Definition
• The most common primary lung lymphoma; however, overall a rare cause of primary lung malignancy
Clinical features
Epidemiology
• Most patients are older than 50 years; slight female predominance
• May be seen in younger patients, especially if immunosuppressed
Presentation
• Asymptomatic pulmonary nodule(s) incidentally found on chest radiographs
• May have dyspnea, coughing, hemoptysis, fever, sweats, weight loss, or autoimmune disorder
• Monoclonal gammopathy and/or bone marrow involvement may be present
Prognosis and treatment
• Treated with local radiation therapy
• Indolent course with long disease-free intervals; however, may recur
• Widespread disease does not appear to confer a worse prognosis
• Rarely transforms to diffuse large B-cell lymphoma
Pathology
Histology
• Nodular interstitial infiltrate of lymphoma cells along bronchovascular bundles and interlobular septae (lymphangitic pattern)
• Sheets of infiltrating lymphoma cells can obliterate underlying lung architecture
• Reactive B-cell follicles with germinal centers surrounded by monomorphic marginal zone B cells with scant cytoplasm, small slightly irregular or cleaved nuclei, and inconspicuous nucleoli resembling centrocytes or small lymphocytes
• Less often, marginal zone B cells may have moderate amounts of cytoplasm and resemble monocytoid B cells or may have eccentric nuclei and plasmacytic differentiation
• Larger transformed cells with prominent nucleoli resembling centroblasts, plasma cells with Dutcher bodies, and small lymphocytes are usually present in small numbers
• Lymphoepithelial lesions, characterized by epithelial infiltration by lymphoma cells, are common
• Lymphoma cell infiltration of bronchial cartilage, pleura, or blood vessel walls may be present, and cells may extend into and widen alveolar septae
• Lymphoma cells may colonize follicles
• Amyloid deposition may be present
Immunopathology/special stains
• Lymphoma cells are positive for CD20, CD79a, PAX5, bcl2, and IgM
• Lymphoma cells are negative for CD10, CD23, cyclin D1, and bcl6
• CD5 is negative in the majority of cases
• CD21 is positive in the lymphoma cells and also highlights expanded follicular dendritic cell networks
• Most cases are kappa or lambda light chain restricted
Main differential diagnoses
• Malignant lesions
• Follicular lymphoma: CD10 positive
• Mantle cell lymphoma: cyclin D1 and CD5 positive
• Small lymphocytic lymphoma: CD5 positive and bcl2 negative
• Benign lesions: no light chain restriction, no immunoglobulin heavy chain rearrangement
• Nodular lymphoid hyperplasia: usually localized
• Follicular bronchiolitis: lacks lymphangitic spreading pattern
• Lymphoid interstitial pneumonia: immunosuppressed patients
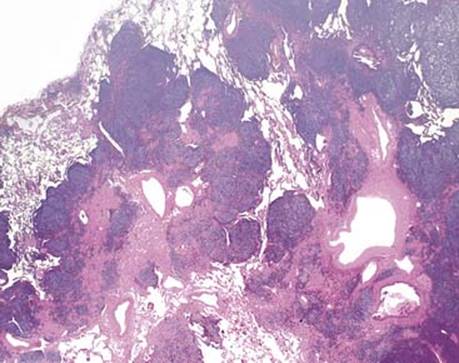
Fig 1 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. At low power, BALT lymphoma has a nodular and lymphangitic pattern.
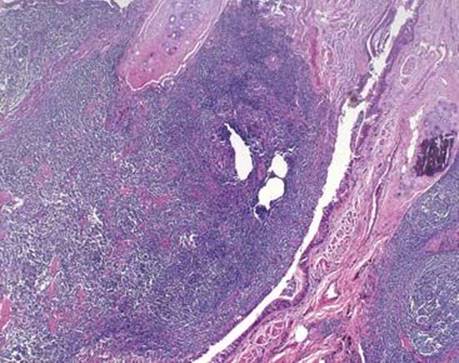
Fig 2 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. BALT lymphomas often invade beyond bronchial cartilage and infiltrate the airway epithelium.
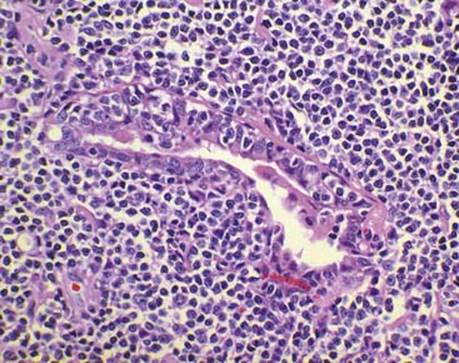
Fig 3 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. High magnification of a lymphoepithelial lesion involving a bronchiole.
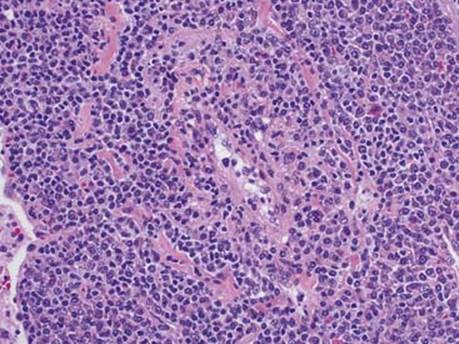
Fig 4 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. High magnification of BALT lymphoma cells invading a blood vessel wall.
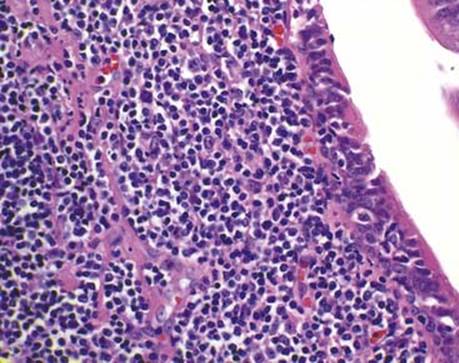
Fig 5 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. The characteristic small cleaved cells of BALT lymphoma can be appreciated in a diffuse sheet and infiltrating the bronchial epithelium. Occasional larger centroblast-like cells with prominent nucleoli are also present.
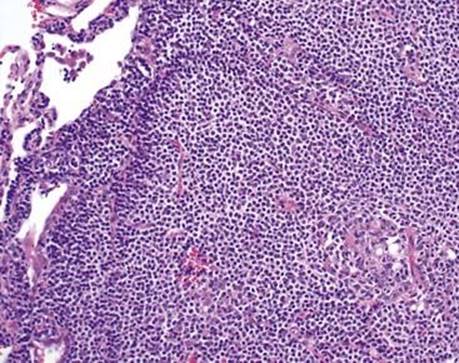
Fig 6 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. An atrophic germinal center (lower right) is surrounded by a monomorphic population of small cleaved BALT lymphoma cells, which extend into and widen adjacent alveolar septae.
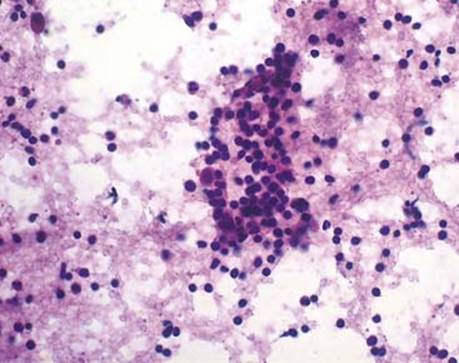
Fig 7 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. This touch preparation shows monotonous small lymphoma cells and rare larger cells with more abundant cytoplasm.

Fig 8 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. CD20 is strongly and diffusely positive in BALT lymphoma of the lung.
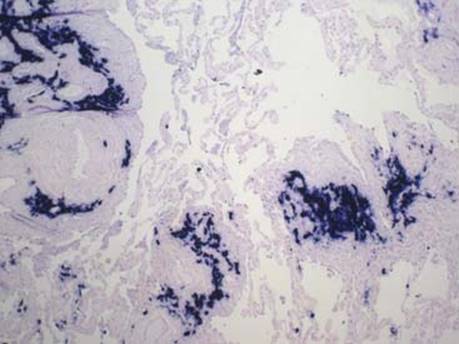
Fig 9 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. Kappa light chain restriction is demonstrated by in situ hybridization in this case of pulmonary BALT lymphoma.
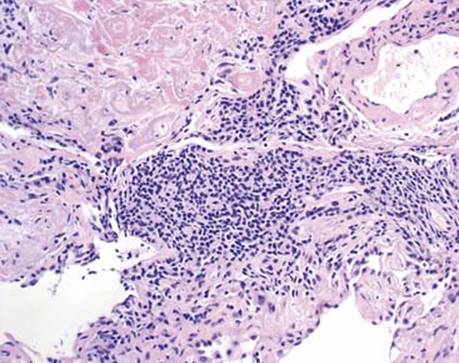
Fig 10 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. In this case of BALT lymphoma of the lung, amyloid deposition is seen with this H&E stain as homogeneous eosinophilic material with cracking artifact (upper left).
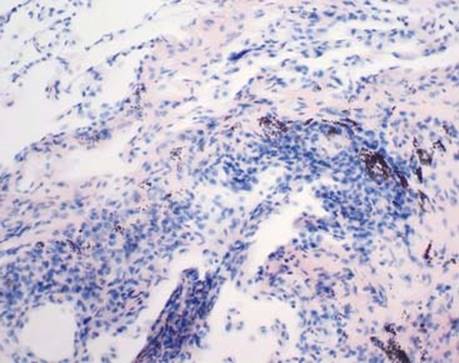
Fig 11 Extranodal marginal zone B-cell lymphoma of bronchial-associated lymphoid tissue. Amyloid deposition is highlighted by a Congo red stain.