Todd A. Taylor
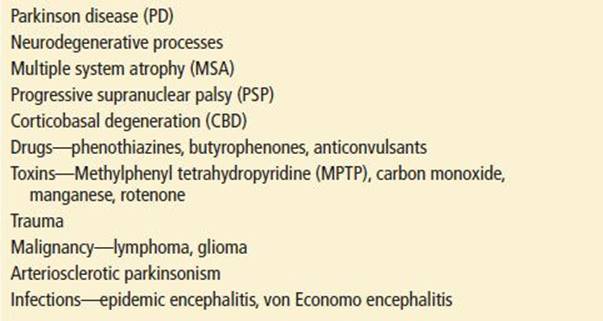
Parkinsonism, or Parkinson syndrome, is a group of progressive degenerative central nervous system disorders characterized by cardinal motor signs of bradykinesia, tremor, rigidity, and postural instability. Idiopathic Parkinson disease (PD) is the most common cause of parkinsonism and accounts for 80% of cases. Secondary parkinsonism, from a host of disparate causes, constitutes the remaining 20% (see Table 162.1).
TABLE 162.1
Causes of Parkinsonism
The incidence and prevalence of parkinsonism and PD are increasing, reflecting the aging population, and are now afflicting 1 million in America (1–3). There does not appear to be a genetic predisposition for PD when the disease begins after age 50 years, although there may be one for early-onset disease (3). PD is more common in men than in women and appears to be more common in whites than in other groups (1). Both PD and secondary parkinsonism have increased morbidity and mortality rates compared with the general population (1,4,5).
Although the precise cause and pathophysiology of PD is not known, recent studies suggest inflammation, oxidative stress, and abnormal protein accumulation leading to cell death in the substantia nigra (6–8). Profound localized depletion of the neurotransmitter dopamine in the substantia nigra is the biochemical marker for the disease (9,10). The mainstay of therapy for PD is neurotransmitter replacement in the form of levodopa or dopamine agonists. Infections (von Economo pandemic of encephalitis lethargica), toxins (the designer drug methylphenyl tetrahydropyridine [MPTP], the pesticide rotenone) (7), and medications (phenothiazines) are known causes of secondary parkinsonism (Table 162.1).
In practice, the diagnosis of parkinsonism and PD is made on clinical grounds, but the ultimate diagnosis still rests with neuropathologic confirmation at autopsy (11). Neuroimaging is typically used to rule out other causes but is unrevealing in cases of PD. PD has distinct cellular degeneration of the substantia nigra with characteristic Lewy bodies (12). The various secondary parkinsonian syndromes show etiology-specific pathologic changes in the extrapyramidal system and the cortex of the brain. Precisely how the neurochemical and pathologic changes in parkinsonism result in dysfunction of the regulation of tone and motor activity is not completely understood (5). Advanced imaging techniques such as functional magnetic resonance imaging (MRI) and positron-emission tomography are contributing to a better understanding of functional anatomy (13).
CLINICAL PRESENTATION
Patients can present to the emergency department (ED) with complaints referable to undiagnosed parkinsonism or with complications of previously diagnosed illness. Emergent interventions are rarely needed for the disease itself. However, it is important to make the diagnosis as soon as possible because effective symptomatic treatment is available, and there is the possibility of slowing disease progression.
The clinical manifestations of parkinsonism develop insidiously and gradually. The four cardinal signs are resting tremor, bradykinesia, rigidity, and gait disturbance (14). Typically some combination of these, together with a good response to levadopa therapy, is used to make the diagnosis (14). Motor deficiencies are usually asymmetric. Rigidity may be present on flexion and extension of the extremities and neck, and “cogwheel” rigidity on passive extension of the elbow or circumduction of the wrist may be noted. There are two types of rigidity in PD. The “lead pipe” rigidity is an increase in resistance to passive movement (15). Cogwheel rigidity is described as a catching sensation throughout passive range of motion (15). Early on, ambulation is generally slow; short or shuffling steps (marche à petits pas), instability, and falls occur later. The classic tremor of PD is a 3 to 6 Hz distal resting tremor that increases in periods of anxiety. An essential tremor is often confused for the resting tremor of PD. An essential tremor is an action tremor occurring during intentional motion as opposed to the resting tremor of PD. The resting tremor of PD disappears during voluntary movement (1). Monotonous speech and decreased speech volume are other early features, and there is eventual development of drooling, dysphagia, and masked facies. Sensory findings are generally absent. The presence of early dementia and psychosis (unrelated to medicines), autonomic dysfunction (orthostasis), cerebellar findings, and supranuclear gaze palsy suggest one of the secondary causes of parkinsonism (5,11).
In patients with known PD, complications of therapy or a worsening of symptoms while on therapy is often the reason for presentation to the ED. The so-called on–off phenomenon, sudden wide fluctuations in motor function, ranging in severity from dyskinesia to freezing, can be particularly troubling to patients. This is thought to correlate with fluctuating drug levels throughout the day. “Wearing off,” or loss of therapeutic effect, should prompt a reassessment of the medication regime and also confirmation that secondary parkinsonism has not been erroneously diagnosed as PD, as one of the ways to rule out PD is the nonresponse to dopamine therapy. Orthostasis, nausea, vomiting, and acute psychosis can be caused by various dopaminergic and anticholinergic agents. Differentiating disease progression from medication inadequacy or excess can be difficult but is an important part of ED management.
Other complications related to general motor disability (e.g., traumatic injuries caused by falls) are significant reasons for ED presentation. In addition, many older patients, the cohort most affected by parkinsonism, have multiple medical conditions that can be more difficult to manage in the setting of progressive parkinsonism.
DIFFERENTIAL DIAGNOSIS
The primary entities in the differential diagnosis of parkinsonism are idiopathic PD and secondary parkinsonism. To help distinguish PD from secondary parkinsonism on a clinical basis, Gelb et al. (11) have suggested specific diagnostic criteria for PD: bradykinesia, rigidity, and the asymmetric onset of resting tremor, all of which must have a substantial and sustained response to levodopa or dopamine-agonist therapy. The presence of postural instability, freezing phenomena, hallucinations, dementia, severe dysautonomia, or supranuclear gaze palsy within the first 3 years of disease presentation suggests a secondary form of parkinsonism (12). PD has a gradually progressive course; rapid progression strongly suggests another form of parkinsonism (12).
ED EVALUATION
The ED evaluation of a patient with clinical symptoms suggestive of parkinsonism consists primarily of a history and physical examination. For patients with new symptoms, clinical assessment is aimed at identifying patients with a clinical picture that is consistent with parkinsonism and parkinsonian syndromes. It should be noted that even neurologists, according to one study, make the correct diagnosis only 82% of the time (16). The focus of the emergency physician should not be to make the diagnosis but rather to recognize patients who have parkinsonism symptomatology and referring them to a neurologist. MRI is useful in the comprehensive evaluation of parkinsonism but rarely is indicated in the ED (17).
For patients previously diagnosed with parkinsonism, evaluation should focus on progression of disease, complications of medical treatment, and concomitant medical conditions.
ED MANAGEMENT
Strategies for the management of parkinsonism in the ED should be coordinated with the physician who will treat the patient for the long term.
For patients who are newly diagnosed with PD, treatment includes agents to alleviate disabling symptoms, as well as agents that are potentially neuroprotective. Table 162.2 outlines treatment options. Levodopa and dopamine agonists are the mainstay of symptomatic treatment. Levodopa, a dopamine precursor, is more commonly used for initial treatment. Carbidopa blocks the peripheral metabolism of levodopa, allowing lower doses of levodopa to be effective centrally. The levodopa–carbidopa combination drug (Sinemet) has thus become a mainstay of treatment. It is desirable to use the minimum amount of levodopa necessary to control symptoms, because the metabolism of levodopa is thought to contribute to an excess of oxyradicals in the substantia nigra, leading to further cell degeneration. For this reason, dopamine agonists are sometimes used instead of levodopa. These medications are not as effective as levodopa but avoid the associated theoretical increase in cell destruction. Moreover, limiting the dose of levodopa reduces the drug’s peripheral side effects (nausea, vomiting, and orthostasis) (10). Agents with neuroprotective effects (dopamine agonists, monomine-oxidase [MAO]-B inhibitors) are other common alternatives (6). The anticholinergic drug benzatropine is prescribed selectively for patients with tremor predominance. For those with severe disease refractory to medical management, deep-brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus has been shown to significantly improve motor symptoms, although this therapy does have inherent risks and limitations as well (18–20).
TABLE 162.2
Management of Parkinson Diseasea
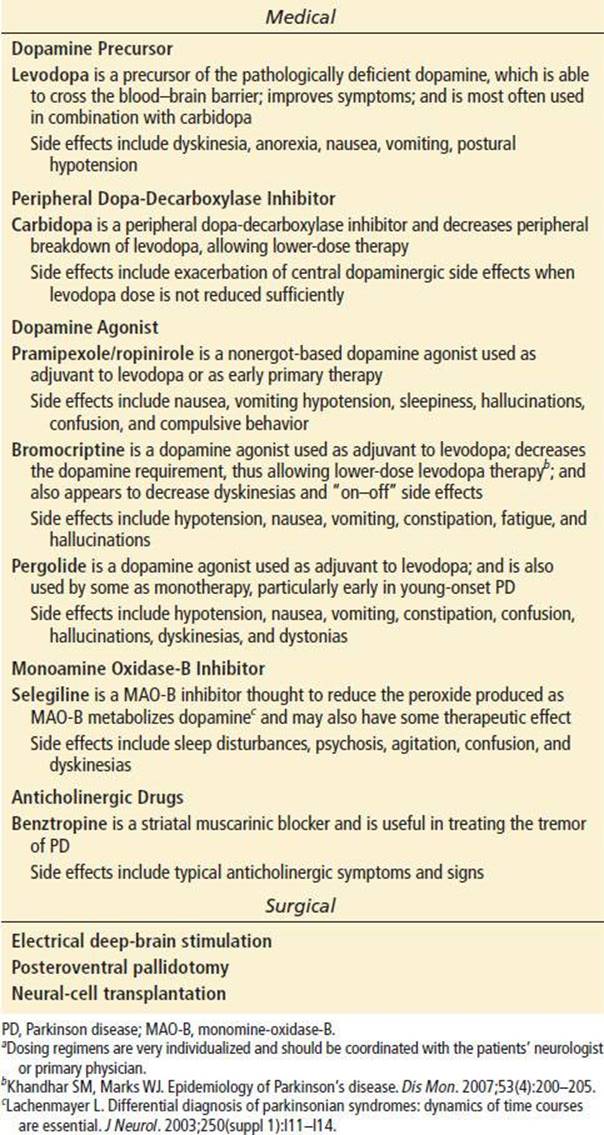
For patients with known PD, ED management is directed at recognizing the inadequacy or excess of the medication regimen and adjusting dosages accordingly. The “on–off ” phenomenon is thought to be caused by fluctuations in drug concentrations. Changing doses or dosing intervals and adding other antiparkinsonism agents should be done only after consultation with the neurologist. A sustained-release levodopa–carbidopa combination appears to reduce the total levodopa requirement, as well as variations in drug concentration (21). Medication excess may cause acute psychiatric and cognitive side effects, such as psychosis, hallucinations, delusions, agitation, and confusion. This may require a decrease in dopaminergic and anticholinergic medications and the initiation of antipsychotics (10). The peripheral side effects of excessive dopamine (nausea, vomiting, and orthostasis) can also be treated by reducing levodopa doses. There also appears to be a small chance that the discontinuation of dopaminergic therapy may cause neuroleptic malignant syndrome (NMS) (22). The symptoms of NMS closely mimic those of PD (i.e., confusion, rigidity, tremor), so the clinician should ensure that medications are continued on patients being admitted to the hospital. The treatment of NMS in this circumstance consists of administering bromocriptine and restarting the patient’s Parkinson medications. Optimizing the balance of various agents can be difficult and should be coordinated with the patient’s primary physician.
The management of the parkinsonian syndromes other than PD is generally less effective. Parkinsonism caused by prescription medications may improve with cessation of the implicated agent, but parkinsonism associated with prior MPTP use is not reversible. Symptoms of neurodegenerative parkinsonism can be managed with the same agents used for those of PD, but there tends not to be a sustained response to therapy.
For all parkinsonian syndromes, injuries from falls, infections (e.g., aspiration pneumonia), and concomitant medical conditions should be evaluated and managed as with other patients, keeping in mind the limitations imposed by the patient’s chronic level of functioning.
CRITICAL INTERVENTIONS
• Keep NMS on the differential for the decompensated Parkinson patients with medication noncompliance
• Coordinate all management strategies and medication changes of Parkinson patients with the patient’s long-term physician
DISPOSITION
Whether the diagnosis of parkinsonism is being considered in the ED or the patient is being seen for complications of therapy or progression of symptoms, the patient’s primary care physician or neurologist should be consulted. This assures continuity of care, which is essential to optimize the management of this chronic condition. Rarely is admission to the hospital or transfer to a tertiary care center indicated for parkinsonism itself. Complications such as sepsis or injuries from falls are more likely to be indications for inpatient management.
Common Pitfalls
• The diagnosis of parkinsonism may be missed in patients with vague complaints of dizziness, unsteadiness, or inability to walk, unless the signs are specifically sought on careful neurologic examination.
• The complex medical regimens for PD require precise modifications to maximize clinical benefit while minimizing side effects.
REFERENCES
1. Nutt JG, Wooten GF. Clinical practice. Diagnosis and initial management of Parkinson’s disease. N Engl J Med. 2005;353(10):1021–1027.
2. Rajput AH, Offord KP, Beard CM, et al. Epidemiology of parkinsonism: Incidence, classification, and mortality. Ann Neurol. 1984;16(3):278–282.
3. Tanner CM, Ottman R, Goldman SM, et al. Parkinson disease in twins: An etiologic study. JAMA. 1999;281(4):341–346.
4. Lang AE, Lozano AM. Parkinson’s disease. First of two parts. N Engl J Med. 1998;339(15):1044–1053.
5. Litvan I. Parkinsonian features: When are they Parkinson disease? JAMA. 1998;280(19):1654–1655.
6. Riess O, Berg D, Kruger R, et al. Therapeutic strategies for Parkinson’s disease based on data derived from genetic research. J Neurol. 2003;250(suppl 1):I3–I10.
7. Siderowf A, Stern M. Update on Parkinson disease. Ann Intern Med. 2003;138(8):651–658.
8. Wullner U, Klockgether T. Inflammation in Parkinson’s disease. J Neurol. 2003;250(suppl 1):I35–I38.
9. Duvoisin RC. A brief history of parkinsonism. Neurol Clin. 1992;10(2):301–316.
10. Stern MB. Contemporary approaches to the pharmacotherapeutic management of Parkinson’s disease: An overview. Neurology. 1997;49(1 suppl 1):S2–S9.
11. Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol. 1999;56(1):33–39.
12. Gibb WR. Neuropathology of Parkinson’s disease and related syndromes. Neurol Clin. 1992;10(2):361–376.
13. Ceballos-Baumann AO. Functional imaging in Parkinson’s disease: Activation studies with PET, fMRI and SPECT. J Neurol. 2003;250(suppl 1):I15–I23.
14. Tolosa E, Wenning G, Poewe W. The diagnosis of Parkinson’s disease. Lancet Neurol. 2006;5(1):75–86.
15. Albin RL. Parkinson’s disease: Background, diagnosis, and initial management. Clin Geriatr Med. 2006;22(4):735–751, v.
16. Hughes AJ, Daniel SE, Kilford L, et al. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55(3):181–184.
17. Lachenmayer L. Differential diagnosis of parkinsonian syndromes: Dynamics of time courses are essential. J Neurol. 2003;250(suppl 1):I11–I14.
18. Deep-Brain Stimulation for Parkinson’s Disease Study Group. Deep-brain stimulation of the subthalamic nucleus or the pars interna of the globus pallidus in Parkinson’s disease. N Engl J Med.2001;345(13):956–963.
19. Deuschl G, Schade-Brittinger C, Krack P, et al. A randomized trial of deep-brain stimulation for Parkinson’s disease. N Engl J Med. 2006;355(9):896–908.
20. Krack P, Batir A, Van Blercom N, et al. Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson’s disease. N Engl J Med. 2003;349(20):1925–1934.
21. Capildeo R. Implications of the 5-year CR FIRST trial. Sinemet CR Five-Year International Response Fluctuation Study. Neurology. 1998;50(6 suppl 6):S15–S17; discussion S44–S48.
22. Keyser DL, Rodnitzky RL. Neuroleptic malignant syndrome in Parkinson’s disease after withdrawal or alteration of dopaminergic therapy. Arch Intern Med. 1991;151(4):794–796.