Julia Johnson
Infertility affects approximately 14% of couples and is a medical concern for 2.7 million women of reproductive age in the United States. Over the past decade, successful treatments for virtually all causes of infertility have been developed, offering hope for couples with this medical condition. Unfortunately, many states continue to offer limited insurance coverage for infertility minimizing effective diagnosis and treatment despite evidence that providing infertility care does not increase insurance costs. It is the goal of this chapter to identify the basic diagnostic testing for couples with infertility that can allow the couple to rapidly move on to proven therapeutic options. Prompt diagnosis and effective treatment will maximize the opportunity for conception while minimizing the cost of infertility care.
Infertility is defined as 1 year of unprotected intercourse without conception. Fecundability is the chance of conception in one menstrual cycle, and per cycle fecundity is commonly used to identify the success rate of an infertility treatment. It is expected that approximately 25% of healthy young couples will conceive in a single cycle, although clearly the chance of conception drops throughout the first year without contraception. The per cycle fecundity falls below 10% after 7 cycles and only 3% of couples conceive during the 12th cycle. Although it is reasonable to wait 1 year to begin the infertility evaluation for young couples with no history suggestive of reproductive disorders, it is reasonable to begin the workup sooner in couples with a positive history for a fertility-lowering disease or advancing age. Decreased fecundity begins for women in the mid-30s, making it reasonable to begin the diagnosis and treatment of infertility for this age group following 6 months of unsuccessful attempts at pregnancy. When one or both members of the couple have a history suggestive of a disorder potentially altering reproduction, the diagnostic testing of infertility should begin immediately. Thus, it is critical for the obstetrician-gynecologist to consider both the history and physical examination of both members of the couple as well as advanced maternal age when deciding when to begin the infertility evaluation.
The increased diagnostic techniques and available treatments for infertility have raised the concern that infertility is a new disorder, increased by the exposure of men and women to environmental factors or high-risk behavior. Although the advancing age of the first pregnancy in our society does increase the risk of infertility, the primary explanation for advancing infertility treatment is the increased awareness of this disorder by patients. It is now socially acceptable for men as well as women to seek treatment for infertility. As patients continue to increase their knowledge of this disorder and learn of successful therapies, providers will increasingly be asked to provide prompt diagnosis and effective treatment.
EVALUATION: INITIAL ASSESSMENT
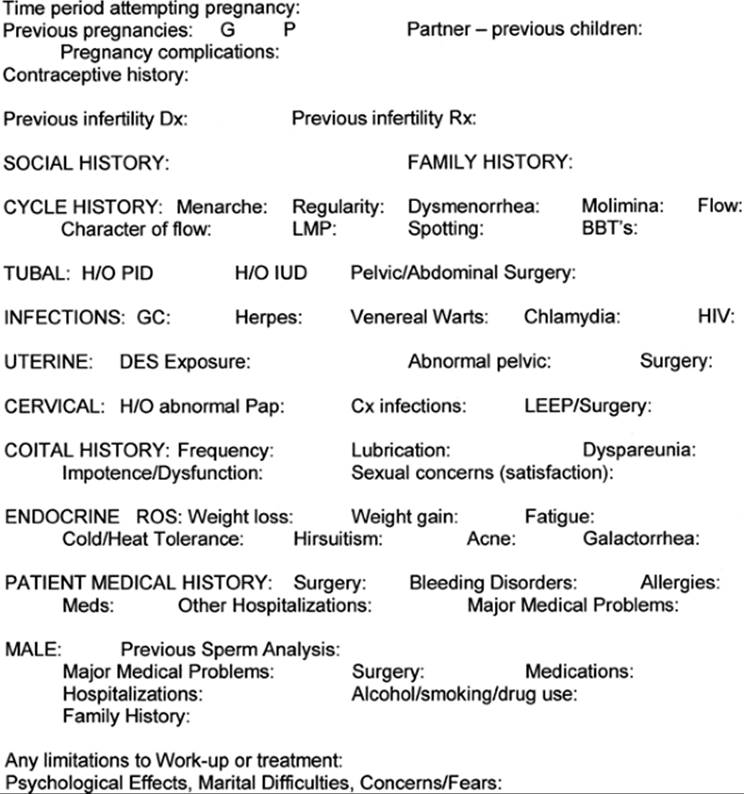
As with all medical problems, the first step in the evaluation of infertility is a thorough medical history and physical examination. Figure 38.1 demonstrates the history form used by the Reproductive Endocrinology and Infertility Division at the University of Vermont. Ovulation dysfunction, tubal risk factors, uterine and cervical abnormalities, peritoneal factors, and male factors are often identified at the initial visit. It is important for both members of the couple to be interviewed at this first meeting with the health care provider.
|
|
|
FIG. 38.1. Infertility history form. |
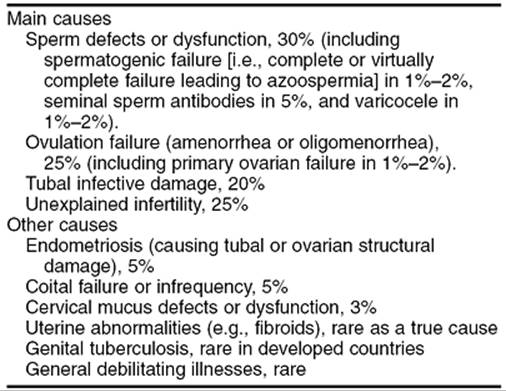
The known causes of infertility and their incidences are listed in Table 38.1. The history should explore for ovulatory dysfunction by examining the age of menarche, cycle length, history of increased or decreased intervals between cycles, and physical symptoms of ovulation and hormone production such as mittelschmerz and premenstrual molimina. If ovulatory dysfunction is identified, an endocrine review of systems is valuable to determine the etiology of the irregular menses. Information regarding thyroid symptoms, androgen excess, marked weight changes, and galactorrhea should be obtained. Signs of decreased ovarian function, such as shortened menstrual cycle length, new onset of irregular cycles, or hot flashes can indicate a contributing factor to infertility. The menstrual history may also point to other causes of infertility. Worsening dysmenorrhea, intermenstrual bleeding, and menorrhagia may point to diseases in the pelvic peritoneum or uterus.
|
|
|
TABLE 38.1. Causes of infertility and their approximate frequencies |
Risk factors for tubal factor infertility have been shown to be excellent predictors of tubal damage. A history of sexually transmitted diseases (STDs), pelvic inflammatory disease, pelvic surgery, ruptured appendix, septic abortion, endometriosis, and ectopic pregnancy can point to a heightened risk of tubal factor infertility. A history of uterine leiomyoma or uterine and cervical surgery may also affect fertility. The abdominal and pelvic exam can identify pelvic masses, cul-de-sac nodularity, irregular uterine contour, and fixed pelvic structures, suggestive of tubal damage or peritoneal disease.
The history from the male partner is crucial, as sperm abnormalities account for 30% to 40% of infertility. STDs and other genitourinary infections, chemotherapy or radiation therapy, mumps during adolescence, testicular surgery or injury, and decreased ejaculatory function suggest reasons for infertility. Chronic exposure to extreme heat may alter sperm motility and exposure to gametotoxic chemicals, such as the nematocide dibromocloropropane, may affect sperm production. Certain medications, such as cimetidine and sulfasalazine, are associated with decreased sperm production. Cystic fibrosis is associated with bilateral absence of the vas deferens. An examination of the male partner, either by the obstetrician-gynecologist or a medical colleague, is critical.
Abnormal body habitus, lack of testicular descent, penile abnormalities, diminished size and consistency of the testes, and the presence of a varicocele may offer explanations for infertility.
Medical histories and family histories from the couple are important to identify factors that may complicate pregnancy. Preconceptual counseling is typically recommended for women with a history of diabetes, hypertension, heart disease, autoimmune diseases, severe pulmonary disease, breast or gynecologic cancer, and infectious diseases such as human immunodeficiency virus (HIV) and hepatitis. The use of medications, particularly those associated with fetal malformations such as isotretinoin for severe cystic acne, should be considered. Carrier screening can be offered for inherited disorders, such as cystic fibrosis, Tay-Sachs, thalassemia, and sickle cell anemia, based on the risk profile for each couple. A family history of genetic disorders such as fragile X and Down syndrome (trisomy 21) may lead to a need for genetic counseling. Women anticipated to be over the age of 35 at delivery should receive information about diagnostic testing during pregnancy by chorionic villus sampling and amniocentesis. The American College of Obstetricians and Gynecologists (ACOG) technical bulletin on preconceptional care is a valuable tool for all providers evaluating couples with infertility.
The social and lifestyle history is also very important for the infertile couple. Smoking, alcohol abuse, and drug abuse have an adverse effect of fertility in both men and women. Smoking is particularly harmful as it is associated with oocyte toxicity and an earlier age of menopause. Excessive exercise and anorexia may adversely affect both ovulation and sperm production. Exposure to potential teratogens, such as lead, should be excluded by the history. Although alterations in the usual dietary intake do not benefit the infertile couple, it is critical for women to begin taking at least 400 µg of folic acid and avoid alcohol intake once they conceive. Victims of sexual and physical abuse may be markedly affected by the intensive testing and treatment required for infertility. It is important to identify these potential emotional barriers prior to beginning the evaluation. Finally, infertility is remarkably stressful and can lead to dysfunction or even dissolution of the couple's relationship. One of the key members of any infertility team is the counselor or psychologist who is experienced in helping couples deal with the stresses involved in testing and treatment for infertility. Appropriate referrals to this individual will be discussed in the “Treatment” section of this chapter, but often it is best to involve this member of team from the start of the evaluation.
EVALUATION: TESTING
The amount of testing for most medical conditions has increased markedly over the past decade. By contrast, as our understanding of infertility increases, the testing has simplified. Some tests have been eliminated as they are now known to be of limited value or do not alter the treatment decisions. The basic evaluation now includes only three tests—semen analysis, ovulation monitoring, and uterine/tubal evaluation—that can be completed in 1 to 2 months. Although additional testing may be indicated, for most couples the cause of infertility is identified and they may proceed rapidly to the appropriate treatment. This lessens the stress of the workup and minimizes the cost. Studies suggest that the majority of reproductive endocrinology and infertility subspecialists have minimized their infertility evaluation and authors have noted that a “targeted” evaluation is cost-effective and limits stresses for the couple. This section will examine the basic evaluation, the indications for expanded evaluation, and the justification for the elimination of previous testing methods.
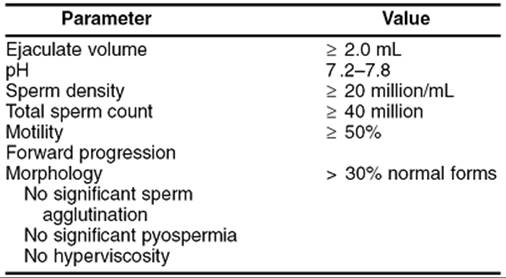
The semen analysis remains the primary method for evaluation of the male partner. This test clearly identifies subfertile men. The World Health Organization criteria in Table 38.2 are well established and were republished in 1999. Alternatives in the basic criteria may occur at some centers; the use of Kruger's strict morphology has been associated as an improved predictor of sperm function during in vitro fertilization (IVF) cycles. Some centers use a computer-assisted semen analysis (CASA). It is important that your laboratory is experienced in the assessment of sperm, but the basic semen analysis is satisfactory for clinical care. If the initial semen analysis is abnormal, it is important to be certain that the specimen was fully collected, without undue stress, not exposed to excessive heat, not contaminated by lubricants or soaps, and that the patient did not have a recent severe illness within the past 3 months that might adversely impact sperm production. Repeat semen analysis is typically obtained to confirm male infertility. Although it is ideal to wait 90 to 108 days to allow new production of sperm, this delay in the workup is not generally recommended, and collection within a month is acceptable.
|
|
|
TABLE 38.2. Semen analysis: minimal standards of World Health Organization (WHO) criteria for normal semen values |
Although ovulation can be assumed in women with regular menses and premenstrual moliminal symptoms, ovulation should be confirmed. Only 1 month of documented ovulation is required; there is no value and significant frustration with many months of ovulation testing. There are three methods to evaluate ovulation. The classic method is a basal body temperature chart. This method is low cost, fairly reliable, and informs the patient of her timing of ovulation. It is important for the provider to evaluate this form with the patient, as it is notoriously difficult for patients to interpret. A simpler, but more costly method is the luteinizing hormone (LH) or ovulation predictor kit. Unlike the temperature chart, this method identifies the timing of ovulation 24 to 36 hours prior to release of the oocyte. This may be of value to patients whose lifestyles limit midcycle coitus. Finally, a serum progesterone greater than 3 ng/mL indicates ovulation is occurring. Although the timing of ovulation and the length of the follicular and luteal phase are not identified, this simple test unequivocally documents ovulation. Ultrasound, cervical mucus examination, and endometrial biopsy can also suggest or confirm ovulation, though these tests are less frequently used because of consideration of reliability and cost.
For women over the age of 30, testing for decreased ovarian function should be added to the assessment of ovulation. The effect of advancing maternal age on fertility will be fully discussed later in the chapter, but there is no doubt that fertility begins to decrease in the mid-30s. Although the method of testing may improve as our understanding of the menopausal transition increases, the classic test is a day 3 follicle-stimulating hormone (FSH) level. Normal values for day 3 FSH vary between laboratories with the current assays identifying decreased ovarian function with a level greater than 10 to 15 IU/L. Although pregnancy can occur in women with elevated day 3 FSH levels, the chance of pregnancy is markedly reduced with IVF. Alternatively, a low day 3 FSH should not falsely reassure women of the success of infertility treatment. This test primarily reassures the number of oocytes remaining (i.e., ovarian reserve), not oocyte quality. The chance of pregnancy in the late 30s and 40s is reduced, compared to younger women, even with a normal day 3 FSH level. This test cannot be used to offer hope for women with advanced maternal age. Other forms of ovarian reserve testing: the clomiphene citrate challenge test and a day 3 inhibin B level, have been used by some infertility specialists but are not of general applicability. The clomiphene challenge test measures a day 3 FSH and estradiol level, followed by 100 mg per day of clomiphene citrate on cycle days 5 to 9 and a day 10 FSH. Studies have suggested that the clomiphene challenge test may be a better predictor of decreased ovarian reserve for older women and those with unexplained infertility.
Following the semen analysis and ovulation monitoring, the basic investigation is completed by an evaluation of the uterus and fallopian tubes. As with ovulation monitoring, there are several options for testing, but the primary method is the hysterosalpingogram (HSG). This test, although mildly uncomfortable and having a 1% risk of postprocedure infection, offers the benefit of visualization of both the uterine cavity and the fallopian tubes. The test is performed in the early to mid-follicular phase to avoid interfering with tubal function following ovulation. Slow introduction of dye into the cervical canal below the internal os by someone skilled in the technique allows the best visualization of the uterine cavity and minimizes discomfort during the procedure. If any abnormality of tubal architecture is identified, antibiotics, usually doxycycline 100 mg b.i.d. for 5 days, are typically advised. Oil-based dye has been associated with increased pregnancy rates for a few months following the HSG, but its persistence in obstructed tubes is problematic. Water-based dye can be used initially to assure tubal patency, followed by oil-based dye as a therapeutic measure. If tubal patency does not need to be assessed, the woman can undergo uterine evaluation using ultrasound with saline injection sonohysterography, or office hysteroscopy. For women with known or strongly suspected tubal damage, moving promptly to operative laparoscopy and diagnostic hysteroscopy avoids the need for the HSG. A strong argument can be made for screening for tubal damage secondary to sexually transmitted diseases by testing for antichlamydial antibodies, and proceeding directly to surgery if the testing is positive. For women with no apparent risk factors for tubal factor infertility, however, the HSG offers valuable information and results in increased fertility.
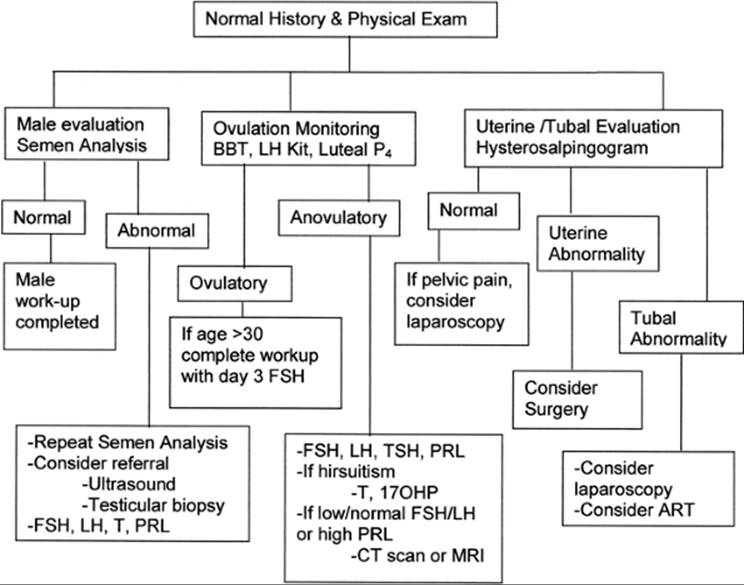
Following the basic workup, the couple will benefit from consultation with the provider. If additional testing is required to fully define the cause of male factor, ovulatory factor, or tubal/uterine factor infertility, this advanced evaluation and potential treatment options can be discussed and planned with the couple. If infertility remains unexplained, the provider may advise moving directly to treatment. In the past, all couples underwent advanced male factor testing, postcoital testing, timed endometrial biopsies, and laparoscopy/hysteroscopy before the infertility evaluation was considered complete. Although advanced testing may still be advised in selected cases, most couples benefit from rapid completion of testing and prompt initiation of effective therapy. The value of advanced testing for selected patients will be considered, but the basic workup is adequate to determine effective treatment options for most couples. Figure 38.2 demonstrates the basic infertility workup followed by more advanced evaluation.
|
|
|
FIG. 38.2. Basic workup for couple with infertility. |
EVALUATION: ADVANCED
Male Factor
If an abnormal semen analysis is identified, further workup may be indicated prior to moving on to treatment. If a history and physical exam have not yet been done, this may identify the cause of the abnormal test. Although controlled trials have not demonstrated efficacy, surgical ligation of a varicocele increases sperm motility, and finding a varicocele may lead to potential therapy. Hormonal testing—testosterone, FSH, LH, and prolactin—is of value for identifying a hypothalamic, pituitary, or testicular etiology for oligospermia or azoospermia, particularly when low male libido is noted. A fructose level and possible testicular biopsy can differentiate obstruction from testicular failure in men with azoospermia. If leukocytes are present in semen, bacterial cultures and antibiotic treatment are indicated. Unfortunately, most men with an abnormal semen analysis have idiopathic oligoasthenospermia. Although this is frustrating for the patient, very effective treatment options are available for unexplained male factor infertility.
The value of additional sperm testing in men with normal examination and hormonal testing, prior to proceeding with therapy, is debated. Abnormalities in seminal fluid have also been evaluated by antisperm antibody testing. Although studies suggest decreased fertility with the presence of antisperm antibodies, this finding does not affect the therapeutic choices of intrauterine insemination (IUI) or IVF. As a result, the value of this test remains unproven. The value of sperm function testing is also controversial. Many assays have been developed to evaluate sperm function—in vitro sperm penetration of hamster oocytes, hypoosmotic swelling, viability staining, sperm capacitation, acrosomal reaction bovine cervical mucus, sperm penetration, and human zona binding. Unfortunately, these tests have limited prognostic value and cannot consistently predict the effectiveness of selected treatments. Currently, these tests are limited to experimental use.
Inherited and medical problems can adversely affect fertility. Retrograde ejaculation can occur with diabetes, certain neurologic disorders, and pelvic surgery. The presence of sperm in the bladder can be determined by examining a post-ejaculation urine sample. Klinefelter syndrome can result in azoospermia and men with cystic fibrosis may have bilateral congenital absence of the vas deferens. Microdeletions of the Y chromosome have been associated with oligospermia. Testing for microdeletions of the Y chromosome is not yet standard practice, but it is important to inform men of the possibility of an inherited condition being passed to male children as a result of newer treatment techniques. Genetic screening can be offered to all men with nonobstructive severe oligospermia and azoospermia.
Ovulation Dysfunction
Women with oligomenorrhea and amenorrhea should be evaluated for the hypothalamic, pituitary, ovarian, or adrenal etiology of their condition. Often the history and physical examination will point to the cause of her irregular menses; there is limited value in obtaining a basal body temperature chart of LH predictor kit for women with markedly irregular menses. The most common causes of hypothalamic amenorrhea are due to weight loss (eating disorders) and excessive exercise. Rare causes include Kallmann syndrome and hypothalamic lesions. Pituitary disorders include hyperprolactinemia, thyroid disease, Cushing disease, and Sheehan syndrome. Women with significant hyperprolactinemia or unexplained hypothalamic hypogonadism should undergo a computed tomography (CT) scan or magnetic resonance imaging (MRI) to determine if a hypothalamic lesion or pituitary adenoma is present. Ovarian dysfunction is most commonly due to anovulation (World Health Organization [WHO] type II or polycystic ovarian syndrome accounting for the majority of cases). A less common etiology is premature ovarian failure, although decreased ovarian function occurs many years before menopause. The classic laboratory testing for women with oligoamenorrhea is a fasting prolactin, thyroid-stimulating hormone (TSH), FSH, and LH. Women with hirsutism should also have testosterone and 17-hydroxyprogesterone levels drawn to rule out ovarian neoplasm or late-onset adrenal hyperplasia. Women with suspected polycystic ovary syndrome (PCOS) are known to be at increased risk for hyperlipidemia, insulin resistance, and adult-onset diabetes (type II); a lipid profile and fasting glucose are recommended. The classic progestin challenge test, 10 mg of medroxyprogesterone acetate for 10 days, may be of some value, as women with hypoestrogenism will typically not have withdrawal bleeding due to progestins. Chapter 34 and Chapter 37 further discuss the evaluation of women with ovulatory dysfunction.
The use of the timed, luteal phase endometrial biopsy to assess for a minor ovulatory disturbance is now in question. There is a false-positive rate of 30% to 40% with a single endometrial biopsy. The rate of luteal phase defect when two biopsies are performed is estimated to be 7%. Luteal phase defects appear to be a rare cause of infertility and extensive testing is required to identify this problem. Additionally, the medications used for the treatment of unexplained infertility are also used to correct luteal phase defects, making a precise diagnosis less important. Women with a markedly shortened luteal phase by basal body temperature chart and normal hormonal workup may be treated empirically with medication, such as progesterone, clomiphene citrate, and gonadotropins for correction of a presumed luteal phase defect or unexplained infertility.
Uterine/Tubal Factor
Women with a history of tubal disease or significant risk factors for pelvic adhesions, such as extensive pelvic surgery, a ruptured appendix, or pelvic inflammatory disease, may elect to avoid the hysterosalpingogram and proceed directly to laparoscopic surgery. The risk of postprocedure infection is increased in these women and some authors have recommended preprocedure antibiotic therapy (100 mg doxycycline p.o. b.i.d. × 5 to 7 days). For most women, however, the HSG remains a reasonable test for uterine and tubal disorders. To evaluate the uterus alone, or in women with iodine allergies, sonohysterography or hysteroscopy can identify leiomyoma, polyps, and müllerian anomalies, and can replace the HSG.
The use of routine diagnostic laparoscopy following a normal HSG is no longer the standard infertility workup. Extensive peritubal adhesions in women with a negative history and normal HSG is rare. The most common finding at laparoscopy for women with otherwise unexplained infertility is endometriosis. The effect of severe endometriosis on fertility is not questioned, but the link between mild to moderate endometriosis and infertility remains an enigma. Research does suggest decreased fertility in women with endometriosis undergoing donor insemination. One study demonstrated an increase in fertility following laparoscopic laser ablation of mild endometriosis, but the value of surgical therapy requires further evaluation. Women with debilitating pain related to possible endometriosis, such as dysmenorrhea and dyspareunia, may benefit from laparoscopic treatment. The delay in conception required by medical therapy for pain argues for surgical treatment when symptomatic endometriosis is suspected. However, routine diagnostic laparoscopy for the identification and treatment of possible endometriosis must be compared to the benefit of proceeding with other treatment options. As will be discussed, the successful treatment of unexplained and endometriosis-related infertility argues for the selected use of laparoscopy surgery for the infertile woman.
Evaluation of cervical mucus was previously a routine part of the evaluation for infertility. Although women with a history of cervical surgery such as conization or loop electroexcision may benefit from treatment that bypasses the cervix, the postcoital test was shown to have limited predictive value of future fertility. The primary limitation of this test is its inability to predict fertility based on the number of motile sperm. It is clear that the postcoital test cannot replace the semen analysis as a test for male factor infertility. An argument can be made for an evaluation of preovulatory cervical mucus without a postcoital evaluation of sperm in the mucus. The woman herself can assess her spinnbarkeit, or mucus stretchability to 8 to 10 cm, prior to ovulation. If she has a history of cervical surgery and poor mucus production, a cervical factor can be presumed and treated appropriately.
The evaluation for infertility is now simplified in couples with negative histories and normal physical examinations. Although hormonal testing may be indicated for both men and women, and laparoscopy or hysteroscopy has a role in the evaluation of selected women, the basic workup should be limited to semen analysis, ovulation monitoring, and uterine/tubal evaluation. The value of advanced male testing, endometrial biopsy, and postcoital test is limited. Until research can confirm that these tests are consistent and have predictive value, they can be removed from the basic infertility evaluation.
TREATMENT
Once the cause of infertility is determined to the extent possible by current techniques, the health care provider can advise the couple regarding treatment choices. Advances in infertility treatment offer virtually all couples a reasonable opportunity for pregnancy. Before moving onto treatment, it is critical for the provider to recognize the stress of infertility therapy and actively involve a counselor or psychologist in the care of couples with infertility. There are limited data that suggest increased pregnancy rates with stress reduction, but the primary benefit is to maintain the well-being of couples seeking to achieve their family. RESOLVE, the national support organization for couples with infertility, is an excellent source of information and support for infertile men and women. It is also important for providers to encourage and support a couple's decision to pursue adoption or remain child-free. The program at the University of Vermont College of Medicine offers free exams for adoption physicals for the couple as a symbol of our support for these alternative decisions.
The remainder of this section highlights the treatment options for male factor, ovulatory disorders, uterine/tubal factor, unexplained infertility, and advanced maternal age.
Male Factor
The basic treatments for male factor infertility have improved over the past decade. Although donor sperm continues to be a viable option for many couples, IUI (intrauterine insemination) and IVF (in vitro fertilization) with intracytoplasmic sperm injection (ICSI) now offer an excellent opportunity for many couples. Surgery remains the primary treatment for obstructive azoospermia secondary to previous vasectomy or injury. Additionally, surgical ligation of a varicocele improves sperm motility, although controlled trials demonstrating an improvement in fertility are lacking. Medical therapy for male factor infertility, with the exception of treatment for hypothalamic hypogonadism, has not been shown to be effective.
When there is a relatively mild oligoasthenospermia, IUI with the male partner's sperm offers a reasonable chance for pregnancy. Successful treatment with less than 1 million motile sperm is low, but most studies have shown improved pregnancy rates with higher levels of motile sperm. Whole semen cannot be used for IUI due to the reactions to the prostaglandins and bacteria in the semen. The IUI sample uses sperm washed in culture medium, often using a swim up procedure to isolate motile sperm. The IUI is often combined with ovarian stimulation and timed ovulation, although it can be timed using an ovulation predictor kit.
With more severe oligoasthenospermia, or as a primary treatment for less severe male factor infertility, IVF offers the highest per cycle fecundity of any therapy. ICSI has increased the ability of sperm to fertilize oocyte in vitro, even with very low numbers of motile sperm. ICSI is typically recommended with severe oligospermia (<2–10 × 106 sperm/mL), severe asthenospermia (<5%–10% motile sperm), or poor morphology (<4% normal forms by strict criteria). Fertilization rates match those seen with traditional IVF procedures. Microsurgical epididymal sperm aspiration (MESA) or percutaneous epididymal sperm aspiration (PESA) obtain epididymal sperm for the treatment of obstructive azoospermia. Cases such as failed vasectomy reversal, postinflammatory obstruction, and congenital obstruction can be treated with MESA or PESA. Testicular sperm extraction (TESE) can be used to obtain sperm with nonobstructive or severe obstructive azoospermia. Even men with Sertoli-cell-only syndrome (up to 40%) have successful sperm retrieval with TESE.
Concerns about the risks associated with IVF and ICSI continue to be raised. Most studies to date have not shown an increase in congenital anomalies in children born by ICSI as compared to standard IVF. However, when a Y chromosome deletion is present, the defect will be passed to any male offspring. Data from the Society for Assisted Reproductive Technology and the Centers for Disease Control and Prevention have shown the risk of serious malformations to be 2%, which is the same rate as found with spontaneous pregnancies. Studies have suggested a possible increased risk of sex chromosome aneuploidy, particularly monosomy X and the presence of an extra X or Y chromosome. There is no increased risk of chromosomal structural defects with intracytoplasmic sperm injection.
Ovulatory Dysfunction
Excellent treatment options are available for all causes of amenorrhea and anovulation. The ACOG Practice Bulletin on the management of infertility caused by ovulation dysfunction offers a well-written overview of these therapies. Hypothalamic hypogonadism due to weight loss or excessive exercise may be treated by a change in lifestyle, although this does not always result in correction of menstrual cyclicity. Ovulation can be accomplished with either pulsatile gonadotropin-releasing hormone (GnRH) administration or injectable gonadotropins in women with ongoing amenorrhea or Kallmann syndrome. The GnRH pump delivers 50 to 75 ng per kg every 60 to 90 minutes; ovulation typically occurs in 10 to 20 days. Although side effects are minimal and the risk of multiple gestations is not increased over the general population, this method is labor-intensive for patients and health care providers, requiring continuous use of the pump for up to 3 weeks. Injectable human gonadotropins are now available as human menopausal gonadotropins, purified urinary FSH, and recombinant FSH, and can be given intramuscularly and subcutaneously. The use of any of these products requires close monitoring, including ultrasound and estradiol levels to lower the risk of multiple gestation and ovarian hyperstimulation. Human chorionic gonadotropin (hCG) is typically given when the follicle diameter reaches 15 to 18 mm. The risk of these medications will be further discussed in the section on “Unexplained Infertility” later in the chapter.
Women with hyperprolactinemia can be treated with dopamine-agonist therapy. Bromocriptine mesylate and cabergoline are oral agents that successfully lower prolactin levels and routinely restore ovulation. Side effects, including headache, nausea, orthostatic hypotension, and dizziness, can be severe. Starting with a low dose and a slow, steady increase in the medication will minimize side effects. With bromocriptine we typically start with one-half tablet, 1.25 mg, at bedtime, increasing weekly to a maximum of 2.5 mg twice daily. Often one tablet at bedtime is sufficient to lower prolactin levels and restore ovulation. Cabergoline is taken only once or twice weekly at doses of 0.5 to 3 mg per week. Side effects are reported to be lower with this dopamine agonist, although it is still important to gradually increase the dose of the medication. Once women achieve pregnancy the medication is stopped, although there are no reports of harmful effects on the fetus. There is no restriction to breast-feeding in women with hyperprolactinemia, assuming there is no worsening of symptoms after pregnancy.
Our understanding of the etiology of PCOS has undergone a rapid expansion over the past decade. The methods of inducing ovulation have expanded, although the standard treatments remain effective for many women. For some women weight loss will allow them to ovulate and achieve pregnancy. Although long periods of time cannot be spent on unsuccessful attempts at weight loss, it is reasonable to start with this treatment option for obese women with PCOS. For slender women with PCOS or those who are not successful with weight loss, many other options are available. The classic medication is clomiphene citrate. The usual dose starts with 50 mg, or one tablet, daily on cycle days 5 to 9 following spontaneous or progestin-induced menses. Ovulation should be confirmed using temperature charts, ultrasound, or luteal progesterone levels. The maximal dose is typically 150 mg for 5 days, although higher doses (to 250 mg) for a longer period (to 8 days) are occasionally successful. In general, the higher the dose required for ovulation, the lower the pregnancy rate. Adding 0.5 mg of dexamethasone to clomiphene may increase the response in women with high adrenal androgen levels. Eight-five percent of women with PCOS will ovulate after taking clomiphene citrate. Side effects include hot flashes, headache, visual changes, breast tenderness, and bloating. Serious side effects are rare. A 10% chance of twins is the greatest risk, and the risk of higher order multiple gestations is less than 1%. It is important for women to realize that not all women conceive with clomiphene citrate; typically do not administer this medication beyond six ovulatory cycles.
Three additional options for women with PCOS include surgical treatment, injectable human gonadotropins, and insulin-sensitizing agents. The classic ovarian wedge resection for the treatment of PCOS fell into disrepute due to a high incidence of postoperative adhesions. Laparoscopic cautery, diathermy, and laser treatment have been used to allow spontaneous ovulation. The theory is that a reduction in the ovarian cortex by the surgical injury will allow ovulation to occur. Fifteen to twenty sites on each ovary are removed and 70% to 80% of women ovulate following surgery. Studies are currently limited and the advantages of surgical therapy versus medical therapy are limited as well. A significant advantage is a decrease in the risk of multiple gestations. Injectable gonadotropins affectively induce ovulation in women with PCOS. The need for close monitoring, to minimize the risk of multiple gestation and ovarian hyperstimulation, is greatest for women with PCOS. For women who do not ovulate with clomiphene, injectable gonadotropins are usually successful at inducing ovulation.
Studies suggest that a large percentage of women with PCOS are insulin-resistant and the use of insulin-sensitizing medications will restore ovulatory menstrual cycles. It is clear that women with PCOS are at increased risk for adult-onset diabetes and often have elevated fasting insulin levels despite a normal fasting glucose. The impact of insulin resistance and chronically elevated insulin levels on ovarian function has been studied and treatment with insulin-sensitizing agents—biguanide and thiazolidinediones—may induce ovulation in women with PCOS. Indeed, in comparison to low-dose clomiphene citrate alone, metformin increases ovulation rate in limited studies. Although the side effects with these medications are common, primarily nausea and diarrhea, they offer a potential treatment option for women with PCOS. This is not a Food and Drug Administration–approved use of these medications, and insulin-sensitizing agents may be less effective in slender women and those with normal fasting insulin levels. Future research on the use insulin-sensitizing agents to control obesity, hirsutism, and anovulation in women with PCOS will be of great interest to patients and providers alike.
Limited treatment options are available for women with premature ovarian failure. Women with hypergonadotropic hypogonadism, secondary to a chromosomal abnormality, chemotherapy or radiation therapy, autoimmune disorder, or idiopathic loss of ovarian function, do not respond to gonadotropins, as there are simply no functional follicles remaining. Although pregnancies are reported with ovulation-induction agents after use of hormone replacement therapy, these are rare cases and do not justify the use of fertility medications with these women. Hormone replacement, to prevent osteoporosis and minimize hypoestrogenic symptoms, is the standard of care. Fortunately, donor oocytes can be offered as an option for these women. The generous contribution of oocytes by a donor undergoing gonadotropin stimulation and oocyte retrieval, offers women with premature ovarian failure an opportunity for pregnancy. As with women of decreased ovarian reserve and advanced maternal age, donor oocyte is a reasonable option for women with premature ovarian failure. The choice to pursue adoption or the decision to remain child-free should also be discussed with these couples in a nonjudgmental fashion.
Uterine/Tubal Factor
Limited studies are available to determine the value of surgical treatment of uterine abnormalities in women seeking fertility. Some studies demonstrate increased pregnancy rates in women undergoing hysteroscopic polypectomy or myomectomy, suggesting the value of this surgery. It is presumed that submucosal lesions, leiomyoma or endometrial polyps, should be removed prior to attempting pregnancy. Hysteroscopic surgery is recommended for women with intrauterine adhesions, or Asherman syndrome, and for removal of a uterine septum. The benefit of abdominal surgery—laparotomy or laparoscopy—for the removal of intramural and subserosal leiomyoma is less clear. An increase in pregnancy rate of 40% to 60% following abdominal leiomyoma was reported, but this surgery increases the risk of peritubal and periovarian adhesions. The risk of recurrence following surgery of leiomyoma is at least 30% and increases with time.
The treatment of known tubal factor infertility depends on the severity of the disease. Proximal tubal blockage can be treated hysteroscopically, radiographically, or by microsurgical reanastomosis. A meta-analysis documented an intrauterine pregnancy rate of 50% in women undergoing surgery for proximal tubal blockage, with the highest success rates achieved with selective salpingography and transcervical cannulation. Laparoscopic removal of thin, avascular adhesions involving the tube and ovaries offers a reasonable chance for pregnancy, with a success rate up to 70% but with an ectopic pregnancy rate of 20%.
Women with significant symptoms, such as pelvic pain, secondary to adhesions or endometriosis, also benefit from laparoscopic surgery. Removal of severe tubal adhesions and treatment of hydrosalpinges by neosalpingostomy offers a less predictable pregnancy rate. The per cycle fecundity following extensive tubal surgery is only 2% to 4%. Repair of bilateral tubal damage—proximal and distal tubal adhesions—has the lowest chance of an intrauterine pregnancy and is not recommended. The success of IVF, as will be discussed in Chapter 39, suggests this is a superior treatment for women with severe tubal factor infertility. IVF offers a reasonable chance for pregnancy, lowers the risk of ectopic pregnancy, and avoids the prolonged delay required to determine the success of treatment. Studies suggest an increased pregnancy rate if large hydrosalpinges are removed laparoscopically prior to IVF. Thus tubal surgery, with removal of the damaged fallopian tubes prior to IVF, increases the chance for successful infertility treatment.
Cervical factor infertility, although difficult to identify with standard testing, can be treated effectively with IUI. Limited studies have suggested a benefit of low-dose oral estrogen 1 week prior to ovulation for women with decreased cervical mucus; this treatment can be attempted for women with a history of cervical trauma, surgery, or diethylstilbestrol exposure. The standard therapy for these women is timed IUI, using washed sperm placed in the uterus the day following the LH surge or using ovarian hyperstimulation for timing ovulation.
Unexplained Infertility
Unexplained infertility is determined in 15% to 25% of infertile couples. This diagnosis often leads to significant distress, as the cause of infertility remains unknown. The good news is that treatment options for these couples allow a significant chance for pregnancy. One option, for a young couple, may be no therapy. Approximately one-half of couples who do not conceive in 1 year will do so within 2 years; up to 70% to 80% will conceive in 5 years. The primary benefit of treating unexplained infertility is to shorten the time to conception, a treatment of particular interest to couples in which the woman is over 30. The three primary treatment options are clomiphene with IUI, injectable gonadotropins with IUI, and IVF. IUI alone may also significantly increase per cycle fecundity from 1% to 3%, to 7%. Adding clomiphene citrate to the IUI, 50 to 100 mg daily on cycle days 5 to 9, increases the per cycle fecundity to 7% to 9% per cycle. A large group study demonstrated a two- to three-fold increase in pregnancy rate when controlled ovarian hyperstimulation occurred with gonadotropin and IUI compared to insemination alone. Studies have reported a per cycle fecundity rate of 10% to 18% with injectable gonadotropins and IUI; meta-analysis reports a 33% pregnancy rate with three cycles of gonadotropins and IUI. The pregnancy rate is increased with injectable gonadotropins alone, but the chance for pregnancy is increased with the addition of an IUI. The highest per cycle fecundity is accomplished with IVF. The 1998 data collected by the Society for Assisted Reproductive Technology reported a delivery rate per retrieval of 29.1% per IVF cycle. Gamete interfallopian transfer and zygote intrafallopian transfer also offer an excellent per cycle fecundity of 27.4% and 29.6%. The cost and invasive nature of these procedures however has limited their use. IVF, compared to clomiphene or citrate gonadotropin use, requires the greatest commitment of time, effort, and financial resources. But as is the case for couples with male factor or tubal factor infertility, IVF provides the highest per cycle fecundity for couples with unexplained infertility.
Women with endometriosis are often placed in the unexplained infertility category. Debate continues regarding the effect of mild endometriosis on fertility. If a woman is asymptomatic and has completed the evaluation, laparoscopy can be bypassed allowing the couple to move on to treatment for unexplained infertility. If laparoscopy is elected, and mild endometriosis is identified and removed, the treatment options are the same. As with unexplained infertility, the young couple with treated endometriosis may elect to have no infertility therapy.
Advanced Maternal Age
The American Society for Reproductive Medicine began a campaign in 2001 designed to alert women to the causes of infertility. Included in this campaign was information regarding the effect of advanced maternal age on fertility. Indeed, the age of first pregnancy has increased over the past several decades. In 1975 less than 20% of women attempted their first pregnancy between the ages of 35 to 39; in 1995, 44% of first pregnancies were attempted among this age group.
The Hutterites study published in the 1950s demonstrated the effect of age on fertility. In this population the overall rate of infertility was 2.4%; after age 34 it rose to 11%, after age 40 to 33%, and after age 45 to 87%. The average woman did not conceive after age 40. Donor insemination studies in France and the U.S. confirm this pattern. Cycle fecundity clearly increases with advancing age, likely beginning in the mid-30s. The risk of infertility increases at least 10 to 15 years prior to menopause, as does the risk of spontaneous abortion and chromosomal anomalies of ongoing pregnancies. Unfortunately, many women expect normal fertility until shortly before menopause and are surprised by the realization that natural infertility begins many years before their last menstrual period.
What can health care providers do to prevent this health issue from affecting their patients? Discussing the effect of aging on natural fertility with patients seeking contraceptive care provides them with useful information with which to make personal decisions. Although many women and couples do not pursue pregnancy until their lifestyle allows them to support and care for a child, awareness of age-related infertility is of great value. An active decision to remain child-free is better for women than an unexpected outcome due to simply delaying conception based on misinformation. Once a woman of advanced maternal age decides to pursue pregnancy, information about the timing of intercourse during the cycle is of value. If history or exam suggests a potential cause of infertility, for example irregular menses or history of STD, the workup can begin immediately. The new basic workup can be accomplished in 1 to 2 months, allowing rapid diagnosis of the cause of infertility once a couple does not conceive within a year or earlier, if the woman is over 35. Providing patients with information and rapid evaluation and treatment maximizes the chance that they will achieve their desired family.
It is now easier and faster for couples to determine the cause of infertility. The limited basic workup includes a semen analysis, ovulation monitoring, and uterine/tubal evaluation. For women over 30, a day 3 FSH or clomiphene challenge test is recommended to screen for decreased ovarian reserve. For selected couples, further male factor evaluation, hormonal testing, postcoital testing, endometrial biopsy, and laparoscopy can be considered. Treatment options for infertility now offer a variety of highly successful options for male factor infertility, ovulation dysfunction, uterine/tubal factor, and unexplained infertility.
SUMMARY POINTS
· Infertility is a common problem in the United States, occurring in approximately 14% of couples.
· The basic workup for infertility should begin 1 year after discontinuance of contraception. The workup includes a semen analysis, documentation of ovulation, and uterine/tubal evaluation with a hysterosalpingogram.
· A thorough history and physical examination of both the man and woman may identify the etiology of infertility and direct further testing to the most likely cause of infertility.
· Treatment for male factor infertility includes donor insemination, surgery, IUI, and IVF. Intracytoplasmic sperm injection and testicular sperm extraction, despite severe oligoasthenospermia or azoospermia, allow couples to conceive.
· Treatment of hypothalamic dysfunction includes the GnRH pump and injectable gonadotropins. Hyperprolactinemia is successfully treated with dopamine agonists. Polycystic ovarian syndrome can be treated with clomiphene citrate, surgery, injectable gonadotropins, and insulin-sensitizing medications. Premature ovarian failure can be treated with donor oocytes.
· Uterine and tubal factor infertility may be treated surgically. Severe tubal factor infertility is most successfully treated with IVF.
· Unexplained infertility can be treated with clomiphene citrate/intrauterine insemination, injectable gonadotropin/intrauterine insemination, or IVF.
· Women with advanced maternal age are best served by rapid workup and treatment.
SUGGESTED READINGS
Chandra A, Stephen EH. Impaired fecundity in the United States: 1982–1995. Fam Planning Persp 1998;30:34–42.
Griffin K Panak WF. The economic cost of infertility-related services: an examination of the Massachusetts infertility insurance mandate. Fertil Steril1998;70:22–29.
Hull MGR, Cahill DJ. Female infertility. Endo Meta Clin North Am 1998;27:851–876.
Zinaman MJ, Clegg ED, Brown CC, et al. Estimates of human fertility and pregnancy loss. Fertil Steril 1996;65:503–509.
Evaluation: Testing
Guzick DS, Carson SA, Coutifaris C, et al. Efficacy of superovulation and intrauterine insemination in the treatment of fertility. N Engl J Med 1999;340:177–183
Kruger TF, DuToit, TC, Franken DR, et al. A new computerized method of reading sperm morphology (strict criteria) is as efficient as technician reading. Fertil Steril 1993:59:202–209.
Sharara FI, Scott RT, Seifer DB. The detection of diminished ovarian reserve in infertile women. Am J Obstet Gynecol 1998;179:804–812.
Silverberg KM. Evaluation of the couple with infertility in a managed care environment. Clin Obstet Gynecol 2000;43:844–853.
Sperm morphology, motility, and concentration in fertile and infertile men. N Engl J Med 345:1388–1393.
Vanderkerckhove P, Watson A, Lilford R, et al. Oil-soluble versus water-soluble media for assessing tubal patency with hysterosalpingography or laparoscopy in subfertile women. In: Cochrane Database of Systemic Reviews. The Cochrane Library 2002; Issue 1. Oxford: Update Software.
Ventura SJ, Mosher WD, Curtin SC, et al. Trends in pregnancies and pregnancy rates by outcome: estimates for the United States, 1976–1996. National Center for Health Statistics. Vital Health Stat 2000;21:56.
Evaluation: Advanced
Bush MR, Walmer DK, Couchman GM, et al. Evaluation of the postcoital test in cycles involving gonadotropins. Obstet Gynecol 1997;89:780–784.
Davis OK, Berkeley AS, Naus GJ, et al. The incidence of luteal phase defect in normal, fertile women, determined by serial endometrial biopsies. Fertil Steril 1989;51:582–586.
Mao C, Grimes DA. The sperm penetration assay: can it discriminate between fertile and infertile men? Am J Obstet Gynecol 1998;159:279–286.
Marcoux S, Maheux R, Berube S, et al. Laparoscopic surgery in infertile women with minimal or mild endometriosis. N Engl J Med 1997:337:217–222.
Reijo R, Alagappan, Patrizio P, et al. Severe oligospermia resulting from deletions of azoospermia factor gene on Y chromosome. Lancet 1996;347:1290–1293.
Treatment
Abma J, Chandra A, Mosher W, et al. Fertility, family planning, and women's health: new data from the 1995 National Survey of Family Growth. National Center for Health Statistics. Vital Health Stat 1997;23:19.
ACOG Practice Bulletin No. 34. Management of infertility caused by ovulatory dysfunction. Obstet Gynecol 2002;99:347–358.
Cohlen BJ, Vanderkerckhove P, teVelde ER, et al. Timed intercourse versus intra-uterine insemination with or without ovarian hyperstimulation for subfertility in men. In: Cochrane Database of Systemic Reviews. The Cochrane Library 2002; Issue 1. Oxford: Update Software.
Guzick DS, Sullivan MW, Adamson GD, et al. Efficacy of treatment for unexplained infertility. Fertil Steril 1998;70:207–213.
Hughes E, Collins J, Vandekerckhove P. Clomiphene citrate for ovulation induction in women with oligo-amenorrhea. In: Cochrane Database of Systemic Reviews. The Cochrane Library 2002; Issue 1. Oxford: Update Software.
Khorram O, Patrizio P, Wang C, et al. Reproductive technologies for male infertility. J Clin Endo Metab 2001;86:2373–2379.
Nestler JE, Jakubowicz DJ, Evans WS, et al. Effects of metformin on spontaneous and clomiphene-induced ovulation in the polycystic ovary syndrome. N Engl J Med 1998;338:1876–1880.
Penzias AS, DeCherney AH. Is there ever a role for tubal surgery? Am J Obstet Gynecol 1996;174:1218–1223.
Society for Assisted Reproductive Technology and American Society for Reproductive Medicine. Assisted reproductive technology in the United States: 1998 results generated from the American Society for Reproductive Medicine/Society for Assisted Reproductive Technology Registry. Fertil Steril 2002;77:18–31.
Varasteh NN, Neuwirth RS, Levin B, et al. Pregnancy rates after hysteroscopic polypectomy and myomectomy in infertile women. Obstet Gynecol1999;94:168–171.