Christian A. Tomaszewski
EPIDEMIOLOGY
![]() Chemicals are considered hazardous if they present a risk to health or physical safety.
Chemicals are considered hazardous if they present a risk to health or physical safety.
![]() Children have increased sensitivity to hazardous materials due to higher minute volumes and smaller airways that increase susceptibility to respiratory toxicity, and thinner skin and larger surface area, that increase dermal absorption.
Children have increased sensitivity to hazardous materials due to higher minute volumes and smaller airways that increase susceptibility to respiratory toxicity, and thinner skin and larger surface area, that increase dermal absorption.
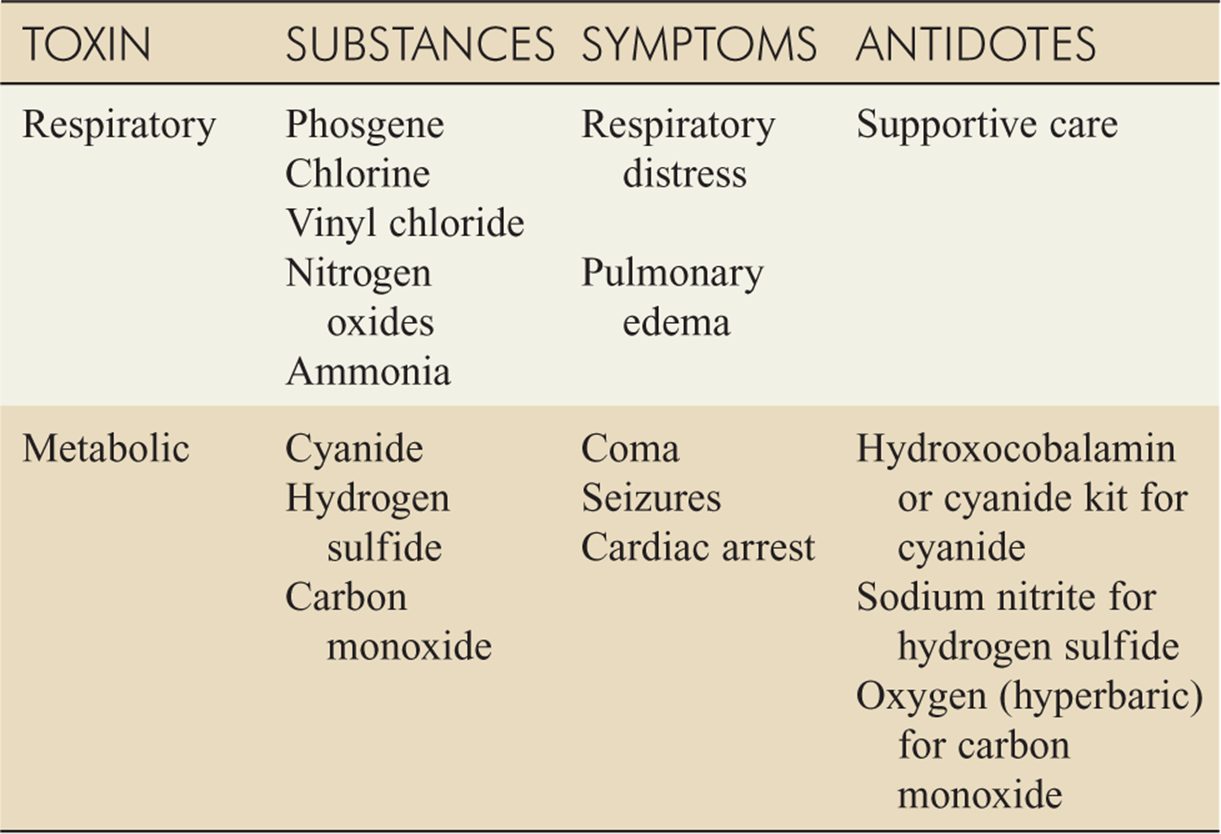
![]() Common industrial toxins that cause respiratory and metabolic toxicity are listed in Table 117-1.
Common industrial toxins that cause respiratory and metabolic toxicity are listed in Table 117-1.
TABLE 117-1 Common Signs and Symptoms of Exposure to Hazardous Chemicals
RESPIRATORY TOXINS
![]() Toxicity from airborne agents is affected by concentration, duration, and exposure in an enclosed space. Host factors such as metabolic rate, preexisting lung disease, and allergies are also important.
Toxicity from airborne agents is affected by concentration, duration, and exposure in an enclosed space. Host factors such as metabolic rate, preexisting lung disease, and allergies are also important.
![]() Treatment starts with removal of the victim from the source, delivery of 100% oxygen, and bronchodilators for bronchospasm.
Treatment starts with removal of the victim from the source, delivery of 100% oxygen, and bronchodilators for bronchospasm.
![]() Physical examination should focus on the presence of burns, singed nasal hairs, soot, hoarseness, cough, carbonaceous sputum, and respiratory difficulty.
Physical examination should focus on the presence of burns, singed nasal hairs, soot, hoarseness, cough, carbonaceous sputum, and respiratory difficulty.
![]() Antibiotics and steroids are usually not indicated in toxic inhalations, except possibly in nitrogen dioxide exposure or in patients with preexisting asthma and bronchospasm.
Antibiotics and steroids are usually not indicated in toxic inhalations, except possibly in nitrogen dioxide exposure or in patients with preexisting asthma and bronchospasm.
![]() Appropriate laboratory tests include carboxyhemoglobin, methemoglobin, lactate, ECG, and chest radiography.
Appropriate laboratory tests include carboxyhemoglobin, methemoglobin, lactate, ECG, and chest radiography.
PHOSGENE
![]() Phosgene is widely used in the production of plastics, dyes, polyurethane, and pesticides.
Phosgene is widely used in the production of plastics, dyes, polyurethane, and pesticides.
![]() Phosgene forms hydrochloric acid, causing lower airway burns with noncardiogenic pulmonary edema that can be delayed as much as 24 hours.
Phosgene forms hydrochloric acid, causing lower airway burns with noncardiogenic pulmonary edema that can be delayed as much as 24 hours.
![]() The main symptoms after inhalation are dyspnea and chest tightness.
The main symptoms after inhalation are dyspnea and chest tightness.
![]() Large exposures can cause mucous membrane irritation with pulmonary edema within 4 hours.
Large exposures can cause mucous membrane irritation with pulmonary edema within 4 hours.
![]() Care is supportive. A 24-hour observation period is recommended for asymptomatic patients with definite exposure. Recovery can be expected in 3 to 4 days.
Care is supportive. A 24-hour observation period is recommended for asymptomatic patients with definite exposure. Recovery can be expected in 3 to 4 days.
CHLORINE
![]() Chlorine is widely available and used in water treatment, paper manufacturing, and industrial lab work.
Chlorine is widely available and used in water treatment, paper manufacturing, and industrial lab work.
![]() Chlorine is a green-yellow gas with good warning properties because of its acrid, pungent odor. Because of its intermediate water solubility, it can cause both airway damage and pulmonary edema.
Chlorine is a green-yellow gas with good warning properties because of its acrid, pungent odor. Because of its intermediate water solubility, it can cause both airway damage and pulmonary edema.
![]() Chlorine gas forms hydrochloric and hypochlorous acids and oxidants on contact with moist membranes.
Chlorine gas forms hydrochloric and hypochlorous acids and oxidants on contact with moist membranes.
![]() Early eye and upper airway irritation accompany mild exposures.
Early eye and upper airway irritation accompany mild exposures.
![]() Severe exposures cause coughing, hoarseness, and pulmonary edema, usually within 6 hours.
Severe exposures cause coughing, hoarseness, and pulmonary edema, usually within 6 hours.
![]() Provide supportive care with humidified oxygen and bronchodilators as needed.
Provide supportive care with humidified oxygen and bronchodilators as needed.
![]() The use of nebulized sodium bicarbonate and steroids is controversial.
The use of nebulized sodium bicarbonate and steroids is controversial.
NITROGEN OXIDES
![]() Nitrogen dioxide and other nitrogen oxides are found in silo gas (“silo filler disease”), combustion, blast weapons, obscurants, and certain industrial processes.
Nitrogen dioxide and other nitrogen oxides are found in silo gas (“silo filler disease”), combustion, blast weapons, obscurants, and certain industrial processes.
![]() Oxides of nitrogen have low water solubility leading primarily to lower airway toxicity.
Oxides of nitrogen have low water solubility leading primarily to lower airway toxicity.
![]() Nitrogen dioxide is slowly converted to nitric acid in the alveoli.
Nitrogen dioxide is slowly converted to nitric acid in the alveoli.
![]() A triphasic response to toxicity starts with mild discomfort even with high concentrations, accompanied by dyspnea and flu-like symptoms.
A triphasic response to toxicity starts with mild discomfort even with high concentrations, accompanied by dyspnea and flu-like symptoms.
![]() Patients then have mild improvement or persistent symptoms.
Patients then have mild improvement or persistent symptoms.
![]() Finally, 24 to 72 hours later, there may be worsening dyspnea due to ensuing pulmonary edema.
Finally, 24 to 72 hours later, there may be worsening dyspnea due to ensuing pulmonary edema.
![]() Methemoglobinemia may occur after nitrogen oxide exposure.
Methemoglobinemia may occur after nitrogen oxide exposure.
![]() Although unproven, early corticosteroids have been used for acute lung injury.
Although unproven, early corticosteroids have been used for acute lung injury.
AMMONIA
![]() Ammonia is a common component of various chemicals and fertilizers, as used in the production of plastics.
Ammonia is a common component of various chemicals and fertilizers, as used in the production of plastics.
![]() It is highly water-soluble, forming ammonium hydroxide on contact with wet surfaces.
It is highly water-soluble, forming ammonium hydroxide on contact with wet surfaces.
![]() Immediate symptoms include mucous membrane, eye, and throat irritation.
Immediate symptoms include mucous membrane, eye, and throat irritation.
![]() Massive exposures, especially in enclosed spaces, can lead to lower airway irritation with bronchospasm and pulmonary edema.
Massive exposures, especially in enclosed spaces, can lead to lower airway irritation with bronchospasm and pulmonary edema.
![]() Supportive care with humidified oxygen and bronchodilators is the main treatment.
Supportive care with humidified oxygen and bronchodilators is the main treatment.
![]() Eye exposures to concentrated ammonia require aggressive ocular irrigation and evaluation for corneal burns.
Eye exposures to concentrated ammonia require aggressive ocular irrigation and evaluation for corneal burns.
METABOLIC TOXINS
HYDROGEN SULFIDE
![]() Hydrogen sulfide is a colorless gas found in petroleum industry and sites of organic decomposition, such as sewers and manure pits.
Hydrogen sulfide is a colorless gas found in petroleum industry and sites of organic decomposition, such as sewers and manure pits.
![]() It is the most common cause of fatal gas inhalational exposure.
It is the most common cause of fatal gas inhalational exposure.
![]() Hydrogen sulfide inhibits cytochrome oxidase a3, uncoupling oxidative phosphorylation, which causes lactic acidosis from cellular asphyxia.
Hydrogen sulfide inhibits cytochrome oxidase a3, uncoupling oxidative phosphorylation, which causes lactic acidosis from cellular asphyxia.
![]() High concentrations or prolonged exposure blunts the ability to detect the characteristic rotten egg odor.
High concentrations or prolonged exposure blunts the ability to detect the characteristic rotten egg odor.
![]() Respiratory and ocular irritation is common after exposure.
Respiratory and ocular irritation is common after exposure.
![]() High concentrations can lead to syncope, seizures, and death within a few breaths.
High concentrations can lead to syncope, seizures, and death within a few breaths.
![]() Delayed pulmonary edema and corneal ulceration can occur after massive exposure.
Delayed pulmonary edema and corneal ulceration can occur after massive exposure.
![]() Treatment is primarily supportive and includes prompt removal from the scene, dermal and ocular decontamination, and administration of 100% oxygen.
Treatment is primarily supportive and includes prompt removal from the scene, dermal and ocular decontamination, and administration of 100% oxygen.
![]() Consider administration of the nitrite component of the cyanide antidote kit (see below) withholding the thiosulfate portion.
Consider administration of the nitrite component of the cyanide antidote kit (see below) withholding the thiosulfate portion.
CYANIDE
![]() Cyanide is found in chemical laboratories and in industry, particularly plastics, electroplating, mining, precious metal reclamation, and hide preparation. It is also used as a rodenticide, fumigant, and fertilizer.
Cyanide is found in chemical laboratories and in industry, particularly plastics, electroplating, mining, precious metal reclamation, and hide preparation. It is also used as a rodenticide, fumigant, and fertilizer.
![]() The burning of wool, synthetic fabrics, and certain plastics can result in liberation of hydrogen cyanide.
The burning of wool, synthetic fabrics, and certain plastics can result in liberation of hydrogen cyanide.
![]() Cyanide avidly binds to cytochrome a3, shutting down oxidative phosphorylation for cellular respiration; therefore, tissues like the brain and heart with high oxygen consumption are the most affected.
Cyanide avidly binds to cytochrome a3, shutting down oxidative phosphorylation for cellular respiration; therefore, tissues like the brain and heart with high oxygen consumption are the most affected.
![]() Chronic low dose exposure to cyanogens can occur from foods and inhalation of cigarette smoke. Detoxification in these cases occurs naturally through enzymatic transformation of thiocyanate by rhodanese.
Chronic low dose exposure to cyanogens can occur from foods and inhalation of cigarette smoke. Detoxification in these cases occurs naturally through enzymatic transformation of thiocyanate by rhodanese.
![]() Inhalational exposure to hydrogen cyanide gas causes immediate symptoms. At concentrations less than 50 ppm, patients may experience anxiety, dyspnea, palpitations, and headache. Higher concentrations can cause severe dyspnea, syncope, seizures, and dysrhythmias. Continued exposure or higher concentrations can cause coma, cardiovascular collapse, and death.
Inhalational exposure to hydrogen cyanide gas causes immediate symptoms. At concentrations less than 50 ppm, patients may experience anxiety, dyspnea, palpitations, and headache. Higher concentrations can cause severe dyspnea, syncope, seizures, and dysrhythmias. Continued exposure or higher concentrations can cause coma, cardiovascular collapse, and death.
![]() Ingestion of cyanide usually leads to symptoms within minutes.
Ingestion of cyanide usually leads to symptoms within minutes.
![]() Signs and symptoms of acute cyanide toxicity are listed in Table 117-2.
Signs and symptoms of acute cyanide toxicity are listed in Table 117-2.
![]() Delayed cyanide toxicity may be seen after ingestion of acetonitrile, a cosmetic nail polish remover, and amygdalin from apricot pits. Prolonged infusions of sodium nitroprusside can also lead to mild cyanide toxicity.
Delayed cyanide toxicity may be seen after ingestion of acetonitrile, a cosmetic nail polish remover, and amygdalin from apricot pits. Prolonged infusions of sodium nitroprusside can also lead to mild cyanide toxicity.
![]() The diagnosis of cyanide poisoning is primarily clinical.
The diagnosis of cyanide poisoning is primarily clinical.
![]() The odor of bitter almonds supports the diagnosis of cyanide toxicity, but only 60% to 80% of the populations can smell this.
The odor of bitter almonds supports the diagnosis of cyanide toxicity, but only 60% to 80% of the populations can smell this.
![]() Table 117-3 lists the laboratory findings in cyanide poisoning. The hallmark is an unexplained metabolic acidosis and plasma lactate levels >10 mmol/L are predictive of toxic cyanide levels.
Table 117-3 lists the laboratory findings in cyanide poisoning. The hallmark is an unexplained metabolic acidosis and plasma lactate levels >10 mmol/L are predictive of toxic cyanide levels.
![]() Treatment of cyanide toxicity should not wait for whole blood cyanide levels, but should be administered promptly and empirically when exposure is suspected and signs and symptoms present.
Treatment of cyanide toxicity should not wait for whole blood cyanide levels, but should be administered promptly and empirically when exposure is suspected and signs and symptoms present.
![]() Initially, treatment should focus on aggressive supportive care: provide 100% oxygen to all patients and support the airway and breathing.
Initially, treatment should focus on aggressive supportive care: provide 100% oxygen to all patients and support the airway and breathing.
![]() Treat hypotension with crystalloids and pressors.
Treat hypotension with crystalloids and pressors.
![]() Consider sodium bicarbonate in severe acidosis, which may enhance efficacy of cyanide antidotes.
Consider sodium bicarbonate in severe acidosis, which may enhance efficacy of cyanide antidotes.
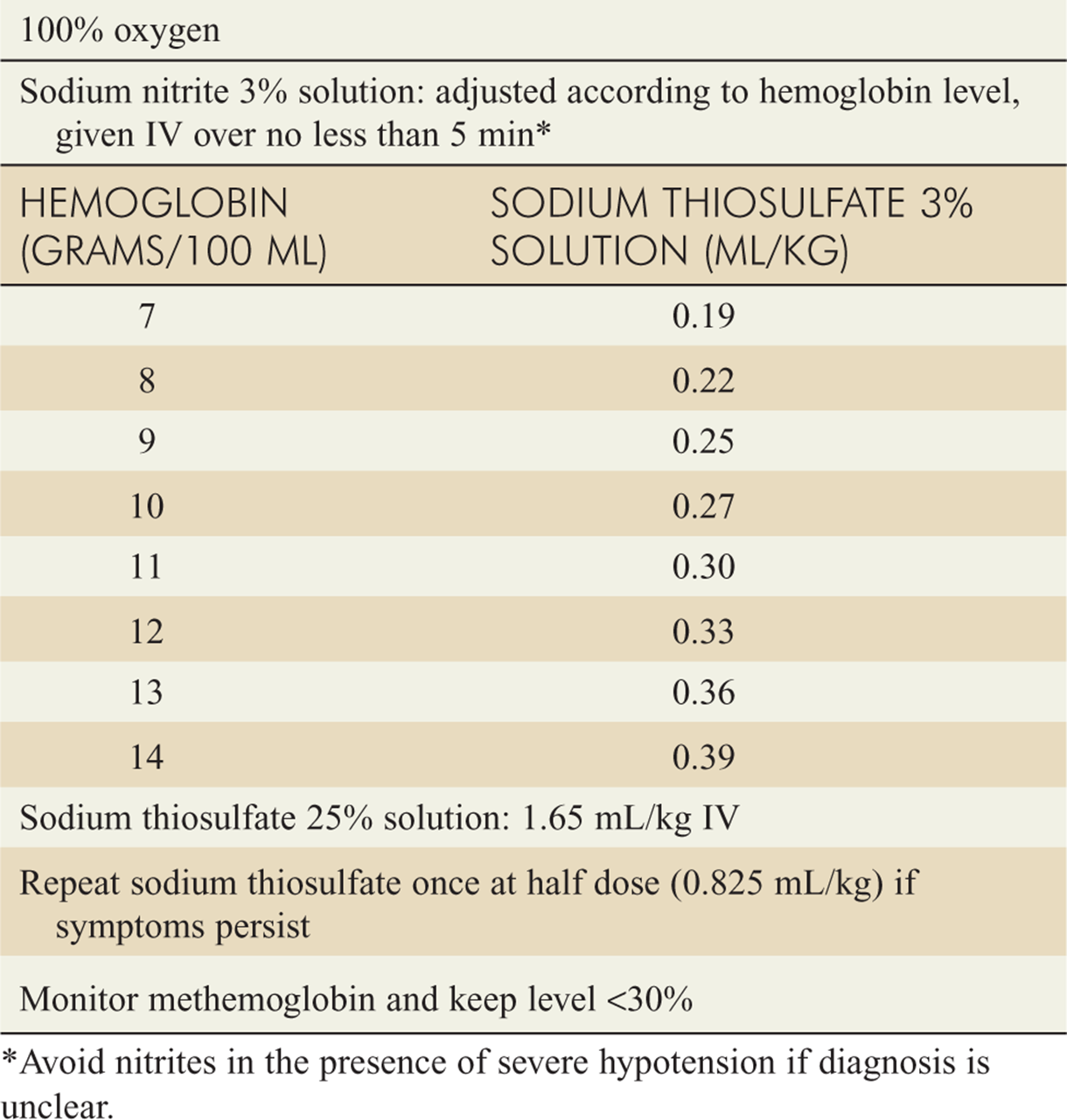
![]() Table 117-4 lists the specific antidotal treatment for cyanide poisoning in the adult, and Table 117-5 lists the hemoglobin-based dosing of sodium nitrite recommended for children.
Table 117-4 lists the specific antidotal treatment for cyanide poisoning in the adult, and Table 117-5 lists the hemoglobin-based dosing of sodium nitrite recommended for children.
![]() Amyl nitrite can be administered via inhalation when vascular access is not immediately obtained.
Amyl nitrite can be administered via inhalation when vascular access is not immediately obtained.
![]() The FDA has approved a new antidote for cyanide, hydroxocobalamin (vitamin B12A). Due to its low toxicity, it is ideal for questionable cases and smoke inhalation victims where methemoglobin formation from nitrite therapy may be detrimental. Administer 2 vials, each 2.5 grams reconstituted in 100 mL NS, over 7.5 minutes, for a total dose of 5 grams in 200 mL NS over 15 minutes. Although not approved for pediatric use, a dose of 70 milligrams/kg has been suggested. Side effects include red discoloration of the skin and urine, transient hypertension, and rarely, anaphylactoid reactions.
The FDA has approved a new antidote for cyanide, hydroxocobalamin (vitamin B12A). Due to its low toxicity, it is ideal for questionable cases and smoke inhalation victims where methemoglobin formation from nitrite therapy may be detrimental. Administer 2 vials, each 2.5 grams reconstituted in 100 mL NS, over 7.5 minutes, for a total dose of 5 grams in 200 mL NS over 15 minutes. Although not approved for pediatric use, a dose of 70 milligrams/kg has been suggested. Side effects include red discoloration of the skin and urine, transient hypertension, and rarely, anaphylactoid reactions.
![]() Hyperbaric oxygen is recommended only for cyanide-poisoned patients with concomitant carbon monoxide poisoning.
Hyperbaric oxygen is recommended only for cyanide-poisoned patients with concomitant carbon monoxide poisoning.
![]() Observe patients with mild to moderate symptoms from cyanide exposure prior to initiating treatment.
Observe patients with mild to moderate symptoms from cyanide exposure prior to initiating treatment.
![]() Treat severely ill patients with altered mental status and bradycardia or hypotension immediately if cyanide is suspected. Hypotension is not a contraindication for nitrite therapy, but one may want to substitute hydroxocobalamin, especially for smoke inhalation cases with high carboxyhemoglobin levels.
Treat severely ill patients with altered mental status and bradycardia or hypotension immediately if cyanide is suspected. Hypotension is not a contraindication for nitrite therapy, but one may want to substitute hydroxocobalamin, especially for smoke inhalation cases with high carboxyhemoglobin levels.
TABLE 117-2 Signs and Symptoms of Acute Cyanide Toxicity
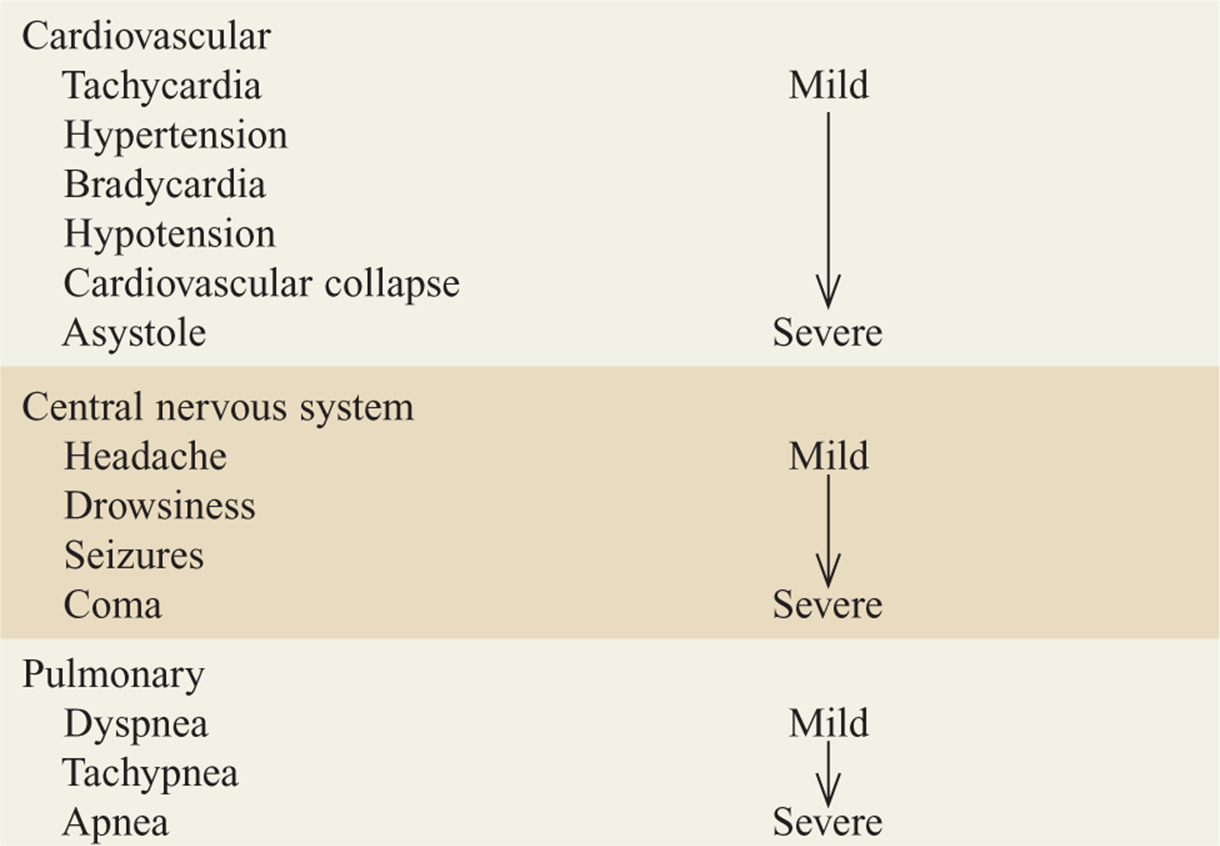
TABLE 117-3 Anticipated Laboratory Findings in Cyanide Poisoning
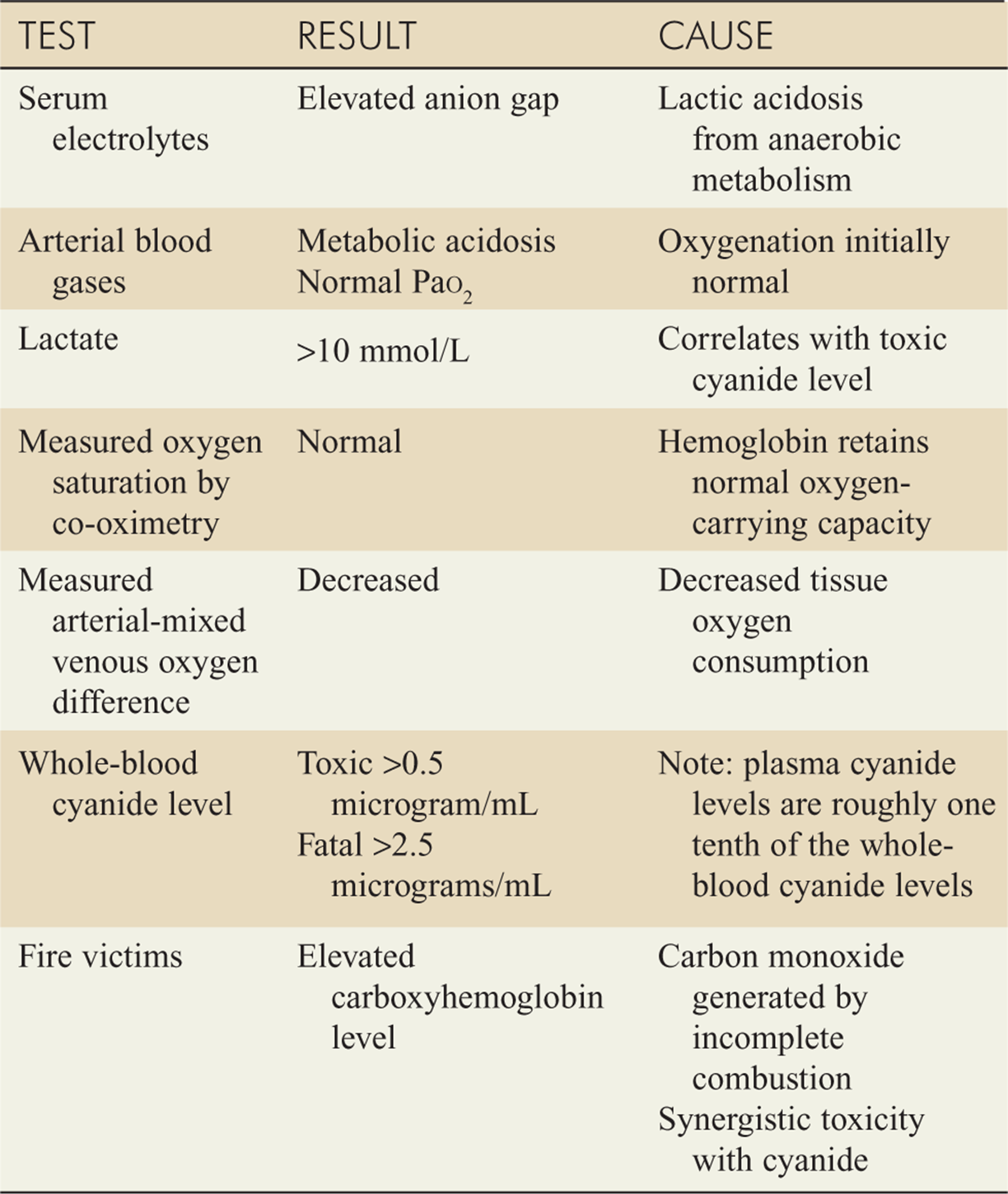
TABLE 117-4 Treatment of Cyanide Poisoning in Adults
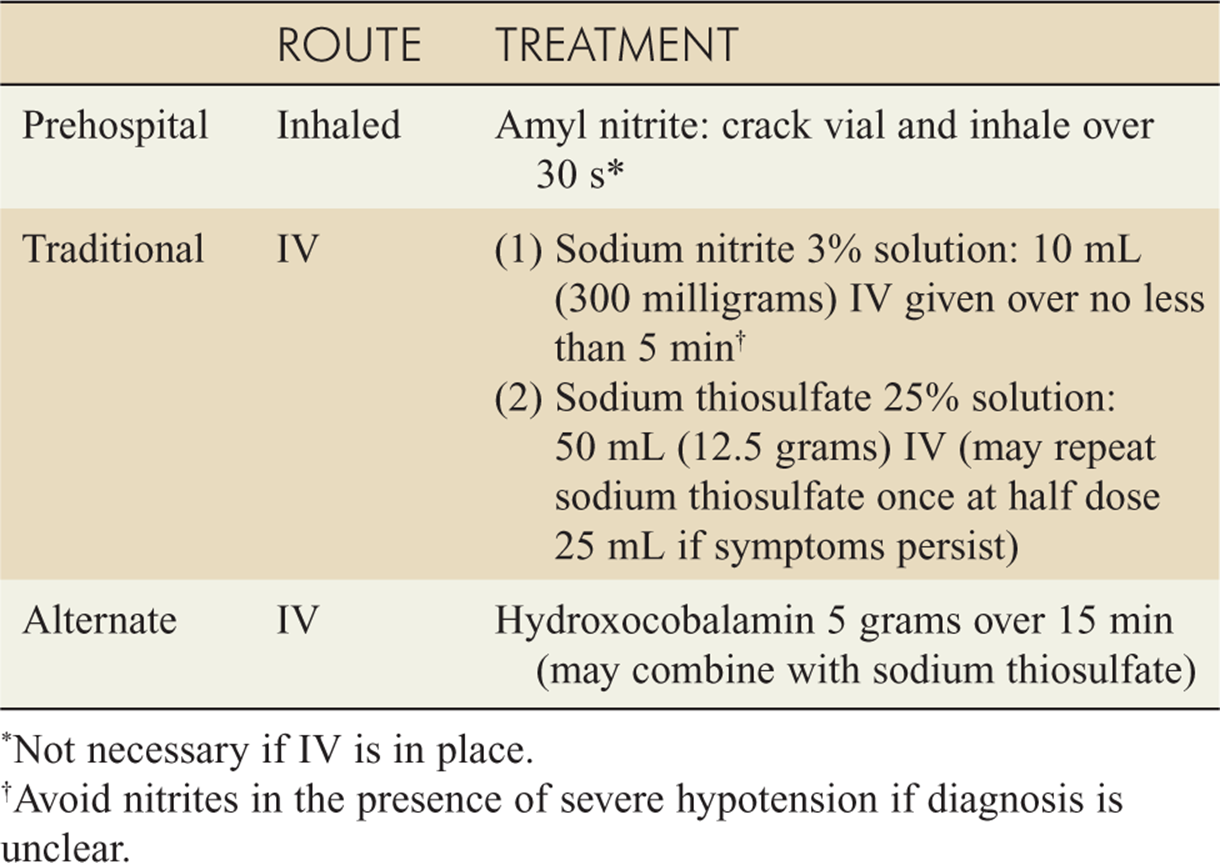
TABLE 117-5 Treatment of Cyanide Poisoning in Children
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 198, “Industrial Toxins,” by Chip Gresham and Frank LoVecchio.