Definition
• An intermediate-grade neuroendocrine carcinoma with focal necrosis and/or 2 to 10 mitoses per 10 high-power fields (hpf)
Clinical features
Epidemiology
• Accounts for 10% to 20% of pulmonary carcinoids
• Mean age at diagnosis, 55 years
• No causal association with smoking
Presentation
• Same as other carcinoids; more frequently peripheral; can also be central
• About 40% to 50% of cases have regional lymph node metastases and 10% have distant metastases at presentation
Prognosis and treatment
• Surgical resection with or without chemotherapy
• Worse prognosis compared with typical carcinoids; 5- and 10-year survival rates are approximately 65% and 45%, respectively
Pathology
Histology
• Criteria for diagnosis: focal necrosis, and/or 2 to 10 mitoses per 10 hpf
• Nuclear atypia and pleomorphism are not criteria for atypical carcinoid
Immunopathology/special stains
• Same as other carcinoids
• Usually show more reduced staining for neuroendocrine markers than typical carcinoids
Main differential diagnoses
• Typical carcinoid: 0 to 1 mitosis per 10 hpf and no necrosis
• Large-cell neuroendocrine carcinoma: >10 mitoses per 10 hpf; usually 60 mitoses per 10 hpf
• Metastatic low-grade neuroendocrine cell carcinoma

Fig 1 Atypical carcinoid. Atypical carcinoid with focal necrosis: A, low power; B, high power. Note “salt and pepper” chromatin in B.
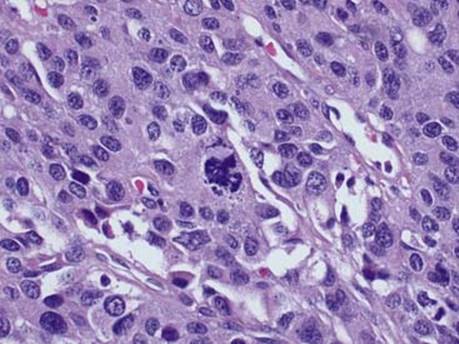
Fig 2 Atypical carcinoid. Atypical carcinoid with one abnormal mitotic figure in this field (center).


Fig 3 Atypical carcinoid. Atypical carcinoid with liver metastasis: A, H&E; B, keratin CAM5.2 (note both the hepatocytes and bile ducts are strongly immunoreactive); C, neuroendocrine marker synaptophysin; D, nuclear staining for TTF-1 (note the granular cytoplasmic staining of normal hepatocytes [lower left]); E, Ki-67 staining (mitotic index) of atypical carcinoid is low (approximately 5%).