Andrea G. Barthwell, MD, FASAM and Lawrence S. Brown Jr., MD, MPH, FASAM
CHAPTER OUTLINE
■ GOALS OF DRUG ADDICTION TREATMENT
■ TREATMENT SETTINGS
■ RESIDENTIAL PROGRAMS, INCLUDING THERAPEUTIC COMMUNITY
■ TREATMENT SERVICES
■ PHARMACOLOGIC THERAPIES
■ CONCLUSION
Drug addiction is a complex illness. Compulsive (at times uncontrollable) drug seeking and use, which persist even in the face of extremely negative consequences, characterize the disorder. For many patients, drug addiction is a chronic disease, with relapses possible even after long periods of abstinence. Patients with substance use disorders are heterogeneous in a number of clinically important features and domains. Because addiction has so many dimensions and disrupts so many aspects of an individual’s life, treatment for this illness never is simple; generally, a multimodal approach to treatment is required. Drug treatment must help the individual stop using drugs and maintain a drug-free lifestyle while achieving productive functioning in the family, at work, and in society. After repeated failures of appropriately matched treatment, some individuals are deemed unable to stop using drugs. In this instance, it is appropriate to work to achieve intermediate outcomes that include a reduction in the use and effects of substances, reduction in frequency and severity of relapse to substance use, and improvement in psychological and social functioning. Physicians are cautioned that the latter is hard to achieve with continued drug use.
Effective treatment programs typically incorporate many components, each directed to a particular aspect of the illness and its consequences. In practice, specific pharmacologic and psychosocial treatments are often combined because combined treatments lead to better treatment retention and outcomes (1). Three decades of scientific research and clinical practice have yielded a variety of approaches to addiction treatment; the most effective match the patient’s assessed needs to services that, research suggests, might have the most impact. Evidence suggests that substance-dependent individuals who achieve sustained abstinence from the abused substance have the best long-term outcomes (2,3). Extensive data show that such treatment is as effective as treatment for most other chronic medical conditions (4). Of course, not all drug treatment is equally effective or applied in a standardized way. To overcome inconsistency and to improve fidelity to conceptualized models, the National Institute on Drug Abuse has manualized therapies. Research also has revealed a set of overarching principles that characterize the most effective drug addiction treatments and their implementation (Table 24-1).
TABLE 24-1 PRINCIPLES OF EFFECTIVE TREATMENT
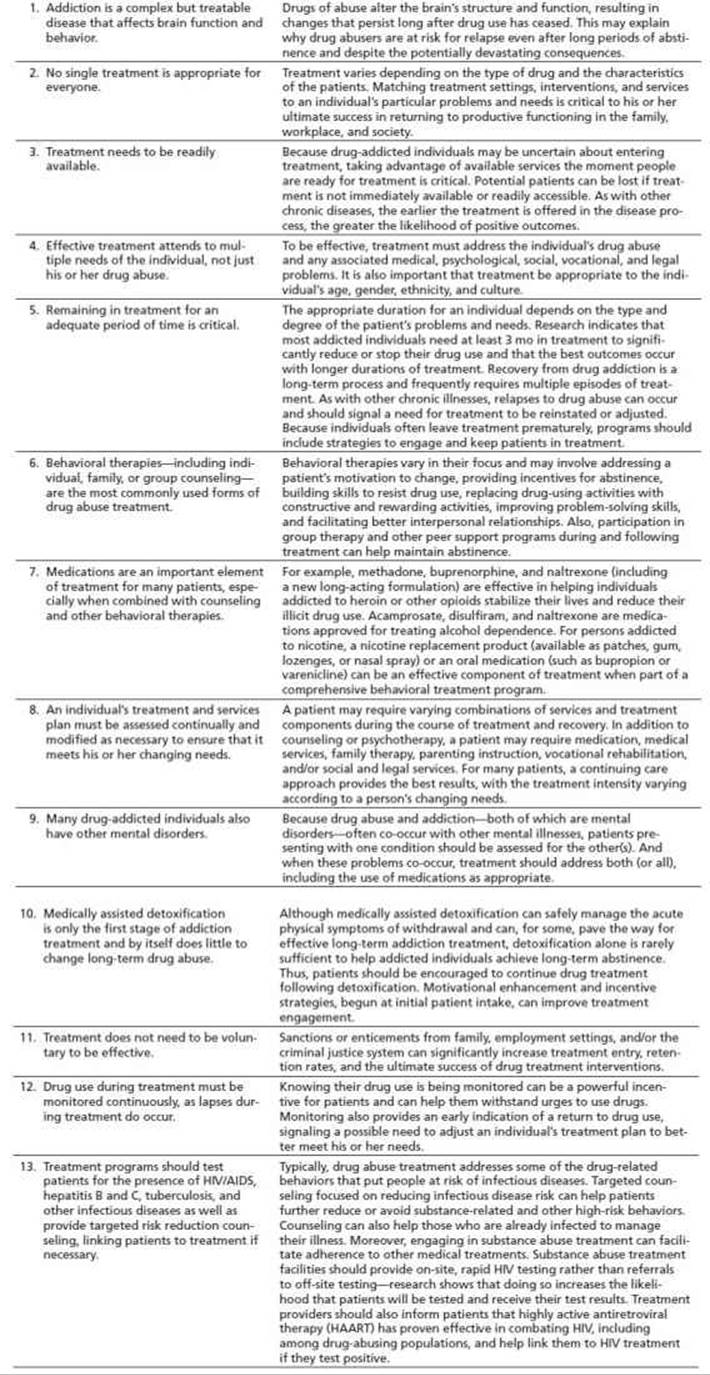
From National Institute on Drug Abuse. Principles of drug addiction treatment: a research-based guide, 3rd ed. Rockville, MD: NIDA (NIH Publication No. 12–4180), 1999:2–5.
GOALS OF DRUG ADDICTION TREATMENT
Drug addiction is a complex disorder that can involve virtually every aspect of an individual’s functioning—in the family, at work, and in the community. Because of addiction’s complexity and pervasive consequences, addiction treatment typically must involve many components. Some of those components focus directly on the individual’s drug use, whereas others, such as employment training, focus on restoring the addicted individual to productive membership in the family and society (Fig. 24-1). Treatment of drug abuse and addiction is delivered in many different settings, using a variety of behavioral and pharmacologic approaches. In the United States, more than 11,000 specialized drug treatment facilities provide rehabilitation, counseling, behavioral therapy, medication, case management, and other types of services to persons with drug use disorders.
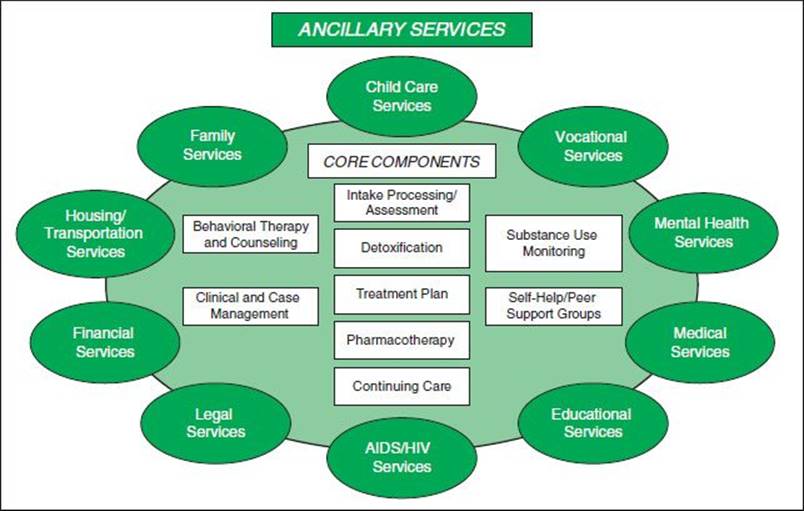
FIGURE 24-1 Components of addiction treatment. (From National Institute on Drug Abuse. Principles of drug addiction treatment—a research-based guide, 3rd ed. NIH Publication No. 12–4180, 2012.)
Care of individuals with substance use disorders includes assessing needs, providing treatment for intoxication and withdrawal, and developing, with appropriate support, the treatment plan that may consist of referrals to psychosocial care. The treatment plan should address how the patient will achieve abstinence without medical compromise, achieve and maintain abstinence after withdrawal, and gain improvement in functioning in the medical, social, and psychological domains.
TREATMENT SETTINGS
The addiction treatment delivery system is primarily a specialty care delivery system, often separate from the medical–surgical delivery system. Funding for care in the system is usually separate, and the professionals in the system are different. Treatment settings vary widely with regard to services and medical support available and the milieu or philosophy. For physicians, assessment for treatment matching and knowledge of referral and funding options in the community are important, as every community is different. Hospital social work departments generally know the local resources, and health maintenance organization case managers can assist with locating specialty providers of addiction medicine. Mental health carve-outs make accessing care complicated for the patient, and physicians may not be allowed to refer to preferred providers who are out of the network of care. Underinsurance for addiction care is common, and benefit limits (any coverage) or lifetime caps (remaining coverage) may preclude care for patients relapsing following prior treatment.
Decisions regarding the site of care should be based on the patient’s ability to cooperate with and benefit from the treatment offered, to refrain from illicit use of substances, and to avoid high-risk behaviors, as well as the patient’s need for structure and support or particular treatments that may be available only in certain settings. Patients move from one level of care to another based on these factors and an assessment of their ability to benefit from a different level of care. Delivery system discontinuities occur when coverage is available for a limited number of levels of care, but not the one indicated based on the assessment carried out using a standardized system such as the American Society of Addiction Medicine (ASAM) Patient Placement Criteria (PPC). ASAM PPC describes four levels of care: (a) general outpatient, (b) intensive outpatient or day hospital, (c) medically monitored inpatient residential care, and (d) medically managed inpatient care. An in-hospital consultant or a member of the medical staff who is knowledgeable and interested in patients with addictive disorders can make criterion-based placement. Sometimes, the payer will insist that external case managers employed by the payer make criterion-based decisions. In some instances, placement decisions are not criteria based.
Hospital-based physicians may find their management of addiction limited to detoxification and referral. It is uncommon to refer outside of the hospital, because either the payer requires referral to a contracted provider or the patient lacks coverage and needs referral to the public system of care. Hospital-based physicians can create an inpatient Addiction Medicine Consultation Service with specialty-trained clinicians and nonphysician clinicians who assess addiction severity and withdrawal potential, manage withdrawal, and refer to posthospital addiction care when the patient no longer requires care in the hospital setting.
Detoxification
According to ASAM PPC-2R, detoxification refers not only to the attenuation of the physiologic and psychological features of withdrawal syndromes but also to the process of interrupting the momentum of compulsive use in persons diagnosed with substance dependence (5). This phase of treatment frequently requires a great intensity of treatment to establish treatment engagement and patient role induction. It can be delivered in ambulatory settings with and without extended on-site monitoring. In residential or inpatient settings, it is delivered under clinically managed, medically monitored, or medically managed conditions. There is increasing intensity of services and involvement of nursing and medical personnel across the latter continuum. A full description of services available in each setting can be found elsewhere in this text.
Hospital Settings
Hospitalization is appropriate for patients whose assessed need cannot be treated safely in an outpatient or emergency department setting because of (a) acute intoxication, (b) severe or medically complicated withdrawal potential, (c) co-occurring medical or psychiatric conditions that complicate detoxification or impair treatment engagement and response, (d) failure of engagement in treatment at a lower level of care, (e) life- or limb-threatening medical conditions that would require hospitalization, (f) psychiatric disorders that make the patient an imminent threat to self or others, and (h) failure to respond to care at any level such that the patient endangers others or poses a self-threat. Aside from detoxification and management of overdose or intoxication, most patients are receiving services incident to a medical–surgical need to manage a biomedical condition or complication or a psychiatric need to manage an emotional or behavioral condition in a primary psychiatric setting. The physician must evaluate the timing and intensity of addiction medicine services in the context of other concerns.
Partial Hospital Programs and Intensive Outpatient
Partial hospitalization is considered for patients who require intensive care but have a reasonable chance of making progress on treatment goals in the intertreatment interval, including maintenance of abstinence. It is often provided to individuals whose treatment is hospital or residential initiated and who still require frequent and concentrated contact with treatment professionals to monitor their behavior and manage their risk of relapse. These patients often have a history of relapse after completion of treatment or are returning to a high-risk environment and have a need to develop support for their recovery-focused efforts beyond the treatment system. Lack of motivation to continue to build on the gains made in the treatment, allowing the treatment effect to erode, is often cause to continue the patient in this highly intensive and structured setting. Intensive outpatient programs have been proven to be effective when working with special subgroups of patients, such as those who are economically disadvantaged, psychiatrically compromised, and pregnant or who have been coerced into treatment by the criminal justice system or outside parties (6). The difference between partial hospital programs and intensive outpatient is seen in intensity, number of hours per day, setting of the program, and structure of the program. Patients who are not successful in intensive outpatient may have clinical contact increased by transfer to partial hospital programs.
Outpatient Programs
This treatment varies in the types and intensity of services offered, ranging from specialty programs to individual physician offices and primary care settings. It costs less than residential or inpatient treatment and often is more suitable for individuals whose ASAM PPC shows insight into his or her disease, a high degree of predicted compliance, low symptomatology, high resource availability and use, and a supportive structure in his or her home environment. Low-intensity programs may offer little more than drug education and admonition; however, as in the other treatment settings, a comprehensive approach is optimal, using— where indicated—a variety of psychotherapeutic and pharmacologic interventions along with behavioral monitoring. High rates of attrition can be problematic, particularly in the early phase. Because outcomes are highly correlated with time in treatment, retention should be one focus of treatment, along with self-efficacy regarding adherence to the abstinence plan. Self-help participation is useful (7).
Other outpatient models, such as intensive day treatment, can be comparable to residential programs (see below “Residential Programs, Including Therapeutic Community”) in services and effectiveness, depending on the individual patient’s characteristics and needs. In many outpatient programs, as in much of treatment in general, group counseling is emphasized. Some outpatient programs are designed to treat patients who have medical or mental health problems in addition to their drug disorder (8).
Most alcohol abuse and dependence are treated outside of the hospital after medical complications associated with detoxification are addressed (9,10). Similarly, cocaine abuse and dependence (11), nicotine dependence (12), and marijuana abuse and dependence are treated on an outpatient basis as long as the focus on reduced substance use can be maintained and there are no other reasons for hospitalization (13,14).
RESIDENTIAL PROGRAMS, INCLUDING THERAPEUTIC COMMUNITY
Residential programs provide care 24 hours a day, generally in nonhospital settings. Residential care is generally provided to patients who do not meet the clinical criteria for hospitalization but whose lives are transformed by and focused on substance use. These individuals are unlikely to maintain abstinence in the absence of continued application of a variety of therapeutic techniques in a highly structured and supportive environment. Short-term programs provide intensive but relatively brief residential treatment based on a modified 12-step approach and may or may not include elements of therapeutic communities (TCs) (see the following paragraph). The duration of residential treatment should be determined by the clinical response to therapy and the length of time necessary for the patient to meet specific criteria predictive of success in a lower level of care according to ASAM PPC. In general, longer programs provide better outcomes (15). These programs originally were designed to treat alcohol problems, but during the cocaine epidemic of the mid-1980s, many began to treat illicit drug abuse and addiction. The original residential treatment model consisted of a 3- to 6-week hospital-based inpatient treatment phase, followed by extended outpatient therapy and participation in a self-help group such as Alcoholics Anonymous. Reduced health care coverage for addiction treatment has resulted in a diminished number of these programs, and the average length of stay under managed care review is much shorter than in early programs.
One residential treatment model is the TC, but residential treatment programs also employ other models, such as cognitive–behavioral therapy. TCs are residential programs with planned lengths of stay from 6 to 12 months. TCs focus on the “resocialization” of the individual and use the program’s entire “community”—including other residents, staff, and the social context—as active components of treatment. Addiction is viewed in the context of an individual’s social and psychological deficits, so treatment focuses on developing personal accountability and responsibility and socially productive lives. Treatment is highly structured and can at times be confrontational, with activities designed to help residents examine damaging beliefs, self-concepts, and patterns of behavior and to adopt new, more harmonious and constructive ways to interact with others. Many TCs are quite comprehensive and include employment training and other support services on-site or through formal linkage agreements. Compared with patients in other forms of drug treatment, the typical TC resident has more chronicity and criminal involvement. Research shows that TCs can be modified to treat individuals with special needs, including adolescents, women (16,17), those with severe mental disorders (18), and individuals in the criminal justice system. Recently, with pressure from reimbursement sources, the elements of TCs have been incorporated into shorter-term residential programs and institutional criminal justice settings.
Heroin addiction has been effectively treated in the TC; however, return to use rates after TC treatment is higher than 80% in most long-term follow-up studies, indicating a need for selectivity in application of this modality over medication-assisted clinical settings (19). Data regarding the effectiveness of traditional long-term TC are limited by the low completion rates of 15% to 25%, with most attrition occurring during the first 3 months (20). Retention lengths predict outcomes on abstinence with abstinence success rates of 90% for graduates of 2-year programs and 25% for dropouts of the same programs completing less than 1 year (21). Retention rates differ with program sites (22).
Community Residential Rehabilitation
Community residential rehabilitation facilities include “halfway houses” or “sober living facilities,” with the former providing more structure and supervision. Individuals referred to these settings are generally deemed to be at risk for relapse without such support. Often, this setting is offered to the individual whose environmental risk is great or those needing a number of services after primary treatment to address deficits in vocation, employment, and social supports. These services have been shown to significantly improve substance use outcomes for both sexes, but are variable in their impact on young people (23–25).
Case Management
Case management is a collaborative process that assesses, plans, implements, coordinates, monitors, and evaluates the options and services to meet an individual’s health needs (26). It uses communication and available resources to promote quality, cost-effective outcomes.
Case management, although difficult to assess for effectiveness in a rigorous fashion, has been shown to be an effective adjunctive treatment for patients with alcohol use disorders, patients with substance use disorders co-occurring with psychiatric disorders (26), and adolescents (27). Case management is provided to individuals whose social situation and complex needs would impair their ability to adhere to a prescribed treatment plan and follow-up care. Basic needs are often met as part of the service array, which includes as psychoeducation and assistance in comprehension of the extent and nature of the disease for which treatment is provided and advocated (28,29).
Aftercare Programs
Aftercare generally follows an episode of care and is focused on maintenance of gains made in treatment over a prescribed period with less frequent contact than the primary episode of care (e.g., once-weekly monitoring and group therapy after a 6-week intensive outpatient program in which the patient is seen nightly for 3 hours). The patient’s affiliation with a 12-step program is encouraged, and the transition to self-efficacy is monitored.
Treatment in the Physician’s Office, Including Screening and Brief Interventions
The addiction treatment enterprise has traditionally been separate and distinct from addiction medicine, with addiction medicine provided in the context of addiction treatment in sometimes limited ways. Public policies, practices, and laws have worked against the provision of care by physicians for the addicted. For example, the Harrison Narcotics Tax Act was a US federal law that regulated and taxed the production, importation, and distribution of opioids. The courts interpreted this to mean that physicians could prescribe narcotics to patients in the course of normal treatment but not for the treatment of addiction. Despite long-standing barriers to care and the risk of prosecution, physicians have recognized a need to provide care to addicted individuals. Early identification through screening for addictive disorders and brief interventions or referral to treatment is a federal initiative supported by demonstration grants from the Center for Substance Abuse Treatment of the U.S. Department of Health and Human Services. Medications are also available for office-based treatment of alcohol and opioids. Buprenorphine and naltrexone, for example, are both FDA-approved medications used for opioid addiction. Buprenorphine is a synthetic opioid medication that acts as a partial agonist at opioid receptors—it does not produce the euphoria and sedation caused by heroin or other opioids but is able to reduce or eliminate withdrawal symptoms associated with opioid dependence and carries a low risk of overdose. Naltrexone is a synthetic opioid antagonist—it blocks opioids from binding to their receptors and thereby prevents their euphoric and other effects. Naltrexone is also used in office-based alcohol addiction treatment as it blocks opioid receptors that are involved in the rewarding effects of drinking and the craving for alcohol. Other medications used for alcohol addiction treatment are acamprosate, which acts on the gamma-aminobutyric acid and glutamate neurotransmitter systems and is thought to reduce symptoms of protracted withdrawal, and disulfiram, which interferes with the degradation of alcohol, resulting in the accumulation of acetalde-hyde, which, in turn, produces a very unpleasant reaction.
Brief interventions for alcohol use disorders had been studied before being adopted and expanded for substance use disorders (30). Interventions were intended to facilitate treatment of alcohol abuse in settings other than those in the addiction treatment enterprise (e.g., mental health clinics, physician’s offices) (31,32).
Brief interventions include assessment, feedback, responsibility for change, advice, and menu of options provided using empathic listening and encouraged self-efficacy (33). A more extensive review of this area is offered elsewhere in this textbook. The most critical take-home message is that this clinical approach can be used by primary care providers for their patients with harmful substance use because only a small portion of these patients warrant a clinical diagnosis of substance abuse or substance dependence.
Criminal Justice Settings for Mandated Treatment, Including Drug Courts
Research has shown that combining criminal justice sanctions with drug treatment can be effective in decreasing drug use and related crime. Individuals under legal coercion tend to stay in treatment for a longer period and do as well as or better than others not under legal pressure (34). Often, drug-addicted persons encounter the criminal justice system earlier than other health or social systems, and intervention by the criminal justice system to engage the individual in treatment may help to interrupt and shorten a career of drug use (35). Addiction treatment may be delivered before, during, after, or in lieu of incarceration.
Prison-Based Treatment Programs
Offenders with drug disorders may encounter a number of treatment options while incarcerated, including didactic drug education classes, self-help programs, and treatment based on TC or residential milieu therapy models. The TC model has been studied extensively and found to be quite effective in reducing drug use and recidivism to criminal behavior (36). Those in treatment are generally segregated from the general prison population, so that the “prison culture” does not overwhelm progress toward recovery. As might be expected, treatment gains can be lost if inmates are returned to the general prison population after treatment. Research shows that relapse to drug use and recidivism to crime are significantly lower if the drug offender continues treatment after returning to the community (37,38).
Community-Based Treatment for Criminal Justice Populations
Several criminal justice alternatives to incarceration have been tried with offenders who have drug disorders, including limited diversion programs, pretrial release conditional on entry into treatment, and conditional probation with sanctions. The drug court is a promising approach. Drug courts mandate and arrange for drug addiction treatment, actively monitor progress in treatment, and arrange other services for drug-involved offenders. Federal support for planning, implementation, and enhancement of drug courts is provided under the U.S. Department of Justice Drug Courts Program Office. As a well-studied example, the Treatment Accountability and Safer Communities program provides an alternative to incarceration by addressing the multiple needs of drug-addicted offenders in a community-based setting (34). Treatment Accountability and Safer Communities programs typically include counseling, medical care, parenting instruction, family counseling, school and job training, and legal and employment services. The key features of Treatment Accountability and Safer Communities include coordination of criminal justice and drug treatment; early identification, assessment, and referral of drug-involved offenders; monitoring offenders through drug testing; and use of legal sanctions as inducements to remain in treatment.
TREATMENT SERVICES
This section presents several examples of evidence-based treatment approaches and components that have been developed and tested through research supported by the National Institute on Drug Abuse. Each approach is designed to address certain aspects of drug addiction and their consequences for the individual, family, and society. These approaches are best used to enhance and standardize the quality of best practices in existing treatment programs. This section is not a complete list of empirically supported treatment approaches. Additional approaches are under development as part of National Institute on Drug Abuse’s continuing support of treatment research and are reviewed in this section, as well as in Chapters 6, 7, and 8of this textbook.
Somatic services are defined as those used to manage intoxication, withdrawal syndromes, and pathophysiologic effects and other clinical manifestations of the substance used. Medications are seen as adjunctive to behavioral therapies and self-help involvement and are viewed as best used on a platform of talk therapy. Behavioral therapies and medications are provided in a number of settings, including hospitals and by hospitalists and other primary care specialists in office-based settings. These services are based on scientific advances in the behavioral sciences and neurobiology of a wide range of drugs, alcohol, tobacco, and other psychoactive substances. These services are discussed in more detail in Sections 7 and 8 of this textbook.
Clinical Monitoring
As with the treatment of other medical disorders and irrespective of the therapeutic approach chosen, clinical monitoring is extremely important in achieving successful clinical options. Although many studies have underscored the limitations of relying solely on a patient’s self-report (39), this type of information is most useful in the context of a non-confrontational, nonjudgmental, patient–provider relationship based on openness, understanding, and empathy. It should also be explicitly recognized that patients receiving care for other chronic disorders also underreport unhealthy behaviors to their caregivers, and, because substance use is stigmatized and often illegal, underreporting is understandable as is the expectation that reports be objectively verified.
Because of the limitations of self-report in the initial assessment and during clinical monitoring, clinical drug testing represents an important tool for addiction medicine specialists (40,41) but is underused and often misunderstood by primary care providers (42,43). When used in concert with a good history, physical examination, and biologic markers, clinical drug testing facilitates screening, assessment, diagnosis, and clinical monitoring of a substance use disorder in the hands of an experienced practitioner. Drug testing provides useful information about a patient’s potential for achieving desirable clinical outcomes with co-occurring medical or psychiatric disorders.
Managing Intoxication and Withdrawal
Similar to the treatment of other clinical disorders, patients with substance use disorders exhibit varied clinical presentations, from acute and subacute to chronic manifestations. Some manifestations, such as intoxication and withdrawal, can be life-threatening without appropriate, if not emergent intervention. The therapeutic response is contingent on the substance used, the presence or absence of evidence of a compromised cardiopulmonary system, and the underlying health status of the patient. Pharmacotherapy is the cornerstone for patients suffering from either intoxication or withdrawal, although effective treatment for intoxication requires a hospital setting, whereas withdrawal can be treated in either an inpatient or outpatient setting.
Detoxification is a commonly used approach in responding to patients with clinical signs of intoxication or withdrawal. It is a process in which, under the care of a physician, individuals are systematically withdrawn from addicting drugs in an inpatient or outpatient setting. Detoxification is intended to reduce or eliminate the medical consequences of withdrawal, the pain of withdrawal, or the acute increase in craving experienced by the patient. Detoxification is a precursor to treatment because it addresses the acute physiologic effects of stopping drug use. Medications are available for detoxification from opioids, nicotine, benzodiazepines, alcohol, barbiturates, and other sedatives. Detoxification is not designed to address the psychological, social, and behavioral problems associated with addiction; therefore, this clinical approach does not typically produce the type of lasting behavior changes necessary for recovery. Detoxification is most useful when it incorporates formal processes of assessment and referral to subsequent addiction treatment (43).
Behavioral Therapy
Numerous studies have demonstrated that behavioral counseling is effective treatment for substance use disorders. Although these services are a part of most treatment modalities in most settings, they are particularly important for the treatment of substance use disorders for which pharmacologic treatments are inefficacious. These therapies attempt to arrest compulsive substance use through modification of behaviors, feelings, social functioning, and thoughts. They address a set of common tasks and attempt to increase motivation, expand the coping repertoire, change reinforcement contingencies to increase the frequency of positive behaviors, improve mood, and enhance interpersonal connection and the number of social supports. Because no form of psychotherapy has proven superior to another for all patients, successful referral to services is more important than physician determination of the most useful approach. In other words, a lack of knowledge regarding how to match patients to the various techniques should not be an excuse to avoid this task. In fact, failure to refer to adjunctive psychotherapy is associated with reduced efficacy of known effective pharmacotherapy because medications frequently address only part of the substance dependence syndrome (44–46).
Cognitive–Behavioral Therapy
Cognitive–behavioral therapy is based on the theory that learning processes play a critical role in the development of maladaptive patterns of behavior. Cognitive–behavioral therapy targets two processes: dysfunctional thoughts and maladaptive behaviors. Thought-based interventions focus on increasing the patient’s resolve not to use—based on negative and positive consequences of use—and confronting thoughts about use. Relapse prevention is an example of cognitive–behavioral therapy with which physicians might be familiar. Relapse prevention was developed for the treatment of problem drinking and later adapted to other substance use disorders. Relapse prevention encompasses several cognitive–behavioral strategies that facilitate abstinence as well as provide help for persons who experience relapse. The goal of relapse prevention is to help addicted individuals learn to identify and correct problematic behaviors. For example, the relapse prevention approach to the treatment of cocaine addiction consists of a collection of strategies intended to enhance self-control (47). Specific techniques include exploring the positive and negative consequences of continued use, self-monitoring to recognize drug cravings early on and to identify situations that pose high risk of use, and developing strategies for coping with and avoiding high-risk situations and the desire to use. A central element of this treatment is anticipating the problems patients are likely to meet and helping them develop effective coping strategies. Research indicates that the skills individuals learn through relapse prevention therapy remain after the completion of treatment (48). In one study, most persons receiving this cognitive–behavioral approach maintained the gains they made in the treatment throughout the year after discharge (49–54).
Motivational Enhancement Therapy
Motivational enhancement therapy is a patient-centered counseling approach that attempts to initiate behavior change by helping patients resolve their ambivalence about engaging in treatment and stopping drug use. This approach employs strategies to evoke rapid and internally motivated change in the client, rather than guiding the client stepwise through the recovery process. The therapy provides feedback generated from an initial assessment to stimulate discussion regarding personal substance use and to elicit self-motivational statements. Motivational interviewing principles are used to strengthen motivation and build a plan for change. Coping strategies for high-risk situations are suggested and discussed with the client. Over time, the therapist monitors change, reviews cessation strategies being used, and continues to encourage commitment to change or to sustained abstinence. Clients sometimes are encouraged to bring a significant other to sessions. This approach has been used successfully with alcohol- and cannabis-dependent individuals (50–52).
Community Reinforcement Approach Plus Vouchers
Community reinforcement approach is an intensive outpatient therapy for the treatment of cocaine addiction. The treatment has dual goals: to achieve cocaine abstinence long enough for patients to learn new life skills that will help sustain abstinence and to reduce alcohol consumption for patients, whose drinking is associated with cocaine use. Patients attend one or two individual counseling sessions per week, where they focus on improving family relations, learning a variety of skills to minimize drug use, receiving vocational counseling, and developing new recreational activities and social networks. Those who also abuse alcohol receive clinic-monitored disulfiram (Antabuse) therapy. Patients submit urine samples two or three times per week and receive vouchers for cocaine-negative samples. The value of the vouchers increases with consecutive clean samples. Patients may exchange their vouchers for retail goods that are consistent with a cocaine-free lifestyle. This approach facilitates patients’ engagement in treatment and systematically aids them in gaining substantial periods of cocaine abstinence. The approach has been tested in urban and rural areas and used successfully in outpatient detoxification of opioid-addicted adults and with inner-city methadone maintenance patients who have high rates of intravenous cocaine abuse (53,54).
A computer-based version of CRA plus vouchers called the therapeutic education system was found to be nearly as effective as treatment administered by a therapist in promoting abstinence from opioids and cocaine among opioid-dependent individuals in outpatient treatment. A version of CRA for adolescents addresses problem-solving, coping, and communication skills and encourages active participation in positive social and recreational activities.
Voucher-Based Reinforcement Therapy in Methadone Maintenance Treatment
Voucher-based reinforcement therapy helps patients achieve and maintain abstinence from illegal drugs by providing them with a voucher each time they provide a drug-free urine sample. The voucher has monetary value and can be exchanged for goods and services consistent with the goals of treatment. Initially, the voucher values are low, but their value increases with the number of consecutive drug-free urine specimens the individual provides. Cocaine- or heroin-positive urine specimens reset the value of the vouchers to the initial low value. The contingency of escalating incentives is designed specifically to reinforce periods of sustained drug abstinence. Studies show that patients receiving vouchers for drug-free urine samples achieved significantly more weeks of abstinence and significantly more weeks of sustained abstinence than patients who were given vouchers independent of urine toxicology results. In another study, urine toxicology positive for heroin decreased significantly when the voucher program was started and increased significantly when the program was stopped (12).
Day Treatment with Abstinence Contingencies and Vouchers
This approach was developed to treat crack addiction among homeless persons (55). For the first 2 months, participants were required to spend 5.5 hours daily in the program, which provided lunch and transportation to and from shelters. Interventions included individual assessment and goal setting, individual and group counseling, multiple psychoeducational groups (e.g., didactic groups on community resources, housing, cocaine, and HIV/AIDS prevention; establishment and review of personal rehabilitation goals; relapse prevention; and weekend planning), and patient-governed community meetings, in which patients reviewed contract goals and provided support and encouragement to each other. Individual counseling occurs once per week, and group therapy sessions are held three times per week. After 2 months of day treatment and at least 2 weeks of abstinence, participants graduate to a 4-month work component that pays wages, which can be used to rent inexpensive, drug-free housing. A voucher system also rewards drug-free social and recreational activities (56). This innovative day treatment was compared with treatment consisting of twice-weekly individual counseling and 12-step groups, medical examinations and treatment, and referral to community resources for housing and vocational services. Innovative day treatment followed by work and housing (dependent on drug abstinence) had a more positive effect on alcohol use, cocaine use, and days of homelessness (57,58).
Psychodynamic Therapy/Interpersonal Therapy
Individualized counseling focuses directly on reducing or stopping the patient’s illicit drug use. It also addresses related areas of impaired functioning—such as employment status, illegal activity, and family/social relations—as well as the content and structure of the patient’s recovery program. Through its emphasis on short-term behavioral goals, individualized drug counseling helps the patient develop coping strategies and tools for abstaining from drug use and then maintaining abstinence. The addiction counselor, social worker, or psychologist encourages 12-step program participation and makes referrals for needed supplemental medical, psychiatric, employment, and other services. Individuals are encouraged to attend sessions one or two times per week. In a study that compared opioid-dependent patients receiving methadone alone with those receiving methadone coupled with counseling, individuals who received methadone alone showed minimal improvement in reducing opioid use (59). The addition of counseling produced significantly more improvement. The addition of on-site medical, psychiatric, employment, and family services further improved outcomes. In another study with cocaine-dependent patients, individualized drug counseling, together with group counseling, was quite effective in reducing cocaine use (60). Thus, it appears that this approach has great utility in outpatient treatment for both heroin and cocaine addiction.
Supportive expressive psychotherapy is a time-limited, focused psychotherapy that has been adapted for heroin-and cocaine-addicted individuals (61). The therapy has two main components: supportive techniques to help patients feel comfortable in discussing their personal experiences and expressive techniques to help patients identify and work through interpersonal relationship issues. Special attention is paid to the role of drugs in relation to problem feelings and behaviors and how problems may be solved without recourse to drugs. The efficacy of individual supportive– expressive psychotherapy has been tested with patients in methadone maintenance treatment who had co-occurring psychiatric disorders (62). In a comparison with patients receiving drug counseling only, both groups fared similarly with regard to opioid use, but the supportive–expressive psychotherapy group had lower cocaine use and required less methadone. In addition, the patients who received supportive–expressive psychotherapy maintained many of the gains they had made. In an earlier study, supportive– expressive psychotherapy, when added to drug counseling, improved outcomes for opioid-dependent patients in methadone treatment with moderately severe psychiatric problems (57,58).
Treatment of the Adolescent with Multidimensional Family Therapy
Multidimensional family therapy is an outpatient, family-based, drug treatment approach for adolescents. It approaches adolescent drug use in terms of a network of influences (individual, family, peer, and community) and suggests that reducing unwanted behavior and increasing desirable behavior occur in multiple ways in different settings. Treatment includes individual and family sessions held in the clinic, in the home, or with family members at the family court, school, or other community locations. During individual sessions, the therapist and adolescent work on important developmental tasks, such as decision-making, negotiation, and problem-solving skills. Teens acquire skills in communicating their thoughts and feelings to deal better with life stressors and vocational skills. Parallel sessions are held with family members. Parents examine their particular parenting styles, learn to distinguish influence from control, and learn how to have a positive and developmentally appropriate influence on their child (63,64).
Multisystemic Therapy
Multisystemic therapy addresses the factors associated with serious antisocial behavior in children and adolescents who use drugs. These factors include characteristics of the adolescent (e.g., favorable attitudes toward drug use), the family (poor discipline, family conflict, or parental drug abuse), peers (positive attitudes toward drug use), school (dropout, poor performance), and neighborhood (criminal subculture) (65). By participating in intense treatment in natural environments (homes, schools, and neighborhood settings), most youths and families complete a full course of treatment. Multisystemic therapy significantly reduces adolescent drug use during treatment and for at least 6 months after treatment. Reduced numbers of incarcerations and out-of-home placements of juveniles (66) offset the cost of providing this intensive service and maintaining the clinicians’ low caseloads (67). For more information on treatment of adolescents, see Section 13 of this textbook.
Computer-Assisted Therapy
There is a growing body of literature that supports the use of technology in the treatment of the addictions, using computer-assisted therapies (CAT) through online counseling, self-help resources, and text messaging. A number of randomized controlled trials (RCTs) have been conducted in recent years examining the efficacy of CAT for addiction to a number of substances, with some of these demonstrating that this intervention approach may significantly reduce substance use behavior and biochemical measures of substance use. Formal CAT programs are usually clinician facilitated, although some are developed to be used independently by the addicted individual. A number of online CAT programs were developed and evaluated in RCTs, including a smoking cessation program, CHESS (68), and a computerized version of cognitive–behavioral therapy (CBT4CBT). When compared with participants receiving standard treatment, participants receiving the CBT4CBT and/or the CHESS program were demonstrated to provide a significantly higher number of negative urine samples and achieve longer periods of abstinence (69). Further CAT programs are used throughout the addictions treatment field, although there is a paucity of RCT data to support their use. For example, the MAP Program at the Origins Recovery Centers and Hazelden MORE (My Ongoing Recovery Experience) program are CAT programs used within these treatment centers that are not available to individuals who are not receiving such “in-house” treatment.
In addition to formal CAT, online counseling and information programs have also been evaluated. In an RCT with 206 young people with cannabis misuse problems, the “quit the shit” program (70) was evaluated. This program incorporates self-help, counseling, keeping a diary of cannabis consumption, and monitoring of a range of mental health outcomes such as anxiety and depression. Compared to wait-list controls, participants randomized to the “quit the shit” program were demonstrated to have significantly reduced self-reported cannabis use, and there were some small improvements in mental health outcomes.
Removing the need for direct therapist involvement, online self-help resources for the addictions have also been evaluated in a number of studies. For example, an RCT of an online, multicomponent, self-help program for problem alcohol consumption (71) with 261 problem drinkers provided some support for the efficacy of this kind of intervention. When compared with control participants exposed to an online brochure regarding the effects of problem alcohol consumption, participants exposed to the self-help program reduced their self-reported alcohol consumption significantly more than the control group.
The Internet may also provide a useful format for screening for substance problems and also for providing brief interventions. An RCT of a Web-based alcohol screening and brief intervention program (72) with 576 problem drinking university students found that compared to no-treatment controls, those using the program experienced a reduction in problem drinking. This reduction in drinking was accompanied by a reduction in associated psychosocial problems, with both these outcomes being maintained at 6- and 12-month follow-up.
Moving beyond online programs, the use of technology to treat addictions has extended into the use of cell phones and text messaging interventions. For example, the “txt2stop” smoking cessation program has recently been evaluated using an RCT methodology with 5,524 smokers. Compared to controls, significantly more participants using the “txt2stop” program achieved abstinence from smoking at 6-month follow-up, with this abstinence being biochemically verified. These findings appear to be partially verified by a recent Cochrane Review (73), in which five studies were included in a meta-analysis, resulting in an outcome indicating an overall benefit at 6-month follow-up in terms of abstinence. However, the authors of the review report that this finding should be interpreted with caution due to some heterogeneity across the five studies included. Some research has now started looking at the efficacy of using cell phone technology in treating problem alcohol consumption (74) and cannabis use (75), although more research is needed before any firm conclusions can be drawn regarding the efficacy of such a treatment approach for the addictions.
PHARMACOLOGIC THERAPIES
Opioid Agonist Treatment
Also referred to as agonist or maintenance treatment for opioid-dependent patients, opioid agonist treatment usually is conducted in outpatient treatment settings, such as methadone treatment programs or the physician’s office. These programs use a long-acting synthetic opioid medication, usually methadone or buprenorphine, administered orally for a sustained period at a dose sufficient to prevent opioid withdrawal, block the effects of illicit opioid use, and decrease opioid craving. Buprenorphine is currently available in two formulations that are taken sublingually: (a) a pure form of the drug and (b) a more commonly prescribed formulation called Suboxone, which combines buprenorphine with the drug naloxone, an antagonist (or blocker) at opioid receptors. Naloxone has no effect when Suboxone is taken as prescribed, but if an addicted individual attempts to inject Suboxone, the naloxone will produce severe withdrawal symptoms. Thus, this formulation lessens the likelihood that the drug will be abused or diverted to others. Buprenorphine treatment for detoxification and/or maintenance can be provided in office-based settings by qualified physicians who have received a waiver from the Drug Enforcement Administration, allowing them to prescribe it. The availability of office-based treatment for opioid addiction is a cost-effective approach that increases the reach of treatment and the options available to patients.
Patients stabilized on adequate, sustained doses of methadone or buprenorphine can function normally. They can hold jobs, avoid the crime and violence of the drug culture, and reduce their exposure to HIV by stopping or decreasing injection drug use and drug-related high-risk sexual behaviors (76–80). Indeed, the infection-reducing benefit of substance abuse treatment programs is most robust in those programs providing opioid agonist therapies (81,82). Patients stabilized on opioid agonists can engage more readily in counseling and other behavioral interventions that are essential to recovery and rehabilitation. The most effective opioid agonist maintenance programs include individual or group counseling, as well as provision of, or referral to, other needed medical, psychological, and social services. Criteria for management in the physician’s office have been described, and physicians are advised to engage with local providers of substance abuse care to provide services that may be beyond the scope or ability of the office-based practice.
Narcotic Antagonist Treatment Using Naltrexone
Antagonist therapies are used to block or counteract the physiologic or subjective reinforcing effects of substances. Treatment of opioid-dependent patients with naltrexone usually is conducted in outpatient settings, although initiation of the medication often begins after medical detoxification in a residential setting. Naltrexone is a long-acting synthetic opioid antagonist with few side effects that is taken orally, either daily or three times per week, for a sustained period. Candidates for therapy with naltrexone must be medically detoxified and opioid-free for several days before the drug can be given, to avoid precipitating the opioid abstinence syndrome. When naltrexone is used in this fashion, it completely blocks the effects of self-administered opioids, including euphoria. The theory behind this treatment is that the repeated lack of the desired opioid effects, as well as the perceived futility of using the opioid, will gradually extinguish the habit of opioid addiction. Naltrexone itself has no subjective effects or potential for abuse and is not addicting. Patient noncompliance is a common problem; therefore, a favorable treatment outcome requires that there also be a positive therapeutic relationship, effective counseling or therapy, and careful monitoring of medication compliance (83). Many experienced clinicians have found naltrexone most useful for highly motivated, recently detoxified patients who desire total abstinence because of external circumstances, including impaired professionals, parolees (84), probationers, and prisoners in work-release status. Patients stabilized on naltrexone can function normally. They can hold jobs, avoid the crime and violence of the street culture, and reduce their exposure to HIV by stopping injection drug use and drug-related high-risk sexual behaviors. Compared to naloxone, naltrexone has a good oral bioavailability and a relatively long half-life. Its availability as a long-acting injectable preparation may improve treatment adherence (85,86).
CONCLUSION
Although this chapter has not been exhaustive in its coverage of all the behavioral or medication-assisted therapies in use, at the writing of this chapter, many other pharmacotherapies are in various stages of development. Similarly, variants of current behavioral therapies and combinations of pharmacotherapies and behavioral therapies are also under investigation, focused on expanding the array of options to treat substance use disorders associated with the most prevalent psychoactive substances. Even so, dissemination remains a challenge that requires the highest priorities if patients with substance use disorders in various clinical settings are to benefit from the advances in the past 30 years and those in the future.
REFERENCES
1.Siqueland L, Crits-Christoph P. Current developments in psychosocial treatments of alcohol and substance abuse. Curr Psychiatry Rep 1999;1:179–184.
2.Vaillant GE. A long-term follow-up of male alcohol abuse. Arch Gen Psychiatry 1996;53:243–249.
3.Vaillant GE. A 60-year follow-up of alcoholic men. Addiction 2003;98:1043–1051.
4.McLellan AT, O’Brien CP, Lewis DL, et al. Drug addiction as a chronic medical illness: implications for treatment, insurance, and evaluation. JAMA 2000;284:1689–1695.
5.Mee-Lee D, ed. ASAM patient placement criteria for the treatment of substance-related disorders, 2nd ed. revised. Chevy Chase, MD: American Society of Addiction Medicine, 2001.
6.Center for Substance Abuse Treatment. Substance Abuse: Clinical Issues in Intensive Outpatient Treatment. 2006. Substance Abuse and Mental Health Services Administration (US), Rockville, MD. http://www.ncbi.nlm.nih.gov/books/NBK64093/. Accessed February 4, 2013.
7.Klamen DL. Education and training in addictive diseases. Psychiatric Clin N Am 1999;22(2):471–480.
8.Kleber H, Slobetz F. Outpatient drug-free treatment. In: DuPont RL, Goldstein A, O’Donnell J, eds. Handbook on drug abuse. Rockville, MD: National Institute on Drug Abuse, 1979:31–38.
9.Institute of Medicine. Treating drug problems. Washington, DC: National Academy Press, 1990.
10.McLellan AT, Grisson G, Durell J, et al. Substance abuse treatment in the private setting: are some programs more effective than others? J Subst Abuse Treat 1993;10:243–254.
11.Simpson DD, Joe GW, Brown BS. Treatment retention and follow-up outcomes in the Drug Abuse Treatment Outcome Study. Psychol Addict Behav 1997;11:294–307.
12.Higgins ST, Budney AJ, Bickel WK, et al. Incentives improve outcome in outpatient behavioral treatment of cocaine dependence. Arch Gen Psychiatry 1994;51:568–576.
13.Fiore MC, Smith SS, Jorenby DE, et al. The effectiveness of the nicotine patch for smoking cessation: a meta-analysis. JAMA 1994;271:1940–1947.
14.Miller WR, Wilbourne PL, Hettema JE. What works? A summary of alcohol treatment outcome research. In: Hester RK, Miller WR, eds. Handbook of alcoholism treatment approaches: effective alternatives, 3rd ed. Needham Heights, MA: Allyn & Bacon, 2003:13–63.
15.Leukefeld C, Pickens R, Schuster CR. Improving drug abuse treatment: recommendations for research and practice. In: Pickens RW, Luekefeld CG, Schuster CR, eds. Improving drug abuse treatment (NIDA research monograph series). Rockville, MD: National Institute on Drug Abuse, 1991.
16.Lewis BF, McCusker J, Hindin R, et al. Four residential drug treatment programs: project IMPACT. In: Inciardi JA, Tims FM, Fletcher BM, eds. Innovative approaches in the treatment of drug abuse. Westport, CT: Greenwood Press, 1993:45–60.
17.Stevens S, Arbiter N, Glider P. Women residents: expanding their role to increase treatment effectiveness in substance abuse programs. Int J Addict 1989;24(5):425–434.
18.Stevens SJ, Glider PJ. Therapeutic communities: substance abuse treatment for women. In: Tims FM, De Leon G, Jainchill N, eds. Therapeutic community: advances in research and application (NIDA research monograph 144). Rockville, MD: National Institute on Drug Abuse, 1994;162–180.
19.Sacks S, Sacks J, DeLeon G, et al. Modified therapeutic community for mentally ill chemical abusers: background; influences; program description; preliminary findings. Subst Use Misuse 1998;32(9):1217–1259.
20.Simpson DD, Sells S, eds. Opioid addiction and treatment: a 12-year follow-up. Melbourne, FL: Robert E. Krieger, 1990.
21.De Leon G, Schwartz S. Therapeutic communities: what are the retention rates? Am J Drug Alcohol Abuse 1984;10:267–284.
22.De Leon G. The therapeutic community: study of effectiveness. Rockville, MD: National Institute on Drug Abuse, 1984.
23.Friedmann PD, Hendrickson JC, Gerstein DR, et al. The effect of matching comprehensive services to patients’ needs on drug use improvement in addiction treatment. Addiction2004;99:962–972.
24.Lemke S, Moos RH. Treatment and outcomes of older patients with alcohol use disorders in community residential programs. J Stud Alcohol 2003;64:219–226.
25.Jason LA, Davis MI, Ferrari JR, et al. Oxford house: a review of research and implications for substance abuse recovery and community research. J Drug Educ 2001;31:1–27.
26.National Case Management Task Forces. CCM certification guide. Rolling Meadows, IL: CIRSC/Certified Case Manager, 1993.
27.Weiner DA, Abraham ME, Lyons J. Clinical characteristics of youths with substance use problems and implications for residential treatment. Psychiatr Serv 2001;52:793–799.
28.Drake RE, Mercer-McFadden C, Mueser KT, et al. Review of integrated mental health and substance abuse treatment for patients with dual disorders. Schizophr Bull 1998;24:589–608.
29.Godley MD, Godley SH, Dennis ML, et al. Preliminary outcomes from the assertive continuing care experiment for adolescents discharged from residential treatment. J Subst Abuse Treat 2002;23:21–32.
30.Graham K, Timney CB. Case management in addictions treatment. J Subst Abuse Treat 1990;7:181–188.
31.McNeese-Smith DK. Case management within substance abuse treatment programs in Los Angeles County. Care Manag J 1999;1:10–18.
32.Miller WR, Rollnick S. Motivational interviewing: preparing people for change, 2nd ed. New York, NY: Guilford, 2002.
33.Edwards G, Orford J, Egert S, et al. Alcoholism: a controlled trial of “treatment” and “advice.” J Stud Alcohol 1977;38:1004–1031.
34.Bien TH, Miller WR, Tonigan JS. Brief interventions for alcohol problems: a review. Addiction 1993;88:315–335.
35.Baker A, Lewin T, Reichler H, et al. Evaluation of a motivational interview for substance use within psychiatric in-patient services. Addiction 2002;97:1329–1337.
36.Anglin MD, Hser Y. Treatment of drug abuse. In: Tonry M, Wilson JQ, eds. Drugs and crime. Chicago, IL: University of Chicago Press, 1990;393–460.
37.Hiller ML, Knight K, Broome KM, et al. Compulsory community based substance abuse treatment and the mentally ill criminal offender. Prison J 1996;76(2):180–191.
38.Inciardi JA, Martin SS, Butzin CA, et al. An effective model of prison-based treatment for drug-involved offenders. J Drug Issues 1997;27(2):261–278.
39.Wexler HK. Therapeutic communities in American prisons. In: Cullen E, Jones L, Woodward R, eds. Therapeutic communities in American prisons. New York, NY: Wiley & Sons, 1997.
40.Chen JT, Fang CC, Shyu RS, et al. Underreporting of illicit drug use by patients at emergency departments as revealed by two-tiered urinalysis. Addict Behav 2006;31:2304–2308.
41.Brown RL. Identification and office management of alcohol and drug disorders. In: Fleming MF, Barry KL, eds. Addictive disorders. Baltimore, MD: Mosby Yearbook, 1992.
42.Cone EJ. New developments in biological measures of drug prevalence. In: Harrison L, Hughes A, eds. The validity of self-reported drug use: improving the accuracy of survey estimates (NIDA research monograph 167). Bethesda, MD: National Institute on Drug Abuse, 1997.
43.Warner EA, Friedmann PD. Laboratory testing for drug abuse. Arch Pediatr Adolesc Med 2006;160:854–864.
44.Reisfield GM, Bertholf R, Barkin RL, et al. Urine drug test interpretation: what do physicians know? J Opioid Manag 2007;3:80–86.
45.Kleber HD. Outpatient detoxification from opiates. Prim Psychiatry 1996;1:42–52.
46.Carroll KM, Sinha R, Nich C, et al. Contingency management to enhance naltrexone treatment of opioid dependence: a randomized clinical trial of reinforcement magnitude. Exp Clin Psychopharmacol2002;10:54–63.
47.Fuller RK, Branchey L, Brightwell DR, et al. Disulfiram treatment of alcoholism: a Veterans Administration cooperative study. JAMA 1986;256:1449–1455.
48.Rounsaville BJ, Carroll KM, Back S. Individual psychotherapy. In: Lowinson JH, Ruiz P, Millman RB, et al., eds. Substance abuse: a comprehensive textbook, 4th ed. Baltimore, MD: Lippincott Williams & Wilkins, 2004:653–670.
49.Carroll K, Rounsaville B, Keller D. Relapse prevention strategies for the treatment of cocaine abuse. Am J Drug Alcohol Abuse 1991;17(3):249–265.
50.Carroll K, Rounsaville B, Nich C, et al. One-year follow-up of psychotherapy and pharmacotherapy for cocaine dependence: delayed emergence of psychotherapy effects. Arch Gen Psychiatry1994;51:989–997.
51.Marlatt G, Gordon JR, eds. Relapse prevention: maintenance strategies in the treatment of addictive behaviors. New York, NY: Guilford Press, 1985.
52.Budney AJ, Kandel DB, Cherek DR, et al. College on problems of drug dependence meeting, Puerto Rico (June 1996). Marijuana use and dependence. Drug Alcohol Depend1997;45:1–11.
53.Miller WR. Motivational interviewing: research, practice and puzzles. Addict Behav 1996;61(6):835–842.
54.Stephens RS, Roffman RA, Simpson EE. Treating adult marijuana dependence: a test of the relapse prevention model. J Consult Clin Psychol 1994;62:92–99.
55.Higgins ST, Budney AJ, Bickel WK, et al. Outpatient behavioral treatment for cocaine dependence: one-year outcome. Exp Clin Psychopharmacol 1995;3(2):205–212.
56.Silverman K, Higgins ST, Brooner RK, et al. Sustained cocaine abstinence in methadone maintenance patients through voucher-based reinforcement therapy. Arch Gen Psychiatry1996;53:409–415.
57.McLellan AT, Woody GE, Luborsky L, et al. Is the counselor an “active ingredient” in substance abuse treatment? J Nerv Ment Dis 1988;176:423–430.
58.Woody GE, Luborsky L, McLellan AT, et al. Psychotherapy for opiate addicts: does it help? Arch Gen Psychiatry 1983;40:639–645.
59.Silverman K, Wong C, Higgins S, et al. Increasing opiate abstinence through voucher-based reinforcement therapy. Drug Alcohol Depend 1996;41:157–165.
60.Milby JB, Schumacher JE, McNamara C, et al. Abstinence contingent housing enhances day treatment for homeless cocaine abusers. (NIDA research monograph series 174). Rockville, MD: National Institute on Drug Abuse, 1996.
61.Milby JB, Schumacher JE, Raczynski JM, et al. Sufficient conditions for effective treatment of substance abusing homeless. Drug Alcohol Depend 1996;43:39–47.
62.McLellan AT, Arndt I, Metzger DS, et al. The effects of psychosocial services in substance abuse treatment. JAMA 1993;269(15):1953–1959.
63.Luborsky L. Principles of psychoanalytic psychotherapy: a manual for supportive-expressive (SE) treatment. New York, NY: Basic Books, 1984.
64.Woody GE, McLellan AT, Luborsky L, et al. Twelve month follow-up of psychotherapy for opiate dependence. Am J Psychiatry 1987;144:590–596.
65.Woody GE, McLellan AT, Luborsky L, et al. Psychotherapy in community methadone programs: a validation study. Am J Psychiatry 1995;152(9):1302–1308.
66.Diamond GS, Liddle HA. Resolving a therapeutic impasse between parents and adolescents in multidimensional family therapy. J Consult Clin Psychol 1996;64(3):481–488.
67.Schmidt SE, Liddle HA, Dakof GA. Effects of multidimensional family therapy: relationship of changes in parenting practices to symptom reduction in adolescent substance abuse. J Fam Psychol1996;10(1):1–16.
68.Japuntich SJ, Zehner ME, Smith, SS, et al. Smoking cessation via the internet: a randomized clinical trial of an internet intervention as adjuvant treatment in a smoking cessation intervention. Nicotine Tob Res 2006;8:S59–S67.
69.Carroll K, Ball S, Martino, S. et al. Computer-assisted delivery of cognitive-behavioral therapy for addiction: a randomized trial of CBT4CBT. Am J Psychiatry 2008;165(7):881–888.
70.Tossmann HP, Jonas B, Tensil MD, et al. A controlled trial of an internet-based intervention program for cannabis users. Cyberpsychol Behav Soc Netw 2011;14(11):673–679.
71.Riper H, Kramer, J, Smit F, et al. Web based self help for problem drinkers: a pragmatic randomized trial. Addiction 2008;103(2):218–227.
72.Kypri K, Langley JD, Saunders, JB, et al. Randomized controlled trial of web-based alcohol screening and brief intervention in primary care. Arch Intern Med 2008;168(5):530–536.
73.Whittaker R, Borland R, Bullen C, et al. Mobile phone-based interventions for smoking cessation. Cochrane Database Syst Rev 2009;(4):CD006611.
74.Mctavish FM, Chih MY, Shah D, et al. How patients recovering from alcoholism use a smartphone intervention. J Dual Diagn 2012;8(4):294–304.
75.Laursen D. Counseling young cannabis users by text message. J Comput Med Comm 2010;15(4):646–665.
76.Dole VP, Nyswander M, Kreek MJ. Narcotic blockade. Arch Intern Med 1996;118:304–309.
77.Lowinson JH, Payte JT, Joseph H, et al. Methadone maintenance. In: Lowinson JH, Ruiz P, Millman RB, et al., eds. Substance abuse: a comprehensive textbook. Baltimore, MD: Lippincott Williams & Wilkins, 1996:405–414.
78.Simpson DD. Treatment for drug abuse: follow-up outcomes and length of time spent. Arch Gen Psychiatry 1981;38(8):875–880.
79.Simpson DD, Joe GW, Bracy SA. Six-year follow-up of opioid addicts after admission to treatment. Arch Gen Psychiatry 1982;39(11):1318–1323.
80.Novick DM, Joseph J, Croxson TS, et al. Absence of antibody to human immunodeficiency virus in long-term, socially rehabilitated methadone maintenance patients. Arch Intern Med1990;150(1):97–99.
81.Brown LS, Kritz SA, Goldsmith RJ, et al. Health services for HIV/AIDS, hepatitis C virus, and sexually transmitted infections in substance abuse treatment programs. Public Health Rep2007;122:441–451.
82.Brown LS, Kritz SA, Goldsmith JR, et al. Characteristics of substance abuse treatment programs providing services for HIV/AIDS, hepatitis C virus infection, and sexually transmitted infections: the National Clinical Trials Network. J Subst Abuse Treat 2006;30:315–321.
83.Cornish JW, Metzger D, Woody GE, et al. Naltrexone pharmacotherapy for opioid dependent federal probationers. J Subst Abuse Treat 1997;14(6):529–534.
84.Greenstein RA, Arndt IC, McLellan AT, et al. Naltrexone: a clinical perspective. J Clin Psychiatry 1984;45(9 Part 2):25–28.
85.Resnick RB, Schuyten-Resnick E, Washton AM. Narcotic antagonists in the treatment of opioid dependence: review and commentary. Compr Psychiatry 1979;20(2):116–125.
86.Resnick RB, Washton AM. Clinical outcome with naltrexone: predictor variables and follow-up status in detoxified heroin addicts. Ann N Y Acad Sci 1978;11:241–246.