Heather Long
Smoke inhalation is the number one cause of death from fire and is the most common cause of acute inhalation injury seen in the emergency department (ED). Furthermore, burn patients with smoke inhalation have much greater morbidity and mortality, with increased rates of pneumonia, infection, sepsis, and increased length of hospital stay. The overall mortality rate from burns averages 13.9% but, among those with concomitant smoke inhalation injury, mortality rises to 27.6% (1).
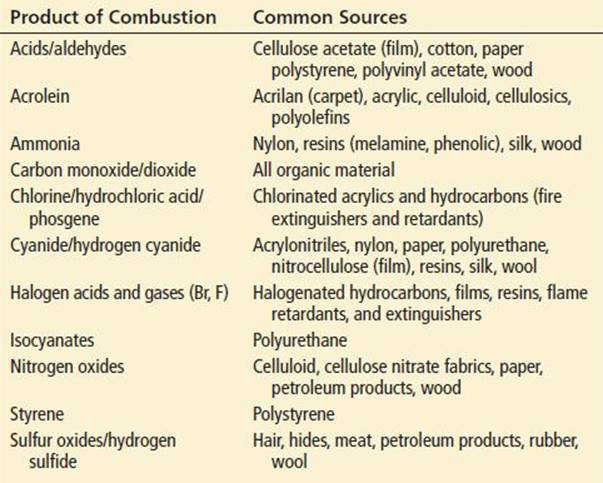
Smoke is a mixture of heated air, gases, fumes, aerosols, vapors, and solid and liquid particles in suspension. Smoke toxicity depends on the composition of the fuel, the availability of oxygen, the completeness of combustion, and the heat intensity. Even within the same building, smoke composition can vary considerably with duration of the fire and location. Toxic combustion products (TCPs) from naturally occurring materials and synthetic polymers in the modern environment contribute to smoke toxicity (Table 337.1).
TABLE 337.1
Toxic Products of Combustion
TCPs like other inhaled toxins (Chapter 336, “Inhaled Toxins”) are categorized as simple asphyxiants, chemical asphyxiants, or irritant toxins (Table 337.2). Simple asphyxiants displace oxygen from the ambient environment causing suffocation but they generally have no inherent toxicity. The process of combustion itself depletes oxygen from the environment as well.
TABLE 337.2
Toxic Combustion Products
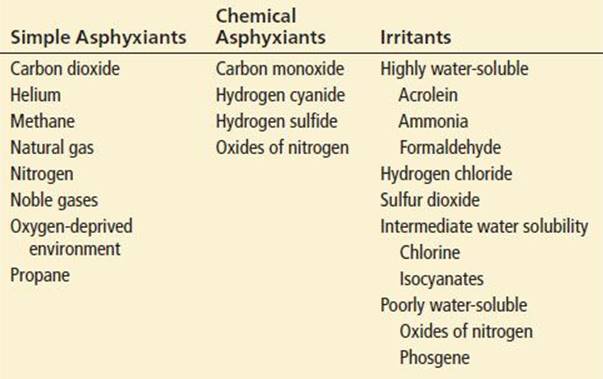
Chemical asphyxiants inhibit cellular respiration by inhibiting mitochondrial electron transport or by impairing oxygen delivery. Agents inhibiting mitochondrial electron transport include carbon monoxide (Chapter 327), hydrogen cyanide (Chapter 329), and hydrogen sulfide (Chapter 332). Carbon monoxide and oxides of nitrogen, by inducing carboxyhemoglobin (COHgb) formation or methemoglobinemia (see Chapter 335), respectively, impair oxygen transport and delivery to tissues.
Carbon monoxide, produced by the incomplete combustion of any carbon-containing compound such as wood, charcoal, and propane, is still the major toxicant in modern fires. However, COHgb fractions in smoke inhalation deaths are often <50%. An oxygen-poor environment combined with even sub-lethal levels of carbon monoxide significantly reduces the time to death. Blood ethanol concentrations correlate strongly with the COHgb fraction, suggesting that ethanol intoxication impairs the ability to recognize and escape danger, consequently prolonging smoke exposure.
Cyanide is produced from the combustion of nitrogen-containing products such as wool, silk, nylon, plastics, polyurethane, nitrocellulose, and synthetic rubber. Cyanide is present in appreciable amounts in air samples from fires and in blood from fire victims and is thought to have an additive, even synergistic effect, on smoke toxicity. Cyanide levels >0.1 mg/L are considered abnormal.
Combustion of nitrogen-containing materials generates oxides of nitrogen. These oxides are capable of inducing methemoglobinemia and may also directly oxidize cells of the respiratory tract or generate free radicals that induce delayed damage to the respiratory epithelium. Methemoglobinemia is rarely reported in smoke inhalation victims. Combustion of nitrocellulose, a major component of radiographic film, caused 125 deaths as a result of cyanide and nitrogen dioxide poisoning in the 1929 fire in the Cleveland Clinic radiology department (2).
Irritant toxins are a varied group of chemically reactive compounds that ultimately exert their toxic effects through damage to the respiratory tract. Mechanisms of injury vary with the different agents. The lipid-soluble acrolein penetrates cell membranes and denatures proteins and nucleic acids. Ammonia, hydrogen chloride, and sulfur dioxide react with the moisture of respiratory mucosa to yield ammonium hydroxide, hydrochloric acid, and sulfurous acid, respectively. Chlorine and phosgene generate free radicals, mediating oxidative stress on cellular membranes.
Inhalation of soot and aerosols results in enhanced delivery of irritant gases to the respiratory tract. As soot deposits, adsorbed gases are able to react with the moist mucosal surface. Size of the soot particle determines where it is deposited; particles of 1 to 3 microns are able to reach the alveoli. Particles generated from building fires predominately range from 3 to 5 microns and affect the bronchioles.
Direct heat injury from smoke is confined to the upper airway because of its marked ability to dissipate heat. Because steam has 4,000 times the heat-carrying capacity of hot air, steam inhalation may be rapidly fatal as a result of laryngeal and glottic edema, thermal tracheitis, and hemorrhagic edema of the bronchial mucosa.
Smoke inhalation injury is a product of the inherent toxicity of the TCPs, the victim’s minute ventilation, and the duration of exposure. Duration of exposure may be prolonged by anxiety; confusion; impaired visibility as a result of darkness, tearing, smoke, and physical obstacles; respiratory distress and altered cognition from TCP exposure; a low ambient oxygen concentration; and impaired awareness and mobility from drug and alcohol intoxication, physical handicaps, or extremes of age.
Inhaled particles and toxic gases damage mucosal cells and alveoli, triggering release of inflammatory mediators. Chemotaxins actuate diffuse protein-rich exudate formation. Increased vascular permeability results in interstitial edema. There is increased airway resistance, decreased lung compliance, and bronchoconstriction; acute lung injury may ensue 12 to 24 hours after injury with lung injury scores typically reaching their nadir 72 hours following initial insult. Severity of inhalation injury correlates with alveolar neutrophilia, enhanced production of inflammatory mediators, elevated COHgb, prolonged mechanical ventilation and intensive care unit (ICU), and hospital length of stay (3).
Among firefighters, the type of respirator used influences the risk of smoke inhalation. Atmosphere purifying respirators (APRs) protect against some inhaled particles but not heated gases or CO; oxygen-supplying, self-contained breathing apparatus (SCBA) is the only NIOSH-approved respirator for firefighting. If oxygen is supplied via a demand valve requiring negative inspiratory pressure, smoke inhalation may occur if the mask does not fit tightly. With continuous positive-pressure devices, smoke inhalation will not occur unless the oxygen supply, which typically lasts 20 to 30 minutes, runs out. If either type of mask is removed during clean-up activities after the flames are extinguished, smoke inhalation may still occur. Wildfire fighters do not typically wear oxygen masks or APRs and may be at special risk for inhalation injury.
Smoke inhalation injuries pose significant potential for mass casualties. A train hauling hydrochloric acid, hydrofluoric acid, and acetic acid derailed in Baltimore in July 2001, causing a fire that burned for 5 days and sent hundreds of people to local EDs (4). In November 2000, 155 people died, most of them from smoke inhalation, after a fire broke out in a cable car traveling through a tunnel in Austria. In the 1990 Happy Land Social Club fire in New York City, all 87 deaths were due to smoke inhalation (5).
CLINICAL PRESENTATION
Respiratory signs and symptoms are the primary clinical manifestations of smoke inhalation toxicity. Clinical effects range from transient respiratory tract irritation to severe upper airway compromise and respiratory failure. Cough is often the first symptom. Other initial responses include increased mucous secretion and sneezing. Upper airway involvement results in hoarseness and stridor. Injury to the lower respiratory tract results in crackles and/or wheezing. Breath sounds may be inaudible in cases of severe bronchospasm. Important signs of potential inhalation injury include cough, dyspnea, hoarseness, soot in the oral cavity, singed nasal hair, edema of the posterior pharynx, burns to the face, and any major burn to the body.
Smoke inhalation may cause systemic manifestations as well. Examination of the eye may reveal the irritant effects of increased tearing, conjunctival injection, and blepharospasm. Progressive airway compromise and toxicity from agents with systemic effects, notably carbon monoxide, will produce signs and symptoms of hypoxia—tachycardia, tachypnea, dizziness, headache, nausea and vomiting, chest pain, and deteriorating mental status manifesting as agitation, confusion and ultimately seizures, coma, and death.
Laboratory evaluation may detect hypoxemia, metabolic acidosis, and elevated lactate levels, COHgb, and methemoglobin fractions. The electrocardiogram (ECG) may detect dysrhythmias or evidence of myocardial ischemia or infarction.
DIFFERENTIAL DIAGNOSIS
Patients with smoke inhalation are usually easily identified by history but may have concomitant dermal burns, traumatic injuries, or drug or alcohol intoxication and may be victims of arson, attempted murder, or attempted suicide. For patients presenting with coma and shock, hypoglycemia, intracranial hemorrhage and diffuse brain injury, spinal cord injuries, hypovolemia, myocardial injury, carbon monoxide poisoning, cyanide poisoning, methemoglobinemia, alcohol intoxication, and drug overdose must also be considered.
ED EVALUATION
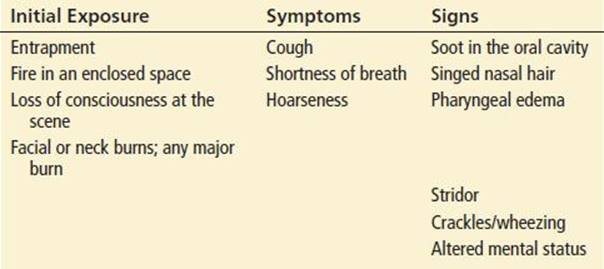
Significant smoke inhalation injuries may be delayed after exposure. History of entrapment, fire within an enclosed space, and altered consciousness at the scene should raise the suspicion of inhalation injury. Key risk factors associated with inhalation injury are in Table 337.3. The history should address the nature of burning material, presence of steam, evidence of trauma or suicidality and, for rescuers presenting as patients, the type of mask used.
TABLE 337.3
Risk Factors Associated with Inhalation Injury
Examination begins with obtaining vital signs and oxygen saturation, however, transcutaneous pulse oximetry overestimates the true oxygen saturation in the presence of COHgb and methemoglobin. Co-oximetry directly measures an accurate oxygen saturation even in the presence of dyshemoglobinemias. A trauma survey with attention to signs associated with increased risk of smoke inhalation including facial burns, singed facial hair, soot in the nasal passages and airway, and burns involving extensive body surface area (>15%) should follow. The eyes in comatose patients or those with eye complaints should be examined with fluorescein staining to detect corneal burns and lacerations. Other causes of altered mental status including drug and ethanol intoxication should be considered. Repeat examinations should focus on respiratory status and alterations in mental status. Lung injury scores typically worsen, reaching their nadir about 72 hours after the initial smoke inhalation.
COHgb and methemoglobin should be measured by co-oximetry. An elevated COHgb fraction in a fire victim is an indicator of significant exposure to combustion products and is associated with a markedly increased risk of smoke inhalation injury and toxicity. However, a low or undetectable COHgb concentration does not rule out the possibility of developing even severe inhalation injury.
Whole-blood cyanide levels are not timely but a plasma lactate concentration >8 mmol/L refractory to adequate ventilation, oxygenation, and perfusion is a surrogate marker of cyanide toxicity in the setting of smoke inhalation (6). Methemoglobin should be determined in symptomatic patients, particularly with cyanosis that does not improve with supplementary oxygen (Chapters 329 and 335).
Blood gas measurements should be obtained to assess arterial oxygenation, alveolar ventilation, and the presence of metabolic acidosis. Initially, the blood gas of even a significantly injured patient may be normal; serial measurements are recommended.
An ECG and a chest radiograph are recommended in symptomatic patients, especially in those with pre-existing cardiovascular or pulmonary disease. Chest radiographs may appear normal early in the course of smoke inhalation and therefore lack sensitivity as indicators of inhalation injury. Early findings, if present, are subtle: perivascular cuffing, bronchial wall thickening, and subglottic edema (7). Serial chest radiographs, however, may be very useful in monitoring disease progression. Common complications that do not typically manifest radiographically until more than 24 hours after the initial insult include acute lung injury/acute respiratory distress syndrome, aspiration, volume overload, and infection.
Fiberoptic bronchoscopy is considered the gold standard for diagnosis and evaluation of inhalation injury. Chest CT scan at time of hospital admission appears to complement bronchoscopy in predicting severity of inhalation injury. Bronchial wall thickening measured by CT correlates with subsequent development of pneumonia and other markers of severity including ICU stay and ventilator requirement (8).
KEY TESTING
• Obtain a COHgb level, chest x-ray, and ECG in all patients with signs of smoke inhalation and/or cardiopulmonary symptoms
• Obtain a lactate level to evaluate for potential cyanide toxicity in seriously ill patients
• Obtain a methemoglobin level in patients with cyanosis and/or other signs including tachycardia, tachypnea, and altered mental status
• Consider early bronchoscopy in admitted patients
• Consider testing for ethanol and other drugs for altered mental status
ED MANAGEMENT
Prehospital directives include the rapid, safe removal of victims from the scene by those with adequate training and protection. Basic and advanced life-support measures are instituted as indicated, including cervical spine immobilization with trauma. Supplemental oxygen is indicated for all patients. Whether a patient should be transported to a burn center, trauma center, or hyperbaric facility is determined by local practice guidelines. Intravenous access and cardiac monitoring may be established en route.
On arrival to the ED, upper airway patency must be determined immediately. Airway compromise may be present initially, rapidly ensue, or develop insidiously over the next few hours. Failure to appreciate the potential for rapid decline in airway status is the major pitfall in managing the smoke inhalation patient. The factors that best correlate with the need for intubation and edema of either the true or false vocal cords are soot in the oral cavity, facial burns, and/or body burns (9). Early endotracheal intubation, performed in a controlled setting before edema makes it impossible, may be life-saving and should be undertaken when these risks are present. In the patient with the edematous or difficult airway, fiberoptic laryngoscopy, flexible intubation guides, intubation laryngeal masks, retrograde intubation, transtracheal jet ventilation, and ultimately cricothyroidotomy may be necessary for establishing tracheal intubation. Aggressive rehydration of the burn victim may also cause airway edema requiring early intubation.
Early consultation for fiberoptic bronchoscopy should be considered if there is suspicion of inhalation injury. It may also assist in clearing debris from the respiratory tract and permits fiberoptically assisted intubation if required.
β2-Adrenergic agonists may be useful in improving airflow. Corticosteroids are not indicated with smoke inhalation injury as they are associated with increased incidence of bacterial pneumonia and mortality and are not associated with improved pulmonary function (10). Prophylactic antibiotics also have no demonstrated benefit in the treatment of inhalation injury. Fever and leukocytosis that develop 2 days or more after the injury do suggest infection, and empiric antibiotic treatment that covers Staphylococcus aureus and gram-negative organisms should be instituted until culture results become available. Progressive respiratory failure and the development of pneumonitis, acute lung injury/adult respiratory distress syndrome, or other complications may require mechanical ventilation, continuous positive airway pressure, positive end-expiratory pressure, and frequent suctioning of pulmonary secretions.
Trauma-related injuries as a result of falls or explosions and burns must be managed concurrently with inhalation injury. Perform a fingerstick glucose or administer dextrose in the patient with altered mental status and coma and consider naloxone for possible opiate intoxication.
Treat suspected carbon monoxide poisoning with 100% oxygen via nonrebreather mask or endotracheal tube until confirmatory COHgb level is obtained. Consider referral for hyperbaric oxygen therapy (see Chapter 327). Suspect cyanide poisoning in patients with coma and hypotension and treat with an antidote (see Chapter 329). Hydroxocobalamin (Cyanokit) does not induce methemoglobinemia and may be safely administered to the smoke inhalation patient with suspected cyanide toxicity. The other commercially available antidote kit contains sodium nitrite 3% solution and sodium thiosulfate 25% solution. Sodium nitrite is a potent vasodilator and may cause hypotension. It can also induce methemoglobinemia. When oxygen transport is already compromised, as in a patient with concomitant carbon monoxide poisoning, further impairment by the inducement of methemoglobinemia may exacerbate cellular hypoxia. If hydroxocobalamin is unavailable, a reasonable approach in the smoke inhalation patient with suspected cyanide toxicity, particularly the seriously ill patient with a lactate level >8 mmol/L refractory to resuscitation, is to administer 12.5 g of sodium thiosulfate (50 mL of a 25% solution for adults; pediatric dose, 1.65 mL/kg).
Symptomatic methemoglobinemia and/or concentrations >20% to 30% should be treated with methylene blue (see Chapter 335).
CRITICAL INTERVENTIONS
• Perform early endotracheal intubation in patients with oropharyngeal burns or edema, soot in the oral cavity, full-thickness circumferential neck burns, stridor, coma, or hypoxemia or respiratory distress unresponsive to oxygen administration.
• Administer 100% oxygen to patients with significant smoke exposure or respiratory symptoms.
DISPOSITION
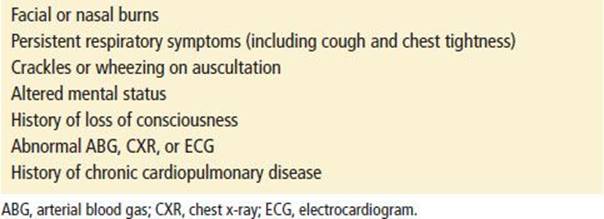
Indications for admission for observation and further treatment are listed in Table 337.4. Severity of illness and the presence of concomitant burns or traumatic injuries should guide the decision to admit to an ICU, telemetry unit, or floor bed. Patients with carbon monoxide poisoning may require transfer for HBO therapy (see Chapter 327), and those with significant surface burns or physical injuries may require transfer to a burn or trauma center. Advanced life-support capability should be available during transfer.
TABLE 337.4
Indications for Admission after Smoke Inhalation
Patients in good health who are asymptomatic (on arrival or after a short period of oxygen therapy) and have a normal physical examination including pulse oximetry, blood gas analysis (while breathing room air), ECG, chest radiograph, and COHgb level may be discharged. These patients should be observed for at least 3 or 4 hours before discharge, and they should be instructed to return immediately if any respiratory symptoms develop. Scheduled follow-up at 24 hours may be prudent.
Common Pitfalls
• Failure to anticipate deterioration despite an initially normal initial physical examination, laboratory evaluation, and chest radiograph and failure to frequently reevaluate the respiratory status.
• Failure to evaluate and treat for coexisting carbon monoxide poisoning, drug or alcohol intoxication, traumatic injuries, and psychiatric problems.
• Failure to give oxygen to all patients (including those with chronic obstructive pulmonary disease).
• Failure to fluid-resuscitate patients with trauma or surface burns for fear of exacerbating the edema of inhalation injury.
• Failure to recognize the potential hazards of inappropriate corticosteroid and antibiotic administration.
ACKNOWLEDGMENT
The author gratefully acknowledges the contributions of Christopher H. Linden to the content of this chapter.
REFERENCES
1. Colohan SM. Predicting prognosis in thermal burns with associated inhalational injury: A systematic review of prognostic factors in adult burn victims. J Burn Care Res. 2010;31;529–539.
2. Gregory KL, Malinoski VF, Sharp CR. Cleveland Clinic fire survivorship study 1929–1965. Arch Environ Health. 1969;18:508–515.
3. Albright JM, Davis CS, Bird MD, et al. The acute pulmonary inflammatory response to the graded severity of smoke inhalation injury. Crit Care Med. 2012;40:1113–1121.
4. Hsu EB, Grabowski JG, Chotani RA, et al. Effects on local emergency departments of large-scale urban chemical fire with hazardous materials spill. Prehosp Disaster Med. 2002;17:196–201.
5. Gill JR, Goldfeder LB, Stajic M. The happy land homicides: 87 deaths due to smoke inhalation. J Forensic Sci. 2003;48:161–163.
6. Baud FJ, Borron SW, Megarbane B, et al. Value of lactic acidosis in the assessment of the severity of acute cyanide poisoning. Crit Care Med. 2002;30:2044–2050.
7. Lee MJ, O’Connell DJ. The plain chest radiograph after acute smoke inhalation. Clin Radiol. 1988;39:33–77.
8. Yamamura H, Kaga S, Kaneda K, et al. Chest computed tomography performed on admission helps predict the severity of smoke inhalation injury. Crit Care. 2013;17;R95.
9. Madnani DD, Steele NP, de Vries E. Factors that predict the need for intubation in patients with smoke inhalation injury. Ear Nose Throat J. 2006;85:278–280.
10. Cha SI, Lee JH, Park JY, et al. Isolated smoke inhalation injuries: Acute respiratory dysfunction, clinical outcomes, and short-term evolution of pulmonary functions with the effects of steroids. Burns.2007;33:200–208.