Definition
• Injuries to the thorax & its structures caused by penetrating or blunt trauma (25% all trauma deaths; immediate: heart/great vessel injury, early: Airway obstruction/tamponade/tension PTX, Late: PNA/PE)
Approach
• Evaluate anatomical categories although many injuries do not occur in isolation: Cardiac/vascular, pulmonary, skeletal, esophageal, diaphragmatic
Inspection
• External trauma: Open wounds (do not probe wounds: Clot dislodgement → hemorrhage), exit/entrance wounds, flail segments (may require external fixation or PPV), seat belt marks, impaled objects (stabilization → removal in OR)
Palpation
• Crepitance (PTX), unequal pulses (vascular trauma, mediastinal hematoma), wounds below nipple line/tip of scapula ↑ risk abdominal trauma (25% have both intra-abdominal + thoracic trauma) (J Trauma1998;45:87)
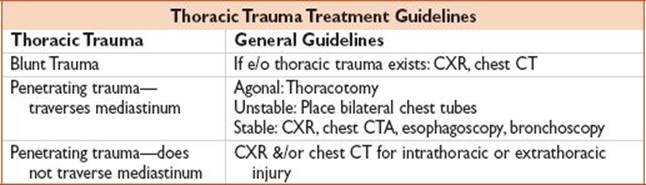
Radiology
• See table
Thoracotomy
• Blunt Traumatic Arrest
• CPR> 10 min, do not perform
• CPR< 10 min or profound refractory shock
• Penetrating Trauma Arrest
• CPR> 15 min, do not perform
• CPR< 15min or profound refractory shock
• Do not transport pt only if pulseless & no electrical cardiac activity in field
• Survival rate in pt w/ arrest from blunt trauma 1.6%, survival rate for arrest from penetrating trauma w/ some signs of life is 31.1% (J Trauma Acute Care Surg 2012;73(6):1359)
Traumatic Aortic Rupture
Definition
• Traumatic rupture of the aorta (descending aorta → fixed to thorax) caused by deceleration injury (fall from height, high-speed MVC, T-boned MVC)
History
• Retrosternal/intrascapular pain (80% die immediately)
Physical Findings
• Exam has poor sens for detecting injury, must have high index of suspicion w/ high mechanism
• Hypotension, asymmetric pulses/BP
Evaluation
• CXR (>8 cm widening of mediastinum, esophageal/trachea deviation, loss of aortic knob/aortopulmonary window, L apical cap, fractures of 1st rib/2nd rib/sternum, widening of paravertebral strip), CTA, TEE
Treatment
• BP control (labetalol/esmolol/nitroprusside): Allow permissive hypotension (SBP 70–90), surgical consult
Disposition
• Admit
Pearl
• 90% who survive have contained hematoma near ligamentum arteriosum
• nl CXR does not rule or aortic injury
Pneumothorax
Definition
• Air in the plural space (simple: W/o shift/communicating w/ outside air, tension: Injury acts as one-way valve/increased intraplural pressures, open: Wall deficit/collapse on inspiration/expansion on expiration/ineffective ventilation)
History
• Blunt (simple) or penetrating (tension/open) trauma
Physical Findings
• Decreased BS, hyperresonance, tension: Tracheal deviation/neck vein distension/hypotension, open: Chest wound w/ “sucking”
Evaluation
• US, CXR (treat tension PTX prior to imaging), chest CT
Treatment
• 100% O2
• Tension: Needle decompression (large-bore needle/IV catheter → 2nd intercostal space, midclavicular line), chest tube to 4th–5th intercostal space mid/anterior axillary line
• Open: Sterile occlusive dressing to taped down on 3 sides → allows efflux/not influx of air, chest tube
• Simple: <10% → serial CXR, mod/large → chest tube directed anteriorly/serial CXR
• Occult: No tx other than O2
• PPx abx indicated in tube thoracostomy in setting of trauma (World J Surg 2006;30:1843)
Disposition
• Admit
Pearl
• Chest tube must be placed if mechanical ventilation required
Hemothorax
Definition
• Blood in the plural space, most common from lung lacerations
History
• Blunt/penetrating trauma
Physical Findings
• Pain, decreased BS, dullness to percussion
Evaluation
• CXR: Costophrenic angle blunting (upright)/diffuse haziness (supine), US, chest CT
Treatment
• Chest tube directed inferiorly, surgical consult → OR if >1.5 L bloody output initially/>200 cc/h or if unstable (↑ likelihood of injury to intercostal/internal mammary/hilar vessels)
• PPx abx indicated in tube thoracostomy in setting of trauma
Pearl
• ∼300 cc needed to see hemothorax on CXR
Disposition
• Admit
Flail Chest
Definition
• Fracture >3 or more ribs in 2 or more places → discontinuous segment of chest wall → paradoxical movement w/ respiration (5% of thoracic trauma)
History
• Blunt trauma, SOB
Physical Findings
• Respiratory distress, tenderness, crepitus, paradoxical movement of chest wall
Evaluation
• CXR
Treatment
• External stabilization (pillow), CPAP (1st line if poor oxygenation/ventilation in awake/cooperative pt → lower mortality/PNA rates vs. intubation) (EMJ 22(5):325), ± chest tube placement, pain control (rib block catheter/epidural is best), intubate only if necessary (obtunded, airway obstruction, respiratory distress)
Disposition
• Admit
Pearl
• 35–50% mortality → related to underlying injuries & cx (pulmonary contusions, PNA)
Pulmonary Contusion
Definition
• Injury to lung parenchyma → hemorrhage/edema → V/Q mismatch
History
• Blunt trauma, SOB
Physical Findings
• Respiratory distress, tenderness, tachypnea, tachycardia, hemoptysis, hypoxia ↑ 1–2 d/resolve 7 d
Evaluation
• CXR: May be nl initially, bilateral alveolar infiltrates
Treatment
• Restrict IVF to euvolemia, intubate if needed
Disposition
• Admit
Cardiac Tamponade
Definition
• Hemopericardium → constriction of the heart → decreased CO, most commonly due to penetrating injury (rarely blunt trauma)
History
• Penetrating trauma
Physical Findings
• Beck triad (hypotension/JVD/muffled heart sounds), tachycardia, pulsus paradoxus
Evaluation
• Bedside/formal US: Pericardial effusion/diastolic collapse of RA/RV, ECG: Low voltage/electrical alternans, CXR: Usually unremarkable
Treatment
• Aggressive IVF (preload dependent)
• Hypotension + pericardial effusion → OR/pericardiocentesis (blood usually clotted, if fresh may be in RV)
• Arrest → thoracotomy
Disposition
• Admit
Pearl
• JVD is rare in trauma pts given hypovolemia
Cardiac Contusion
Definition
• Contusion of the myocardium/coronary vessels/valves/septum
History
• Blunt trauma
Physical Findings
• Tachycardia, hypotension
Evaluation
ECG: New BBB, dysrhythmias (rare after 1st 24 h), ST changes/conduction abnormalities/RV Dysfxn, ± cardiac enzymes (poor sens, levels not predictive of outcome)
Treatment
• IV fluid resuscitation (RV damage → preload dependence), see table
Disposition
• Admit to Tele
Pearl
• New ECG changes consider primary cardiac event → trauma

Esophageal Injury
Definition
• Injury to the esophagus most commonly from penetrating trauma (possible w/ significant epigastric blunt trauma)
History
• Penetrating trauma
Physical Findings
• Respiratory distress, neck/chest crepitus, hematemesis
• Often will have severe other injuries in blunt trauma
Evaluation
• CXR: Mediastinal/deep cervical air, neck films: Esophageal + laryngeal injury → air column in the esophagus, flexible esophagoscopy + esophagram (90% sens), CT
Treatment
• Surgical consult for operative management, broad-spectrum abx
Disposition
• Admit
Tracheobronchial Tear
Definition
• Tear to trachea/bronchus, most commonly due to penetrating trauma
History
• Penetrating trauma or severe deceleration injury, often die at scene
Physical Findings
• Crepitance, large persistent air leak or recurrent ptx after chest tube placement (if cervical injury may not have air leak)
Evaluation
• CXR: PTX/pneumomediastinum/ “fallen lung sign,” chest CT, bronchoscopy (gold standard, may miss injuries >2 cm above carina)
Treatment
• Fiberoptic intubation (in major bronchial lesions → consider double lumen ETT), chest tube placement (may require >1 chest tube)
Disposition
• Admit
Pearl
• May p/w difficulty passing ETT/difficulty w/ ventilation after ETT intubation