Keith H. Nelson
Lewis H. Nelson III
The use of ultrasonography in obstetrics and gynecology has made sweeping changes in the management of pregnant patients. The purpose of this chapter is to review existing recommendations regarding the use of ultrasonography in pregnancy. The background setting of a patient's progress in pregnancy—from her initial visit confirming an intrauterine pregnancy through the anatomic survey to her third-trimester testing—was chosen. Many excellent textbooks dedicated to obstetric ultrasonography already exist. This chapter is intended to provide information about current ultrasonographic practice, guidance for performing the examination, and assistance in recognizing common anomalies. Future ideas and new technology will be reviewed at the end of the chapter.
Most ultrasound providers recognize two categories of examination: a basic ultrasonographic examination that includes a routine anatomic survey, estimate of gestational age, evaluation of placenta and amniotic fluid, and evaluation of maternal anatomy; and a more comprehensive examination that may be targeted based on the abnormal findings in a basic examination. In the past, the terms “level I” and “level II” examination were used erroneously to describe these two categories. Such classification schemes must be avoided to prevent misguided patient and physician expectations for the purposes of the examination. Every ultrasonographic examination should be as complete as possible within the limits of the provider and equipment. An ultrasonogram performed simply for the purpose of sex determination that fails to identify an anencephalic fetus has certainly done only harm. A limited ultrasonographic examination for a specific purpose, such as evaluation of fetal presentation, is appropriate in cases in which the pregnancy has been examined previously or in a clinical emergency.
GENERAL PRINCIPLES
Ultrasound images are generated using the same principle as sonar. High-frequency sound waves (3.5-7.5 MHz) pass from the surface of the ultrasound transducer through the tissues of the imaging target. Echoes of the transmitted sound waves return to the transducer. Because the average speed of ultrasound in human tissue is known (1,540 m/s), the distance of the reflector from the transmitter can be calculated using the time required for the echo to return. The resulting depth and signal strength data are plotted on a display screen. The position on the screen corresponds to the depth in the tissue. The brightness of the picture element corresponds to the strength of the return signal. Ultrasound systems display a black background and use increasingly bright shades of gray and white to represent stronger echoes.
The acoustic impedance for a tissue determines the degree to which that tissue reflects or transmits ultrasound energy. Because the acoustic impedance of tissue varies by density and consistency, interfaces between dissimilar tissues and within heterogeneous tissues act as reflectors that echo part of the transmitted signal back to the transducer. The degree of dissimilarity between one tissue type and the next determines the strength of the return echo received. Simple fluids such as water or amniotic fluid generate very few echoes, because they are homogeneous. Bone generates very strong echoes because the adjacent soft tissues have very dissimilar acoustic properties, producing a marked acoustic impedance mismatch. The strength of the return echo also depends on the angle between the face of the reflector and the ultrasound beam. As the reflector becomes closer to perpendicular with the transmitting source, a greater proportion of the echo is received. This property is well illustrated by the midline structures of the fetal brain, which are imaged best when perpendicular to the incident beam. The strength of the transmitted signal, which is controlled by the ultrasound operator, also contributes to the strength of the return echo.
Transducers spend only a small fraction of the time generating the ultrasound signal compared with the time spent detecting return echoes. The duty factor, expressed as the time spent transmitting divided by the time spent listening, is on the order of 0.01 for modern equipment. When a patient has an ultrasonographic examination lasting 20 minutes, the maternal and fetal total exposure to ultrasound energy is only 12 seconds. This exposure increases when Doppler sonography is employed due to the longer energy pulses.
The American College of Obstetricians and Gynecologists (ACOG) and American Institute of Ultrasound in Medicine (AIUM) recommend that ultrasound systems used for obstetrics display the thermal index (TI) and mechanical index (MI) of acoustic output on the screen. The TI is an estimate of the increase in temperature in tissue due to conversion of mechanical energy from the ultrasound beam to heat. Values of the TI less than 1.0 are not of concern for generating significant temperature changes. Temperature increases are most likely to occur during Doppler ultrasonography because of the larger duty factors. The MI estimates the compressive and decompressive forces caused by the ultrasound beam. If these mechanical forces are excessive, microscopic bubbles might form in the tissue being imaged. This bubble formation is called cavitation. As long as the MI values are less than 1.0, cavitation is not a concern.
The Food and Drug Administration has set the upper limit of acoustic intensity at 94 mW/cm2 (spatial peak temporal average) for obstetric ultrasonography. For other applications, ultrasound systems are limited to a maximum output of 720 mW/cm2. Furthermore, the systems must display the TI and MI if either or both of these indices can exceed 1.0. Because many systems can be used for both obstetric and nonobstetric ultrasonography, the provider should be aware of the acoustic output and TI and MI of the system in use. Overuse of power Doppler and color Doppler imaging is especially noteworthy as settings in which the recommended maximums could be exceeded. The ALARA principle (as low as reasonably achievable) has been suggested to govern the amount of fetal exposure to ultrasound energy while obtaining useful image data. The ultrasound provider should also remember that although there are no known bioeffects of diagnostic ultrasonography, future discoveries of adverse effects are certainly possible. As such, obstetric ultrasonography should be used only when indicated (Table 8.1).
|
|
|
TABLE 8.1. Indications for ultrasonography in pregnancy |
Ultrasonographic images are most correctly described using terms that acknowledge sound as the source of the image. Highly sound-reflective structures that produce large reflections and correspondingly bright screen images are called hyperechoic or hyperechogenic structures. Regions that produce very few echoes are termed hypoechoic or hypoechogenic. Regions that are echo free are termed anechoic. The reader is encouraged to avoid terms such as translucent or sonolucent, which are derived from the Latin root lucere, meaning “to shine.”
INDICATIONS
The currently accepted ACOG recommendations for ultrasonographic examination in pregnancy are based on the opinion of a National Institutes of Health consensus panel and are summarized in Table 8.1.
Several studies have addressed the question of whether routine ultrasonographic screening for all pregnancies should be performed. Recommendations from ACOG, based on an analysis of existing literature, suggest that women with low-risk pregnancies should not receive screening ultrasonography unless medically indicated. Thus far the evidence indicates that there is no reduction in perinatal morbidity or mortality from routine ultrasonographic screening in the low-risk population. The rate of unnecessary interventions in pregnancies screened with routine ultrasonography is also unchanged. There are not yet enough data to conclude whether fetuses with life-threatening anomalies have an improved outcome because of routine ultrasound use.
Although these studies demonstrate that routine ultrasonography in the low-risk pregnancy is not effective in improving perinatal mortality or morbidity, there are articles and editorials challenging those conclusions. Many of these studies offered routine screening to all patients except those who would stand to benefit most. Furthermore, a population agreeing to participate in a randomized study of routine screening does not necessarily constitute an accurate cross-section of the intended study population. The ability to perform a physical examination on the second patient—the fetus—is important. When performed with adequate equipment by properly trained personnel, prenatal ultrasonographic examinations can and do offer important information to the provider and patient.
Good evidence exists to demonstrate that fetal anatomic surveys are over 99% specific in detecting anomalies; that is, when ultrasonographic examination findings are normal, the fetus will indeed be normal over 99% of the time. The sensitivity of the anatomic survey, or the probability that an ultrasonogram will demonstrate an anomaly if one is present, varies widely depending on the ultrasound provider, the quality and age of the ultrasound system, the anomaly in question, and the frequency of the anomaly in the practitioner's own population. For this reason, it is recommended that ultrasound specialists perform examinations for genetic screening or evaluation of abnormal scan results.
FIRST TRIMESTER
With the advent of extremely sensitive home pregnancy tests which can detect human chorionic gonadotropin (hCG) levels down to 20 to 30 mIU/mL, the early diagnosis of pregnancy is now within reach of the typical consumer. Initial visits to the obstetrician can occur earlier instead of later, sometimes even before the first missed menstrual period.
Ultrasonographic examinations in the first trimester should be performed with transvaginal imaging and augmented with transabdominal imaging, if necessary. Although first-trimester detection of an intrauterine gestation is possible, it still is limited by the size of the gestation. Corresponding levels of serum β-hCG help to determine a threshold level at which sonographic evidence of an intrauterine pregnancy should be detected. Various sources place this level between 1,500 and 2,000 mIU/mL for transvaginal sonography and 3,000 and 5,000 mIU/mL for the transabdominal approach. Protocols have been developed for the management of patients with a positive pregnancy test but no ultrasonographic evidence of intrauterine gestation. This scenario may be of concern for ectopic pregnancy, especially when there is pain or vaginal bleeding. In the clinically stable patient, a repeat ultrasonogram in 3 to 7 days may yield more useful information and help avoid errors in management.
Two methods are commonly used for determining the gestational age in the first trimester. These are the mean sac diameter (MSD) and the more accurate crown-rump length (CRL). The MSD is determined by two methods. The method selected depends on the reference table used to determine the gestational age. The first method involves imaging the sac and measuring the longest axis (length) and the largest axis perpendicular to the long axis (width). These two orthogonal measurements are averaged and the value used to estimate a gestational age. The second technique requires the addition of the depth of the sac from an image that is transverse and perpendicular to the length. The three values are averaged and an appropriate table used (Fig. 8.1). The CRL is measured from an image of the fetus that includes the maximum distance from the cephalic pole to the caudal pole. Although the CRL is regarded as highly accurate in determining the gestational age, the biparietal diameter (BPD) in the late first trimester and before 20 weeks of gestation offers comparable accuracy. The MSD is more useful if no embryo is present in a gestational sac. The identification of a yolk sac or an embryo determines that a gestational sac is present. Using transvaginal ultrasonography, an embryo should be seen by 5 to 6 weeks of gestation as measured from the first day of the last menstrual period.
By the time the CRL equals 5 millimeters, cardiac activity should be seen. If the CRL is less than 5 millimeters, the examination should be repeated. Table 8.2lists the signs of an abnormal gestation. If the patient is at 6 weeks of gestation with a positive pregnancy test and there is no gestational sac visualized in the uterus, an ectopic pregnancy is highly suspect.
|
|
|
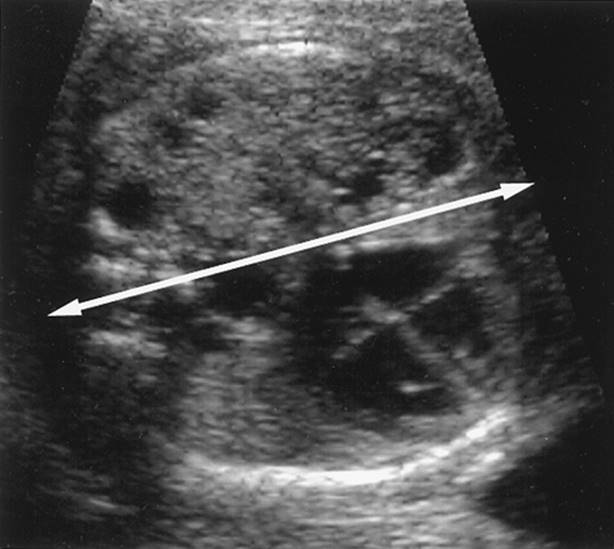
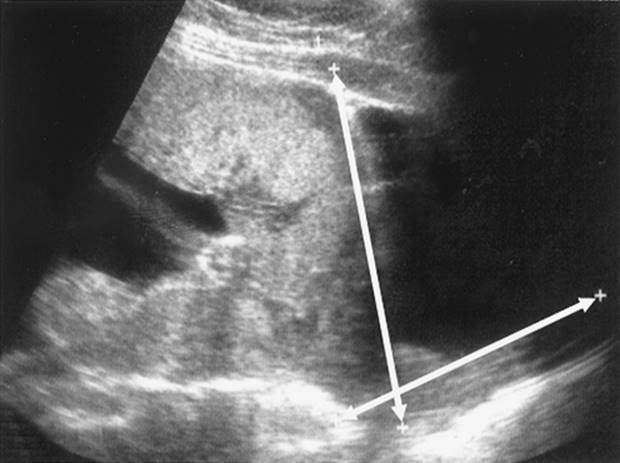
FIG. 8.1. Measurement of the mean sac diameter (MSD). The distances measured by the calipers in the longitudinal axis (A, number one) and the depth (A, number two) and the transverse diameter measured in (B) are added together and divided by three to produce the MSD. Some authors use only the sum of the longitudinal and depth measurements divided by two. |
|
|
|
TABLE 8.2. Signs of an abnormal gestation |
The obvious diagnosis of an ectopic pregnancy, in which a small gestational sac with cardiac activity present is seen outside the uterus, can be made even when serum β-hCG levels are not at the threshold for determination of intrauterine pregnancy. The more difficult ectopic pregnancy cases usually involve abnormal adnexal findings such as ovarian or paratubal cysts, free peritoneal or pelvic fluid, but no definite pregnancy sac. The pseudogestational sac may be seen when the endometrium responds to chemical changes of pregnancy and may resemble a fluid-filled structure within the endometrial cavity. Some authors describe a ring of fire that may be seen around ectopic pregnancies developing in the adnexa when evaluated with color Doppler interrogation or power Doppler imaging (Fig. 8.2). The ring represents increased blood flow about the developing embryo, but it is possible for a corpus luteal cyst or even normal ovarian tissue to demonstrate such a ring. It is recommended that further diagnostic information be gathered, using sequential determination of serum β-hCG levels and clinical findings, as long as the clinical situation is stable.
|
|
|
FIG. 8.2. Ring of fire. A corpus luteum (A) can be confused with an ectopic pregnancy (B). The arrow indicates blood flow in the embryo (B). (From Diana M. Strickland, RDMS, RDCS; with permission.) See color figure 8.2. |
When the serum β-hCG levels are abnormally high (greater than 100,000 mIU/mL) for the estimated gestational age by last menstrual period dating or by the uterine size, the diagnosis of molar gestation should be entertained. The classic “snowstorm” description of ultrasonographic imaging in molar gestation has been discarded to reflect the improved resolution of ultrasound transducers. A complete molar pregnancy, in which no fetal tissue is identified, may demonstrate clusters of vesicles on ultrasonographic examination. Identification of a partial molar pregnancy is more difficult, but it may be suggested by the presence of a fetus with a cystic or multicystic placenta (Fig. 8.3). The fetus might demonstrate numerous anomalies, including findings consistent with triploidy.
|
|
|
FIG. 8.3. Partial mole. The placenta appears cystic and enlarged for gestation. No fetal heartbeat was noted and, although fetal tissue was found at pathology, no chromosome studies were obtained. |
During imaging of the early fetus several important features should be visualized. The number of fetuses in the uterus should be reported. A multiple gestation should not be diagnosed until the yolk sacs or embryos can be counted. This will avoid counting the empty gestational sac of an anembryonic pregnancy or blighted ovum as a viable pregnancy. Early gestation may be the best possible time to determine the amnionicity and chorionicity of multiple gestations, information of crucial importance in the later management of these pregnancies. A thick rim of tissue surrounding each fetus is more suggestive of dichorionic, diamniotic gestations. If the intervening tissue is thin or absent, monochorionic, diamniotic, or even monoamniotic gestations are more probable. Conjoined twins may also be detected in the first trimester (Fig. 8.4). Determination of zygosity is possible only if a monoamniotic with monochorionic or diamniotic with monochorionic configuration is found, in which case the twins are monozygotic. Placentation in multiple gestations is often an important clue in determining zygosity and the risk of twin-to-twin transfusion syndrome. The single placenta associated with monochorionic monoamniotic twinning can be identified during the first and second trimesters. A fused placenta will appear as a single placenta but with the additional finding of dichorionic diamniotic membranes (Fig. 8.5). Determination of fetal sex also may be helpful in determining zygosity.
|
|
|
FIG. 8.4. Conjoined twins. In (A) the twins are joined at the abdomen (abdominophagus) and separated at the chest (B). |
|
|
|
FIG. 8.5. Fused placenta with diamniotic, dichorionic membranes. The fused chorions (open arrow) are noted between the amnions (closed arrow) of each twin. The twins could be either mono- or dizygotic. |
The fusion of the expanding amnion with the chorion, obliterating the intervening space, occurs around 12 weeks. Prior to this union, the unfused amnion may be seen as a wispy echogenic membrane surrounding the developing fetus and should not be confused with a gestational sac (Fig. 8.6). It is theorized that rupture of the unfused amnion followed by settling of the fragmented ends onto the surface of the developing embryo is the source of amniotic band syndrome. These disruptions of normally developing fetal anatomy may lead to amputations of random fetal parts or even to fetal death.
|
|
|
FIG. 8.6. Incomplete fusion of the amnion in the first trimester (A). The amnion in the singleton gestation resembles the membrane in a multiple gestation. However, in a different plane (B) the amnion surrounds the embryo in a more characteristic manner. |
Later in the first trimester it may be possible to identify the normal rotation of the fetal gut, which occurs in the proximal part of the umbilical cord (Fig. 8.7). Such normal development may be confused with an omphalocele, an abnormality of the abdominal wall at the umbilical ring. Completion of gut rotation occurs by week 14, with subsequent resolution of the normal developmental hernia.
|
|
|
FIG. 8.7. Normal rotation of the fetal gut. The double arrow indicates the portion of the umbilical cord transiently occupied by the fetal gut during migration and rotation. |
One of the earliest markers for aneuploidy in the developing fetus is an abnormally thick but hypoechoic ridge of skin over the nuchal portion of the skull. This may be detected in the first trimester and is suggestive of, but not diagnostic of, Down syndrome (trisomy 21). Some authors believe that this thickened region represents a resolving cystic hygroma that is characteristic of many fetuses with Down syndrome. Further discussion of nuchal hypoechogenicity can be found in the “Second Trimester” section.
The placenta is due more than the typical cursory glance during the first trimester. Early detection of placenta previa is possible but should be interpreted with caution. As the lower uterine segment develops in pregnancy, placentas that were previously low lying or covering the internal cervical os may no longer occupy that precarious location. The placenta may seem to migrate away from the os. The change actually occurs due to preferential placental development in areas of improved blood flow and regression in poorly supplied regions. Blood flow in the lower uterine segment is less marked than in the fundus, encouraging placental development away from the lower uterine segment. Other abnormalities such as succenturiate lobes and circumvallate or circummarginate placentas may also be seen in the first trimester (Fig. 8.8). In cases of suspected placenta previa, transvaginal imaging can be performed to confirm the placental location relative to the cervix. Doppler flow studies may also reveal a vasa previa, in which the fetal vessels lie across the internal cervical os. This phenomenon may occur secondary to a succenturiate lobe or velamentous umbilical cord insertion.
|
|
|
FIG. 8.8. Succenturiate lobe. The succenturiate lobe (S) is connected to the placenta (P) by the bridge of tissue and vessels. |
Careful imaging of maternal anatomy should not be neglected in the excitement of finding a new pregnancy. Abnormal uterine masses such as leiomyomata (Fig. 8.9) or maternal embryologic abnormalities such as a bicornuate or septate uterus (Fig. 8.10) may be identified most easily when the pregnancy is not large enough to occlude good visualization. More unusual developments such as anterior and posterior sacculation of the uterus may be visualized, but these findings are extremely rare. Abnormalities of the adnexal structures in pregnancy may include any of the typically encountered abnormalities in the nonpregnant state. The most commonly encountered ovarian neoplasm in pregnancy is the mature teratoma or dermoid. Hemorrhagic cysts of the corpus luteum have the sonographic appearance of complex adnexal masses, but they usually will resolve over time (Fig. 8.11).
|
|
|
FIG. 8.9. The fibroid is located anteriorly in the uterine wall and distorts the outer contour of the uterus, which helps to differentiate this from a uterine contraction. |
|
|
|
FIG. 8.10. Transverse section of a bicornuate uterus in the first trimester. The gestational sac is in the right horn and the left horn shows decidual changes. |
|
|
|
FIG. 8.11. Hemorrhagic corpus luteum cyst. In February (Feb) the cyst is complex, but by April (Apr) it has resolved and a normal ovary is present. |
SECOND TRIMESTER
A complete fetal anatomic survey can be performed most comprehensively in the late second trimester. This head-to-toe examination of the fetus identifies normal fetal anatomy, many but not all structural abnormalities, and markers for aneuploidy. As previously mentioned, there is not a consensus on the best use of ultrasonography in screening for abnormal pregnancies in low-risk populations. Additional information should be used to identify patients who will benefit from ultrasonographic examination. This information includes a family history of abnormal pregnancies or genetic anomalies, teratogenic exposures, abnormal laboratory findings including the maternal serum α-fetoprotein-human chorionic gonadotropin-estriol triple test, and abnormal clinical findings in the developing pregnancy.
In some cases, the second trimester marks the first prenatal visit for patients. Such patients often will depend on ultrasonography for an accurate estimation of the gestational age. This estimation is based on ultrasonographic measurements of the BPD, head circumference (HC), abdominal circumference (AC), and femur length (FL). These values are averaged to generate a composite score that is compared with standards. Some equipment calculates the average automatically. Additional measurements that may improve the accuracy of age determination include other long bone lengths, foot length, cerebellar width, and intraocular distance.
The physician must ascertain that only normal measurements are averaged. For example, adding the abnormal measurement of a shortened femur in skeletal dysplasia to the head and abdominal measurements will produce an incorrect gestational age. Two approaches can be used to calculate the gestational age if the anatomy is abnormal. One is to omit the data from the abnormal part. For example, obtaining the estimated fetal weight of an anencephalic fetus using the ultrasound system may require the BPD or HC. Because cranial measurements will be abnormal in this case, an equation that uses only the AC and FL can be used. The other option is to substitute a normal measurement from a table containing such data for the same point in the gestation as the patient. In the case of the anencephalic fetus, the appropriate head measurements for gestational age can be found in a reference table and substituted for the abnormal measurements.
The anatomic survey seeks to identify major structures in the developing fetus. During this survey, many abnormal ultrasonographic findings may be discovered. Such findings will lead to referral or subsequent diagnosis of abnormal conditions. Table 8.3 contains only a few of the more commonly encountered findings and anomalies that warrant further investigation.
|
|
|
TABLE 8.3. Abnormal ultrasonographic findings by location and potentially associated diagnoses |
DOCUMENTATION AND THE BASIC ULTRASONOGRAPHIC EXAMINATION
Standards for performing an ultrasonographic examination can be found on the Web sites of the national organizations involved in ultrasound practice: the American College of Obstetricians and Gynecologists (ACOG.org), the American Institute of Ultrasound in Medicine (AIUM.org), and the American College of Radiology (ACR.org). Because these standards are being updated continually, they are not repeated here. These standards are developed with the intention of improving patient care and assisting the physicians and sonographers performing the examinations. The flow of the basic examination is important because, with a disciplined approach, the examiner will have the opportunity to recognize a majority of congenital defects while obtaining information about the normal pregnancy. The examiner should develop a technique for performing the examination that is logical and consistent with published standards. The technique that follows is not the only method but is one that has proved helpful to the initiate and the experienced.
Standard orientation should be used. On a transverse scan, the patient's right is on the left of the image. On a longitudinal scan, the patient's head is placed on the left of the image. If standard orientation is not used, the images should be labeled to provide orientation to the interpreter. Any measurement should be accompanied by an image. Documentation can be by any combination of thermal photographs, videotape, digital images, or radiographic film. Thorough documentation of the ultrasonographic examination is imperative for providing a historical reference for future examinations, images for referrals, and a permanent record for the patient's file.
After fetal heart activity is confirmed, begin imaging in the long axis of the uterus and move to the maternal adnexae to look for ovarian and adnexal masses. The large venous complexes in the adnexae during pregnancy should not be confused with pathology. Return to the midline of the uterus, and locate and document the lowest edge of the placenta. Although this image will not help with the lateral location of the placenta, it will document anterior or posterior orientation and the extent to which the edge approaches the cervical os. A transvaginal or translabial ultrasonographic examination may be necessary to locate the lower edge of the very low-lying placenta (Fig. 8.12). Document the area of the cervix unless the bladder is overly filled. Document the placental umbilical cord insertion site in order to diagnose possible marginal or velamentous cord insertions and to assess for vasa previa. The number of vessels in the umbilical cord should be documented in a cross-section of the cord, at the fetal cord insertion, or by visualization of the umbilical arteries around the bladder (Fig. 8.13). By this point in the examination, there should be a general impression of amniotic fluid volume. An amniotic fluid index (AFI) is not required in most standards; a subjective determination is acceptable. If more examinations are anticipated during the pregnancy or there is a question about the trend in fluid volume, the AFI provides consistency among examiners.
|
|
|
FIG. 8.12. Low-lying, posterior placenta. In (A) the placenta (P) could be mistaken for a posterior placenta previa. Transvaginal ultrasound (B)demonstrates the lower border of the placenta (P) separate from the internal os (OS) by the distance indicated between the plus signs (+). |
|
|
|
FIG. 8.13. The umbilical arteries around the fetal bladder frequently can be seen without the use of color Doppler as in (B). |
Document the lie and presentation of the fetus with a longitudinal scan of the fetal axis. Subsequent imaging of the fetus transverse to the longitudinal fetal axis is usually most helpful. Begin with the fetal head. This provides an opportunity to diagnose cranial defects, which are both common and serious, and to locate the anatomy for the head measurements (BPD and HC) used in determining gestational age (Fig. 8.14). A normal cavum septum pellucidum eliminates the diagnoses of agenesis of the corpus callosum, hydranencephaly, hydrocephaly, holoprosencephaly, and anencephaly (Fig. 8.15). The plane used for measurements should be documented. The choroid plexuses are near the anatomic plane for the BPD. Choroid plexus cysts will appear as smooth-walled anechoic spaces within the echogenic choroid plexus (Fig. 8.16). The risk of a chromosomal anomaly with the isolated finding of choroid plexus cysts during a routine ultrasonographic examination is less than the risk associated with amniocentesis, regardless of the number or persistence of the cysts.
|
|
|
FIG. 8.14. Reference plane for the biparietal diameter and head circumference. The cavum septum pellucidum is a major landmark for this reference plane and for anomaly screening. |
|
|
|
FIG. 8.15. The cavum septum pellucidum is absent in anencephaly (A) because the cranium and majority of the brain are absent. In holoprosencephaly (B) it is absent because the normal brain midline is not developed. |
|
|
|
FIG. 8.16. Unilateral choroid plexus cyst. In the absence of other ultrasonographic findings or risk factors, the chances for trisomy 18 are less than the risk from an amniocentesis. This is also the case even if there are multiple or bilateral cysts (inset). |
Posterior and inferior to the BPD plane is the cerebellum. Documentation of a normal configuration will provide assurance that there is a minimal chance of an open neural tube defect (Fig. 8.17). Slightly more inferior, the nape of the neck is visualized. Abnormalities in this area include cystic hygromas or posterior encephaloceles (Fig. 8.18). Identification of nuchal translucency, more properly termed nuchal hypoechogenicity, is accomplished in the same plane. Although the finding of nuchal hypoechogenicity in the first trimester appears to be a promising tool to screen for aneuploidy, it should be regarded as investigational. The most recent ACOG recommendation is that nuchal skin measurements should not be used clinically until better standardization is developed and more convincing data support such a practice. The fetal neck is smaller than the fetal head, so any enlargement should be evident. Fetal goiters or teratomas may be seen anteriorly (Fig. 8.19).
|
|
|
FIG. 8.17. The normal cerebellum (A) has a characteristic “doughnut” shape compared with the elongated cerebellum (B) described as the “banana sign” associated with an open neural tube defect. |
|
|
|
FIG. 8.18. A cystic hygroma (A) is more fluid filled than a cephalocele (B), which contains brain tissue and generally contains a septum. Usually the bony defect in the skull can be also be detected in the latter case. |
|
|
|
FIG. 8.19. An anterior cervical teratoma is seen in longitudinal section (A) and transverse (B). Although the diagnosis was made prenatally, intubation at delivery was unsuccessful. Tracheal compression is a significant risk with cervical tumors in the fetus and generally is the cause of death. |
The upper part of the fetal chest is symmetric and consists mostly of lung tissue and the fetal thymus, which is difficult to image. The normal orientation of the fetal heart lies along a 45-degree left axis relative to the anterior-posterior thoracic diameter. The apex of the heart overlying the fetal stomach is an important relationship. Malrotations and situs inversus can be missed if careful correlation with the fetal lie is not included (Fig. 8.20). A lack of homogeneous lung tissue with or without displacement of the heart suggests cystic adenomatoid malformations, diaphragmatic hernias, teratomas, or other lesions. The fetal heart can still maintain a normal 45-degree axis but be displaced laterally by these and other anomalies (Fig. 8.21). Documentation of a normal four-chamber view eliminates the majority of fetal heart defects (Fig. 8.22). A short-axis view is not currently a requirement of a basic examination but increases the sensitivity for detecting cardiac defects.
|
|
|
FIG. 8.20. Situs inversus. Using standard orientation, in a transverse image (A), the maternal right (R) and left (L) appear on the left and right of the image, and in the longitudinal image (B), the maternal feet are to the right of the image. This indicates a vertex presentation with the fetal back to the left side of the mother, which means the apex of the fetal heart points to the right side of the fetus in (A). |
|
|
|
FIG. 8.21. The heart is displaced from a more central position by the cystic adenomatoid malformation in the right side of the chest, but the normal 45-degree axis of the heart is preserved. The line from the fetal spine to the sternum normally should pass through the atria. |
|
|
|
FIG. 8.22. A normal four-chamber view (A) compared with the same view in Ebstein anomaly (B) and in transposition of the great vessels (C). RV, right ventricle; LV, left ventricle; RA, right atrium; LA, left atrium; AO, aorta; PA, pulmonary artery. (From Dr. Alfred Abuhamad; with permission.) |
With the transducer held in the same orientation for the four-chamber heart view, move inferiorly in the fetus to locate and document the plane for the AC measurement. The fetal gall bladder, which may be seen during this transition, is one of the three anechoic areas normally seen in the fetal abdomen. The other two are the stomach and urinary bladder. The observation of additional areas requires explanation. The fetal liver occupies most of the abdominal cavity in the plane used for the circumference measurement, which is why that measurement is sensitive for fetal weight and disturbances in growth. Below the AC plane, the abdomen consists mostly of fetal bowel and the kidneys posteriorly. An image showing both kidneys is useful for eliminating unilateral agenesis, horseshoe kidney, and multicystic or polycystic kidneys (Fig. 8.23). The fetal umbilical cord insertion site should be documented. If a gastroschisis or omphalocele is present, further investigation is needed (Fig. 8.24).
|
|
|
FIG. 8.23. The cysts (c) of the multicystic kidney (A) involve the left kidney. A normal contralateral kidney with normal amniotic fluid volume portends a good prognosis. In (B) the polycystic horseshoe-shaped kidney is accompanied by oligohydramnios, a poor prognosis. |
|
|
|
FIG. 8.24. Although the umbilical cord insertion site is normal, a gastroschisis will appear as a mass to the right of the insertion site. B: The umbilical cord inserts into the sac of an omphalocele which, in this case, contains fetal liver (L). Isolated gastroschisis is not associated with an increased risk of chromosomal anomalies, contrary to an omphalocele which has significant associated risk. A smaller omphalocele has further increased risks. |
Moving caudally in the fetus, document the fetal urinary bladder. Following that image, rotate the transducer to image the femur. Although documentation of the FL suggests that a portion of the lower extremity has formed, an additional image of the fetal feet is helpful. Be aware of the orientation of the foot with respect to the tibia in order to diagnose clubfoot (Fig. 8.25). Images of the fetal hands, although difficult and not required in standards, are useful in finding soft markers of aneuploidy such as shortened phalanges, characteristic posturing of the fetal hands, or polydactyly.
|
|
|
FIG. 8.25. The clue to the diagnosis of clubfoot is that the sole of the foot and the toes are in the same plane as the longitudinal axis of the leg. |
THIRD TRIMESTER
There are a few anatomic structures that may be seen in the second trimester that can be visualized more easily in the third trimester. The fetal adrenal glands can be located on the superior poles of the kidneys. It is usually possible to distinguish the adrenal cortex and adrenal medulla. The lens of the eye and fetal scalp hair are more easily distinguished in the early third trimester.
Helpful adjuncts to estimation of gestational age also appear in the third trimester. Ossification of the distal femoral epiphysis occurs predictably around 32 weeks. The proximal tibial epiphysis ossifies around 35 weeks. These two ossification centers of the long bones are seen as prominent echoes distinct from the ends of the long bones. Because fetal growth rate varies widely in the third trimester, estimation of fetal weight alone may not accurately predict the gestational age. Finding the additional ossification centers of the long bones may provide more guidance for the patient who has not entered prenatal care until late in the pregnancy.
A worrisome source of third-trimester bleeding is placental abruption, which is mainly a diagnosis made on clinical grounds. In some cases ultrasonography provides information about gestational age and fetal life, allowing for more informed management decisions. In extreme cases, ultrasonography may reveal a portion of an abruption (Fig. 8.26) or a free-floating placenta and intrauterine fetal death.
|
|
|
FIG. 8.26. Placental abruption. The edge of the placenta (P) has been elevated by the bleeding. A portion of the amnion and chorion attached to the edge appears to be floating in the uterine cavity. |
Transvaginal scanning with appropriate caution in cases of undiagnosed vaginal bleeding in pregnancy can be very useful. The transducer should be inserted slowly while the sonographer watches the path of the transducer on the monitor. The ability to guide the tip of the transducer relative to maternal anatomy avoids the pitfalls of blind digital or speculum examination. Placental tissue overlying the internal os is seen clearly (Fig. 8.27), so the uncertainty of terms such as partial placenta previa or low-lying placenta previa can be avoided. The percentage of placenta overlying the internal cervical os can be reported to provide more information. The largest reportable percentage is 50%, indicating a central placenta previa (Fig. 8.28).
|
|
|
FIG. 8.27. Transvaginal ultrasonogram of a placenta previa. The placenta (P) covers the internal os. The tip of the transvaginal probe is in the anterior fornix. See color figure 8.27. |
|
|
|
FIG. 8.28. Transabdominal ultrasonogram of a central placenta previa. The intersection of arrows indicates the approximate location of the cervix, which cannot always be visualized using transabdominal sonography. The arrows are drawn along the bladder-uterine interface and the axis of the vagina. |
TECHNIQUES OF FETAL TESTING
The amount of amniotic fluid surrounding the fetus has been shown to be a very sensitive indicator of fetal status. Poor placental blood flow in cases of maternal hypertension or diabetes results in a diminished substrate for fetal kidney filtration and a subsequent decrease in the amount of fetal urine. A low AFI is one of the early indicators of such compromise, although a wide variation in the normal range is possible. Estimation of the fluid index requires measurement of the deepest vertical pocket of amniotic fluid not occupied by fetal parts or umbilical cord. This measurement is performed in each of four quadrants of the uterus. Measurements should be performed with the patient supine and the transducer held perpendicular to the floor. The sum of the four measurements expressed in centimeters equals the AFI. Two approaches have been suggested to define oligohydramnios and polyhydramnios using the AFI. One method is to use fixed values of less than or equal to 5 centimeters for oligohydramnios and greater than or equal to 18 centimeters for polyhydramnios. The second approach is to use gestational-specific percentiles below or equal to the fifth percentile for oligohydramnios and above or equal to the 95th percentile for polyhydramnios. Some authors have also proposed defining adequate amniotic fluid volume as the presence of a pocket of fluid measuring at least 2 centimeters horizontally and vertically. The method selected should depend on the experience and data from each sonographer's institution and further correlation with outcomes.
Manning and Platt described the biophysical profile (BPP) as a method for noninvasive monitoring of fetal status. There are five parts to the BPP. Four of these parameters are ultrasonographic variables that are evaluated during a 30-minute observation period: fetal breathing, fetal movement, fetal tone, and amniotic fluid volume. Fetal breathing can be observed by watching the fetal diaphragm or chest wall for characteristic breathing motion. The fetus must breathe continuously for 30 seconds during the 30-minute observation period to receive a normal score. Fetal movement of the limbs or body must occur at least 3 times to be considered adequate. Normal fetal tone is demonstrated by one active extension and flexion of the limbs or trunk. Opening and closing of the fetal hand also qualifies for a normal tone score. Slow extension of the extremity or trunk with incomplete return to flexion is not considered normal. The fourth part of the BPP is measurement of the amniotic fluid volume. Originally the normal fluid volume was described as the presence of at least one pocket of amniotic fluid measuring 1 centimeter in vertical dimension. Manning and colleagues later modified this definition to 2 centimeters measured vertically. Many centers use a normal AFI as a substitute measurement. Each ultrasonographic variable is scored zero (abnormal) or two points (normal). The fifth component of the BPP is a nonstress test, which receives a score of two points when reactive and zero when nonreactive. The best possible BPP score is ten. A detailed discussion of the use of the BPP in antepartum care can be found in Chapter 9.
Doppler velocimetry of both maternal and fetal vessels is based on the principle that sound waves returning from a moving reflector will be affected by the direction and speed of that reflector relative to the transmitting or receiving source. A reflector traveling toward the receiver will cause the return signal to be higher in frequency. The opposite is true for a reflector moving away from the receiver. Return echoes from the receding reflector will be lower in frequency than the transmitted pulse. The degree of change in the returning signal can be used to calculate the velocity (speed and direction) of the reflector. By applying this property to the red blood cell mass moving within maternal or fetal vasculature, characteristic profiles were obtained for mother and fetus. Doppler interrogation of the maternal uterine artery may reveal a characteristic notch during diastole, which is a sensitive predictor for preeclampsia during the pregnancy. The umbilical artery Doppler waveforms can be used to evaluate the resistance of the placental circuit. The systolic-to-diastolic (S/D) ratio is defined as the ratio of peak velocity in systole to the velocity nadir in diastole. This value is typically between 1.5 and 2.5 in the third trimester. As placental flow resistance increases with vascular compromise, the S/D ratio also increases. Increased resistance to the point of stopping or reversing diastolic blood flow is worrisome for fetal outcome and should prompt further evaluation (Fig. 8.29).
|
|
|
FIG. 8.29. Absent diastolic flow with or without reverse flow (R) is an indicator of poor fetal health. S, systole. (From Diana M. Strickland, RDMS, RDCS; with permission.) |
INTERVENTIONAL ULTRASONOGRAPHY
Ultrasonography is now a standard adjunct for amniocentesis, chorionic villus sampling, percutaneous umbilical blood sampling (PUBS), and other invasive procedures. Amniocentesis for genetic studies generally is performed after 13 weeks gestation. The tip of the amniocentesis needle is visualized during insertion to reduce the number of attempts. Post-procedure determination of fetal heart rate usually is performed to assure that the procedure was well tolerated. Chorionic villus sampling can be performed blindly, but many providers find that the procedure is easier and less risky when transabdominal imaging provides visualization of the uterus and guidance of the catheter. PUBS depends heavily on ultrasonographic imaging to locate the placental umbilical cord insertion for needle placement, for monitoring the fetus during sampling, and for post-procedure monitoring to watch for hemorrhage.
Ultrasonographic guidance may be employed during interventional procedures for fetal benefit. Intrauterine fetal blood transfusion can be performed in severe cases of isoimmunization when the fetus is too premature to deliver. Replacement of fetal thyroid hormone in cases of maternal thyroid dysfunction can also be performed.
The fetus can then be treated and followed with ultrasonography for resolution of the goiter, indicated by return of the thyroid gland to normal size. Selected obstructions of the fetal urinary tract can be bypassed with percutaneous catheters that are removed after birth. This procedure may also be performed in cases in which fluid-filled areas are found to be compressing thoracic structures (Fig. 8.30). In cases of twin-to-twin transfusion syndrome, therapeutic drainage of the polyhydramnic twin may permit the pregnancy to progress to a reasonable chance of viability.
|
|
|
FIG. 8.30. Insertion of shunt in unilateral hydrothorax. The anechoic, fluid-filled area is drained by the needle during insertion of the shunt. The baby was delivered at term with no pulmonary complications. |
FUTURE DIRECTIONS
New developments in the field of diagnostic ultrasonographic imaging include power Doppler imaging, harmonic imaging, three-dimensional (3D) ultrasonography, real-time 3D ultrasonography (often called four-dimensional [4D] imaging), compound imaging, B-flow imaging, and panoramic ultrasonographic imaging.
Power Doppler imaging uses the same principle as Doppler velocimetry. However, instead of targeting a single vessel, power Doppler imaging is used over a region of tissue. When the Doppler shift is detected in the return echoes, that region of tissue is assigned flow data that appear on the screen as colors different than those of the surrounding image. Direction of flow is not indicated. The resulting image contains a standard ultrasonographic image of the target tissue, with a color overlay representing vascular flow. This type of imaging may become useful in placental flow studies, analysis of the umbilical cord, or detection of ectopic pregnancy. Use of power Doppler should be monitored carefully, because the acoustic output increases dramatically with its use.
Harmonic imaging utilizes the harmonics of the transmitted pulse to receive double the transmitted frequency. This improves the image by removing clutter and artifact and improving resolution. This feature is very useful for the patient whose body habitus makes imaging difficult.
Three-dimensional ultrasonography relies on a special transducer that can sample tissue in multiple sections simultaneously and on computer processors that can reconstruct the data as a virtual block of tissue. This block can then be viewed at any angle and in any section. Proponents of 3D ultrasonography advocate its use in first-trimester anatomic surveys, monitoring of cervical cerclage, and evaluation of fetal surface defects such as cleft lip or myelocele. This technology requires good fetal position and a moderate amount of amniotic fluid in front of the targeted tissue in order to create adequate images. Special transducers, for both transvaginal and transabdominal imaging, are required to insonate the tissue of interest. The extra graphics processors and memory required to generate 3D images are the rate-limiting steps to producing real-time 3D ultrasonography. Also known as 4D ultrasonography, real-time 3D ultrasonography is currently in development. This technology requires the same transducers as 3D ultrasonography but uses faster processors to generate 3D images in actual real time. The same limitations apply to fetal position and amniotic fluid. It might be possible eventually to assess the functional status of fetal organs with 4D ultrasonography. The results from current research will provide the evidence for using real-time ultrasonography in different applications.
Compound imaging utilizes electronic beam focusing to emit ultrasound energy at angles to the axis of the transducer. A single target will be insonated from numerous different angles by the array of emitters across the transducer face. Shallow reflectors that would otherwise block tissue penetration are bypassed by the angled signals from and to the transducer. Reflectors from deeper in the tissue are imaged more precisely and a more detailed grayscale image is produced.
The increased resolution of modern transducers and data processing capabilities of systems have led to the development of B-flow imaging. Rather than using the Doppler effect to calculate velocities of blood flow, the B-mode function actually collects the tiny echoes emitted from blood cells. The resulting image is a real-time anatomic image combined with grayscale flow imaging. Color is not required for the display. An advantage of B-flow is the decreased exposure of the patient to ultrasound energy compared with Doppler interrogation.
Panoramic imaging relies on the ultrasound system to link a series of images into a large single image, much as a vacationer would align snapshots into a panoramic landscape photo. Although this mode is not real time, it has the advantage of displaying images much larger than the transducer's field of view.
CONCLUSION
In the changing spectrum of obstetric practice, ultrasonography has established a niche that is unlikely to be challenged significantly. It is a safe imaging modality when used properly. Numerous applications exist, from anatomic surveys to guidance during interventional procedures. The skills of the provider and the quality of the equipment have a direct impact on the sensitivity of the examination in detecting anomalies. Although the usefulness of screening every pregnant woman with an ultrasonographic examination is still in question, there is no doubt that under the guidelines of accepted medical indications, ultrasonography improves prenatal care.
SUMMARY POINTS
· Every ultrasonographic examination should be as complete as possible within the scope of the provider and the equipment.
· There is no evidence to suggest that medical ultrasonography carries a risk to the mother or fetus; nevertheless, such risks might be identified in the future. An ultrasonographic examination should be performed only when medically indicated.
· The sensitivity of ultrasonography in detecting fetal anomalies is variable and relies on the experience of the provider and the quality of equipment. Specialists with additional training in ultrasonography, such as a maternal-fetal medicine fellowship, should perform ultrasonographic examinations for abnormal findings or for genetic indications.
RECOMMENDED READINGS
Introduction
American College of Obstetricians and Gynecologists. First Trimester Screening for Fetal Anomalies with Nuchal Translucency. Committee Opinion, 1999.
American College of Obstetricians and Gynecologists. Ultrasound in Pregnancy. Technical Bulletin 187, 1993.
General Principles
American College of Obstetricians and Gynecologists. New ultrasound output display standard. Committee Opinion No. 180, Nov 1996.
Copel JA, Pilu G, Green J, et al. Fetal echocardiographic screening for congenital heart disease: the importance of the four-chamber view. Am J Obstet Gynecol 1987;157:648–655.
Ewigman BG, Crane JP, Frigoletto FD, et al. Effect of prenatal ultrasound screening on perinatal outcome, RADIUS study group. N Engl J Med1993;329:821–827.
Fleischer A, et al., eds. Sonography in obstetrics and gynecology: principles and practice, sixth ed. New York: McGraw-Hill, 2001.
Kremkau, Frederick W. Diagnostic ultrasound: principles and instruments, sixth ed. Philadelphia: WB Saunders, 2002.
Manning FA, Platt LD, Sipos L. Antepartum fetal evaluation. Development of a fetal biophysical profile score. Am J Obstet Gynecol 1980;136:787.
Nelson, Lewis H. Ultrasonography of the placenta-a review. Laurel, MD: American Institute of Ultrasonography in Medicine, 1994.
Documentation and the Basic Ultrasonographic Examination
AIUM Guidelines for performance of the antepartum obstetrical examination, 1994. From AIUM.org. Accessed December 6, 2002.
Techniques of Fetal Testing
Moore TR, Cayle JE. The amniotic fluid index in normal human pregnancy. Am J Obstet Gynecol 1990;162:1168–1173.
Phelan JP, et al. Amniotic fluid volume assessment with the four-quadrant technique at 36-42 weeks gestation. J Reprod Med 1987;32:540–542.