PULMONARYQ
INTERSTITIAL LUNG DISEASE
WORKUP OF ILD
Rule out mimickers of ILD
• Congestive heart failure (✓ BNP, trial of diuresis)
• Infection: viral, atypical bacterial, fungal, mycobacterial, parasitic
• Malignancy: lymphangitic carcinomatosis, bronchoalveolar, leukemia, lymphoma
History and physical exam
• Occupational, travel, exposure (including tobacco), meds, FHx, precipitating event
• Tempo (acute → infxn, CHF, hypersens pneumonitis, eos PNA, AIP, COP, drug-induced)
• Extrapulmonary s/s (skin Ds, arthralgias/arthritis, clubbing, neuropathies, etc.)
Diagnostic studies (see Appendix & Radiology inserts)
• CXR and high-resolution chest CT: reticular, nodular or ground glass pattern upper → coal, silicon, hypersens, sarcoid, TB, RA; lower → IPF, asbestos, scleroderma adenopathy → sarcoidosis, berylliosis, silicosis, malignancy, fungal infections pleural disease → collagen-vascular diseases, asbestosis, infections, XRT
• PFTs: ↓ DLCO (early sign), restrictive pattern (↓ volumes), ↓ PaO2 (esp. w/ exercise); if also obstructive, consider sarcoid, LAM, silicosis
• Serologies: ✓ ACE, ANA, RF, ANCA, anti-GBM, HIV
• Bronchoalveolar lavage: dx infxn, hemorrhage, eosinophilic syndromes, PAP
• Biopsy (transbronch, CT-guided, VATS, open) if no clear precipitant and w/u unrevealing
ETIOLOGIES OF ILD
Sarcoidosis (NEJM 2007;357:2153; JAMA 2011;305:391)
• Prevalence: African Americans, northern Europeans and females; onset in 3rd–4th decade
• Pathophysiology: depression of cellular immune system peripherally, activation centrally

• Löfgren’s syndrome: erythema nodosum + hilar adenopathy + arthritis (good prognosis)
• Diagnostic studies: LN bx → noncaseating granulomas + multinucleated giant cells 18FDG PET can be used to identify extent and potentially targets for dx bx ↑ ACE (Se 60%, 90% w/ active dis., Sp 80%, false ![]() in granulomatous diseases)
in granulomatous diseases)
• To assess extent: CXR, PFTs, full ophtho exam, ECG, CBC (lymphopenia, ↑ eos), Ca, 24-h urine for Ca, LFTs; ± Holter, echo, cardiac MRI, brain MRI, etc., based on s/s
• Rx: steroids (eg, prednisone 20–40 mg/d) if sx or extrathoracic organ dysfxn (improves sx, but doesn’t Δ long-term course); hydroxychloroquine for extensive skin disease; anti-TNF, MTX, AZA, mycophenolate or cyclophosphamide for chronic/refractory disease
• Prognosis: ~2/3 spontaneously remit w/in 10 y (60–80% of stage I, 50–60% stage II, 30% stage III), w/ relapses uncommon; ~1/3 have progressive disease
Iatrogenic
• Amiodarone (~10%; dose & duration depend.): chronic interstitial pneumonia ↔ ARDS; bx → vacuolized Mf w/ lamellar inclusions on EM; Rx: d/c amio, give steroids
• Other drugs: nitrofurantoin, sulfonamides, thiazides, INH, hydralazine, gold
• Chemo: bleomycin (triggered by hyperoxia), busulfan, cyclophosphamide, MTX, etc.
• XRT: COP/BOOP w/ sharply linear, nonanatomic boundaries; DAH
Idiopathic interstitial pneumonias (IIPs) (AJRCCM 2005;172:268)
• Definition: ILD of unknown cause; dx by radiographic, histologic and clinical features
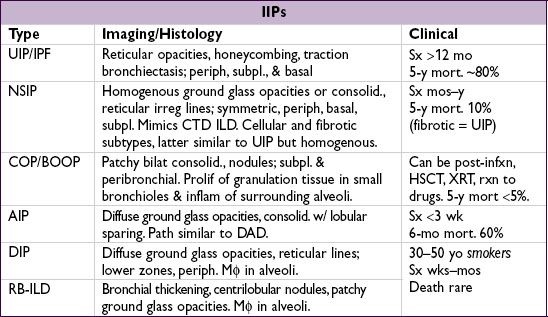
UIP, usual interstitial PNA (IP); IPF, idiopathic pulm fibrosis (Lancet 2011;378:1949); NSIP, nonspecific IP; COP, cryptogenic organizing PNA; BOOP, bronchiolitis obliterans w/ organizing PNA; AIP, acute IP (Hamman-Rich syndrome); DIP, desquamative IP; RB-ILD, resp bronchiolitis-assoc ILD.
• Rx for UIP/IPF: ?? NAC (NEJM 2005;353:2229); pred + AZA harmful (NEJM 2012;366:1968)
Experimental: tyrosine kinase inhib (NEJM 2011;365:1079); pirfenidone (Lancet 2011;377:1760; not avail in U.S.); ? sildenafil (NEJM 2010;363:621); thalidomide for cough (Annals 2012;157:398)
• Steroids for other IIPs: NSIP (esp. cellular type) and COP (AJRCCM 2000;162:571); ? benefit for AIP and DIP/RB-ILD (for which Pts should stop smoking)
Environmental & occupational exposures (NEJM 2000;342:406; Lancet 2012;379:2008)
• Pneumoconioses (inorganic dusts)
Coal worker’s: upper lobe coal macules; may progress to massive fibrosis
Silicosis: upper lobe opacities ± eggshell calcification of lymph nodes; ↑ risk of TB
Asbestosis: lower lobe fibrosis, calcified pleural plaques, DOE, dry cough, rales on exam. Asbestos exposure also → pleural plaques, benign pleural effusion, diffuse pleural thickening, rounded atelectasis, mesothelioma, lung Ca (esp. in smokers).
Berylliosis: multisystemic granulomatous disease that mimics sarcoidosis
• Hypersensitivity pneumonitides (organic dusts): loose, noncaseating granulomas
Antigens: farmer’s lung (spores of thermophilic actinomyces); pigeon fancier’s lung (proteins from feathers and excreta of birds); humidifier lung (thermophilic bacteria)
Collagen vascular diseases (NEJM 2006;355:2655)
• Rheumatologic disease
Scleroderma: fibrosis in ~67%; PHT seen in ~10% of CREST Pts
PM-DM: ILD & weakness of respiratory muscles; MCTD: PHT & fibrosis
SLE & RA: pleuritis and pleural effusions more often than ILD; SLE can cause DAH
• Vasculitis (can p/w DAH)
Wegener’s granulomatosis (![]() c-ANCA) w/ necrotizing granulomas
c-ANCA) w/ necrotizing granulomas
Churg-Strauss syndrome (![]() c- or p-ANCA) w/ eosinophilia & necrotizing granulomas
c- or p-ANCA) w/ eosinophilia & necrotizing granulomas
Microscopic polyangiitis (![]() p-ANCA) w/o granulomas
p-ANCA) w/o granulomas
• Goodpasture’s syndrome = DAH + RPGN; typically in smokers; ![]() anti-GBM in 90%
anti-GBM in 90%
• Lymphangioleiomyomatosis (LAM): cystic, ↑ in ![]() , Rx w/ sirolimus (NEJM 2011;364:1595)
, Rx w/ sirolimus (NEJM 2011;364:1595)
Pulmonary infiltrates w/ eosinophilia (PIE) = eos on BAL ± periph. blood
• Allergic bronchopulmonary aspergillosis (ABPA): allergic reaction to Aspergillus
Criteria: asthma, pulm infiltrates (transient or fixed), skin rxn & serum precipitins to Aspergillus, ↑ IgE to Aspergillus & total (>1000), ↑ eos, central bronchiectasis
Rx: steroids ± itraconazole for refractory cases (NEJM 2000;342:756)
• Löffler’s syndrome: parasites/drugs → transient pulm infilt + cough, fever, dyspnea, eos
• Acute eosinophilic PNA (AEP): acute hypox febrile illness; Rx: steroids, tobacco cessation
• Chronic eosinophilic pneumonia (CEP): “photonegative” of CHF, typically in women
• Other: Churg-Strauss syndrome; hypereosinophilic syndrome
Miscellaneous
• Pulm alveolar proteinosis (PAP): accum of surfactant-like phospholipids; ![]() smokers; white & gummy sputum; BAL milky fluid (NEJM 2003;349:2527); Rx w/ lung lavage & GMCSF
smokers; white & gummy sputum; BAL milky fluid (NEJM 2003;349:2527); Rx w/ lung lavage & GMCSF
• Langerhans cell granulomatosis (LCG): young ![]() smokers; apical cysts; PTX (25%)
smokers; apical cysts; PTX (25%)
• Lymphocytic interstitial PNA: polyclonal B-cell infiltration (? lymphoma); Rx: steroids