Kaushal Shah and Natasha Desai
Ankle injuries are among the most common sports-related and extremity injuries presenting to the emergency department (ED) accounting for approximately 20 million injuries per year and up to 20% of all sports injuries (1,2,3). Although the vast majority are benign injuries, there are instances when immediate action and emergent consultation are necessary.
The ankle and foot are relatively simple structures. The ankle is formed by (a) the tibia, which forms the medial malleolus, the posterior malleolus, and the plafond (ceiling); (b) the fibula, which forms the lateral malleolus; and (c) the talus (Fig. 45.1). The ankle is held together by (a) the medial ligaments collectively termed deltoid ligament; (b) the lateral ligaments–-anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular ligament (PTFL); and (c) the syndesmosis between the distal tibia and fibula (Fig. 45.2). The foot has three general parts: the hindfoot (calcaneus and talus), the midfoot (navicular, cuboid, and cuneiforms), and the forefoot (metatarsals and phalanges) (Fig. 45.1).
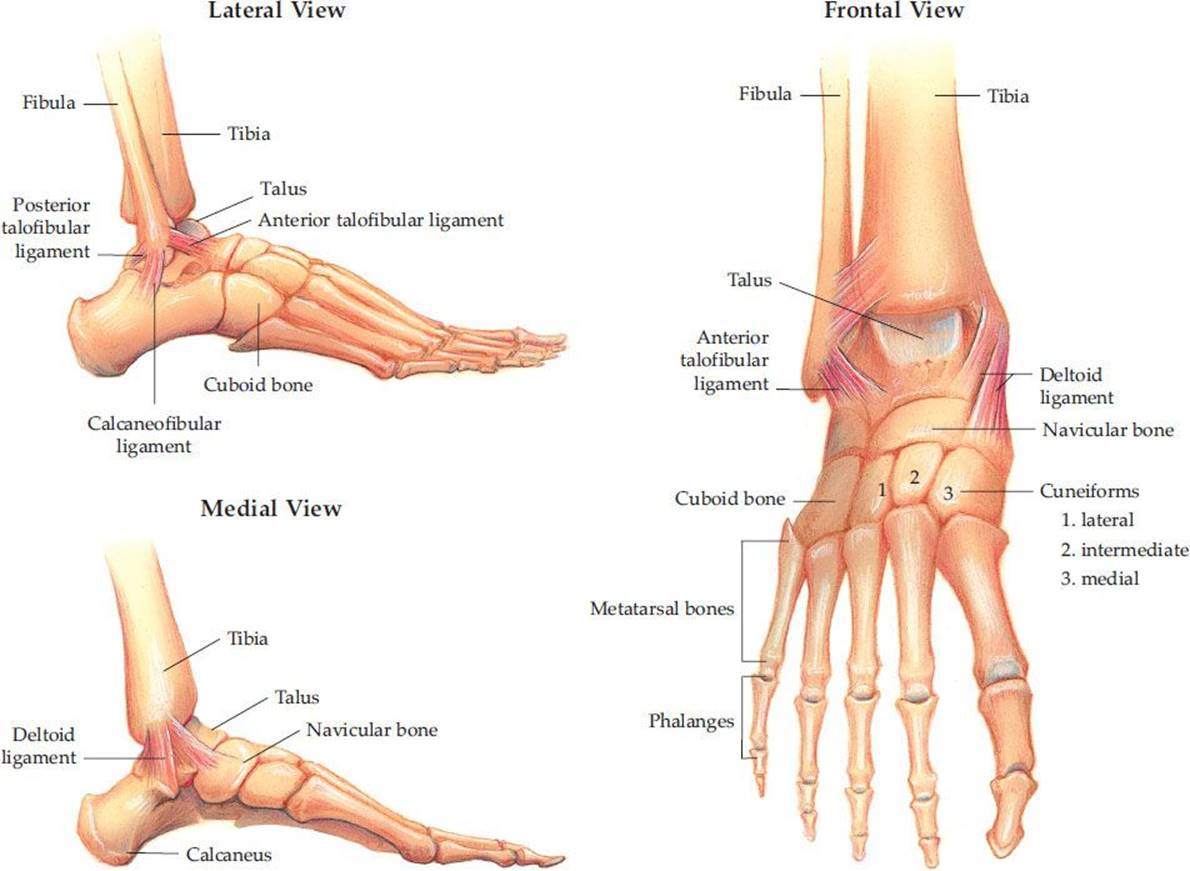
FIGURE 45.1 Anatomy of ankle and foot.
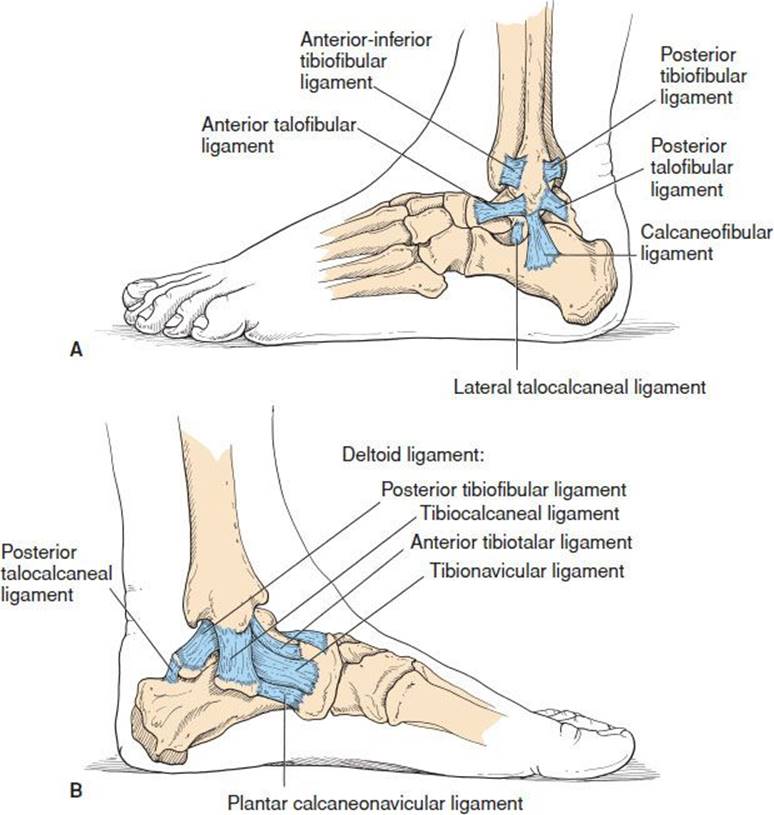
FIGURE 45.2 Ankle and foot – ligaments (A) lateral view; (B) medial view. (From Cipriano J. Photographic Manual of Regional Orthopaedic and Neurological Tests, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins; 1991.)
CLINICAL PRESENTATION
Ankle injuries can be anticipated by the position of the foot and direction of the force at the time of injury. Other key factors include the ability to ambulate after injury and a history of previous injuries (1). Most common “red flags” suggestive of a fracture rather than a sprain are inability to bear weight, significant swelling, or tenderness. The ankle should be considered as a closed ring with the tibia, fibula, and talus as the main parts held together by ligaments. A break in two or more places results in instability.
ED EVALUATION AND MANAGEMENT
Ankle Ligamentous Injuries
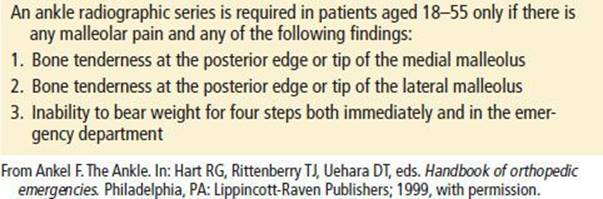
Approximately 90% of ankle ligamentous injuries are due to inversion of the ankle, resulting in sprain of the lateral ligaments, most commonly the ATFL (1). Significant injuries from an eversion mechanism are far less common because the broad deltoid ligament is strong and resistant to tears. The clinical findings associated with ankle sprains range from mild pain and swelling to severe pain with edema and ecchymosis. Neurovascular status should be checked by palpating the posterior tibial and dorsalis pedis pulses, checking capillary refill, and assessing distal sensation. However, without gross deformity, it is extremely unlikely that the neurovascular status will be compromised. Palpation of the medial and lateral malleoli and the base of the fifth metatarsal for focal tenderness are critical to evaluate for associated fracture. The Ottawa Ankle Rules (OAR) are useful in determining which patients do not need radiographic evaluation for an ankle injury; the sensitivities range from 97% to 100% (Table 45.1) (4–6). In the pediatric population, the OAR have been shown to be 98.5% sensitive for predicting significant ankle and midfoot fractures in a meta-analysis of 12 studies which included 3,130 children older than 5 years (B). If x-rays are obtained, the physician should inspect the AP view for talar shift and malleolar fractures, the mortise view for widening of the tibiotalar joint, and the lateral view for posterior malleolar fracture and general alignment.
TABLE 45.1
Ottawa Criteria for Ankle Radiographs
Provocative tests for ankle stability are necessary to determine the grade of injury. eTable 45.1 describes the grading of ankle sprains. The anterior drawer test assesses the integrity of the ATFL (Fig. 45.3). The test is positive if greater subluxation is noted on the injured ankle than the opposite one. The talar tilt test can be used to assess the lateral and medial ligaments (Fig. 45.3). If there is significant subluxation with inversion, tears of the ATFL or CFL should be suspected. Significant subluxation with eversion raises suspicion for a tear of the deltoid ligament. Integrity of the tibiofibular syndesmosis can be tested via the squeeze test, which involves squeezing the proximal tibia and fibula together. If pain is elicited, the test is positive (eFig. 45.1).
eTABLE 45.1
Classification of Ankle Sprains

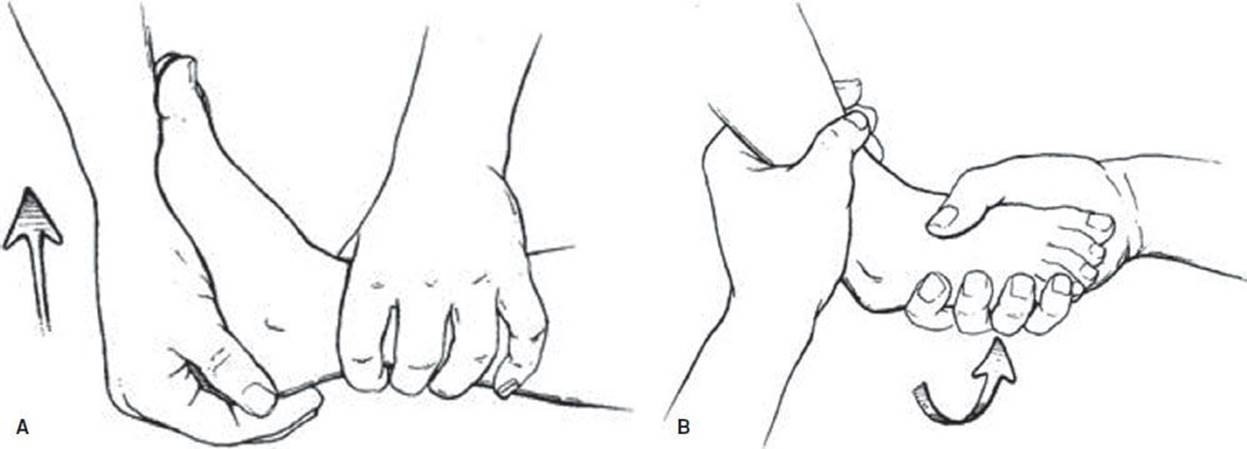
FIGURE 45.3 A: The anterior drawer test is performed by placing the patient’s heel in the palm of the examiner’s hand with the ankle at a 90-degree angle to the long axis of the leg. The examiner gently, but firmly, moves the heel and foot forward (arrow). B: In the talar tilt maneuver, the heel is firmly adducted (arrow) and assessed for increased laxity or instability compared with the noninjured side. (Adapted from Fleisher GR, Ludwig S, Henretig FM, et al. Textbook of Pediatric Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.)

eFIGURE 45.1 The squeeze test—practitioner squeezes the tibia and the fibula together. If pain is elicited, it suggests a tibiofibular syndesmosis injury. (From Dale Berg, Katherine Worzala. Atlas of Adult Physical Diagnosis. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.)

eFIGURE 45.2 X-ray of a pilon fracture in a 46-year-old man, resulting from an axial load in a motorcycle accident. A: AP view. B: Lateral view.
Acutely, ibuprofen 10 mg/kg (not to exceed 800 mg) PO or acetaminophen 15 mg/kg (not to exceed 1,000 mg) PO should be administered for pain. Ketorolac 30 to 60 mg IM or IV, in an adult, is also effective. General management guidelines follow the “RICE” mnemonic: rest ankle and avoid reinjury which may entail use of crutches; ice the ankle for 20 minutes three to four times per day for the first day to reduce swelling; compress with an elastic ACE wrap or ankle brace to reduce swelling and pain; elevate the extremity as often as possible to reduce swelling. eTable 45.1 describes the management based on the grade of the injury. If serious ligamentous injury is suspected, resulting in joint laxity (i.e., grade II and higher sprains), more rigid splinting methods should be considered. An air stirrup splint is moderately effective in preventing inversion and eversion of the ankle and is appropriate for grades I and II ankle sprains. For grade III injuries, a short-leg posterior rigid splint (e.g., plaster) that runs from midcalf to the toes should be used to further immobilize the ankle to prevent worsening of the injury and promote healing.
All patients with ankle sprains can be discharged home but should have appropriate follow-up within 1 week. Although pain and swelling should abate and the ability to ambulate should improve with time, occult fractures and high-grade sprains may require further orthopedic or sports medicine care. Other indications for orthopedic referral include (a) a “pop” that is heard or felt, (b) a history of several previous injuries, (c) medial ankle tenderness, (d) a positive squeeze test or other stress test, and (e) grade II and higher sprains in children with open growth plates (7). In children, less force is required to sustain a Salter–Harris I fracture than is required to tear a ligament (see Chapter in Pediatric Section, “Extremity fractures”). Thus, any patient who is suspected of having a significant ankle sprain and no clear fracture on x-ray should be splinted and referred to an orthopedic surgeon for follow-up.
Ankle Fractures
Ankle fractures can present after a significant traumatic mechanism or after a simple ankle inversion or eversion twisting injury. There are several types of ankle fractures that should be considered in the differential diagnosis. A lateral malleolus fracture is the most common type of ankle fracture resulting from inversion of the ankle. Isolated medial malleolus fractures are less common because the injury requires more force than a lateral malleolus fracture. Therefore, other associated fractures and joint instability should be suspected. Patients with bi- or trimalleolar fractures present with significant pain, swelling, and ecchymosis, and associated dislocations are common. A distal tibial fracture through the articular surface is called a plafond fracture. Although commonly used interchangeably with the term plafond fracture, a pilon fracture is specifically a comminuted plafond fracture that results from an axial compression force to the tibial plafond (eFig. 45.3). The Maisonneuve fracture is an oblique fracture of the proximal fibula associated with a medial malleolus fracture or deltoid ligament tear. It can easily be missed if the proximal fibula is not routinely palpated in patients with ankle-twisting injuries. These last two fractures require radiographs of the entire tibia and fibula.

eFIGURE 45.3 Technique for posterior dislocation reduction.
As with ankle sprains, neurovascular status should be checked immediately. The history and physical examination are identical to that of ankle sprains. If there is gross deformity, a dislocation should be considered and should be reduced emergently if there is neurovascular compromise. Lacerations and wounds should be examined closely to ensure that an open fracture is not present.
Suspected ankle fractures require x-rays in three views as described above. The two most common classification systems for ankle fractures are the Lauge-Hansen and Danis–Weber. The Danis–Weber classification system is simpler and is based on the location of the fibular fracture (Fig. 45.4). A fibular avulsion fracture below the tibiotalar joint line is called a Weber type A fracture. If the fibular fracture is in the joint line, it is a Weber type B fracture. Fractures above the joint line disrupting the syndesmosis ligament are termed Weber type C fractures.
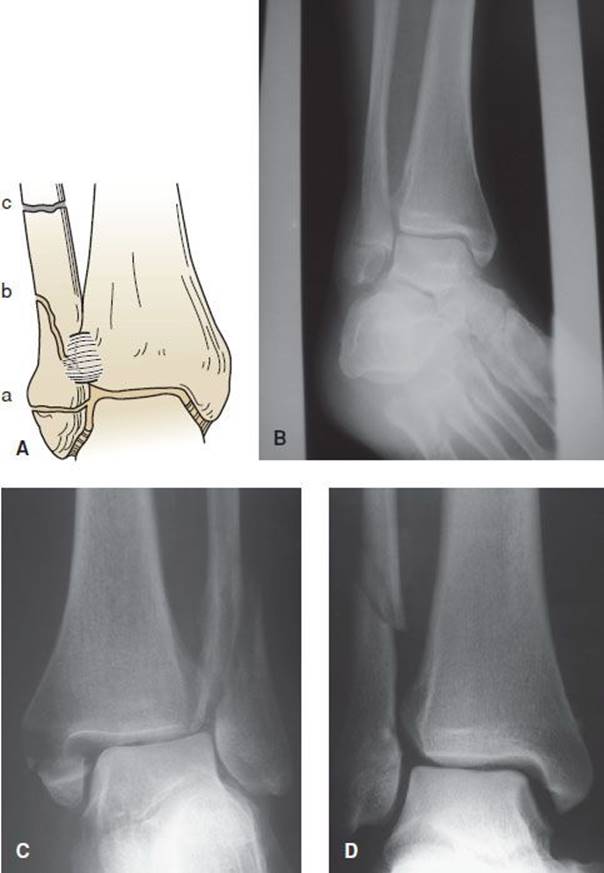
FIGURE 45.4 A: Schematic diagram of the Danis–Weber classification of ankle fractures. B: A type A fracture where the anterior tibiofibular ligament remains intact. C: A type B fracture with the fracture extending through the ligament. D: A type C fracture where the fracture is above the joint line. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.)
Patients should receive adequate analgesia. Intravenous, intramuscular, and subcutaneous injections are preferred (rather than oral administration) until it is certain the patient will not require an operative procedure. Isolated lateral or medial malleolar fractures without instability can be safely discharged home without orthopedic consultation in the ED. The emergency physician should first place the ankle in a posterior splint, provide crutches for nonweight bearing, provide adequate analgesia, and ensure close orthopedic follow-up. All other ankle fractures will require orthopedic consultation in the ED.
Isolated fractures of the distal tibia and fibula should be immobilized in a short-leg posterior splint. A sugar tong splint (U-splint) can also be used; it wraps along both the medial and lateral sides of the leg with the base of the “U” under the foot (similar to an air stirrup) and is more effective in stabilizing the medial and lateral ligaments. Patients with severe injuries to the ankle, such as bi- and trimalleolar fractures, should be placed in both a posterior splint and a sugar tong splint (“AO” splint). This provides immobilization similar to that of casting but allows for the expected ankle swelling.
Ankle Dislocations
For the talus to dislocate from the distal tibia, multiple ligaments are torn, and there are often associated malleolar fractures. Significant force is required, and there is always gross deformity and inability to bear weight.
The emergency physician should perform immediate reduction if there is neurovascular compromise or significant skin tenting with concern for conversion into an open fracture–dislocation. In cases of uncomplicated dislocations, x-ray evaluation should precede reduction.
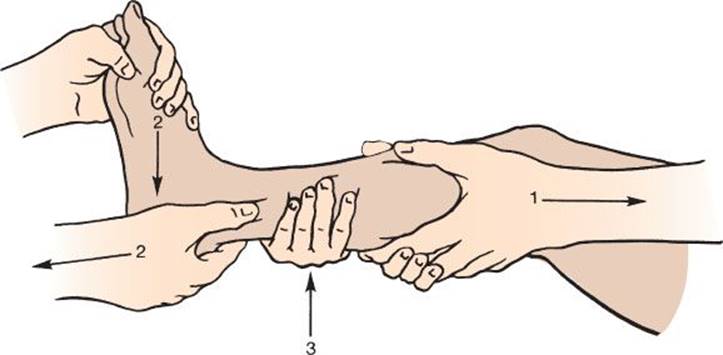
Reduction of the ankle requires conscious sedation and two assistants. For posterior dislocations, the first assistant flexes the knee to 45 degrees and applies counter-traction over the calf while the second assistant pushes down on the front of the lower leg. The physician applies traction to the heel and forefoot after first plantar flexing the foot and then lifting the heel (eFig. 45.3). For anterior dislocations, the first assistant flexes the knee to 45 degrees and applies counter-traction over the calf while the second assistant lifts up on the lower leg. The physician should dorsiflex the foot initially to disengage the talus and then push downward on the foot (eFig. 45.4). For lateral dislocations, the physician applies longitudinal and medial traction whereas an assistant applies counter-traction.
eFIGURE 45.4 Technique for anterior dislocation reduction.
Orthopedic consultation is necessary for all fracture–dislocations of the ankle. If a patient needs to be transferred, the emergency physician should reduce the ankle and place the ankle in a short-leg posterior splint (with or without a sugar tong splint). For open dislocations, IV antibiotics should be administered prior to transfer. Cefazolin 1 to 2 gm IV in adults is usually adequate, but patients with contaminated wounds should also receive gentamicin 2 mg/kg IV.
Achilles Tendon Rupture
The classic presentation is a middle-aged man complaining of ankle pain and inability to bear weight after hearing a “pop” while playing sports. Risk factors for rupture include steroid injections and tendonitis. The Achilles tendon usually ruptures at the narrowest segment, approximately 5 cm above its attachment to the calcaneus.
Occasionally an obvious defect in the Achilles tendon can be palpated. However, the most useful signs of this injury are weakness of plantar flexion and a positive Thompson test (the foot does not plantar flex when the calf is squeezed) (eFig. 45.5). The test is performed with the patient prone and the knee flexed to 90 degrees.

eFIGURE 45.5 The Thompson test for continuity of the gastrocnemius-soleus complex. Without rupture of the Achilles tendon, squeezing the calf causes active plantar flexion of the foot. With rupture, squeezing the superficial posterior compartment of the leg does not induce plantar flexion of the foot. (Adapted from Browner B, Jupiter J, Levine A. Skeletal Trauma: Fractures, Dislocations, and Ligamentous Injuries, 2nd ed. Philadelphia, PA: WB Saunders; 1997.)
Orthopedic consultation should be obtained. Operative versus conservative management is currently under debate; surgical repair has been shown to decrease rate of rerupture; however, complication rates increase (8). It is also appropriate to place a posterior splint with the foot in plantar flexion and refer to an orthopedist within 48 to 72 hours.
Peroneal Tendon Subluxation
These patients present very similar to those with a simple ankle sprain. However, the mechanism is different. The injury is caused by dorsiflexion and eversion of the ankle resulting in contraction of the peroneal muscle and disruption of the peroneal retinaculum. Because the peroneal tendon subluxes out of its groove along the posterior lateral malleolus, the ankle is swollen, tender, and ecchymotic around the lateral malleolus.
Although x-rays are usually negative for bony disruptions, these patients should be placed in a sugar tong splint with extra lateral malleolar padding. Patients should be referred to an orthopedist within a week for casting and should remain nonweight bearing for 4 to 6 weeks. Occasionally, surgery is recommended for athletes, those who fail nonoperative management, and those with chronic subluxations (9).
Calcaneal Fractures
A vertical compression force, such as jumping or falling from a height and landing directly on the feet, is the most common etiology of calcaneal fractures. They occur more commonly in men who are 30 to 50 years old. Patients complain of heel pain and have difficulty bearing weight.
Three radiographic views (AP, lateral, and axial) of the heel should be obtained. Fractures are often not clearly visible owing to a predominantly compressive force. A helpful measurement to make the diagnosis is determination of Boehler angle on the lateral view (Fig. 45.5). A normal angle is 20 to 40 degrees, and an angle less than 20 degrees indicates a calcaneal fracture.

FIGURE 45.5 Lateral view of the calcaneous. A: A schematic outlining Boehler (also known as Böhler) angle and the crucial angle of Gissane. B: Lateral radiograph showing both anatomical angles. (From Bucholz RW, Heckman JD. Rockwood & Green’s Fractures in Adults. 5th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001.)
Owing to the mechanism and force required, a thorough trauma evaluation is important. Calcaneal fractures are specifically associated with lumbar spine injuries in 10% of patients.
Patients with calcaneal fractures require emergent orthopedic evaluation. It is likely that the specialist will request a computed tomography (CT) scan or magnetic resonance imaging (MRI) to better delineate the fracture pattern. Operative verses nonoperative management is controversial. However, both are associated with a high incidence of chronic pain and loss of joint mobility and function. If orthopedic consultation is not immediately available and the patient has no associated injuries warranting admission, the physician should provide analgesia and place the patient in a short-leg posterior splint. The patient should be nonweight bearing. Orthopedic follow-up should occur within 24 to 48 hours (10).
Talus Fractures
A high-impact mechanism is required to fracture the talus. A hyperdorsiflexion injury from a motor vehicle collision or fall from a height is necessary to compress the talus between the tibia and calcaneus. Osteochondral fractures of the talar dome (also termed osteochondritis dessicans) occur after an inversion mechanism. Patients usually present with chronic pain after the diagnosis is missed on the initial visit because physical findings are nonspecific and plain radiographs may be normal. Suspected talar dome fractures may benefit from bone scan, CT, or MRI for further evaluation and classification.
Unlike talar dome fractures, fractures through the body and neck are usually visible on plain radiographs. It is particularly important to evaluate for the commonly associated subtalar dislocation. In addition, the os trigonum(accessory bone) can occasionally be mistaken for a posterior process fracture.
Recently, there has been increased attention to fractures of the lateral process of the talus (LPT). This fracture is closely associated with snowboarding and was relatively rare prior to the advent of the sport. It now accounts for less than 1% of all ankle injuries and for 15% of snowboarders’ ankle injuries (11,12), leading to the name snowboarder’s fracture. The LPT is a wedge-shaped prominence which articulates with the fibula and the calcaneus. Although the incidence is increasing because of the growing popularity of the sport, this fracture is frequently misdiagnosed as an ATFL sprain, leading to inadequate immobilization and less orthopedic intervention. Misdiagnosis can lead to significant morbidity, such as nonunion and degenerative arthritis (13,14). The mechanism of injury is still under investigation. It is most commonly believed to be a high impact injury on an axially loaded and dorsiflexed ankle, combined with foot inversion (13). Like other talus fractures, it can be difficult to identify an LPT fracture on plain radiographs, with a miss rate of approximately 40%. CT or MRI is often required to make the diagnosis, and thus a high index of suspicion is necessary (15). These fractures often present to the ED as chronic pain after an ankle sprain. All LPT fractures should be immobilized, and require nonweight bearing and close orthopedic evaluation. Operative management is dependent on severity (11,12).
Talus fractures require evaluation and continued care by an orthopedic surgeon because the bone has a tenuous blood supply and, as a result, there is a high rate of avascular necrosis. Most talar fractures require short-leg casting for 6 to 8 weeks, but some require open reduction and internal fixation. Patients should be nonweight bearing. Disposition is based on recommendations by the orthopedist. Patients can be referred for an outpatient CT or MRI for suspected talar dome fractures (10).
Subtalar Dislocation
A subtalar dislocation involves the talocalcaneal and talonavicular joints (without disruption of the tibiotalar joint). This injury results from a significant torsional force usually causing a medial or lateral dislocation. There is usually an obvious deformity of the foot, but swelling can occasionally mask the deformity.
As with any dislocation, assessing the neurovascular status is important. Although uncommon, compromised neurovascular status is an indication for immediate reduction. Plain films of the foot are diagnostic; the AP view is most likely to reveal the subtalar dislocation.
Subtalar dislocations require urgent closed reduction either under conscious sedation or general anesthesia. Reduction is performed by flexing the knee and applying longitudinal traction on the foot with initial reproduction of the injury followed by reversal of the deformity. If closed reduction in the ED is unsuccessful, orthopedic consultation is essential. Successfully reduced subtalar dislocations should be immobilized with a short-leg posterior splint and sugar tongs (U-splint). After reduction, if orthopedic consultation is not available in the ED, follow-up should occur within 24 to 48 hours.
Lisfranc Fracture–Dislocation
The Lisfranc joint is the joint between the midfoot and forefoot (metatarsals and phalanges). Direct trauma or hyperdorsiflexion of the Lisfranc joint (e.g., in a motor vehicle collision) can result in a Lisfranc fracture–dislocation, defined as a fracture at the base of the second metatarsal or second cuneiform with dislocation of the lateral four metatarsals. The occurrence is rare but results in significant morbidity when there is a delay in treatment. This particular fracture has a high misdiagnosis rate of approximately 20%.
The foot is usually very swollen and tender over the tarsometatarsal joint. Plantar ecchymosis has been described as a relatively common finding in patients with Lisfranc fracture–dislocations (17).
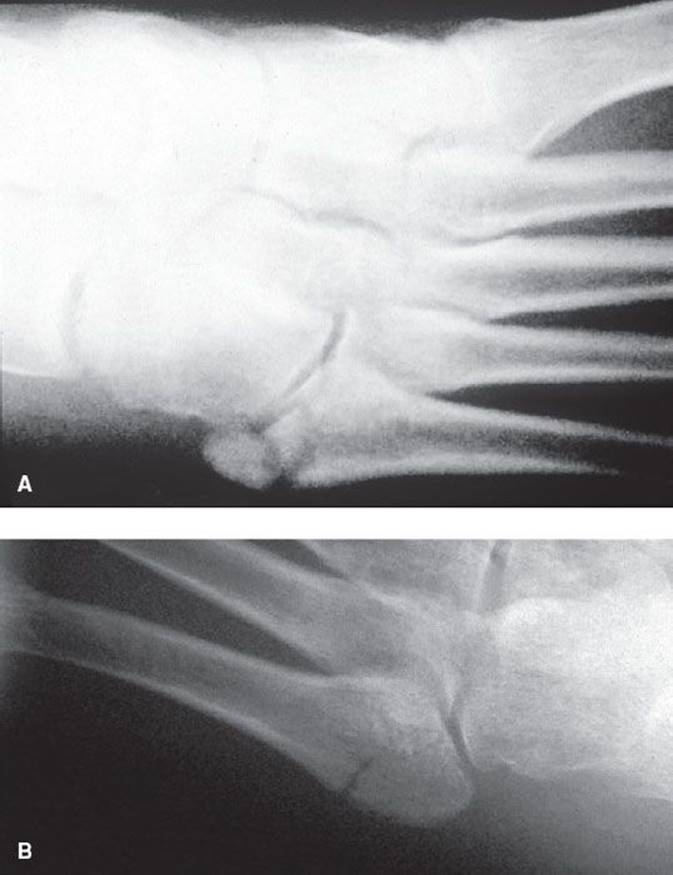
When examining an AP foot x-ray, the physician should look for a fracture at the base of the second metatarsal and assess alignment of the cuneiform bones with the metatarsals. The space between the bases of the metatarsal bones is widened (Fig. 45.6). The standard foot x-ray series can miss up to 50% of Lisfranc fractures. If there is suspicion and standard plain films are normal, then stress- or weight-bearing AP and lateral views can be obtained to reveal the widening (17).

FIGURE 45.6 Radiograph of a Lisfranc dislocation: (a) first metatarsal; (b) second metatarsal; (c) third, fourth, and fifth metatarsals, which have been dislocated laterally.
Lisfranc fracture–dislocations require orthopedic consultation in the ED. These injuries require open reduction and internal fixation to improve outcome and reduce complications. If an orthopedic consultant is not immediately available, the physician should provide analgesia and place the patient in a short-leg posterior splint, preferably with a sugar tong splint. The patient should be nonweight bearing. Orthopedic follow-up should occur within 24 to 48 hours, and the timing of definitive treatment and the degree of reduction are critical to the outcome.
Midfoot Fractures
Fractures of the midfoot (cuboid, navicular, and cuneiforms) are rare and usually occur from direct blunt trauma. Most midfoot injuries involve a combination of fractures, isolated bone fractures are the exception. There is typically focal tenderness and swelling over the fractured bones.
Midfoot fractures are usually visible on plain radiographs. Nondisplaced fractures can be immobilized and nonweight bearing with a posterior splint. They can be discharged with prompt orthopedic follow-up for evaluation and a short-leg cast for 6 to 8 weeks.
Proximal Fifth Metatarsal Fractures
Fractures of the fifth metatarsal usually result from an ankle inversion mechanism. The Jones and pseudo-Jones fractures present with pain over the base of the fifth metatarsal. A Jones fracture is a transverse fracture at the proximal diaphysis of the fifth metatarsal. A pseudo-Jones or Dancer’s fracture is an avulsion fracture of the proximal end of the fifth metatarsal by the peroneus brevis tendon resulting from plantar flexion and inversion of the foot.
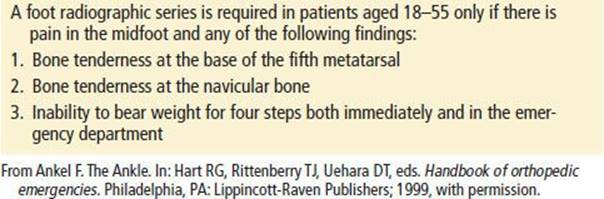
Palpation of the fifth metatarsal is essential in any patient with an ankle-twisting injury to determine the need for foot films in addition to ankle films to make the diagnosis of Jones or pseudo-Jones fractures (eFig. 45.6). The Ottawa criteria are useful to determine the need for foot x-rays (Table 45.2).
eFIGURE 45.6 Proximal fifth metatarsal injuries. A: Avulsion or pseudo-Jones fracture. B: Jones fracture.
TABLE 45.2
Ottawa Criteria for Foot Radiographs
Jones fractures have a high incidence of delayed healing or nonunion. Orthopedic evaluation in the ED is recommended. If immediate consultation is not available, the foot should be immobilized with a posterior splint with or without a sugar tong splint, and the patient should have an orthopedic referral in 24 to 48 hours. Athletes are usually treated operatively, and nonathletes are treated with a walking cast for 4 to 6 weeks (17).
Pseudo-Jones fractures are stable and can be treated with a hard-sole shoe or a Jones dressing with weight bearing as tolerated. A Jones dressing is a bulky dressing used for injuries that require moderate immobilization when swelling is expected. The dressing consists of multiple layers: a thick layer of Webril (cotton roll), followed by an ACE wrap (elastic bandage), then another layer of Webril and another layer of ACE wrap.
Forefoot Injuries
The most common metatarsal and phalangeal fractures result from direct trauma and present with swelling, tenderness, and ecchymosis. Dislocations of the metatarsophalangeal (MP) and interphalangeal (IP) joints are caused by dorsiflexion and compression of the phalanges. In addition to swelling and tenderness, there is usually visible deformity.
More subtle stress fractures can occur to the second and third metatarsal bones. During push off, the maximum load is placed on the forefoot. As a result, these bones are prone to stress fractures. Patients usually have a history of increased walking, jogging, or marching activity, and they complain of poorly localized pain in the foot with minimal swelling (17).
The neurovascular status of the foot should be documented, especially the presence of the dorsalis pedis pulse. Dislocations with neurovascular compromise should be reduced immediately; otherwise it is prudent to assess the plain films for fractures before manipulation.
Plain films are adequate to evaluate for acute traumatic fractures and dislocations. However, initial radiographs will often not reveal stress fractures. Stress fractures are usually apparent 2 to 3 weeks later as callus formation or periosteal reaction, but they can also be detected earlier by bone scan.
In patients with MP joint dislocations, the phalanx is usually dorsally displaced. Reduction is performed by hyperextension, followed by longitudinal traction and dorsal pressure. Patients can be discharged with a dorsal toe splint, crutches, and orthopedic follow-up. IP joint dislocations can occur in a dorsal or volar direction. The reduction technique is similar for both types. Patients can be discharged after the injured toe is buddy taped to the adjacent toe. Patients should follow up with an orthopedist in a week because of the possibility of unstable dislocations.
Nondisplaced fractures should be placed in a short-leg splint and follow-up should be arranged. Displaced fractures require reduction by an orthopedist. Stress fractures or suspected stress fractures require close orthopedic follow-up and discontinuation of any pain-producing activity.
Turf Toe
Turf toe is a sprain of the MP joint of the great toe that results from pushing off of a hyperdorsiflexed toe. The toe is tender and swollen. An x-ray should be obtained to rule out fracture. Like most sprains, the treatment is joint rest with a hard-soled shoe limiting dorsiflexion, ice and analgesia, and ibuprofen or acetaminophen for pain. Orthopedic consultation is necessary only for patients with persistent pain beyond 1 to 2 weeks.
Plantar Fasciitis
Patients with plantar fasciitis complain of pain in the arch and heel of the foot that is worse in the morning or when climbing stairs. There is usually a history of overuse (hill running or sprinting) or poor arch support. Evaluation reveals tenderness over the plantar fascia and reproduction of the pain with dorsiflexion of the toes. If there is focal tenderness or a stress fracture is suspected, plain films of the foot are indicated. Treatment involves rest, ice, analgesia, and splinting for comfort. Follow-up with an orthopedist, sports medicine specialist, or physical therapist is recommended. These patients may require evaluation for an orthotic device or exercise program.
Puncture Wounds
Plantar puncture wounds have the potential for serious complications (e.g., soft tissue infection and osteomyelitis). Wounds should be inspected, cleansed, irrigated, and explored, especially if a foreign body is suspected. Deep probing, extensive coring, or debridement of vital tissue does not improve outcome. Radiographic studies are warranted if the history suggests a foreign body and exploration is inconclusive. Puncture through tennis shoes have been implicated in pseudomonal infections, but most soft tissue infections are due to streptococcus and staphylococcus species. Most cases of osteomyelitis are due to pseudomonas (18,19). The use of prophylactic antibiotic for puncture wounds to the foot is controversial. Given the risk of complications such as osteomyelitis, its use should be considered. If the decision is made to use antibiotics, a first-generation cephalosporin should be given. For clean, superficial wounds with no concern for retained foreign body, local wound care is the sufficient treatment. A wound check in 48 hours is recommended for contaminated wounds and those with possible retained foreign bodies.
Patients presenting with infection after a puncture wound should be treated with broad-spectrum antibiotics, and the physician should search for a foreign body via exploration, radiographs, or CT scan. Surgical consultation may be needed.
KEY TESTING
• Perform a complete neurovascular examination distal to injury
• Assess for ankle instability with provocative testing
• Obtain three-view ankle x-rays or three-view foot x-rays according to Ottawa Ankle Rule
• Obtain stress- or weight-bearing views to assess for Lisfranc injury if there is a high suspicion
CRITICAL INTERVENTIONS
• In a patient with neurovascular compromise and a visibly deformed extremity, reduce the fracture emergently to restore sensation and blood flow.
• Obtain radiographic confirmation in patients with dislocated joints without neurovascular compromise and then reduce the joint.
• In patients with open fractures, administer antibiotics and obtain emergent orthopedic consultation for wash-out and admission.
• Provide appropriate follow-up care for all patients with ankle and foot injuries.
DISPOSITION
Most patients with ankle or foot injuries should have close follow-up in the event that symptoms do not improve and further investigation and treatment are required. Exceptions are minor ankle sprains and turf toe. Patients who are sent home in a posterior short-leg or sugar tong splint should have orthopedic follow-up within 24 to 48 hours for reassessment and definitive immobilization with a cast.
Orthopedic consultation should be obtained in the ED for the following fractures and dislocations: plafond, bi-, or trimalleolar fractures; calcaneal, talar, or Jones fractures; Lisfanc fracture/dislocation; and ankle and subtalar dislocations. If orthopedic consultation is not immediately available, appropriate reduction or splinting should be performed, and arrangements should be made for orthopedic evaluation within 24 to 48 hours. Open fractures will require immediate orthopedic consultation.
Common Pitfalls
• Failure to palpate the base of the fifth metatarsal to evaluate for a Jones fracture.
• Treating a Jones fracture as a pseudo-Jones fracture.
• Failure to squeeze the proximal tibia–fibula area to evaluate for a Maisonneuve fracture in patients with presumed ankle sprains.
• Applying the Ottawa Ankle Rules to patients younger than 5 and older than 55 years.
• Failure to recognize a Lisfranc fracture.
• Treating grade I and II ankle sprains with prolonged immobilization rather than early mobilization and exercise.
ACKNOWLEDGMENTS
The author gratefully acknowledges the contributions of Daniel R. Martin and Wenzel Tirheimer to the content of this chapter.
REFERENCES
1. Ivins D. Acute ankle sprain: An update. Am Fam Physician. 2006;74(10):1714–1720.
2. Title CI, Katchis SD. Traumatic foot and ankle injuries in the athlete. Orthop Clin North Am. 2002;33:587–598.
3. Wedmore IS, Charette J. ED Evaluation and treatment of ankle and foot injuries. Emerg Med Clin North Am. 2000;18:85–113.
4. Leddy JJ, Smolinski RJ, Lawrence J, et al. Prospective evaluation of the Ottawa Ankle Rules in a university sports medicine center. With a modification to increase specificity for identifying malleolar fractures. Am J Sports Med.1998;26:158–165.
5. Dowling S, Spooner CH, Liang Y, et al. Accuracy of Ottawa Ankle Rules to exclude fractures of the ankle and midfoot in children: A meta-analysis. Acad Emerg Med. 2009;16:277–287.
6. Bachmann LM, Kolb E, Koller MT, et al. Accuracy of Ottawa ankle rules to exclude fractures of the ankle and midfoot: Systematic review. BMJ. 2003; 326:417.
7. Swain RA, Holt WS Jr. Ankle injuries. Tips from sports medicine physicians. Postgrad Med. 1993;93:91–92, 97–100.
8. Wilkons J, Bisson LJ. Operative versus nonoperative management of acute Achilles tendon ruptures: A quantitative systematic review of randomized controlled trials. Am J Sports Med. 2012;40(9):2154–2160.
9. Trevino S, Baumhauer JF. Tendon injuries of the foot and ankle. Clin Sports Med. 1992;11:727–739.
10. Newton EJ. Emergency department management of selected orthopedic injuries. Emerg Med Clin North Am. 2009;27(3):545.
11. Chan GM, Yoshida D. Fracture of the lateral process of the talus associated with snowboarding. Ann Emerg Med. 2003;41(6):854–858.
12. Wijdicks CA, Rosenbach BS, Flanagan TR, et al. Injuries in elite and recreational snowboarders. Br J Sports Med. 2014;48:11–17.
13. Boon AJ, Smith J, Zobitz ME, et al. Snowboarder’s talus fracture: Mechanism of injury. Am J Sports Med. 2001;29:333–338.
14. Funk JR, Srinivasan SC, Crandall JR. Snowboarder’s talus fractures experimentally produced by eversion and dorsiflexion. Am J Sports Med. 2003;31:921–928.
15. Von Knoch F, Reckord U, von Knoch M, et al. Fracture of the lateral process of the talus in snowboarders. J Bone Joint Surg Br. 2007;89-B:772–777.
16. Ross G, Cronin R, Hauzenblas J, et al. Plantar ecchymosis sign: A clinical aid to diagnosis of occult Lisfranc tarsometatarsal injuries. J Orthop Trauma. 1996;10:119–122.
17. Hatch RL, Alsobrook JA, Clugston JR. Diagnosis and management of metatarsal fractures. Am Fam Physician. 2007;76(6):817–826.
18. Niall DM, Murphy PG, Fogarty EE, et al. Puncture wound related pseudomonas infections of the foot in children. Ir J Med Sci. 1997;166:98–101.
19. Pennycook A, Makower R, O’Donnell AM. Puncture wounds of the foot: Can infective complications be avoided? J R Soc Med. 1994;87:581–583.