Definition
• Any complication involving dialysis catheters or fistulas as well as infection, electrolyte imbalances, cardiac complaints, or signs of fluid overload among others
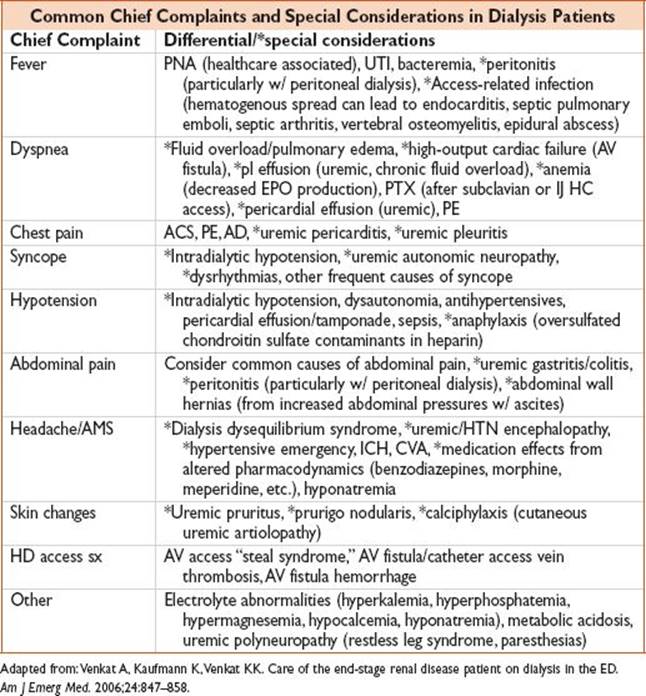
• Common complaints & special considerations include:
Approach to the Patient
History
• Should focus on assessing for common causes of respective chief complaints, w/ attention to special considerations unique to ESRD pt
Physical
• Attention to abnl vital signs
• Pulmonary & cardiac exam including assessment of friction rub, rhonchi, & rales
• Abdominal exam, esp in pts w/ PD catheters
• Extremity exam & JVP for signs of fluid overload
• Skin exam for e/o calciphylaxis
• Assess graft site for thrill & signs of bleeding, infection, edema, & bruising; assess tunneled catheter site for e/o cellulitis or underlying abscess formation
Diagnostics
• CBC, Chem 10; consider ABG w/ STAT potassium & to assess acid–base status
• Consider LFTs, BNP, cardiac markers if indicated
• Consider contacting PD access nurse for sample of PD dialysate fluid (cell count [WBC >50–100 cell/mm3 suggest peritonitis], gram stain, culture)
• EKG for cardiac electrical instability from potential electrolyte abx, ischemia
• Consider point-of-care cardiac & lung US & FAST exam to assess for effusion & ascites, respectively
• Imaging: Appropriate imaging for respective complaints; Doppler imaging of AF fistula site if concern for thrombosis
Treatment
• Refer to appropriate sections for tx of conditions noted above
• Special considerations:
• Peritonitis: Vancomycin 2 g AND cefepime/ceftazidime 1 g each added to 1 bag of dialysate infused into & allowed to dwell in the peritoneal cavity for 6 h
• Dialysis disequilibrium syndrome: Reduce ICP (HOB elevation >30°, hyperosmolar therapy [mannitol, hypertonic saline], euglycemia, euthermia, eunatremia, MAP > 65, CO2 40 mmHg, CPP 50–70 mmHg); renal consult
• Clotted AV graft/fistula: Immediate vascular surgery consultation for consideration of catheter-directed thrombolysis, pharmacomechanical thrombolysis, surgical thrombectomy
• Clotted Vascular Access Catheters: Consult institutional policies; if feasible, attempt catheter-directed tPA via infusion of 2 mg tPA into occluded lumen & fill remainder w/ saline. After 15 min, inject 0.3 mL saline to move the active enzyme toward the tip of the catheter. After another 15 min, inject another 0.3 mL to move the active enzyme toward the tip of the catheter. After another 15 min, try to aspirate catheter. If unsuccessful, send pt for catheter exchange.
• Vascular Access Hemorrhage: Apply direct pressure for 10–15 min; if occurs w/ hours of dialysis, consider protamine 1 mg per 100 U heparin received (or 10–20 mg if dose unknown) to reverse heparin anticoagulation; consider application of gelfoam, surgical, or other hemostatic agent; immediate vascular surgery consultation for uncontrolled hemorrhage
Disposition depends upon presenting complaint, but most will invariably require admission
Pearls
• BP measurement over & use of AV fistula sites for blood draw/administering therapy is contraindicated
• BNP levels are not reliable in diagnosing fluid overload/HF in dialysis pts as basal BNP levels are typically elevated & increased BNP levels from baseline may not correlate w/ clinical HF
• Chronically elevated troponin common & a/w increased mortality; makes assessment of ACS challenging; however, the National Academy of Clinical Biochemistry (NACB) recommends a 20% change in troponin concentration from baseline for Dx of AMI