GENERAL PRINCIPLES
Lower gastrointestinal tract tumors are the third most commonly diagnosed cancers in the United States, and second leading cause of cancer death. Surgery cures a high percentage of these cases (50% of all diagnosed cases). This chapter gives an overview of colorectal and anal cancer presentation, pathophysiology, staging, and general principles of treatment.
Epidemiology
Colorectal cancer (CRC) is the fourth most frequently diagnosed cancer and the second leading cause of cancer death in the United States. It accounts for 9% of all cancers deaths. In the United States, the estimated number of new cases and deaths from colorectal cancer in 2010 are 142,570 and 51,370, respectively. The overall incidence of CRC in the United States has been declining for unclear reasons. The current incidence of CRC is ~60.4 per 100,000 population. Incidence increases with age, with ~90% of cases diagnosed in those >50 years old. Peak incidence occurs in the eighth decade of life. The lifetime risk for CRC is 6% in average-risk persons living in the United States.1
Pathophysiology
Most CRCs are thought to develop from adenomatous polyps that arise from the colonic mucosa. Studies have shown that adenomatous polyps can become malignant over a period of 5 to 20 years. The common histologies of a polyp are tubular, tubulovillous, and villous. Villous adenomas are most likely to become malignant. Other characteristic polyps to develop into malignancies are a size >1 cm in diameter and a high grade of dysplasia. Adenomatous polyps are found in ~35% of persons in autopsy studies. Up to 5% of polyps are believed to become malignant over time. More than 95% of CRCs are adenocarcinomas. Of these, >80% are moderately differentiated. Other histologic types seen are undifferentiated, squamous, carcinoid, leiomyosarcomas, and lymphoid neoplasias. Poor prognosis is associated with colloid and signet ring subtypes of adenocarcinoma, which together represent ~20% of tumors.
Risk Factors
Risk factors for CRC are listed below.
![]() First-degree relative with CRC
First-degree relative with CRC
![]() Personal history of CRC
Personal history of CRC
![]() Historyof other malignancies
Historyof other malignancies
![]() History of radiation therapy to the abdomen or pelvis
History of radiation therapy to the abdomen or pelvis
![]() Increasing age
Increasing age
![]() Ureterosigmoidostomies
Ureterosigmoidostomies
![]() Inflammatory bowel disease, especially ulcerative colitis but also Crohn disease
Inflammatory bowel disease, especially ulcerative colitis but also Crohn disease
![]() Family history of a CRC syndrome
Family history of a CRC syndrome
![]() Familial adenomatous polyposis (FAP) is an autosomal dominant disease caused by a defect in the APC gene that leads to colon cancer in 100% of patients by the age of 40 years if they are left untreated. Affected persons will have up to thousands of adenomatous polyps with malignant potential in their bowel. Persons with FAP should have a prophylactic subtotal colectomy by age 30 years. Aggressive precolectomy screening for the development of cancer is also indicated. Other cancers such as medulloblastoma, papillary thyroid carcinoma, hepatoblastoma, pancreatic cancer, and gastric cancer are also associated with this syndrome.
Familial adenomatous polyposis (FAP) is an autosomal dominant disease caused by a defect in the APC gene that leads to colon cancer in 100% of patients by the age of 40 years if they are left untreated. Affected persons will have up to thousands of adenomatous polyps with malignant potential in their bowel. Persons with FAP should have a prophylactic subtotal colectomy by age 30 years. Aggressive precolectomy screening for the development of cancer is also indicated. Other cancers such as medulloblastoma, papillary thyroid carcinoma, hepatoblastoma, pancreatic cancer, and gastric cancer are also associated with this syndrome.
![]() Hereditary nonpolyposis colorectal cancer (HNPCC) is inherited in an autosomal dominant manner and often leads to malignancies with mucinous histology in the right side of the colon. Often these tumors may arise without going through a polyp phase and, therefore, are seen as flat adenomas. HNPCC is also associated with cancers of the endometrium, ovary, stomach, and hepatobiliary system. Prophylactic subtotal colectomy is also recommended for persons with HNPCC.
Hereditary nonpolyposis colorectal cancer (HNPCC) is inherited in an autosomal dominant manner and often leads to malignancies with mucinous histology in the right side of the colon. Often these tumors may arise without going through a polyp phase and, therefore, are seen as flat adenomas. HNPCC is also associated with cancers of the endometrium, ovary, stomach, and hepatobiliary system. Prophylactic subtotal colectomy is also recommended for persons with HNPCC.
![]() Other inherited syndromes associated with an increased risk of CRC include MYH-associated polyposis, Gardner’s syndrome, Turcot’s syndrome, Muir–Torre syndrome, and Peutz–Jeghers syndrome.
Other inherited syndromes associated with an increased risk of CRC include MYH-associated polyposis, Gardner’s syndrome, Turcot’s syndrome, Muir–Torre syndrome, and Peutz–Jeghers syndrome.
Prevention/Screening
Screening methods used to detect CRC include fecal occult blood testing (FOBT), endoscopy, and barium enema. Early detection improves survival through detection of more curable lesions, and CRC incidence is high enough that screening can be cost-effective with an acceptable positive predictive value. Patients with warning signs of CRC require more aggressive investigations, typically colonoscopy.
For the asymptomatic patient:
![]() FOBT is the least expensive and most widely used screening test for the detection of CRC. There are problems with its sensitivity, which has been reported to be from 25% to 80% with a specificity of >90%. Sensitivity will be affected by polyp size and frequency of bleeding. Specificity is affected by NSAID use, other sources of gastrointestinal bleeding, consumption of red meat, and consumption of certain vegetables in the diet. Hydration of samples before testing them is not recommended, as this worsens the specificity of the test.
FOBT is the least expensive and most widely used screening test for the detection of CRC. There are problems with its sensitivity, which has been reported to be from 25% to 80% with a specificity of >90%. Sensitivity will be affected by polyp size and frequency of bleeding. Specificity is affected by NSAID use, other sources of gastrointestinal bleeding, consumption of red meat, and consumption of certain vegetables in the diet. Hydration of samples before testing them is not recommended, as this worsens the specificity of the test.
![]() Flexible sigmoidoscopy examines up to 60 cm of the rectum and distal colon and can detect ~50% of CRC cases. Its advantages are that it can be performed in the primary care physician’s office and that it has a specificity of nearly 100%. However, it has the disadvantage of not assessing the entire colon, and biopsies cannot be obtained during the procedure. Abnormalities necessitate a follow-up colonoscopy for biopsy.
Flexible sigmoidoscopy examines up to 60 cm of the rectum and distal colon and can detect ~50% of CRC cases. Its advantages are that it can be performed in the primary care physician’s office and that it has a specificity of nearly 100%. However, it has the disadvantage of not assessing the entire colon, and biopsies cannot be obtained during the procedure. Abnormalities necessitate a follow-up colonoscopy for biopsy.
![]() Double-contrast barium enema is a radiologic method for detection of CRC and is the safest of the visualization methods. It also requires a bowel preparation and, like FOBT, has the disadvantage of requiring subsequent endoscopy for biopsy of identified lesions.
Double-contrast barium enema is a radiologic method for detection of CRC and is the safest of the visualization methods. It also requires a bowel preparation and, like FOBT, has the disadvantage of requiring subsequent endoscopy for biopsy of identified lesions.
![]() Colonoscopy is considered the gold standard for detection of CRC but is associated with a higher complication rate and a higher cost than the other methods. It also involves more extensive preparation before the procedure and sedation during it. For the general population after age 50 years, National Comprehensive Cancer Network (NCCN) guidelines recommend colonoscopy every 10 years or annual FOBT combined with flexible sigmoidoscopy every 5 years. If risk factors such as a history of inflammatory bowel disease, family members with CRC, or a known defect such as HNPCC or FAP are present, then more frequent and earlier testing is recommended. For patients with a familial history of colorectal cancer, screening begins 10 years before the age of cancer diagnosis of the affected family member.
Colonoscopy is considered the gold standard for detection of CRC but is associated with a higher complication rate and a higher cost than the other methods. It also involves more extensive preparation before the procedure and sedation during it. For the general population after age 50 years, National Comprehensive Cancer Network (NCCN) guidelines recommend colonoscopy every 10 years or annual FOBT combined with flexible sigmoidoscopy every 5 years. If risk factors such as a history of inflammatory bowel disease, family members with CRC, or a known defect such as HNPCC or FAP are present, then more frequent and earlier testing is recommended. For patients with a familial history of colorectal cancer, screening begins 10 years before the age of cancer diagnosis of the affected family member.
DIAGNOSIS
Colonoscopy with biopsy is the diagnostic procedure of choice and is potentially curative for benign polyps and carcinoma in situ. Diagnosis depends on tissue pathology consistent with invasive colon cancer.
Clinical Presentation
History
![]() CRC may present with symptoms such as fatigue, anorexia, failure to thrive, lower gastrointestinal bleeding, and right upper quadrant pain associated with liver metastasis, although it is often asymptomatic until the tumor is large in size. Patients may also present due to a positive screen test.
CRC may present with symptoms such as fatigue, anorexia, failure to thrive, lower gastrointestinal bleeding, and right upper quadrant pain associated with liver metastasis, although it is often asymptomatic until the tumor is large in size. Patients may also present due to a positive screen test.
![]() Symptoms associated with CRC are often related to the location of the tumor within the bowel. Therefore, right-sided lesions often present with symptoms of anemia and, occasionally, of melena. Left-sided lesions commonly cause obstruction, tenesmus, constipation, bright-red blood per rectum, and other changes in bowel habits. Patients often have an iron-deficiency anemia and may have symptoms of pica.
Symptoms associated with CRC are often related to the location of the tumor within the bowel. Therefore, right-sided lesions often present with symptoms of anemia and, occasionally, of melena. Left-sided lesions commonly cause obstruction, tenesmus, constipation, bright-red blood per rectum, and other changes in bowel habits. Patients often have an iron-deficiency anemia and may have symptoms of pica.
![]() Because CRC is a cause of anemia, it is important to evaluate any person who presents with unexplained anemia for CRC, especially men and postmenopausal women.
Because CRC is a cause of anemia, it is important to evaluate any person who presents with unexplained anemia for CRC, especially men and postmenopausal women.
![]() CRC most often metastasizes to the liver, lung, adrenals, ovaries, and bone, so symptoms of organ compromise such as abdominal discomfort, shortness of breath, and bone pain may be present in metastatic disease.
CRC most often metastasizes to the liver, lung, adrenals, ovaries, and bone, so symptoms of organ compromise such as abdominal discomfort, shortness of breath, and bone pain may be present in metastatic disease.
Physical Exam
Signs of CRC on physical exam include gross blood or melanotic stool in the rectal vault, pallor in the conjunctivae and the nail beds, or a palpable mass in the abdomen or the rectum. If liver metastases are present, patients may have hepatomegaly and be tender to palpation in the right upper quadrant. On barium enema, an apple core lesion may be seen, which suggests colon cancer. Bacteremia or endocarditis with Streptococcus bovis is also a sign of CRC, and these findings should trigger an evaluation for colon cancer.
Diagnostic Testing
Laboratories
![]() CBC to evaluate for associated iron-deficiency anemia
CBC to evaluate for associated iron-deficiency anemia
![]() Chemistry and liver function tests to evaluate for liver involvement
Chemistry and liver function tests to evaluate for liver involvement
![]() Carcinoembryonic antigen (CEA): if initially elevated, then a rise in CEA after treatment may indicate a recurrence
Carcinoembryonic antigen (CEA): if initially elevated, then a rise in CEA after treatment may indicate a recurrence
Imaging Studies
![]() Chest/abdomen/pelvis CT scan to rule out metastasis
Chest/abdomen/pelvis CT scan to rule out metastasis
Diagnostic Procedures
![]() All patients should have the entire colon evaluated by colonoscopy or barium enema to rule out synchronous lesions. Up to 5% of patients have another focus of CRC in their bowels. Patients should have a tissue biopsy before therapy to confirm the diagnosis.
All patients should have the entire colon evaluated by colonoscopy or barium enema to rule out synchronous lesions. Up to 5% of patients have another focus of CRC in their bowels. Patients should have a tissue biopsy before therapy to confirm the diagnosis.
Staging
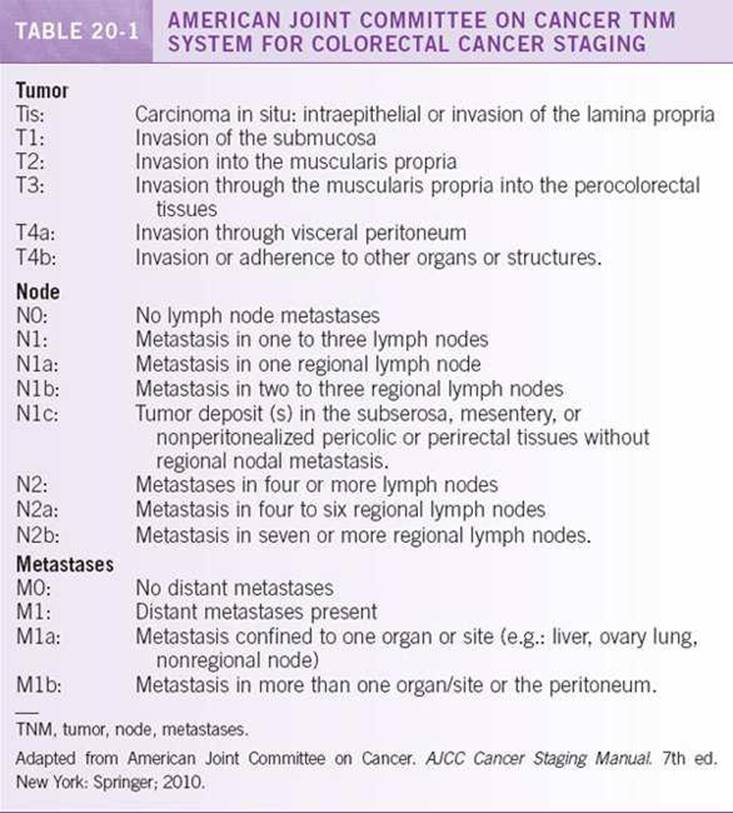
![]() Surgery is important for accurate staging of CRC. The preferred staging system for CRC is the American Joint Committee on Cancer (AJCC) TNM (tumor, node, metastases) system (Table 20-1). TNM uses the degree of tumor invasion, the presence of positive lymph nodes, and the presence of distant metastasis to classify the disease in one of four stages. Although the AJCC TNM staging system is the preferred staging system today, the Duke staging system with the Astler–Coller modification is often referred to in older literature (Table 20-2).
Surgery is important for accurate staging of CRC. The preferred staging system for CRC is the American Joint Committee on Cancer (AJCC) TNM (tumor, node, metastases) system (Table 20-1). TNM uses the degree of tumor invasion, the presence of positive lymph nodes, and the presence of distant metastasis to classify the disease in one of four stages. Although the AJCC TNM staging system is the preferred staging system today, the Duke staging system with the Astler–Coller modification is often referred to in older literature (Table 20-2).

TREATMENT
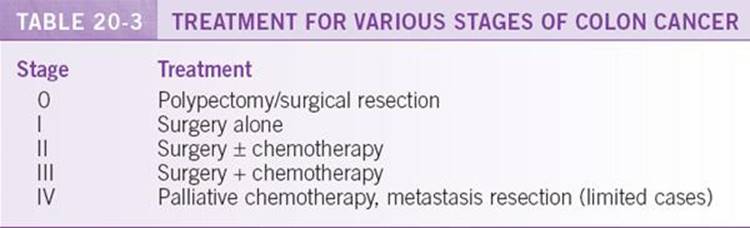
The goals of therapy need to be clearly delineated from the beginning and reevaluated throughout the patient’s course. Colon cancer that has not metastasized is a curable disease with surgery. Chemotherapy can be added to improve cure rates for stage II or III tumors or as palliation for incurable tumors (Table 20-3).
![]() Surgery is undertaken with intent to cure in 75% of those with colon cancer. Many of the remainder will require surgery to prevent obstruction, perforation, or bleeding. Wide excision of the tumor with a distal margin of ~5 cm is recommended for curative surgery. The length of colon and mesentery resected is determined by vascular anatomy. If the tumor is adherent to or invades another organ, an en bloc excision must be done to prevent seeding to allow for the possibility of cure. If the surgical intent is palliation instead of cure, a simple resection or diversion is used to lessen morbidity from the procedure. In stage IV cancer, some patients may benefit from resection of metastases. Five-year survival rates of up to 40% have been obtained with resection of limited liver metastases.3
Surgery is undertaken with intent to cure in 75% of those with colon cancer. Many of the remainder will require surgery to prevent obstruction, perforation, or bleeding. Wide excision of the tumor with a distal margin of ~5 cm is recommended for curative surgery. The length of colon and mesentery resected is determined by vascular anatomy. If the tumor is adherent to or invades another organ, an en bloc excision must be done to prevent seeding to allow for the possibility of cure. If the surgical intent is palliation instead of cure, a simple resection or diversion is used to lessen morbidity from the procedure. In stage IV cancer, some patients may benefit from resection of metastases. Five-year survival rates of up to 40% have been obtained with resection of limited liver metastases.3
![]() Adjuvant chemotherapy is administered to patients who have undergone potentially curative resection of colon cancer. The goal of adjuvant therapy is to eradicate micrometastases, thereby reducing the likelihood of disease recurrence. 5-Fluorouracil (5-FU), leucovorin, and oxaliplatin (FOLFOX) is preferred but may consider 5-FU with leucovorin or capecitabine for patients who cannot tolerate oxaliplatin after resection of stage III colon cancer. Capecitabine is an oral prodrug that is converted to 5-FU in tumor tissues. Adjuvant chemotherapy has demonstrated approximately a 30% reduction in the risk of disease recurrence and 10% reduction in mortality. However, controversy remains over adjuvant chemotherapy for stage II disease. Because there seems to be only a small benefit from treating stage II colon cancer, chemotherapy should be considered for high-risk disease, including those patients who present with a total obstruction, T4 tumors (stage IIB), perforation, poor histological grade, lymphovascular invasion, or positive surgical margins and inadequately sampled nodes (<12 lymph nodes).4–9 In patients with stage II disease, a deficiency in MMR (mismatch repair) protein expression or high levels of microsatellite instability protein (MSI-H) are markers of a more favorable outcome with decreased benefit (possibly detrimental impact) from adjuvant therapy with 5-FU alone. 10
Adjuvant chemotherapy is administered to patients who have undergone potentially curative resection of colon cancer. The goal of adjuvant therapy is to eradicate micrometastases, thereby reducing the likelihood of disease recurrence. 5-Fluorouracil (5-FU), leucovorin, and oxaliplatin (FOLFOX) is preferred but may consider 5-FU with leucovorin or capecitabine for patients who cannot tolerate oxaliplatin after resection of stage III colon cancer. Capecitabine is an oral prodrug that is converted to 5-FU in tumor tissues. Adjuvant chemotherapy has demonstrated approximately a 30% reduction in the risk of disease recurrence and 10% reduction in mortality. However, controversy remains over adjuvant chemotherapy for stage II disease. Because there seems to be only a small benefit from treating stage II colon cancer, chemotherapy should be considered for high-risk disease, including those patients who present with a total obstruction, T4 tumors (stage IIB), perforation, poor histological grade, lymphovascular invasion, or positive surgical margins and inadequately sampled nodes (<12 lymph nodes).4–9 In patients with stage II disease, a deficiency in MMR (mismatch repair) protein expression or high levels of microsatellite instability protein (MSI-H) are markers of a more favorable outcome with decreased benefit (possibly detrimental impact) from adjuvant therapy with 5-FU alone. 10
![]() Palliative treatment for metastatic disease depends on the functional status of the patient. It typically involves 5-FU with leucovorin, capecitabine alone, or 5-FU and leucovorin in combination with either the topoisomerase I inhibitor irinotecan (the FOLFIRI regimen) or oxaliplatin (the FOLFOX regimen).11–16 Both of the combination regimens have improved efficacy by the addition of the vascular endothelial growth factor antibody, bevacizumab (Avastin)17,18 or endothelial growth factor receptor inhibitory antibodies, cetuximab (Erbitux), or panitumumab (Vectibix) in patients with K-Ras wild-type gene. After disease progression, patients are usually switched to another one of the primary regimens and may also receive either of the endothelial growth factor receptor inhibitory antibodies, cetuximab (Erbitux), or panitumumab (Vectibix)19–21 if the tumors are K-Ras wild type. Patients with stage IV disease should be referred for clinical trials when possible.
Palliative treatment for metastatic disease depends on the functional status of the patient. It typically involves 5-FU with leucovorin, capecitabine alone, or 5-FU and leucovorin in combination with either the topoisomerase I inhibitor irinotecan (the FOLFIRI regimen) or oxaliplatin (the FOLFOX regimen).11–16 Both of the combination regimens have improved efficacy by the addition of the vascular endothelial growth factor antibody, bevacizumab (Avastin)17,18 or endothelial growth factor receptor inhibitory antibodies, cetuximab (Erbitux), or panitumumab (Vectibix) in patients with K-Ras wild-type gene. After disease progression, patients are usually switched to another one of the primary regimens and may also receive either of the endothelial growth factor receptor inhibitory antibodies, cetuximab (Erbitux), or panitumumab (Vectibix)19–21 if the tumors are K-Ras wild type. Patients with stage IV disease should be referred for clinical trials when possible.
Treatment of Rectal Cancer
![]() Surgery is used in rectal cancer to cure the disease, and it also plays a role in palliative therapy. The most important feature of the rectum is the lack of a serosa for these tumors. Because of this anatomy, local recurrence for rectal cancer is high, and neoadjuvant therapy may be needed to make a tumor resectable. Accordingly, surgery is used in conjunction with radiation or chemoradiation,22–24 and this multimodality approach has been associated with decreased recurrence. Approaches aimed at sphincter preservation, obviating the need for colostomy, can often be performed if a 2-cm margin can be obtained.
Surgery is used in rectal cancer to cure the disease, and it also plays a role in palliative therapy. The most important feature of the rectum is the lack of a serosa for these tumors. Because of this anatomy, local recurrence for rectal cancer is high, and neoadjuvant therapy may be needed to make a tumor resectable. Accordingly, surgery is used in conjunction with radiation or chemoradiation,22–24 and this multimodality approach has been associated with decreased recurrence. Approaches aimed at sphincter preservation, obviating the need for colostomy, can often be performed if a 2-cm margin can be obtained.
![]() Compared to colon cancer, rectal cancer is much more likely to recur locally than distally. Adjuvant chemoradiation is therefore tailored to prevent local recurrence in stage II and III cancers. 22,23 Currently, stage II rectal cancer is treated with surgery along with FOLFOX, 5-FU, or capecitabine and radiation, leading to significant improvements in overall survival compared to treatment with surgery alone. 25,26For stage III tumors, part of the systemic chemotherapy and radiation therapy may be given before surgery to increase resectability.24–26
Compared to colon cancer, rectal cancer is much more likely to recur locally than distally. Adjuvant chemoradiation is therefore tailored to prevent local recurrence in stage II and III cancers. 22,23 Currently, stage II rectal cancer is treated with surgery along with FOLFOX, 5-FU, or capecitabine and radiation, leading to significant improvements in overall survival compared to treatment with surgery alone. 25,26For stage III tumors, part of the systemic chemotherapy and radiation therapy may be given before surgery to increase resectability.24–26
COMPLICATIONS
Tumor Related
Complications that can result from CRC include bowel obstruction, anemia, and abdominal pain. More serious complications can include peritonitis after perforation, fistula formation, and malnutrition. Complications can also result from sites of metastatic disease. Liver metastases can lead to hyperbilirubinemia and coagulopathies. Pulmonary metastases, when advanced, may result in cough or shortness of breath. Patients may also develop pain at sites of metastases.
Treatment Related
Complications of treatment are commonly related to surgery and chemotherapy but can also occur with radiation therapy. Postoperative mortality rates are 1% to 5%. Major morbidity includes bowel and bladder dysfunction, sexual dysfunction, anastomotic leaks, and bowel obstruction. The need for a permanent colostomy can be psychologically upsetting. Chemotherapy complications may include neuropathy (possibly long term), nausea, diarrhea, and hand-foot syndrome. Radiation may cause local radiation dermatitis with pain, desquamation, and color changes.
MONITORING/FOLLOW-UP
Current recommendations are for a history, physical, and CEA every 3 months for 2 years, and then every 6 months for another 3 years. At 1 year, a colonoscopy should be performed to look for local recurrence and synchronous disease. If the colonoscopy is negative, then it should be repeated in 3 years and then every 5 years. If the patient had a high-grade tumor or lymphovascular invasion, then a CT of the chest, abdomen, and pelvis should be repeated annually for the first 3 years to monitor for metastatic spread.
OUTCOMES/PROGNOSIS
Stage has great significance in the prognosis and treatment of the disease. In the United States between 1996 and 2002, the overall 5-year survival rate for patients with CRC was 65.1%. The 5-year survival for stages I/II, III, and IV was 90.4%, 68.1%, and 9.8%, respectively. Other prognostic factors include the number of positive lymph nodes and if the tumor invasion was through the bowel wall into adjacent organs or into veins.
ANAL CANCER
GENERAL PRINCIPLES
Epidemiology
Anal cancer accounts for ~1.6% of all alimentary malignancies in the United States. Its incidence generally increases with age, with the peak incidence in the sixth and seventh decades of life. The incidence is increasing in men <40 years old due to increased risk in the HIV+ population. Histologically, 63% of anal cancers are squamous cell carcinomas. Basaloid transitional cell carcinomas (cloacogenic) make up 23% of cases. More rare types of anal cancers are adenocarcinoma, basal cell carcinoma, and melanoma.
Risk Factors
![]() The risk factor most commonly associated with anal cancer is human papilloma virus (HPV) infection particularly with serotypes 16 and 18. In women, increased anal cancers are seen with HPV-associated cervical cancer. In men, anal cancer is more frequently associated with receptive anal intercourse and HPV. As many as 70% of anal cancers are positive for HPV.
The risk factor most commonly associated with anal cancer is human papilloma virus (HPV) infection particularly with serotypes 16 and 18. In women, increased anal cancers are seen with HPV-associated cervical cancer. In men, anal cancer is more frequently associated with receptive anal intercourse and HPV. As many as 70% of anal cancers are positive for HPV.
![]() Other risk factors include immunosuppression, such as that seen after renal transplant or HIV infection. Current cigarette smoking is also a risk factor for anal cancer, with a relative risk of seven- to ninefold for smokers.
Other risk factors include immunosuppression, such as that seen after renal transplant or HIV infection. Current cigarette smoking is also a risk factor for anal cancer, with a relative risk of seven- to ninefold for smokers.
DIAGNOSIS
Clinical Presentation
History
Anal cancers present with bleeding 50% of the time. Other symptoms include pain, mass, constipation, diarrhea, and pruritus. Often the symptoms are ascribed to hemorrhoids, which may delay diagnosis. Approximately 25% of people are asymptomatic when the cancer is discovered.
Physical Exam
Physical exam findings include an anal mass and lymphadenopathy. On palpation, an anal mass will often be firm and indurated. Anoscopy, proctoscopy, and transrectal ultrasonography are used to visualize the mass. Diagnosis is made by incisional biopsy of the mass and any suspicious inguinal lymphadenopathy.
Diagnostic Testing
Procedures
Digital rectal exam and inguinal lymph node exam should be accompanied by anoscopy. Notes should be made of the location of the mass, including its position relative to the dentate line. Anal cancers are divided into those of the anal margin and those of the anal canal. The line of demarcation is a zone approximately halfway between the dentate line and the anal verge. Women should have a pelvic exam for cervical cancer screening due to the association with HPV. Men and women should be tested for HIV, especially if any risk factors are present.
Imaging
Imaging may include chest x-ray or chest CT, abdominal/pelvic CT or MRI, and possible PET scan to rule out metastatic disease.
Staging
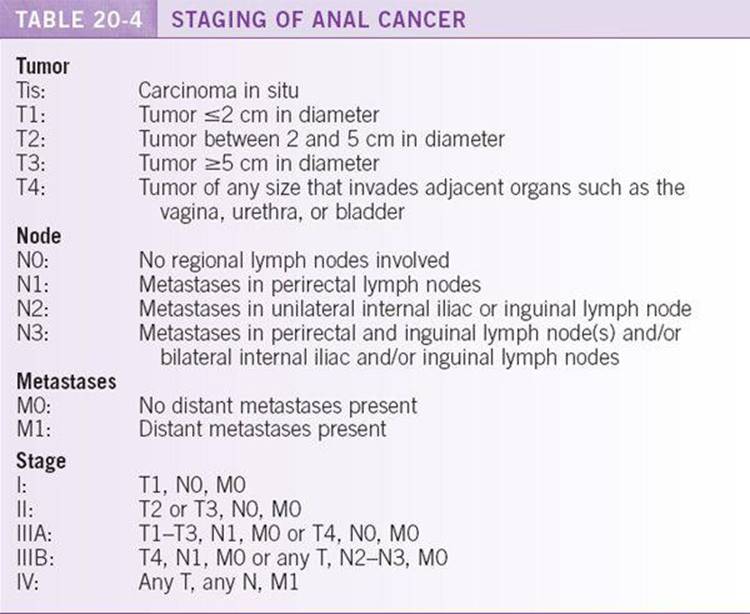
Staging is based on the TNM system (Table 20-4).
TREATMENT
Very small tumors at the anal margin may be treated with wide local excision. Larger (T2-T4) and node positive cancers should be treated similar to anal canal carcinomas with concurrent chemoradiation (5-FU and Mitomycin). 27,28 In several trials, 5-year survival varied between 64% and 83% with combined-modality therapy. After treatment, close medical follow-up is needed to screen for recurrence. Recurrences may be treated surgically if resectable, or if unresectable consider cisplatin-based chemotherapy or clinical trial.
OUTCOME/PROGNOSIS
Prognosis is related to the size of the primary tumor and the presence of lymph node metastases.
The 5-year survival rate for patients with tumors that are treated with chemoradiation and that are ≤2 cm is 80%, whereas if they are ≥5 cm it is less than 50%.29,30 Tumors in the anal margin have a more favorable prognosis than those in the canal.
REFERENCES
1. Jemal A, Siegal R, Xu J, et al. Cancer statistics 2010. CA Cancer J Clin. 2010;60:277–300.
2. Edge SB, Byrd DR, Compton CC, et al. AJCC (American Joint Committee on Cancer) Cancer Staging Manual. 7th ed. NewYork: Springer; 2010.
3. Choti MA, Sitzmann JV, Tiburi MF, et al. Trends in long term survival following liver resection for hepatic colorectal metastases. Ann Surg. 2002;235(6):759–766.
4. Benson AB, Schrag D, Somerfield MR, et al. American society of clinical oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol. 2004;22:3408–3419.
5. Andre T, Boni C, Navarro M, et al. Improved survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the mosaic trial. J Clin Oncol. 2009;27:3109–3116.
6. National Comprehensive Cancer Network (NCCN) guidelines. www.nccn.org (accessed on 12/02/10)
7. O’Connell MJ, Mailliard JA, Kahn MJ, et al. Controlled trial of fluorouracil and low dose leucovorin given for 6 months as postoperative adjuvant therapy for colon cancer. J Clin Oncol. 1997;15:246–250.
8. Gill S, Loprinzi CL, Sargent DJ, et al. Pooled analysis of flurouracil-based adjuvant therapy for Stage II and Stage III colon cancer: who benefit and by how much? J Clin Oncol. 2004;22:1797–1806.
9. Quasar Collaborative group, Gray R, Barnwell J, et al. Adjuvant chemotherapy versus observation in patients with colorectal cancer: a randomised study. Lancet. 2007;370:2020–2029.
10. Sargent DJ, Marsoni S, Monges G, et al. Defective mismatch repair as a predictive marker for lack of efficacy of fluorouracil-based adjuvant therapy in colon cancer. J Clin Oncol. 2010;28:3219–3223.
11. Van Custem E, Twelves C, Cassidy J, et al. Oral capecitabine compared with intravenous flurouracil plus leucovorin in patients with metastatic colorectal cancer: results of a large phase III study. J Clin Oncol. 2001;19:4097–4106.
12. Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. N Engl J Med. 2000;343:905–914.
13. De Gramont A, Figer A, Seymour M, et al. Leucovorinandflurouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol. 2000;18:2938–2947.
14. Goldberg RM, Sargent DJ, Morton RF, et al. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol. 2004;22:23–30.
15. Tournigand C, Andre T, Achille E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol. 2004; 22:229–237.
16. Cassidy J, Clarke S, Diaz–Rubio E, et al. Randomized phase III study of capecitabine plus oxaliplatin compared with fluorouracil/folinic acid plus oxaliplatin as first line therapy for metastatic colorectal cancer. J Clin Oncol. 2008;26:2006–2012.
17. Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350:2335–2342.
18. Saltz LB, Clarke S, Diaz–Rubio E, et al. Bevacizumab in combination with oxaliplatin based chemotherapy as first line therapy in metastatic colorectal cancer: a randomized phase III study. J Clin Oncol. 2008;26:2013–2019.
19. Van Custem E, Kohne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360:1408–1417.
20. Bokemeyer C, Bondarenko I, Makhson A, et al. Fluorouracil, leucovorin and oxaliplatin with and without cetuximab in the first-line treatment of metastatic colorectal cancer. J Clin Oncol. 2009;27:663–671.
21. Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med. 2004;351:337–345.
22. Roh MS, Colangelo LH, O’Connell MJ, et al. Preoperative multimodality therapy improves disease-free survival in patients with carcinoma of the rectum: NSABP R-03. J Clin Oncol. 2009;27(31):5124–5130.
23. Bosset JF, Collette L, Calais G, et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med. 2006;355(11):1114–1123.
24. Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351(17):1731–1740.
25. Krook JE, Moertel CG, Gunderson LL, et al. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med. 1991;324(11):709–715.
26. Douglass HO, Moertel CG, Mayer RJ, et al. Survival after postoperative combination treatment of rectal cancer. N Engl J Med. 1986;315:1294–1295.
27. Ajani JA, Winter KA, Gunderson LL, et al. Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled trial. JAMA. 2008;299:1914–1921.
28. Faivre C, Rougier P, Ducreux M, et al. 5-Fluorouracil and cisplatin combination chemotherapy for metastatic squamous–cell anal cancer. Bull Cancer. 1999;86:861–865.
29. Cummings BJ, Ajani JA, Swallow CJ. Cancer of the anal region. In: DeVita VT, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 8th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2008:1301–1313.
30. Bilimoria KY, Bentrem DJ, Rock CE, et al. Outcomes and prognostic factors for squamous-cell carcinoma of the anal cancer: analysis of patients from the national cancer data base. Dis Colon Rectum. 2009;52:624–631.