Autonomic Plexuses
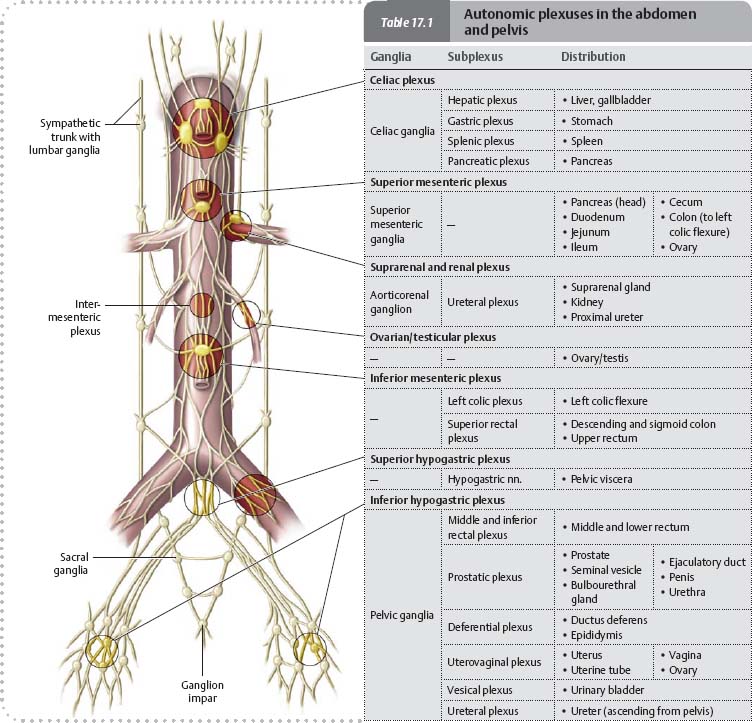
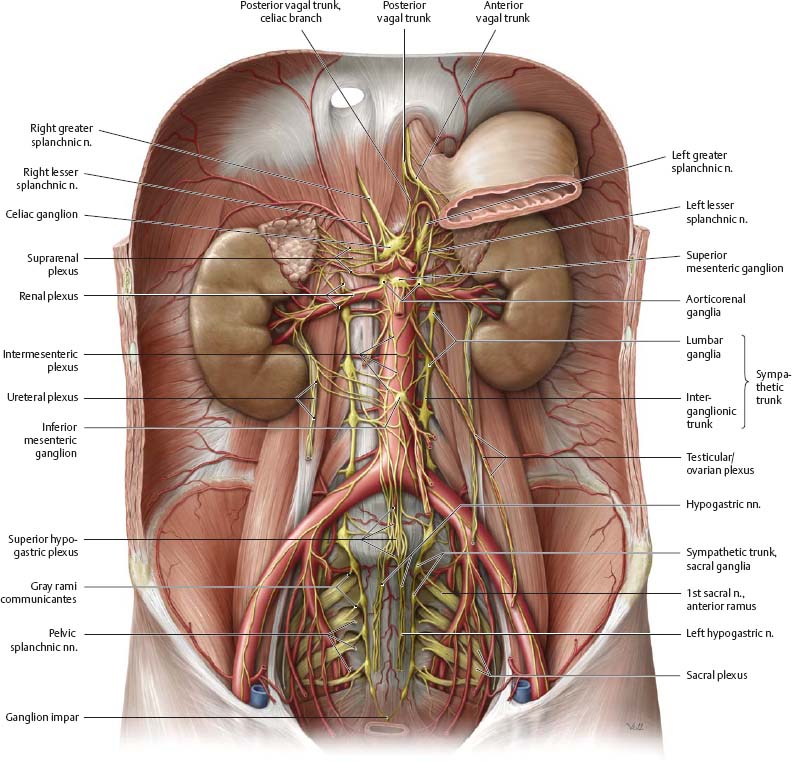
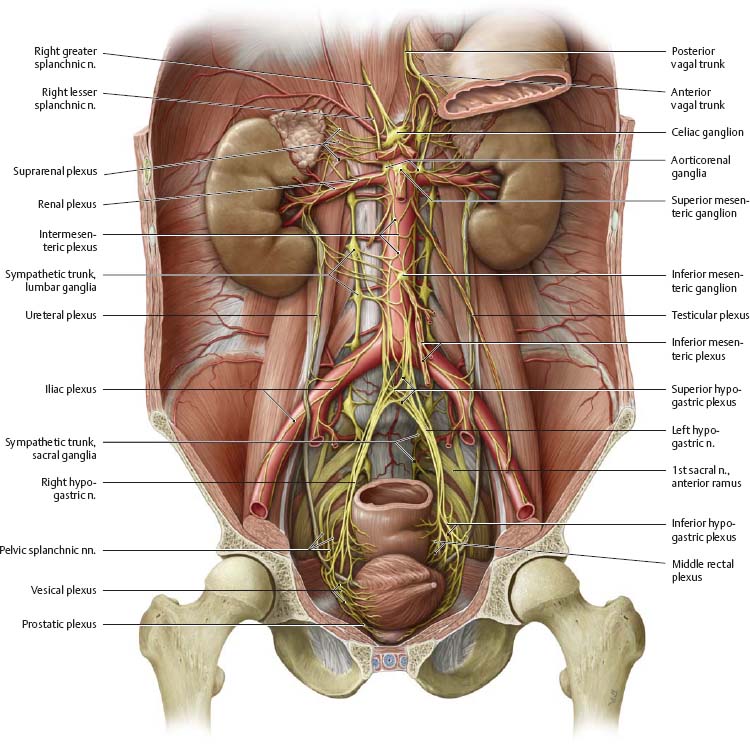
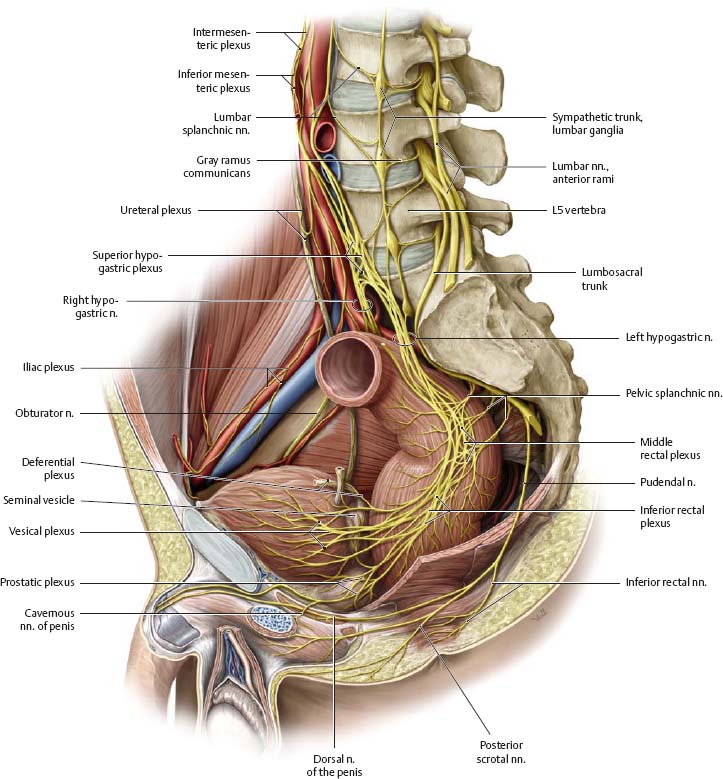
Fig. 17.1 Autonomic plexuses in the abdomen and pelvis
Anterior view of the male abdomen. Removed: Peritoneum and majority of the stomach
Innervation of the Abdominal Organs
Fig. 17.2 Innervation of the anterior abdominal organs
Anterior view. Removed: Lesser omentum, ascending colon, and parts of the transverse colon. Opened: Lesser sac. The anterior and posterior vagal trunks each produce a celiac, hepatic, and pyloric branch, and a gastric plexus. See p. 245 for schematic.
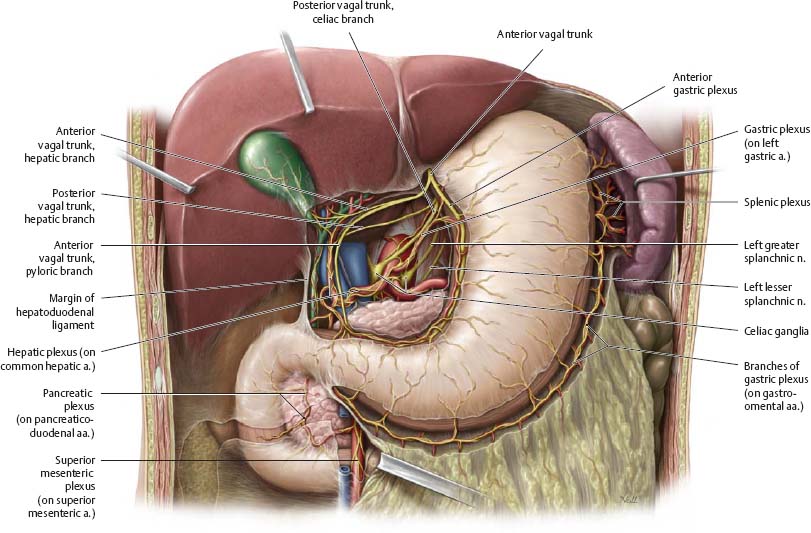
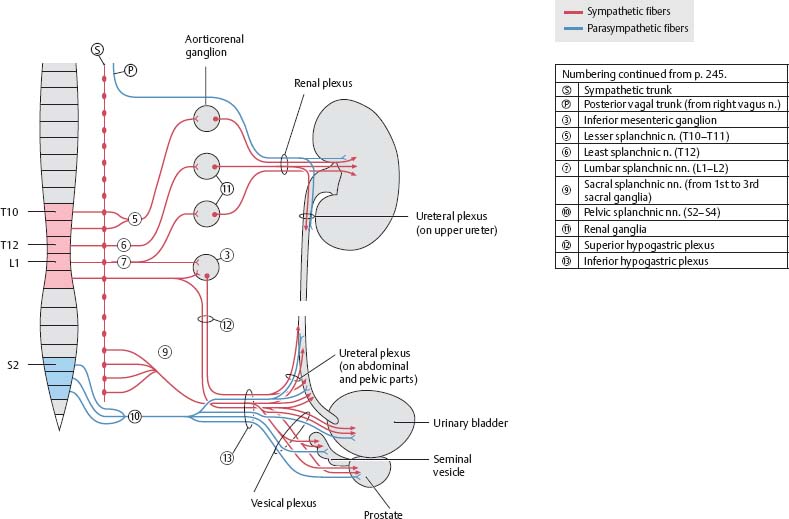
Fig. 17.3 Innervation of the urinary organs
Anterior view of the male abdomen and pelvis. Removed: Abdominal organs and peritoneum. See p. 246 for schematic.
Innervation of the Intestines
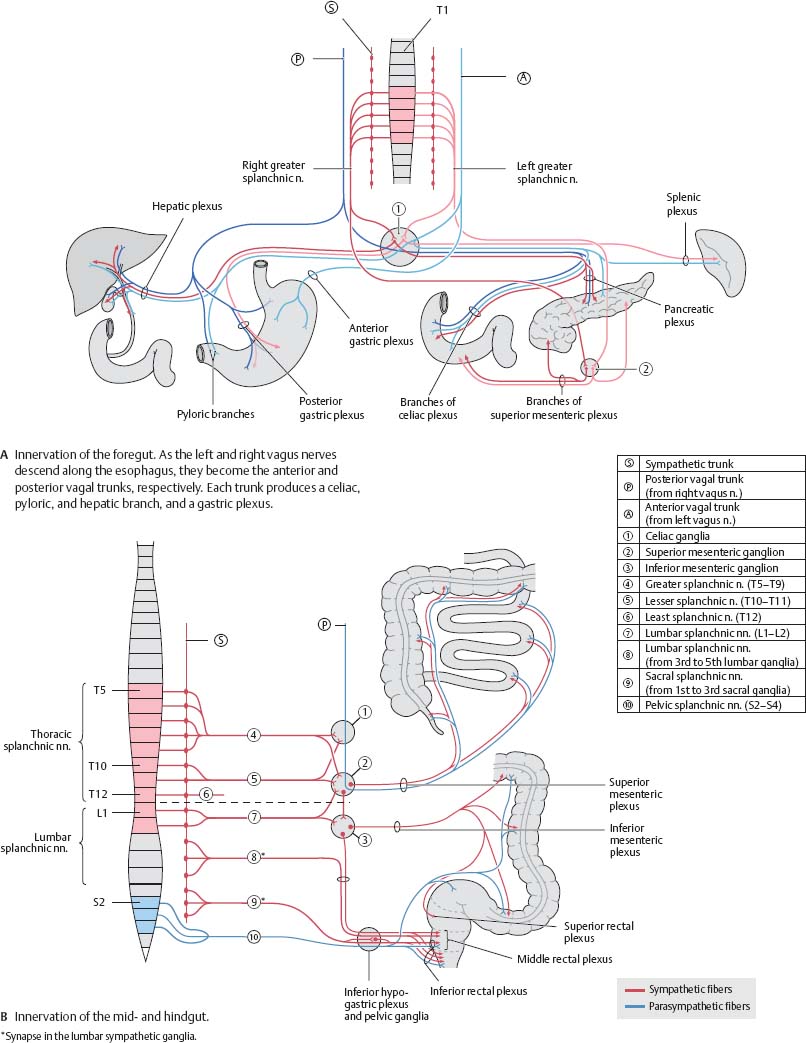
Fig. 17.4 Innervation of the small intestine
Anterior view. Partially removed: Stomach, pancreas, and transverse colon (distal part). See p. 245 for schematic.
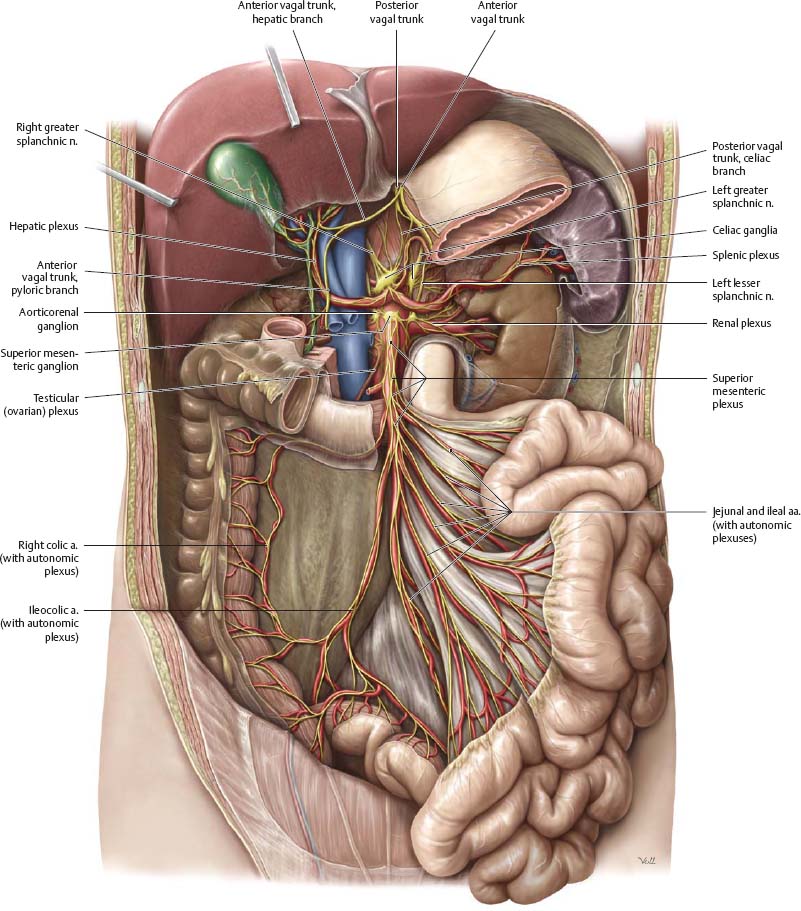
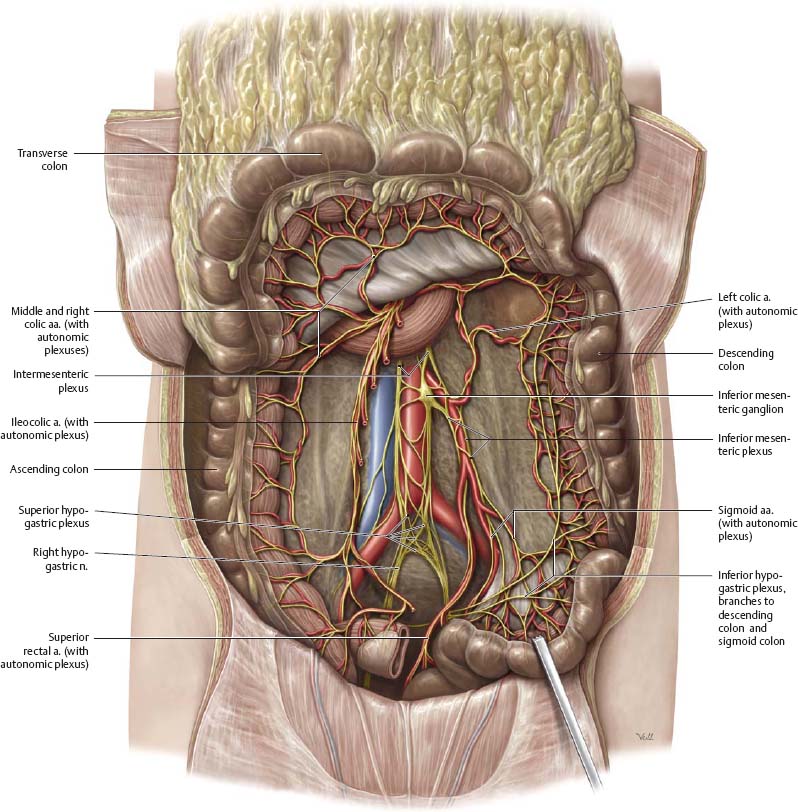
Fig. 17.5 Innervation of the large intestine
Anterior view. Removed: Jejunum and ileum. Reflected: Transverse and sigmoid colons. See p. 245 for schematic.
Innervation of the Pelvis
Fig. 17.6 Innervation of the female pelvis
Right pelvis, left lateral view. Reflected: Uterus and rectum. See p. 247 for schematic.
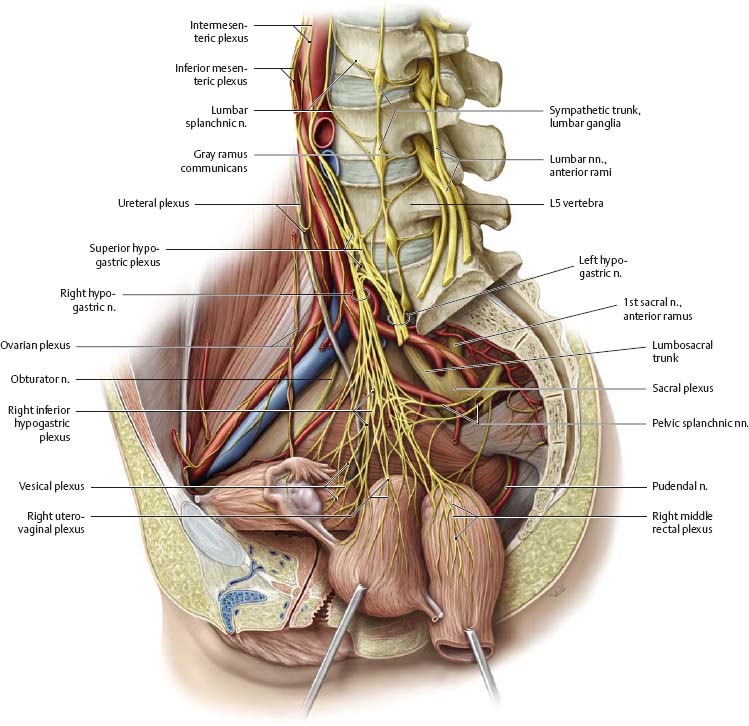
Fig. 17.7 Innervation of the male pelvis
Right pelvis, left lateral view. See p. 247 for schematic.
Autonomic Innervation: Overview
Fig. 17.8 Sympathetic and parasympathetic nervous systems in the abdomen and pelvis
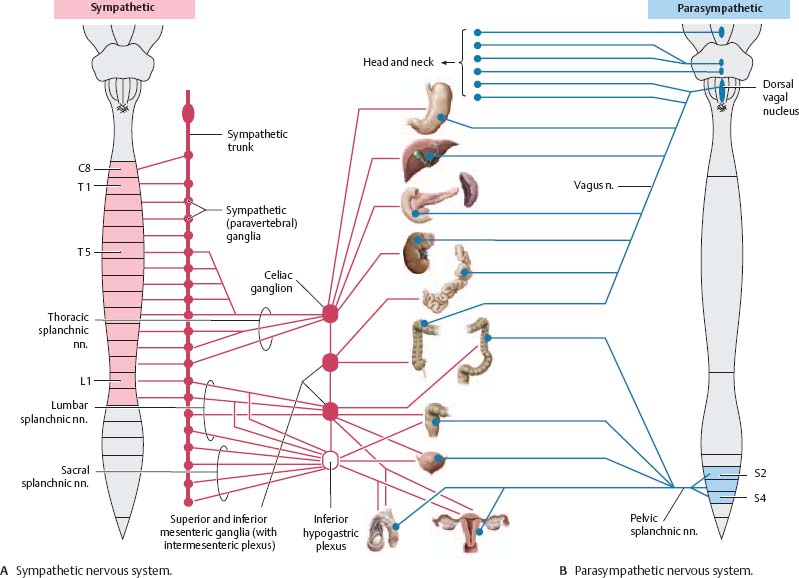
Fig. 17.9 Autonomic innervation of the intraperitoneal organs
Autonomic Innervation: Urinary & Genital Organs
Fig. 17.10 Autonomic innervation of the urinary organs
![]() Clinical
Clinical
Referred pain from the internal organs
The convergence of somatic and visceral afferent fibers to a common level of the spinal cord confuses the relationship between the perceived and actual sites of pain, a phenomenon known as referred pain. Pain impulses from a particular organ are consistently projected to the same well-defined skin area.
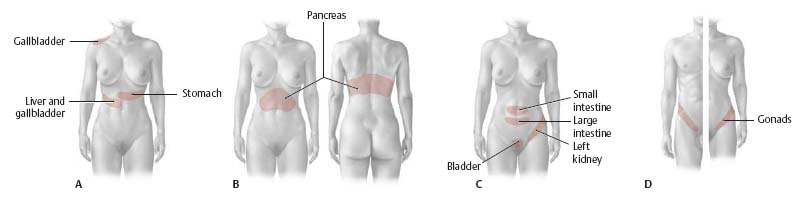
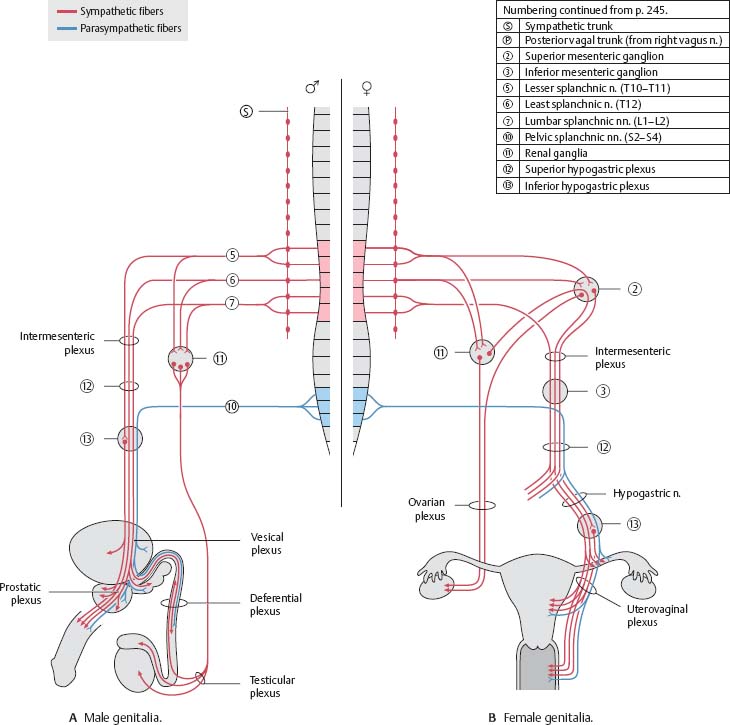
Fig. 17.11 Autonomic innervation of the genitalia