Definition
• Clinical: bronchiolitis obliterans syndrome (BOS) is defined by irreversible decrease in FEV1 posttransplantation that is not due to any other cause
• Pathological (BO): submucosal fibrosis of small airways with or without inflammation; intimal vascular fibrosis can occur but is of much less clinical significance
Pathogenesis
• Multifactorial; risk factors include acute rejection and, potentially, infection, prolonged graft ischemic time, and reperfusion injury
Clinical features
Epidemiology
• Present in 49% at 5 years and in 75% by 10 years after transplantation
Presentation
• May occur within weeks to several months to years after transplantation
• Increased difficulty in breathing
• Worsening pulmonary function tests
Prognosis and treatment
• With aggressive treatment, chronic rejection may remain stable for a few years
• Chronic rejection is the main limiting factor for long-term survival of lung transplantation patients
Pathology
• The diagnosis of BOS is made clinically; pathological confirmation is not necessary for treatment. BO is patchy and often not seen on transbronchial biopsy. If clinically indicated, wedge lung biopsy may be done to diagnose BO
Histology
• Chronic airway rejection:
• BO characterized by the formation of polypoid or eccentric submucosal fibrosis resulting in partial or complete luminal obstruction
• Active BO: in addition to fibrosis, intrabronchiolar and/or peribronchiolar mononuclear infiltrates are present
• Inactive BO: characterized by the presence of dense fibrous scarring without mononuclear infiltrates
• Chronic vascular rejection:
• Fibrointimal thickening of arteries and veins
Immunopathology/special stains
• Trichrome stain helps highlight the fibrosis
Main differential diagnoses
• Multiple levels of transbronchial biopsy specimens need to be examined to exclude tangential cuts

Fig 1 Lung transplantation: chronic rejection. This example of active bronchiolitis obliterans shows an eccentric polypoid fibrosing lesion partially occluding an airway in addition to cellular mononuclear infiltrates. Note the unaffected bronchiole in lower right.
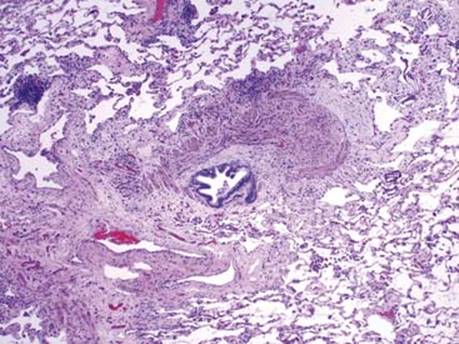
Fig 2 Lung transplantation: chronic rejection. This is an example of inactive bronchiolitis obliterans characterized by the presence of dense scarlike fibrous tissue in the bronchiolar submucosa without significant inflammation, causing subtotal occlusion of the lumen.
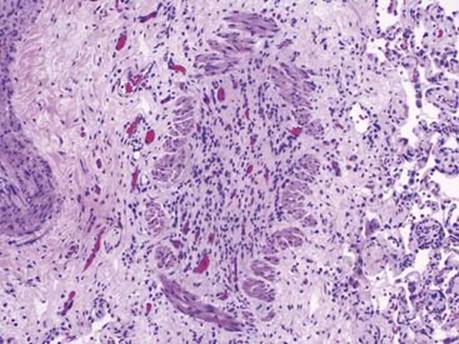
Fig 3 Lung transplantation: chronic rejection. This is an example of a completely obliterated bronchiolar lumen by granulation tissue and fibrosis in a patient who underwent retransplantation for bronchiolitis obliterans.
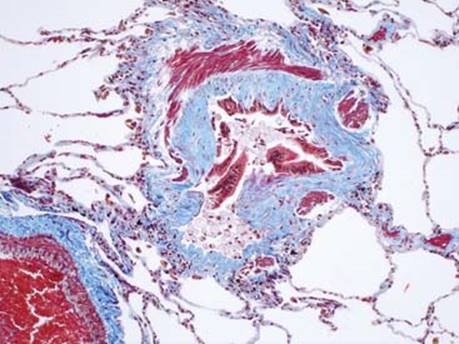
Fig 4 Lung transplantation: chronic rejection. A Masson trichrome special stain highlights submucosal fibrosis.

Fig 5 Lung transplantation: chronic rejection. Residual smooth muscle bundles can be very helpful in identifying obliteration of small airways as illustrated here.