Ido Laskov1 and Walter H. Gotlieb2
(1)
Division of Gynecologic Oncology, Jewish General Hospital & Lady Davis Research Institute, McGill University, Montreal, QC, Canada
(2)
Division of Gynecologic Oncology, Jewish General Hospital, McGill University, 3755 Cote Ste Catherine Road, Room E716, Montreal, QC, Canada, H3T1E2
Walter H. Gotlieb
Email: walter.gotlieb@mcgill.ca
1 Introduction
Endometrial cancer is the most common gynecologic malignancy in affluent countries [1]. Approximately 15 % of women will be diagnosed with endometrial cancer before menopause, and 4 % will develop the disease before the age of 40 years [2, 3]. The current therapeutic approach for early-stage endometrial cancer includes total abdominal hysterectomy with bilateral salpingo-oophorectomy, and lymphadenectomy (pelvic and aortic), depending on preoperative or intraoperative pathologic risk profiles. Women with grade 1 endometrial cancer without myometrial invasion (consistent with FIGO 1988 stage Ia) treated by conventional surgery have a disease-specific survival of 99.2 % after 5 years, and 98 % after 10 years [4]. Many endometrial cancer patients carry an increased burden of medical co-morbidities, such as obesity, diabetes mellitus and hypertension, conditions that have been associated with a higher risk of surgical adverse events [5, 6]. Some patients carry severe medical co-morbidities that may preclude them having surgery [7, 8]. This high risk group of patients with endometrial cancer may sometimes have received progestin treatment as an alternative to surgery, or as treatment until they are deemed as fit for surgery.
A second group of patients that might benefit from progestin treatment are young women diagnosed with endometrial cancer who still wish to have children. The excellent cure rates that are attained for well differentiated endometrial cancer have allowed us to shift the focus, from the high survival towards quality of life issues after treatment. In particular, there has been increased attention focused on fertility preservation, as approximately one of ten patients with endometrial cancer develop the disease during reproductive age. Considering that the average age at first birth has steadily increased in developed nations. First births are now 1 in 12 births in women above the age of 35 (compared to only 1 in 100 in 1970) [9]. Hence, it is not surprising that many of these younger women with endometrial cancer desire fertility preserving options. The decision to proceed with conservative management is complex. Many issues related to fertility-preservation for endometrial cancer remain uncertain, and warrant further consideration. The optimal work-up to evaluate the extent of disease in young patients with endometrial cancer who desire to maintain their uterus remains unclear, as is the lack of uniformity in the medical management and surveillance.
In this chapter we will discuss the role of progestin hormonal therapy in the conservative management of endometrial cancer, including the potential risks associated with medical management compared to surgical care, the appropriate candidate selection and work up, the expected outcomes, the variety of progestational agents that have been used, and the recommended follow-up (Fig 11.1). We will also describe the role of progestins in advanced endometrial cancer and the foreseeable future of progesterone treatments in endometrial cancer.

Fig. 11.1
Progesterone in endometrial cancer, chapter summary. MPA medroxyprogesterone acetate, MA megesterol acetate, LNG-IUD levonorgestrel releasing intrauterine device
2 Progesterone for Fertility Preservation
2.1 Are There Any Risks?
The development of endometrial cancer in young women usually results from a hyperestrogenic state that leads to endometrial hyperplasia. A tissue biopsy of atypical endometrial hyperplasia has been associated with a 29 % risk of progression to endometrial cancer [10], and endometrial cancers have been found in up to 43 % of patients with a preoperative diagnosis of atypical endometrial hyperplasia [11]. This high association warrants consideration in management decisions. According to a review of over 2,000 women aged 40 years or younger collected from the National Cancer Institute database, the majority of patients (75 %) had disease confined to the uterus, but approximately 17 % had stage III or IV disease [10]. These younger patients are also at increased risk of other pathological gynecologic conditions, including ovarian tumors. In a review of young women with endometrial cancer by Walsh et al. [11], 26 of 102 women (25 %) were found to have coexisting epithelial ovarian tumors (23 synchronous primaries and 3 metastases). Therefore, any decision to deviate from the standard approach of hysterectomy with oophorectomy and staging should take account of the risk of an undetected, and therefore subsequently untreated, synchronous or metastatic cancer. These studies confirm the need for thorough examination and careful patient selection, while highlighting the risks inherent in conservative management of an unstaged cancer.
Based on these data, the patient’s outcome may be adversely affected when choosing to pursue fertility preservation. In the absence of randomized trials, the largest study to evaluate this matter is a retrospective study by Koskas et al. [12] who examined 489 patients aged 40 or younger with grade 1 endometrial adenocarcinoma. The patients were divided into groups who underwent uterine preservation, ovarian preservation, or hysterectomy with oophorectomy. Ovarian and uterine preservation had no effect on either cancer-specific or overall survival. The limitations of Koskas et al’s. [12] study include the absence of information on which agents and treatment protocols were used and how they found no evidence for the 17–25 % of young patients with concomitant/metastatic adnexal carcinomas published in other reports [12, 13].
2.2 Workup Prior to Treatment
The optimal work-up to evaluate the extent of disease in young patients with endometrial cancer who desire to maintain their uterus has not been established. Every effort should be taken to ensure that the cancer is confined to the endometrium and low grade, and therefore likely to respond to hormonal therapy without compromising curability (Table 11.1). As a rule, the pretreatment evaluation should consist of a full workup for any signs or symptoms suspicious for advanced/metastatic disease (Tables 11.2 and 11.3).
Table 11.1
Suggested criteria for progesterone treatment [39]
|
I |
Absence of frank myometrial invasion |
|
II |
Well-differentiated (G1) endometrioid adenocarcinoma |
|
III |
No contraindications for progesterone therapy |
|
IV |
Potential for fertility |
|
V |
Informed consent on the indications and limitations of progesterone therapy |
Table 11.2
Suggested procedures for the assessment of a patient with endometrial cancer seeking fertility sparing treatments
|
Procedure |
Purpose |
|
Complete history and physical exam |
Look for signs or symptoms suspicious for advanced/metastatic disease |
|
D&C |
− Tumor grading − Possible therapeutic effect |
|
MRI |
Assess myometrial invasion and loco-regional disease spread |
|
Diagnostic laparoscopy |
Partial surgical staging |
|
Sentinel lymph node biopsy |
Value to be determined |
|
Genetic counseling |
Risk assessment for patient and family |
Table 11.3
Fertility sparing options; advantages and disadvantages
|
Drug |
Dose |
Advantages |
Disadvantages |
|
Medroxyprogesterone acetate |
400–600 mg/day for at least 3 months |
Well studied |
Known side effects |
|
Megesterol acetate |
160–320 mg/day for at least 3 months |
Well studied |
− Known side effects − Might have higher recurrence rate compared to MPA |
|
Progesterone - intrauterine device |
20–65 mcg/day |
Low systemic toxicity |
− Limited data − Intra-uterine placement required |
|
Natural progesterone |
200 mg/days, days 14–25 |
– |
Limited data |
|
Hydroxyprogesterone |
500 mg/days |
– |
Limited data |
|
Norethisterone |
5 mg/days |
– |
Limited data |
|
Progestogens at various doses |
– |
– |
Limited data |
2.2.1 Tissue Biopsy
Prior to initiating conservative management, dilatation and curettage (D&C) is recommended because it better defines the grade of the tumor compared to office endometrial biopsy [13]. Additionally, there might be value in the removal of most of the endometrial cancer cells by the D&C before starting hormonal treatment [14].
2.2.2 Imaging
Attempts should be made to rule out myometrial invasion, adnexal involvement and lymph node metastases, which are regarded as contra-indications for conservative management. MRI has proven to be superior to transvaginal ultrasound or CT for determining myometrial invasion [15]. Pooling of 11 studies, comparing T2-weighted imaging and contrast-enhanced magnetic resonance imaging, revealed similar positive predictive values for myometrial invasion of 0.65 and negative predictive values of 0.85 [16]. MRI is used to assess loco-regional disease spread [17], and Sironi et al. [15] reported a sensitivity and specificity of 74 % for MR assessment of superficial myometrial invasion, although the importance of superficial myometrial involvement on response to progestins is not clear.
2.2.3 Additional Invasive Procedures
There is an increased risk of concomitant adnexal involvement in premenopausal patients with endometrial cancer, reaching up to 25 % in the series from Cedars Sinai [11]. Consequently, some physicians perform a diagnostic laparoscopy at the time of D&C [18]. With the evolving data on sentinel lymph node biopsy for endometrial cancer, lymph node biopsy could be considered in selected cases [19].
2.2.4 Genetic Counseling
Women diagnosed with endometrial cancer at a young age are at increased risk for mismatch repair gene mutations associated with Lynch syndrome [20]. Hence, these women should also be referred for genetic counseling [21], as counseling might reveal important implications concerning the risk of adnexal pathology and colon cancer necessitating screening in these young patients and their families.
2.3 Prognostic Factors
Although the majority of carefully selected patients will respond to progestin therapy, there is at present no way to accurately predict who will respond.
Data remain scarce on clinical or pathologic predictors of response to progestin treatment in premenopausal women with complex and Grade 1 endometrial adenocarcinoma. Park et al. analyzed 148 patients (age ≤40 years) with stage IA, grade 1, endometrioid adenocarcinoma of the uterus who underwent fertility-sparing management using daily oral medroxyprogesterone acetate or megestrol acetate [24]. One hundred and fifteen (77.7 %) showed complete response to progestin treatment, and 35 (30.4 %) experienced recurrence after a median follow-up period of 66 months. A body mass index (BMI) ≥25 was the only significant factor associated with a failure to achieve cure (odds ratio [OR], 3.00; 95 % CI, 1.35–6.66; P = 0.007). A BMI ≥25 was also significantly associated with a higher risk of recurrence (OR, 2.14; 95 % CI, 1.06–4.31; P = 0.033). The use of MPA (compared to MA) (OR, 0.44; 95 % CI, 0.22–0.88; P = 0.021), continuing maintenance treatment (OR, 0.22; 95 % CI, 0.05–0.94; P = 0.042), and a previous pregnancy (OR, 0.25; 95 % CI, 0.11–0.56; P = 0.001) were significantly associated with a lower risk of recurrence [22]. Penner et al. [23] looked at the histopathologic features, using a qualitative abnormal endometrial architecture score, comparing pretreatment and follow-up endometrial specimens to identify predictors of resolution [25]. The score is composed of five features: polypoid, cribriform, papillary, budding and back to back endometrial glands. Resolution rates expressed as the Standardized Resolution Ratio (SRR) were highest in individuals with a low pre-treatment score and a BMI <35 (SRR = 1.48, p = 0.03), lower among subjects with a high pre-treatment score (SRR = 0.37, p < 0.03), and lowest in subjects whose first follow-up specimen showed persistent complexity, atypia, or carcinoma with adjacent stromal decidualization (SRR = 0.24, p = 0.002) [23]. The presence of progesterone receptors also predicts response to progestin therapy [24, 25]. In one study the response rate was 8 % (seven of 86 patients) for patients who were progesterone receptor-negative and 37 % (17 of 46) for patients who were progesterone receptor-positive (P < .001) [26]. In addition, PTEN and KRAS status in combination with the progesterone receptor expression in the tumor appear promising as biomarkers of response [25]. Further investigations in predictors of response may ultimately lead to personalized treatments for young women with endometrial cancer.
2.4 Types of Progesterone
At present, there is no consensus on the optimal medication, dose, or length of treatment. In a 2004 review, the most commonly used agents were medroxyprogesterone acetate 500–600 mg (MPA; 44 %) and megesterol acetate 160 mg (35 %) for at least 3 months [27]. Both regimens appear to have similar response rates although it has recently been suggested that the recurrence rate is higher after megestrol acetate compared to medroxyprogesterone acetate [22].
Additionally, treatment has been reported with the levonorgestrel intrauterine device (LNG-IUD) (MirenaTDM) that releases 20 mcg of levonorgestrel per day [28], in combination with hysteroscopic resection [29], medroxyprogesterone acetate [30] or GnRH analogues [31]. Other treatments used include intramuscular 17-hydroxyprogesterone, oral contraceptive pills, norethisterone, dihydrogesterone, and natural progesterone either utilized alone or in a combination of progestin agents [7, 32].
The choice of progestin should be based on measurable outcomes, including efficacy, side-effects, and patient tolerability. Orally administered progestins are not without side-effects, including mood alterations, headaches, weight gain, breast pain and/or tenderness, and increased risk of thrombus formation. Thrombosis is a serious adverse reaction to MPA. It is caused by the inhibitory activity of MPA against plasminogen activator [33]. Thrombosis can be fatal especially if leading to cerebral infarction, myocardial infarction, or pulmonary embolism. Clotting factors should be checked monthly, and treatment with MPA should be discontinued on detection of clotting abnormalities. A prospective trial using 600 mg MPA [34] reported that the most common side effects were weight gain and liver dysfunction. There were no cases of thromboembolism. Progesterone therapy is contraindicated in the presence of a history of thromboembolus, breast cancer, or hepatic dysfunction. The progesterone-releasing IUD might be a means of achieving a localized effect within the endometrium while avoiding the adverse systemic toxicity. There is no consensus regarding the optimal progestin duration. Progestin therapy has an impact on the endometrial cells as early as 10 weeks after initiation of treatment, but most physicians suggest the need for a minimum of 3 months of treatment before assessing the response with endometrial hyperplasia and even longer for endometrial cancer [34]. Obese and anovulatory women have been shown to require longer periods of progestin therapy to attain a complete response, and are more prone to relapse [22, 23].
2.5 Outcome
Although the first publication describing fertility preserving, conservative treatment with hormones was published in 1961 [35], the number of publications describing the outcome is still limited (Fig. 11.2) and many questions remain. The possibility of publication bias in the studies analyzed should be borne in mind. Studies showing treatment success are more likely to be reported and published than negative trials, leading to overestimating the success rate. In a recent metaanalysis [36], including 34 observational studies, the authors evaluated the regression, relapse, and live birth rates of 408 women diagnosed with early-stage endometrial cancer. The primary studies included the outcome of women with well-differentiated endometrial cancer with 386 women being classified as G1 and 22 women with moderate or poor differentiation (G2 or G3). Half of the studies were prospective cohorts (17 of 34) and only in 6 of the 34 studies, was the follow-up more than 5 years. Overall, resolution occurred in 76 % (301/408) of reported patients (Table 11.4), and 89 (40.6 %) responders relapsed during follow-up. 75 women achieved at least 1 live birth, yielding a live birth rate of 28 %.
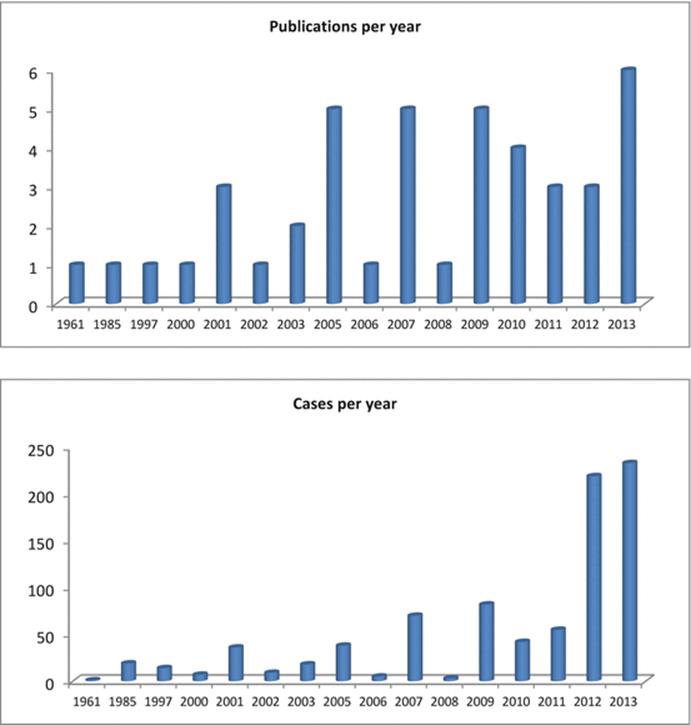
Fig. 11.2
Number of publications and number of reported cases treated conservatively
Table 11.4
Overview of studies and outcomes of progestogen treatment, adapted from Gallos et al. [36]
|
Study (year, reference) |
Total of patients |
Regressed (%) |
Relapsed (%) |
Live births (%) |
|
Bokhman (1983, [61]) |
19 |
15 (79) |
– |
– |
|
Randall (1999, [62]) |
14 |
10 (71) |
1/10 (10) |
3/14 (21) |
|
Kim (2000, [63]) |
7 |
4 (57) |
2/4 (50) |
0/7 (0) |
|
Imai (2001, [64]) |
14 |
8 (57) |
3/8 (38) |
2/14 (14) |
|
Kaku (2001, [65]) |
12 |
9 (75) |
2/9 (22) |
1/12 (8) |
|
Duska (2001, [2]) |
12 |
9 (75) |
– |
– |
|
Wang (2002, [66]) |
9 |
8 (89) |
4/8 (50) |
2/9 (22) |
|
Gotlieb (2003, [67]) |
13 |
13 (100) |
6/13 (46) |
3/13 (23) |
|
Jadoul (2003, [68]) |
5 |
3 (60) |
0/3 (0) |
3/5 (60) |
|
Niwa (2005, [69]) |
12 |
12 (100) |
8/12 (67) |
– |
|
Ota (2005, [70]) |
12 |
5 (42) |
2/5 (40) |
2/12 (17) |
|
Yahata (2005, [71]) |
8 |
7 (88) |
7/7 (100) |
2/8 (25) |
|
Yang (2005, [72]) |
6 |
4 (67) |
2/4 (50) |
2/6 (33) |
|
Le Digabel (2006, [73]) |
5 |
3 (60) |
1/3 (33) |
0/5 (0) |
|
Elizur (2007, [74]) |
8 |
8 (100) |
3/8 (38) |
4/8 (50) |
|
Minaguchi (2007, [75]) |
18 |
14 (78) |
5/14 (36) |
1/18 (6) |
|
Ushijima (2007, [34]) |
22 |
14 (64) |
8/14 (57) |
3/22 (14) |
|
Wheeler (2007, [76]) |
21 |
7 (33) |
1/7 (14) |
– |
|
Yamazawa (2007, [77]) |
9 |
7 (78) |
2/7 (29) |
3/9 (33) |
|
Li (2008, [78]) |
3 |
3 (100) |
0/3 (0) |
– |
|
Eftekhar (2009, [79]) |
21 |
18 (86) |
3/18 (17) |
2/21 (10) |
|
Hahn (2009, [80]) |
35 |
22 (63) |
9/22 (41) |
8/35 (23) |
|
Han (2009, [81]) |
7 |
7 (100) |
0/7 (0) |
5/7 (71) |
|
Signorelli (2009, [82]) |
11 |
6 (55) |
4/6 (67) |
4/11 (36) |
|
Yu (2009, [83]) |
8 |
6 (75) |
1/7 (17) |
0/8 (0) |
|
Mao (2010, [84]) |
6 |
4 (67) |
0/4 (0) |
3/6 (50) |
|
Mazzon (2010, [85]) |
6 |
6 (100) |
0/6 (0) |
4/6 (67) |
|
Minig (2010, [31]) |
14 |
8 (57) |
2/8 (25) |
1/14 (7) |
|
Cade (2010, [7]) |
16 |
10 (63) |
– |
– |
|
Laurelli (2011, [29]) |
14 |
14 (100) |
1/14 (7) |
1/14 (7) |
|
Park (2011, [86]) |
14 |
13 (93) |
3/13 (23) |
13/14 (29) |
|
Perri (2011, [87]) |
27 |
24 (89) |
9/24 (38) |
12/27 (44) |
|
Total |
408 |
301 (76 %) |
89/267 (40.6 %) |
75/325 (28 %) |
3.6 % of patients were diagnosed with ovarian malignancy during follow-up. It is unclear whether these represent concurrent ovarian malignancies or metastatic ovarian involvement from the primary endometrial neoplasm. There were also ten women (1.8 %) diagnosed with stage II disease or greater following treatment failure, and there were two deaths reported (0.5 %). Another recent systemic review by Gunderson et al. [32] reported oncologic and reproductive outcomes with progestin therapy in women with endometrial hyperplasia and grade 1 endometrial cancer. Forty-five studies with 391 study subjects were identified including 280 women that had grade 1 endometrial adenocarcinoma. The median age for the overall cohort was 31.7 years (range 19–80 years). When stratified by disease type, the durable complete response rate was significantly higher in women with complex atypical hyperplasia (65.8 %) compared to those with carcinoma (48.2 %; p = .002). The rate of initial response in women with complex atypical hyperplasia was also significantly higher (85.6 %), than women with carcinoma (74.6 %; p = 0.03). Disease recurrence was more likely to occur in the carcinoma cohort (35.4 %) than the hyperplasia group (23.2 %; p = .03). Further, persistent disease was noted in only 14.4 % of women with complex atypical hyperplasia compared with 25.4 % of those with carcinoma (p = .02). Reproductive outcomes did not differ between the cohorts.
2.5.1 Repeat Treatment for Recurrence After Complete Response?
Park and colleagues recently published a retrospective multicenter study that shows the safe and effective outcome of re-treating 33 young patients who still wanted to preserve fertility following recurrence after a complete response to progestins [37]. Five of the 33 women failed to respond to a second conservative approach, and another five patients recurred after a second complete response. Three received a third cycle of progestins and two responded again. Five patients delivered six healthy babies following this second conservative approach. The responders were followed for a mean of period of 51 months, no patient died of disease or suffered an adverse outcome.
2.5.2 Outcome for Progestin Releasing Intrauterine Devices
Levonorgestrel releasing intrauterine devices (LNG-IUD) are associated with contraceptive efficacy, powerful reduction of menstrual blood volume through suppression of endometrial growth, and accompanying relief of menstrual pain [38]. It has also been shown that the use of LNG-IUD in combination with hormone replacement therapy during or after menopause can prevent endometrial cancer [39]. The efficacy of the LNG-IUD in suppressing the growth of endometrium has also been shown in patients with “non-atypical” endometrial hyperplasia, with a response seen in 96 % of all cases within 1 year and 92 % within 2 years after insertion [40]. Efficacy in patients with endometrial cancer is presently being investigated. Preliminary data obtained from two separate studies suggests that progestin treatment provided by an IUD in 22 patients with grade 1 Stage I endometrial cancer [29, 41] was followed by a 68 % (15/22) complete response after six months or longer compared to 72 % (73/102) of patients on oral progestin [8]. No relapses or progressions were reported after 6–71 months of follow-up. Fertility outcomes were not reported. In addition, a few more studies, all with a small number of patients [30, 31] suggests that treatment with oral or intrauterine progestin is similarly effective. Large prospective trials for LNG-IUD are presently underway in order to clarify some of the unresolved issues (Table 11.5).
Table 11.5
Progestin and endometrial cancer, ongoing clinical trials and time of expected results
|
ClinicalTrials.gov Identifier # |
Title |
Estimated study completion date |
|
NCT00483327 |
Management of atypical endometrial hyperplasia and endometrial carcinoma using megestrol acetate |
October 2013 |
|
NCT01594879 |
Treatment with medroxyprogesterone acetate plus LNG-IUS in young women with early stage endometrial cancer |
December 2014 |
|
NCT00788671 |
Levonorgestrel intrauterine device (IUD) to treat complex atypical hyperplasia (CAH) and Grade 1 endometrioid endometrial cancer |
November 2015 |
|
NCT01943058 |
Megestrol acetate or levonorgestrel-releasing intrauterine system in treating patients with atypical endometrial hyperplasia or endometrial cancer |
October 2016 |
|
NCT02035787 |
Metformin with the levonorgestrel-releasing intrauterine device for the treatment of complex atypical hyperplasia (CAH) and endometrial cancer in non-surgical patients |
March 2017 |
|
NCT00003179 |
Surgery plus medroxyprogesterone in preventing endometrial cancer |
N/A |
2.6 Follow Up
In view of the high relapse rates (35–41 % [32, 36]), the frequency of concomitant adnexal malignancy, and the risk of upgrading of the cancer, close follow is essential.
Thinning of the endometrium as seen on transvaginal ultrasound is associated with an increased chance of responding to progestin therapy [34]. However, the predictive value is insufficient to negate endometrial sampling. It is important to note that the diagnostic accuracy of endometrial aspiration biopsy (pipelle) while the LNG-IUD is in place may not be as accurate as dilatation & curettage (D&C) [42].
It is sensible to recommend staging hysterectomy with bilateral salpingo-oophorectomy once the family is complete or if fertility-sparing treatment fails, either due to failure of regression or relapse. When regression occurs, some recommend assisted reproduction to maximize the chances of a live birth and decrease the time to definitive treatment. Additionally, immediate assisted reproduction avoids prolonged unopposed estrogen stimulation, which could cause relapse.
The need for oophorectomy together with hysterectomy remains debateable in view of the risk of concomitant ovarian involvement [11]. One series based on the database from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) suggested that there was no increase in cancer related mortality associated with ovarian preservation in young women with early stage endometrial cancer [43].
3 Progesterone in Advanced Endometrial Cancer
Progesterone has long been used for advanced or recurrent endometrial cancer. Kauppila [44] reviewed 1,068 patients treated with medroxyprogesterone acetate (MPA), megestrol acetate, or hydroxyprogesterone caproate in different trials, and found an overall response rate of 34 %, with a mean duration of response ranging from 16 to 28 months and a mean survival ranging from 18 to 33 months. However subsequent clinical studies, based on more stringent criteria for response assessment, reported lower response rates ranging from 11 to 16 %, without any significant difference according to the type of progestin used [45, 46]. When MPA 200 or 1,000 mg/day was administered to 229 patients with advanced or recurrent endometrial cancer, the low-dose group (200 mg/day group) showed better outcomes (17 % complete remission and 8 % partial remission) than the high-dose group (1,000 mg/day group) (9 % complete remission and 6 % partial remission) [26]. Median progression free survival and overall survival rates were 3.2 months and 11.1 months, respectively, for the low-dose group, and 2.5 and 7 months for the high dose group, with no differences in toxicity noted between the two arms. This GOG trial showed that the response rate was higher in the low-dose group than in the high-dose group with the responses being particularly favorable in G1 and PR-positive cases [26]. The combination of progesterone therapy and chemotherapy has been tested in small series and has not shown any clinical advantage compared with either treatment alone [24]. The activity of progestins in this condition is often limited by the frequent down-regulation of PR within the target tissues, resulting in a relatively short duration of response. Tamoxifen can increase PR content in endometrial cancer tissues, but clinical studies on alternating treatment with tamoxifen and progestin have given conflicting results [47–49]. Therapeutic strategies targeted at enhancing PR expression are currently being investigated worldwide and could potentially improve the clinical outcome of endometrial cancer patients (Table 11.6) [50].
Table 11.6
Hormonal therapy with progestins and tamoxifen in advanced or recurrent endometrial cancer
|
Study |
Hormonal agent |
Patients |
CR (%) |
PR (%) |
OR (%) |
|
Thigpen JT [26] |
MPA (200 mg/day) |
145 |
17 |
8 |
25 |
|
MPA (1,000 mg/day) |
154 |
9 |
6 |
15 |
|
|
Thigpen JT [88] |
TAM |
68 |
4 |
6 |
10 |
|
Pandya KJ [49] |
MA |
20 |
5 |
15 |
20 |
|
TAM/MA |
42 |
2 |
17 |
19 |
|
|
Whitney CW [47] |
TAM/MPA |
58 |
10 |
23 |
33 |
|
Fiorica JV [48] |
TAM/MA |
56 |
21 |
5 |
26 |
CR complete response, PR partial response, OR overall response, MPA medroxyprogesterone acetate, TAM tamoxifen, MA megestrole acetate
4 Novel Approaches
4.1 Fourth-Generation Progestins
The fourth-generation progestin dienogest is an effective means of treating endometriosis. At present, its anti-tumor activity is also attracting close attention following a report that dienogest suppresses the proliferation of endometrial cancer-derived cell lines in vitro which fail to respond to other progestins such as medroxyprogesterine acetate (MPA) [51]. The mechanism for antitumor activity of dienogest appears different to conventional progestin preparations. It has been shown to suppress neovascularization [52, 53], the cell cycle [54] and to inhibit PGE2 formation through selective antagonist activity on the PR [55].
4.2 Progesterone Receptor Expression and Reversal of Progesterone Resistance
Many patients with endometrial cancer are resistant to progestin therapy apparently associated with the absence of the progesterone receptor (PR). Studies aimed at the restoration of PR expression in endometrial cancer have been conducted at the gene and protein levels. Several preclinical studies have been carried out on the control of epigenetic mutations (hypomethylation or hypermethylation) often seen in cases of endometrial cancer for the purpose of stimulating apoptosis and restoration of susceptibility of the cancer to chemotherapy [56]. PR gene hypermethylation, responsible for the disappearance of the PR in certain endometrial cancers, can be reversed by DNA methyltransferase inhibitors, shown to stimulate re-expression of the PR at both the mRNA level and the protein level [57–59]. Epidermal growth factor receptor (EGFR) has also been implicated as a factor involved in progesterone resistance. The EGFR has been detected in histological specimens and cell lines of endometrial cancer and is known to be over expressed in endometrial cancer, although its role in resistance to progestin has not been clarified. One study analyzed differences in EGFR function and resistance to progestin in relation to the presence or absence of PR expression in endometrial cancer, reporting that EGFR was detected in 60 % of PR positive specimens and 90.5 % of PR negative specimens. Furthermore, when further EGFR expression was stimulated in Ishikawa cells (an endometrial cancer cell line), the susceptibility to progestin decreased, accompanied by a reduction in PR expression [60]. AG1478 (a specific inhibitor for EGFR tyrosine kinase) effectively suppressed the proliferation of EGFR over expression in endometrial cancer cells [60]. On the basis of these findings, it is assumed that excessive expression of EGFR in endometrial cancer cells can reduce the susceptibility to progestin therapy. Therefore, inhibitors specific to EGFR tyrosine kinase may be effective against endometrial cancer resistant to progestin therapy.
5 Conclusions
Hysterectomy remains the gold standard for patients with endometrial cancer, but may not be an acceptable option for young women who wish to preserve their fertility or for women with severe co-morbidities compromising surgical survival.
Cohort studies with fertility-sparing treatment followed by assisted reproduction show a high chance of disease regression and encouraging live birth rates for patients with early-stage endometrial cancer. The risk of disease relapse during follow-up is significant and women wanting to pursue this treatment need to undergo thorough counseling.
Progestins are probably not curative, because the underlying cause usually persists. Based on our present understanding of the disease, hysterectomy is advocated once family planning is complete. The disease remains confined to the endometrium at the time of hysterectomy in the overwhelming majority of patients, and the outcome and survival are for the vast majority not jeopardized by conservative treatment [36].
Although hormonal management of complex atypical hyperplasia and low-grade, apparent early-stage endometrial carcinoma has been utilized for 50 years, many questions remain unanswered. Large prospective trials are presently underway to clarify some of the unresolved issues, including the role for levonogestrel containing intrauterine devices (Table 11.5). Similar to other rare cancers, an international registry would further advance our understanding. Investigations on novel therapeutic options targeting the underlying causes and molecular pathways are eagerly awaited.
References
1.
Jemal A, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60(5):277–300.CrossRefPubMed
2.
Duska LR, et al. Endometrial cancer in women 40 years old or younger. Gynecol Oncol. 2001;83(2):388–93.CrossRefPubMed
3.
Gitsch G, et al. Endometrial cancer in premenopausal women 45 years and younger. Obstet Gynecol. 1995;85(4):504–8.CrossRefPubMed
4.
Lajer H, et al. Survival after stage IA endometrial cancer; can follow-up be altered? A prospective nationwide Danish survey. Acta Obstet Gynecol Scand. 2012;91(8):976–82.CrossRefPubMed
5.
Mourits MJ, et al. Safety of laparoscopy versus laparotomy in early-stage endometrial cancer: a randomised trial. Lancet Oncol. 2010;11(8):763–71.CrossRefPubMed
6.
Obermair A, et al. Total laparoscopic hysterectomy versus total abdominal hysterectomy for obese women with endometrial cancer. Int J Gynecol Cancer. 2005;15(2):319–24.CrossRefPubMed
7.
Cade TJ, et al. Progestogen treatment options for early endometrial cancer. BJOG. 2010;117(7):879–84.CrossRefPubMed
8.
Baker J, et al. Efficacy of oral or intrauterine device-delivered progestin in patients with complex endometrial hyperplasia with atypia or early endometrial adenocarcinoma: a meta-analysis and systematic review of the literature. Gynecol Oncol. 2012;125(1):263–70.CrossRefPubMed
9.
Matthews TJ, Hamilton BE. Delayed childbearing: more women are having their first child later in life. NCHS Data Brief. 2009;21:1–8.PubMed
10.
Lee NK, et al. Prognostic factors for uterine cancer in reproductive-aged women. Obstet Gynecol. 2007;109(3):655–62.CrossRefPubMed
11.
Walsh C, et al. Coexisting ovarian malignancy in young women with endometrial cancer. Obstet Gynecol. 2005;106(4):693–9.CrossRefPubMed
12.
Koskas M, et al. Safety of uterine and/or ovarian preservation in young women with grade 1 intramucous endometrial adenocarcinoma: a comparison of survival according to the extent of surgery. Fertil Steril. 2012;98(5):1229–35.CrossRefPubMed
13.
Leitao Jr MM, et al. Comparison of D&C and office endometrial biopsy accuracy in patients with FIGO grade 1 endometrial adenocarcinoma. Gynecol Oncol. 2009;113(1):105–8.CrossRefPubMed
14.
Daniel AG, Peters 3rd WA. Accuracy of office and operating room curettage in the grading of endometrial carcinoma. Obstet Gynecol. 1988;71(4):612–4.PubMed
15.
Sironi S, et al. Myometrial invasion by endometrial carcinoma: assessment by MR imaging. AJR Am J Roentgenol. 1992;158(3):565–9.CrossRefPubMed
16.
Wu LM, et al. Predictive value of T2-weighted imaging and contrast-enhanced MR imaging in assessing myometrial invasion in endometrial cancer: a pooled analysis of prospective studies. Eur Radiol. 2013;23(2):435–49.CrossRefPubMed
17.
Manfredi R, et al. Local-regional staging of endometrial carcinoma: role of MR imaging in surgical planning. Radiology. 2004;231(2):372–8.CrossRefPubMed
18.
Gotlieb WH. Fertility preserving treatments for endometrial cancer: the unanswered questions. Gynecol Oncol. 2013;129(1):1–2.CrossRefPubMed
19.
Kim CH, et al. Sentinel lymph node mapping with pathologic ultrastaging: a valuable tool for assessing nodal metastasis in low-grade endometrial cancer with superficial myoinvasion. Gynecol Oncol. 2013;131(3):714–9.CrossRefPubMed
20.
Lancaster JM, et al. Society of Gynecologic Oncologists Education Committee statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol. 2007;107(2):159–62.CrossRefPubMed
21.
Kauff ND. How should women with early-onset endometrial cancer be evaluated for lynch syndrome? J Clin Oncol. 2007;25(33):5143–6.CrossRefPubMed
22.
Park JY, et al. Long-term oncologic outcomes after fertility-sparing management using oral progestin for young women with endometrial cancer (KGOG 2002). Eur J Cancer. 2013;49(4):868–74.CrossRefPubMed
23.
Penner KR, et al. Predictors of resolution of complex atypical hyperplasia or grade 1 endometrial adenocarcinoma in premenopausal women treated with progestin therapy. Gynecol Oncol. 2012;124(3):542–8.CrossRefPubMed
24.
Markman M. Hormonal therapy of endometrial cancer. Eur J Cancer. 2005;41(5):673–5.CrossRefPubMed
25.
Janzen DM, et al. Progesterone receptor signaling in the microenvironment of endometrial cancer influences its response to hormonal therapy. Cancer Res. 2013;73(15):4697–710.PubMedCentralCrossRefPubMed
26.
Thigpen JT, et al. Oral medroxyprogesterone acetate in the treatment of advanced or recurrent endometrial carcinoma: a dose-response study by the Gynecologic Oncology Group. J Clin Oncol. 1999;17(6):1736–44.PubMed
27.
Ramirez PT, et al. Hormonal therapy for the management of grade 1 endometrial adenocarcinoma: a literature review. Gynecol Oncol. 2004;95(1):133–8.CrossRefPubMed
28.
Giannopoulos T, Butler-Manuel S, Tailor A. Levonorgestrel-releasing intrauterine system (LNG-IUS) as a therapy for endometrial carcinoma. Gynecol Oncol. 2004;95(3):762–4.CrossRefPubMed
29.
Laurelli G, et al. Conservative treatment of early endometrial cancer: preliminary results of a pilot study. Gynecol Oncol. 2011;120(1):43–6.CrossRefPubMed
30.
Kim MK, et al. Combined medroxyprogesterone acetate/levonorgestrel-intrauterine system treatment in young women with early-stage endometrial cancer. Am J Obstet Gynecol. 2013;209(4):358e1–4.CrossRef
31.
Minig L, et al. Progestin intrauterine device and GnRH analogue for uterus-sparing treatment of endometrial precancers and well-differentiated early endometrial carcinoma in young women. Ann Oncol. 2011;22(3):643–9.CrossRefPubMed
32.
Gunderson CC, et al. Oncologic and reproductive outcomes with progestin therapy in women with endometrial hyperplasia and grade 1 adenocarcinoma: a systematic review. Gynecol Oncol. 2012;125(2):477–82.CrossRefPubMed
33.
Ashino-Fuse H, et al. Medroxyprogesterone acetate, an anti-cancer and anti-angiogenic steroid, inhibits the plasminogen activator in bovine endothelial cells. Int J Cancer. 1989;44(5):859–64.CrossRefPubMed
34.
Ushijima K, et al. Multicenter phase II study of fertility-sparing treatment with medroxyprogesterone acetate for endometrial carcinoma and atypical hyperplasia in young women. J Clin Oncol. 2007;25(19):2798–803.CrossRefPubMed
35.
Kelley RM, Baker WH. Progestational agents in the treatment of carcinoma of the endometrium. N Engl J Med. 1961;264:216–22.CrossRefPubMed
36.
Gallos ID, et al. Regression, relapse, and live birth rates with fertility-sparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: a systematic review and metaanalysis. Am J Obstet Gynecol. 2012;207(4):266e1–12.CrossRef
37.
Park JY, et al. Progestin re-treatment in patients with recurrent endometrial adenocarcinoma after successful fertility-sparing management using progestin. Gynecol Oncol. 2013;129(1):7–11.CrossRefPubMed
38.
Kim ML, Seong SJ. Clinical applications of levonorgestrel-releasing intrauterine system to gynecologic diseases. Obstet Gynecol Sci. 2013;56(2):67–75.PubMedCentralCrossRefPubMed
39.
Banno K, et al. Progestin therapy for endometrial cancer: the potential of fourth-generation progestin (review). Int J Oncol. 2012;40(6):1755–62.PubMed
40.
Varma R, et al. The effectiveness of a levonorgestrel-releasing intrauterine system (LNG-IUS) in the treatment of endometrial hyperplasia–a long-term follow-up study. Eur J Obstet Gynecol Reprod Biol. 2008;139(2):169–75.CrossRefPubMed
41.
Montz FJ, et al. Intrauterine progesterone treatment of early endometrial cancer. Am J Obstet Gynecol. 2002;186(4):651–7.CrossRefPubMed
42.
Kim MK, et al. Comparison of dilatation & curettage and endometrial aspiration biopsy accuracy in patients treated with high-dose oral progestin plus levonorgestrel intrauterine system for early-stage endometrial cancer. Gynecol Oncol. 2013;130(3):470–3.CrossRefPubMed
43.
Wright JD, et al. Safety of ovarian preservation in premenopausal women with endometrial cancer. J Clin Oncol. 2009;27(8):1214–9.CrossRefPubMed
44.
Kauppila A. Progestin therapy of endometrial, breast and ovarian carcinoma. A review of clinical observations. Acta Obstet Gynecol Scand. 1984;63(5):441–50.CrossRefPubMed
45.
Piver MS, et al. Medroxyprogesterone acetate (Depo-Provera) vs. hydroxyprogesterone caproate (Delalutin) in women with metastatic endometrial adenocarcinoma. Cancer. 1980;45(2):268–72.CrossRefPubMed
46.
Podratz KC, et al. Effects of progestational agents in treatment of endometrial carcinoma. Obstet Gynecol. 1985;66(1):106–10.PubMed
47.
Whitney CW, et al. Phase II study of medroxyprogesterone acetate plus tamoxifen in advanced endometrial carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2004;92(1):4–9.CrossRefPubMed
48.
Fiorica JV, et al. Phase II trial of alternating courses of megestrol acetate and tamoxifen in advanced endometrial carcinoma: a Gynecologic Oncology Group study. Gynecol Oncol. 2004;92(1):10–4.CrossRefPubMed
49.
Pandya KJ, et al. Megestrol and tamoxifen in patients with advanced endometrial cancer: an Eastern Cooperative Oncology Group Study (E4882). Am J Clin Oncol. 2001;24(1):43–6.CrossRefPubMed
50.
Gadducci A, Cosio S, Genazzani AR. Old and new perspectives in the pharmacological treatment of advanced or recurrent endometrial cancer: hormonal therapy, chemotherapy and molecularly targeted therapies. Crit Rev Oncol Hematol. 2006;58(3):242–56.CrossRefPubMed
51.
Katsuki Y, et al. Dienogest, a novel synthetic steroid, overcomes hormone-dependent cancer in a different manner than progestins. Cancer. 1997;79(1):169–76.CrossRefPubMed
52.
Nakamura M, et al. Dienogest, a synthetic steroid, suppresses both embryonic and tumor-cell-induced angiogenesis. Eur J Pharmacol. 1999;386(1):33–40.CrossRefPubMed
53.
Katayama H, et al. Effect of dienogest administration on angiogenesis and hemodynamics in a rat endometrial autograft model. Hum Reprod. 2010;25(11):2851–8.CrossRefPubMed
54.
Shimizu Y, et al. Dienogest, a synthetic progestin, inhibits the proliferation of immortalized human endometrial epithelial cells with suppression of cyclin D1 gene expression. Mol Hum Reprod. 2009;15(10):693–701.CrossRefPubMed
55.
Shimizu Y, et al. Dienogest, a synthetic progestin, inhibits prostaglandin E2 production and aromatase expression by human endometrial epithelial cells in a spheroid culture system. Steroids. 2011;76(1–2):60–7.CrossRefPubMed
56.
Yang S, et al. Endometrial cancer: reviving progesterone therapy in the molecular age. Discov Med. 2011;12(64):205–12.PubMed
57.
Ren Y, et al. Down-regulation of the progesterone receptor by the methylation of progesterone receptor gene in endometrial cancer cells. Cancer Genet Cytogenet. 2007;175(2):107–16.CrossRefPubMed
58.
Xiong Y, et al. Histone deacetylase inhibitors decrease DNA methyltransferase-3B messenger RNA stability and down-regulate de novo DNA methyltransferase activity in human endometrial cells. Cancer Res. 2005;65(7):2684–9.CrossRefPubMed
59.
Balch C, et al. Role of epigenomics in ovarian and endometrial cancers. Epigenomics. 2010;2(3):419–47.CrossRefPubMed
60.
Ai Z, et al. Overexpressed epidermal growth factor receptor (EGFR)-induced progestin insensitivity in human endometrial carcinoma cells by the EGFR/mitogen-activated protein kinase signaling pathway. Cancer. 2010;116(15):3603–13.CrossRefPubMed
61.
Bokhman JV, et al. Can primary endometrial carcinoma stage I be cured without surgery and radiation therapy? Gynecol Oncol. 1985;20(2):139–55.CrossRefPubMed
62.
Randall TC, Kurman RJ. Progestin treatment of atypical hyperplasia and well-differentiated carcinoma of the endometrium in women under age 40. Obstet Gynecol. 1997;90(3):434–40.CrossRefPubMed
63.
Kim YB, et al. Progestin alone as primary treatment of endometrial carcinoma in premenopausal women. Report of seven cases and review of the literature. Cancer. 1997;79(2):320–7.CrossRefPubMed
64.
Imai M, et al. Medroxyprogesterone acetate therapy for patients with adenocarcinoma of the endometrium who wish to preserve the uterus-usefulness and limitations. Eur J Gynaecol Oncol. 2001;22(3):217–20.PubMed
65.
Kaku T, et al. Conservative therapy for adenocarcinoma and atypical endometrial hyperplasia of the endometrium in young women: central pathologic review and treatment outcome. Cancer Lett. 2001;167(1):39–48.CrossRefPubMed
66.
Wang CB, et al. Fertility-preserving treatment in young patients with endometrial adenocarcinoma. Cancer. 2002;94(8):2192–8.CrossRefPubMed
67.
Gotlieb WH, et al. Outcome of fertility-sparing treatment with progestins in young patients with endometrial cancer. Obstet Gynecol. 2003;102(4):718–25.CrossRefPubMed
68.
Jadoul P, Donnez J. Conservative treatment may be beneficial for young women with atypical endometrial hyperplasia or endometrial adenocarcinoma. Fertil Steril. 2003;80(6):1315–24.CrossRefPubMed
69.
Niwa K, et al. Outcome of fertility-preserving treatment in young women with endometrial carcinomas. BJOG. 2005;112(3):317–20.CrossRefPubMed
70.
Ota T, et al. Clinicopathologic study of uterine endometrial carcinoma in young women aged 40 years and younger. Int J Gynecol Cancer. 2005;15(4):657–62.CrossRefPubMed
71.
Yahata T, et al. Long-term conservative therapy for endometrial adenocarcinoma in young women. Hum Reprod. 2006;21(4):1070–5.CrossRefPubMed
72.
Yang YC, et al. Reevaluating the safety of fertility-sparing hormonal therapy for early endometrial cancer. Gynecol Oncol. 2005;99(2):287–93.CrossRefPubMed
73.
Le Digabel JF, et al. Young women with atypical endometrial hyperplasia or endometrial adenocarcinoma stage I: will conservative treatment allow pregnancy? Results of a French multicentric survey. Gynecol Obstet Fertil. 2006;34(1):27–33.CrossRefPubMed
74.
Elizur SE, et al. Outcome of in vitro fertilization treatment in infertile women conservatively treated for endometrial adenocarcinoma. Fertil Steril. 2007;88(6):1562–7.CrossRefPubMed
75.
Minaguchi T, et al. Combined phospho-Akt and PTEN expressions associated with post-treatment hysterectomy after conservative progestin therapy in complex atypical hyperplasia and stage Ia, G1 adenocarcinoma of the endometrium. Cancer Lett. 2007;248(1):112–22.CrossRefPubMed
76.
Wheeler DT, Bristow RE, Kurman RJ. Histologic alterations in endometrial hyperplasia and well-differentiated carcinoma treated with progestins. Am J Surg Pathol. 2007;31(7):988–98.CrossRefPubMed
77.
Yamazawa K, et al. Fertility-preserving treatment with progestin, and pathological criteria to predict responses, in young women with endometrial cancer. Hum Reprod. 2007;22(7):1953–8.CrossRefPubMed
78.
Li HZ, Chen XN, Qiao J. Letrozole as primary therapy for endometrial hyperplasia in young women. Int J Gynaecol Obstet. 2008;100(1):10–2.CrossRefPubMed
79.
Eftekhar Z, et al. Efficacy of megestrol acetate (megace) in the treatment of patients with early endometrial adenocarcinoma: our experiences with 21 patients. Int J Gynecol Cancer. 2009;19(2):249–52.CrossRefPubMed
80.
Hahn HS, et al. Conservative treatment with progestin and pregnancy outcomes in endometrial cancer. Int J Gynecol Cancer. 2009;19(6):1068–73.CrossRefPubMed
81.
Han AR, et al. Pregnancy outcomes using assisted reproductive technology after fertility-preserving therapy in patients with endometrial adenocarcinoma or atypical complex hyperplasia. Int J Gynecol Cancer. 2009;19(1):147–51.CrossRefPubMed
82.
Signorelli M, et al. Fertility-sparing treatment in young women with endometrial cancer or atypical complex hyperplasia: a prospective single-institution experience of 21 cases. BJOG. 2009;116(1):114–8.CrossRefPubMed
83.
Yu M, et al. Outcome analysis of conservative treatment of well-differentiated endometrial adenocarcinoma and severe atypical hyperplasia in young women. Zhonghua Fu Chan Ke Za Zhi. 2006;41(4):242–5.PubMed
84.
Mao Y, et al. Outcomes of conservative therapy for young women with early endometrial adenocarcinoma. Fertil Steril. 2010;93(1):283–5.CrossRefPubMed
85.
Mazzon I, et al. Conservative surgical management of stage IA endometrial carcinoma for fertility preservation. Fertil Steril. 2010;93(4):1286–9.CrossRefPubMed
86.
Park H, et al. Effectiveness of high-dose progestin and long-term outcomes in young women with early-stage, well-differentiated endometrioid adenocarcinoma of uterine endometrium. Arch Gynecol Obstet. 2012;285(2):473–8.CrossRefPubMed
87.
Perri T, et al. Prolonged conservative treatment of endometrial cancer patients: more than 1 pregnancy can be achieved. Int J Gynecol Cancer. 2011;21(1):72–8.CrossRefPubMed
88.
Thigpen T, et al. Tamoxifen in the treatment of advanced or recurrent endometrial carcinoma: a Gynecologic Oncology Group study. J Clin Oncol. 2001;19(2):364–7.PubMed