Lila O’Mahony and George A. Woodward
Interfacility transport is an integral component of the continuum between optimal emergency and definitive care of acutely injured or ill pediatric patients, and when executed safely, efficiently, and by appropriately skilled teams, contributes to improved patient outcomes (1–4). Given that 89% of acutely injured or sick children are initially cared for at hospitals that typically do not have pediatric specialty or critical care services (5); a substantial number of children will require transfer to a higher level of pediatric care (Fig. 292.1).
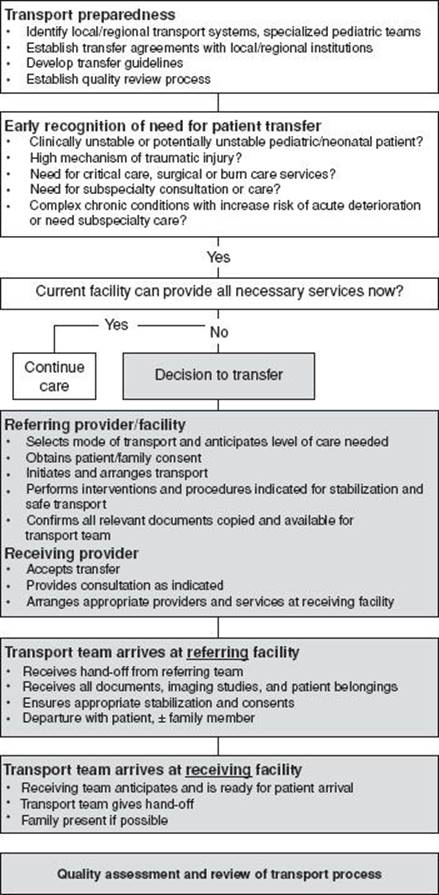
FIGURE 292.1 Pediatric interfacility transfer algorithm.
It is imperative that referring and receiving hospitals have processes and resources to safely and efficiently transfer pediatric patients. Ideally, these should be identified in advance to ensure optimal preparation. Some hospitals have pre-existing agreements with facilities that have comprehensive pediatric services outlining expectations and conditions, as well as the standard mode of transfer for critically ill or injured patients. A practical resource for the development of such guidelines is the 2013 “Interfacility transfer tool kit for the pediatric patient,” published by the Emergency Nurses Association, Emergency Medical Services for Children, and the Society of Trauma Nurses (http://www.ena.org/practice-research/Practice/Pages/Toolkit.aspx).
MEDICAL LEGAL ISSUES FOR REFERRING AND RECEIVING PROVIDERS
The Emergency Medical Treatment and Active Labor Act (EMTALA) is the cornerstone of civil transport regulation. It applies specifically to clinically unstable patients and is meant to (1) protect patients from being denied appropriate care due to an inability to pay and (2) prevent institutions from inappropriately transferring patients due to an inability to pay when the institution is able to provide needed care. Under EMTALA, referring providers are responsible for (1) stabilizing a patient within the capabilities of their institution, (2) initiating the transport process, and (3) selecting the mode of transportation, whether air or ground, and (4) the level of care the patient should be transferred to. In addition, referring providers ensure that patient care during transport remains at the level initiated and does not place the patient at undue risk. On the receiving end, providers and hospitals are responsible for ensuring they are able to provide the services the patient requires. Receiving providers and transport-related supervisors may act as consultants to the referring team to optimize ongoing care and select an appropriate transport mode. However, unless the receiving physician provides medical advice, or is serving as the transport’s online medical control physician or provides the transport service, accepting institutions are not legally responsible for patients’ care until they arrive at the receiving facility. Under EMTALA, there are circumstances under which a receiving provider may deny acceptance of a patient transfer. Caution must be taken when considering the determinants of an individual’s clinical “stability”; for under EMTALA, unstable patients cannot be denied transfer if the receiving facility has the capability to treat them (Table 292.1).
TABLE 292.1
Acceptable Conditions for Refusing Transfer of a Pediatric Patient
![]()
MODE OF TRANSPORT AND TEAM COMPOSITION
Referring institutions must appreciate the constraints of geography, traffic, weather, and other pertinent issues affecting transport logistics. These factors must be carefully weighed when selecting the composition of the transport team and the mode of transport.
Not all transport teams have comparable pediatric skills, experience, or equipment. Transport providers and teams lie on a spectrum from volunteers to basic emergency medical technicians with limited pediatric-specific skills to highly trained specialized pediatric and neonatal critical care teams. Awareness of the skill level and clinical capabilities of available transport teams will aid in the selection of the most appropriate transport team and mode (6–8).
When transferring critically ill children, the referring provider should strongly consider a team with specialized pediatric critical care skills since care by such providers is associated with decreased morbidity, improved survival, and better outcomes (1). While use of such a team may result in a longer period of stabilization at the referring facility, it allows for the initiation and continuation of consistent treatment at both facilities and ensures that an appropriately skilled team is able to respond to critical events or changes during transport. This is a fundamental difference from prehospital practice where the concept of rapid transfer and the “golden hour” to definitive care is often emphasized (9). In locations or circumstances where specialized teams are not available, the referring provider should ensure that a team is selected which can meet the patient’s needs at the highest level without compromising clinical care. Any appropriate treatments initiated at the referring facility should be continued during transport.
Neonatal transfers are often due to critical illness, congenital disorders, and the need for subspecialty or surgical care not available at a referring institution. Critically ill newborns are infrequent patients in most emergency departments, but may present in the context of trauma, a complicated home birth, or an unexpected precipitous delivery. Neonates who are critically ill or who have the potential for acute decompensation, such as those who are premature or of very low birth weight, require providers with special skills in assessment, management, and procedures, including vascular access and neonatal airway management. Thus, these patients should be transported by specialty teams with the highest level of pediatric and neonatal skills and expertise.
Travel distance to a referral center is a major factor to consider. Ground transport is always an option with an appropriately composed team. As a general rule, distances between 20 and 100 miles may warrant rotor wing aircraft and distances greater than 100 miles may dictate the need for rotor or fixed wing aircraft. These rules of thumb must be weighed against many factors. For example, a critically ill patient 10 miles from a referral center may be better served by rotor wing transport than ground transport during rush hour in an urban setting, while the same patient may travel 300 miles by ground in a rural area with dangerous winter weather that precludes flying.
Pediatric patients, their parents, and their healthcare providers will benefit from maintaining a family centered, supportive, and safe environment for the child, which in most circumstances means enabling parents to travel with their child (10).
REFERENCES
1. Orr RA, Felmet KA, Han Y, et al. Pediatric specialized transport teams are associated with improved outcomes. Pediatrics. 2009;124:40–48.
2. Kanter RK. Regional variation in child mortality at hospitals lacking a pediatric intensive care unit. Crit Care Med. 2002;30:94–99.
3. Pracht EE, Tepas JJ, Langland-Orban B, et al. Do pediatric patients with trauma in Florida have reduced mortality rates when treated in designated trauma centers? J Pediatr Surg. 2008;43:212–221.
4. Woodward GA, Insoft RM, Pearson-Shaver AL, et al. The state of pediatric interfacility transport: Consensus of the second national pediatric and neonatal interfacility transport medicine leadership conference. Pediatr Emerg Care.2002;18(1):38–43.
5. Gausche-Hill M, Schmitz C, Lewis RJ. Pediatric preparedness of US emergency departments: A 2003 survey. Pediatrics. 2007;120:1229–1237.
6. King BR, King TM, Foster RL, et al. Pediatric and neonatal transport teams with and without a physician. Pediatr Emerg Care. 2007;23(2):77–82.
7. King BR, Foster RL, Woodward GA, et al. Procedures performed by pediatric transport nurses: How “advanced” is the practice? Pediatr Emerg Care. 2001; 17(6):410–413.
8. Ajizian SJ, Nakagawa TA. Interfacility transport of the critically ill pediatric patient. Chest. 2007;132:1361–1367.
9. Stroud MH, Prodhan P, Moss MM, et al. Redefining the golden hour in pediatric transport. Pediatr Crit Care Med. 2008;9:425–437.
10. Woodward GA, Fleegler EW. Should parents accompany pediatric interfacility ground ambulance transports? Results of a national survey of pediatric transport team managers. Pediatr Emerg Care.2001;17(1):22–27.