Doorway Information
Opening Scenario
Jack Edwards, a 27-year-old male, comes to the ED complaining of seeing strange writing on the wall.
Vital Signs
BP: 140/80 mm Hg Temp: 98.3°F (36.8°C)
RR: 15/minute
HR: 110/minute, regular
Examinee Tasks
1. Take a focused history.
2. Perform a focused physical exam (do not perform rectal, genitourinary, or female breast exam).
3. Explain your clinical impression and workup plan to the patient.
4. Write the patient note after leaving the room.
Checklist/SP Sheet
Patient Description
Patient is a 27 yo M.
Notes for the SP
■ Sit up on the bed.
■ Give the impression that you are staring at the wall.
Challenging Questions to Ask
“Do you think someone is trying to give me instructions through the writing I see on the wall?”
Sample Examinee Response
“I don’t think anyone is trying to give you instructions. If you have been taking illicit drugs, it may be that the drugs are causing you to see this writing. In any case, we are going to do some tests to try to figure out what is going on.”
Examinee Checklist
Building the Doctor-Patient Relationship Entrance
□ Examinee knocked on the door before entering.
□ Examinee introduced self by name.
□ Examinee identified his/her role or position.
□ Examinee correctly used patient’s name.
□ Examinee made eye contact with the SP.
Reflective Listening
□ Examinee asked an open-ended question and actively listened to the response.
□ Examinee asked the SP to list his/her concerns and listened to the response without interrupting.
□ Examinee summarized the SP’s concerns, often using the SP’s own words.
Information Gathering
□ Examinee elicited data efficiently and accurately.
Connecting with the Patient
□ Examinee recognized the SP’s emotions and responded with PEARLS.
Physical Examination
□ Examinee washed his/her hands.
□ Examinee asked permission to start the exam.
□ Examinee used respectful draping.
□ Examinee did not repeat painful maneuvers.
Closure
□ Examinee discussed initial diagnostic impressions.
□ Examinee discussed initial management plans.
□ Follow-up tests.
□ Examinee asked if the SP had any other questions or concerns.
Sample Closure
Mr. Edwards, your symptoms could be caused by your illicit drug use, or they may be the result of a mental problem or even a medical condition. We will run some tests to try to clarify your condition. In addition, I recommend that you stop using illicit drugs and quit smoking. Do you have any questions for me?
History
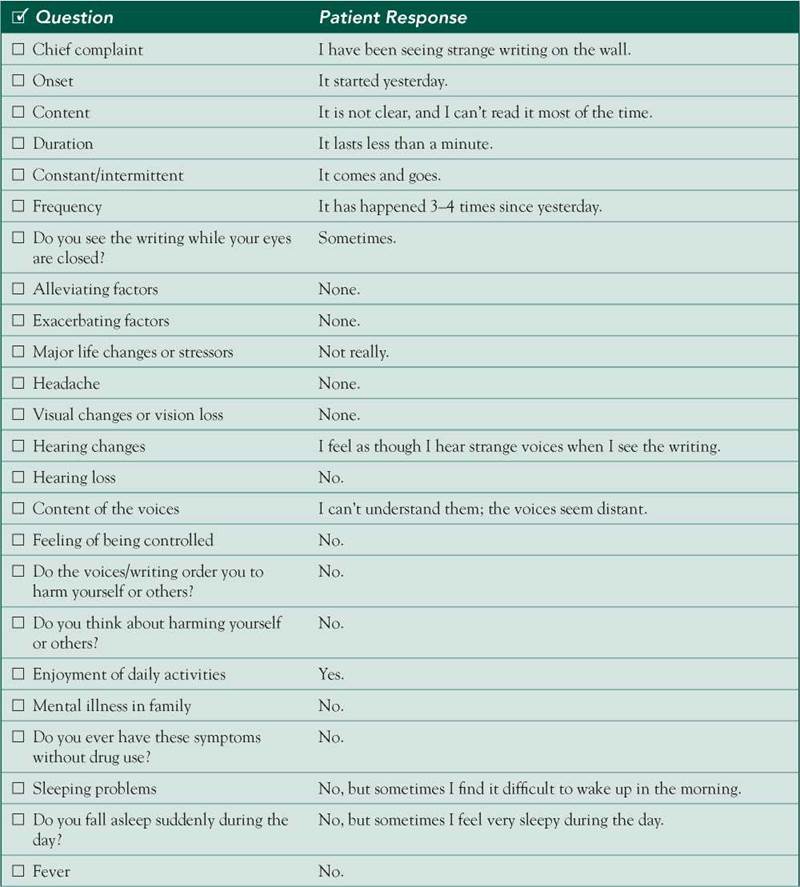
HPI: 27 yo M c/o episodes of seeing strange writing on the wall since yesterday. These episodes last less than a minute and have happened 3-4 times. The patient states that the writing is not clear and he cannot read the messages, but he thinks he might be getting instructions from them. He denies any other visual changes or visual loss. The patient also mentions hearing strange voices associated with the writing, adding that he cannot understand them either. He admits to having used illicit drugs 1 day before these events. He denies any headache, seizures, head trauma, or previous similar episodes. No appetite or weight changes, fever, or sleep problems.
ROS: Negative except as above.
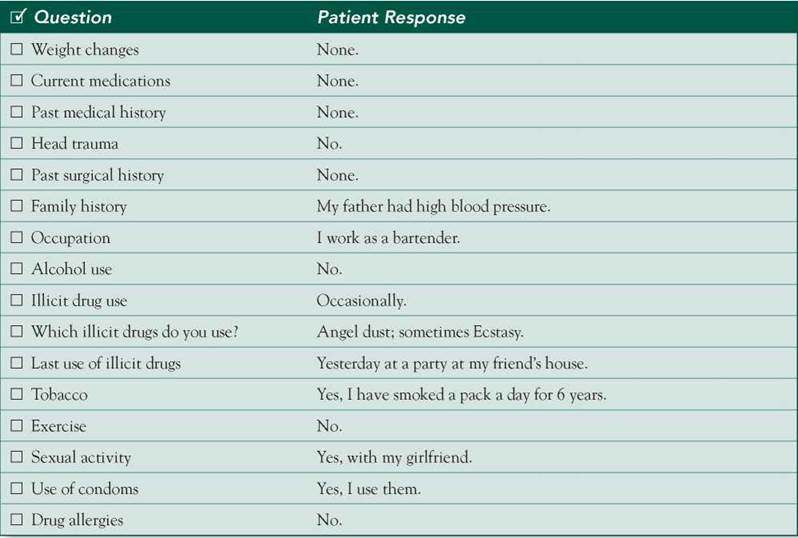
Allergies: NKDA.
Medications: None.
PMH: None.
PSH: None.
SH: 1 PPD for 6 years; uses PCP ("angel dust") and MDMA (Ecstasy) occasionally; no EtOH. Works as a bartender.
FH: Noncontributory.
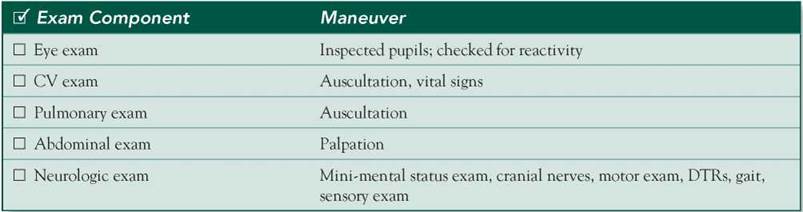
Physical Examination
Patient seems anxious and in mild distress.
VS: HR 110, BP 140/80
HEENT: Pupils dilated, vertical gaze nystagmus.
Chest: Clear breath sounds bilaterally.
Heart: Tachycardic; normal S1/S2; no murmurs, rubs, or gallops.
Abdomen: Soft, nontender, nondistended, no hepatosplenomegaly
Neuro: Mental status: Alert and oriented x 3, spells backward and recalls 3 objects. Cranial nerves: 2-12 intact. Motor: Strength 5/5 in all muscle groups. DTRs: Symmetric. Gait: Normal.
Differential Diagnosis
CASE DISCUSSION
Patient Note Differential Diagnoses
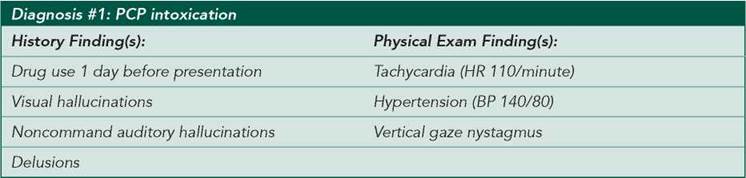
■ PCP intoxication: This patient clearly shows signs of PCP intoxication. Hallucinations, delusions, nystagmus, tachycardia, and hypertension are common in PCP intoxication. The mnemonic RED DANES helps recall common symptoms of PCP intoxication: Rage, Erythema, Dilated pupils, Delusions, Amnesia, Nystagmus, Excitation, and Skin dryness. This patient does not complain of myalgias, although rhabdomyolysis can occur in cases of large ingestions. Serum CPK and urine myoglobin should be measured to rule out this complication.
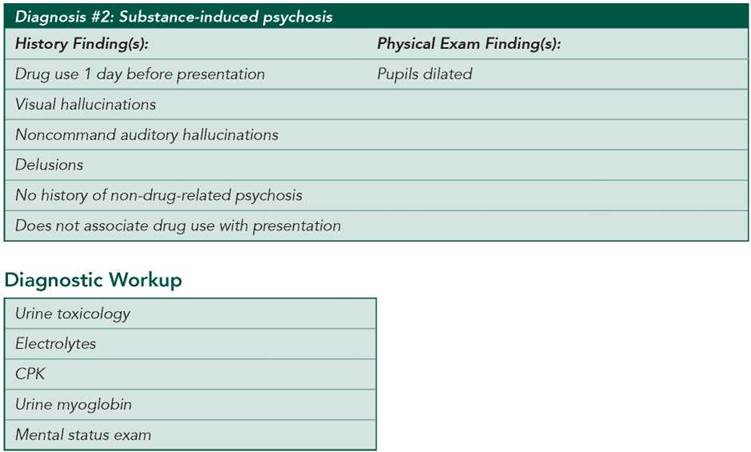
■ Substance-induced psychosis: It is important to note that patients with substance-induced psychosis lack the insight to identify their recent drug use as a cause of their symptoms. The presentation is consistent with this diagnosis. Substance-induced psychosis requires that the substance ingested (medications, alcohol, or illicit drugs) be capable of causing psychosis and that the symptoms be more severe than expected for intoxication or withdrawal. In contrast to intoxication with perceptual disturbances, hallucinations and delusions are more prominent than other symptoms.
Additional Differential Diagnoses
■ Brief psychotic disorder: Symptoms of psychosis may be induced by stressful events and may resolve with removal of the stressor. Auditory hallucinations are more common and typically accompany visual hallucinations. This patient describes both visual and auditory hallucinations. However, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), a diagnosis of brief psychotic disorder cannot be contemplated here because the patient has recently ingested a substance known to induce psychosis.
■ Psychosis secondary to a medical condition: A variety of medical conditions can lead to hallucinations. These include neurologic problems such as CNS infections and neoplasms; endocrine conditions such as thyroid, parathyroid, or adrenal abnormalities; and hepatic and renal disorders. However, there is nothing in this patient’s history to support a secondary medical condition.
■ Narcolepsy: The visual hallucinations of narcolepsy are complex, generally occurring immediately before falling asleep (hypnagogic) or just after waking up (hypnopompic). Auditory or tactile sensations can be associated with visual hallucinations as well. Although this patient complains of daytime sleepiness, his symptoms are not severe enough to merit this diagnosis. Narcolepsy without cataplexy (muscular weakness with or without an emotional trigger) is classified as major somnolence disorder in DSM-5.
■ Seizure: Visual hallucinations of epileptic origin can be simple or complex. They are variable in frequency and usually last for a few seconds. This diagnosis is unlikely because the patient has no known history of seizures.
Diagnostic Workup
■ Urine toxicology: To detect commonly used illicit drugs, such as amphetamines, barbiturates, benzodiazepines, cannabinoids, cocaine, opioids, and phencyclidine (PCP).
■ Electrolytes: To detect any medical condition that may cause neurologic or mental changes.
■ CPK and urine myoglobin: To evaluate for rhabdomyolysis.
■ Mental status exam: To evaluate for a possible psychiatric disorder, although in the setting of a recent substance exposure, the diagnosis of psychopathology is not possible.