Definition
• Intimal tear → blood enters & traverses the aortic media
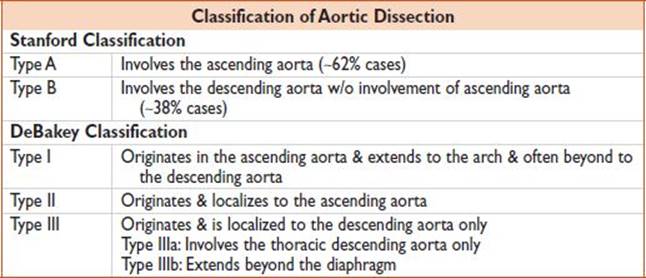
• Classification important b/c this impacts management & prognosis
• Can also have intramural hematoma, penetrating ulcer, pseudoaneurysms of thoracic aorta, & traumatic rupture of thoracic aorta
Approach
• Obtain imaging & consult cardiothoracic surgery early, esp for type A dissection if clinically suspected
History
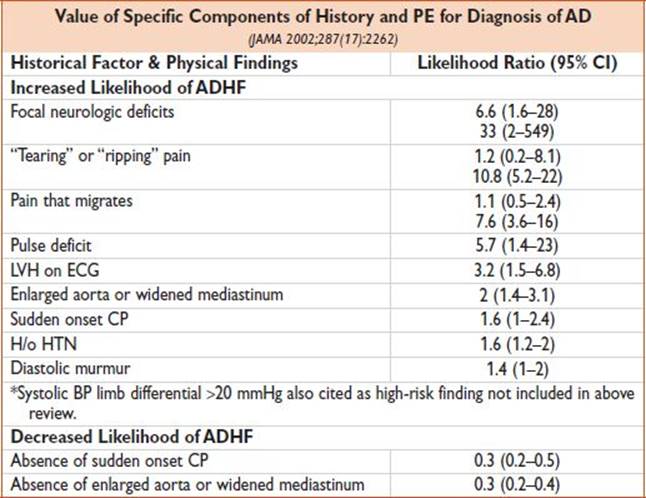
• Abrupt onset CP (ascending), interscapular back pain (descending), neck pain; maximal @ onset, severe, ripping/tearing (∼1/2 pts); syncope, neurologic deficits
Findings
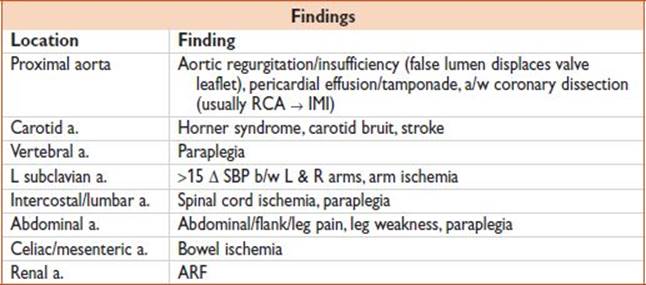
• ↑ BP, though ↓ BP/↑ HR are ominous. Pt is very uncomfortable, other findings depend on location.
Evaluation (Circulation 2005;112:3802)
• Labs: Type/crossmatch, Hct, Cr (↑ suggests renal artery involvement), PT/PTT; consider cardiac markers & D-dimer to r/o other life-threatening causes of CP
• ECG: LVH, MI (RCA → IMI); ∼4–8% of thoracic dissections will present w/ signs of STEMI
• POC cardiac US: Parasternal long-axis & suprasternal notch views may reveal dissection flap or pericardial effusion
• CXR: nl (20%), wide mediastinum, abnl aortic knob, L apical cap, trachea shift → R, depressed L bronchus, L pl effusion
• Advanced imaging modalities include TEE, CTA, MRI, angiography

• Angiography: “Gold standard” though rarely used
Treatment (Circulation 2010;121:e266)
• Surgical tx for Stanford A & medical tx for Stanford B
• At least 2 large-bore IVs
• Close BP monitoring/A line
• Initial management of TAD should be directed at decreasing aortic wall stress by controlling HR & BP:
• In the absence of CIs, IV βB should be initiated to target HR<60
• If IV βB CI, nondihydropyridine CCB (diltiazem, verapamil) should be used
• If SBP >120 mmHg after HR goal achieved, then ACE &/or other vasodilator should be used to target SBP <120 mmHg
• Standard agents:
βB
• Labetolol: 20 mg q5–10min to max 300 mg, or 1–2 mg/min gtt
• Esmolol: Bolus 0.25–0.5 mg/kg over 1–2 min, then 10–200 mcg/kg/min gtt
Vasodilators
• Nitroprusside: 0.5–3 mcg/kg/min
• Morphine or fentanyl gtt: For pain
• Urgent surgical consultation should be obtained (cardiac surgery for Type A, vascular surgery for Type B) for all pts diagnosed w/ thoracic aortic dissection regardless of the location as soon as the Dx is made or suspected
• Acute TADs of ascending aorta should be urgently evaluated for emergent surgical repair
• Acute TADs of descending aorta should be managed medically unless life-threatening comp develop (ie, malperfusion, enlarging aneurysm, inability to control BP or sx)
• Consult vascular or thoracic surgery for open repair vs. stent
Disposition
• ICU
Pearls

• Pts may present atypically, sometimes w/ minimal pain, or only neurodeficit or MI
• Pts may appear very well, then suddenly decompensate
• Neurodeficit = presenting complaint in 20% cases & is present in 40%
• Pain patterns frequently change as the dissection migrates
Guideline: Hiratzka LF, Bakris GL, Beckan JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. Circulation.2010;121:e266–e369.