Frederick Larsen
Historically, assessment of abnormal physical findings in the gynecologic patient was limited to rudimentary plain film x-rays or exploratory surgery. Today, there are multiple diagnostic modalities including ultrasonography (US), computed tomography (CT), and magnetic resonance imaging (MRI) that can be used in the evaluation of gynecologic disorders. This chapter emphasizes the use of US for the initial evaluation of the most common gynecologic disorders for which imaging is indicated. The roles of MRI and CT are also briefly mentioned in this chapter as adjunctive tests in circumstances where sonography is nondiagnostic, or as a means to enhance diagnostic accuracy.
The use of gynecologic sonography has become widespread in gynecologists' offices and in emergency and radiology departments. Its accessibility and high patient acceptance make it applicable as an initial means for assessing many gynecologic disorders. Some practitioners have incorporated transvaginal sonography (TVS) in their routine pelvic assessment, even using it as a surrogate for a pelvic examination, particularly when the patient is obese. Others use it as a problem-solving tool only when a gynecologic disorder is suspected. Without commenting on the wisdom of following either pathway, it can be said that the US machine has become an extremely useful tool found in many, if not most, practitioners' offices. TVS is operator-dependent, and significant clinical experience with pathoanatomic correlation is required for effective use. For those who do not routinely perform pelvic sonograms as part of their practice, but rather order them, it is crucial that they have a working understanding of not only the lexicon of US but also at least a rudimentary ability to interpret the images that are collected.
In selected cases in which standard pelvic sonography is not diagnostic, however, MRI or CT may be used to better delineate anatomic abnormalities. Other advances in the use of pelvic US, such as saline infusion hysterosonography, have eliminated some of the indications for these more expensive examinations. These two imaging modalities are available only in diagnostic imaging departments and are more costly than TVS. However, their selective use may help improve the diagnostic evaluation, especially in disorders that may have only subtle sonographic findings such as adenomyosis. MRI and CT might be better suited for initial staging or workup of certain neoplasms because they can both better delineate retroperitoneal structures such as lymph nodes and images can be obtained in a variety of scan planes that may not be obtainable with US.
This chapter discusses and illustrates the common uses of these imaging modalities in evaluation of a variety of gynecologic disorders. The subsections are divided according to the most common indications for imaging evaluation of gynecologic disorders. Additional information can be found in several texts that provide more extensive coverage of this topic.
SONOGRAPHIC INSTRUMENTATION AND TECHNIQUE
A unique feature of US is that it allows orientation from an internal perspective rather than one based on external landmarks. In other words, the uterus, for example, can be viewed not just in cross-section but in its normal longitudinal orientation, much closer to the real anatomic orientation. US uses sound waves at various frequencies to allow imaging of internal organs or vessels. The sound waves emitted by the transducer are transmitted through the soft tissue and reflect off any perpendicular tissue/fluid interface and return (much like a sonar) to the transducer while a portion of the sound waves continue through until they encounter another perpendicular tissue/fluid interface and send back a reflected echo delayed in time. The US machine collates the information from the returning sound waves based on their return time and intensity and reconstructs a two-dimensional image. Both the origin of the signal, the transducer, and the receiver are contained in the same unit. Simplistically speaking, three-dimensional ultrasonography (3DUS) uses computer software to rapidly collate multiple two-dimensional images into a three-dimensional image.
The most commonly used probe or transducer configurations are those in which transducer elements are rotated (mechanical sector) and those that are made up of multiple send–receive sub-elements, in which the beam is formed by selective electronic activation (curvilinear or phased array). Other recent technologic advances allow newer US machines to make use of the physics principle known as the Doppler effect. This principle states that sound or light waves reflected by a moving object will undergo a change in frequency proportional to the relative velocity of that object, toward or away from the transducer. Detecting these frequency changes can help determine the blood flow through vessels coming to or from a structure being imaged.
US is particularly useful in defining the internal acoustic characteristics of a structure, thus distinguishing fluid-filled structures from solid structures. This makes US the imaging modality of choice in evaluating the ovary and any associated cysts or neoplasms. This imaging technique is not as well adapted to distinguish solid structures from other adjacent, or surrounding, solid structures. A perfect example of this is the ease at which an intrauterine gestational sac can be seen while a comparably sized intracavitary uterine polyp or fibroid can be quite difficult to distinguish from the adjacent endometrium or myometrium.
Diagnostic sonography of the pelvic organs can be performed using the transabdominal sonography (TAS) approach in which the uterus and adnexa are imaged through a distended urinary bladder or transvaginal sonography (TVS), in which the probe is inserted into the vagina for imaging of the uterus and ovaries. In general, the lower the frequency emitted by the US transducer, the further the penetration and the deeper the window of visibility. Therefore, TAS ordinarily uses lower frequency sound waves (3.5–5.0 MHz) to allow for the deeper penetration required to visualize underlying structures beneath a layer of subcutaneous and adipose tissue through the bladder. A TAS is useful in fully assessing the uterus if markedly enlarged or severely anteverted. Due to problems visualizing the pelvic organs through intervening tissues such as small and large bowel as well as the anterior abdominal wall, the transabdominal approach is best performed with a fully distended urinary bladder enabling a better global depiction of the uterus and adnexa (Fig. 28.1). Despite this, TAS is limited by body habitus and intervening bowel or fat that tend to increase artifact and scatter the incident US beam. In general, TAS is best used for large masses such as fibroid uteri that extend out of the pelvis above the urinary bladder. Occasionally, the ovaries of some women can be better imaged transabdominally than with a transvaginal probe, in particular those that are high in the pelvis, are adjacent to an enlarged uterus, and are very anteriorly located.
|
|
|
FIG. 28.1. Transabdominal sonography. A: Parasagittal image through right adnexal region showing right ovary (between cursors) and normal uterus. B:Parasagittal image in the transverse plane showing the transverse dimension of the right ovary (between cursors). |
TVS uses higher frequency sound (5–8 MHz) which allows higher image resolution at the sacrifice of not being able to penetrate and “see” clearly objects more distant than 10 cm. The higher frequency sound waves used in TVS give much better definition because of the closer proximity of the transducer to the structures being imaged, although there is limited penetration. TVS is also an optimal modality with which to image obese women who have a large amount of adipose tissue in the anterior abdominal wall because the US transducer is positioned immediately adjacent to the uterus and ovaries. For most applications a tightly curved transducer probe that has high line density affords the most detailed image (Fig. 28.2). It becomes increasingly difficult to see the fundal region of the uterus as the uterus leaves the pelvis, as in the case of the large fibroid uterus. By contrast, the transvaginal component of an examination of the uterus and associated fibroids can typically better establish the relationship or proximity of the fibroids to the endometrial cavity than can TAS alone. Visual clarity with TVS is usually superior when imaging ovarian abnormalities as compared to TAS and can also be helpful as a means of distinguishing between ovarian and uterine masses. In addition, TVS with Doppler sonography affords assessment of flow of vessels adjacent to and within the uterus and ovaries.
|
|
|
FIG. 28.2. Transvaginal sonography. A: Diagram showing transvaginal probe adjacent to cervix in a retroflexed uterus. (Drawing by Paul Gross, MS.) B:Picture of tightly curved curvilinear array transvaginal transducer probe. C: Flat-faced transvaginal probe with needle guide attached to the shaft. |
To perform TVS, the patient is placed in the lithotomy position. After the probe is wiped with a disinfectant, it should be covered by a latex sheath before insertion into the vagina. Nonlatex vinyl covers are also available for those women allergic to latex. For optimal patient comfort, the probe should be inserted into the vagina while the operator's finger gently depresses the posterior introitus. The orientation on the screen for TVS is by convention displayed with the apex of the image at the top of the monitor. A US examination must be thorough and reproducible; for this reason, most would suggest performing each US following the same order and same routine. A complete pelvic US examination begins with images of the uterus as the central pelvic landmark in both long and short axis. The probe can be withdrawn into the midvagina and directed anteriorly to provide short-axis views of a uterus that is anteflexed. The retroflexed uterus is easily imaged without major manipulation of the probe because it is in the anatomic plane of the vagina, though some vaginal probes angle the US beam superiorly making this somewhat more difficult or uncomfortable for the patient. The operator can then orient the probe into the adnexal regions using the internal iliac artery and vein as landmarks for delineation of the ovarian fossa. The normal ovary can usually be found within close proximity to the internal iliac artery and vein but there is substantial variation in the location of the ovaries, particularly in women who have undergone hysterectomy or who have enlarged ovaries. Typically, enlarged ovaries or ovaries with cysts are relatively easy to identify while the normal postmenopausal ovary might be more difficult to visualize. The operator can use one hand to mildly compress the abdominal wall and evaluate the mobility of these organs. If there are no adhesions, the uterus and ovaries should move smoothly away from each other as the probe is advanced. This has been termed the “sliding organ sign” and, if absent, may suggest the presence of agglutinating pelvic adhesions.
Transvaginal color Doppler sonography (TV-CDS) combines the anatomic information provided by TVS with flow information provided by CDS. This probe and attached equipment are more expensive than the standard TVS scanner and do not improve acoustic visualization; rather, they allow detection of flow within blood vessels. However, TV-CDS can provide additional information that is useful in evaluating some patients with pelvic masses (Fig. 28.3). The TV-CDS involves assessment of flow within the uterus and adnexal structures. The flow to or within a structure can be quantified by analysis of the waveform using either resistive index, which is maximum systolic velocity–minimum systolic velocity, divided by maximum systolic velocity. Alternatively, the pulsatility index, which is maximum systolic velocity–maximum diastolic velocity, divided by the mean velocity, can be used. These parameters are unitless values and angle-independent parameters of relative impedance to forward flow. One must obtain signals between 30 and 60 degrees of the angle of the vessel in order to provide optimal waveforms. Waveforms reflect the change in frequency over time, which is related to flow velocity (i.e., the Doppler effect). Standard, frequency-based color Doppler is encoded with red colors indicating flow toward the transducers or blue colors indicating flow away from the transducers. A new type of processing known as amplitude or power Doppler allows determination of overall blood flow. It is more sensitive than frequency-based measurements but is degraded by motion.
|
|
|
FIG. 28.3. Transvaginal color Doppler sonography (TV-CDS). A: Diagram showing the components of a TV-CDS, which include real-time imaging and display of vessels, with subsequent selection of sample volume for Doppler analysis by evaluation of the Doppler waveform. (Drawing by Paul Gross, MS.) B: TV-CDS showing low-impedance flow (resistive index = 0.45; pulsatile index = 0.60) within the wall of a corpus luteum. See color figure 28.3. |
The technique of TV-CDS is highly operator-dependent but can provide important information as to the character of the blood flow in the uterus and adnexal structures. Depending on the clinical indication, the examination should include evaluation of arterial and venous blood flow to and within the uterus and ovaries. There is a range of sensitivity to flow between scanners from different manufacturers and there is no minimal clinical standard.
Documentation of US studies performed, particularly in an office setting, represents a major issue. Hard copy images should be included as part of the patient's medical record. In the past, hard copy images or videotaping of the study were the only ways to objectively document what was found. More recently, many have begun digitalizing the images and storing them on optical or compact disk devices. This method of documentation and storage of US images has the advantage of being readily available for review without loss of image quality over time. When digital storage of images is used, there should always be safeguards in place to avoid loss or destruction of the information saved, a standard no different than what we should adhere to with hard copy images. US is, to some extent, subjective and attempts to document results of a US are incomplete without a narrative description of the overall impression by the operator.
While becoming more widely available and used in obstetric practice, the clinical value of 3DUS in gynecology over the standard technique has yet to be proven. It has been shown to be efficient and accurate in detecting müllerian abnormalities (Fig. 28.4) and shows promise in some urogynecologic applications. Some investigators have shown 3DUS volumetric measurements of embryonic pole and gestational sacs to be predictive of pregnancy outcome, while others have shown that 3DUS may enhance sensitivity in the diagnosis of ovarian neoplasms. It appears likely that 3DUS will be more frequently used in the future as its role is further clarified and accepted or proven to be of benefit in specific clinical circumstances.
|
|
|
FIG. 28.4. Three-dimensional ultrasound examination of a septate uterus. Upper left: Transverse view of the uterus at the plane indicated. Upper right:Uterus in the longitudinal plane. Lower left: Coronal section. Lower right: Composite three-dimensional rendering that can be manipulated with computer software in a variety of ways, enhancing diagnostic accuracy. |
Abnormal Uterine Bleeding
TVS has an important role in the evaluation of women of reproductive age presenting with unexplained uterine bleeding. TVS can help distinguish dysfunctional uterine bleeding (i.e., hormonally related) from mechanical or anatomic sources of abnormal bleeding (i.e., uterine leiomyomas, polyps, retained IUD, etc.). Because of the proximity of the transvaginal probe to the uterus, the endometrial and myometrial architecture can be accurately depicted in detail in most patients. However, high resolution delineation of the uterus requires proper imaging technique. For example, because the endometrium is not a precise geometric shape, operator error can account for over- or underestimation of its thickness. Thus, it is of utmost importance to orient the scan of the endometrium for measurement purposes in its greatest long-axis plane and maximal thickness in the fundal region, which optimizes its bi-layer measurement (Fig. 28.5). Saline infusion sonohysterography (SIS) has become an important and effective adjunct to standard TVS and replaced more costly procedures such as pelvic MRI. The endometrial cavity is a potential space where the opposing anterior and posterior uterine walls are normally in contact with, but not adherent to, each other. A fibroid or polyp within the endometrial cavity is often difficult to visualize on standard TVS because its US characteristics are similar to the contacting endometrium or myometrium. SIS uses saline as an acoustic contrast medium that distends the endometrial cavity and that enables visualization of any structures within the space in greater detail than with TVS alone where both uterine walls are in contact (Fig. 28.6). With saline infused into the cavity, the walls of the uterus separate and polyps or intracavitary fibroids that might otherwise have been missed are readily visualized. SIS also has been shown to be useful in evaluating müllerian abnormalities such as distinguishing uterine septa from a bicornuate uterus.
|
|
|
FIG. 28.5. Endometrial disorders. A: Diagram showing proximity of the endometrium of an anteflexed uterus to the transvaginal probe. The field of view depicting the long axis of the uterus and endometrium is shown. (Drawing by Paul Gross, MS.) See color figure 28.5A. B: Transvaginal sonogram showing multilayered endometrium typical of follicular phase endometrium. C: Typical secretory phase endometrium demonstrating increased thickness (between cursors) and homogeneous echogenicity. D: Echogenic mass (arrowhead) within endometrium containing punctate cystic area representing an endometrial polyp. |
|
|
|
FIG. 28.6. Saline infusion sonohysterography (SIS). A: Diagram showing intrauterine catheter used for distension of lumen with saline for detailed evaluation of the endometrium from the inside. (Diagram by Paul Gross, MS.) See color figure 28.6A. B: Standard transvaginal ultrasonography showing a secretory phase endometrial stripe. C: Same uterus evaluated with SIS revealing an anterior endometrial polyp not seen with standard sonography. D: SIS revealing intrauterine synechiae with saline having filled above and below the adhesion. On standard sonography the endometrial stripe appeared normal, with a 6-mm thickness. |
Clinically, it is important to remember that the differential diagnosis of premenopausal women presenting with bleeding is different from bleeding seen in postmenopausal women. In general, premenopausal bleeding is usually associated with anovulation or some mechanical factor such as intracavitary fibroids or endometrial polyps, whereas a variety of pathologies including atrophic endometritis, hyperplasia, and endometrial carcinoma are most common in the postmenopausal woman.
In women of childbearing age, the endometrial thickness varies according to the stage of the menstrual cycle. During menses, the normal endometrium is 3- to 5-mm thick with a mildly echogenic texture. Real-time examination of the endometrium while a patient is menstruating will often allow visualization of myometrial contractions associated with an efflux of solvent. As the endometrium proliferates in the periovulatory period, a multilayered texture can be seen with thicknesses ranging from 5 to 8 mm. The outer echogenic layer represents the basalis, whereas the inner layer is the enlarging functionalis. In the secretory phase, the endometrium becomes diffusely echogenic and enlarges up to 12 to 14 mm in thickness.
No specific US findings confirm anovulation as the cause of abnormal bleeding. In essence, all other potential anatomic or pathologic sources of bleeding must be excluded before arriving at the diagnosis of dysfunctional or anovulatory uterine bleeding. There are several US findings that are suggestive of an intracavitary abnormality that might be the source of abnormal bleeding such as a thickened endometrium, an endometrial stripe that is distorted, or an acoustic appearance that is not uniform or is heterogenous.
Uterine fibroids are clonal expansions that disrupt the normal arrangement of the myometrial bundles and are typically hypoechoic or of mixed echogenicity when compared to normal myometrium. Some fibroids contain calcifications that appear as areas of high acoustic reflection similar to that seen in bone. The pedicle of a subserosal fibroid can often be demonstrated during scanning and palpation of the mass relative to actual uterine body. The effect of submucosal fibroids on the endometrium can be assessed by visualizing the endometrial stripe in the area immediately adjacent to the fibroid. Submucosal fibroids typically displace and thin the overlying endometrium, something best visualized with SIS. Occasionally, fibroids may be present as solid masses in the adnexal regions, representing either interligamentary or pedunculated tumors. Endometritis usually produces a thickened endometrium sometimes surrounding intraluminal fluid but neither of these findings is pathognomonic. Intraluminal fluid may be seen in postmenopausal women and is usually a benign finding as long as the single-layer thickness of the endometrium is less than 4 mm. Intracavitary fluid collections due to a hematometra or pyometra may also be seen in the presence of cervical stenosis, particularly in the setting of secondary amenorrhea.
One of the more valuable roles of TVS is evaluating unexplained bleeding in the postmenopausal woman. Typically, an endometrial stripe thickness of less than 3 mm is observed in postmenopausal women not on hormone replacement therapy (HRT) and 2- to 3-mm thicker in those on HRT. In patients with a thickened or highly echogenic endometrium, TVS can suggest the presence of abnormal histology such as hyperplasia or endometrial polyps, but it is not histologically specific. That is to say, there is no endometrial stripe thickness above which carcinoma or hyperplasia is always found and conversely no thickness below which cancer is never encountered. Many studies have been published assessing whether there is an optimal cutoff below which one can safely presume a low likelihood of pathology and avoid invasive diagnostic procedures to assess endometrial histology. Earlier meta-analyses concluded that using 5 mm as the cutoff, irrespective of whether the patient was on HRT, resulted in a sensitivity of 92% in identifying any endometrial pathology and 96% for detecting carcinoma. An endometrial thickness of less than 5 mm was associated with a significantly reduced risk of an underlying carcinoma. More recent literature suggests that this 5-mm cutoff is not as reliable. For this reason, especially in the face of continued bleeding or in a high-risk patient, tissue sampling should always be considered.
Pelvic Mass
Sonography provides a means to evaluate the size, location, and internal acoustic characteristics of pelvic masses (Fig. 28.7). Larger masses (over 10 cm) may best be delineated using TAS. TVS provides important information about the location of the pelvic mass relative to the ovary and uterus and provides higher resolution for better delineation of the internal architectural characteristics compared with TAS. CDS can assess vascular integrity in cases of possible torsion or detect neovascularity, helpful in predicting whether a mass is benign or malignant. This is less frequently performed in an office setting due to the expense of a US unit with CDS capability and the high level of training required to perform CDS. A general outline of diagnostic considerations according to location and internal acoustic characteristics is shown in Table 28.1.
|
|
|
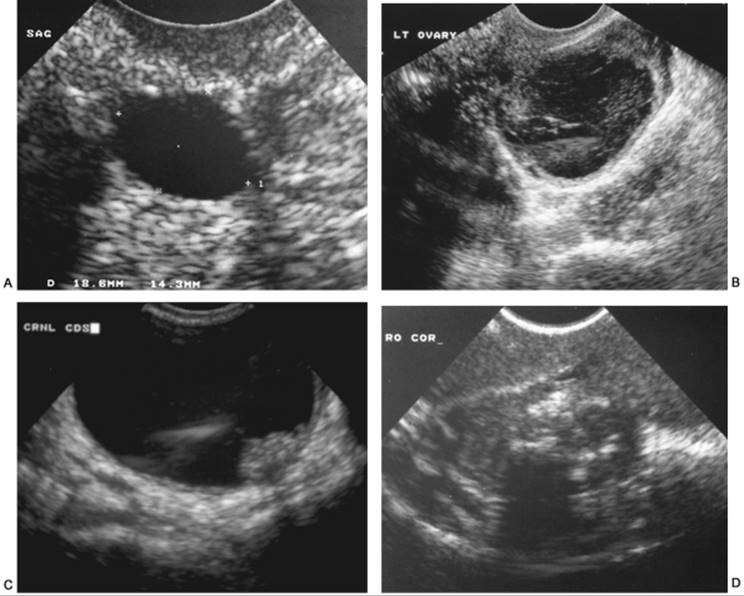
FIG. 28.7. Pelvic masses. A: Transvaginal sonogram of a smooth-walled cyst (between cursors) exhibiting the sonographic features consistent with a functional or physiologic cyst. B: Hemorrhagic corpus luteum with organized hemorrhage containing thin fibrin strands and internal echoes within the mass. C: Papillary excrescence arising from the wall of a mostly cystic ovarian mass. This morphologic feature is highly suggestive of cancer. D: Mass containing several echogenic foci and solid areas indicative of a dermoid cyst. |
|
|
|
TABLE 28.1. Differential diagnoses of pelvic masses by TAS and TVS |
Any woman of childbearing age can have a physiologic or functional “cyst” present when undergoing TVS. Most of these functional “cysts” demonstrate fluid free of internal echoes and smooth walls. The cysts have no internal septations and are typically less than 5 cm in size. In the follicular phase, there may be multiple unilocular cysts less than 2 cm in size that represent the pool of available developing follicles from which a dominant follicle is selected. Following ovulation, this dominant follicle becomes a corpus luteum, which is also typically a smooth-walled unilocular “cyst” but with more internal echoes. Labeling these physiologic structures “cysts” is the source of a great deal of unnecessary concern for women that can be best avoided by using terms such as “follicle” instead of “cyst” or by emphasizing the fact that these are completely normal findings in women of reproductive age. In the absence of abnormal or suspicious US findings or in the absence of symptoms such as continuing pelvic pain, repeat sonography of physiologic or functional-appearing cysts found on US is unnecessary.
Up to 15% of asymptomatic postmenopausal woman have been shown to have simple ovarian cysts with acoustic characteristics associated with benign histology. Indeed, one of the pitfalls of the readily available office US may be that incidental masses might be found in this age group, prompting unnecessary surgery. It has been shown that the risk of malignancy in unilocular cysts with a mean diameter less than 5 cm is very low in both premenopausal and postmenopausal women. Conservative management should therefore be the method of choice for women with such cysts identified by TVS. Larger “unilocular” simple cysts have been shown to have higher rates of actually having small papillations or internal growths that were undetectable by TVS and higher rates of malignancy, and thus warrant surgical excision
In the premenopausal woman, it is important to differentiate functional cystic masses that may spontaneously regress from ovarian neoplasms that will persist or continue to enlarge. Hemorrhagic corpus luteum cysts typically exhibit thin fibrin strands of echogenic material within a mostly hypoechoic mass contained by a somewhat thickened and irregular wall. On the other hand, the presence of a papillary excrescence or irregular and thickened internal septations is more indicative of ovarian neoplasms. The morphologic findings of early ovarian cancers can be subtle, but persistent internal septations with irregularity suggesting papillations, especially with any increase in peritoneal fluid, suggests the possibility of malignancy and warrants surgical intervention.
Although the sonographic appearance of masses are typically nonspecific and cannot give a precise diagnosis, there are a few patterns that demonstrate relatively high specificity. One of these is the “ground glass” appearance of an ovarian endometrioma, the other is the echogenic focus seen within benign cystic teratomas. With the improved resolution of modern US scanners, it is not uncommon to see small teratomas that appear as heterogenous echogenic regions within a normal ovary. If a dermoid cyst is found in one ovary, it is important to evaluate the contralateral ovary carefully because approximately 15% of patients have bilateral dermoid cysts.
The TV-CDS provides an adjunctive evaluation of patients with pelvic masses to help lessen the potential of the mass being malignant (Table 28.2). For best results, the TV-CDS findings need to be correlated with morphologic and clinical findings. Although the technique has some limitations, it is helpful in preoperative assessment of women with pelvic masses. Depending on the patient population studied, diagnostic accuracies in the 80% to 90% range have been reported. There is some overlap of impedance values between some functional and neoplastic ovarian cysts. Even so, in the proper clinical setting, TV-CDS improves the confidence in distinguishing benign from malignant lesions over that possible with TVS alone. Malignant lesions tend to have abnormally low-impedance flow, a sign of decreased vascular impedance seen in neovascularity of tumor vessels (see Fig. 28.3) with clusters of vessels in morphologically abnormal areas. The TV-CDS test has better sensitivity in the postmenopausal age group because the prevalence of ovarian cancer is higher at this age and because benign masses, which may also demonstrate low-impedance flow (pelvic inflammatory disease, endometriosis, or hemorrhagic corpora lutea), are far more prevalent in the premenopausal age group.
|
|
|
TABLE 28.2. Sonographic features of benign and malignant pelvic masses |
To date, no single screening test or combination of surveillance modalities has been shown in a well-conducted clinical trial or even through substantial indirect evidence to reduce ovarian cancer mortality. The major limiting factor in screening for ovarian cancer is its low prevalence. Methods that have been extensively investigated for ovarian cancer screening have included serum tumor markers, primarily serum CA125, and TVS. For women with a known germline mutation (BRCA1 or BRCA2) or with a family history suggestive of a significant possibility of a genetic predisposition to a heightened ovarian cancer risk, an effective screening strategy remains to be developed. Given the high risk in this population, most experts advocate multimodality screening with serum CA125 levels and TVS in patients who elect to delay or decline prophylactic oophorectomy.
Pelvic Pain
TVS plays an important role in evaluating patients with acute pelvic pain (Fig. 28.8). Demonstrably normal-appearing ovaries with no free intraperitoneal fluid on TVS virtually eliminate a primary ovarian source for acute pain. The uterus can be evaluated sonographically and pathologic causes of pelvic pain such as uterine fibroids, with or without degeneration, can be ruled out. TVS is relatively poor at identifying peritoneal endometriosis that is more commonly seen in the setting of chronic pain but is excellent at detecting ovarian endometriomas which can rupture and cause an acute exacerbation. If present, TVS can detect ovarian enlargement with a high degree of sensitivity. Care must be exercised, however, as presence of an enlarged ovary does not necessarily correlate with presence of symptoms. Tuboovarian abscesses can easily be visualized by TVS and the diagnosis considered in the presence of pelvic pain, fever, and complex adnexal masses.
|
|
|
FIG. 28.8. Pelvic pain. A: Composite transvaginal sonogram showing enlarged left ovary (top right and bottom left) without flow and associated with a paraovarian cyst in left adnexa (lower right). The right ovary (top left) was normal, showing intraparenchymal flow. The left adnexa was found to be twisted three times and was surgically untwisted with good result. See color figure 28.8A. B: Doppler sonogram of enlarged left ovary containing venous flow. This finding suggests potential viability of this partial ovarian torsion. C: Irregular echogenic area within myometrium suggestive of adenomyosis. D:Sagittal T2-weighted magnetic resonance image confirming the presence of adenomyosis in the fundal region. |
Ovarian torsion, a surgical emergency, must be eliminated as a cause of acute pelvic pain when a tender mass is noted on pelvic examination. TVS can confirm the presence of a complex adnexal mass and allow assessment of its size and internal acoustic characteristics. CDS provides additional useful information by determining whether there is normal blood flow to the ovary. Because venous flow is the first function affected by torsion, CDS is helpful in determining its presence or absence in an enlarged, edematous ovary. The absence of venous flow suggests the possibility of torsion in a properly performed CDS examination. It is important to examine flow in the contralateral ovary to confirm that the absence of flow is a real finding and not an artifact produced by improper color priority settings on the US machine. The CDS findings in ovarian torsion will also depend on the degree of vascular compromise and chronicity of this disorder. Intermittent ovarian torsion cannot be eliminated as a potential cause of pain even with demonstrable blood flow on CDS, though it will confirm the presence of a pelvic mass without which torsion is unlikely. CDS can also be used to confirm the reestablishment of flow after surgical detorsion. Isolated torsion of a paraovarian cyst is an infrequent event but is manifested on US by a cystic structure separate from, but adjacent to, the ovary that has absent or reversed diastolic flow.
One of the most common causes of acute pelvic pain is a hemorrhagic ovarian cyst. Blood within the hemorrhagic cyst can have several sonographic appearances. Fresh or acute bleeding within an ovarian cyst can appear echolucent. Organized clot has a more heterogenous and echogenic appearance. The hemorrhagic component typically demonstrates no flow, whereas the surrounding normal ovary has both arterial and venous flow. Free peritoneal fluid from a ruptured hemorrhagic cyst can also be observed and is certainly not rare as a cause of acute pelvic symptoms as blood is irritating to the peritoneal lining. Other ovarian neoplasms, such as endometriomas and benign cystic teratomas, can also rupture leading to peritoneal irritation accompanied by acute pelvic pain.
Often, pelvic pain originates in the uterus. Degenerating fibroids may cause severe midline pelvic pain most often seen during pregnancy. TAS or TVS can confirm the presence of fibroids though there is no specific US appearance of a fibroid with degeneration. However, the presence of fibroids on US does not necessarily mean that they are the cause of the pain as asymptomatic fibroids are quite prevalent in the general population. Adenomyosis is a cause of acute pelvic pain and may produce subtle findings that can be seen on TVS which include irregular echogenic areas in the subendometrial myometrium. Rarely, actual cystic spaces within the myometrium are seen. It can be difficult to distinguish adenomyosis or an adenomyoma from an intramural leiomyoma. The vascularity associated with adenomyosis is usually diffuse compared to that of a fibroid, but it can mimic the vascularity surrounding fibroids in appearance. Contrast-enhanced MRI has been most often used to detect the presence of adenomyosis.
When evaluating acute pelvic pain, one must also consider nongynecologic causes of pain such as appendicitis and renal calculi. An understanding of pathologic findings possible in these settings is important. On TAS, an inflamed appendix will appear as a noncompressible fusiform structure in the right lower quadrant that has a thickened (over 6 mm) wall. When ruptured, fluid may be seen surrounding the abnormal appendix. US can also detect hydronephrosis suggestive of ureteral obstruction that may accompany ureterolithiasis. In the hands of skilled operators, TAS may be able to localize renal calculi in the distal ureter in some patients; these will appear as a highly echogenic focus within the ureter. If a ureteral jet is clearly seen within the urinary bladder on CDS, ureteral patency can be confirmed and complete ureteral obstruction ruled out.
Ectopic Pregnancy
Prior to the advent of sensitive β-human chorionic gonadotropin (β-HCG) assays and US, the diagnosis of ectopic pregnancy was most often made after the tube had ruptured and the patient became hemodynamically unstable with an acute abdomen, necessitating immediate laparotomy. With TVS and sensitive β-HCG assays, ectopic gestations are often diagnosed prior to the onset of symptoms, making a ruptured ectopic pregnancy much less common and providing an opportunity for medical management with methotrexate. TVS provides an accurate means for detection of ectopic pregnancy (Fig. 28.9). An ectopic pregnancy will often not be observed on TVS, but its presence may be presumed based on the absence of an intrauterine gestation in the face of a quantitative β-HCG measurement above a “discriminatory zone,” generally (depending on the assay) around 2,000 mIU/mL. In identifying or evaluating an intrauterine fluid collection, care must also be taken to distinguish a true gestational sac from a collection of blood termed a “pseudosac.” Classically, a “double ring” sign within the uterine cavity is consistent with an intrauterine pregnancy (IUP) but the presence of either a yolk sac or fetal pole within the intrauterine fluid collection is diagnostic. There are certain clinical settings in which this discriminatory zone may be less reliable such as after a recent spontaneous abortion or where there is a multiple gestation. In the absence of assisted reproductive technologies (ARTs) (controlled ovarian hyperstimulation [COH] or in vitro fertilization), finding an IUP effectively eliminates the risk of ectopic pregnancy. In patients who have undergone controlled ovarian hyperstimulation or in vitro fertilization, heterotopic pregnancy rates are as high as 1 in 100.
|
|
|
FIG. 28.9. Ectopic pregnancy. A: Unruptured ectopic pregnancy appearing as a “tubal ring” in left adnexa. B: Transvaginal color Doppler sonogram showing vascularity of “tubal ring” of an unruptured ectopic pregnancy. See color figure 28.9. |
On TVS, ectopic pregnancy should be suspected in the presence of a cystic circular structure in the adnexa separate from the ovary in women in whom an IUP cannot be detected. The “tubal ring” is an indication of an unruptured ectopic pregnancy when not associated with surrounding fluid. One should be able to differentiate a corpus luteum or hemorrhagic ovarian cyst from an ectopic gestation in that the corpus luteum can be delineated to be within the contour of the ovary. Another finding associated with ectopic pregnancy is the presence of intraperitoneal fluid; indeed, this is one of the more sensitive findings in patients who will require surgical intervention. The presence of intraperitoneal fluid combined with an extraovarian adnexal mass in a pregnant patient without an intrauterine gestation should be viewed as a surgical emergency. Careful examination of the uterus with TVS can also help identify cornual and cervical ectopic pregnancies as well as aid in the diagnosis of abdominal pregnancy.
CDS may provide an additional means for delineation of ectopic pregnancies based on blood flow. The CDS provides a vascular “road map” separating the ovary from other adnexal structures. The vascularity of ectopic pregnancies varies from hypovascular to hypervascular depending on the viability of the ectopic gestation. The “tubal ring” of an ectopic pregnancy will most often have increased vascularity with blood flow present circumferentially, or nearly so. If present, this “ring of fire” is highly suggestive of ectopic pregnancy. While there are no specific or unique waveforms that arise from ectopic pregnancies, a waveform showing reversed diastolic flow can be seen in ectopic pregnancies with necrotic trophoblastic tissue.
Infertility
TVS can provide important information in the evaluation of the infertile patient (Fig. 28.10) and is indispensable in the management of COH induced by parenteral gonadotropins necessary for modern ARTs such as in vitro fertilization. During COH, TVS is used in the serial assessment of follicular maturity as well as for the evaluation of the thickness and texture of endometrium. The number of follicles and their size can be determined, with mature preovulatory follicles measuring between 18 and 20 mm. In the periovulatory period, the endometrial thickness is typically 7 to 11 mm and a trilaminar appearance of the endometrial stripe has been associated with higher rates of implantation. Prior to the widespread use of TVS for oocyte retrieval, egg collection from mature follicles was accomplished by laparoscopy under general anesthesia. Today, oocyte retrieval is routinely accomplished by a TVS-guided, multi-follicle aspiration. In addition, TVS or TAS is used to monitor the transfer of embryos to the uterus at the completion of an in vitro fertilization cycle.
|
|
|
FIG. 28.10. Infertility. A: Mature follicle (between cursors) containing a small protrusion from the posterior wall representing the cumulus oophorus. B:Image taken during follicular aspiration showing echogenic needle tip within deflating mature follicle. C: Classic appearance of ovary seen in women with polycystic ovarian syndrome (“string of pearls”). |
More recently, various investigators have used TVS in conjunction with uterine cannulation as a screening tool for assessing the endometrial cavity and tubal patency. Using various contrast media (including saline, as in SIS), the endometrial cavity can be evaluated for the presence of fibroids or polyps that may result in subfertility as well as for müllerian abnormalities such as a uterine septum often associated with recurrent miscarriage. In conjunction with SIS, the escape of saline out the fimbriated end of the tube is readily apparent in women with patent fallopian tubes as the cul-de-sac fills rapidly with fluid. The presence of cul-de-sac fluid during or after SIS confirms that at least one fallopian tube is patent. Attempts have been made to use CDS to assess in real time the efflux of echogenic contrast from each fallopian tube, with varying degrees of success.
SONOGRAPHICALLY GUIDED PROCEDURES
US can be very useful in assisting in difficult gynecologic procedures, particularly those involving the uterus. In cases in which dilation of the uterine cervix has been unsuccessful or more difficult than usual, simultaneous TVS or TAS can decrease the risk of uterine perforation and creation of a false tract. If perforation of the uterus is suspected, the path that the dilator or curette has followed, and its tip, can be readily visualized using sonography, as long as the instrument has not been moved once perforation is suspected. Traditionally, the internal US transducer was placed in the rectum or the abdominal transducer used to assist in directing the dilator as it traversed the cervix or confirmed the correct path to take. With the smaller transducers found on most vaginal US probes today, the transducer can usually be placed next to the cervix through an open speculum, particularly in patients whose cervix is flush with the vagina as in postmenopausal patients, or in those who have undergone cervical conization. Once the dilator is through the internal cervical os, TVS or TAS can localize the dilator or curette within the uterine cavity. Real-time monitoring of the procedure can virtually eliminate the risk of uterine perforation. US can also be helpful in monitoring a curettage being performed for the surgical management of either an incomplete miscarriage or early pregnancy termination. A US done at the end of the procedure can decrease the likelihood of the patient needing a second procedure at a later date by identifying those with an inadequate curettage. TAS monitoring of a mid-trimester abortion is critical to ensure complete evacuation of the uterine cavity and to decrease the likelihood of significant uterine or other organ injury. TAS can also be used to ensure correct placement of a uterine tandem being used for local radiation treatment of cervical or uterine cancer.
TVS can provide real-time delineation of the location of a needle relative to an area of interest within the ovary or adjacent structures (Fig. 28.11). For this purpose, a needle guide with an internal opening can be attached to the shaft of the vaginal transducer, which confines the course of the needle to a prescribed path in the exact plane of the two-dimensional scan. The most common use of this technique is transvaginal oocyte retrieval during an in vitro fertilization cycle, which is accomplished by aspirating individual follicles under direct US guidance. Cystic ovarian or adnexal masses may also be drained in this manner. Ovarian or adnexal masses that are amenable to transvaginal drainage include endometriomas (at the start of a controlled ovarian hyperstimulation cycle or when needed for the short-term relief of acute pain), symptomatic yet relatively small simple ovarian cysts (where there is no concern for malignancy), or hydrosalpinges (at the time of transvaginal oocyte retrieval for an in vitro fertilization cycle, particularly for those in whom surgical intervention is relatively contraindicated). Likewise, tuboovarian abscesses may be drained using the TVS-guided approach. In the case of endometriomas or hydrosalpinges, it is unlikely that transvaginal drainage will be curative, as they typically reaccumulate over time. If a cyst is drained and subsequently reaccumulates, only surgical excision will be curative.
|
|
|
FIG. 28.11. Sonographically guided procedures. A: Guided aspiration of complex mass representing tuboovarian abscess. The needle tip is echogenic and within the abscess cavity. The patient defervesced after the procedure. B: Guided aspiration of large endometrioma. Note the classic “ground glass” appearance. The needle tip is easily seen within the mass. C: Transrectal sonography guidance for dilation and curettage in a patient with cervical stenosis. The curette is clearly within the lumen of the uterus. |
OTHER IMAGING MODALITIES
MRI is an excellent, albeit expensive modality for secondary evaluation of a variety of pelvic disorders. These include adenomyosis, endometriosis, and certain pelvic masses such as benign cystic teratomas. The MRI provides global depiction of pelvic structures in selectable imaging planes, and it can identify lymphadenopathy associated with tumors. MRI can be particularly helpful in certain cases where it is not altogether clear if a pelvic mass originates from the ovary or from the uterus on physical examination or on US. MRI is also useful in clarifying müllerian abnormalities such as the bicornuate or septate uterus, although SIS appears to be equally effective. Enhanced MRI can also be helpful in assessing the extent of myometrial invasion in patients with endometrial cancer.
CT scanning is particularly helpful in the evaluation of the bony pelvis and has improved resolution and reduced scan times compared with MRI. Either MRI or CT may be used to delineate intraabdominal abscesses, though CT is often more readily available and less expensive. The presence of a rim-enhancing mass is diagnostic of an abscess.
SUMMARY POINTS
· Transabdominal and transvaginal scanning are both useful in establishing the source of abnormal uterine bleeding, characterizing pelvic masses found on physical examination, evaluating acute pelvic pain, diagnosing ectopic pregnancies, and assessing and treating infertility.
· Advances in technology such as higher transducer frequencies for improved resolution, rapid computerized assembly of two-dimensional images to yield virtual three-dimensional images, and smaller equipment have fostered wider clinical applications and made office use routine.
· US guidance during gynecologic surgical procedures has proved very useful in making difficult intrauterine procedures safer and diagnosing and treating selective pelvic masses by needle aspiration. It is the single most important advance in collecting oocytes for in vitro fertilization.
· Saline infusion sonohysterography has improved the diagnostic capability of TVS in circumstances of abnormal uterine bleeding.
· Pelvic US is the initial diagnostic modality of choice in most circumstances, whereas secondary tests such as CDS, MRI, and CT scanning provide a means to further enhance diagnostic specificity in difficult or nondiagnostic US studies.
SUGGESTED READINGS
Callen PW. Ultrasonography in obstetrics and gynecology, fourth ed. New York: Elsevier, 2000.
Reece EA. Fundamentals of obstetric and gynecologic ultrasound. Norwalk, CT: Appleton & Lange, 1994.
Smelka R, Reinhold C, Ascher S. MRI of abdomen and pelvis. New York: Wiley, 1997.
Thurman A, Jones M, Cohen D. Gynecologic obstetric and breast imaging. Baltimore: Williams & Wilkins, 1997.
Sonographic Instrumentation and Technique
Baba K, Jurkovic D, eds. Three-dimensional ultrasound in obstetrics and gynecology. New York: Parthenon Publishing Group, 1997:1–110.
Babinszki A, Nyari T, Jordan S, et al. Three-dimensional measurement of gestational and yolk sac volumes as predictors of pregnancy outcome in the first trimester. Am J Perinatol 2001;18:203–211.
Granberg G, Karlsson B, Wikland M, et al. Transvaginal sonography of uterine and endometrial disorders. In: Fleischer A, ed. Sonography in Ob-Gyn: principles and practice. Stamford, CT: Appleton & Lange, 1996:851–868.
Jurkovic D, Geipel A, Gruboeck K, et al. Three-dimensional ultrasound for the assessment of uterine anatomy and detection of congenital uterine anomalies. A comparison with hysterosalpingography and two-dimensional sonography. Ultrasound Obstet Gynecol 1995;5:233–237.
Jurkovic D. Three-dimensional ultrasound in gynecology: a critical evaluation. Ultrasound Obstet Gynecol 2002;19:109–117.
Timor-Tritsch I. Transvaginal sonography. New York: Elsevier, 1988:24.
Abnormal Uterine Bleeding
Bombieri L, Hogston P. Endometrial carcinoma with an endometrial thickness of 3.2 mm on vaginal ultrasonography. J Obstet Gynecol 1995;15:421–422.
Dueholm M, Lundorf E, Hansen ES, et al. Evaluation of the uterine cavity with magnetic resonance imaging, transvaginal sonography, hysterosonographic examination, and diagnostic hysteroscopy. Fertil Steril 2001;76:350–357.
Ferrazzi E, Torri V, Trio D, et al. Sonographic endometrial thickness: a useful test to predict atrophy in patients with postmenopausal bleeding. An Italian Multicenter Study. Ultrasound Obstet Gynecol 1996;7:315–321.
Goldstein RB, Bree RL, Benson CB, et al. Evaluation of the woman with postmenopausal bleeding: Society of Radiologists in Ultrasound—sponsored consensus conference statement. J Ultrasound Med 2001;10:1025–1036.
Langer RD, Pierce JJ, O'Hanlan KA, et al. Transvaginal ultrasonography compared with endometrial biopsy for the detection of endometrial disease. Postmenopausal estrogen/progestin intervention trial. N Engl J Med 1997;337:1792–1798.
Smith-Bindma R, Kerlikowske K, Feldstein VA, et al. Endovaginal ultrasound to exclude endometrial cancer and other endometrial abnormalities. JAMA1998;280:1510–1517.
Tabor A, Watt HC, Wald NJ. Endometrial thickness as a test for endometrial cancer in women with postmenopausal bleeding. Obstet Gynecol 2002;99:663–670.
Pelvic Mass
Ekerhofd E, Wienerroith H, Staudach A, et al. Preoperative assessment of unilocular adnexal cysts by transvaginal ultrasonography: a comparison between ultrasonographic morphologic imaging and histopathologic diagnosis. Am J Obstet Gynecol 2001;184:48–54.
Fleischer A, Cullinan J, Peery C, et al. Early detection of ovarian carcinoma with transvaginal color Doppler ultrasonography. Am J Obstet Gynecol1996;174:101–106.
Hata K, Hata T, Manabe A, et al. A critical evaluation of transvaginal Doppler studies, transvaginal sonography, magnetic resonance imaging, and CA125 in detecting ovarian cancer. Obstet Gynecol 1992;80:92.
Levine D, Gosink B, Wolf S, et al. Simple adnexal cysts: the natural history in postmenopausal women. Radiology 1992;184:653–659.
Paley, Pamela J. MD. Screening for the major malignancies affecting women: current guidelines. Am J Obstet Gynecol 2001;184:1021–1030.
Smith-Bindma R, Kerlikowske K, Feldstein VA, et al. Endovaginal ultrasound to exclude endometrial cancer and other endometrial abnormalities. JAMA1998;280:1510–1517.
Soper JT. Radiographic imaging in gynecologic oncology. Clin Obstet Gynecol 2001;44:485–494.
Pelvic Pain
Eskenazi B, Warner M, Bonsignore L, et al. Validation study of nonsurgical diagnosis of endometriosis. Fertil Steril 2001;76:929–935.
Fleischer A, Stein S, Cullinan J, Warner M. Color Doppler sonography of adnexal torsion. J Ultrasound Med 1995;14:523–528.
Molander P, Paavonen J, Sjoberg J, et al. Transvaginal sonography in the diagnosis of acute appendicitis. Ultrasound Obstet Gynecol 2002;20:496–501.
Rheinhold C, McCarthy S, Bret PM, et al. Diffuse adenomyosis: comparison of endovaginal US and MR imaging with histopathologic correlation. Radiology1996;199:151–158.
Ectopic Pregnancy
Emerson DS, Cartier MS, Altieri LA, et al. Diagnostic efficacy of endovaginal, color Doppler flow imaging in an ectopic pregnancy screening program. Radiology 1992;183:413–420.
Gamzu RI, Almog B, Levin Y, et al. The ultrasonographic appearance of tubal pregnancy in patients treated with methotrexate. Hum Reprod 2002;17:2585–2587.
Rogers RG, Kammerer-Doak D, Miller M, et al. A comparison of ultrasound and surgical findings in suspected ectopic pregnancy. J Diagn Med Sonogr2000;16:60–64.
Sadek AL, Schiotz HA. Transvaginal sonography in the management of ectopic pregnancy. Acta Obstet Gynecol Scand 1995;74:293–296.
Infertility
Brown SE, Coddington CC, Schnorr J, et al. Evaluation of outpatient hysteroscopy, saline infusion hysterosonography, and hysterosalpingography in infertile women: a prospective, randomized study. Fertil Steril 2000;74:1029–1034.
Fleischer AC, Vasquez JM, Cullinan JA, et al. Sonohysterography combined with sonosalpingography: correlation with endoscopic findings in infertility patients. J Ultrasound Med 1997;16:381–384.
Inki P, Palo P, Anttila L. Vaginal sonosalpingography in the evaluation of tubal patency. Acta Obstet Gynecol Scand 1998;77:978–982.
Prefume F, Serafini G, Martinoli C, et al. The sonographic evaluation of tubal patency with stimulated acoustic emission imaging. Ultrasound Obstet Gynecol2002; 20:386–389.