. It has a short half-life. The usual recommended dose is 1 mg intravenously every 5 minutes to a maximum dose of 0.07 mg per kg or 5 mg in the office setting.
The opioids are medications that will decrease the patient's awareness of painful stimuli. These drugs can produce respiratory suppression and should be used cautiously. The preferred drug in this class for conscious sedation is fentanyl. Fentanyl has a quick onset of action and short half-life. In the office setting the standard dose is 25 to 50 µg every 5 minutes, to a maximum of 3 µg per kg, or 250 µg intravenously. Morphine and meperidine have also been used instead of fentanyl, however, they have a longer duration of action. It is important to note that morphine and meperidine appear to work better for patients with visceral discomfort.
Naloxone and flumazenil are two drugs that are essential to have available while providing conscious sedation using opioids and benzodiazepines. Naloxone (40 mg intravenously) is used to reverse the respiratory depression seen with opioids and flumazenil (0.2 mg intravenously) is a benzodiazepine antagonist (Table 27.3).
|
|
|
TABLE 27.3. Agents approved for conscious sedation and dosing regimens for adults |
PREVENTING COMPLICATIONS
There are two basic groups of complications from surgical procedures:
1. Allergic reaction to the medications used.
2. Technical difficulty with the procedure.
Being prepared is the key to managing procedure complications. Careful history will help eliminate most allergic reactions, but a staff member trained in resuscitation and having agents like Benadryl (50 mg i.v.) and epinephrine may be lifesaving. It is imperative that the recommended limits for in-office sedation for the medication being used are not exceeded. An approximately 0.2% mortality rate occurs with conscious sedation. Those deaths are mostly due to the lack of adequate monitoring of cardiac and respiratory functions during the procedure. Good judgment is the key to avoiding complications. It is much better to discontinue the office procedure if it appears more complex than originally planned. To help improve outcome after any surgical complication it is important to have an emergency plan available for these unforeseen surgical complications (i.e., local ambulance number, local emergency room number, crash cart, and staff trained in ACLS techniques).
THE PROCEDURES
Office Hysteroscopy
Setup, Equipment, and Preoperative Care
Office hysteroscopy is a useful tool for the evaluation of abnormal uterine bleeding, infertility, and recurrent pregnancy loss. Typically an office hysteroscopy can be performed in a regular exam room without much modification. The most common medium used for distention with office hysteroscopy procedures is CO2. CO2 is readily available and uses a low-flow insufflator (100 mL/min). It is essential to note that a CO2 insufflator for laparoscopy is a high-flow insufflator and should never be used for office hysteroscopy. Advantages of CO2 is its low cost, low “mess,” and overall performance and safety. It is important to remember however that CO2 is not a good medium for evaluation of patients with abnormal bleeding while they are bleeding. These patients may be better served with a “liquid” distention medium including high-molecular-weight dextran, sorbitol, normal saline, or lactated Ringer solutions. Several hysteroscopy manufacturers have developed low-cost complete fluid systems for office hysteroscopy procedures that aid in making the procedure safe and simple.
When starting to perform office hysteroscopy procedures it is important to make sure you have the correct equipment available. For office hysteroscopy there are two different kinds of hysteroscopes—rigid and flexible. Flexible hysteroscopes tend to be more expensive and have slightly poorer quality images when compared to rigid hysteroscopes. Most physicians prefer rigid hysteroscopes for office procedures. The standard office rigid hysteroscope is 4 mm in size, however, microhysteroscopes with 2.4 mm and 2.7 mm optics are available. The smaller size decreases the need for cervical dilation, which has the advantage of decreasing the pain and bleeding associated with the procedure. In addition to the sheath size for the hysteroscope physicians have a choice of telescope angle. Most physicians prefer to use a telescope at 0, 12, 15, or 30 degrees. Many hysteroscopy systems are available for operating room and office use. All systems have their particular advantages and disadvantages. Several systems should be tested in your office setting to determine which system is the best for you before purchasing a system. Look for a system from a company with reliable service that has the operating equipment you will need (graspers, forceps, scissors) and a telescope with the brightest, clearest image within your budget.
Surgical Technique
After the patient has checked in and appropriate vital signs have been taken adequate analgesia should be given (see “Anesthesia” earlier in the chapter). An attempt to pass the hysteroscope without dilation should be made. However, the cervix may need to be dilated. Good techniques for cervical dilation include laminaria or misoprostol. Since these techniques require preplanning it is best at the preoperative appointment to assess the cervix to determine if dilation will be necessary. The problem with laminaria insertion is it requires a visit to the office the day prior to the procedure and many patients experience severe cervical/uterine cramping. Another option is the use of misoprostol 400 mg orally 4 to 6 hours prior to the procedure.
The hysteroscope is usually inserted under direct visualization passing through the cervical canal into the endometrial cavity. To aid in visualization during the hysteroscopy, the cervix should be cleared of all blood using a sponge forceps prior to entering the cervical canal. Another way to keep the lens clean when using a liquid distention medium is to start the distention medium prior to entering the cervix. The running fluid at the tip of the hysteroscope upon entering the cervical canal aids in keeping the lens clean and in visualization at the start of the procedure. In addition, if the medium is cloudy upon entry, waiting 15 to 30 seconds to allow the continuous flow process to work will provide a clearer field of vision. In contrast, if CO2 is used as the distention medium, do not start the CO2 until after entrance into the cervical canal. This will avoid making blood-tinged bubbles within the cavity which will obstruct the view.
Once the hysteroscope is passed through the cervical canal into the uterus a systemic overview of the cavity should be performed prior to performing any operative procedures. Inspect the fundus and locate both tubal ostia first then pull back to the level of the internal os and inspect the entire anterior then posterior wall of the uterus (Fig. 27.2).
|
|
|
FIG. 27.2. Demonstrating a posterior wall intrauterine mass in an office hysteroscopy evaluation. |
Postoperative Care
Most patients will have light spotting or light bleeding for up to 5 days after their hysteroscopy procedure and should be advised of such. Intercourse and douching should be restricted for 24 hours. Tampons may be used for the postoperative bleeding that occurs. Patients should be advised that they could have minimal cramping which is best resolved with a nonsteroidal antiinflammatory drug (NSAID) or other analgesic. Patients should be instructed to call if they have heavy bleeding, severe pain unresolved by the NSAID, or fever greater than 100.5°F.
Microlaparoscopy
Setup, Equipment, and Preoperative Care
Microlaparoscopy under local anesthesia has raised interest in the medical community due its cost-effectiveness in comparison to in-hospital procedures. Several different microlaparoscopy procedures can be performed in the office setting, however, the difficulty in performing office microlaparoscopy for most physicians is not obtaining the training or equipment needed to do these procedures but rather having adequate office facilities to accommodate a microlaparoscopy suite. In addition to adequate facility size, the following equipment should be available for the office procedure:
· “micro” laparoscope and microlaparoscope lens
· video camera
· video monitor
· trocar sheaths
· laparoscopic scissors, graspers, and bipolar coagulation
· a table capable of accommodating the Trendelenburg position
· resuscitation equipment
· intravenous line supplies
v sterile surgical gowns and drapes.
Several “micro” laparoscopes are available for use. The refinements in fiberoptic technology have led to excellent quality 2-mm laparoscopes. Microlaparoscopes range from 25 to 27 mm in working length and have a 0-degree angle of view. There are 2-mm accessories available such as graspers, blunt probes, and biopsy forceps. While concerns remain over optical clarity with these “micro” laparoscopes, comparison of the accuracy of a 1.98-mm microlaparoscope with the standard 10-mm laparoscope (endometriosis scores and adhesions scores) yields no difference between the two. To avoid major complications, candidates for office laparoscopy should have no more than a minimal amount of prior abdominal surgery and no medical history suggestive of a significant risk of abdominal adhesions.
Surgical Technique
It is important to realize that even experienced laparoscopic surgeons should perform office microlaparoscopy with an experienced microlaparoscopic surgeon prior to performing these procedures on their own. Even experienced laparoscopic surgeons will find the “micro” equipment more difficult to use at first until a feeling is established for the differences in depth perception and smaller field of view when compared to their full-size counterparts. Procedures best suited for the microlaparoscopic technique include infertility evaluations with chromopertubation, tubal ligation procedures, conscious pain mapping, and second-look procedures. The average length of an infertility evaluation procedure is 18 minutes. Some patients undergoing microlaparoscopy can have the procedure performed strictly under local anesthesia. However, this limits the length of the procedures and the amount of gas that can be used for insufflation. Most patients are better served with some conscious sedation as this often allows the procedure to last 30 to 45 minutes in contrast to only 15 minutes with local anesthetic alone.
For the microlaparoscopy procedure, the patient is placed in dorsal lithotomy position on a table capable of performing Trendelenburg. A paracervical block should be give if a uterine manipulator is used such as the Cohen cannula. The patient is sterilely prepped and draped. If conscious sedation is used, this is given according to the guidelines described previously. Local anesthetic is then given in the area of the umbilicus. The use of a Verres needle/sheath combination system allows entry of the Verres needle without reintroduction of a trocar sheath for the procedure. The abdomen is insufflated and the pelvic organs visualized. Remember insufflation pressures will be higher in these patients because they do not have abdominal muscle relaxation. Pressures and gas flow should be titrated to patient comfort. Observation and chromopertubation are performed in a manner similar to that using the 10-mm laparoscope.
Postoperative Care
Routine postoperative care for laparoscopic procedures should be followed for patients undergoing in office laparoscopic procedures. Patients should be stabilized prior to discharge and return for a postoperative incision check in 1 to 2 weeks. Patients should be advised to call if they experience heavy vaginal bleeding, pain that is not resolved by NSAIDs, or a fever greater than 100.5°F.
Office Dilation and Curettage (D&C) and Endometrial Sampling
Setup, Equipment, and Preoperative Care
The vast majority of office endometrial samplings and D&C procedures can be performed with minimal office modifications. Most of the equipment needed is readily available and disposable. In addition to the obvious cost savings for office D&C procedures, the office procedures are more time-efficient for the physician.
Office D&C procedures may be performed for a variety of reasons but the most common indications include pregnancy termination and management of an incomplete abortion prior to 12 weeks gestation. It is very important to confirm pregnancy status and location by ultrasound prior to performing the procedure. The most common reasons for in-office endometrial sampling include evaluation for abnormal uterine bleeding, postmenopausal bleeding, recurrent pregnancy loss evaluation, and as part of an infertility workup.
Surgical Technique
The most popular technique for office D&C uses the Karman cannula. The Karman cannula is a soft catheter and is an efficient suction device as it has two suction ports. The larger the bore of the catheter the more effective is the aspiration procedure. As the soft catheter works so well we find that there is a limited role for the sharp curettage technique. The soft catheter probably reduces the risk of uterine perforation when compared to the traditional sharp curette. In choosing the size of the cannula the diameter of the cannula should equal the size of the uterus using the standard sizing of the number of weeks of pregnancy. Therefore when performing a D&C for an incomplete abortion in a uterus measuring 8 weeks gestation, an 8-mm cannula should be used. Office procedures should be used only on those patients with a uterine size less than 12 weeks gestation. Prior to arrival at the office we usually pretreat the patient with Valium, 5 to 10 mg orally. After check in and routine vital signs are obtained, a bimanual exam is performed to determine the uterine size. A speculum is inserted to perform a paracervical block (see “Anesthesia” earlier in the chapter for description of this technique). After adequate anesthesia is induced the catheter should be passed through the cervical os. Sometimes cervical dilation is needed and this may be accomplished with dilators, laminaria (or its synthetic counterpart), or misoprostol.
Initially the chief purpose of uterine curettage was for endometrial sampling, however, the classic curettage has been essentially replaced with the office endometrial sampling. Endometrial sampling is a diagnostic screening test and the use of an in-office endometrial sampling procedure has essentially eliminated the need for many D&Cs performed in the operating room. During the past 50 years many different instruments have been developed for office endometrial biopsies. Most of the sampling devices used for this purpose have a 5-mm or less outer dimension and are made of plastic. Some of these devices require a syringe or suction pump, however, the most popular endometrial sampling device is the disposable hollow plastic tube with an aspiration port that has a solid plastic obturator (Pipelle).
Postoperative Care
Most patients do well after an in-office endometrial curettage or sampling. The patients should be advised that they might have cramping and bleeding for 3 to 4 days after the procedure. Patients often respond well to NSAIDs for uterine cramping. They should be advised to call the office if they develop a fever, have vaginal discharge, or have bleeding past 4 days.
Endometrial Ablation
New technology now allows the physician to perform office endometrial ablation. Several types of endometrial ablation devices are on the market, some using water, balloons, or impedance-controlled bipolar radio frequency. In randomized studies 46% of patients were able to use the balloon technology in the office under local anesthesia (some with i.v. sedation) and 73% using the bipolar radio-frequency system were able to be performed in the office setting.
Novasure (bipolar radio frequency) technology can be performed as an outpatient or office-based procedure. The average treatment time is 90 seconds compared to 8 to 12 minutes for balloon technology. With the Novasure system, the Novasure introducer sheath is introduced through the cervical os (Fig. 27.3). The three-dimensional bipolar electrode expands from the introducer sheath and with the aid of CO2 conforms and checks the integrity of the uterine cavity. The ablation is accomplished and the electrode is retracted into the sheath and removed. There is a 91% success rate (decrease in flow) and 41% amenorrhea rate (Table 27.4). The endometrial balloon (Thermachoice) is very easy to use (Fig. 27.4). The catheter is primed and tested. The catheter is then introduced into the uterus much like a sound. The balloon is filled and the Thermachoice heats the fluid. After a heating period, 8-minute treatment period, and cooling period the catheter is removed. Temperatures and uterine pressures are measured continuously. This helps confirm uterine integrity.
|
|
|
FIG. 27.3. Novasure endometrial ablation technology using a balloon system. |
|
|
|
TABLE 27.4. Endometrial ablation procedures |
|
|
|
FIG. 27.4. Thermachoice endometrial ablation technology using a balloon system. (Reprinted with permission from Gynecare, Somerville, NJ.) |
Surgical Technique
The surgical technique will depend upon the equipment used. Physicians who desire to use the ablation technology should be trained by those experienced in using the equipment. Contacting your local equipment sales representatives and surgeons to serve as experienced preceptors should be the easiest way to become proficient using ablation equipment. If these procedures are being performed in conjunction with hospital systems, there may be information on credentialed individuals in the medical staff office.
Postoperative Care
Most patients will do well after discharge. Generally an NSAID or similar medication is prescribed to control postoperative pain. Patients should be advised to contact the office with excessive postoperative pain that is not relieved by the NSAIDs or if they experience excessive postprocedure bleeding. In order to insure that the patient is satisfied with the ablation results it is important to educate patients about the typical results seen with endometrial ablation. Most patients will not experience a decrease in the menstrual flow for approximately three menstrual cycles after the ablation. The percentage of decrease in flow and amenorrhea rates, which vary with the technology used, should be reviewed prior to the procedure. As many as 30% to 40% of women may need further intervention within 4 to 5 years; however, patient satisfaction remains high if the limitations are discussed preoperatively.
Saline Infusion Sonography
Since the development of high-resolution ultrasound, saline infusion sonography (SIS) has been gaining in popularity. Numerous studies have looked at the benefit of ultrasound in establishing the diagnosis in women with abnormal uterine bleeding. However, it is sometimes difficult to image the endometrial contents and rule out pathology on a reliable basis. The use of fluid instillation into the uterine cavity coupled with ultrasound has become a useful diagnostic tool. SIS is easily performed in the clinical setting and is remarkably well tolerated in most patients. The clinical use of SIS is not in its use to replace surgery but to identify those patients who need surgical intervention. Multiple indications for SIS are listed in Table 27.5.
|
|
|
TABLE 27.5. Indications for saline infusion sonography |
Setup, Equipment, and Preoperative Care
The minimum supplies required to perform SIS include a SIS catheter, instillation medium, a 20-cc syringe, povidone-iodine solution, scopettes, an open-sided speculum, and an ultrasound that preferably has transvaginal capabilities. The most widely used medium for instillation into the uterine cavity is saline; however other contrast media have been investigated, including Echovist and Albunex. These media do not appear to perform better than normal saline and are more costly. SIS can be performed during any time of the cycle; however performing SIS during the follicular phase will avoid the disruption of an early pregnancy. In addition during the follicular phase there is a thinner endometrium, which may aid in better evaluation of the uterine lining. Instilling saline during menses may lead to poor uterine distention so avoiding the procedure during the menstrual cycle is preferred.
There are several SIS catheters on the market (Fig. 27.5, Fig. 27.6 and Fig. 27.7). Alternatively, pediatric Foley catheters, insemination catheters, and pediatric feeding tubes, can be used. The choice of the catheter will depend on the patient and therefore several catheter types should be available to the physician performing the SIS. In particular, one should have a thin, stiff catheter available for nulliparous cervices and a balloon or cone type catheter for multiparous cervices. The balloon should be used in patients with multiparous cervices to occlude the os. This will limit the amount of medium leaking out of the uterus and improve uterine distention.
|
|
|
FIG. 27.5. Placement of the Goldstein catheter for saline infusion sonography using a cone to occlude the cervical os. (Reprinted with permission from Cook Ob/Gyn, Spencer, IN.) |
|
|
|
FIG. 27.6. Saline infusion sonography catheter, balloon type. |
|
|
|
FIG. 27.7. Saline infusion sonography catheter, insemination type. |
Technique
After performing a bimanual exam or baseline ultrasound to determine uterine position, a speculum is inserted and the cervix is identified. The cervix may be cleansed with povidone-iodine or similar antiseptic solution. The catheter is primed with saline and then inserted through the cervical os. The exact placement will depend upon the catheter used. For a balloon-type catheter, the balloon should be positioned in the cervical canal or lower uterine segment and inflated. However the Goldstein SIS cone-type catheter is inserted to 7 cm, or near the uterine fundus, with the white acorn cone occluding the cervical os (see Fig. 27.5). A ring forceps may be needed to assist in placing the SIS catheter. Once the catheter is in place the speculum is removed with special care taken so that the catheter is not dislodged. The vaginal ultrasound probe is inserted into the vagina and the uterus is imaged as the saline is infused slowly. Usually about 5 to 10 cc of saline is used in order to get good distention. It is important to remember the seal will not be watertight. Although a watertight seal may produce better images, this will result in significantly more cramping with the procedure. When there is a large efflux of saline out the cervix, more saline may be needed to get good images. Visualization in both the longitudinal and transverse axis should be performed. The entire uterine cavity should be visualized from left to right broad ligaments longitudinally and from the cervix to the fundus in the coronal plane (Fig. 27.8). It is important to realize that full distention of the uterus is not necessary to get a good quality evaluation. Indications for SIS are summarized in Table 27.5.
|
|
|
FIG. 27.8. Saline infusion sonography (SIS) evaluation of the uterine cavity. A: SIS demonstrating a normal uterine cavity. B: SIS demonstrating an intrauterine mass. C: SIS demonstrating a localized posterior wall thickening. D: Bicornuate or septate uterus visualized prior to instillation of saline. |
Postoperative Care
Most patients have minimal discomfort after a SIS procedure. Patients usually do well using NSAIDs or similar analgesics for pain control. Patients should be advised to call if they are experiencing heavy bleeding not associated with menses that continues for more than 4 days. Additionally patients should be evaluated if they have a fever greater than 100.5°F or vaginal discharge.
Contraceptive Procedures
As part of residency training most obstetrician-gynecologists will obtain the clinical training needed to perform insertion and removal of an intrauterine device (IUD) and the Norplant system.
Two IUDs are available in the United States: Mirena and Paragard. IUDs are generally recommended as a contraceptive method to women in a stable monogamous relationship who are not at risk for pelvic inflammatory disease, sexual transmitted diseases, or ectopic pregnancies. IUDs are contraindicated in the following situations:
· suspicion of pregnancy
· congenital uterine anomaly
· fibroid uterus which severely distorts the uterine cavity
· pelvic infections
· unresolved abnormal Pap smear
· untreated cervicitis or vaginitis
· genital bleeding of unknown etiology
· women with multiple sexual partners
· leukemia
· acquired immunodeficiency syndrome (AIDS)
· breast cancer
· ectopic pregnancy or history of ectopic pregnancy.
The Mirena IUD consists of a T-shaped polyethylene frame with a steroid reservoir around the vertical stem (Fig. 27.9). The reservoir consists of a cylinder made up of a mixture of levonorgestrel and silicone. There are 52 mg of levonorgestrel within the system which provides levonorgestrel at a rate of 20 µg per day initially. This level declines to half the 52-mg level at 5 years. Levonorgestrel is a progestogen, which is used in a variety of contraceptive products. There is a stable blood level of 150 to 200 pg/mL 3 weeks after insertion of the Mirena device. The T system is 32 mm in length and width. The T-shaped body also has barium embedded which makes it radiopaque. There is a monofilament string attached to the T-shaped body stem. Although the exact mechanism for contraception is not clearly identified it appears that the Mirena IUD has mostly local effects within the uterine cavity. Additionally, Mirena may have an effect on ovulation. In a 1-year study of the system only 45% of cycles were ovulatory; however, in a 4-year study 75% of cycles were noted to be ovulatory. Contraceptive effectiveness is quoted to be 0.2 pregnancies per 100 women and the cumulative 5-year pregnancy rate is 0.7 per 100 women. Half of the pregnancies that occur while using the Mirena IUD are ectopic gestations, at a rate of 1 ectopic pregnancy per 1,000 users per year. It is important to inform patients that the Mirena IUD can alter the menstrual bleeding pattern. During the first 3 to 6 months of use there may be an increase in vaginal spotting. Additionally, it has been noted that approximately 20% of users will amenorrheic after 1 year of use.
|
|
|
FIG. 27.9. The Mirena intrauterine device. A: Insertion of Mirena into uterine cavity. B: The arms of the Mirena are released. C: Mirena is positioned near the uterine fundus. D: Releasing the Mirena IUD and withdrawing the inserter. E: The Mirena IUD. |
The Paragard IUD has a T-shaped polyethylene body. The vertical portion of the T is wound with 176 mg of copper wire along with a copper collar of 68.7 mg on each of the transverse arms. The exposed areas of copper are approximately 380 mm2. Paragard has a monofilament thread attached the bulb end of the base of the T-shaped device. The available data indicate that the copper is continuously released into the uterine cavity. The additional copper load to the body from a copper IUD may precipitate symptoms in patients with Wilson disease. The exact mechanism in which the copper provides contraception is unclear; however it is thought that there is interference with sperm transport, fertilization, and embryo implantation. The Paragard should be kept in place no longer than 10 years. Women who use the copper IUD should be advised that blood loss at the time of menses might increase. There is an approximately 35% increase in menstrual blood loss among copper IUD users.
If a woman becomes pregnant while an IUD is in place, the manufacturers recommend removing the IUD if the string is visible. Removal under these conditions is usually simple. It is important to confirm the location and viability of the pregnancy prior to removal of the IUD. Patients in whom the IUD cannot be removed or those who choose not to have the IUD removed should be informed that there is an increased risk of septic abortion and preterm labor/delivery.
IUD Insertion Technique
An IUD should only be inserted, managed, and removed only by clinicians trained in IUD use. The Mirena and Paragard have different techniques for preparing the IUD insertion, so clinicians should refer to the package inserts for guidance. IUDs can be inserted at any time during the menstrual cycle. Traditionally physicians have preferred to insert an IUD at the time of menses to insure that the patient is not pregnant. However insertion at the time of menses increases the risk of expulsion of the IUD during the first 2 months of use. It is best to give patients an NSAID 1 hour prior to IUD insertion. After loading the IUD into its insertion device the uterus should be examined by bimanual examination and a speculum inserted into the vagina and the uterus sounded. With both IUDs there is an adjustable flange that should be set to the length to which the IUD should be inserted. A single tooth tenaculum is applied to the anterior lip of the cervix to aid in cervical and uterine straightening. Benzocaine spray or local infiltration of lidocaine may be used prior to tenaculum placement.
The IUD must be inserted within 5 minutes of loading so that the arms will spring back open after insertion. The IUD is then passed through the cervical canal to the fundus. The plastic flange should be at the level of the internal os if the IUD is inserted correctly. Once correct placement is confirmed, the insertion device is used to release the arms of the IUD. The insertion device is then removed gently so as not to disturb the placement of the IUD. The monofilament thread should be cut approximately 2 cm from the external os. The risk of uterine perforation is 1 in 1,360 insertions. Insertion immediately in the postpartum period, particularly during lactation has been associated with an increased risk of uterine perforation. However there is no increased risk of perforation if the IUD is inserted immediately after expulsion of the placenta. It is our preference, however, to delay insertion of an IUD until the second postpartum month.
Postoperative Care
After insertion of an IUD the patient should be taught how to palpate the strings monthly. Patients should be seen in 3 months to review bleeding pattern and concerns with the IUD. At that time, a speculum examination should be performed to rule out partial expulsion of the IUD.
Removal of an IUD is generally easy. It is important to note the type of IUD prior to removal. The strings are grasped with a ring forceps and pulled outward through the vagina until the IUD is expelled. If the strings break off during removal or the strings are not visible, removal under ultrasound guidance is advisable. Under ultrasound guidance, while using packing forceps, the lower stem is located. Using gentle traction, it is removed through the internal then external os. If gentle force does not produce the IUD then the IUD may be embedded and, in such cases, hysteroscopic removal in the operating room may be needed. It is important to note that some IUDs that are used outside the U.S. do not have strings and are designed for permanent placement. These should not be removed in the office setting.
Norplant
The Norplant contraceptive system consists of six Silastic capsules each filled with 36 mg of levonorgestrel powder. The capsules should be placed in the subcutaneous layer of the inner aspect of a woman's nondominant arm. Norplant capsules are designed for 5 years of use with a typical first year failure rate of 0.09% and a cumulative failure rate of 1.1% over 5 years. Discontinuation of use prior to 5 years appears to be the major problem with the Norplant system. The major reasons for discontinuation of use include bleeding abnormalities, weight change, headaches, and change in libido. Women with active venous thrombosis, unexplained vaginal bleeding, or history of stroke or breast cancer are not candidates for Norplant. Women using the drugs listed in Table 27.6 should not use Norplant as these drugs increase the metabolic clearance of levonorgestrel, which can decrease its efficacy. The most common side effects of the Norplant system include changes in the menstrual pattern, weight changes, and headaches.
|
|
|
TABLE 27.6. Drugs that decrease the effectiveness of the Norplant system |
Norplant Insertion Technique
Both insertion and removal of the Norplant system require formal training to avoid complications. Norplant insertion should be scheduled during the first week after menses. Patients should be told to avoid intercourse during this time to avoid inadvertently becoming pregnant. Location for placement of the Norplant capsules is the first decision that should be made. Ideally the capsules should not be noticeable. It is important to remember good placement of the capsules translates into easy removal. The location of the Norplant capsules to avoid detection should be on the inner aspect of the upper arm. Ideally the location should be above the level of the nipple and medial enough that it lies on the medial aspect of the arm. The capsules are traditionally fanned, and are placed approximately 15 degrees apart from each other. Once a location is chosen, the physician should use the Norplant template included in the kit and mark a dot for the incision site and a dot for the position of each of the distal tips. The Norplant kit contains all the necessary equipment needed for a standard simple insertion.
Patients should be in the supine position when the capsules are inserted. The arm should be placed flat on the examining table with the palm upward and the elbow bent to 90 degrees (as if the patient is signaling to make a right-hand turn). Local anesthesia is given at the incision site, taking care not to use too much anesthesia which may distort the tissue planes. The needle should be advanced its full length just under the skin along the planned tract of each capsule. After adequate anesthesia is obtained, a 3-mm horizontal incision should be made at the incision site that has been chosen. The obturator should be loaded into the trocar provided in the kit. The trocar, with obturator in place, is introduced directly through the incision with the open end of the bevel facing the ceiling. The skin below the incision site should be held in place for traction. The trocar is then advanced until the level of the second line on the trocar is at the incision site. The obturator is removed and the Silastic capsule is introduced. The obturator in then replaced. The obturator is used to push the implant down the shaft of the trocar and into place. Once in place the obturator and trocar are removed gently and slowly. This procedure is performed a total of 6 times at 15-degree angles until all capsules are placed. After all 6 capsules are placed, the edges of the incision should be reapproximated with Steri-Strips.
Postoperative Care of Norplant
Patients who have the Norplant inserted close to the time of ovulation should use barrier contraception for 1 week. Patients should be advised to check for signs of infection at the incision/insertion site, which occurs in less than 1% of Norplant insertions.
Norplant Removal
The most important thing to remember is that good placement of the Norplant capsules leads to easy removal. One method of removal of the Norplant system is described here. As with other procedures many techniques have been developed to aid with the removal of the capsules. No particular procedure appears to have an advantage over another. It is recommended that removals be scheduled for a 20-minute appointment. Most Norplant removals take 15 minutes, however on rare occasions we have known them to take up to 45 minutes. Patients should be advised that removal is more painful than insertion. The incidence of difficult removal is quoted by the manufacturer to be about 13%. The area should be palpated and the location of the Norplant capsules identified. The following equipment is needed for removal:
· examining table
· sterile gloves
· sterile drapes
· antiseptic solution
· lidocaine or similar anesthetic
· needles and syringes
· scalpel
· marker
· straight and curved mosquito's or a similar clamp
· Steri-Strips, sterile gauze, and tape.
The location of each capsule is marked. If all capsules cannot be identified, localization by ultrasound or radiograph may be necessary. The area is then cleansed with Betadine and a local anesthesia is administered prior to making an incision where all the capsules converge. Additional anesthesia should then be given under the base of each capsule and behind each capsule for about a 1 cm of its length. In addition to providing anesthesia this will serve to raise the capsules. Injection of the anesthetic above the capsules may obscure their location and this should be avoided. Pressure is then applied to the distal end of the implant toward the incision to see if the tip can be “milked” into view. Most of the time, a fibrous sheath will be noted around the implant. This sheath should be nicked and the implant is then “milked out” through this nick and then through the incision on the arm. Unfortunately not all implants can be removed this easily; occasionally the incision will need to be probed and the capsule grabbed. Using a forceps to grab the fibrous tissue over the implant, it may be necessary to nick this tissue prior to removing the implant. Occasionally it is difficult to grab the implant with the forceps and manipulating the skin and implant to an area over the forceps may be easier than fishing for the capsule. Other techniques have been described for Norplant removal and are summarized in Table 27.7. After all the capsules are removed, a Steri-Strip should be applied and the incision dressed with sterile gauze.
|
|
|
TABLE 27.7. Norplant removal techniques |
SUMMARY POINTS
· Many gynecologic procedures can be performed in an office setting as they require minimal anesthesia and have minimal risk of complication.
· Performance of office procedures requires a clinician with sufficient training and experience and a facility with proper capabilities and appropriate staffing.
· The facility should allow for easy access, have an electronic table capable of comfortable patient positioning, and have available appropriate medical instrumentation required for local anesthesia and conscious sedation.
· Procedures that can be performed in the office include saline infusion sonography, intrauterine device placement, subcutaneous implant placement, dilation and curettage, hysteroscopy, endometrial ablation, and microlaparoscopy.
SUGGESTED READINGS
Anesthesia
Barash PB, Cullen BF, Stoelting RK. Clinical anesthesia. In: Anesthesia for Thoracic Surgery, 994.
Cohen MM, Duncan PG, Tate RB. Does anesthesia contribute to operative mortality? JAMA 260:2859, 1988.
Duke JC. Education Module for nonanesthesiologists providing sedation and analgesia for diagnostic and therapeutic procedures. Denver Health Department of Anesthesiology, Denver Colorado.
Hysteroscopy
Bieber EJ. Distention media. In: Bieber EJ, Loffer FD eds. Gynecologic resectoscopy. Cambridge, MA: Blackwell Science, 1995:62.
Cohen MR, Dmowski WP. Modern hysteroscopy: diagnostic and therapeutic potential. Fertil Steril 1973;24:905.
Salat-Baroux J, Hamou JE, Maillard G. Complications from microhysteroscopy. In Siegler A, Lindemann HJ, eds. Hysteroscopy: principles and practices.Philadelphia: JB Lippincott Co, 1984:112.
Microlaparoscopy
Almedia OD, Val-Gallas JM. Conscious pain mapping. J Am Assoc Gynecol Laparosc 1997;4:587–590.
DeQuattro N, Hilbert M, Buller J, et al. Microlaparoscopic tubal ligation under local anesthesia. J Am Assoc Gynecol Laparosc 1998;5:55–58.
Faber BM, Coddington CC III. Microlaparoscopy: a comparative study of diagnostic accuracy. Fertil Steril 1997;67:952–954.
Milki AA, Tazuke SI. Office laparoscopy under local anesthesia for gamete intrafallopian transfer: technique and tolerance. Fertil Steril 1997;68:128–132.
Ory HW. Women's Health Study: ectopic pregnancy and intrauterine contraceptive devices: new perspectives. Obstet Gynecol 1981;57:137–144.
Palter S. Office microlaparoscopy under local anesthesia. Obstet Gynecol Clin North Am 1999;26:109–120, vii.
Palter SF, Olive DL. Office laparoscopy under local anesthesia for chronic pelvic pain: utility, acceptance, and cost-benefit analysis. J Am Assoc Gynecol Laparosc 1996;3:359–364.
Dilation and Curettage
Gimpelson RJ, Rappold HO. A comparative study between panoramic hysteroscopy with directed biopsies and dilatation and curettage. Am J Obstet Gynecol1988;158:489–492.
Goldstein SR. Use of ultrasonohysterography for triage of perimenopausal patients with unexplained uterine bleeding. Am J Obstet Gynecol 1994;170:565–570.
Grimes DA. Diagnostic dilation and curettage: a reappraisal. Am J Obstet Gynecol 1982;142:1–6.
Randolph JF, Ying YK, Maider DB, et al. Comparison of real-time ultrasonography, hysterosalpingography, and laparoscopy/hysteroscopy in the evaluation of uterine abnormalities and tubal patency. Fertil Steril 1986;46:828–832.
Endometrial Ablations
Aberdeen Endometrial Ablations Trials Group. Br J Obstet Gynecol 1999;106:360–366.
Novasure System. Available at: http://www.Novacept.com. Accessed January 13, 2003.
Saline Infusion Sonography
Alatas C, Aksoy E, Akarsu C, et al. Evaluation of intrauterine abnormalities in infertile patients by sonohysterography. Hum Reprod 1997;12:487–490.
Cicinelli E, Romano F, Anastasio PS, et al. Transabdominal sonohysterography, transvaginal sonography, and hysteroscopy in the evaluation of submucous myomas. Obstet Gynecol 1995;85:42–47.
Dietrich M, Suren A, Hinney B, et al. Evaluation of tubal patency by hysterocontrast sonography (HyCoSy, Echovist) and its correlation with laparoscopic findings. J Clin Ultrasound 1996;24:523–527.
Fan P, Czuwala PJ, Nanda NC, et al. Comparison of various agents in contrast enhancement of color Doppler flow images: an in vitro study. Ultrasound Med Biol 1993;19:45–47.
Holte J, Rasmussen C, Morris J. First clinical experience with sonicated human serum albumin (Albunex) as an intrafallopian ultrasound contrast medium. Ultrasound Obstet Gynecol 1995;6:62–65.
Keltz MD, Olive DL, Kim AH, et al. Sonohysterography for screening in recurrent pregnancy loss. Fertil Steril 1997;67:670–674.
Kennedy S. Transvaginal hysterosonogram, a means of evaluating the endometrium in postmenopausal women. J Diag Med Sonography 1998;12;34–38.
Laughead MK, Stones LM. Clinical utility of saline solution infusion sonohysterography in a primary care obstetric-gynecologic practice. Am J Obstet Gynecol1997;176:1313–1316.
Parsons AK, Lense JJ. Sonohysterography for endometrial abnormalities: preliminary results. J Clin Ultrasound 1993;21:87–95.
Intrauterine Devices
Heartwell SF, Schlesselman S. Risk of uterine perforation among users of intrauterine devices. Obstet Gynecol 1983;61:31–36.
Nelson A. Contraceptive procedures in the office setting. Infertil Reprod Med Clin North Am 1999:63–88.
Nelson AL. Patient selection key to IUD success. Contemp Obstet-Gynecol 1995;40:49–62.
Nelson AL, Sulak PJ. IUD patient selection and practice guidelines. Dialog Contracept 1998;5:7–12.
Ory HW. Women's Health Study: ectopic Pregnancy and intrauterine devices: new perspectives. Obstet Gynecol 1981;57:137–144.
Sivin I, Schmidt F. Effectiveness of IUDs: a review. Contraception 1987;36:55–84.
White MK, Ory HW, Rooks JB et al. Intrauterine device termination rates and the menstrual cycle day of insertion. Obstet Gynecol 1980;55:220–224.
Wilson JC. A prospective New Zealand study of fertility after removal of copper intrauterine device for contraception and because of complications: a four year study. Am J Obstet Gynecol 1989;160:391–396.
Norplant
Darney PD, Klaisle CM. How to remove contraceptive implants. Contemp Obstet Gynecol 1995;Jan:52–65.
Darney PD, Klaisle CM, Walker DM. The pop-out method of Norplant removal. Adv Contracept 1992;8:188–189.
Glauser SJ, Scharling ES, Stovall TG, et al. Ultrasonography: usefulness in localization of the Norplant contraceptive implant system. J Ultrasound Med1995;14:411–413.
Klavon SL, Grubb GS. Insertion site complications during the first year of Norplant use. Contraception 1990;41:27–37.
Miller L, Grice J. Intradermal proximal field block: an innovative anesthetic technique for levonorgestrel implant removal. Obstet Gynecol 1998;91:292–297.
Praptohardjo U, Wibowo S. The “U” technique: a new method for Norplant implants removal. Contraception 1993;48:526–535.
Rosenberg MJ, Alvarez F, Barone MA, et al. A comparison of “U” and standard techniques for Norplant removal. Obstet Gynecol 1997;89:168–173.
Sarma SP, Hatcher R. The Emory method: a modified approach to Norplant implant removal. Contraception 1994;49:551–556.
Shihata AA, Salzetti RG, Schnepper FW, et al. Innovative technique for Norplant implants removal. Contraception 1995;51:83–85.
Shoupe D, Mishell DR. Norplant: subdermal implant system for long-term contraception. Am J Obstet Gynecol 1989;160:1286–1292.
Twickler DM, Schwarz BE. Imaging of the levonorgestrel implantable contraceptive device [Letter]. Am J Obstet Gynecol 1992;167:572–573.