Sarah Janssen, MD, PhD, MPH
The occurrence of adverse reproductive outcomes is of fundamental concern to the individuals and families affected. This is especially true if the individuals perceive that they are living or working in areas with potential exposure to hazardous agents over which they have little or no control. Concern has been fueled by incidents such as the contamination of fish with methyl mercury in Minamata Bay, Japan, which was caused by a release from a manufacturing plant. Consumption of the contaminated fish by pregnant women resulted in an epidemic of mental retardation, cerebral palsy, and developmental delay in their offspring. Use of polychlorinated biphenyl (PCB)–contaminated cooking oil in Taiwan resulted in intrauterine growth retardation and hyperpigmentation of the skin in infants of exposed women. Effects on that cohort continue to be uncovered today, including on offspring pubertal development. In recent years, there have been concerns about the reproductive effects of occupational exposure to solvents, pesticides, and video-display terminals or electromagnetic fields. A new area of research has sprung up to identify and study chemicals that may act to disrupt the endocrine system, affecting both wildlife and humans.
Only a few substances are known to have strong associations with adverse reproductive outcomes in humans, but relatively little research has been devoted to these outcomes until the last few decades. A larger number of agents are suspected to cause reproductive harm based on the animal literature and toxicologic assessment. In addition to the emotional stress on affected families, the societal burden of these adverse health outcomes includes high medical costs for compromised children and the increasing use of advanced technology to achieve conception and monitor pregnancy. Another reason to better understand reproductive outcomes is that they may act as sentinels for detecting occupational and environmental hazards because of the relatively short latency between exposure and clinical health event. If workers or community residents are protected from exposures that are harmful to the fetus, they usually will be protected from other health effects associated with these exposures as well. Measures that can be taken to prevent further exposure include substitution or containment of the suspect hazard. Thus, preventing exposure should be a primary goal in the health care provider’s overall assessment of the patient’s situation.
POPULATION AT RISK
In the United States, women comprise greater than 70% of all employees in the following job categories: office and administrative support, education/library, health care provider or support, and personal care and service. Some of the leading occupations for women have potential exposures to known reproductive toxicants (eg, large numbers of women work in the nursing profession or health service occupations with potential exposure to chemotherapeutic agents, anesthetic gases, ionizing radiation, and biologic agents). In addition, there is an increasing number of women in occupations traditionally held by men where there is potential for exposure to reproductive hazards. For example, 2% of construction workers; 4.4% of installation, maintenance, or repair workers; 12.7% of transportation or material-moving workers; and 18.5% of farming, fishing, or forestry workers are women. When women are employed in jobs traditionally held by men, there can be difficulty in obtaining personal protective equipment that fits, accessing separate changing rooms and wash areas, and getting health and safety information that is gender-specific, where appropriate.
Women also may be exposed to reproductive hazards in the environment, which can be more difficult to detect than in the workplace. Often these environmental hazards may be local exposures, but some are of nationwide interest, such as the widespread use of pesticides that persist in the environment and food chain. In addition, exposure to fetuses or children may have lasting effects, so these represent a wider population at risk.
REPRODUCTIVE OUTCOMES & RATES
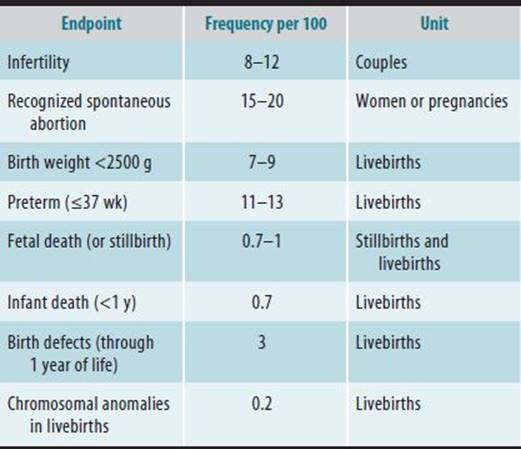
A number of adverse reproductive effects may result from exposure to chemical and physical agents either pre- or postconception. These effects range from infertility to birth defects in the infant. Several of these outcomes are quite frequent and represent a serious public health concern (Table 28–1). Accurate data on the rates of these outcomes can be difficult to obtain because of the lack of national monitoring systems and methodologic differences between individual epidemiologic studies. Approximately 10% of couples in the United States are infertile, which is defined as an inability to conceive during 12 months of unprotected intercourse. Additional couples may experience periods of subfertility or delayed conception. After conception, a continuum of reproductive loss may occur from the time of implantation to delivery. Up to 50% of embryos may be lost after implantation (the earliest time at which conception can be detected), with approximately 15–20% of pregnancies ending in clinically detected spontaneous abortion (SAB) and approximately 1% ending in fetal death. Of all liveborn infants, 7–9% are of low birth weight (LBW), approximately 11% are born prematurely, and approximately 3% will have a congenital anomaly. Whereas rates of fetal and infant death have decreased over the past few decades, rates of LBW and preterm delivery have not, and in some areas they have shown slight increases. Some of the observed risk patterns for these outcomes include (1) older maternal age associated with increased rates of infertility, SAB, and some birth defects and (2) black race associated with nearly doubled rates of LBW, preterm delivery, and fetal death. Ethnic differences may reflect in part unequal access to regular or early prenatal medical care. Other reproductive endpoints that may be affected by exogenous exposures include menstrual function and age at menopause or menarche. Recent studies indicate trends to earlier onset of puberty in girls; about 12% of white girls and 28% of black girls in the United States enter puberty by age 8.
Table 28–1. Prevalence of selected adverse pregnancy outcomes in the United States.
REPRODUCTIVE & DEVELOPMENTAL PHYSIOLOGY & SENSITIVE PERIODS
Germ Cell Development & Menstrual Cycle Function
The female reproductive cycle is a complex process regulated by the autonomic nervous and endocrine systems and mediated by the hypothalamic-pituitary-gonadal axis (Figure 28–1). Unlike males, the female germ cells (oogonia) develop and begin the first meiotic division in utero, with no new generation after birth. The oocytes remain arrested until follicular activation occurs 15–40 years later. Under gonadotropin hormone stimulation at the start of each menstrual cycle, a group of primary follicles begins to develop. Increased levels of the follicle-stimulating hormone (FSH) lead to the selection and growth of a dominant follicle, which produces estrogen to support proliferation of endometrial tissue. A midcycle release of the gonadotropins, FSH, and luteinizing hormone (LH) results in the release of the ovum, or ovulation. The remaining corpus luteum secretes increasing amounts of progesterone and other hormones to prepare for implantation, exerting a negative feedback on the gonadotropins. In the absence of fertilization, the corpus luteum degenerates. The subsequent decrease in ovarian steroids leads to sloughing of the endometrium, as well as to rising levels of FSH, and menstruation occurs after a 12- to 14-day luteal phase. Although this general pattern of menstrual function is known, there is much interwoman variation, and the exact mechanisms are not well understood. If a sperm successfully fertilizes an ovum, the ovum completes a second meiotic division and forms a zygote. This zygote undergoes several rapid cell divisions as it is transported down the fallopian tube to the uterus.
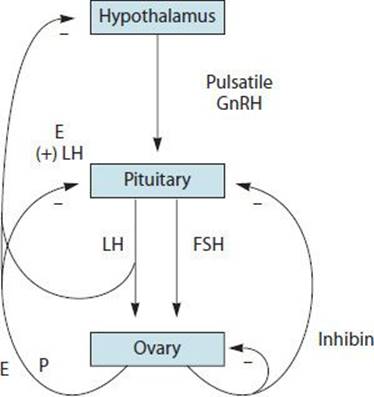
![]() Figure 28–1. Feedback regulation of the hypothalamic-pituitary-ovarian axis. E, estrogens; P, progesterone; LH, luteinizing hormone; FSH, follicle-stimulating hormone; GnRH, gonadotropin-releasing hormone.
Figure 28–1. Feedback regulation of the hypothalamic-pituitary-ovarian axis. E, estrogens; P, progesterone; LH, luteinizing hormone; FSH, follicle-stimulating hormone; GnRH, gonadotropin-releasing hormone.
Endocrine control of the reproductive process might be disrupted by chemicals that, in turn, could lead to menstrual disorders and infertility. This is especially true for those chemicals with steroid-like activity (eg, certain pesticides and dioxins; see below). Because the germ cells are present from birth and many exposures occur during a woman’s life, there is great potential for genetic or cytotoxic harm to the oocytes. It is postulated that the cumulative effects of occupational, environmental, and other exposures may explain the increased incidence of chromosomal abnormalities and SAB that occurs as maternal age increases. But because the greatest potential for genetic damage is most likely to occur during replication and division of the genetic material, the actual sensitivity during the relatively long dormant period is unknown. Genetic damage could result in lack of fertilization or unsuccessful implantation, which can be seen clinically as infertility, or could lead to later fetal loss. Preconception mutagenesis also might result in a birth defect in an infant. Certain mutagenic chemicals are in use in industry, such as organic solvents, ethylene oxide, and metals (eg, arsenic and nickel). Oocyte destruction by chemicals such as polyaromatic hydrocarbons (PAHs) could lead to infertility or to early menopause.
Development of the Fetus
The dividing zygote reaches the uterus approximately 1 week after fertilization, and approximately 1 week later, implantation is complete. The placental villi secrete human chorionic gonadotropin (hCG), which is necessary to maintain pregnancy, and the placenta also takes over the secretion of estrogen and progesterone. The next 6 weeks are called the embryonic period and are the most critical for development because all the major organ systems are formed in precise sequence (Figure 28–2). During the subsequent fetal period, growth and organ maturation continue until term. In particular, the central nervous, genitourinary, and immune systems continue to develop throughout pregnancy. The period of most rapid fetal growth is considered to occur during the last trimester. Full term is typically 38 weeks after conception, with a normal fetal weight of 6.6–7.9 lb (3000–3600 g) and a length of 19–20 in (360 mm).
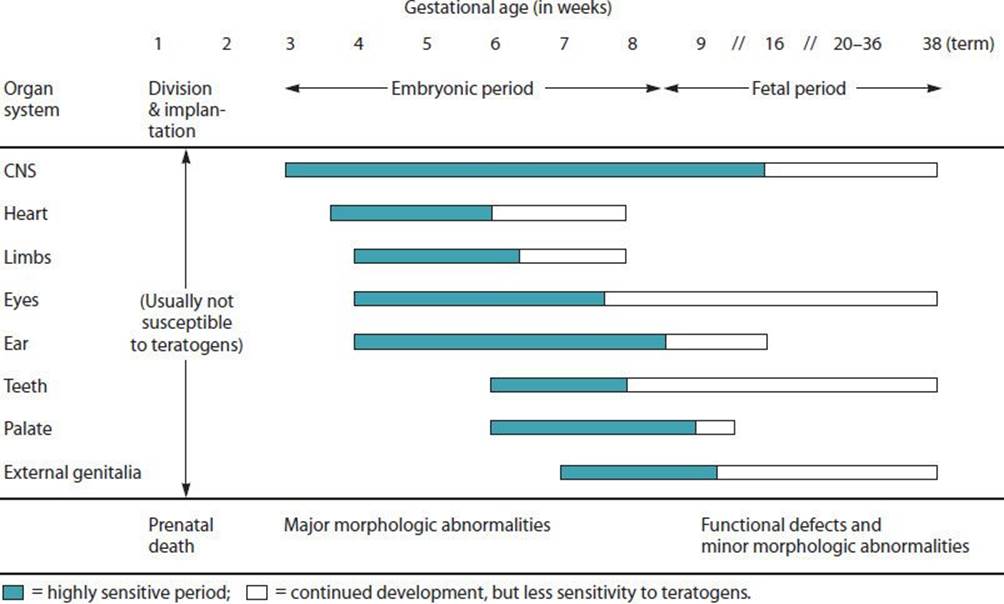
![]() Figure 28–2. Critical periods of fetal development by organ system.
Figure 28–2. Critical periods of fetal development by organ system.
Exposures during weeks 1 and 2 after conception may cause early pregnancy loss if they interfere with tubal transport, implantation, or endocrine control or if they are cytotoxic to the fetus itself. Such a loss may appear only as a late or heavy menstrual flow. With increasingly sensitive laboratory assays available, women trying to conceive or being studied for pregnancy outcome can have these very early losses detected by a short rise and subsequent fall in hCG. The embryo may be less sensitive to structural damage at this time because differentiation has not yet begun, and damage is potentially correctable by the rapidly dividing cells. Thus congenital anomalies are unlikely to result from very early embryo exposures.
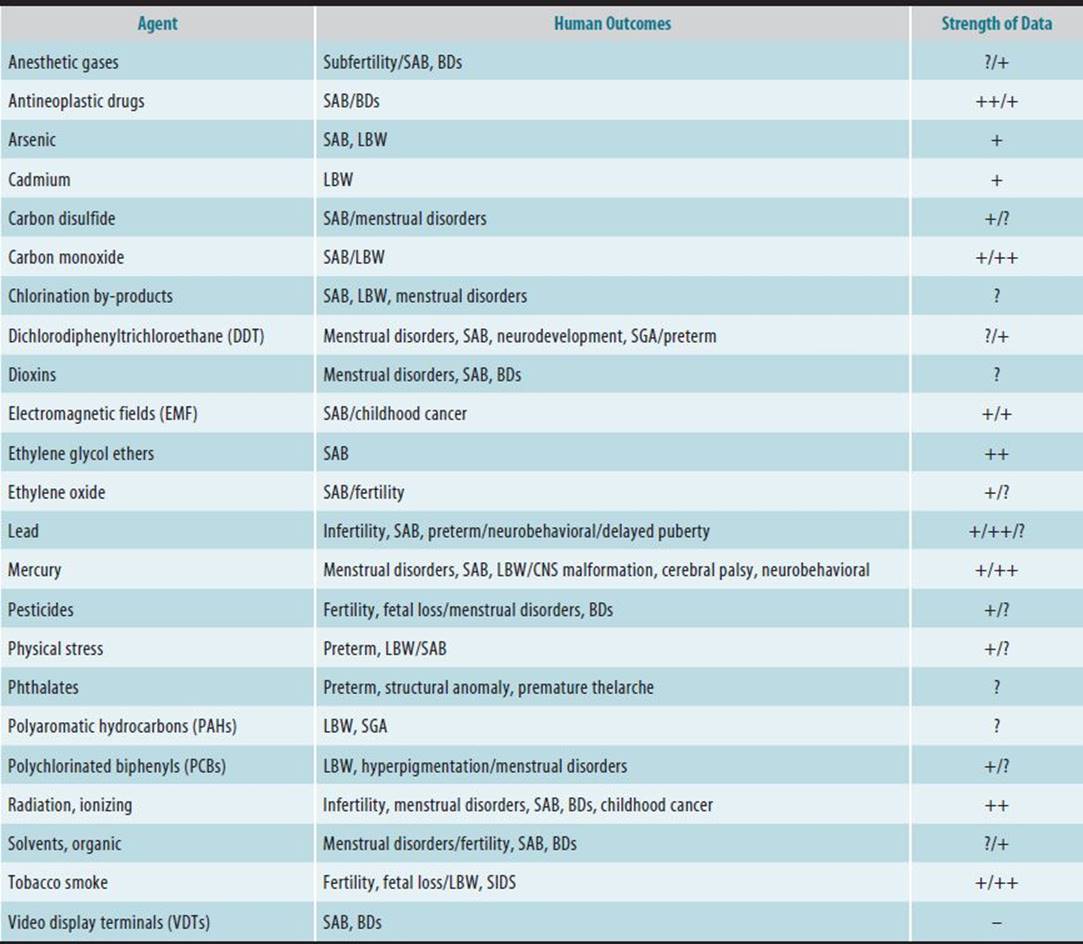
The greatest susceptibility to teratogenic agents occurs during the embryonic period, or organogenesis, when major morphologic abnormalities may be induced. The timing of an effect can be very specific. Although different agents administered at the same time may cause the same anomaly, the same agent given at two different times may induce different anomalies. Known or suspected human teratogens include antineoplastic drugs, diethylstilbestrol (DES), lead, and ionizing radiation (Table 28–2). The embryonic period is when the highest rates of pregnancy loss occur, with approximately 60–75% of recognized losses in the first trimester. Approximately 35% of aborted conceptuses are karyotypically abnormal, and another 30% have morphologic abnormalities.
Table 28–2. Human evidence for adverse female reproduction or developmental effects of selected agents.
Exposure after the first trimester may induce minor morphologic abnormalities or growth deficits. Since the endocrine, central nervous, and other systems are still developing, their respective function might be affected by exposures during this time. Organic mercury, tobacco smoke, and lead are examples of substances that have adverse effects with exposure later in pregnancy. Potentially, carcinogens could cross the placenta and exert an effect at any stage of development.
Postnatal Development & Lactation
The young infant continues development after birth, with general body growth and central nervous system maturation the most obvious changes. In children, prenatal exposures may result in deficits in growth or behavior and mental function (eg, fetal alcohol syndrome). Prenatal maternal cigarette smoking is strongly related to sudden infant death syndrome and is thought to be related to growth. In addition, prenatal exposures may exert effects manifested during reproductive maturation of the offspring, with early pubertal development an increasing concern in industrialized countries. Prenatal exposures or conditions are also being investigated for long-term effects into adulthood.
Child development also may be affected by postnatal exposures. Environmental exposures may be present in the residence or community, and parental occupational exposures may be brought home on clothing or delivered through breast-feeding. Contamination of breast milk occurs primarily by passive diffusion. Thus low-molecular-weight lipophilic nonpolar substances can have higher concentrations in breast milk than in maternal serum. Substances with higher milk-to-plasma ratios (>3) include the polychlorinated biphenyls (PCBs) and dichlorodiphenyltrichloroethane (DDT) residues. Lactation is the main route of excretion for toxicants that bioaccumulate in maternal adipose tissue. Although acute toxicity in infants from contaminated breast milk has been reported (eg, PCBs), the effects of low-level chronic exposures have not been well studied. Therefore, most pediatricians would continue to recommend the benefits of breast-feeding, except for unusual exposure circumstances.
Maternal Physiologic Changes
A number of physiologic changes and medical complications can occur in the pregnant woman that might be affected by occupational or environmental exposures. These changes are also noteworthy to the physician for the way in which they may modify fetal exposures or require accommodation in the workplace. For example, increased tidal volume and respiratory rate of the pregnant woman may increase the absorbed dose of aerosolized chemicals. An increased metabolic rate also may lead to changes in metabolism of specific compounds, leading to a different effective dose. Pregnant women also can experience fatigue and nausea. The nausea may increase sensitivity to substances with strong odors or tastes. Thus potential changes in exposure dose and common consumption patterns (eg, caffeinated or alcoholic beverages) could occur.
SCIENTIFIC LITERATURE
Toxicologic risk assessment is the means of characterizing health effects of hazards in the workplace or environment by combining evidence from scientific studies with likely exposure scenarios using mathematical modeling. When evaluating a patient, the clinician will identify potential exposures via a detailed environmental and occupational history. Existing databases should be consulted for information about reproductive hazards; however, many chemicals and physical hazards have not been studied adequately with respect to reproduction. Because the clinician may need to consult the original literature, this section provides an explanation of basic issues in conducting or interpreting experimental and epidemiologic studies.
As a consequence of the scarcity of human data dealing with reproductive effects, regulatory and oversight agencies often must rely on animal studies when identifying toxicants. Animal studies are applicable to humans with respect to whether there is any harm but are not necessarily predictive of specific human effects. Furthermore, animal studies generally use a range of doses extending well beyond typical human exposures that may involve different routes of exposure and examine endpoints not seen in humans (eg, fetal resorptions). In the evaluation of the animal literature and its relevance to humans, the following aspects need to be considered: species tested; route, timing, and dose of exposure; endpoints examined; systemic or maternal toxicity; litter effects; consistency among animal studies; concordance with reproductive biology; and biologic plausibility of the mechanism of action. From the higher-quality animal studies, the dose-response relationship is assessed to set standards for exposure levels. One goal is to try to ascertain the no-observed-adverse-effect level (NOAEL), which is the highest dose level at which no biologically adverse effects occur, or alternatively, the lowest-observed-adverse-effect level (LOAEL). Then it is customary to apply uncertainty factors (or safety factors) to this level when estimating the “safe” exposure level for humans.
Epidemiologic Studies
Well-conducted epidemiologic studies should provide the best means of evaluating whether a specific agent or group of agents adversely affects human reproduction and development but are less often used for setting standards. Human studies have many limitations, so certain criteria or a weight-of-evidence type of scheme is often used in evaluating whether a substance reasonably can be considered as having an adverse effect. Besides performing qualitative comparison of consistency of results, quality of studies, and biologic plausibility, this might involve conducting a meta-analysis where results from several studies are combined statistically.
A. Study Designs
The basic study designs used to examine the association of an exposure and possible outcomes include the cross-sectional, case-control, and cohort studies, which are discussed in the Appendix. The cross-sectional design is the simplest and has been used often in occupational and environmental reproductive studies. In these studies, there is potential selection bias because the population existing in the workplace at the time of study may not be representative of the workforce during the time of previous exposure. For example, women with live births may leave the workforce temporarily to care for their infants, whereas women experiencing SABs may continue to work and are at greater risk for subsequent SABs. On the other hand, women who experience adverse outcomes that they associate with a workplace exposure may change jobs. The case-control study is most appropriate for evaluating relatively rare diseases (eg, birth defects or childhood cancers). Because the outcome of interest is specified at the onset, the continuum of reproductive effects that may result from a given exposure cannot be evaluated. The cohort study is the preferred study design for most reproductive outcomes. A prospective cohort study allows specific measures of an exposure and potential confounders to be ascertained at the etiologically relevant time periods, before the health endpoint is ascertained.
The cohort and case-control studies are considered hypothesis-testing studies and usually are conducted after a possible association has been suggested. For example, an acute clinician may recognize a series of cases that seem to have a factor in common. This situation is most likely to occur with a rare disease or new syndrome and was instrumental in identifying such associations as thalidomide and severe limb defects and DES and vaginal clear-cell carcinoma. A reported cluster of adverse outcomes occurring in a group of persons is a common way for environmental and occupational problems to be brought to attention, but such clusters often remain unexplained on further investigation.
Valuable data could be obtained from surveillance systems, but there are few established systems in place for adverse reproductive outcomes other than birth defects and, very recently but on a limited basis, autism and other developmental disabilities. Reasons for this include the fact that not all outcomes attract medical attention or require hospitalization (eg, SABs and subfertility), so they are more difficult to ascertain routinely.
B. Exposure Assessment
Although the methods used to measure occupational or environmental exposure are beyond the scope of this chapter, a brief overview of issues specific to evaluating exposure with respect to reproductive outcomes is presented. It should be kept in mind that the exposures of three individuals may be involved (eg, each parent and the fetus/offspring).
To cause reproductive damage, an agent must be absorbed into the bloodstream, and to harm the fetus directly (eg, changes in maternal hormones could affect the fetus) it also must cross the placenta. This process is affected by individual metabolism and the molecular structure of the compound. Some chemicals react with the first tissues they encounter, such as the lungs or skin, and are not absorbed into the bloodstream unless they are ingested (eg, acids, chlorine, and asbestos). Once in the bloodstream, agents that are of low molecular weight, are lipophilic, and are in a non-ionized state are most likely to cross the placenta. Maternal metabolism may result in a metabolite that is more or less toxic to the fetus than the original substance. Unless chronic exposure results in a steady-state level in the body, the rapidity with which a substance is cleared also can affect its toxicity. Often these issues are beyond the scope of epidemiologic studies but should be considered within the overall body of evidence about the toxicity of a substance. When evaluating epidemiologic studies, an association with an exposure at the critical time is more relevant to establishing causality. In addition to timing, a dose-response relationship is examined if exposure data are sufficiently detailed. However, this relationship may not be evident with reproductive outcomes because different doses may result in different outcomes (eg, birth defect versus fetal death).
In epidemiologic studies, exposures can be ascertained from interviews, existing records, or biomarkers. If exposure history is obtained by retrospective interview, the possibility of biased recall among cases or misclassification because of a lack of records or diminished memory is of concern. Ascertainment of current exposure status for cohort studies limits possible recall bias, but women may not be aware of all their exposures, and asking one spouse about the other may not provide sufficiently accurate information.
Existing records often do not provide detailed information but rather serve to group women broadly. For example, residence on the birth certificate might be used to assign likelihood of an environmental exposure. However, residence at delivery may not reflect residence in the first trimester, nor does it account for individual behavioral differences, such as how much time is spent away from the area. Similarly, occupational registries may be used to group women by broad exposures, but specific worksite practices will be unknown. The most accurate occupational exposures are obtained by an industrial hygienist, but such studies are also more costly and often limited in sample size to allow for more detailed study.
Laboratory measurement of exposure provides a quantification of exposure that is less likely to be biased. Techniques for measuring environmental levels in air, water, and soil have been developed for many agents, including radon, electromagnetic fields, solvents, pesticides, metals, and particulate levels. Measurements on biologic samples provide an indication of internal dose, which would be more biologically relevant. For example, cotinine (a metabolite of nicotine) is used to assess tobacco smoke exposure. Biologic monitoring requires a prospective study unless stored samples are available. A number of difficulties can arise with such studies, for example, small sample size or selection bias because of the higher costs and greater participation required of subjects. Sampling at one point in time may not reflect the critical exposure period, particularly if the substance is metabolized rapidly.
C. Health Endpoints & Study Design Issues
Numerous endpoints have been examined in reproductive and developmental toxicity studies. Table 28–3 summarizes the definition and ascertainment of these outcomes as well as potential confounders. For a factor to be a confounder, it must be related to both the endpoint and the exposure in the study of interest. Lack of control for one of the variables in the list does not imply that the study is deficient if the investigators found that this factor did not act as a confounder in their study.
Table 28–3. Developmental and reproductive outcomes, definitions, and source of ascertainment in epidemiologic studies.
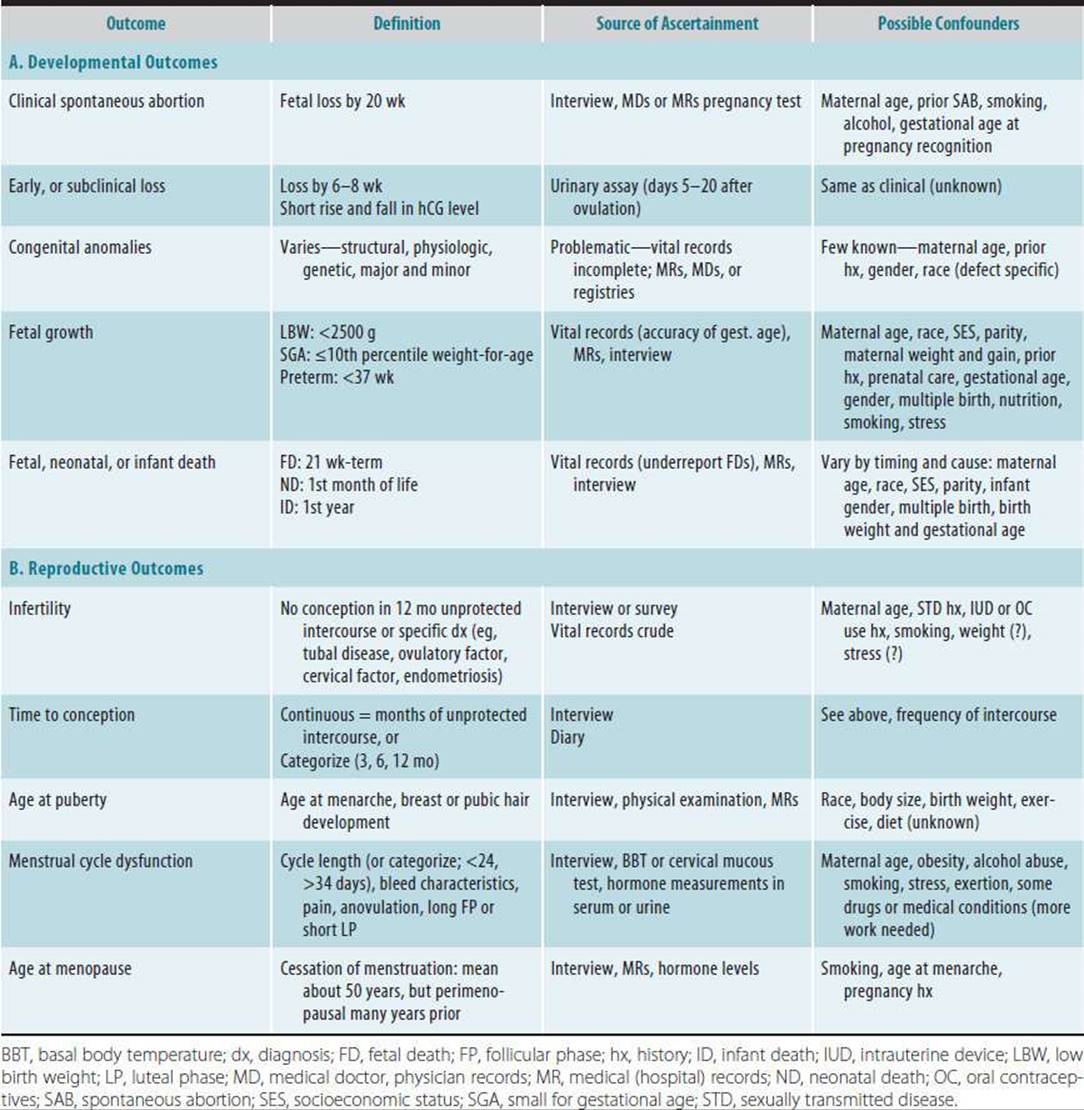
Many of the pregnancy outcomes in Table 28–3A are relatively frequent and lend themselves to a prospective study design. One design is to enroll women when they come in for a prenatal visit and then ascertain pregnancy outcomes by medical records, vital records, or both. However, the detection of SAB depends on the time at which the pregnancy is recognized. Women who have had prior losses and are worried about an exposure may seek medical attention sooner than other women, and thus more of their losses will be detected. A case-control design also can be used to study SAB, but when SABs are ascertained from medical or laboratory records, a certain percentage of early losses will be missed, which may be related to exposure status. Studies have been conducted that collect urine samples for the measurement of hCG and early pregnancy loss (or for ovulation detection). These studies are very labor intensive, and the types of participants may represent a selected population.
In contrast to fetal loss, specific congenital anomalies are not common, and thus a case-control study design is usually used. The primary concerns with these types of studies are ascertainment of relevant cases, selection of appropriate control subjects, and possible recall bias. Classification of defects is problematic because they may have varying etiologies, but any single defect is extremely rare. Many defects are not evident at birth; therefore, additional postnatal follow-up may be necessary for identification.
Because birth weight is recorded fairly accurately and is associated with subsequent mortality and morbidity, it has been the subject of much perinatal research using a variety of study designs. Mean birth weight can be examined, or it is often categorized as low birth weight (<2500 g). However, this category includes infants who are born prematurely, as well as those who are growth retarded for their age. These two groups may be etiologically different and experience different risks of mortality. To distinguish these, investigators can examine LBW among only term infants or small-for-gestational-age infants (SGA; usually defined as births below the tenth percentile on standard-weight-for-gestational-age curves).
Perinatal deaths include a variety of causes with a number of classification schemes developed to summarize them. For occupational or environmental factors, it is useful to distinguish between prepartum and peripartum stillbirths because a toxic effect is more likely to be related to death in utero. When infant deaths are examined, neonatal deaths are found to be more likely to be related to exposures or conditions of pregnancy, whereas postnatal deaths also reflect conditions of infancy.
The reproductive endpoints in Table 28–3B are less well studied epidemiologically than are pregnancy outcomes. This is partly because the population at risk is harder to determine, and such outcomes only recently have come under more public concern. Infertility and subfertility often are studied retrospectively because it is difficult to assemble a population of women trying to become pregnant. The definition of infertility is based on waiting time and may include some people in whom no physiologic change has occurred. If cases are limited to a medically diagnosed population, the study may be biased by a differential likelihood of seeking treatment after varying waiting times, potentially dependent on suspected exposures. Often control subjects are difficult to select for these studies. Because the label of infertility ignores the potential continuum of effects, time to pregnancy is a preferred measure. Retrospectively, women who are pregnant or have delivered recently can be questioned about past use of contraception. The choice of a reference date about when exposures are determined in controls is critical. If the time of conception is used, women who had been trying unsuccessfully before that time may have changed their exposures, and the true period at risk (when contraception is stopped) will not be included. Prospective studies may be conducted by having women keep diaries of when their menstrual periods occur, when they have intercourse, and when they use contraception to identify cycles truly “at risk” of pregnancy, as well as monitoring conception by hormone tests. Menstrual cycle function is the least well investigated but is best studied prospectively with the use of diaries to record signs and symptoms. Cycle length can be used as a crude measure of function, but normal lengths may mask such problems as insufficient luteal phase and progesterone production. Studying such defects requires accurate determination of day of ovulation and measurement of hormone patterns. These types of studies have become relatively easier to conduct in population-based groups by the recent development of cost-efficient serial-sample laboratory assays of urinary hormone metabolites. Such studies may be well suited to an occupational cohort in which a well-defined worker population is assembled and has the advantage of including more women, not just those who are pregnant. The ages at menarche and menopause define the length of natural reproductive capacity and are also related to other endpoints such as breast cancer. Age at menarche is relatively well recalled, even by adults, but other measures of puberty are determined most accurately by trained physical examiners, so prospective or cross-sectional studies would be necessary.
Selected Reproductive Hazards
As noted, few chemicals have been studied adequately in terms of their reproductive effects, and most exposure standards are not based on reproductive effects. Nevertheless, a number of potential reproductive or developmental hazards have been identified in humans. Many of the toxic agents in Table 28–2 have been examined in occupational settings, where exposures tend to be higher than those encountered in the environment and relatively easier to document. However, some of these hazards are encountered environmentally from long-term use and disposal by industry, natural occurrence, or acute releases. After brief discussion of the evidence for some of these, the following section presents three more detailed examples of accumulating epidemiologic data.
The agents that have been shown conclusively to be reproductive toxicants in humans, other than medications, are few and include ionizing radiation, mercury, lead, and polychlorinated biphenyls (PCBs). Among the others listed, anesthetic gases induced fetal loss and congenital defects in animals, and early studies, although flawed, suggested effects in humans. The National Institute for Occupational Safety and Health (NIOSH) recommended exposure limits that led to reductions in exposure, making further study difficult. A meta-analysis yielded a pooled risk ratio for SAB of 1.5 in all studies or 1.9 in the best. Health care workers may be exposed to other hazards, including biologics and antineoplastic drugs, associated with increased risks of SAB. Workers involved in the manufacture of these and other pharmaceuticals also may be put at risk. Pesticides are used commonly worldwide and represent different classes, such as insecticides, herbicides, and fungicides, some of which may be endocrine disruptors (see below). A recent review particularly implicated phenoxy herbicides, pyrethroids, and organophosphates as affecting multiple reproductive endpoints. General exposure to pesticides most likely occurs via the diet or home use, but worker exposures tend to be the highest. In addition to diet, chemicals in air and water may lead to environmental exposures. Increasing evidence shows that air pollutants may be associated with adverse pregnancy outcomes on a population level, including low birth weight, preterm delivery, stillbirth, and infant death.
Reports of clusters of malformations in women working with video-display terminals (VDTs) in the early 1980s led to extensive public and scientific interest. A review of subsequent analytical studies from several countries did not generally support much association of adverse reproductive outcomes with VDT work; a meta-analysis found a pooled odds ratio of 1.0 for VDT use and SAB. However, a Finnish report released later showed an elevated risk (odds ratio [OR]: 3.4) among women who used VDTs with a high level of extremely low-frequency magnetic fields. The concern shifted to electromagnetic fields (EMFs) that are present in all workplaces and homes. The next generation of EMF studies examining electric appliance use, residential wire coding, and residential spot measurements yielded inconsistent results with respect to SAB and little evidence of increased risk for birth defects. Two studies with better exposure measures (eg, the subjects wore measuring devices for 24 hours) subsequently found increased risks of SAB (OR: 1.7–1.8) associated with various EMF metrics. These findings led the California EMF Program to conclude in their risk-evaluation document that EMFs were a possible risk for miscarriage and that further research to study the nature of changing or high magnetic fields was warranted. The evidence for birth defects continues to be examined as well but was inconclusive at the time.
Whether employment per se has a harmful effect on pregnancy outcome has been evaluated, with the general consensus that it does not. Physical exertion at work has been a cause of concern because of the extreme effects seen in professional athletes and dancers. The American College of Obstetricians and Gynecologists published guidelines on exertion levels during later stages of pregnancy indicating that moderate or light exertion levels should be safe throughout pregnancy. Heavy lifting, prolonged standing, or repetitive stooping and bending are recommended to be discontinued early during the second trimester. The most consistent adverse effect of physical exertion seems to be on preterm delivery and possibly low birth weight and SAB, with less consistent results seen for fecundability and menstrual disorders. Several studies show that shift work, or working irregular hours, is associated with a moderately increased risk of SAB, with similar results for LBW and decreased fecundability or longer time to pregnancy.
A. Endocrine-Disrupting Chemicals
In the last two decades, concern has risen about a variety of compounds that may affect the endocrine system by mimicking or antagonizing endogenous hormones. Hormones act as chemical messengers, directing a wide variety of biologic functions through gene expression, and are particularly important during fetal development. Alterations were first noticed in the 1980s among various wildlife populations and later confirmed experimentally. Disruption of the hormone system by chemical contaminants now has been seen in a wide range of species from birds to fish, mollusks, frogs, alligators, and polar bears. Effects in both males and females have been observed, with one unusual but predominant finding being the development of intersex reproductive systems, with both male and female aspects. Originally focused on chemicals that interfered with estrogen receptor pathways, research from a variety of disciplines during the last 5 years has revealed a number of other actions such as antiandrogens, progesterone blockers, or interference with thyroid hormone.
These so-called endocrine-disrupting chemicals (EDCs) or hormonally active agents (HAAs) vary structurally, from persistent pesticides such as DDT/dichlorodiphenyl dichloroethylene (DDE) to PCBs and plasticizers such as phthalates and bisphenol-A. Because some of these compounds persist for years in the environment and have entered the food chain, low exposure may continue despite bans on the use of some of them in the United States. Immigrants from Southeast Asia or Latin America have higher body burdens of persistent pesticides such as DDT, as well as ongoing exposure to other pesticides in agricultural work. More recently, a group of chemicals structurally similar to PCBs, called polybrominated diphenyl ethers (PBDEs), has become a cause for concern because their concentration in human tissues has increased in the United States and Europe. Thyroid hormone disruption and neurodevelop-mental deficits have been found in animal studies. These compounds are used widely as flame retardants in plastics used in electrical appliances, computers, building materials, and furnishings. Exposure may occur in manufacture and dismantling of these products as well as from their degradation in the environment. Another class of compounds with similar manufacturing uses owing to their chemical stability that are now being measured in the environment and wildlife are perfluorinated organic compounds (PFOCs).
Relatively few studies of health effects had been conducted in humans until a national research agenda sped up the process, providing some examples of effects, with even more data anticipated in upcoming years. Furthermore, most of these chemicals have been measured in humans by the Centers for Disease Control and Prevention and others. A number of studies now have shown effects of DDT/DDE on pregnancy loss, low birth weight, and preterm delivery but not entirely consistently. One study with daily measures of hormone metabolites found that luteal-phase progesterone levels generally were lower with higher DDE body burdens. PCBs and mercury have been associated with adverse neurodevelopmental effects in prenatally exposed children. Polybrominated biphenyl (PBB) and PCB exposure in utero also have been associated with earlier menarche, whereas lead exposure has been associated with delayed puberty. Thus a variety of effects from these ubiquitous compounds may be revealed in humans as the research progresses, including other reproductive endpoints such as infertility and tumorigenesis.
Some unique aspects of EDCs are that effects may occur not only at high doses but also lower doses, making classic high-dose experiments potentially misleading. Furthermore, the developing fetus is exquisitely sensitive to both natural hormone signals and exogenous chemical signals. Besides guiding the fetus through critical developmental pathways, these early interactions also help to set its sensitivity to subsequent hormonal signals, leading to potential lifelong consequences. These compounds also may act by creating changes that are permanent to the lineage, leading to transgenerational effects.
B. Solvents
Solvents may well be one of the most pervasive chemical exposures of women because they include many compounds used in the workplace and the home. In the early 1980s, solvent exposure was considered a potential reproductive hazard when increased risks for adverse outcomes were identified among laboratory workers in Scandinavia. In some industries (eg, dry-cleaning and pharmaceutical industries), use of specific solvents, such as perchloroethylene, methylene chloride, toluene, xylene, and glycol ethers, has been associated with concurrent elevation in SAB risk. Several case-control studies show associations of solvent exposure and cardiac and other congenital anomalies. A meta-analysis that combined raw data from five studies for each outcome found that the odds for major malformations increased 64% (eg, OR: 1.64) and for SAB increased 25% with solvent exposure. Confounding and dose-response patterns were not assessed. Suggestive study findings indicate a potential association between solvent use and fetal growth or preterm delivery. A recent study found that offspring of pregnant women occupationally exposed to organic solvents obtained lower scores on various tests of neurodevelopmental function. These results would be consistent with effects of heavy maternal alcohol consumption. Because alcohol is a type of solvent, a “fetal solvent syndrome” has been proposed. Many of the epidemiologic studies suffer from crude exposure assessment, making definitive conclusions difficult, but animal data support the findings. Some studies have examined menstrual patterns, but few consistent results have emerged. At least one study reported reduced fecundability among women with daily or high solvent exposure. Exposures in the semiconductor industry, which employs a largely female workforce, have become of increased interest. A collaborative study of 14 semiconductor companies nationwide reported rates of SAB to be slightly increased, fecundability reduced, and menstrual cycle length increased in exposed workers. The investigators implicated exposures to photoresist and developer solvents (eg, glycol ethers and xylene) and fluoride compounds as the primary etiologic agents.
C. Tobacco Smoke Exposure
Active smoking has been causally associated with a number of developmental and reproductive endpoints; infants of women who smoke during pregnancy are estimated to have twice the risk of low birth weight or a decrement in mean birth weight of 150–200 g compared with infants of nonsmokers. Other adverse developmental outcomes associated with maternal tobacco smoking include preterm delivery, fetal and infant death, and behavioral deficits in offspring. Tobacco smoking is also associated with infertility, menstrual disorders, and earlier age at menopause. In the workplace or other environments, nonsmokers may be exposed to passive smoke, also called environmental tobacco smoke (ETS). Tobacco smoke contains thousands of compounds; those with potential reproductive toxicity include nicotine, carbon monoxide, PAHs, heavy metals, aromatic solvents, and others. Based on studies measuring biomarkers in the early to mid-1990s, from 40% to nearly 100% of nonsmokers may be exposed to some ETS, with working representing, on average, 35% of exposure time.
Reviewing the evidence for adverse effects of ETS exposure on reproduction, over 30 studies have examined mean birth weight, with the better studies indicating a weight decrement ranging from 25 to 100 g. In an earlier meta-analysis, the adequate studies conducted among nonsmoking mothers yielded a pooled weight decrement of 31 g (CL: −42, −20). Studies base on measurement of cotinine (a metabolite of nicotine) in nonsmokers yield even greater weight decrements, particularly as assays have gotten more sensitive so that a truly not (or very low) exposed comparison group can be identified. Of the studies that examined dose-response effects, several found evidence for such trends, further strengthening the argument for causality. At least 20 studies of LBW or SGA have been conducted; the higher-quality studies of LBW yielded a pooled OR of 1.4, or a 40% increase. Some evidence suggests that specific subsets of women may be more susceptible to effects, including older women and nonwhites.
Reviews by several agencies generally conclude there is a consistent slight effect of ETS exposure on reducing mean birth weight (or slightly increasing the risk of growth retardation). There is also good evidence that ETS exposure can lead to sudden infant death syndrome in offspring and may be associated with preterm delivery, SAB, and adverse effects on cognition and behavior. There is a lack of studies of effects of ETS exposure on adult reproductive function, although a few have consistently found earlier mean age at menopause. Therefore, women who are pregnant or attempting it should be counseled to avoid areas where exposure to ETS is likely. In the workplace, other exposures, such as particulates or chemicals, may interact to magnify the effects of ETS. Exposure in other places, such as in commuting or recreation, may become more important sources of exposure as workplace restrictions on smoking are increasingly imposed.
REPRODUCTIVE ASSESSMENT
The medical evaluation of the patient with potential exposure to a reproductive hazard follows the traditional components of history taking, physical examination, and laboratory assessment. In addition, special consideration is needed in the evaluation, communication, and management of reproductive risk for the patient.
Medical Evaluation
In the clinical setting, infertility is defined as an inability to conceive after 12 months of unprotected intercourse. Potential causes for infertility in the female include ovulatory dysfunction, tubal or pelvic factors, and uterine or cervical factors. It is estimated that the cause of infertility is a result of male factors in 40% of affected couples, a result of female factors in 40–50% of affected couples, and of no known etiology in 10–20% of the affected couples. Therefore, for the infertility workup, the male partner needs to be assessed concurrently (see Chapter 29). Adverse pregnancy outcomes include SAB, stillbirth, prematurity, congenital birth defects, low birth weight, and developmental disorders (see Tables 28–1 and 28–3). A full discussion of the diagnosis and treatment of various obstetric/gynecologic or pediatric conditions is beyond the scope of this chapter. However, the following is a general overview of the types of evaluation techniques that can be used to assess the female reproductive system.
![]() Interview
Interview
The patient interview should start with the following areas: demographic data, general medical history, and reproductive history (including age at puberty, menstrual function, past pelvic surgeries or gynecologic procedures, pregnancy and birth outcomes, sexually transmitted diseases, contraception, and familial illness). In addition, it should cover lifestyle habits (such as smoking and alcohol consumption, exercise, and stress), work history and current job tasks and exposures, and potential environmental exposures (eg, ETS; commuting; residential proximity to industry, waste sites, or heavy traffic; and possibly hobbies or home products use).
![]() Physical Examination
Physical Examination
This examination should assess the physical integrity of the reproductive system and rule out any extraneous mass or structural abnormality.
![]() Laboratory
Laboratory
A hormonal profile can be obtained for the assessment of potential fetal loss (hCG and LH), ovarian function (progesterone and estrogen metabolites), and pituitary function (LH and FSH). A wide range of tests and assays is available and needs to be selected based on the medical conditions under consideration. During field biologic monitoring studies, urine samples are relatively easy to collect for hormonal assays. Exposure burden for some hazards may be measured in biologic tissues (eg, exhaled breath, blood, or urine), but few of these lead to diagnostic interpretation.
Risk Evaluation
The steps generally conducted in the toxicologic risk assessment may be adapted in simplified form for the clinical workup, including
1. Hazard identification of any hazardous agents the patient may be exposed to from a detailed occupational and environmental history during interview
2. Hazard evaluation to determine whether a given substance or physical agent may be a reproductive hazard by consulting databases and the literature
3. Exposure assessment, which is performed by estimating the level of exposure from patient work history, product labels, material safety data sheets, industrial hygiene data, environmental sampling, or biologic monitoring results, as well as potential routes of exposure and consistency of symptoms
4. Risk characterization with respect to effects on the reproductive system (This activity is based on information gathered in the first three steps and considers toxicity, timing and extent of exposure, potency, severity of outcome, and degree of uncertainty in animal and human studies.)
Often, not all the needed information is available, and an educated guess is necessary. It is very helpful to have established contacts for additional consultation when a more difficult risk assessment is involved. Potential contacts include local or state health departments, university medical centers, poison control centers, NIOSH, Environmental Protection Agency (EPA), Agency for Toxic Substances and Disease Registry (ATSDR), Occupational Safety and Health Administration (OSHA), and the Association of Occupational and Environmental Clinics (AOEC). Access to online literature databases is very useful (eg, REPRORISK, REPROTOX, and TERIS; see references).
Risk Communication
Building on the information gathered during the risk-assessment process, risk communication is the logical follow-up by which the involved person or persons obtain the information needed to make informed and independent decisions about health and safety risks. In general, there is an underlying principle that needs to be acknowledged and dealt with sensitively: The threat or actual fact of adverse reproductive outcome has a profound impact on an individual’s life. All questions must be answered truthfully and completely. A description of the limitations in knowledge may be needed. The timing of exposure and of the first contact with the involved person is very important. When possible, the risk communication is conducted prior to actual exposure in order to intervene at the primary prevention stage. The options available for the female worker should be presented in such a way that the medical impact and the economic consequences of decisions are understood and discussed. The clinician may need to communicate the risks to an employer as well in order to resolve the situation, but the medical confidentiality of the involved individual must be maintained.
Risk Management
It is very important that the employer, involved employee(s), and medical consultant work together in resolving a particular situation. Ideally, a general policy on reproductive hazards in the workplace that involves both genders is developed within a safety committee composed of representatives from management and labor and consultants in occupational medicine and industrial hygiene. Remediation should occur before conception (which is not always planned) to provide protection during organogenesis, as well as to prevent fertility problems. Furthermore, it may be important to extend protection postpartum during lactation. This may require a written request from the personal physician.
In order of priority, the following actions may be considered for managing the risks of a given reproductive hazard situation: (1) Exposure reduction or elimination, replacement of hazards with safer agents, improved engineering controls, safer work practices, and personal protective equipment (the latter should not be the primary mode of protection). Exposure reduction or elimination is the most desirable option and should be attempted in all situations involving a reproductive hazard. (2) Temporary job transfer: Remove individual from work environment in which reproductive hazard exists. Problems may occur when there is no nonexposed job location. Thus this option should be considered when there is a high-risk situation and exposure reduction/elimination is not possible. (3) Disability leave: Paid leave is subject to company policy, and temporary pregnancy disability leave must be treated the same as any other medical disability leave. The early embryo sensitivity period already has occurred during potential workplace exposure by the time a disability leave is granted. There is no guarantee that the medical disability will be approved, and benefits rarely are equivalent to the individual’s current wage. This option should be considered when there is a high-risk situation in which the employer will not reduce exposure and a temporary transfer is not possible (see also Chapter 7). (4) Remove individual from work: This is the least desirable action. It is illegal for an employer to terminate the affected individual because of pregnancy. A woman may choose to quit work because of personal reasons, but it is important to help her evaluate all options and to understand the possible consequences. This option is to be considered only when all other options have been explored, and the woman is comfortable with the possible consequences.
If an environmental exposure is of concern, options for individual amelioration are less but generally follow the principles just outlined (eg, substitution, safer practices, and removal). Since some exposures may act synergistically, reducing those possible for an individual in the workplace, the home, or the diet is desirable. Additionally, this points to the need to control other environmental exposures at the population level.
LEGAL ISSUES & WORKPLACE STANDARDS
In the lawsuit involving International Union, UAW versus Johnson Controls, Inc., the U.S. Supreme Court held that an employer violated Title VII’s ban on sex discrimination by excluding from production jobs in a lead-battery factory all women who could not prove their sterility. The Court indicated that a policy directed only at fertile women is overt discrimination on the basis of sex regardless of the scientific evidence of heightened safety concerns for mothers or potential mothers. In addition, any policies or actions taken by the employer must not violate existing laws prohibiting discrimination on the basis of pregnancy, childbirth, or related medical conditions. Employers cannot require that an individual be sterilized as a condition of employment. If an employee disabled by pregnancy, childbirth, or a related medical condition transfers to a less hazardous job, an employer must allow her to return to her original job or to a similar one when the disability has resolved.
OSHA has the mandate to promulgate standards that protect workers from adverse health effects (including reproductive effects) resulting from workplace hazards. However, only a few agents have OSHA standards that are based partially on reproductive effects. Included among these agents are dibromochloropropane (DBCP), lead, ethylene oxide, glycol ethers, and ionizing radiation. There are OSHA standards requiring reporting of employee exposure to hazardous chemicals and training of employees using these chemicals. But it should be recognized that many chemical and physical agents found in the workplace are not covered by an OSHA standard and that those standards that do exist for the most part are not based on reproductive endpoints. This is why the simplified risk evaluation process should be implemented at any worksite that has potential reproductive hazards present.
REFERENCES
Bellinger DC: Prenatal Exposures to Environmental Chemicals and Children’s Neurodevelopment. Saf Health Work 2013;4:111 [PMID: 23515885].
Cherniack M: Statement on national worklife priorities. Am J Ind Med 2011;54:10 [PMID: 20949545].
Cordier S: Exposure during pregnancy to glycol ethers and chlorinated solvents and the risk of congenital malformations. Epidemiology 2012;23:806 [PMID: 23007043].
Engel SM: Causal inference considerations for endocrine disruptor research in children’s health. Annu Rev Public Health 2013;34:139 [PMID: 23514318].
Forand SP: Adverse birth outcomes and maternal exposure to trichloroethylene and tetrachloroethylene through soil vapor intrusion in New York State. Environ Health Perspect 2012;120:616 [PMID: 22142966].
Gilboa SM: Association between maternal occupational exposure to organic solvents and congenital heart defects. Occup Environ Med 2012;69:628 [PMID: 22811060].
Macdonald LA: Clinical guidelines for occupational lifting in pregnancy: evidence summary and provisional recommendations. Am J Obstet Gynecol 2013;209:80 [PMID: 23467051].
Meeker JD: Exposure to environmental endocrine disruptors and child development. Arch Pediatr Adolesc Med 2012;166:952 [PMID: 23367522].
Nieuwenhuijsen MJ: Environmental risk factors of pregnancy outcomes. Environ Health 2013;12:6 [PMID: 23320899].
Pelé F: Occupational solvent exposure during pregnancy and child behavior at age 2. Occup Environ Med 2013;70:114 [PMID: 23112267].
Salihu HM: Pregnancy in the workplace. Occup Med (Lond) 2012;62:88 [PMID: 22355087].
Shy CG: Neurodevelopment of infants with prenatal exposure to polybrominated diphenyl ethers. Bull Environ Contam Toxicol 2011;87:643 [PMID: 21953308].
![]() SELF-ASSESSMENT QUESTIONS
SELF-ASSESSMENT QUESTIONS
Select the one correct answer to each question.
Question 1: Chemical exposures
a. during weeks 1 and 2 after conception may cause early pregnancy loss if they interfere with tubal transport, implantation, or endocrine control
b. predictably appear as a late or heavy menstrual flow
c. cause a short rise and subsequent plateau in hCG
d. are likely to cause congenital anomalies from very early embryo exposures
Question 2: Chemical exposures
a. later in pregnancy spare the endocrine, central nervous, and other systems
b. that are of less concern later in pregnancy are organic mercury, tobacco smoke, and lead
c. after the first trimester may induce minor morphologic abnormalities or growth deficits
d. to carcinogens are of no concern because they do not cross the placenta
Question 3: Endocrine-disrupting chemicals (EDCs)
a. do not vary structurally to persistent pesticides such as DDT and plasticizers such as phthalates and bisphenol-A
b. are hormonally active agents (HAAs)
c. may persist for years in the environment but do not enter the food chain
d. are not implicated in thyroid hormone disruption
Question 4: Solvents
a. include many compounds used in the workplace but seldom in the home
b. are considered a potential reproductive hazards only among laboratory workers
c. such as perchloroethylene, methylene chloride, toluene, xylene, and glycol ethers have been associated with concurrent elevation in SAB risk
d. show associations with cardiac but no other congenital anomalies
Question 5: Tobacco smoking
a. is always associated with a number of developmental and reproductive endpoints
b. results in ten times the risk of low birth weight compared with infants of nonsmokers
c. does not induce preterm delivery, fetal and infant death, and behavioral deficits in offspring
d. is associated with infertility, menstrual disorders, and menopause at earlier age