Definition
• A malignant tumor of mesothelial cells arising from the visceral or parietal pleura
Clinical features
Epidemiology
• Usually age 50 to 70 years; male predominance
• Strong association with asbestos exposure but with long latent period (usually 30-40 years)
• Not associated with smoking (the combination of smoking and asbestos exposure greatly increases the risk of lung carcinoma only)
Presentation
• Patients usually present with recurrent pleural effusions, chest pain, or shortness of breath
• Chest X-ray film and CT scan show irregular thickening of pleura and interlobar fissures
• Usually diagnosed at advanced stage
Prognosis and treatment
• Treatment: surgical (extrapleural pneumonectomy or pleurectomy and decortication), not curative; radiation therapy and chemotherapy have not improved the survival time; radiation therapy has been shown to alleviate pain in the majority of patients treated; talc pleurodesis often done for palliation of pleural effusion
• Poor prognosis; most patients die within 1 year; few live more than 2 years; longer survival with epithelioid histological features
Pathology
Gross
• Diffuse growth of yellow tan tumor over parietal and visceral pleura including fissures
• As the tumor gets larger, it invades into lung, diaphragm, chest wall, and mediastinum
• Rarely, may be seen as a localized mass
Histology
• Three histological variants: epithelioid, sarcomatoid, and biphasic (see specific sections further on)
Immunopathology/special stains
• IHC and molecular tests (including FISH) that are useful on tissue specimens can be reliably applied to cytological material, especially cell blocks
• Positive for keratin AE1/AE3, CAM5.2, and CK7 and negative for CK20
• Mesothelial markers include calretinin, WT-1, CK5/6, and D2-40; all usually positive in epithelioid component; some or all may be negative in sarcomatoid component
• Electron microscopy: most useful for epithelioid malignant mesothelioma (MM); sarcomatoid MM typically does not show mesothelial features
• When immunohistochemical results are equivocal, formalin-fixed material retrieved from a paraffin block can be used for electron microscopic examination; combination of several features may be useful and include long, slender apical microvilli (length:diameter ratio, >10) with no glycocalyx (adenocarcinoma has short stubby microvilli with glycocalyx), perinuclear tonofilament bundles, the presence of basal lamina, and long desmosomes
• Typical pattern of cytogenetic defects, although not specific for mesothelioma; most are chromosomal deletions
• The most common genetic alteration is the homozygous deletion of the 9p21 locus resulting in loss of p16/CDKN2A gene; reported in up to 80% of pleural MM
• This deletion can be detected by FISH on formalin fixed, paraffin embedded tissue
Main differential diagnoses
• Depend on histological variant (see following specific sections)

Fig 1 Malignant mesothelioma of pleura. Chest CT image of an MM with irregular thickening of pleura on the left.

Fig 2 Malignant mesothelioma of pleura. Gross photograph of pneumonectomy specimen showing markedly thickened pleura.

Fig 3 Malignant mesothelioma of pleura. Cut surface of specimen in Fig 2 demonstrates tumor encasing the lung. Diaphragm is adherent, undersurface of which has been inked black.

Fig 4 Malignant mesothelioma of pleura. Gross photograph of fragmented pleurectomy specimen, including portions of ribs. At our institution, this is a more common procedure than pneumonectomy for MM.

Fig 5 Malignant mesothelioma of pleura. This relatively large pleurectomy specimen shows rib markings, tumor nodules, and intercostal muscle.
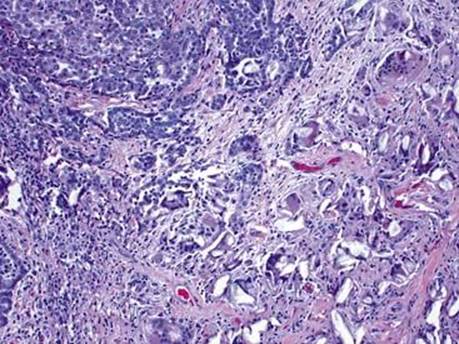
Fig 6 Malignant mesothelioma of pleura. Foreign body giant cell reaction due to prior talc pleurodesis in a patient with MM.
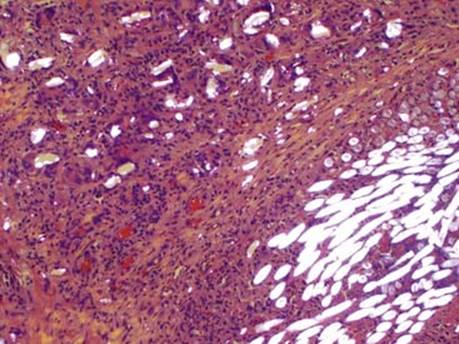
Fig 7 Malignant mesothelioma of pleura. Under polarized light, talc (top left) and suture (bottom right) are brightly birefringent.