RHEUMATOLOGY
RHEUMATOID ARTHRITIS (RA)
Definition & epidemiology (Lancet 2010;376:1094; NEJM 2011;365:2205)
• Chronic, symmetric, debilitating and destructive inflammatory polyarthritis characterized by proliferative synovial tissue (pannus) formation in affected joints
• Genetic (~50% of risk) & environmental factors (eg, smoking, silica dust exposure)
• ↑ risk w/ shared epitope & smoke b/c gene–environment interaction (Ann Rheum Dis 2010;69:70)
• Prevalence=1% adults; 5% of ![]() >70 y;
>70 y; ![]() to
to ![]() ratio=3:1; peak incidence 50–75 y
ratio=3:1; peak incidence 50–75 y
Clinical manifestations (Medicine 2010;38:167)
• Usually insidious onset pain, swelling and impaired function of joints (typically PIPs, MCPs, wrists, knees, ankles, MTPs and cervical spine) with morning stiffness for ≥1 h
• Typically polyarticular (60% small joints, 30% large joints, 10% both), may be monoarticular (knee, shoulder, wrist) early in course; nb, rheumatoid joints can become infected
• Joint deformities: ulnar deviation, swan neck (MCP flexion, PIP hyperextension, DIP flexion), boutonnière (PIP flexion, DIP hyperextension), cock-up deformities (toes)
• C1–C2 instability → myelopathy, ∴✓ C-spine flex/ext films prior to elective intubation
• Constitutional symptoms: low-grade fever, weight loss, malaise
• Extra-articular manifestations (18–41% of Pts) can occur at any time; ↑ frequency in seropositive (RF or anti-CCP) (Autoimmun Rev 2011;11:123)

Laboratory & radiologic studies
• RF (IgM/IgA/IgG anti-IgGAb) in ~70% of Pts; also seen in other rheumatic diseases (SLE, Sjögren’s), infection (SBE, hepatitis, TB), types II & III cryo, 5% of healthy population
• Anti-CCP (Ab to cyclic citrullinated peptide): in ~80% of Pts, similar Se (~70%), more Sp (>90%) than RF particularly for early RA (Arth Rheum 2009;61:1472); a/w increased joint damage and low remission rates
• ~20% are seronegative (RF and anti-CCP negative)
• ↑ ESR/CRP but nl in ~30%; ![]() ANA in ~15%; ↑ globulin during periods of active disease
ANA in ~15%; ↑ globulin during periods of active disease
• Radiographs of hands and wrists: periarticular osteopenia, bone erosions, joint subluxation
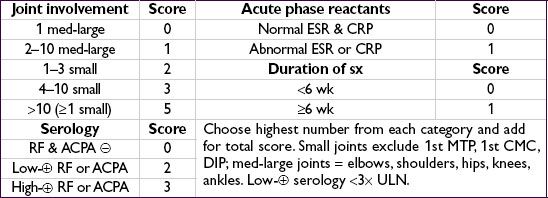
ACR/EULAR classification criteria (Arth Rheum 2010;62:2569)
• Use for Pts with ≥1 joint with synovitis not better explained by another disease
• Summed score of ≥6 c/w RA
Management (Lancet 2009;373:659; Ann Rheum Dis 2010;69:631)
• Early dx and Rx (esp. DMARD) w/ frequent follow-up and escalation of Rx as needed to achieve clinical remission or low disease activity
• ↓ time to remission ![]() ↑ length of sustained remission (Arthritis Res Ther 2010;12:R97)
↑ length of sustained remission (Arthritis Res Ther 2010;12:R97)
• Sero-![]() disease (eg, RF or anti-CCP) a/w aggressive joint disease & EAM
disease (eg, RF or anti-CCP) a/w aggressive joint disease & EAM
• Start both rapid acting agent (to acutely ↓ inflammation) and Disease-Modifying Anti-Rheumatic Drug (DMARD) (typically take 1–3 mo to have max effect) at dx
• Rapid-acting drugs: NSAIDs or COX-2 inhibitors (↑ CV adverse events);
glucocorticoids [low-dose (<20 mg/d oral) or joint injection]; or
NSAIDs + glucocorticoids: ↑ GI adverse events, minimize long-term concurrent use
• DMARDs
MTX (1st line unless CKD, hepatitis, EtOH or lung disease), SAS or leflunomide; consider HCQ if seronegative and mild disease;
if inadequate response after 3 mo (despite DMARD dose escalation): combination Rx w/ other traditional DMARDs (ie, MTX, SAS and HCQ) or biologic (anti-TNF typically 1st line unless contraindication)
• Given ↑ r/o early CV morbidity/mortality, ↓ risk w/ lifestyle mgmt, lipid & DM screening
