Definition
• The sensation of disorientation in space combined w/ sensation of motion/spinning
Approach
• Onset, duration & severity of sxs, exacerbating & alleviating factors, associated sxs
• Ask about trauma & risk for vertebral artery injury (torsional neck injury, chiropractic)
• Careful history: Distinguish b/w vertigo & presyncope or lightheadedness
• Consider ECG to r/o arrhythmia/MI, glucose to r/o hypoglycemia, CBC to r/o anemia
• Exam should include carotid bruits, otoscopy, cerebellar exam, gait, nystagmus ± Hallpike
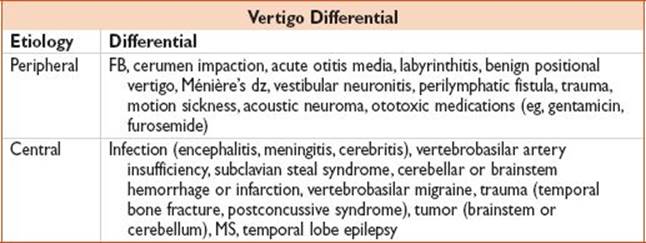
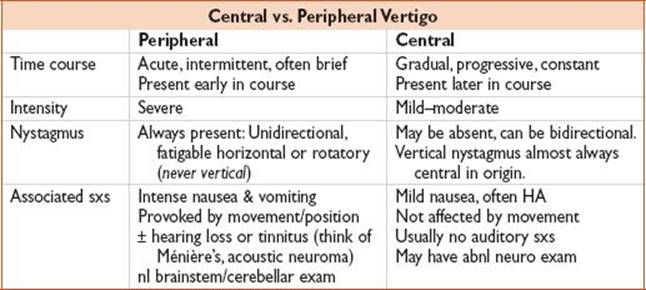
• Vertigo is broadly classified as peripheral or central in etiology
• Peripheral etiologies are usually nonemergent
• Central etiologies are generally emergent diagnoses, account for 10% of cases
• RFs for central vertigo: Older age, males, HTN, CAD, DM, AF, h/o CVA/TIA
Central Vertigo
History
• See tables above. Consider RFs when determining w/u.
Evaluation
• Head CT useful as initial exam for hemorrhage but limited utility for cerebellum/brainstem
• MRI, when available, is diagnostic modality of choice for cerebellar process
• Consider CTA or MRA to evaluate for vascular dz (carotid, vertebrobasilar)
Treatment
• Symptomatic relief (antiemetics, benzodiazepines). Neurology consult.
Disposition
• Depends on findings, severity of sxs. Admit if high risk for vascular etiology.
Peripheral Vertigo
Treatment
• Usually supportive care w/ antivertigo medications:
• Diazepam 2–4 mg IV/5–10 mg PO, meclizine 25 mg PO, diphenhydramine, promethazine
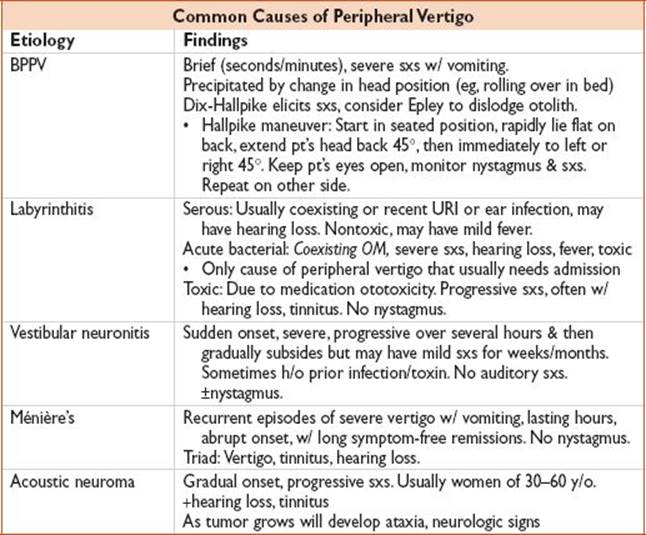
• For BPPV, consider trying Epley maneuver (or modified self-Epley maneuver at home)
• For acute bacterial labyrinthitis: ENT consult, IV abx, usually need admission
• For Ménière’s: Supportive medications, encourage decreased salt intake, close ENT f/u
Disposition
• Home once sxs improve w/ PCP/ENT f/u
• Admit if vertigo refractory to ED tx or acute bacterial labyrinthitis