Definition
• Trauma to the abdomen & its structures
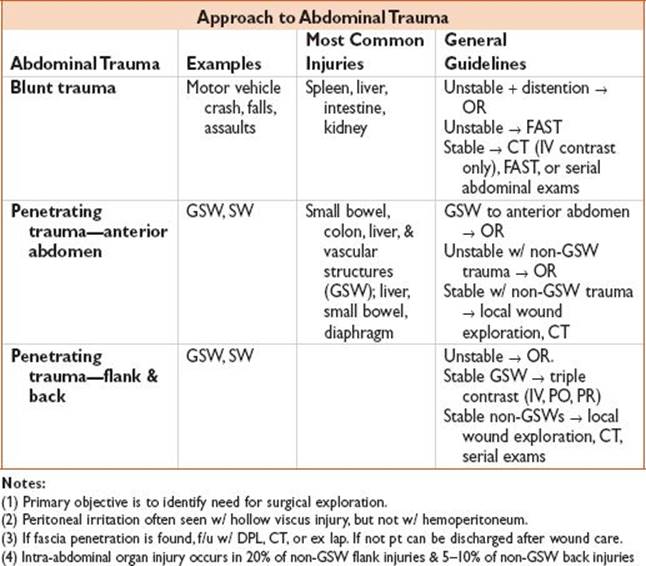
Approach
Evaluate 4 Main Areas
• Anterior abdomen: Transnipple line → inguinal ligaments/pubic symphysis → anterior axillary line, Flank: B/w anterior & posterior axillary lines from 6th rib → iliac crest, Back: Inf scapular tips → iliac crest, gluteal region: Iliac crest → gluteal fold
Inspection
• Entrance/exit wounds (check b/w buttock/thigh/axilla/neck), seat belt sign (↑ risk mesenteric tear/avulsion, bowel perforation, aorta/iliac thrombosis, chance fracture of L1/L2), do not remove objects, cover eviscerated organs in saline soaked gauze
Palpation
• Peritoneal signs (operative management), rectal exam (high-riding prostate/blood/one)
Labs
• CBC (Hct may be nl initially in setting of hemorrhage), ABG, lactate, LFTs, lipase, UA
Radiology
• FAST (90–100% sens for hemoperitoneum, not spec), CXR (abdominal free air), pelvic x-ray (loss of psoas shadow → retroperitoneal injury, location of bullets), CT (definitive test, low sens for early pancreatic/diaphragmatic/bowel)
Diagnostic Peritoneal Lavage (DPL)
• Rarely used given FAST/CT scans, positive study → gross blood, blunt trauma/stab wound >100000 RBCs, GSW >5000 RBC
Liver Laceration
Definition
• Laceration to liver (most commonly injured organ)
History
• Blunt or penetrating trauma
Physical Findings
• ± RUQ tenderness
Evaluation
• LFTs, HCT, FAST, CT scan: Grading of laceration (I–VI)
Treatment
• Surgical consultation for operative vs. conservative management (HD stable, serial exams/HCT)
Disposition
• Admit ICU vs. floor
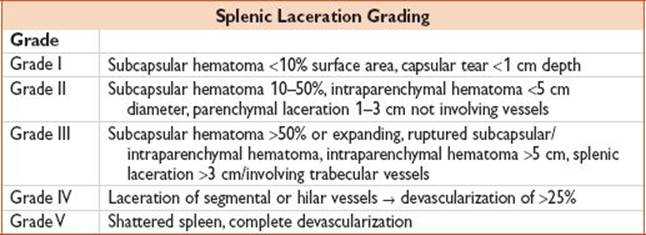
Splenic Laceration
Definition
• Laceration to spleen (most commonly injured organ in blunt trauma)
History
• Blunt or penetrating trauma, L shoulder pain (Kehr sign)/chest/flank/upper quadrant pain
Physical Findings
• LUQ pain
Evaluation
• FAST, CT scan: Grading of laceration (I–V)
Treatment
• Surgical consultation for operative vs. conservative management (HD stable, serial exams/HCT), IR for embolization
Disposition
• Admit ICU vs. floor
Small Bowel Injury
Definition
• Injury to small bowel (GSW > SW > blunt trauma)
History
• Blunt or penetrating trauma, classically handlebar injury
Physical Findings
• Seat belt sign (MVC), peritoneal signs (may be delayed)
Evaluation
• Unstable → FAST/DPL, Stable → CT scan (low sens, fluid collection/bowel-wall thickening/stranding/free air) CXR (rarely shows free air), Lumbar XR (Chance fracture)
Treatment
• Surgical consultation for operative management (perforation or devascularization), abx (ampicillin/ciprofloxacin/metronidazole)
Disposition
• Admit
Colorectal Injury
Definition
• Injury to colon or rectum (transverse colon most common)
History
• Penetrating trauma (GSW)
Physical Findings
• Hypoactive bowels, peritoneal signs, gross rectal blood
Evaluation
• Triple contrast CT scan (Gastrografin, barium is irritating), KUB (air lining psoas), f/u sigmoidoscopy
Treatment
• Surgical consultation for operative management (perforation or devascularization), abx (ampicillin/ciprofloxacin/metronidazole)
Disposition
• Admit
Duodenal Injury
Definition
• Injury to duodenum (80% a/w other injury)
History
• Penetrating trauma, N/V (obstructing hematoma)
Physical Findings
• Epigastric tenderness, heme positive stool, bloody NGT aspirate
Evaluation
• Upright CXR (free air), CT scan (duodenal wall hematoma), Upper GI (“coiled spring” area)
Treatment
• Surgical consultation for operative management (perforation or devascularization), abx (ampicillin/ciprofloxacin/metronidazole), NGT placement
Disposition
• Admit
Pearls
• 2nd portion most commonly injured (contains bile/pancreatic duct openings)
• Mortality 40% if dx delayed 24 h
Gastric Injury
Definition
• Injury to stomach, uncommon
History
• Penetrating trauma
Physical Findings
• Epigastric tenderness, heme positive stool, bloody NGT aspirate
Evaluation
• Upright CXR (free air)
Treatment
• Surgical consultation for operative management, abx (ampicillin/ciprofloxacin/metronidazole)
Disposition
• Admit
Pancreatic Injury
Definition
• Injury to pancreas (75% penetrating trauma)
History
• Penetrating trauma, direct epigastric trauma (steering wheel, bicycle handles)
Physical Findings
• Minimal epigastric tenderness (retroperitoneal structure)
Evaluation
• CT scan (low sens early), lipase (may be nl), ERCP for ductal injury
Treatment
• Surgical consultation
Disposition
• Admit
Pearl
• A/w other injuries 90% of the time
Vascular Trauma
Definition
• Injury to abdominal vasculature (10% of SW, 25% of GSW)
History
• Penetrating trauma
Physical Findings
• Distension, expanding hematoma, Grey-Turner sign (flank ecchymosis)/Cullen sign (periumbilical ecchymosis) → retroperitoneal hemorrhage
Evaluation
• FAST, CT scan (if stable), wound exploration
Treatment
• Surgical consultation, unstable → OR
Disposition
• Admit
Pearl
• Avoid LE venous access
Diaphragmatic Tear
Definition
• Tear to diaphragm from blunt trauma, ↑ lateral impact (large, L-sided 2–3× more likely than R, posterolaterally located) or penetrating trauma (small but enlarge w/ time)
History
• Penetrating/blunt trauma, delayed presentation; pain, ± obstruction
Physical Findings
• BS over chest
Evaluation
• CXR (50% sens): Hemothorax/PTX (penetrating), abnl diaphragmatic shadow (blunt), US, CT scan, careful NGT placement (may be seen in hemithorax)
Treatment
• Respiratory distress → NGT placement for decompression, surgery consult for operative repair
Disposition
• Admit
Pearl
• Intrapericardial diaphragmatic rupture/bowel herniation → tamponade