Benjamin S. Heavrin, Ian D. Jones, and Corey M. Slovis
Infective endocarditis (IE) is an infection of the endothelial lining of the heart usually involving the heart valves. The first reported autopsy evidence of the disease dates to 1647. In 1885, Sir William Osler further reported on the autopsy and clinical findings of the disease in a series of classic papers published in the British Medical Journal.
Traditionally, IE has been divided into two forms: (i) a relatively insidious, chronic disease, subacute bacterial endocarditis (SBE), and (ii) a more abrupt-onset, fulminant form, acute bacterial endocarditis (ABE).
Although there is broad geographic variation in cases of IE, the overall incidence and mortality of IE had remained unchanged for the last 30 years (1). Despite the unchanged number of overall cases of IE, the proportion of cases involving increasing patient age, prosthetic valve infection, and nosocomial infection is increasing (2–4). As the incidence of these cases has increased, the incidence of IE from rheumatic heart disease has decreased and is now relatively uncommon (5). Additionally, the incidence of endocarditis due to Staphylococcus aureus, once primarily associated with intravenous (IV) drug abuse, is now the leading cause of IE in many parts of the world (6).
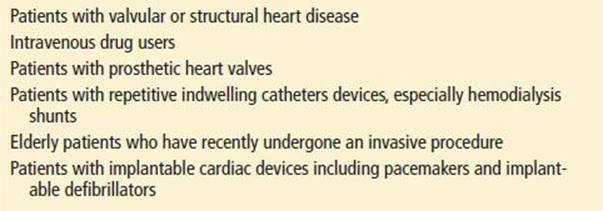
The incidence of IE is highly variable depending on predisposing anatomic risk factors, including prosthetic valves, anatomic valve abnormalities, degenerative valvular disease, and the presence of mechanical intracardiac devices such as pacemakers and implanted defibrillators (4). An increase in risk is also seen in patients with prolonged exposure to indwelling IV catheters, hemodialysis patients, and intravenous drug users (IVDUs) (Table 88.1). Reviews of multiple studies have shown that IE remains uncommon in patients with healthy valves and no identifiable risk factors. Despite considerable advances in detection and therapy, IE remains a challenge to diagnose, and mortality continues to be high.
TABLE 88.1
Emergency Department Patients at Highest Risk for Endocarditis
The organisms most commonly causing IE have also changed. As IE has evolved, the frequency of Streptococcus viridans as a causative agent has decreased, whereas the incidence of Staphylococcus species has risen. S. aureus is now the most common cause of all types of IE and the incidence of methicillin-resistant S. aureus (MRSA) in these isolates has risen dramatically (3,6,7). S. aureus endocarditis also confers a higher risk of embolism, neurologic involvement, persistent bacteremia, and overall mortality than does infection caused by other organisms (6,7). In addition to the changing spectrum of infection, methods for elucidating the causative organism in endocarditis have been improved, including better culture techniques, serologic testing, and the use of polymerase chain reaction (PCR).
There are four steps in the development of SBE: (i) a hemodynamically defective valve produces turbulent blood flow and endothelial disruption; (ii) a sterile platelet–fibrin thrombus forms on the damaged valve lining; (iii) transient bacteremia infects the thrombus; and (iv) high titers of antibodies to the infecting organism are produced. Furthermore, the infecting organism must have the capability to adhere to injured endothelium. Bacterial endocarditis may also develop on previously normal native and prosthetic heart valves. In these cases, the only necessary measure is an inoculum of a highly invasive organism.
Once endocarditis develops on a valve, the clinical manifestations are attributable to the following series of events: (i) local destruction and malfunction of the cardiac valve; (ii) invasive infection of contiguous structures of the heart; (iii) continuous bacteremia, leading to distant infections; (iv) embolization of vegetations that break off from the valve; and (v) an antigen–antibody response, leading to immune-mediated complications.
CLINICAL SUBGROUPS
IE is often classified into one of four distinct patient-centered clinical groups: (i) patients with a damaged native valve; (ii) patients with prosthetic valves (further classified as either early or late infection); (iii) IVDUs; and (iv) patients with nosocomial IE (3). A fifth category has also recently been described: health care-related endocarditis related to implantable intracardiac devices, invasive procedures, and chronic hemodialysis (8). IE in hemodialysis patients is becoming increasingly more common. It has been reported that patients on hemodialysis make up 30% of all cases of hospital-acquired IE and have a 50 to 60 times higher incidence of IE than the rate in the general population (9).
DAMAGED NATIVE VALVE
Any condition causing an alteration in the normal structure of the cardiac valves (e.g., rheumatic, degenerative, and congenital cardiac abnormalities) can predispose a patient to IE. Patients with native-valve IE are most likely to develop a syndrome similar to the classic SBE, a relatively chronic infection with only left-sided cardiac involvement, often with a streptococcal organism. The mitral valve is the most common valve to be infected in the native-valve group. Isolated mitral involvement occurs in 35% to 45% of cases, isolated aortic valve involvement in 15% to 35%, and involvement of both valves in 15% to 30% (10). Mitral valve prolapse by itself is not a risk factor for IE unless accompanied by regurgitation (3). Tricuspid valve and pulmonic involvement is relatively rare in native-valve IE.
Staphylococcus species have now surpassed Streptococcus species as the most common organism causing native-valve IE, being responsible for 44% of native-valve IE, whereas Streptococcus and Enterococcus species account for 31% and 10% of cases, respectively (3). S. aureus and coagulase-negative Staphylococcus are probably introduced via the skin and are most likely to cause infection in patients on hemodialysis and those who have diabetes, implantable cardiac devices, chronic illness, and the elderly or otherwise debilitated (6,7). S. aureus is now the predominant pathogen in all types of IE (3,6). There has also been a significant rise in the percentage of these cases caused by MRSA. Though overall mortality is not statistically different, there is evidence that MRSA endocarditis may actually confer a lower risk for embolism but a higher risk for persistent bacteremia (6).
S. viridans is by far the most common Streptococcus species causing IE. S. viridans bacteremia and subsequent valvular seeding traditionally have been attributed to bacterial seeding during dental procedures in patients with pre-existing valvular or structural heart disease. This presumed cause-and-effect relationship has been increasingly questioned and, to date, there is no compelling evidence that dental procedures are the cause of a significant number of cases of IE. Additional organisms causing native-valve IE include Streptococci bovis and Enterococcus faecalis (3). These infections are more commonly introduced by bowel and urologic infections or procedures, especially in the elderly. Gram-negative organisms, fungi, polymicrobial infections, and diphtheroids are seldom contributors to native-valve IE (3,7).
INTRAVENOUS DRUG USERS
IVDUs are one of the leading groups at high risk for developing IE. Between 5% and 8% of hospital admissions in IVDUs are due to endocarditis (11). Because IV cocaine users inject themselves so frequently relative to other IVDU groups, they appear to have the highest risk of developing IE. Their increased relative risk may also be a result of factors such as lack of heating the drug before injection, needle sharing, immunosuppression from the drug, or direct valvular damage caused by cocaine (12). There are conflicting data in the literature regarding the predominance of right-sided versus left-sided endocarditis in IVDUs. Although left-sided endocarditis is seen in all patient populations, right-sided endocarditis is rarely seen outside of the IVDU population. Thirty-two percent of IE caused by IVDU involves the mitral valve, 19% the aortic valve, and almost all of the remaining cases involve the tricuspid valve (11). In right-sided endocarditis, pulmonic valve involvement is rare and is seen in <1% of patients (11).
Patients who inject illicit drugs often are infected with organisms that are normal skin flora. S. aureus is the most common causative agent in this group of patients, accounting for approximately 69% to 80% of cases Streptococcusspecies are the next most common. Interestingly, coagulase-negative staphylococci are rarely isolated from this patient population (3,11). Fungal infection and large (>2 cm) valve vegetations both portend a significantly worse prognosis in this patient population and may make these patients candidates for early surgery.
PROSTHETIC VALVE INFECTIVE ENDOCARDITIS
As the number of prosthetic valve surgeries increases, the number of cases of prosthetic valve infective endocarditis (PVIE) continues to rise. Once making up only 1% to 5% of the total number of cases of IE, PVIE now accounts for 20% of all cases of IE (13). Individuals with PVIE tend to be significantly older, have a lower likelihood of using injectable drugs, and have a higher likelihood of health care–associated infection and a higher mortality than patients with native valve infective endocarditis (13).
Early-Onset Prosthetic Valve Infective Endocarditis
Patients with early-onset PVIE either are contaminated intraoperatively or develop infection in the perioperative period, which is defined as 60 days after surgery (13,14). The rate of infection is highest in the first 3 months after surgery and diminishes to between 0.3% to 0.6% per year thereafter (14). Early prosthetic valve infections are predominantly nosocomial in etiology. The most common pathogens encountered in the first 2 months after surgery are Staphylococcus species (S. aureus, 36%, and coagulase-negative staphylococci, 15%) (13). S. aureus is now the most frequent organism associated with early-onset PVE with more than 50% of these isolates being methicillin-resistant (13). Though the overall number of cases of early-onset PVIE seems to be falling in comparison to late-onset PVIE, mortality remains very high, with cases due to S. aureus conferring a significantly higher mortality than infection from other organisms (13). Other organisms encountered less frequently include S. viridans,Enterococcus species, gram-negative organisms, and fungi.
Late-Onset Prosthetic Valve Infective Endocarditis
The predominant organisms responsible for late-onset PVIE continue to be Staphylococcus species. Coagulase-negative staphylococci (20%) and S. aureus (18%) were the predominant causative organisms in a recent large-scale observational study (13). In this same population, MRSA made up <20% of the staphylococcal isolates whereas Enterococcus species (12%), Viridans streptococci (10%), and S. bovis(7%) also caused a significant number of infections.
Mechanical valves and tissue valves have an approximately equal incidence of infection (overall incidence, 2.2% to 4.4%), but mechanical valves are more likely to develop early-onset PVIE. Mechanical valves tend to develop perivalvular abscesses, myocardial abscesses with conduction delays, pericarditis, and regurgitation caused by perivalvular leaks. An acute regurgitant murmur caused by partial dehiscence of the valve is a surgical emergency because severe heart failure can develop rapidly or the valve can undergo total dehiscence. Tissue valves, however, are more likely to develop leaflet tears, also resulting in new regurgitant murmurs and heart failure. Valvular stenosis is also a potential complication with tissue valves.
CLINICAL PRESENTATION
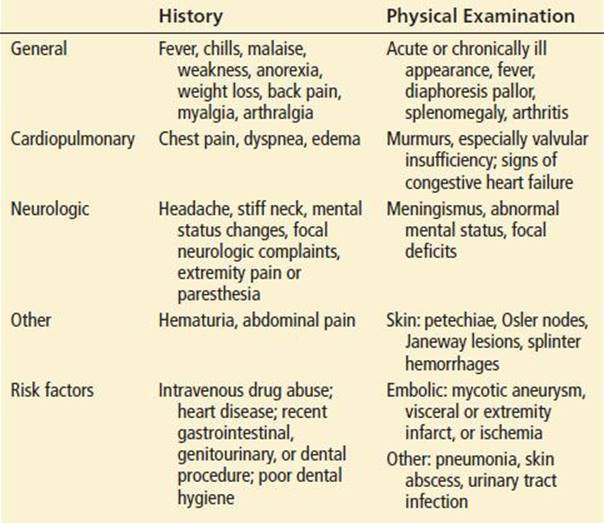
Patients with IE may present acutely with fulminant heart failure and sepsis; with a chronic, indolent, nonspecific disease process; or with a syndrome intermediate between the two extremes. Because of the overlap, the artificial separation of ABE and SBE is usually not clinically helpful. Table 88.2 lists the historical and physical findings seen most often in IE.
TABLE 88.2
Historical and Physical Findings Suggestive of Endocarditis
Complications
Cardiac
Cardiac complications of IE may involve any of the three layers of the heart. Endocardial damage of the valve may result in valvular destruction and variable degrees of congestive heart failure (CHF). CHF is the most common cause of death in patients with IE (15). Severe failure is usually a result of acute aortic insufficiency and, if not promptly amenable to medical intervention, is an indication for emergent valve replacement surgery (15). Myocarditis or perivalvular abscess results when the infecting organism invades the contiguous myocardium.
Electrocardiographic (ECG) abnormalities in cases of IE are much more likely to be seen with perivalvular spread of infection and confer a significant increase in mortality (16). The majority of ECG abnormalities are conduction abnormalities. The infection involving the conduction system results in conduction delays, bundle-branch block, or complete heart block. Mortality is significantly higher if there is a presence of infranodal block (15). Intracranial catastrophes may occur if thrombolytics are used in cases in which complications of IE cause ECG changes that mimic those of acute ischemia resulting from coronary artery disease.
Additional complications include aortocardiac fistula, perforated valves, or perforation of the myocardium (15). A perforated myocardial abscess may result in a purulent pericarditis. Large emboli to the coronary arteries can cause acute myocardial infarction or sudden death (17).
Central Nervous System
Central nervous system complications occur not only in 20% to 40% of patients with IE but may be the presenting complaints in a significant number of cases (7). Mortality is significantly higher in patients with IE and neurologic manifestations. Embolic cerebral infarction or stroke is the most common event and usually involves the middle cerebral artery or its branches (18). Intracerebral hemorrhage, isolated seizures, and transient ischemic attacks are also reported complications (18). Cerebral mycotic aneurysms resulting from septic emboli eroding the vessel wall may remain asymptomatic or may enlarge, leak, or rupture and present as subarachnoid hemorrhage, cerebral abscess, or classic bacterial meningitis (19). A syndrome consisting of lethargy, delirium, hallucinations, and psychosis (i.e., toxic encephalopathy) may occur (17). When these findings are accompanied by a stiff neck and cerebrospinal fluid consistent with aseptic meningitis, the patient has meningoencephalitis. The cause is not clear, but multiple microinfarcts or microabscesses may be responsible. The likelihood of an embolic event decreases markedly after the initiation of antibiotics (18).
Emboli and Immunologic Responses
Peripheral embolization can occur anywhere in the body and is seen in up to one-third of patients with IE (19). In addition to the brain (50% of all events) and heart, other important areas of embolization are the splenic, renal, mesenteric, and extremity vasculature. The emboli result in endarteritis, mycotic aneurysm, local abscess formation, and distal infarction. Studies have shown that patients with large valve vegetations have a worse prognosis most likely because of a higher likelihood of embolic sequelae (17). It is not clear how many of the signs and complications of IE are immune complex–mediated, although it is thought that glomerulonephritis, aseptic arthritis, and most of the classic skin manifestations are immune-related. Prosthetic joint infections and vertebral osteomyelitis may, if seen, be likely a result of bacteremia during the acute phase of the infection (15).
ED EVALUATION
A definitive diagnosis of endocarditis relies on a combination of histologic, microbiologic, clinical, and echocardiographic findings. The Duke criteria, first proposed in 1994, have been well validated, and the modified Duke Criteria remain the gold standard for diagnosing IE. Because culture data are unavailable and most emergency departments (EDs) have limited access to transesophageal echocardiography (TEE), a definitive diagnosis of IE is often impossible to obtain at the time of initial presentation. Therefore, the Duke criteria are of limited use in ED patients, and the clinician must rely on history, physical findings, and other rapidly available tests that will support a presumptive diagnosis of IE and the initiation of additional directed diagnostic testing and empiric antibiotic therapy.
Patients with IE often have numerous vague and nonspecific complaints. The classic patient presenting with persistent fever of unknown origin represents only a fraction of endocarditis cases (15). Most patients have nonspecific extracardiac complaints including fever, malaise, anorexia, and weakness. Approximately one-half of patients report headache, weight loss, night sweats, arthralgias, and myalgias (7). A history of back pain, rash, or dyspnea or a spectrum of neuropsychiatric symptoms is not uncommon in IE (7). Clinicians, however, seldom initially attribute these less-common symptoms to IE. Physicians should also be aware of patients at higher risk for IE such as patients with diabetes, immunocompromised patients, valvular cardiac disease patients, IVDUs, patients with indwelling cardiac devices (pacemakers and implanted defibrillators), and patients receiving chronic hemodialysis (1,3,7,9). Patients should be asked about recent dental, gastrointestinal, and urologic procedures. Elderly patients, in particular, may not volunteer or may forget to relate these high-risk procedures. Young patients who are being evaluated “for the flu” or other febrile illnesses seldom provide information about IV drug use unless specifically questioned.
Physical findings suggestive of endocarditis are listed in Table 88.2. Patients with IE may appear acutely or chronically ill. Nearly all nonimmunocompromised patients have fever. The presence of unexplained fever for more than 1 week should raise the clinician’s suspicion for endocarditis (17). Other abnormal vital signs, especially tachycardia, are relatively common. It is important for the clinician to be vigilant because many of the symptoms of endocarditis are nonspecific and many of the classic findings of endocarditis are not commonly seen.
A careful cardiac examination is critical in patients suspected of having IE. The majority of patients with IE will have a murmur and many of these will be pre-existing (7). Patients most likely to lack murmurs are those with acute IE. Therefore, lack of a murmur in an IVDU should never decrease the suspicion for IE. On the other hand, a new aortic or mitral regurgitant murmur in a febrile patient is very strong evidence for the disease (17). The cardiac examination should also seek any findings suggestive of heart failure. Findings of new-onset heart failure, especially in younger patients without a history of cardiac disease, should prompt a high index of suspicion for endocarditis. Rarely, a large (usually fungal) vegetation may block the outflow tract, resulting in a new stenotic murmur.
A variety of skin lesions are considered classic for IE, but these are relatively uncommon. Petechial lesions may be found in different locations. Splinter hemorrhages are tiny red, purple, brown, or black splinter-like lesions that appear under the fingernails. They are seen in up to 20% of patients with IE, but they are also found in approximately 8% of all hospitalized patients. Osler nodes are small, painful, tender erythematous nodules that are most commonly seen in the distal finger pads; they occur in 5% to 20% of patients. Janeway lesions are small, flat, nontender red spots on the palms and soles; they occur in only about 10% of patients with IE. Conjunctival petechiae may occur in approximately 10% of patients. Roth spots are retinal petechial hemorrhages with central pallor, which may be seen in 10% to 25% of patients with IE. The remainder of the physical examination may reveal abnormal abdominal or neurologic findings. Splenomegaly is a common finding, and a tender, enlarged liver is often noted. The presence of a splenic abscess should raise a high suspicion for IE (19). Neurologic examination may reveal signs consistent with meningitis, encephalitis, embolic stroke, or a leaking aneurysm. Some patients present with subtle mental status changes or behavioral symptoms that appear to be psychiatric in nature (17).
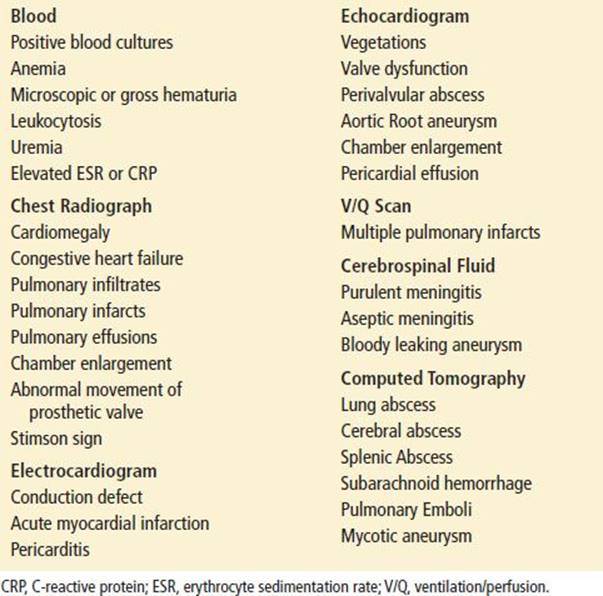
There are numerous nonspecific laboratory findings in IE (Table 88.3). Normochromic, normocytic anemia occurs in up to 75% of patients and microscopic hematuria occurs in nearly 50%. Leukocytosis is seen in about 50% of cases and, thus, its absence should not be used to rule out the diagnosis. Studies differ in regard to the value of the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) in patients ultimately diagnosed with IE. Both tests lack specificity and neither test has perfect sensitivity to rule-out a diagnosis of IE.
TABLE 88.3
Laboratory and Diagnostic Findings in Endocarditis
The most important part of the laboratory evaluation is the blood culture, as precise identification of the organism is critical in tailoring appropriate antibiotic therapy. Approximately 20 mL of blood (not 5 to 10 mL) should be drawn for each set of blood cultures and sent for aerobic and anaerobic cultures. The diagnosis of possible endocarditis should appear on the specimen label so that the laboratory will hold the specimen for at least 3 weeks to ensure detection of slow-growing organisms. Whenever possible, a minimum of three blood cultures should be performed from three separate sites and should be drawn over a period of approximately 1 hour.
Blood cultures may be positive in the majority of patients with IE. Even in cases wherein the blood cultures are negative, other tests can be obtained that may aid in a definitive diagnosis. If the cultures are sterile in cases of proven endocarditis, Coxiella, Bartonella, and Chlamydia species may be identified by the use of serology, immunohistochemical staining, and PCR (7). To maximize the chances of a positive culture and to minimize the confusion caused by contaminant, multiple cultures are recommended as described above in the IE work-up. Recent antibiotic use by the patient and infection with fastidious or slow-growing organisms are the two major reasons for negative cultures in the context of IE. The patients who most commonly have negative cultures are drug users, patients with prosthetic valves, and those who have recently received antibiotics.
Although usually normal, the ECG should always be carefully examined for evidence of pericarditis, ischemia, infarction, conduction delay, or any degree of heart block. These changes may be indirect evidence for the coexistence of myocarditis, myocardial abscess, pericarditis, or coronary artery embolism (16).
The chest radiograph of patients with IE is usually normal. Signs of CHF, including cardiomegaly, isolated chamber enlargement, and abnormal vascular patterns, provide valuable information regarding abnormal valvular or cardiac function. The chest radiograph may also reveal pneumonia, especially in patients who are IVDUs. Multiple pulmonary infarcts or nodular infiltrates suggest right-sided disease, usually tricuspid valve endocarditis. In PVIE, a double shadow of a mechanical valve, known as Stimson sign, indicates movement of a valve that has undergone partial dehiscence.
Echocardiograms are almost always performed in patients who are suspected of having IE. The finding of vegetation is a very strong evidence for the diagnosis of IE. However, a negative echocardiogram should never be used as the definitive test to rule out IE, as up to one-third of patients with IE have nondiagnostic echocardiograms (20). Although it is probably more appropriate to begin with transthoracic echocardiography (TTE), TEE should be performed in all patients in whom there is strong suspicion for IE (20). The greater value of TEE lies in its ability to provide greater spatial resolution of cardiac anatomy and the fact that by placing the probe in the esophagus, limitations from overlying structures and chest wall structures are eliminated (20). Various studies have shown sensitivities for TTE in diagnosing IE at between 18% and 63%. This compares to 48% to 100% sensitivity for TEE in diagnosing IE. Furthermore, TEE is far more sensitive in diagnosing accompanying pathology such as perivalvular abscess. Because of their anterior location, aortic root abscesses may be better visualized with TTE (20). Echocardiographic detection of valve malfunction, chamber enlargement, or an associated pericardial effusion may also be helpful in the clinical management of IE. Mechanical valves are too echo-dense for TTE to be of significant value, and valvular function should instead be evaluated by either TEE or cinefluoroscopy (20,21).
KEY TESTING
• Obtain at least three sets of high-volume blood cultures from separate sites over a period of 1 hour in stable patients suspected of having endocarditis.
• Obtain a transthoracic echocardiogram (TTE) to evaluate for vegetations and valvular insufficiency, followed by a TEE in conjunction with cardiology consultation based on the TTE results.
• Obtain an ECG and chest X-ray to evaluate for conduction disease and signs of heart failure or secondary infectious processes such as pneumonia.
• Laboratory studies such as ESR, CRP, and white count may influence the probability of a diagnosis but are never sufficient to rule-in or rule-out a diagnosis of IE.
ED MANAGEMENT
Definitive therapy for IE is guided by the infecting organism’s sensitivity to specific antimicrobial agents. If a stable patient presents to the ED with the possibility of IE, it is best to obtain at least three sets of blood cultures from three separate sites over a period of 1 hour. Administration of antibiotics reduces the positive blood culture rate by as much as 40% (21). The patient should be admitted to an inpatient area, and subsequent care and additional culturing should be provided at the direction of the patient’s physician or infectious diseases consultant. Antibiotics should, however, be started in the ED if the patient appears septic, is elderly, is debilitated, is immunocompromised, has concomitant pneumonia, is in heart failure, or is hemodynamically unstable. Once blood culture and sensitivity data are available, optimal therapy should follow the most recent AHA guidelines (21). The choice of optimal empiric therapy for presumed IE in a specific patient type is guided by the most commonly suspected organism and the organism’s antibiotic sensitivities.
Empiric Antibiotic Coverage
There is no universal agreement on optimal empiric antibiotic therapy. However, ED physicians can begin therapy by choosing an antibiotic regimen that provides broad-spectrum bactericidal coverage for the most common organisms causing IE. The authors’ specific recommendations for empiric therapy for use in the ED appear in Table 88.4.
TABLE 88.4
Empiric Emergency Department Therapy for Presumed Endocarditis Prior to Culture Results
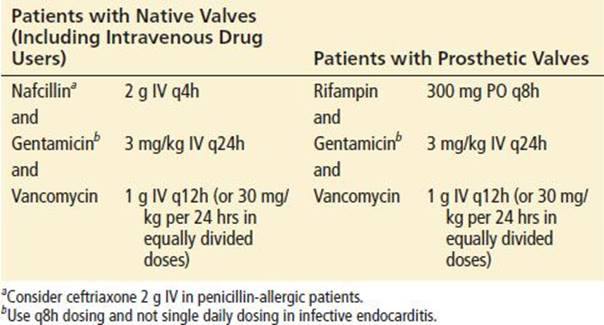
The recommendations attempt to provide broad coverage divided into two regimens: one for presumed IE in a seriously ill patient with native valves and a second for presumed IE in a patient with one or more prosthetic valves. The regimens are designed to be easily remembered and do not address whether the patient may have developed IE in association with IV drug abuse or how long ago the prosthetic valve was implanted. In addition, with the increasing frequency of all types of IE from S. aureus and the increasing frequency of MRSA, empiric therapy must cover MRSA until culture data prove otherwise. Consequently, patients with the possibility of IE should receive nafcillin, gentamicin, and vancomycin. Patients with prosthetic valves who require that therapy be initiated on an emergent basis should receive rifampin, gentamicin, and vancomycin. The regimen should be adjusted after the patient is admitted to the hospital, on the basis of inpatient physician preference and culture and sensitivity data. Consultation with an infectious disease physician should be accomplished at the earliest possible time.
Antibiotics Based on Known Organism
The rapid changes in the epidemiology and antibiotic susceptibilities in all of the major bacterial organisms causing IE make specific recommendations for precise therapy beyond the scope of this chapter. The most recent AHA guidelines give precise details on appropriate antibiotic therapy once organism and antibiotic susceptibilities are known (21). The clinician should be aware of these guidelines as well as the possibilities that empiric therapy will need to be altered, as increasing cases of high level resistance to vancomycin are being reported in both S. aureus and enterococci (21).
Anticoagulants
Anticoagulation is contraindicated in patients with native-valve IE because of the greatly increased risk of intracranial bleeding that occurs in patients with IE who have cerebral emboli. Anticoagulants confer no protection against cerebral or peripheral embolization in native-valve IE, although many experts recommend their continued use. The exception is the patient who develops massive life-threatening pulmonary emboli. Patients with PVIE who are already maintained on anticoagulation should probably continue the medication and be closely monitored for complications related to the prosthetic valve unless there has been a recent central nervous system embolic event (21).
Surgery
Valve replacement has become much more widely accepted as a therapy for complicated IE (22). Surgery is required in 25% to 50% of all cases of acute endocarditis (23). Although there is agreement on the indications for surgery, the timing and specific details are being debated. The following are general indications for valve replacement: heart failure as a result of new valve malfunction, acute valvular insufficiency, major embolic complications, continued bacteremia despite administration of appropriate antibiotics, dysrhythmia or new conduction defect, or a fungal cause (2,21–23). Indications for emergent surgical intervention include acute aortic regurgitation with early closure of the mitral valve, rupture of the pericardium, and rupture of a sinus of Valsalva aneurysm into the right heart chamber (16,23). Furthermore, certain infections such as those caused by Brucella species, Coxiella burnetii, Pseudomonas aeruginosa, Staphylococcus lugdunensis, and Candida species are difficult to manage medically and are best managed by surgery (7).
Traditionally, surgical management has been considered superior to medical management alone with regard to the treatment of PVIE. This continues to be true in the case of patients with hemodynamic instability, heart failure, or perivalvular abscess. Persistent infection, advanced age, and the development of renal failure are associated with an increased postsurgical mortality (21,22). There is emerging evidence that in a subset of stable patients medical management with antibiotics alone may suffice (21). It is not clear to what extent the size of the vegetations seen on the echocardiogram determines the prognosis and need for valve replacement.
CRITICAL INTERVENTIONS
• Obtain at least three sets of high-volume blood cultures from separate sites over a period of 1 hour in stable patients suspected of having endocarditis.
• Initiate antibiotics if the patient appears septic, is elderly, is debilitated, is immunocompromised, has concomitant pneumonia, is in heart failure, or is unstable.
• Administer prophylactic antibiotics to at-risk patients undergoing dental procedures, upper-respiratory tract procedures, or procedures involving infected skin or musculoskeletal tissue.
DISPOSITION
Because of the frequency of serious complications and the need for parenteral antibiotic therapy, all patients who are strongly suspected of having IE should be admitted to the hospital. Patients with overwhelming sepsis, serious embolic complications, or any degree of heart failure or conduction block require admission to an intensive care setting. In addition, intensive care unit admission is mandatory for PVIE patients with any evidence of perivalvular leak.
Blood cultures (20 mL of blood for each set) should be obtained in patients suspected of having IE but in whom the diagnosis is thought to be unlikely. Outpatient follow-up for these patients is appropriate if the patient is reliable and can be readily contacted and if the patient’s private physician agrees.
When IE is strongly suspected, a cardiologist should be consulted for possible echocardiographic examination. TEE must be done as soon as possible in any patient with a prosthetic valve in whom the possibility of IE is considered. Patients with PVIE or those who may need valve replacement should have a cardiac surgeon involved early to ensure that the timing of surgery is optimal. For patients with possible brain abscess or aneurysm, appropriate imaging studies should be performed, and a neurosurgeon should be consulted promptly.
ANTIBIOTIC PROPHYLAXIS AGAINST INFECTIVE ENDOCARDITIS
The aim of antibiotic prophylaxis is to prevent bacteremia from occurring during procedures in patients who have conditions that may predispose them to IE. Prophylactic antibiotics may, in fact, not confer any significant protection from IE and there is no good evidence that prophylactic antibiotics prevent IE caused by dental, GI, or GU procedures (2,24,25). As a result, the AHA has implemented major revisions in its 2007 guidelines that eliminate the antibiotic prophylaxis recommendations for GI and GU procedures and significantly alter the recommendations for dental procedures, respiratory procedures, and those involving infected skin and musculoskeletal structures (Table 88.5). According to current recommendations, only those at the highest risk for IE should receive prophylaxis (24). These include patients with prosthetic heart valves, previous endocarditis or certain types of congenital heart disease, and cardiac transplant recipients with cardiac valvular disease (2,24). Specific antibiotic recommendations and dosages are listed in Table 88.6.
TABLE 88.5
Cardiac Conditions Warranting Antibiotic Prophylaxis for Dental Procedures,a Respiratory Procedures, or Procedures Involving Infected Skin or Musculoskeletal Tissue
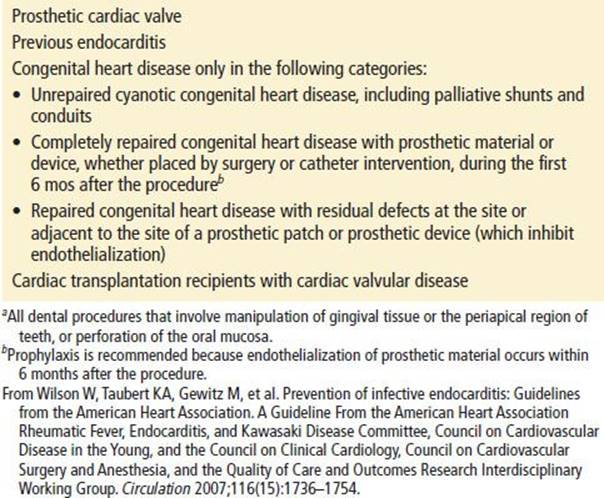
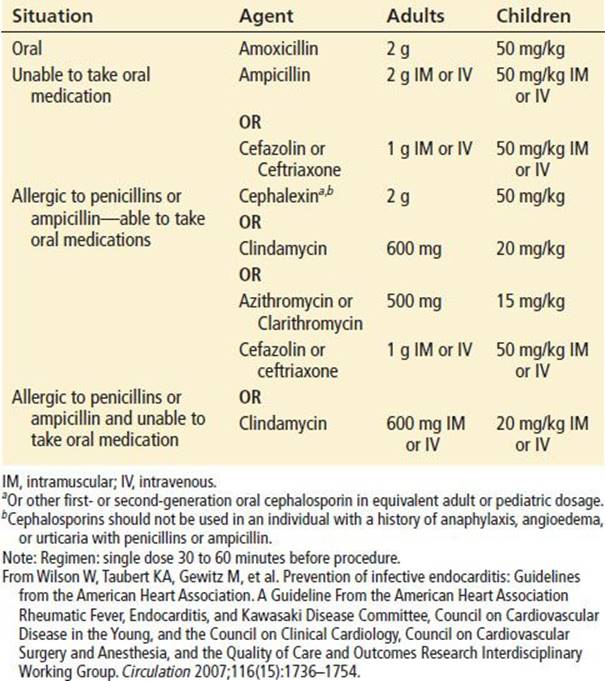
TABLE 88.6
Antibiotic Prophylaxis for Dental Procedures, Respiratory Procedures, or Procedures Involving Infected Skin or Musculoskeletal Tissue
Common Pitfalls
• Not asking about risk factors in patients who present with nonspecific symptoms consistent with IE.
• Missing the diagnosis in the elderly by attributing a cardiac murmur to chronic heart disease.
• Not asking specifically about IV drug use in patients who present with nonspecific symptoms consistent with endocarditis.
• Failing to consider the embolic and immune-mediated complications of IE as the underlying cause of stroke, meningitis, myocardial infarction, septic arthritis, or renal failure.
• Not asking about risk factors for IE in patients about to undergo a procedure prone to cause bacteremia.
REFERENCES
1. Beynon RP, Bahl VK, Prendergast BD. Infective endocarditis. BMJ. 2006; 333(7563):334–339.
2. Hoen B, Duval X. Clinical practice. Infective endocarditis. N Engl J Med. 2013; 368(15):1425–1433.
3. Moreillon P, Que YA. Infective endocarditis. Lancet. 2004;363(9403):139–149.
4. Thuny F, Grisoli D, Collart F, et al. Management of infective endocarditis: Challenges and perspectives. Lancet. 2012;379(9819):965–975.
5. Prendergast BD. The changing face of infective endocarditis. Heart. 2006;92(7):
879–885.
6. Fowler VG Jr, Miro JM, Hoen B, et al. Staphylococcus aureus endocarditis: A consequence of medical progress. JAMA. 2005;293(24):3012–3021.
7. Mylonakis E, Calderwood SB. Infective endocarditis in adults. N Engl J Med. 2001;345(18):1318–1330.
8. Hoen B. Epidemiology and antibiotic treatment of infective endocarditis: An update. Heart. 2006;92(11):1694–1700.
9. Nucifora G, Badano LP, Viale P, et al. Infective endocarditis in chronic haemodialysis patients: An increasing clinical challenge. Eur Heart J. 2007;28(19):2307–2312.
10. Cowgill LD, Addonizio VP, Hopeman AR, et al. Prosthetic valve endocarditis. Curr Probl Cardiol. 1986;11(11):617–664.
11. Brown PD, Levine DP. Infective endocarditis in the injection drug user. Infect Dis Clin North Am. 2002;16(3):645–665, viii–ix.
12. Hoen B, Alla F, Selton-Suty C, et al. Changing profile of infective endocarditis: Results of a 1-year survey in France. JAMA. 2002;288(1):75–81.
13. Wang A, Athan E, Pappas PA, et al. Contemporary clinical profile and outcome of prosthetic valve endocarditis. JAMA. 2007;297(12):1354–1361.
14. Karchmer AW, Longworth DL. Infections of intracardiac devices. Cardiol Clin. 2003;21(2):253–271, vii.
15. Sexton DJ, Spelman D. Current best practices and guidelines. Assessment and management of complications in infective endocarditis. Cardiol Clin. 2003;21(2):
273–282, vii–viii.
16. Meine TJ, Nettles RE, Anderson DJ, et al. Cardiac conduction abnormalities in endocarditis defined by the Duke criteria. Am Heart J. 2001;142(2):280–285.
17. Crawford MH, Durack DT. Clinical presentation of infective endocarditis. Cardiol Clin. 2003;21(2):159–166, v.
18. Heiro M, Nikoskelainen J, Engblom E, et al. Neurologic manifestations of infective endocarditis: A 17-year experience in a teaching hospital in Finland. Arch Intern Med. 2000;160(18):2781–2787.
19. Lester SJ, Wilansky S. Endocarditis and associated complications. Crit Care Med. 2007;35(8 suppl):S384–S391.
20. Jacob S, Tong AT. Role of echocardiography in the diagnosis and management of infective endocarditis. Curr Opin Cardiol. 2002;17(5):478–485.
21. Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: Diagnosis, antimicrobial therapy, and management of complications: A statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation. 2005;111(23):e394–e434.
22. Revilla A, Lopez J, Vilacosta I, et al. Clinical and prognostic profile of patients with infective endocarditis who need urgent surgery. Eur Heart J. 2007;28(1):
65–71.
23. Prendergast BD, Tornos P. Surgery for infective endocarditis: Who and when? Circulation. 2010;121(9):1141–1152.
24. Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: Guidelines from the American Heart Association: A guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116(15):1736–1754.
25. Oliver R, Roberts GJ, Hooper L, et al. Antibiotics for the prophylaxis of bacterial endocarditis in dentistry. Cochrane Database Syst Rev. 2008(4):CD003813.