Overview of the Genital Organs
![]() The genital organs can be classified topographically (external versus internal), functionally (Tables 14.1 and 14.2), or ontogenetically (see p. 204).
The genital organs can be classified topographically (external versus internal), functionally (Tables 14.1 and 14.2), or ontogenetically (see p. 204).

Fig. 14.1 Female genital organs
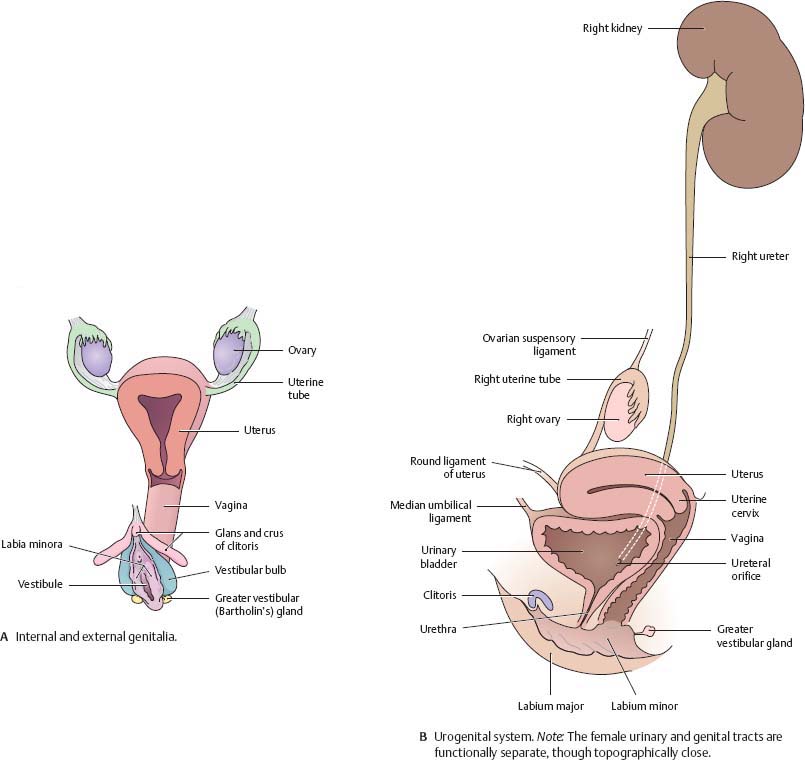
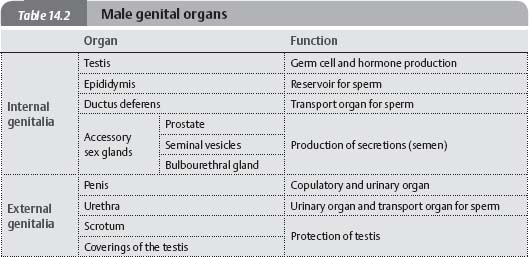
Fig. 14.2 Male genital organs

Uterus & Ovaries
Fig. 14.3 Female internal genitalia
The uterus and ovaries are suspended by the mesovarium and mesometrium (portions of the broad ligament).

Fig. 14.4 Ovary
Posterior view of the right ovary.
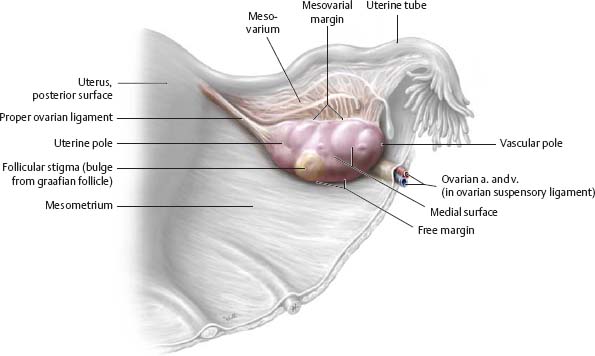
Fig. 14.5 Curvature of the uterus
Midsagittal section, left lateral view. The position of the uterus can be described in terms of flexion (![]() ) and version (
) and version (![]() ).
).
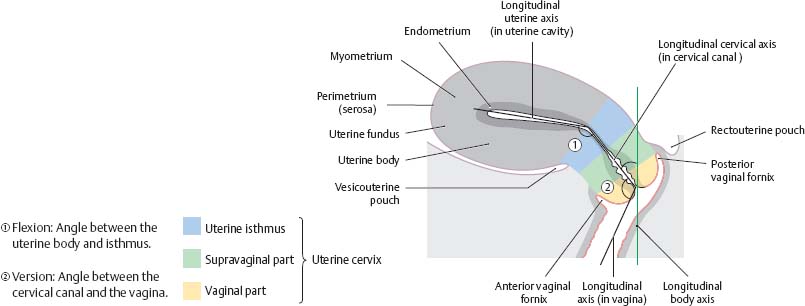
Fig. 14.6 Uterus and uterine tube

![]() Clinical
Clinical
Ectopic pregnancy
After fertilization, the ovum usually implants in the wall of the uterine cavity. However, it may become implanted at other sites (e.g., the uterine tube or even the peritoneal cavity). Tubal pregnancies, the most common type of ectopic pregnancy, pose the risk of tubal wall rupture and potentially life-threatening bleeding into the peritoneal cavity. Tubal pregnancies are promoted by adhesion of the tubal mucosa, mostly due to inflammation.
Vagina
Fig. 14.7 Location
Midsagittal section, left lateral view.

Fig. 14.8 Structure
Posteriorly angled coronal section, posterior view.

Fig. 14.9 Uterine cervix: Transverse section
Inferior view.

Fig. 14.10 Female genital organs: Coronal section
Anterior view. The vagina is both pelvic and perineal in location. It is also retroperitoneal.

Fig. 14.11 Vagina: Location in the pelvic floor
Inferior view.

Female External Genitalia
Fig. 14.12 Female external genitalia
Lithotomy position with labia minora separated.

Fig. 14.13 Vestibule and vestibular glands
Lithotomy position with labia separated.
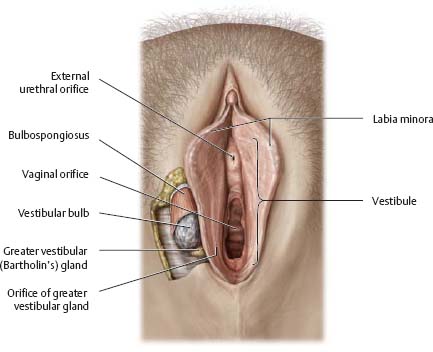
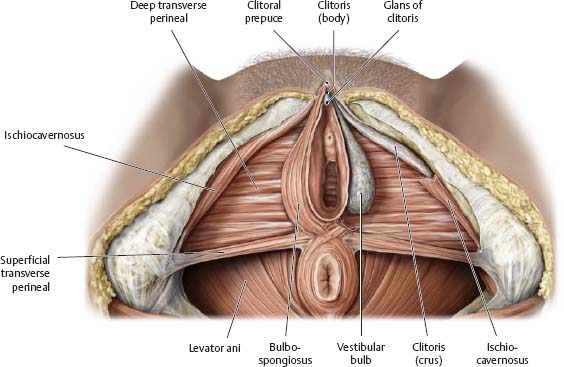
Fig. 14.14 Erectile muscles and tissue: Female
Lithotomy position. Removed: Labia, skin, and perineal membrane; erectile muscles (left side).
![]() Clinical
Clinical
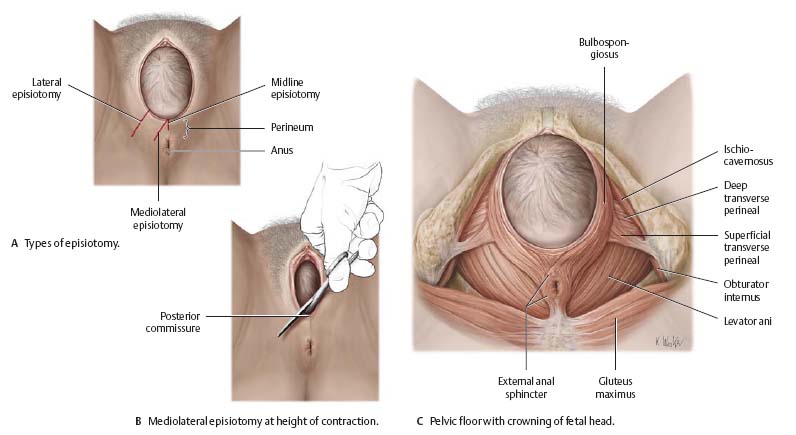
Episiotomy
Episiotomy is a common obstetric procedure used to enlarge the birth canal during the expulsive stage of labor. The procedure is generally used to expedite the delivery of a baby at risk for hypoxia during the expulsive stage. Alternately, if the perineal skin turns white (indicating diminished blood flow), there is imminent danger of perineal laceration, and an episiotomy is often performed. More lateral incisions gain more room, but they are more difficult to repair.
Neurovasculature of the Female Genitalia
Fig. 14.15 Nerves of the female perineum and genitalia

Fig. 14.16 Blood vessels of the female external genitalia
Inferior view.

Fig. 14.17 Neurovasculature of the female perineum
Lithotomy position.

Penis, Scrotum & Spermatic Cord
Fig. 14.18 Penis, scrotum, and spermatic cord
Anterior view. Removed: Skin over the scrotum and spermatic cord.
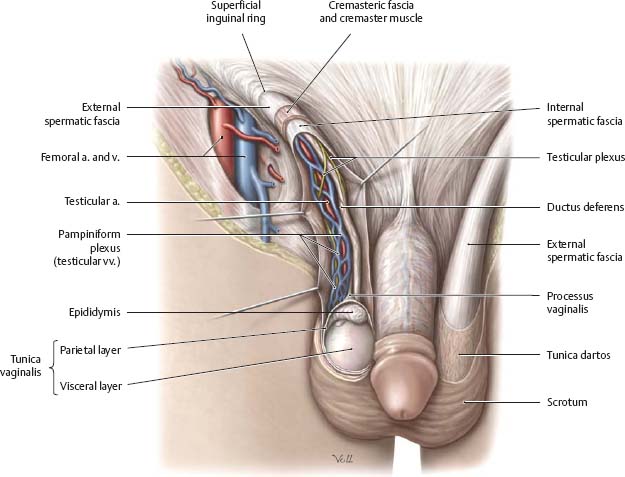
Fig. 14.19 Spermatic cord: Contents
Cross section.

Fig. 14.20 Penis

Testis & Epididymis
Fig. 14.21 Testis and epididymis
Left lateral view.



Fig. 14.22 Blood vessels of the testis
Left lateral view.

Male Accessory Sex Glands
Fig. 14.23 Accessory sex glands
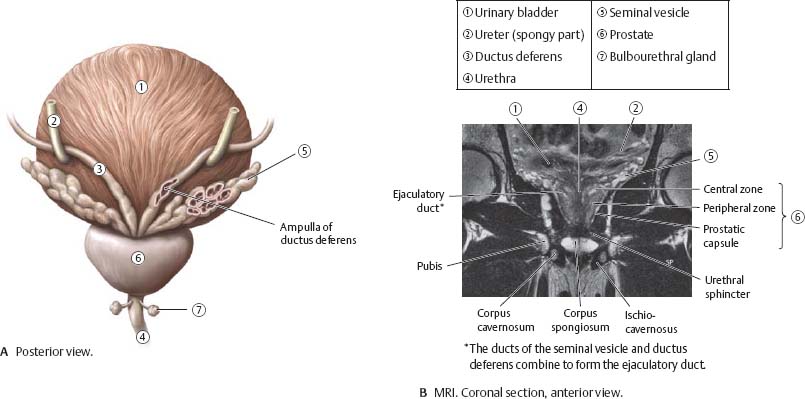
Fig. 14.24 Prostate
The prostate may be divided anatomically (top row) or clinically (bottom row).

Fig. 14.25 Prostate in situ
Sagittal section through the male pelvis, left lateral view.

![]() Clinical
Clinical
Prostatic carcinoma and hypertrophy
Prostatic carcinoma is one of the most common malignant tumors in older men, often growing at a subcapsular location in the peripheral zone of the prostate. Unlike benign prostatic hyperplasia, which begins in the central part of the gland, prostatic carcinoma does not cause urinary outflow obstruction in its early stages. Being in the peripheral zone, the tumor is palpable as a firm mass through the anterior wall of the rectum during rectal examination.

In certain prostate diseases, especially cancer, increased amounts of a protein, prostate-specific antigen or PSA, appear in the blood. This protein can be measured by a simple blood test.
Neurovasculature of the Male Genitalia
Fig. 14.26 Neurovasculature of the male genitalia
Left lateral view.

Fig. 14.27 Neurovasculature of the penis and scrotum
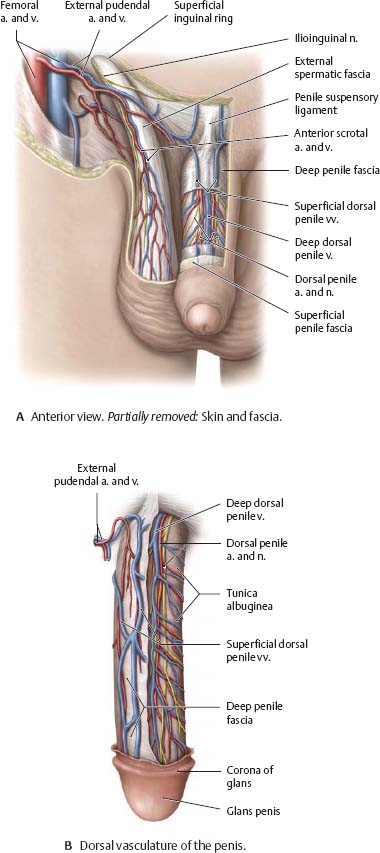
Fig. 14.28 Nerves of the male perineum and genitalia
Lithotomy position.

Fig. 14.29 Neurovasculature of the male perineum
Lithotomy position.

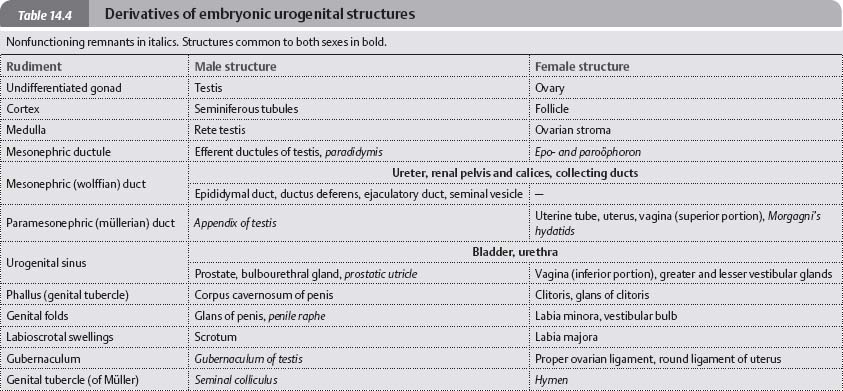
Development of the Genitalia
![]() The male and female genitalia are derived from a common gonadal primordium.
The male and female genitalia are derived from a common gonadal primordium.
Fig. 14.30 Development of the external genitalia

Fig. 14.31 Descent of the testis
Left lateral view.

Fig. 14.32 Development of the internal genitalia
Anterior view.