F. Joseph Kelly
Phillip Y. Roland
James W. Orr Jr.
INTRODUCTION
“One important key to success is self-confidence. An important key to self-confidence is preparation.”
--Arthur Ashe
In this country, obstetrician-gynecologists are the primary surgeons in over 3.6 million pelvic operative procedures completed on an annual basis (Table 44.1). These procedural volumes, when combined with the many thousand minor office and obstetric procedures, are testimony to the enormous potential physical, psychological, and economic impact of surgery and potentially preventable adverse events on women's health care. Importantly, nearly 50% of all adverse perioperative events are preventable. The sheer numbers undeniably suggest that risk prevention should be the ultimate goal of every surgeon. Assuming the role of primary care physician and surgical subspecialist for women, obstetrician-gynecologists should accept responsibility for developing, instituting, and completing all aspects of perioperative management. As an important step to improve quality of care, we should be cognizant of the potential role and benefits that allow objective discussion of nonsurgical options, as well as understand appropriate surgical indications for pelvic disease processes.
|
|
|
TABLE 44.1. Surgical procedures in obstetrics and gynecology |
Our primary goals should consist of prospective preoperative recognition, evaluation, and management of the significant clinical aspects of existing medical comorbidities and development of operative techniques to form a flexible multifaceted surgical skill set that increases the opportunity for safe completion of the procedure, regardless of inherent technical difficulty. Finally, pelvic surgeons should be capable of devising a postoperative care plan that further minimizes the risk of an adverse perioperative outcome, enhances the early recognition of acute perioperative problems, and lessens the risk and the intensity of potentially catastrophic perioperative complications. This care plan should be formalized prior to entering the preanesthetic area or the operating suite, and its execution should contain enough clinical alternatives to ensure a successful result, regardless of the intraoperative findings or postoperative complications encountered. The volumes of existing published literature on surgical alternatives and indications establish a clear message: “optimal” perioperative care is a moving target. Every treatment plan and intervention requires careful aim if the goals of improved quality and optimal patient outcome are to be attained. Mastery of these perioperative planning processes only serves to improve the individual and collective quality of patient care. Proper implementation should result in decreased individual, regional, and national health care expenditures.
SURGICAL INDICATIONS AND CONSENT FOR SURGERY
It is the ultimate responsibility of every obstetrician-gynecologist to evaluate thoroughly the patient's reproductive tract complaints prior to entertaining the possibility of surgical management. In addition to evaluating the pelvic condition, it is vital to conduct a preoperative search for physical or psychological comorbidities. Only when armed with this global information can the surgeon objectively present the risks and realistically relate the expected outcome of the entire spectrum of accepted medical and surgical options. This information should be processed and presented to the patient (and other support persons when appropriate) in a manner that is not demeaning, using understandable language that allows and facilitates an informed decision and consent process. Although the preoperative diagnostic period may be deemed routine by the surgeon and staff, many women consider the prediagnostic interval to be the most stressful time of treatment. This psychological stress contributes to difficulty in understanding the importance and results of diagnostic studies or results and potentially clouds the information discussed during preoperative discussions. Decisions, options, and alternatives, as they relate to the potential need for postoperative therapy, can be lost. The preoperative use of illustrative drawings, pamphlets, videos, or other visual educational materials often can be of assistance in improving patient (and family) comprehension of medical alternatives, operative indications, associated risks, and expected treatment outcomes. Typically, this preoperative encounter (or encounters) to discuss surgical options and obtain consent is best undertaken in a private setting, completed in a manner that is conducive of a two-way flow of communication. Eye contact, a caring touch, an unhurried approach, and other “soft” physician behaviors lower communication barriers and facilitate patient and “significant other” comprehension. The complexity of preoperative discussion and necessary time expenditure may vary dramatically with the surgical indications, as well as with the medical alternatives to the proposed procedure. Regardless, the algorithm of care, surgical risks and outcome expectations should be detailed, recognizing that modification may be required secondary to important or imperative patient desires (e.g., a patient desiring retention of ovaries or fertility). Regardless of the extent of preparation and best surgical technique, any unexpected or adverse intraoperative or postoperative event can alter dramatically the final surgical procedure and ultimate result. The apparently “simple” laparoscopic salpingo-oophorectomy may be complicated by uncontrolled abdominal wall, intraperitoneal, or retroperitoneal bleeding, intestinal injury, or the finding of an ovarian malignancy. Postoperative myocardial infarction (MI), infection, or thromboembolism may occur. A good rule of thumb is to discuss during the explanation of surgical risks adverse events that occur at a frequency of 1% or more. Any preoperative consent discussion should include the risk of death or permanent disability. Failure to address any or all of these risks can result in misunderstanding, fear, and anxiety and fosters mistrust. As important as the consent process, the resultant preoperative patient education decreases the need for postoperative analgesia and is associated with less anxiety and earlier ambulation. Unless the clinical situation is emergent or life-threatening, these discussions are best undertaken at a time remote from the day of surgery. Timely entered, legible chart documentation should follow any and all of these discussions.
Following the mutual decision to bypass medical management, the surgeon is faced with a number of other important procedural questions including the route (i.e., vaginal versus abdominal versus laparoscopic approach), as well as who should perform the procedure. It is intuitive and reported data confirm that, even among subspecialists, individual surgical skills and outcomes of specific procedures differ dramatically. These differences may relate to the surgeon's innate technical ability, the specifics of the individual's previous training, patient selection, or factors unrelated to the physician. Without placing blame, the training demands of our subspecialty have altered the overall extent of residency surgical experience, resulting in fewer major operative procedures being completed per trainee. These educational changes have resulted in a noticeable decrease in resident surgical skill acquisition. Importantly, these relative deficiencies noted by senior observers may not be perceived or recognized by the individual trainees. Coupled with the increasing ratio of postresidency physicians to annual operative procedures and the increasing technical procedural subspecialization, it is easily understood how difficult it is for the pelvic surgeon to obtain, maintain, or refine new surgical skills, even in our restricted subspecialty where the surgical focus is entirely on reproductive tract procedures. These factors lend credence to the adage, “no one can be all things to all people,” and each physician must individualize the decision to operate, consult, or refer. Specific referral guidelines citing evidence-based data have been created to assist practicing obstetrician-gynecologists in the care of women with selective diagnoses. Additionally, a favorable outcome of many procedures is related to increasing surgical experience, surgical volume, and expertise. Although disease-specific guidelines may not relate to “routine procedures,” it is logical and scientific that improved perioperative outcomes should follow increased surgical case volume. Although these effects may be surgeon or program related, arguments against consultation or referral have little scientific merit and may not be in the patient's best interest. Although circumstances may prohibit actual patient referral, the ready availability of curbside, personal, telephone, and internet consultation should encourage information dissemination, and utilization of available resources should improve patient care.
HISTORY AND PHYSICAL EXAMINATION
“Listen to women and they will tell you what's wrong with them.”
--Charles E. Flowers
Every operative procedure requiring anesthesia should be viewed as a physiologic stress test. The intensity of the stress response varies in direct proportion to the extent of the actual surgical procedure and is associated with a clinically and biochemically measurable adverse effect. Nearly every organ system is affected adversely by general anesthesia. The associated 20% reduction in resting heat production and increased surface heat loss predispose patients to hypothermia, increasing the risk of an adverse cardiac event, altered pulmonary response to hypercarbia and hypoxemia, impaired coagulation, and poor wound healing. The untoward anesthesia-related pulmonary effects of impaired oxygenation and altered lung mechanics are likely well tolerated by the 40 year old, but they may have catastrophic consequences in the elderly or in those with coexisting pulmonary disease. Most inhalational drugs directly create increased cardiac risk by altering myocardial oxygen supply and demand kinetics. Myocardial depression, increased arrhythmogenicity (as high as 27% incidence), and altered neural tone form the triad for predisposing women to adverse cardiovascular effects. Importantly, these risks are not lessened with regional anesthesia use. Reduction in renal blood supply (decreased by 30 to 70%), suppression of the immune system, ileus, and stress-related gastric ulceration represent but a few of the other quantitative adverse effects of anesthesia. Many of these effects can be correlated with the duration of operation, and every effort should be made to increase operative efficiency in an attempt to safely shorten the procedure and minimize risks.
Despite these anesthesia-enhanced risks, only a small percentage of operative deaths are attributable solely to anesthesia. Less than 18% of surgical mortality is directly attributable to the surgical procedure. The vast majority of surgical mortality (79%) can be related directly to problems created in great part from the patient's coexisting medical disease. This mortality risk further illustrates the need to undertake a diligent preoperative search to identify and potentially modify the adverse effects of any significant coexisting medical condition.
The literature is inundated with articles espousing the proposed benefits of preoperative radiologic testing and laboratory evaluation; however, the diagnostic power contained in a carefully obtained history and a thorough physical examination is enormous. The reproducible validity of this simple, easily obtainable evaluation is underscored when recognizing that as many as 98% of abnormalities found with preoperative laboratory and radiologic screening can be predicted by historical or physical findings.
Although studies relating to the pelvic process (i.e., urodynamics) frequently are necessary to delineate the need for surgery, attempts to obtain important historical information regarding diagnosed medical comorbidities and clinically silent medical disease are vital to direct additional preoperative evaluation. Review of pertinent medical records combined with initial direct questioning about previous hospitalizations, current treating physicians, concurrent diagnoses, use of prescribed and over-the-counter medications, and allergies will assist in the detection of coexisting medical disease. This information may be vital to the preoperative plan regarding the continuation (e.g., cardiac, hypertensive) or discontinuation (e.g., aspirin, oral contraceptives, anticoagulant) of medications. Over-the-counter and herbal medication usage can create the potential for additional untoward complications and should be evaluated (Table 44.2). Conducting a pointed review of systems allows the determination of performance status and aids in the diagnosis of significant but previously undetected medical disease. Although intended to cover multiple systems, simple questions as to the patient's ability to walk a mile, climb two flights of stairs, or blow out a match from 12 inches away may suffice as a screen for significant cardiopulmonary disease. Historical information obtained by questionnaire can be considered valid; however, the presence or absence of important symptoms should be confirmed during the office visit.
|
|
|
TABLE 44.2. Herbal medicines: possible adverse effects |
A thorough multisystem physical examination is an essential part of every preoperative evaluation. Specific attention to the cardiopulmonary system assists in the detection of important coexisting disease that may alter outcome adversely and directs additional investigation. Every system carries some import, and abnormal findings allow for appropriate morbidity-reducing, cost-effective adjustments in the perioperative plan.
LABORATORY INVESTIGATION
The primary goal of preoperative laboratory preparation is to obtain results that allow reduction of those inherent risks related to the proposed procedural component, as well as those risks associated with occult or recognized coexisting medical morbidities. It has become apparent that a “broadly cast net” preoperative laboratory screening strategy confers little patient benefit for the following reasons. (a) The majority of laboratory abnormalities can be predicted by findings noted in the history and physical examination. It is rare to detect an unexpected abnormality. (b) The physiologic, psychological, and economic costs associated with the evaluation of abnormal laboratory (including false-positive) studies brings little value, and it rarely influences clinical care. (c) As many as 60% of abnormal preoperative test results are not known or evaluated preoperatively, creating potential liability. Multiple reports suggest that nearly 70% of ordered preoperative laboratory tests are not indicated by facts obtained in the history and physical examination.
This information reiterates the importance of the history and physical examination and suggests that a directed preoperative laboratory testing strategy (Table 44.3) for routine procedures is both safe and cost effective. Obviously, special studies such as tumor markers (e.g., CA-125) are appropriate during evaluation and management of women with pelvic malignancies, because they offer diagnostic assistance, facilitate decisions regarding patient triage, are potentially prognostic, and are of significant value during postoperative management. Although care should be individualized, it has become apparent that directed preoperative laboratory testing forms a firm foundation for quality preoperative care for patients undergoing elective procedures.
|
|
|
TABLE 44.3. Preoperative testing strategy |
Although advances in blood banking technology have lessened the risk of transfusion and favorably affected the outcomes of many surgical procedures, it is apparent that women do not need to have a type and crossmatch performed prior to the majority of obstetric or gynecologic surgical procedures. Although maximal surgical blood order schedules have been established, they should be validated at each institution. When deemed necessary, a type and screen allows for identification of specific antibodies and assures rapid availability (≤20 min) of red blood cell products. Individual decisions regarding blood bank strategies should be related to the patient's preoperative status (i.e., hemoglobin and hematocrit, blood volume), anticipated losses, and existing comorbidities that might carry an early transfusion trigger. Anemia is not uncommon among women undergoing pelvic surgery. Although it may constitute an indication (menorrhagia, associated with leiomyomas) or result from an indication (cervical cancer), its presence should prompt an evaluation. As deemed appropriate, a preoperative search for other causes or losses should be undertaken. Additionally, preoperative discussions regarding procedure-associated blood loss and its attendant risks represent an important aspect of informed consent.
Critically ill patients may benefit from having their serum hemoglobin levels maintained at about 10 g/dL, but data suggest little effect of transfusion on survival in patients whose hemoglobin levels are between 8 and 10 g/dL. The majority of women can safely undergo elective procedures without a type and screen.
RADIOLOGIC INVESTIGATION
Routine imaging studies can be obtained safely as directed by findings of the history and physical examination. The indications for a preoperative chest radiograph are relatively straightforward, and abnormalities are associated with an increased risk of perioperative pulmonary complications. Unfortunately, unnecessary chest radiographs and many additional, sometimes unnecessary, undirected diagnostic preoperative imaging studies are obtained frequently.
Diagnostic ultrasonographic examination, pelvic and abdominal computed tomography (CT), and magnetic resonance imaging studies are performed in patients with suspected or known gynecologic malignancies. These studies may suggest the benefit of preoperative triage to a subspecialist but rarely influence the surgical approach. Their results should not be considered binding, typically contribute little to clinical care, and often add significantly to health care costs. Although the radiologist's suggestions for additional studies are noted frequently, the astute pelvic surgeon should combine physical findings, patient symptoms, and laboratory results to develop the perioperative care plan, based on necessity and benefit of histologic confirmation of a radiologic abnormality.
Although proponents of preoperative “radiologic staging studies” suggest relative accuracy, the pelvic surgeon must recognize the subjective aspects of interpretation. In general, their routine use has not been associated with an alteration in perioperative clinical care. Although findings may alter approach, negative results do not exclude the finding of significant pathology. Not to condone or condemn, the value and use of other noncardiac imaging studies have not been evaluated adequately. However, it appears that in specific situations CT scans have a significant false-negative result rate (e.g., for the evaluation of extraovarian disease). Radiologic investigation adds little to clinical care in patients with endometrial cancer in the absence of physical findings. There is little clinical value for intravenous pyelography (IVP) to evaluate ureteral location or displacement, because it is not a substitute for intraoperative ureteral identification. In the absence of malignancy, hydronephrosis is likely related to displacement and is easily corrected or managed during the operative procedure.
The exception is an abnormal finding on a clinically indicated routine cancer screening study (e.g., mammography), in which test results may have a significant impact on clinical care, particularly in those women undergoing “elective pelvic procedures.”
ENDOSCOPIC EVALUATION
There is little evidence to suggest the value of multiple endoscopic procedures prior to most routine gynecologic procedures. However, it is certainly appropriate to consider obtaining history-directed or disease-specific (e.g., inflammatory bowel disease, previous colon cancer) or recommended cancer screening endoscopic procedures prior to elective procedures. For example, endoscopy performed prior to rectovaginal or vesicovaginal fistula repair may render significant and important information and cause the physician to alter the surgical approach or initiate referral.
CARDIAC DISEASE
Preoperative assessment to detect undiagnosed heart disease and direct appropriate perioperative treatment of women with longstanding or newly diagnosed cardiac disease is of vital importance. The majority of inhalational anesthetics are myocardial depressants, modify neural tone, and are arrhythmogenic, creating risk even in the healthy patient. Nearly 50,000 perioperative MIs occur annually. Approximately 20,000 are fatal, and hundreds of thousands of related serious extracardiac complications occur, resulting in poor outcome. The prevalence of cardiovascular disease increases directly with increasing age, and within the aging population serous cardiac events occur regularly. Although no age group is risk free, gynecologic procedures in the aging population are estimated to result in a 25% increase in the incidence of necessary major intraabdominal procedures, potentially increasing the absolute risk of cardiac morbidity. Although heart disease may not be readily apparent, the answers to carefully framed historical questions can assist in unmasking occult cardiac risk factors.
Gynecologists should feel compelled to become familiar with the important aspects of perioperative cardiac care, to improve individual patient outcome as well as the overall health of the entire female population.
Proper preoperative cardiac assessment requires a systematic approach, typically undertaken in close coordination with qualified consultants. Attention to history, physical findings, and the effects of comorbid diseases forms the foundation for initial evaluation. These findings assist in the direction of ordering ancillary cardiac studies, which can clarify risk and improve predictive power for perioperative morbidity associated with the proposed gynecologic surgery. They also allow institution of a sound plan for perioperative monitoring and management A disease-specific approach is important, specifically addressing signs, current symptoms, and management of coronary artery disease (CAD), hypertension, heart failure, valvular heart disease, arrhythmias, pacemakers, pulmonary vascular disease, and type and extent of surgery.
General Considerations
Particular energy should be directed preoperatively to elicit historical or physical evidence of cardiac ischemia. Important elements include angina, a history of MI, past or current signs or symptoms suggesting congestive heart failure, unexplained palpitations, evidence of previous cardiac intervention, and renal impairment. Important aspects of noncardiac diseases that increase the incidence of cardiac risk factors, including diabetes mellitus, hypertension, hypercholesterolemia, family history of CAD, and obesity, should be evaluated. Age greater than 70 years, MI within the preceding 12 months, and evidence of congestive heart failure significantly increase postoperative cardiac complications in patients undergoing gastrointestinal, urologic, and gynecologic surgery. Concurrently, the pelvic surgeon should attempt to determine the patient's “functional capacity.” The simple inability to walk three blocks or climb two flights of stairs portends a poor functional status. Physical examination evaluating the patient's overall status is mandatory. This evaluation, coupled with laboratory and radiologic information and an electrocardiogram (ECG), provides a baseline estimate as to actual perioperative cardiac risk. Numerous schema from Goldman and others intended to quantify cardiac risks have been designed, reported, and verified in an attempt to quantitate perioperative cardiac risk. The American College of Cardiology-American Heart Association (ACC-AHA) published revised practice guidelines based on qualitative analysis. Specific risk categories include ischemic heart disease, congestive heart failure, high-risk surgery, diabetes mellitus, renal insufficiency, and poor functional status (Table 44.4). They define clinical risk stratification for noncardiac surgical procedures. Noncardiac procedures with high (>5%), intermediate (<5%), and low (<1%) risk of cardiac morbidity or mortality have been categorized (Table 44.5).
|
|
|
TABLE 44.4. Factors that increase the risk of perioperative cardiac complications in patients undergoing noncardiac surgery and indications for the use of perioperative β-blocker therapy |
|
|
|
TABLE 44.5. Cardiac risk stratification for noncardiac surgical procedures |
Data prompting development of these guidelines suggest that coronary artery bypass surgery or other invasive interventions (i.e., coronary angioplasty) are appropriate only in an effort to reduce cardiac risks following the stress of noncardiac surgery when they would be indicated for symptoms or to manage test-related cardiac disease nonsurgically. Specific disease states requiring strong consideration of presurgical revascularization include poorly controlled angina pectoris (despite maximal medical therapy), high-risk left main coronary artery stenosis (>50%), severe two- or three-vessel CAD (with involvement of the proximal left anterior descending artery) with greater than 70% stenosis, easily induced myocardial ischemia on preoperative stress testing, and left ventricular systolic dysfunction at rest.
Cardiac Disease–Specific Approach
Coronary Artery Disease
CAD commonly occurs at a lower incidence in females than in males; however, diabetic women are risk equivalent to men. The mortality of an acute MI is greater for women and increases dramatically in the aged patient. Importantly, MIs occurring during the perioperative period carry a higher mortality risk than those occurring otherwise.
Many surgical patients have diagnosed CAD or risk factors for CAD. Women who are potential candidates for attempts at preoperative myocardial revascularization may benefit from noninvasive cardiac testing performed to determine the amount of myocardium in jeopardy, the patient's ischemic threshold, and the objective determination of ventricular function. Test results should be used to assist in stratifying prognostic information and determining the extent and benefit of perioperative surgical or medical intervention and postoperative monitoring.
Hypertension
As the training and practice of obstetricians-gynecologists increasingly stresses the importance of primary care, the preoperative evaluation and the management of hypertension has become a major focus on the gynecologic patient's problem list. Although the identification of early-stage hypertension should lead to the institution of appropriate medical therapy, the ACC-AHA guidelines suggest that those with stage II or milder hypertension (systolic blood pressure below 180 mm Hg and diastolic blood pressure below 110 mm Hg) are not at increased risk for perioperative cardiovascular complications. Surgical delay for medical treatment of women with stage I or II hypertension is not necessary or beneficial. However, elevated blood pressure in patients with stage III hypertension (systolic blood pressure 180 mm Hg or higher and a diastolic blood pressure 110 mm Hg or higher) should be controlled prior to surgery. The administration of β-adrenergic blockers in this clinical situation results in rapid, effective control of severe blood pressure elevation and perioperative hypo- or hypertension, either of which is associated with an increased risk of coronary ischemia. Regardless of actual measured systemic pressures, the ACC-AHA guidelines suggest that the blood pressure of patients with significant hypertension who require urgent surgery be controlled. The goal is to avoid the ischemic complications associated with perioperative blood pressure fluctuations that commonly occur in the surgical patient who has uncontrolled hypertension.
Heart Failure
Ventricular failure is an important predictor of and prognostic factor for perioperative cardiac morbidity. The initial attempt to identify women with ventricular dysfunction begins with a detailed history and organ-specific physical examination. Determination of ventricular status is mandatory in those with evidence or history of congestive heart failure, because the physiology of perioperative ventricular failure portends an ominous situation. Perioperative subspecialty consultation, pharmacologic manipulation to maximize cardiac oxygen supply–demand ratio, careful administration of intravenous fluids, and cardiac monitoring may benefit these patients. During preoperative investigation, gynecologic surgeons should not exclude the possibility of rare causes of cardiomyopathy, including hypertrophic obstructive cardiomyopathy, because their appropriate medical management decreases morbidity.
Echocardiography, to obtain an estimate of ventricular function and to rule out anatomic abnormalities, should be considered and may be necessary for the perioperative assessment for those women with suspected, known, or history of heart failure or cardiomyopathy.
Valvular Heart Disease
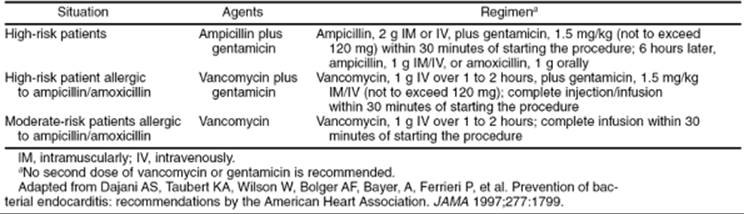
Although interpretation of the physical findings can be challenging, the gynecologic surgeon should attempt to identify significant heart murmurs. Echocardiography aids in defining the anatomic abnormality and in detailing the need and benefit of antibiotic endocarditis prophylaxis (Table 44.6). Failure to diagnose any significant valvular dysfunction or to administer appropriate antimicrobial prophylaxis increases the risk of a catastrophic perioperative consequence.
|
|
|
TABLE 44.6. Cardiac conditions associated with endocarditis |
Aortic stenosis poses the greatest valvular risk for poor postoperative cardiac outcome. Cardiac morbidity in women with untreated aortic stenosis undergoing noncardiac surgery approaches 10%, sufficient to persuade every pelvic surgeon to diagnosis this condition. ACC-AHA practice guidelines advise postponement of elective surgery in women with severe or symptomatic aortic stenosis until valve replacement, the accepted standard intervention, can be performed. In emergent situations, aortic valvuloplasty may be employed but has less certain success.
In general, surgical correction of mitral stenosis is not indicated prior to noncardiac surgery unless the severity would warrant treatment in a nonsurgical setting. If deemed necessary, balloon valvuloplasty is an appropriate corrective option for those with severe mitral stenosis. Mild to moderate mitral stenosis requires control of perioperative heart rate to reduce the risk of heart failure.
Significant aortic regurgitation requires attention to intravascular volume control and attempts at medical afterload reduction. In contrast to mitral stenosis, bradycardia should be avoided or aggressively treated to avoid left ventricular backfill.
Mitral regurgitation most commonly is associated with papillary muscle dysfunction and mitral valve prolapse. Prior to surgical procedures, antimicrobial prophylaxis may be indicated for those with mitral valve prolapse and demonstrable clinical evidence of regurgitation or echocardiographic evidence of anatomic mitral valve leaflet abnormalities. Women with significant mitral regurgitation murmurs require careful monitoring of the left ventricular ejection fraction, because the low-resistance regurgitant valve predisposes perioperative patients to retrograde cardiac flow, resulting in pulmonary edema and high pulmonary artery pressures. Invasive perioperative cardiac monitoring may be necessary, because echocardiography tends to overestimate ejection fraction in patients with mitral regurgitation.
Patients with prosthetic mitral valves receiving systemic anticoagulants require intervention to lessen the risk of endocarditis and intracardiac coagulation. The fifth consensus conference on anticoagulation suggests:
1. For minimally invasive surgical procedures, reduce the international normalized ratio to subtherapeutic range and resume the normal dosage of oral anticoagulation immediately postprocedure.
2. Perioperative heparin is recommended for patients when significant bleeding is anticipated or the risk of thromboembolism is high. These clinical situations include women with a mechanical valve in the mitral position (low flow rate), a Bjork-Shiley valve, or history of thrombosis or embolus associated with valvular replacement during the past year. Systemic anticoagulation is appropriate if three risk factors are present, including atrial fibrillation, previous embolus, hypercoagulable condition, or mechanical prosthesis with left ventricular function of less than 30%.
3. For patients whose clinical condition falls between these extremes, the risk–benefit ratio of anticoagulation should be considered individually.
Arrhythmias
Every gynecologic surgeon will encounter perioperative cardiac arrhythmias. The majority are considered benign, but their underlying etiology should be sought aggressively, because undiagnosed cardiac ischemia may initially become clinically evident as a perioperative arrhythmia. Perioperative arrhythmias may worsen existing ischemia by increasing myocardial demand or decreasing cardiac efficiency. Pulmonary disease, metabolic derangements, or drug toxicities are common causes. Monitoring and treatment is important, because an unstable arrhythmia such as atrial fibrillation occasionally may deteriorate into a life-threatening rhythm (i.e., ventricular fibrillation). In addition to conferring a therapeutic cardiac morbidity risk reduction in patients with CAD, β-blockers may reduce arrhythmia-related perioperative morbidity and mortality.
Premature ventricular contractions occurring at a rate of fewer than 6 per minute are presumably “benign.” Even short and spontaneously converting runs of ventricular tachycardia may not predispose patients to perioperative death from MI. However, underlying coronary ischemia may be unmasked by the occurrence of these rhythms, making it imperative that the underlying etiology of a perioperative arrhythmia be ascertained, even if these are not treated by antiarrhythmic agents other than β-blockade. Atrioventricular (AV) block, especially Mobitz type II or third-degree heart block, may increase operative risk. Patients with type I second-degree AV block, first-degree AV block, and left and right bundle branch blocks are usually asymptomatic and their arrhythmias rarely contribute to postoperative morbidity and mortality. It is reasonable to consider early subspecialty consultation to diagnose and treat women who develop perioperative cardiac arrhythmias.
Patients with known or previously treated or untreated congenital heart disease or pulmonary vascular disease deserve close evaluation. Individuals with previous surgical correction of a ventricular septal defect, patent ductus arteriosis, or tetralogy of Fallot may be at increased operative cardiac risk, possibly due to decreased pulmonary vasculature reactivity to hypoxia.
Risk Stratification According to Type of Surgery
Although individually weighted, existing patient risk factors, the type and extent of operation, and the operative circumstances are important to delineate the risk of perioperative cardiac morbidity. Intuitively, the decision to operate and the choice of operation or operative approach should be made in an attempt to offer the most effective treatment while minimizing patient cardiac risk. Other medical conditions should be addressed to lessen any indirect impact or perioperative cardiac outcome.
Every surgical intervention should be biased by or based on acute or chronic patient-specific factors. Although emergent surgical indications lessen available evaluation time, urgency does not absolve the responsibility to search diligently for significant risk factors. The young woman in shock with a ruptured ectopic pregnancy may provide the physician with only a brief opportunity for cardiac evaluation; however, cardiac risk factors are uncommon in this population, minimizing the necessity for or benefit of an extensive evaluation. The elderly patient with acute intestinal obstruction and strangulated bowel related to ovarian carcinoma may harbor significant cardiac risk factors but may require life-saving surgery despite significant coronary risk and a high potential for morbidity.
Perhaps more problematic is evaluation of those patients who require diagnostic or therapeutic surgery for pelvic malignant neoplasms and who are discovered to have cardiac disease during the presurgical evaluation. The clinical situation surrounding this or semi-urgent gynecologic procedures may preclude the benefit of extensive intervention (i.e., coronary artery bypass grafting [CABG]). In this situation, consultation and maximal medical therapy can improve the patient's perioperative cardiac condition and lessen risks.
Perioperative evaluation of women undergoing elective pelvic surgery should consider the risk of an adverse cardiac event in relation to the extent of the necessary surgical procedure. The benefit of medical management of the gynecologic condition should always be considered carefully. A minimally invasive or a vaginal surgical approach carries less physiologic stress and less risk of associated cardiac morbidity when compared with more extensive intervention (e.g., an abdominal approach). Although it requires planning and technical flexibility, matching the patient's gynecologic and medical conditions to a proper surgical approach should be every surgeon's goal. Good matches most frequently result in good outcomes.
Risk Assessment and Treatment
The ultimate objective of preoperative cardiac risk assessment is to rule out serious CAD that requires cardiac intervention remote from the need for noncardiac surgery. Preoperative evaluation should be designed to recognize existing disease, expose occult underlying heart disease, and provide an opportunity for appropriate cardiac assessment.
Noninvasive Testing
ACC-AHA recommendations for those undergoing noncardiac surgery provide a short-cut to the appropriate application of noninvasive cardiac testing, which is indicated by two of three listed risk factors. This testing schema assumes that the identification of a high-risk patient will identify those who would benefit from preoperative coronary revascularization or maximization of medical therapy. Either would contribute to improving the patient's long-term quantity and quality of life. Noninvasive studies include the 12-lead electrocardiogram, echocardiography, contrast ventriculography, radionuclide angiography, exercise stress testing, nonexercise stress testing, myocardial perfusion imaging, and dobutamine stress echocardiography. The ACC-AHA evaluation guidelines algorithm can be applied to all patients. In general, the gynecologic surgeon should consider the role of noninvasive testing after consultation with qualified specialists to assist in the evaluation, interpret the results of noninvasive testing, and recommend intervention for those patients with cardiac risk factors.
Coronary Artery Bypass Graft-Specific Interventions
The decision to perform CABG prior to noncardiac surgery should be based on potential risks versus the short- and long-term benefits of coronary revascularization. Eagle and colleagues reporting on 3,368 patients (Coronary Artery Surgery Study database) with CAD, found that patients undergoing minimally invasive procedures have a cardiac-related mortality rate of less than 1%, regardless of previous CABG. In contrast, major procedures including abdominal surgery carried a significantly higher risk of cardiac morbidity and mortality. The risk of death (1.7 vs. 3.3%, P = .03) and nonfatal MI (0.8% vs. 2.7%, P = .002) was significantly lower after CABG.
The ACC-AHA task force has recommended that preoperative coronary revascularization be employed in specific clinical situations: in those women with acceptable risks of coronary revascularization and a suitable amount of viable myocardium, those with left main coronary artery stenosis, those with three-vessel CAD in conjunction with left ventricular dysfunction, those with two-vessel disease involving severe proximal left anterior descending artery obstruction, and when intractable coronary ischemia persists despite maximal medical therapy.
These practice guidelines also suggest that the timing of coronary revascularization be weighed against the clinical urgency and extent of noncardiac surgical intervention. Patients requiring elective noncardiac procedures of intermediate or high surgical risk who have significantly abnormal coronary anatomy should be referred for surgical revascularization prior to noncardiac surgery. Those same patients undergoing low-risk noncardiac surgical procedures or patients with less severe coronary artery lesions should not undergo preoperative coronary artery revascularization.
Preoperative Prophylactic Coronary Intervention
The ACC-AHA task force has recommended that percutaneous transluminal coronary angioplasty (PTCA) be used in the perioperative setting in a manner identical to that proposed outside of the perioperative setting. Although debate exists as to the most appropriate interval from PTCA to the pelvic surgical procedure, delay for at least 2 to 4 weeks should be allowed to ensure healing and exclude restenosis of the treated vessel. However, extended delays of more than 6 to 8 weeks after PTCA may allow restenosis of the treated vessel and further increase the risk of perioperative ischemia.
If a coronary artery stent is placed, ACC-AHA recommendations suggest postponing surgery for to 2 to 4 weeks to allow stabilization and to exclude the risks of stent site stenosis. The 2-week delay allows completion of a full course of thienopyridine and aspirin therapy and lessens the risk of subsequent stent thrombosis. There is little evidence available to describe the perioperative effect of prophylactic coronary intervention months to years before noncardiac surgery; however, coronary restenosis is unlikely to occur within 8 to 12 months after prophylactic coronary intervention, with or without stent placement. Obviously, patients with previous cardiac intervention remain at risk to develop subsequent additional coronary artery lesions.
The Bypass Angioplasty Revascularization Investigation (BARI) compared the outcomes of noncardiac surgical procedures following CABG (250 patients) versus PTCA (251 patients) in 1,049 surgeries. The median time interval between the most recent coronary revascularization procedure and noncardiac surgery was 29 months. There were no significantly different outcomes when evaluating morbidity, in-hospital morbidity, and hospitalization costs, suggesting equivalence of revascularization procedures. However, the risk of cardiac death or MI was lower (0.8% vs. 3.6%) when noncardiac surgery was performed less than 4 years after revascularization, emphasizing the need for thoughtful preoperative cardiac evaluation in this patient population.
Perioperative Medical Therapy
Several prospective randomized trials have evaluated the effects of perioperative β-blocker administration. Poldermans and others administered bisoprolol to the 146 patients with high cardiac risk. The risks of both cardiac death (17% vs. 3.4%) and nonfatal MI (0 vs. 17%) were lowered significantly with treatment. Oral atenolol has been compared with placebo for 7 perioperative days. Although there was no significant decrease in MI or cardiac death, a significant decrease in ischemia (24% vs. 39%) was apparent in those receiving atenolol. This report also detailed a significant decrease in the subsequent 6-month death rate (1% vs. 10%) in those treated with atenolol. Ace inhibitors were also evaluated in two studies which showed no demonstrable benefit.
Although randomized prospective clinical trials of β-blockade in a gynecologic population are not available, it seems reasonable to extrapolate the benefits of these interventions to those discovered to have a high cardiac risk during preoperative evaluation prior to a pelvic operation. ACC-AHA practice guidelines recommend perioperative β-blocker treatment for patients with angina, symptomatic arrhythmias, untreated hypertension, known CAD, or major risk factors for CAD.
The potential effect of α-antagonist perioperative cardiac protection has also been evaluated. A randomized placebo-controlled multicenter trial study of mivazerol use during the perioperative period in 2,854 patients with known CAD or significant risk factors reported no difference in MI incidence; however, the cardiac death rate was reduced by nearly 50% (P = .04). The Perioperative Ischemia Research Group also reported a significant reduction in perioperative cardiac ischemia in patients given high-dose perioperative mivazerol. This new information suggests that the perioperative administration of α-antagonists may have a future role in cardiac protection.
Arrhythmias
The perioperative goal of cardiac arrhythmia or conduction disturbance management relates to the desire and need to prevent the deterioration of a given rhythm into one that is incompatible with life, to prevent cardiac ischemia, and to prevent thrombosis and endocarditis.
Electrophysiology studies with ablation of aberrant conduction foci may be necessary for women with demonstrable supraventricular arrhythmias. Advanced Cardiac Life Support (ACLS) guidelines can be used for the pharmacologic treatment of perioperative supraventricular arrhythmias. Electrical or pharmacologic cardioversion may be necessary if patients are symptomatic or hemodynamic compromise is present. Beta adrenergic or calcium channel blockade also may be indicated for rate control in the absence of successful electrical cardioversion.
Depending on the extent of surgery, patients with atrial fibrillation receiving systemic anticoagulation require evaluation and, perhaps, presurgical reversal. Simple discontinuation of the oral anticoagulant (72 hours prior) usually will suffice. However, fresh frozen plasma or parenteral vitamin K may be necessary to reverse anticoagulation and ensure hemostasis.
Frequent asymptomatic premature ventricular contractions or short runs of ventricular tachycardia may not require antiarrhythmic treatment because they do not, in general, increase perioperative cardiac risk. Although other lesser arrhythmias do not require treatment, the gynecologist should be diligent in pursuing causes of new arrhythmias to rule out myocardial ischemia. Sustained ventricular tachycardia should be treated following ACLS guidelines using lidocaine, procainamide, or other agents such as amiodarone. Care of perioperative arrhythmias is likely optimized with close communication and consultation with appropriate internal medicine, cardiac, or critical care consultants.
Other Situations
Implanted Pacemakers and Implantable Cardiac Defibrillators
Occasionally the gynecologic surgeon will encounter a surgical candidate with a pacemaker or implantable cardiac defibrillator. Lack of familiarity with the device and its function can cause perioperative anxiety, particularly when combined with the intraoperative use of electrocautery. General ACC-AHA recommendations include the following. (a) Patients should have the implanted device evaluated before and after surgical procedures to determine the underlying rhythm, program settings, and battery status. If the pacemaker is programmed in a rate-responsive mode, the device should be inactivated during surgery. (b) If patient is pacemaker dependent, the pacing threshold should be determined and evaluated appropriately. (c) Implantable cardiac defibrillators should be turned off during surgery and on again after recovery from anesthesia.
Pulmonary Artery Catheters
Invasive cardiac monitoring, including the use of a pulmonary artery catheter, provides instantaneous information, which may contribute to successful postoperative decision making. Unfortunately, the risks of catheter insertion and malfunction are significant and the rate of complications are operator dependent. Additionally, information generated from pulmonary artery catheterization is sometimes esoteric, and decisions based on the cardiac function data are limited by some degree of observer subjectivity. Evidence does not support the routine perioperative use of a pulmonary artery catheter; however, placement should be considered in specific high-risk patient subsets. It may have particular benefit in those in whom the gynecologic disease (e.g., ovarian cancer) or the surgical procedure (e.g., exenteration) is associated with large fluid shifts in those with a compromised medical condition.
Surveillance for Perioperative Myocardial Infarction
A significant proportion of perioperative MIs are silent but carry a higher mortality rate (40%–70%) than those occurring in a nonsurgical setting. Electrocardiography, cardiac-specific biomarkers, echocardiography, and radioisotope studies have all been proposed and used for detection of postoperative MIs. Although many of these studies used alone or in combination are effective, false-positive findings are common. The measurement of creatinine phosphokinase myocardial bands alone is less diagnostic of MI than the evaluation of serum troponin levels. Guidelines call for standard surveillance in low-risk patients without documented CAD and normal preoperative ECG or serum biomarker findings. However, patients with high or intermediate clinical risks who have known or suspected CAD and are undergoing high- or intermediate-risk procedures are followed appropriately with an ECG obtained in the recovery room and on the first two postoperative mornings, combined with a cardiac troponin level obtained 24 hours postoperatively and on day 4 or at hospital discharge, whichever comes first. If infarction occurs, rapid reperfusion of the myocardium is the cornerstone of therapy. Unfortunately, thromboembolic therapy cannot be used in the immediate postoperative setting, leaving medical therapy (to maximize cardiac oxygen supply–demand ratio), angiography, and revascularization as the only available therapeutic interventions.
Arrhythmia and Conduction Disorders
An arrhythmia should be addressed immediately to determine its etiology and managed according to ACLS guidelines. Tachyarrhythmias should prompt the immediate assessment of potential contributing factors including hypotension, hypoxia, or metabolic derangements. An ECG with rhythm strip should assist in identifying the exact features of the arrhythmia. Narrow-complex regular arrhythmias are likely due to AV node reentry tachycardia or supraventricular tachycardia. Vagal maneuvers should be employed initially. Pharmacologic management consists of administering adenosine or AV nodal blockade using β-blockers, calcium channel blockers, or class I-A or I-C antiarrhythmic agents.
Atrial fibrillation and flutter are unstable rhythms, which often produce a rapid ventricular response. Initial management should be aimed at control of ventricular rate by AV node blockade. Evaluation of the underlying etiology is paramount, and the use of cardioversion should not be entertained until the underlying etiology (e.g., hypothyroidism hypokalemia, hypomagnesemia) has been found and corrected.
Infrequent premature ventricular contractions do not require treatment; however, long runs of ventricular tachycardia may require antiarrhythmic therapy, particularly if symptoms or hemodynamic compromise occurs. In general, ventricular arrhythmias should be treated according to ACLS guidelines in conjunction with appropriate cardiology or internal medicine consultation. Cardiac pacing should be considered when warranted by hemodynamic compromise, symptoms including chest pain, or pulmonary edema.
The pelvic surgeon assumes great responsibility for perioperative care of the patient with cardiac risks. Although performing the best-suited procedure for the gynecologic condition is imperative, an understanding of the factors that influence overall results, the appropriate intervention, and the timely use of consultants can only improve operative outcome.
PERIOPERATIVE PULMONARY EVALUATION
Postoperative pulmonary complications (PPC) commonly occur following abdominal or pelvic surgery. Pulmonary dysfunction occurs in as many as 80% of patients, and clinically significant PPCs include atelectasis, bronchospasm, the need for prolonged ventilatory support, pneumonia, and worsening pulmonary function due to exacerbation of an underlying problem. The combination of general anesthesia and abdominal surgery results in a morbid alteration of pulmonary physiology, with effects that are compounded by postoperative immobilization, narcotics, or inadequate pain relief.
Patient-related Risk Factors
All patients, even those without underlying known pulmonary disease, remain at significant risk following general endotracheal anesthesia and abdominal surgery. Numerous comorbidities have been linked to the risk of developing PPC (Table 44.7). Although the physiologic and economic costs are significant, unfortunately, the ability to qualitatively or quantitatively evaluate or modulate pulmonary risks is not that of cardiac risks.
|
|
|
TABLE 44.7. Potential patient-related risk factors for postoperative pulmonary complications |
Tobacco abuse is a risk factor for PPC, even without clinically apparent pulmonary disease. When compared with nonsmokers, the relative risk of PPC for smokers increases as much as four-fold following abdominal surgery. Although difficult at best, prolonged smoking cessation reduces the risk of PPC by nearly 50% Unfortunately, many of the physiologic effects of smoking are long lasting, and little benefit is gained unless smoking is stopped at least 8 weeks prior to surgery.
A patient who is unable to exercise is at increased risk for PPC following abdominal surgery. The inability to climb a flight of stairs or blow out a match at 6 inches (equals an FEV <1.76 L) suggests a very high pulmonary risk. The Goldman cardiac risk index and the American Society of Anesthesiologists classification reasonably predict pulmonary risk but not necessarily the severity of PPC. Clinically evident chronic obstructive pulmonary disease has been associated with four- to five-fold relative risk of PPC in patients undergoing surgery. Despite common belief, age and obesity, when controlling for other existing comorbidities, do not contribute significantly to the development of PPC.
Active asthma, when severe, can be among the most difficult respiratory conditions to manage, although its presence does not necessarily herald an increase in perioperative bronchospasm if appropriate prophylaxis is administered. Preoperative improvement of small airway patency, as evidenced by freedom from wheezing and a peak flow greater than 80% of predicted value, may minimize pulmonary risk in these patients. A short course of oral steroids may assist in achieving this preoperative goal. Even though history and physical examination may detect those at risk for PPC, no spirometric or other test detects those patients whose abdominal surgery should be canceled. Most patients can undergo surgery even if at high risk.
Although the optimal reduction regimen is unknown, the realization that postoperative pneumonia is extremely morbid and occasionally lethal in even a healthy patient demands adequate attention to perioperative pulmonary management.
Procedure-related Pulmonary Risk Factors
Limitation of surgery to the lower abdomen greatly reduces the extent of pulmonary dysfunction and the risk of developing PPC. Upper abdominal incisions increase this risk by as much as 40% in general surgery patients. A laparoscopic approach significantly reduces the risk of PPC by as much as 33%
The type of anesthesia, anesthetic pharmaceutical agent, and length of surgery play important roles in patient risk. Although reports have shown mixed results, spinal conduction anesthesia (spinal or epidural anesthesia) offers pain relief, improves pulmonary mechanics, and may significantly reduce the chance of PPC when compared with general endotracheal anesthesia.
Preoperative Evaluation
Using findings from the history and physical examination, one can select the majority of patients who are at risk for developing PPC. Although not considered a standard part of routine preoperative evaluation, preoperative pulmonary function testing may be indicated in specific patient subsets. The American College of Physicians has recommended spirometry to determine forced expiratory volume (FEV) in patients who have significant pulmonary risk factors or in those undergoing high-risk surgical procedures, particularly if requiring abdominal or thoracic incisions. Others have suggested minimal benefit of this intervention. These studies may delineate the etiology of pulmonary dysfunction; however, they rarely add value in terms of altering clinical management. Some have recommended that perioperative PaCO2 monitoring can assist in the management of those who are chronic CO2 retainers. Although hypercarbia is a significant risk for PPC, no validated published studies suggest a CO2 threshold which prohibits surgery. Baseline CO2 determination may be useful for postoperative ventilator management.
Although individual risk factors are important, several risk indices have been developed. Unfortunately, none has been validated scientifically to quantitate actual pulmonary risks. Included in these indices are abnormal findings during examination, risks related to Goldman cardiac risk assessment, and the Charleston comorbidity index. The time expenditure and expense of any invalidated algorithm are not justified in clinical practice.
Risk Reduction Strategies
The inability to quantify pulmonary risk highlights the importance for the gynecologist to develop clinical acumen in an effort to reduce pulmonary complications. Several risk-reduction strategies have been proposed (Table 44.8). Attention to maneuvers that enhance postsurgical lung expansion combined with adequate pain control to reduce splinting and subsequent atelectasis are the vital components of good postoperative pulmonary care. Preoperative education engages the patient in her care, increases her willingness and active participation, and assists in overcoming a major psychological obstacle to postoperative pulmonary health. The potential benefits of incentive spirometry, chest physiotherapy, and inhalational nebulizer treatments can be explained and understood preoperatively.
|
|
|
TABLE 44.8. Postoperative pulmonary complication risk-reduction strategies |
RENAL DISEASE
The anatomic relation of the urinary tract to the reproductive organs places it at risk for extrinsic (disease-related) or iatrogenic complications. Although intraoperative technique should be designed to decrease injury risk, perioperative renal insufficiency or failure is among the most foreboding postoperative complications faced by the gynecologic surgeon. The overall risk of urinary tract injury is procedure related and is not uncommon (≤2%). Preoperative urologic studies may reveal congenital anatomic or other abnormalities and a rare renal cancer. Importantly, radiographic evidence of ureteral deviation, displacement, or hydronephrosis should not be considered a substitute for good operative technique and cannot be equated with lessening the risk of injury. The 3% incidence of serious adverse events associated with IVP and its lack of cost effectiveness (approximately 833 IVPs necessary to potentially prevent 1 ureteral injury) draw attention to its routine use.
Total cessation of renal function (i.e., bilateral ureteral obstruction) results in a daily increase of 1 to 2 mg/dL in serum creatinine. Although the postoperative dynamics of measured serum creatinine are complex, lesser degrees of elevation (i.e., > 0.3 mg/dL per day) should raise suspicion for a unilateral ureteral injury.
Although overt oliguric renal failure rapidly becomes clinically obvious, lesser degrees of renal insufficiency may occur silently. Although all patients are at risk, the geriatric patient is at particular risk of perioperative renal insufficiency secondary to an age-related decrease in glomerular filtration rate, a decrease in urinary concentrating ability, and narrowed limits for sodium, potassium, and acid excretion. This population should be monitored carefully to maintain euvolemia and minimize the electrolyte load found in many medications.
Research has detailed the predominant biochemical and physiologic changes occurring in the patient with acute renal failure. Recognizing the important effects of medullary hypoxia, tubular cell injury, and alterations associated with diuretics and electrolytes assists in understanding the mechanisms of disease; however, the clinical usefulness of this new information has yet to make a significant impact on daily practice. Thus, the classic approach of evaluating intrinsic renal, prerenal, or postrenal etiologies of perioperative renal failure remains useful. Prerenal azotemia results from any condition which prevents adequate blood flow to the renal unit. Hypovolemia, renal artery atherosclerotic disease, and pharmacologic etiologies (e.g., a combination of ace inhibitors and diuretics) interfere with normal renal perfusion. Hypovolemia may occur as a result of intrinsic cardiac failure, general anesthesia, excessive blood loss, pre-, intra- or postoperative volume contraction, or physiologic vasodilation (e.g., as in septic shock). Most postoperative causes of prerenal azotemia are reversible with the correction of intravascular volume deficits, minimizing the effect of left ventricular dysfunction or the reversal of anesthesia.
Postrenal failure, which can be related to outflow tract obstruction at any level of the renal collecting system, carries significant importance following pelvic surgery. Functional obstruction due to a neurogenic bladder or the inability to void spontaneously may be related to existing deficits or postsurgical changes. Urethral catheterization typically reverses this problem. Postobstructive oliguria related to causes proximal to the bladder requires significant ureteral obstruction. Although this situation can occur with bilateral renal calculi, bilateral or unilateral obstruction can occur after prolapse surgery and it is most frequently encountered with advanced carcinoma of the cervix or in idiopathic retroperitoneal fibrosis. Renal ultrasonography is an easily obtained diagnostic study. Acute management of most causes of postrenal failure involve appropriate diversion of the urinary units, either by transvesical ureteral stenting or percutaneous nephrostomy, to preserve existing renal function.
Lastly, intrinsic renal dysfunction may be due to acute tubular necrosis, interstitial nephritis, and acute glomerulonephritis. Intrinsic renal failure most often is due to renal parenchymal ischemia or the effects of nephrotoxic agents, including aminoglycoside antibiotics, vancomycin, amphotericin B, and cisplatin. Radiocontrast agents and heme pigments are two agents commonly associated with acute tubular necrosis. The former may have intrinsic parenchymal effects and create a diuresis that aggravates existing volume deficits. Interstitial nephritis associated with an allergic drug reaction, autoimmune diseases, infiltrative diseases, and infectious agents represents another form of intrinsic renal failure. When present, withdrawal of the offending agent usually results in reversal; however, glucocorticoid administration may hasten recovery. Finally, acute glomerular nephritis, rare in the gynecologic patient, may also be responsible for intrinsic renal failure and should be entertained in the differential diagnosis of postoperative renal insufficiency, particularly in the absence of other causes.
Diagnosis, Morbidity, and Mortality
The initial diagnostic evaluation of women with perioperative renal insufficiency requires a systematic method of investigation. Intraoperative suspicion and assessment with cystoscopy (or cystotomy) and methylene blue or indigo carmine dye injection is an important initial step. Postoperative hypovolemia may be obvious. However, volume status determination may be difficult when based on history, physical examination, and quantitation of perioperative input and output data. The urinalysis in those with prerenal azotemia shows a high osmolality (>500 milliosmoles per kilogram), a fractional sodium excretion of less than 1%, and proteinuria. Elevated serum blood urea nitrogen out of proportion to creatinine (greater than 20:1 ratio) is strongly indicative of prerenal azotemia. Renal azotemia often is associated with minimal proteinuria; however, urine osmolality will be less than 350 milliosmoles per kilogram and fractional excretion of sodium will be greater than 1. The surgeon's degree of suspicion based on operative findings and events is an important aspect of assessment to exclude postrenal azotemia, particularly when the procedure required a difficult pelvic dissection, repair of a prolapse, or treatment of a malignancy. Renal ultrasonography can determine quickly the extent of unilateral or bilateral hydronephrosis and eliminate the possibility of clinically significant ureteral ligation or kinking. If an ultrasonograph is not diagnostic, an IVP may answer important questions, although the administration of contract may worsen the clinical condition of a patient with intrinsic renal insufficiency.
Nonoliguric and oliguric renal insufficiency can occur in the postoperative patient, and physicians should not assume that “adequate” urine production indicates intact renal function. Importantly, oliguric renal failure portends a worse prognosis than nonoliguric renal failure. Using low-dose dopamine to increase renal perfusion (and convert an oliguric problem to a nonoliguric situation) has no proven efficacy and, if unsuccessful, should be discontinued, because it creates a propensity for cardiac arrhythmias and alters blood supply to other vital organs.
The morbidity and mortality (fivefold) of renal failure in the postoperative patient is higher than that of individuals treated medically. These adverse outcomes probably are related to many factors, from perioperative ischemic insults to the volume depletion and other changes associated with contrast used for preoperative testing (i.e., IVP, CT) or mechanical bowel preparation. Common predisposing comorbid illnesses, including diabetes mellitus, hypertension, and cardiopulmonary insufficiency, carry their own inherent risks for causing renal insufficiency. Medications such as ace inhibitors and nonsteroidal antiinflammatory drugs, used frequently in the perioperative patient, also increase risk.
Methods to promote perioperative renal protection include practicing good surgical technique, limiting the use of nephrotoxic drugs, maximizing cardiopulmonary function by paying attention to intraoperative blood and volume losses, and replacing intravascular losses. Although invasive monitoring to guide fluid replacement may be helpful, its use and the administration of pharmacologic agents (dopamine, mannitol, furosemide) or other interventions has not been conclusively proven beneficial. Hopefully, continued research on adenosine and prostaglandin administration will prove fruitful.
Women with chronic renal insufficiency are at risk for acute renal insufficiency during the perioperative period. Preoperative internal medicine or nephrology consultation should be considered in an attempt to optimize volume, use dialysis strategically, and manage coexisting morbidities.
Management
Dialysis is the cornerstone of perioperative management of renal insufficiency once postrenal obstructions are relieved. Specialists should be consulted to treat acidemia, recalcitrant hyperkalemia, symptomatic volume overload, or impending cardiovascular failure. All medication dosages and schedules should be reviewed regularly to maximize efficacy and minimize toxicity.
In conclusion, although perioperative renal failure represents a significant danger to the operative patient, insufficient scientific data exist to identify patients at risk and to develop guidelines for postoperative renal surveillance and management. The surgical community awaits a more specific definition of renal failure, additional research regarding renal protection strategies, and better, less invasive treatments for patients with perioperative renal insufficiency.
WOUNDS AND INCISIONS
Once surgery has been deemed appropriate therapy, selecting the operative approach is possibly the most important initial surgical decision. Choice of approach is related primarily to physician bias and comfort, related to previous teaching and experience. However, surgical indications, disease process, previous abdominal incision (and resultant adhesions), patient preference, and existing medical comorbidity should be considered carefully prior to solving this sometimes complex problem. Adequate intraoperative exposure must be a primary consideration. Although a vertical lower midline incision should be the first consideration, some, particularly those with a large body mass index, may be best managed with an upper abdominal incision, avoiding trauma to the infection-prone panniculus. A panniculectomy may be necessary or appropriate. It is evident that many, if not most, gynecologic (even oncologic) and obstetric procedures can be completed safely through a more cosmetic transverse lower abdominal approach. The transverse approach may offer the additional advantage of less pain and diminished postoperative pulmonary dysfunction. Although the Pfannenstiel incision, when combined with a table-stabilized self-retaining retractor, will often suffice, preoperative consideration of a Maylard (rectus muscle splitting) incision or intraoperative conversion to a Cherney (rectus splitting–incision at pubic insertion) may be necessary. Regardless of the initial approach, to avoid hernia risks the incision should not be placed perpendicular to a previous incision. Placing the long axis of the incision in the direction of maximal skin tension creates the most aesthetically pleasing scar.
A more contemporary approach to numerous gynecologic procedures involves laparoscopy. Many, if not most, routine procedures and a significant proportion of complex procedures used for the management of benign or malignant disease can be safely completed laparoscopically, with less physiologic stress, less pain, and a more rapid return to normal activity. Although there are many correct answers to surgical incision placement, performing an incomplete procedure because of a compromised incision is an unacceptable alternative and should be avoided by immediate conversion to a more accommodating approach (e.g., hand-assisted laparoscopy or an open operation).
Operative laparoscopy and abdominal approach are associated with additional inherent surgical risks, so they should not replace vaginal surgery. Although laparoscopy may be complementary to “convert” abdominal procedures and to complete (extensive) operations, stand-alone vaginal surgery should remain an important arm of the obstetrician-gynecologist's surgical repertoire, because it results in less morbidity. Vaginal surgery will suffice for many, if not most, gynecologic procedures. Although lesser invasive (laparoscopic or vaginal) surgical approaches are associated with diminished physiologic stress, their use does not negate the need for appropriate preoperative evaluation, preparation, and management.
Wound Preparation
Although many rituals of preoperative skin preparation exist, only a few add documented value to patient care. Preoperative hair removal is not deemed necessary; however; if performed, clipper removal at a time close to surgery avoids microinjury and is associated with a lower risk of wound infection than is razor preparation.
Routine preoperative skin antisepsis is necessary to minimize the infectious potential of normal flora, as well as of pathogens. Bacterial concentrations in moist body areas (i.e., perineum) reach 106/cm2 of tissue and are greater than those in drier (abdomen) areas, reaching 103/cm2 of tissue. These areas also harbor different ratios of aerobic to anaerobic bacteria. Preparation solutions differ significantly in the immediate or late (>3 hours) mean bacterial reduction. Regardless of solution used, the preparation should be allowed to “set” for no less than 5 minutes to attain its maximal activity and bacterial reduction.
Surgical Technique
Creating an abdominal incision with a single bold knife stroke through the skin and subcutaneous tissue avoids a stairstep effect in the subcutaneous tissues. The use of multiple knife blades to create the incision offers little benefit and contributes to expense. Avoiding the creation of subcutaneous dead space is important because dead space increases the risk of wound infection and poor wound outcome, even when closed. The use of electrical or laser coagulation techniques to create an incision saves little time and adds little value. Their use creates “devitalized” tissue, which may contribute to an adverse wound environment and increase the risk of surgical site infection, resulting in acute or late poor wound outcome. Surgical technique may be of specific impact in those already at high risk because of thick (≥3.0 cm) subcutaneous tissues.
The rationale for proper suture selection rests on the need for tensile strength, the duration of retained tensile strength, and the biologic effects on the involved tissue (Table 44.9). In general, the suture's chemical composition is more important than the physical configuration, although braided and multifilament sutures may potentiate infection. When compared with other absorbable materials, polyglycolic acid suture is associated with less inflammation and decreased pain, and in animal models it lessens the risk of infection. The incorporation of permanent suture material creates an increased risk of (~10%) chronic wound problems (i.e., pain, wound sinus); however, their use is associated with a lessened risk of developing a fascial hernia. Vascular pedicle ligation can be accomplished safely using short-term absorbable sutures, because the risk of bleeding (1.5-mm vessels) is minimal 96 hours after ligation. There is little clinical benefit to be gained from peritoneal closure.
|
|
|
TABLE 44.9. Suture material |
Suture size selection should be based on specific needs. Excluding fascial closure, there is little rationale for using suture larger than 2-0. Additional wound suture material increases the inflammatory response and may predispose to infection, and the tensile strength of a 2-0 absorbable suture is adequate for nearly all pedicle ligations.
Although it seems basic, correct suture-tying techniques can contribute to surgical outcome. Complex knots (e.g., surgeon's) impart greater tensile strength than multiple simple square knots. Avoiding excess knots minimizes the amount of suture material, lessens inflammatory volume, and potentially decreases the risk of poor wound outcome. Although all knots should be secure, tightly tied fascial sutures strangulate the incorporated tissues, increase ischemia, and lessen wound strength. Although good surgical technique always has been tied to attempts to prevent adhesion formation, the development of hyaluronic acid products for adhesion prevention has opened new avenues.
The astute surgeon recognizes the different tissue-related healing curves and selects a suture designed to promote good outcome. Although short-term wound results are important, the risk of late problems (e.g., hernia) can be minimized with appropriate closure technique. A suture length–to–wound length ratio of greater than 4 decreases the risk of hernia formation and can be accomplished by placing sutures at least 1.5 cm from the fascial edge and 1.5 cm apart.
Subcutaneous tissue closure is typically unnecessary. If required to lessen tension on wound edges, small minimally reactive sutures should be chosen. Closed suction and subcutaneous drain placement are of little apparent benefit, and drains increase the risk of surgical site infection.
The best method or material for epithelial approximation should be related to the potential time, cost, need for return visits, and cosmetic results.
GASTROINTESTINAL CARE
Perioperative management of the gastrointestinal tract during pelvic surgery focuses on the following three aspects: (a) avoidance of operative injury and reduction of subsequent complications, (b) the role of early feeding, and (c) the appropriate diagnosis and management of patients with liver disease.
Excluding the need to address important aspects of coexisting intestinal diseases (e.g., inflammatory bowel disease) and issues related to cancer screening, gastrointestinal preparation values the decisions related to the incorporation of bowel preparation. Mechanical intestinal preparation offers a number of potential benefits (Table 44.10). Although suboptimal preparation may increase the risk of contamination, most pelvic surgeons are inclined to use a mechanical bowel preparation when the risk of manipulation or injury is substantial. Several regimens are used. Fleets Phospho-Soda (90 mL) is cost effective, well tolerated, and gives excellent results.
|
|
|
TABLE 44.10. Mechanical bowel preparation potential benefits |
Intestinal bacterial flora colony counts are high in the colon and distal ileum, decreasing dramatically in the more proximal small intestine unless obstructed. Classically the mechanical regimen is combined with oral antibiotics, typically including erythromycin or neomycin or both, to reduce luminal bacterial content. Although debate persists, the benefit of oral antibiotics over intravenous antibiotics is apparently small, and oral use is associated with significant gastrointestinal symptoms.
Early Oral Feeding and Nasogastric Suction
Nasogastric suction often has been incorporated into the postoperative care of women undergoing difficult pelvic operations. Reports not only question its use but deny its benefit as it relates to symptomatic relief, lessened risk of ileus, need for reinsertion, and protection of intestinal anastomosis. Regardless of procedure, fewer than 10% of patients require nasogastric suction, and it appears to be of little benefit to the other 90%. As importantly, early oral feeding is well tolerated, does not increase the risk of ileus or symptoms, and may shorten hospital stay.
Liver Disease
The preoperative detection of liver disease may not be easy, because serum enzymes (transaminase) may not be elevated in patients with late-stage disease. However, the historical and physical findings of significant alcohol intake or exposure to hepatotoxins should raise suspicion. Physical evidence of malnutrition, signs of hepatic encephalopathy, or jaundice usually signify advanced disease. Laboratory evidence of hepatic dysfunction includes an elevated (10-fold) increase in serum transaminase levels, abnormal coagulation study results, elevated total bilirubin values, and low serum albumin levels. Classic surgical risk indices have been based on the Child classification, initially detailed in the 1960s to determine risks associated with surgical management of those with esophageal varices. These indices have been applied to the risks in those with liver disease who are undergoing abdominal surgery.
Perioperative management of women with hepatic disease requires particular attention to drugs (and to their dosing and scheduling) which are metabolized by the liver. For example, patients receiving benzodiazepines and narcotics are at risk for drug accumulation and overdosage due to poor hepatic clearance.
Patients with acute liver disease (vital or other) should not undergo elective surgery until stabilization of liver dysfunction has been secured. Those with chronic liver disease and hepatic encephalopathy in an attempt to stabilize liver function may benefit from subspecialty consultation.
INFECTION
Perioperative surgical site infection occurs in the practice of every gynecologic surgeon. Knowledge of prophylactic measures and the optimal treatment regimen for those with active or acquired infection are expected of every pelvic surgeon. Numerous factors including obesity, diabetes, use of steroids, and even length of preoperative hospitalization are all risk factors for infectious perioperative morbidity (Table 44.11). Although addressing each of them is beyond the scope of this chapter, numerous technical methods can modulate these risks. Proper use of prophylactic antibiotics lessens infectious risks in many pelvic procedures. Numerous antibiotics and regimens are efficacious. In most situations a single dose, administered properly, is as effective as most multiple regimens. However, in longer procedures (i.e., ≥3 hours) when the duration of the procedure is longer than the half-life of the chosen drug or if blood loss exceeds 1,500 milliliters, repeat dosing improves its benefit. The use of antibiotics prophylactically can result in patient hypersensitivity and the development of resistant strains of bacteria. Although careful thought is never to be discouraged, the potential benefit of controlling operative site infection with antibiotic prophylaxis usually outweighs other patient risks. The authors use a second-generation cephalosporin, which has better anaerobic coverage than first-generation cephalosporins and minimizes the loss of Gram-positive coverage that typically occurs with third-generation cephalosporins, recognizing the lack of enterococcus coverage. Patients allergic to penicillin have an 8% risk of cross-reactivity with cephalosporins, but anaphylaxis risk is estimated at 0.0001% to 0.1% in non–penicillin-allergic patients to 0.02% in penicillin-allergic patients. Doxycycline or metronidazole represents an excellent alternative in patients undergoing abdominal or vaginal hysterectomy. Although the benefit of antibiotic prophylaxis has not been demonstrated in patients undergoing laparoscopy-assisted hysterectomy, it would seem prudent to use these drugs. The recommendation of prophylaxis for other procedures varies (Table 44.12). Specific prophylaxis for those women at risk for endocarditis is imperative (Table 44.13).
|
|
|
TABLE 44.11. Infection risk factors |
|
|
|
TABLE 44.12. Antimicrobial prophylactic regimens by procedure |
|
|
|
TABLE 44.13. Prophylactic regimens for prevention of endocarditis in susceptible patients undergoing genitourinary or gastrointestinal procedures. |
Treatment for Existing Infection
Prophylactic drugs are administered to patients in the absence of preoperative evidence of active infection. However, gynecologic patients with an obvious infection prior to surgery should receive an antibiotic treatment regimen appropriate for the type of infection. For example, patients with tuboovarian abscess should be treated with a broad-spectrum antibiotic regimen covering Gram-positive, Gram-negative, and anaerobic bacteria with a single or multiple drug regimen, according to patient acuity.
Postoperatively, antibiotics should be given for documented infection. It is clear that most postoperative febrile illness is not related to a documented infection. When postoperative fever, leukocytosis, and clinical picture suggest postoperative infection, an examination to identify potential sources should be performed. Source-directed therapy is appropriate. Adjunctive procedures, including CT or ultrasonographically guided drainage, may hasten recovery in patients with fluid collections or abscesses. In general, patients should receive adequate, broad-spectrum antibiotic treatment prior to surgical intervention.
THROMBOEMBOLISM
Thromboembolic phenomena, including deep venous thrombosis (DVT) and pulmonary embolism (PE), are inevitable following gynecologic surgery. A 1988 meta-analysis estimated a 6% to 7% proximal DVT risk and a 0.5% to 0.8% fatal PE risk in unprotected patients over 40 years of age undergoing abdominal surgery. This risk makes surgeons anxious because of the difficulty of diagnosing venous thromboemboli and the potential catastrophic outcome of fatal PE.
The impact and importance of postoperative thromboembolic prophylaxis is no longer a question. In a survey by the American College of Surgeons, approximately 96% of surgeons claimed they regularly used antiembolic prophylaxis. However, patient poll and chart review suggest that only one third of patients received adequate prophylaxis.
Despite the perception that venous emboli are a rare and unimportant event, all gynecologic patients should be considered at risk. The misconception regarding incidence is fostered by the high occurrence (~50%) of DVT and PE postdischarge. Additionally, surgeons have been anxious about the potential side effects of prophylaxis, because low-dose unfractionated heparin or low-molecular-weight heparin administration has been associated with postoperative bleeding and wound hematomas. The infrequent occurrence of heparin-induced thrombocytopenia also has created some anxiety regarding prophylaxis. Finally, the initial or primary cost of thromboprophylaxis has deterred some from its use, although some have agreed that prophylaxis is cost effective. Thromboembolic phenomena can be clinically silent, whereas complications related to prophylaxis are not easily missed by the gynecologic surgeon or the patient. Furthermore, according to the Rochester Epidemiology Project and other studies, the incidence of PE and DVT is increasing as women age. Prophylaxis in the gynecologic practice will become more important during the next decade.
Despite these common misperceptions, principles of good gynecologic perioperative care demand careful attention to the role and benefit of thromboprophylaxis. The American College of Chest Physicians published guidelines regarding perioperative thromboprophylaxis. Risk factor stratification (Table 44.14) allows delineation of low risk, moderate risk, high risk, and highest risk categories, with coincident risk of developing DVT, clinical PE, and fatal PE. Proposed recommendations for thromboprophylaxis strategies ranged from aggressive mobilization in the lowest risk patients, to the use of pneumatic compression hose, elastic stockings, or pharmaceutical methods with heparin (unfractionated or low-molecular- weight). Patients at highest risk are deemed candidates for combined mechanical and heparin prophylaxis.
|
|
|
TABLE 44.14. Levels of thromboembolism risk in surgical patients without prophylaxis |
A report suggested that the frequency of DVT following gynecologic procedures was approximately 16% (a range of 4%–38%). Fatal PE was reported in only 0.4% of the pooled sample. The cited risks for postoperative thromboembolic event included age greater than 40, history of venous embolism, surgery for cancer, and an abdominal surgical procedure. It was suggested that gynecologic oncology patients were at particularly high risk, fulfilling Virchow's triad of advanced age, cancer, and the hypocoagulable state; venostasis related to pelvic mass compression; vascular injury due to lymph node dissection; postoperative immobility; and the thrombogenic effect of chemotherapy. Importantly, the authors noted a 75% reduction in fatal PE (from 0.4% to 0.1%) with the use of appropriate thromboprophylaxis. The strongest evidence presented for thromboprophylaxis was a relative risk reduction of 64% with use of low-dose unfractionated heparin (reductive from 20% of patients to 7%). A dose response was suggested. Gynecologic cancer patients derived less protection than the noncardiac patients from the twice daily administration of low-dose unfractionated heparin. It would appear that dosing 3 times a day is more appropriate. Although of concern, the potential risk of bleeding complications was not reproducible. Importantly, aspirin use was deemed insufficient for thromboprophylaxis. Low-molecular-weight heparin has been associated with fewer bleeding complications and is being studied in comparison with low-dose unfractionated heparin. However, low-molecular-weight heparin, although extensively studied, did not meet the criteria for study inclusion by the American College of Chest Physicians, so it was not included in their recommendations.
In general, patients undergoing brief procedures require no prophylaxis except early mobilization. Patients having major gynecologic procedures for benign disease without additional risk factors should receive low-dose unfractionated heparin twice daily, low-molecular-weight heparin, or perioperative external pneumatic compression hose. For the highest risk patients, dual prophylaxis with either low-dose unfractionated heparin plus elastic stockings or external compression hose, low-dose unfractionated heparin 3 times daily, or low-molecular-weight heparin given in daily doses of at least 3,400 anti-Xa units may be useful for DVT/PE prevention. The duration of antithrombotic therapy in the highest risk patients is being studied, because there is some speculation that anticoagulation continued beyond the intermediate postoperative period may reduce the risk of thromboembolic phenomena as well as the risk of death.
NEUROLOGIC COMPLICATIONS
Avoiding serous perioperative neurologic sequelae, including stroke, seizure, altered mental status, and operation-associated nerve injury, is a vital aspect of perioperative management. Most general anesthetics adversely affect central nervous system function. Even short-term anesthetic use impairs psychomotor performance for 5 hours and sleep patterns for 24 hours or more. Women at risk for cerebrovascular disease (as evidenced by transient ischemic attacks, peripheral vascular disease, or other events) may require specific preoperative evaluation and neurologic consultation. Although an asymptomatic carotid bruit may signal the need for imaging studies or consultation, it does not, by itself, increase perioperative risk. Presurgical neurologic and radiologic evaluation, extracranial carotid endarterectomy, systemic anticoagulation, and platelet inhibition are some of the potential perioperative risk-sparing procedures to be considered. Central nervous system function is important for those women with arterial disease who are at risk for other thrombotic events and, regardless of risk, the adverse effect of perioperative hypotension (even of short duration) should be avoided. The overall risk of recurrent stroke approaches 3.0% but, fortunately, the risk of stroke is 0.2% to 0.7% in those with no such history.
Cerebral blood flow is unstable and brain metabolism is depressed for 6 to 8 weeks following a completed stroke, making it prudent to avoid any significant elective operations during this interval. The risk of a second infarct may approach 20%, and the mortality rate is high (~25%). Preoperative central nervous system (CNS) scanning may assist in determining the time of resolution of the initial infarct, when operative procedures are less likely to result in repeated infarct. Emergency procedures in those at risk for CNS infarct should completed in a perioperative environment that maintains an elevated blood pressure and avoids events that may increase the risk of CNS hypoperfusion.
Vertebral basilar ischemic episodes are associated with a lower perioperative stroke risk than is carotid ischemia. Although perioperative neurologic evaluation may be appropriate, these patients usually are managed medically, with minimal surgical risks.
Operative Neurologic Deficits
Nearly 2.0% of gynecologic procedures are associated with postoperative lower extremity neurologic deficits, regardless of attention paid to preoperative care or positioning. Multiple nerves are at risk, regardless of positioning, surgical duration, or approach. Mechanisms of nerve injury include prolonged compression (e.g., femoral nerve), excessive traction, stretch (e.g., sciatic nerve) or transection (e.g., lateral femoral cutaneous nerve). Regardless of the extent of injury, attention to positioning, or retractor placement, these problems occur and are managed by evaluation and rehabilitation. Fortunately, most resolve. Attention to minimizing hip flexion and external rotation potentially lessens the risk of traction injury. Ilioinguinal and iliohypogastric nerve injuries can be diagnosed with relief after local infiltration of nerve block or excision.
SUMMARY POINTS
· The primary goal of the pelvic surgeon involves prospective preoperative recognition, evaluation, and management of existing medical comorbidities. Every pelvic surgeon should commit to the development of operative techniques that form a surgical skill set geared to the safe completion of indicated surgical procedures.
· Appropriate consultation should be sought if the level of qualification does not fit the necessary procedure.
· A thorough, multisystem physical examination is an essential part of the preoperative evaluation to detect important coexisting disease. The suspicion or diagnosis of coexistent morbidities which have not been diagnosed previously requires preoperative investigation. Laboratory and radiologic investigation should be conducted patiently and procedures directed in a safe, cost-effective manner.
· Coexisting or occult cardiac disease represents a significant contributor to perioperative morbidity. Particular attention to the detection, evaluation, and management of cardiac risk factors including CAD, hypertension, congestive heart failure, valvular disease, arrhythmias, and hypercholesterolemia is imperative. Particular attention to ACLS guidelines is important. Perioperative assistance by personnel experienced in cardiac care should be invoked when necessary.
· Perioperative pulmonary care is an important concern. The procedure should be designed to minimize pulmonary risks when possible. Postoperative attention to pulmonary toilet may render the best possible outcome.
· Perioperative renal failure is associated with high morbidity and mortality. No intervention, including prophylactic low-dose dopamine, mannitol, or furosemide therapy, has been shown to be of any benefit in reducing the incidence of perioperative renal insufficiency.
· The optimal surgical incision is chosen according to the procedure done, existing comorbidity, disease process, and patient preference. Appropriate preoperative skin antisepsis is necessary and, in combination with intravenous antimicrobial agents, will decrease the incidence of wound infection. Good surgical technique is mandatory for wound health and maximizing patient outcome.
· Classically, bowel preparation (mechanical, with or without antibiotic) is undertaken prior to many gynecologic procedures. Nasogastric suction has not been shown to lessen the risk of ileus, and only 10% of patients require insertion of a nasogastric tube postoperatively. Most patients can be managed without nasogastric suction.
· Proper use of prophylactic antibiotics lessens infectious risks in many pelvic procedures. Single-agent broad-spectrum antibiotic use, such as cephalosporin, doxycycline, or metronidazole, appears to be safe and effective for women undergoing abdominal or vaginal hysterectomy.
· The American College of Chest Physicians published guidelines regarding perioperative thromboprophylaxis. Patients at low risk should be mobilized aggressively postoperatively. Those at moderate and high risk should use pneumatic compression hose, elastic stockings, or pharmaceutical methods. Patients at highest risk may also benefit from combined mechanical and pharmaceutical prophylaxis.
· Approximately 2% of gynecologic procedures are associated with postoperative lower extremity neurologic deficits. Special attention should be paid to patient positioning, surgical duration, proper use of surgical retractors to prevent excessive traction and stretch, and careful operative techniques.
SUGGESTED READINGS
General Considerations
Rutkow IM. Surgical operation in the United States. Then (1983) and now (1994). Arch Surg 1997;132:983–990.
Surgical Indications and Consent
Guidelines for referral to a gynecologic oncologist: rationale and benefits. Gynecol Oncol 2000;78:S1–S13.
Birkmeyer JD, Siewers AE, Finlayson E, et al. Hospital volume and surgical mortality in the United States. N Engl J Med 2002;346:1128–1135.
Montz HG. “Curbside” consultations in gynecologic oncology: a close look at a common practice. Gynecol Oncol 1999;74:456–459.
Preoperative Evaluation and Testing
Orr JW Jr. Preoperative care. In: Gershenson D, ed. Operative gynecology. Philadelphia: WB Saunders, 2001.
Hodges PJ, Kam PC. The perioperative implications of herbal medicines. Anaesthesia 2000;57:889–899.
Fischer SP. Cost-effective preoperative evaluation and testing. Chest 1999;115:96S–100S.
Roizen MF. More preoperative assessment by physicians and less by laboratory tests. N Engl J Med 2002:342:204–206.
Brooks-Brunn JA. Predicators of postoperative pulmonary complications following abdominal surgery. Chest 1997;111:564–571.
Eagle KA, Brundage BH, Chaitman BR, et al. Guidelines for perioperative cardiovascular evaluation for noncardiac surgery: report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Circulation 2002;105:1257.
Fleisher LA, Eagle KA. Lowering cardiac risk in noncardiac surgery. N Engl J Med 2001;345:1677–1682.
Raymer K, Yang H. Patients with aortic stenosis: cardiac complications in non-cardiac surgery. Can J Anaesth 1998;45:855–859.
Proceedings of the American College of Chest Physicians Fifth Consensus on Antithrombotic Therapy 1998. Chest 1998;114:439S–769S.
Eagle KA, Rihal CS, Mickel MC, et al. Cardiac risk of noncardiac surgery: influence of coronary disease and type of surgery in 3368 operations. CASS Investigators and University of Michigan Heart Care Program. Coronary Artery Surgery Study. Circulation 1997;96:1882–1887.
American Heart Association. ACLS Provider Manual. Dallas: American Heart Association, 2001.
Perioperative Pulmonary Evaluation
Smetana GW. Preoperative pulmonary evaluation. N Engl J Med 1999;340:937–944.
Renal Disease
Novis BK, Roizen MF, Aronson S, et al. Association of preoperative risk factors with postoperative acute renal failure. Anesth Analg 1994;78:143–149.
Gilmour DT, Dwyer PL, Cary MP. Lower urinary tract injury during gynecologic surgery and its detection by intraoperative cystoscopy. Obstet Gynecol1999;94:883–889.
Wounds and Incisions
Orr JW Jr, Orr PF, Bolen D, et al. Radical hysterectomy: does the type of incision matter? Am J Obstet Gynecol 1995;173:399–406.
Labib M, Palfrey S, Paniagua E, et al. The postoperative inflammatory response to injury following laparoscopic assisted vaginal hysterectomy versus abdominal hysterectomy. Ann Clin Biochem 1997;34:543–545.
Orr JW Jr, Orr PF. Perioperative care. In: Greer BE, Montz FJ. Atlas of clinical gynecology, vol 4. 1998.
Soper DE, Bump RC, Hurt WG. Wound infection after abdominal hysterectomy: effect of the depth of subcutaneous tissue. Am J Obstet Gynecol1995;173:465–469.
Vrijland WW, Tseng LN, Eijkman JH, et al. Fewer intraperitoneal adhesions with use of hyaluronic acid-carboxymethylcellulose membrane: a randomized clinical trial. Ann Surg 2002;235:193–199.
Gastrointestinal Care
Zamora O, Pikarsky AJ, Wexner SD. Bowel preparation for colorectal surgery. Dis Colon Rectum 2001;44:1537–1549.
Cheatham ML, Chapman WC, Key SP, et al. A meta-analysis of selective versus routine nasogastric decompression after elective laparotomy. Ann Surg1995;221:469–478.
Andrews FJ. Early postoperative feeding after major gynecologic surgery: evidence-based scientific medicine. Am J Obstet Gynecol 2001;185:1–4.
Pearl ML, Frandina M, Mahler L, et al. A randomized controlled trial of a regular diet as the first meal in gynecologic oncology patients undergoing intraabdominal surgery. Obstet Gynecol 2002;100:230–234.
Infection
ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists. Washington, DC: ACOG, 2001.
Scher KS. Studies on the duration of antibiotic administration for surgical prophylaxis. Am Surgeon 1997;63:59–62.
Cinat ME, Wilson SE, Din AM. Determinants for successful percutaneous image-guided drainage of intra-abdominal abscess. Arch Surg 2002;137:845–849.
Thromboembolism
Gertz W, Heit J, Clagett G, et al. Prevention of venous thromboembolism. Chest 2001;119:132S–175S.
Silverstein MD, Heigh JA, Mohr DV, et al. Trends in the incidence of deep vein thrombosis and pulmonary embolism: 1. 25-year population-based study. Arch Intern Med 1998;158:585–593.
Maxwell GL, Synan I, Dodge R, et al. Pneumatic compression versus low molecular weight heparin in gynecologic oncology surgery: a randomized trial. Am Coll Obstet Gynecol 2001;98:989–995.
Neurologic
Warner MA, Warner DO, Harper CM, et al. Lower extremity neuropathies associated with lithotomy positions. Am Soc Anesth 2000;93:938–942.
Wong GY, Warner DO, Schroeder DR, et al. Risk of surgery and anesthesia for ischemic stroke. Am Soc Anesth 2000;92:425–434.