Ron M. Walls
Approach to the Airway
This chapter presents and discusses the emergency airway algorithms, which the authors have developed, used, taught, and refined for more than 12 years. When we first set out to try to codify the cognitive aspects of emergency airway management, we were both liberated and impaired by the complete lack of any such algorithms to guide us. In developing The Airway Course, then The Difficult Airway Course: Emergency, The Difficult Airway Course: Anesthesia, and The Difficult Airway Course: EMS, and in applying successively each iteration of the emergency airway algorithms to tens of thousands of real and simulated cases involving thousands of providers, we felt guided by both our continuous learning about optimal airway management and the empirical application of these principles on a large scale. These algorithms, or adaptations of them, now appear in many of the major emergency medicine textbooks and online references. They are used in airway courses, for residency training, and in didactic teaching sessions, both for in-hospital and out-of-hospital providers. They have stood the test of time and have benefited from constant updating. This current iteration reflects broader application of flexible fiberoptic (FO) methods, new options with extraglottic devices (EGDs), and a near revolution in video and rigid FO laryngoscopy, causing us to rethink concepts related to the definition and management of the “difficult airway” (see Chapter 7). Together, as before, these algorithms comprise a fundamental, reproducible approach to the emergency airway. The purpose is not to provide a “cookbook,” which one could universally and mindlessly apply, but rather to describe a reproducible set of decisions and actions to enhance performance and maximize the opportunities for success, even in difficult or challenging cases. The specialized algorithms all build from concepts found in the main emergency airway algorithm, which details the evaluation of the patient for the presence of a crash airway, a difficult airway, or a failed airway. The algorithms do not attempt to deal with the decision to intubate. This is covered in Chapter 1. Therefore, the entry point for the emergency airway algorithm is immediately after the decision to intubate has been made.
The algorithms are intended as guidelines for management of the emergency airway. Although they are not meant to be interpreted as strict rules, covering every possible eventuality, they are designed to present distinct, recognizable patterns and to guide the actions to be taken for each pattern. The goal is to simplify some of the complexities of emergency airway management by defining distinct classes of airway problems. For example, we single out those patients who are essentially dead or near death (i.e., unresponsive, agonal) and manage them using a distinct pathway, the crash airway algorithm. Similarly, a patient with a difficult airway must be identified and managed according to sound principles. Serious problems can ensue if a neuromuscular blocking agent is given to a patient with a difficult airway, unless the difficulty was identified and planned for, and the neuromuscular blocking agent is part of that planned approach.
By grouping patients with certain characteristics together, the algorithms assist the clinician in applying basic notions of pattern recognition so that each patient can be identified as a member of one of a small number of groups, and each group has a defined series of actions. For example, in the case of a difficult airway, the difficult airway algorithm facilitates formulation of a distinct, but reproducible plan, which is individualized for that particular patient, yet lies within the overall approach that is predefined for difficult airways.
In human factors analysis, failure to recognize a pattern is often a precursor to medical error.
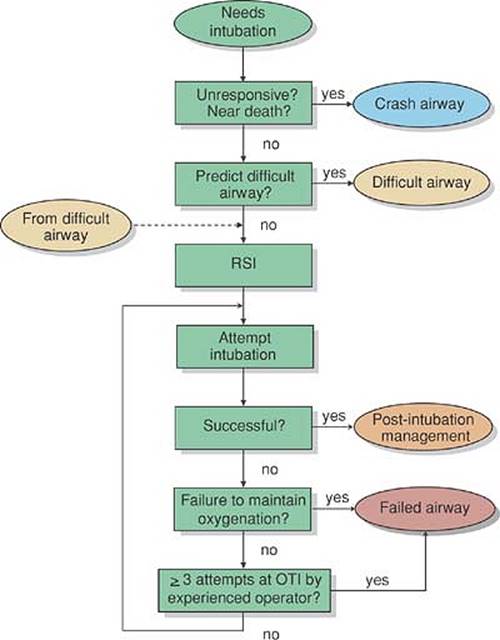
Algorithms are best thought of as a series of key questions and critical actions, with the answer to each question guiding the next critical action. Figures 2-1 and 2-2 provide an overview of the algorithms, and how they work together. When a patient requires intubation, the first question is “Is this a crash airway?” (i.e., is the patient unconscious, near death, with agonal or no respirations, expected to be unresponsive to the stimulation of direct laryngoscopy?). If the answer is “yes,” the patient is managed as a crash airway using the crash airway algorithm (Fig. 2-3). If the answer is “no,” the next question is “Is this a difficult airway?” (see Chapter 7). If the answer is “yes,” the patient is managed as a difficult airway (Fig. 2-4). If the answer is “no,” then neither a crash airway nor a difficult airway is present, and rapid sequence intubation (RSI) is recommended, as described on the main algorithm (Fig. 2-2). Regardless of the algorithm used initially (main, crash, or difficult), if airway failure occurs, the failed airway algorithm (Fig. 2-5) is immediately invoked. The working definition of the failed airway is crucial and is explained in much more detail in the following sections. It has been our experience that airway management errors occur much more often because the provider does not recognize the situation (e.g., failed airway), as opposed to recognizing the situation, but not knowing what actions to take.
|
|
|
Figure 2-1 • Universal Emergency Airway Algorithm. This algorithm demonstrates how the emergency airway algorithms work together. For all algorithms, green represents the main algorithm, yellow is the difficult airway algorithm, blue is the crash airway algorithm, red is the failed airway algorithm, and orange represents an end point. © 2008 The Difficult Airway Course: Emergency. |
The Emergency Airway Algorithm (Main Algorithm)
The main emergency airway algorithm is shown in Fig. 2-2. It begins after the decision to intubate and ends when the airway is secured, whether intubation is achieved directly or via one of the other algorithms. The algorithm is navigated by following defined steps with decisions driven by the answers to a series of key questions:
· Key question 1: Is this a crash airway? If the patient presents in an essentially unresponsive state and is deemed to be unlikely to respond in any way to direct laryngoscopy, then the patient is defined as a crash airway. Here, we are identifying patients who are in full cardiac or respiratory arrest, or patients with agonal cardiorespiratory activity (e.g., agonal, ineffective respirations, pulseless idioventricular rhythm). These patients, who have been referred to as the “nearly dead or the newly dead,” are managed in a manner appropriate for their extremis condition. If a crash airway is identified, exit this main algorithm and begin the crash airway algorithm (Fig. 2-3). Otherwise, continue on the main algorithm.
|
|
|
Figure 2-2 • Main Emergency Airway Management Algorithm. See text for details. © 2008 The Difficult Airway Course: Emergency. |
· Key question 2: Is this a difficult airway? If the airway is not identified as a crash airway, the next task is to determine whether it is a difficult airway, which encompasses difficult laryngoscopy and intubation, difficult bag-mask ventilation (BMV), difficult cricothyrotomy, and difficult extra-glottic device (EGD) use. Chapter 7 outlines the assessment of the patient for a potentially difficult airway using the various mnemonics (LEMON, MOANS, SHORT, and RODS) corresponding to these dimensions of difficulty. It is understood that virtually all emergency intubations are difficult to some extent. However, the evaluation of the patient for attributes that predict difficult airway management is extremely important. If the patient represents a particularly difficult airway situation, then he or she is managed as a difficult airway, using the difficult airway algorithm (Fig. 2-4), and one would exit the main algorithm. Although it is the LEMON assessment for difficult laryngoscopy and intubation that may be the main driver, evaluation for the other difficulties (BMV, cricothyrotomy, EGD) is also critical at this point. If the airway is not identified as particularly difficult, continue on the main algorithm to the next step, which is to perform RSI.
· Critical action: Perform RSI. In the absence of an identified crash or difficult airway, RSI is the method of choice for managing the emergency airway. RSI is described in detail in Chapter 3 and affords the best opportunity for success with the least likelihood of adverse outcome of any possible airway method, when applied to appropriately selected patients. This step assumes that the appropriate sequence of RSI (the seven Ps) will be followed as described in Chapter 3. If the patient is in extreme respiratory distress, or if haste is indicated for any reason, an accelerated or immediate RSI protocol can be used (see Chapter 3).
In the absence of difficult airway predictors, rapid sequence intubation is the most rapid, most effective, and safest method of emergency airway management.
During RSI, intubation is attempted. According to the standard nomenclature of the National Emergency Airway Registry, a multicenter study of emergency intubation, an attempt is defined as activities occurring during a single continuous laryngoscopy maneuver, beginning when the laryngoscope is inserted into the patient's mouth, and ending when the laryngoscope is removed, regardless of whether an endotracheal tube is actually inserted into the patient. In other words, if several attempts are made to pass an endotracheal tube through the glottis during the course of a single laryngoscopy, these aggregate efforts count as one attempt. If the glottis is not visualized and no attempt is made to insert a tube, the laryngoscopy is still counted as one attempt. These distinctions are important because of the definition of the failed airway that follows.
· Key question 3: Was intubation successful? If the first oral intubation attempt is successful, the patient is intubated, postintubation management is initiated, and the algorithm terminates. If the intubation attempt is not successful, continue on the main pathway.
· Key question 4: Can the patient's oxygenation be maintained? When the first attempt at intubation is unsuccessful, it is often possible and appropriate to attempt a second laryngoscopy without interposed BMV because oxygen saturations often remain acceptable for an extended period of time due to proper preoxygenation. In general, supplemental oxygenation with a bag and mask is not necessary until the oxygen saturation falls into the low 90% range. When the oxygen saturation reaches this level, the appropriate first maneuver is BMV of the patient. This approach underscores the importance of assessing the likelihood of successful BMV (MOANS, see Chapter 7) before beginning the intubation sequence. In the vast majority of cases, especially when neuromuscular blockade has been used, BMV will provide adequate ventilation and oxygenation for the patient, defined as maintenance of the oxygen saturation at 90% or higher. If BMV is not capable of maintaining the oxygen saturation above 90%, better technique, including oral and nasal airways, two-person two-handed technique, and optimal positioning of the patient will usually result in effective ventilation (see Chapter 5). If BMV fails despite optimal technique, the airway is considered a failed airway, and one must exit the main algorithm immediately and initiate the failed airway algorithm (Fig. 2-5). Recognition of the failed airway is crucial because delays caused by persistent, futile attempts at intubation will waste critical seconds or minutes and may sharply reduce the time remaining for a rescue technique to be successful before brain injury ensues.
· Key question 5: Have three attempts at orotracheal intubation been made by an experienced operator? There are two essential definitions of the failed airway: (a) “can't intubate, can't oxygenate” (CICO) (described previously); and (b) “three failed attempts by an experienced operator.” If three separate attempts at orotracheal intubation by an experienced operator have been unsuccessful, then the airway is again defined as a failed airway, despite the ability to adequately oxygenate the patient using a bag and mask. If an experienced operator has used a particular method of laryngoscopy, such as direct laryngoscopy or video laryngoscopy, for three attempts without success, the likelihood of success with further attempts is minimal. The airway must be recognized as a failed airway and managed as such using the failed airway algorithm. If there have been fewer than three unsuccessful attempts at intubation, but BMV is successful, then it is appropriate to attempt orotracheal intubation again, provided the oxygen saturation is maintained and the operator can identify an element of the laryngoscopy that can be improved (e.g., patient positioning, longer blade). Similarly, if the initial attempts were made by an inexperienced operator, such as a trainee, and the patient is adequately oxygenated, then it is appropriate to reattempt oral intubation until three attempts by an experienced operator have been unsuccessful. Rarely, a fourth attempt at laryngoscopy may be appropriate before declaring a failed airway. This most often occurs when the operator identifies a particular strategy for success (e.g., using a smaller diameter endotracheal tube or switching to a greatly oversized blade) during the third unsuccessful attempt. Similarly, it is possible that an experienced operator will recognize on the very first attempt that further attempts at orotracheal intubation will not be successful. In such cases, provided that the patient has been optimally positioned for intubation, good relaxation has been achieved, the BURP (see Chapter 6) or other external laryngeal maneuvers have been used, and the operator is convinced that further attempts at laryngoscopy would be futile, the airway should be immediately regarded as a failed airway and the failed airway algorithm initiated.
It is not essential to make three laryngoscopic attempts before labeling an airway as failed, but three failed attempts by an experienced operator should always be considered a failed airway, unless the laryngoscopist identifies a particular opportunity for success during the last attempt.
The Crash Airway Algorithm
Entering the crash airway algorithm (Fig. 2-3) indicates that one has identified an unconscious, unresponsive patient with immediate need for airway management. It is assumed throughout that BMV with high flow oxygen is occurring as preparations are made to intubate.
· Critical action: Intubate immediately: The first step in the crash algorithm is to attempt oral intubation immediately by direct, video, or FO laryngoscopy without pharmacological assist. In these patient circumstances, direct oral intubation has success rates comparable to RSI, presumably because the patients have flaccid musculature and are unresponsive in a manner similar to that achieved by RSI.
· Key question 1: Was intubation successful? If yes, carry on with postintubation management and general resuscitation. If intubation was not successful, resume BMV and proceed to the next step.
· Key question 2: Is bag-mask oxygenation adequate? If oxygenation using a bag and mask is judged to be successful, then further attempts at oral intubation are possible. If BMV is unsuccessful in the context of a single failed oral intubation attempt with a crash airway, then a failed airway is present. One further attempt at intubation may be rapidly tried, but no more than one, because intubation has failed, and the failure of BMV places the patient in serious and immediate jeopardy. This is a CICO failed airway, analogous to that described previously. Exit here and proceed directly to the failed airway algorithm (Fig. 2-5).
Adequacy of bag-mask oxygenation with a crash airway is usually not determined by pulse oximetry, but by assessment of chest rise and the feel of the bag (as it reflects patency of the airway, delivered tidal volume, airway resistance, and pulmonary compliance).
· Critical action: Administer succinylcholine 2 mg/kg intravenous push: If intubation is not successful, it is reasonable to assume that the patient has residual muscle tone and is not optimally relaxed. The dose of succinylcholine is increased here because these patients often have severe circulatory compromise, impairing the distribution and rapidity of the onset of succinylcholine. BMV is continued for 60 seconds to allow the succinylcholine to distribute. Remember, it is oxygen the patient requires most, not the endotracheal tube. From this point onward, the crash airway algorithm is virtually identical to the corresponding portion of the main airway algorithm, with the exception that the patient has not been adequately preoxygenated, and pulse oximetry is generally incapable of accurately reflecting the state of oxygenation in the crash airway patient. The sequence and rationale, however, are identical from this point on.
|
|
|
Figure 2-3 • Crash Airway Algorithm. The portion at the bottom is essentially identical to the corresponding portion of the main emergency airway algorithm. © 2008 The Difficult Airway Course: Emergency. |
· Critical action: Attempt intubation: After allowing time for the succinylcholine to circulate, another attempt is made at oral intubation.
· Key question 3: Was the intubation successful? If intubation is achieved, then proceed to postintubation management. If not, another attempt is indicated if oxygenation is maintained.
· Key question 4: Is oxygenation adequate? If oxygenation cannot be maintained at any time, the airway becomes a CICO failed airway, requiring implementation of the failed airway algorithm.
· Key question 5: Have there been three or more attempts at intubation by an experienced operator? If the answer to this question is “yes,” then consistent with the previous definition, the situation represents a failed airway. If fewer than three attempts have been made by an experienced operator, then a repeated attempt at oral intubation is justified and one cycles through another intubation attempt. Crash airway patients can be anticipated to experience rapid desaturation, so after each unsuccessful intubation attempt, as defined previously, the patient should receive BMV, and this ventilation must be effective.
If succinylcholine is administered to a crash patient, count the subsequent intubation attempt as attempt 1.
The Difficult Airway Algorithm
Assessment and management of the difficult airway is discussed in detail in Chapter 7. This algorithm (Fig. 2-4) represents the clinical approach that should be used in the event of an anticipated difficult airway.
· Critical action: Call for assistance: The “call for assistance” box is linked as a dotted line because this is an optional step, dependent on the particular clinical circumstances, skill of the airway manager, available equipment and resources, and availability of additional personnel. Assistance might include personnel, special airway equipment, or both.
· Key question 1: Is there adequate time? In the context of the difficult airway, oxygen is time. If ventilation and oxygenation are adequate and oxygen saturation can be maintained over 90%, then a careful assessment and a methodical, planned approach can be undertaken, even if significant preparation time is required. However, if oxygenation is inadequate, then additional oxygenation or BMV is initiated. If oxygenation cannot be maintained, the situation is equivalent to a “can't intubate (the identified difficult airway is a surrogate for can't intubate), can't oxygenate (adequate oxygenation saturation cannot be achieved)” failed airway. Move immediately to the failed airway algorithm. Certain difficult airway patients will have chronic pulmonary disease, for example, and may not be able to reach oxygen saturation of 90%, but can be kept stable and viable at, say, 86%. Whether to call this case a failed airway is a matter of judgment, but if a decision is made to proceed down the difficult airway algorithm rather than switching to the failed airway algorithm, it is essential to be aware that in cases such as this desaturation will occur rapidly during intubation attempts (see Chapter 3) and to be vigilant with respect to hypoxemia.
|
|
|
Figure 2-4 • Difficult Airway Algorithm. BMV, bag-mask ventilation; EGD, extra-glottic device; DL, direct laryngoscopy; FO, fiberoptic method; VL, video laryngoscopy; ILMA, intubating laryngeal mask; BNTI, blind nasotracheal intubation. *RSI may require a double set-up. See text for details. †if not used for awake laryngoscopy. © 2008 The Difficult Airway Course: Emergency. |
· Key question 2: Despite the presence of the difficult airway, is RSI indicated? Because we have identified that the patient is adequately oxygenated, the next step is to consider RSI. This decision hinges on two key factors.
The first, and most important, factor is whether one predicts with confidence that gas exchange can be maintained by BMV or the use of some other adjunct (e.g., an EGD [see Chapter 10]) if a neuromuscular blocking drug is administered rendering the patient paralyzed and apneic. This answer may already be known if BMV has been required to maintain the patient's oxygenation. If the patient has been breathing spontaneously and oxygenating adequately to this point, BMV may have not been attempted. Nonetheless, it is crucial that one performs an evaluation as to whether BMV or an EGD is likely to be successful because this is a virtually essential prerequisite for RSI. The assessment of a patient with respect to predicting difficult BMV and EGD use is described in Chapter 7. In some cases, it may be desirable to attempt a trial of BMV, but this approach does not reliably predict the ability to bag-mask ventilate the patient after paralysis.
Second, if BMV or EGD is predicted to be successful, then the next consideration is whether intubation is reasonably likely to be successful, despite the difficult airway attributes. In reality, many patients with identified difficult airways undergo successful emergency intubation employing RSI, so if there is a reasonable likelihood of success with oral intubation, despite the difficult airway, then RSI may be undertaken. Remember, this is predicated on the fact that one has already judged that gas exchange (BMV or EGD) will be successful following neuromuscular blockade. In some cases, the RSI may be done using a “double setup,” in which the patient is evaluated for difficult cricothyrotomy (see Chapter 7) and prepared (i.e., landmarks identified, skin prepped) for cricothyrotomy, and the surgical instruments are open and ready before the RSI is initiated. In most cases, however, when RSI is undertaken despite identification of difficult airway attributes, appropriate care during the technique and planning related to the particular difficulties present will result in success.
To reiterate these two fundamental principles, if gas exchange employing BMV or EGD is not confidently assured of success in the context of difficult intubation, or if the chance of successful oral intubation is felt to be poor, then RSI is not recommended.
Rapid sequence intubation is often both safe and effective even in a patient with an identified difficult airway, but identifying the difficult airway in advance permits careful planning and use of a double setup when indicated.
· Critical action: Perform “awake” laryngoscopy: Just as RSI is the cornerstone of emergency airway management overall, “awake” laryngoscopy is the cornerstone of difficult airway management. The goal of this maneuver is to gain a high degree of confidence that should one induce and paralyze a patient, the airway can be secured. Or, alternatively, the airway can be secured during the “awake look.” This technique, which is discussed in detail in Chapter 8, requires moderate to deep sedation of the patient, similar to that used for painful procedures, and the liberal use of local anesthesia (usually topical) to permit laryngoscopy without inducing and paralyzing the patient. The principle here is that the patient is awake enough to maintain the airway and effective spontaneous ventilation, but sufficiently obtunded to tolerate the awake look procedure. Thus, strictly speaking, “awake” is somewhat of a misnomer. The laryngoscopy can be done with a standard laryngoscope, flexible FO scope, video laryngoscope (e.g., the Glidescope or the Storz Videolaryngoscope) or a semirigid FO intubating stylet, such as the Bonfils or the Shikani Optical Stylet. These devices are discussed in detail in Chapters 12 to 14. Two possible outcomes are possible from this awake examination. First, the glottis may be adequately visualized, informing the operator that oral intubation using that device will succeed. If the difficult airway is static (i.e., chronic, such as with ankylosing spondylitis), then the best approach might be to proceed with RSI, now that it is known that the trachea can be intubated, using that same device. If, however, the difficult airway is dynamic (i.e., acute, as in smoke inhalation or angioedema), then it is likely better to proceed directly with intubation during this awake laryngoscopy, rather than to back out and perform RSI. This decision is predicated on the possibility that the airway might deteriorate further in the intervening time, arguing in favor of immediate intubation during the awake examination, rather than assuming that the glottis will be visualized with equal ease a few minutes later during an RSI. Intervening deterioration, possibly contributed to by the laryngoscopy itself, might make a subsequent laryngoscopy more difficult or even impossible (see Chapter 8). The second possible outcome during the awake laryngoscopic examination is that the glottis is not adequately visualized to permit intubation. In this case, the examination has confirmed the suspected difficult intubation and reinforced the decision to avoid neuromuscular paralysis. A failed airway has been avoided and several options remain. Oxygenation should be maintained as necessary at this point.
Awake laryngoscopy is the cornerstone of difficult airway management when rapid sequence intubation is not believed to be sufficiently likely to result in successful intubation.
Although the awake look is the crucial step in management of the difficult airway, it is not infallible. In a very small number of patients, an awake look may provide a better view of the glottic structures than is visible after the administration of a neuromuscular blocking drug. Thus, although the likelihood that the glottis will be less well seen after paralysis than during the awake look is remote, it is not unheard of, and the airway manager must always be prepared for this rare eventuality.
· Critical action: Select an alternative airway approach: At this point, we have clarified that we have a patient with difficult airway attributes, who has proven to be a poor candidate for laryngoscopy, and thus is inappropriate for RSI. There are a number of options available here. If the awake laryngoscopy was done using a direct laryngoscope, a video or FO laryngoscopy is likely to provide a superior view of the glottis. The main fallback method for the difficult airway is cricothyrotomy (open or Seldinger technique), but the patient may be amenable to an extraglottic airway that facilitates intubation, i.e. one of the intubating laryngeal mask airways (ILMAs). In highly select cases, blind nasotracheal intubation may be possible, but requires an anatomically intact and normal upper airway. The lighted stylet can be used, either with or without an ILMA for some patients, but is limited by obesity and dark skin pigmentation, and the fact that profound topical anesthesia is needed. The choice of which of these to use will depend on the operator's experience, available equipment, the particular difficult airway attributes the patient possesses, and the urgency of the intubation. The devices and techniques are described in Section 2 of this book. Whichever technique is used, the goal is to place a cuffed endotracheal tube in the trachea, so any device that does not result in an intubated, protected airway should not be used.
The Failed Airway Algorithm
At several points in the preceding algorithms, it may be determined that airway management has failed. The definition of the failed airway (see previous discussion in this chapter and in Chapter 7) is based on one of two criteria being satisfied: (a) a failure of an intubation attempt in a patient for whom oxygenation cannot be adequately maintained with a bag and mask, or (b) three unsuccessful intubation attempts by an experienced operator and adequate oxygenation. Unlike the difficult airway, where the standard of care dictates the placement of a cuffed endotracheal tube in the trachea providing a definitive, protected airway, the failed airway calls for action to provide emergency oxygenation sufficient to prevent patient morbidity (especially hypoxic brain injury) by whatever means possible, until a definitive airway can be secured (Fig. 2-5). Thus, the devices considered for the failed airway are somewhat different from, but inclusive of, the devices used for the difficult airway (see Chapter 7). When a failed airway has been determined to occur, the response is guided by whether bag-mask oxygenation is adequate.
· Critical action: Call for assistance: As is the case with the difficult airway, it is best to call for any available and necessary assistance as soon as a failed airway is identified. Again, this action may be a stat consult to emergency medicine; anesthesia; surgery; or an ear, nose, and throat specialist, or it may require a call for special equipment or a respiratory therapist. In the prehospital setting, the consult may be with a second paramedic or other available skilled personnel.
|
|
|
Figure 2-5 • Failed Airway Algorithm. © 2008 The Difficult Airway Course: Emergency. |
· Key question 1: Is oxygenation adequate? As is the case for the difficult airway, this question addresses the time available for a rescue airway. If the patient is a failed airway because of three failed attempts by an experienced operator, in most cases, oxygen saturation will be adequate, and there is time to consider various approaches. If, however, the failed airway is because of a CICO situation, then there is little time left before cerebral hypoxia will result in permanent deficit, and immediate cricothyrotomy is indicated. There may be rare circumstances when cricothyrotomy is contraindicated, for example, by a large hematoma across the anterior neck. Even in such cases, however, the contraindications are relative, and cricothyrotomy remains the first consideration, unless it is the opinion of the operator that cricothyrotomy would not be possible in the particular circumstance at hand. The only partial exception to the rule that a CICO situation mandates immediate cricothyrotomy as the first rescue step is when the operator makes a single attempt to insert a rapidly placed extraglottic airway device, simultaneously with the preparation for a cricothyrotomy. In other words, when the attempt with this alternative device is in parallel with, and not instead of, preparation for immediate cricothyrotomy, it may be prudent and reasonable to attempt a single placement of a rapid, reliable rescue device, which, if successful, converts the CICO situation into a can't intubate, can oxygenate situation, allowing time for consideration of a number of different approaches to securing the airway.
Can't intubate, can't oxygenate = cricothyrotomy in the vast majority of circumstances!
· Critical action: Achieve an airway using an FO method, video laryngoscopy, an extraglottic device, a lighted stylet, or cricothyrotomy. In the can't intubate, but can oxygenate situation, various devices are available to provide an airway, and most also provide some degree of airway protection. In addition to FO intubation and the lighted stylet, both of which establish a cuffed endotracheal in the trachea, the ILMAs have a high likelihood of providing effective ventilation and will usually permit intubation through the device. Other extraglottic airways vary in their ability to facilitate endotracheal intubation (see Chapter 10). In practical terms, if the patient is able to be successfully ventilated and oxygenated with a bag and mask, the preference is to use a device that places a cuffed endotracheal tube in the trachea (e.g., FO or video method, lighted stylet, ILMA) rather than a nondefinitive temporizing device (e.g., Combitube). Cricothyrotomy always remains the final common pathway if other measures are not successful, or if the patient's oxygenation becomes compromised.
· Key question 3: Does the device used result in a definitive airway? If the device used results in a definitive airway (i.e., a cuffed endotracheal tube in the trachea), then one can move on to postintubation management. If an EGD has been used, such as a Combitube or an ILMA, without successful intubation, then arrangements must still be made to provide a definitive airway. A definitive airway may be provided in the operating room, intensive care unit, or emergency department (ED), once the necessary personnel and equipment are available. Until then, constant surveillance is required to ensure that the airway, as placed, continues to provide adequate oxygenation, with cricothyrotomy always available as a backup.
Conclusions
These algorithms are significantly updated and simplified from those in the previous editions of this book. They represent our best thinking regarding a recommended approach to emergency airway management. The algorithms are intended as guidelines only. Individual decision making, clinical circumstances, skill of the physician, and available resources will determine the final, best approach to airway management in any individual case. Understanding the fundamental concepts of the difficult and failed airway; identification, in advance, of the difficult airway; recognition of the crash airway; and the use of RSI as the airway management method of choice for most emergency intubations, however, will result in successful airway management with minimal morbidity.
Evidence
1. Is RSI superior to sedation alone for intubation? Blinded anesthesia studies comparing intubating conditions and success under conditions of deep general anesthesia with various neuromuscular blocking agents have included a control group that received no neuromuscular blocking agent. Despite the deep level of anesthesia, much deeper than that existing in the ED during conditions of RSI, the intubating conditions in the no neuromuscular blockade group were so inferior that both authors subsequently advised against including such a control group in the future (1,2). Recently, 70% of patients undergoing general anesthesia with fentanyl 2 µg/kg and propofol 2 mg/kg, but without succinylcholine, demonstrated unacceptable intubating conditions with vocal cords either adducted or closing, excessive patient movement, or sustained coughing, compared to only 2% of patients receiving 1.0 mg/kg of succinylcholine (3). Increasing the dose of succinylcholine from 0.5 to 1.5 mg/kg increases the incidence of excellent intubating conditions from 56% to 85% (4). In two other studies, 19 of 20 and 10 of 10 patients had poor intubating conditions or impossible intubation when neuromuscular blocking agents were not used, despite appropriate doses of anesthetic agents (5,6). In a study of 49 patients in an air medical service, Bozeman et al. (7) compared intubations done with etomidate alone to those done after introduction of an RSI protocol and reported good or acceptable intubating conditions in 79% of RSI patients versus 13% intubated using etomidate alone. Glottic views and intubation difficult scoring were both significantly superior in the RSI group. Intubation success rates were 92% for RSI versus 25% for etomidate alone (7).
2. What is the success rate of RSI for emergency intubations? Sakles et al. (8) prospectively studied 610 ED intubations from one high-volume center. In this series, RSI was used in 515 (84%), with a success rate of 98.9%; 7 patients underwent cricothyrotomy. The overall complication rate was 8.0%; 95% confidence interval, 6% to 11% (8). Tayal et al. (9) reported on RSI in 417 of 596 (70%) critically ill patients requiring emergent intubation. Intubations by residents and attendings were successfully completed within two attempts in 97% of the patients. Major immediate adverse events (hypotension, hypoxemia, dysrhythmia) were uncommon (1.4%), and there was no death attributable to RSI. Initial reports from the National Emergency Airway Registry project, a multicenter study of ED intubations that has now gathered data on more than 15,000 ED intubations, show very high success rates with a low incidence of adverse events. Sivilotti et al. (10) reported on 3,407 ED intubations, of which 2,380 (70%) were intubated using RSI. Ninety-five percent of the patients were intubated in the first two laryngoscopic attempts, and 98.5% were successfully intubated without requiring a second (rescue) method. Emergency medicine physicians performed the initial intubation in 2,118 (89%) cases (10). Similar success is reported for pediatric intubations in the NEAR I project (11). RSI is the method of choice for most intubations and is also the most common rescue maneuver when another intubation method fails (12). Sagarin et al. (13) reported on 7,498 intubations at 31 centers in the NEAR project. The first intubator was successful in 90% of intubations, and intubation success improved with year of residency training in emergency medicine. Cricothyrotomy was required in less than 1% of cases (13). Graham et al. (14) studied RSIs in seven hospitals in Scotland, and reported Cormack-Lehane grades 1 or 2 in 92% of cases. Zukerbraun et al. (15) reported 100% success in 77 consecutive pediatric patients undergoing RSI at a single center. In a comparison of etomidate and midazolam for prehospital RSI, Swanson et al. (16) found success rates of more than 98%, regardless of which sedative agent was used.
3. What is the evidence supporting the alternate airway devices as rescue devices? Parr et al. (17) reported on the use of the ILMA for two anesthesia patients with failed oral intubation due to impossible laryngoscopic visualization of the glottis. Both patients were successfully ventilated with a bag and mask, had the ILMA placed, then were intubated through the ILMA. One hundred percent of 254 patients with identified difficult airways were successfully ventilated with the ILMA, and 96.5% of those on whom intubation was attempted (n = 200) were successfully intubated within five attempts through the ILMA (18). One hundred patients with identified difficult airways were randomized to undergo intubation either using an ILMA or with an FO scope. Success required intubation within three attempts, and success rates were 45/49 (92%) for FO and 48/51 (94%) for ILMA. When the first method of intubation failed (seven patients total), all patients were successfully intubated within two attempts using the other method (19). Both the Combitube and the LMA appear to be easy to place and ventilate with, even by inexperienced personnel (20). These devices are discussed in more detail in the relevant chapters.
4. Evidence for the algorithms. Unfortunately, there are no systematized data supporting the algorithmic approach presented in this chapter. The algorithms are the result of careful review of the American Society of Anesthesiologists difficult airway algorithm and composite knowledge and experience of the editors, who functioned as an expert panel in this regard. There has not been, and likely never will be, a study comparing, for example, the outcomes of cricothyrotomy versus alternate airway devices in the CICO situation, and clearly randomization of such patients is not ethical. Thus, the algorithms are derived from a rational body of knowledge (described previously) and represent a recommended approach, but cannot be considered to be scientifically proven as the only or even necessarily the best way to approach any one clinical problem or patient. Rather, they are designed to help guide a consistent approach to both common and uncommon airway management situations.
References
1. Cicala R, Westbrook L. An alternative method of paralysis for rapid-sequence induction. Anesthesiology 1988;69:983–986.
2. Baumgarten RK, Carter CE, Reynolds WJ, et al. Priming with nondepolarizing relaxants for rapid tracheal intubation: a double-blind evaluation. Can J Anaesth 1988;35:5–11.
3. Naguib M, Samarkandi A, Riad W, et al. Optimal dose of succinylcholine revisited. Anesthesiology 2003;99:1045–1049.
4. Stewart KG, Hopkins PM, Dean SG. Comparison of high and low doses of suxamethonium. Anaesthesia 1991;46:833–836.
5. Kahwaji R, Bevan DR, Bikhazi G, et al. Dose-ranging study in younger adult and elderly patients of ORG 9487, a new rapid-onset, short duration muscle relaxant. Anesth Analg 1997;84:1011–1018.
6. Pino RM, Ali HH, Denman WT, et al. A comparison of the intubation conditions between mivacurium and rocuronium during balanced anesthesia. Anesthesiology 1998;88:673–678.
7. Bozeman WP, Kleiner DM, Huggett V. A comparison of rapid sequence intubation and etomidate-only intubation in the prehospital air medical setting. Prehosp Emerg Care 2006;10:8–13.
8. Sakles JC, Laurin EG, Rantapaa AA, et al. Airway management in the emergency department: a one-year study of 610 tracheal intubations. Ann Emerg Med 1998;31:325–332.
9. Tayal VS, Riggs RW, Marx JA, et al. Rapid-sequence intubation at an emergency medicine residency: success rate and adverse events during a two-year period. Acad Emerg Med 1999;6:31–37.
10. Sivilotti MA, Filbin MR, Murray HE, et al., on behalf of the NEAR investigators. Does the sedative agent facilitate emergency rapid-sequence intubation? Acad Emerg Med 2003;10:612–620.
11. Sagarin MJ, Chiang V, Sakles JC, et al., on behalf of the NEAR investigators. Rapid sequence intubation for pediatric emergency airway management. Pediatr Emerg Care 2002;18:417–423.
12. Bair AE, Filbin MR, Kulkami R, et al., on behalf of the NEAR investigators. Failed intubation in the emergency department: analysis of prevalence, rescue techniques, and personnel. J Emerg Med 2002;23:131–140.
13. Sagarin MS, Barton ED, Chng YM, et al. Airway management by U.S. and Canadian emergency medicine residents: a multicenter analysis of more than 6,000 endotracheal intubation attempts. Ann Emerg Med 2005;46:328–336.
14. Graham CA, Oglesby AJ, Beard D, et al. Laryngoscopic views during rapid sequence intubation in the emergency department. Can J Emerg Med 2004;6:416–420.
15. Zuckerbraun NS, Pitetti RD, Herr SM, et al. Use of etomidate as an induction agent for rapid sequence intubation in a pediatric emergency department. Acad Emerg Med 2006;13: 602–609.
16. Swanson ER, Fosnocht DE, Jensen SC. Comparison of etomidate and midazolam for prehospital rapid-sequence intubation. Prehosp Emerg Care 2004;8:273–279.
17. Parr MJA, Gregory M, Baskett PJ, et al. The intubating laryngeal mask: use in failed and difficult intubations. Anaesthesia 1998;53:343–348.
18. Ferson DZ, Rosenblatt WH, Johansen MJ, et al. Use of the intubating LMA-Fastrach in 254 patients with difficult airways. Anesthesiology 2001;95:1175–1181.
19. Langeron O, Semjen F, Bourgain JL, et al. Comparison of the intubating laryngeal mask airway with the fiberoptic intubation in anticipated difficult airway management. Anesthesiology 2001;94:968–972.
20. Yardy N. A comparison of two airway aids for emergency use by unskilled personnel. The Combitube and laryngeal mask. Anaesthesia 1999;54:179–183.