C. Crawford Mechem
DELIRIUM
EPIDEMIOLOGY
![]() One quarter of ED patients aged 70 years or older have impaired mental status or delirium.
One quarter of ED patients aged 70 years or older have impaired mental status or delirium.
![]() On admission, 10% to 25% of elderly patients have delirium.
On admission, 10% to 25% of elderly patients have delirium.
PATHOPHYSIOLOGY
![]() Pathologic mechanisms producing delirium are thought to involve widespread neuronal or neurotransmitter dysfunction.
Pathologic mechanisms producing delirium are thought to involve widespread neuronal or neurotransmitter dysfunction.
![]() The four general causes are primary intracranial disease, systemic diseases secondarily affecting the central nervous system (CNS), exogenous toxins, and drug withdrawal.
The four general causes are primary intracranial disease, systemic diseases secondarily affecting the central nervous system (CNS), exogenous toxins, and drug withdrawal.
CLINICAL FEATURES
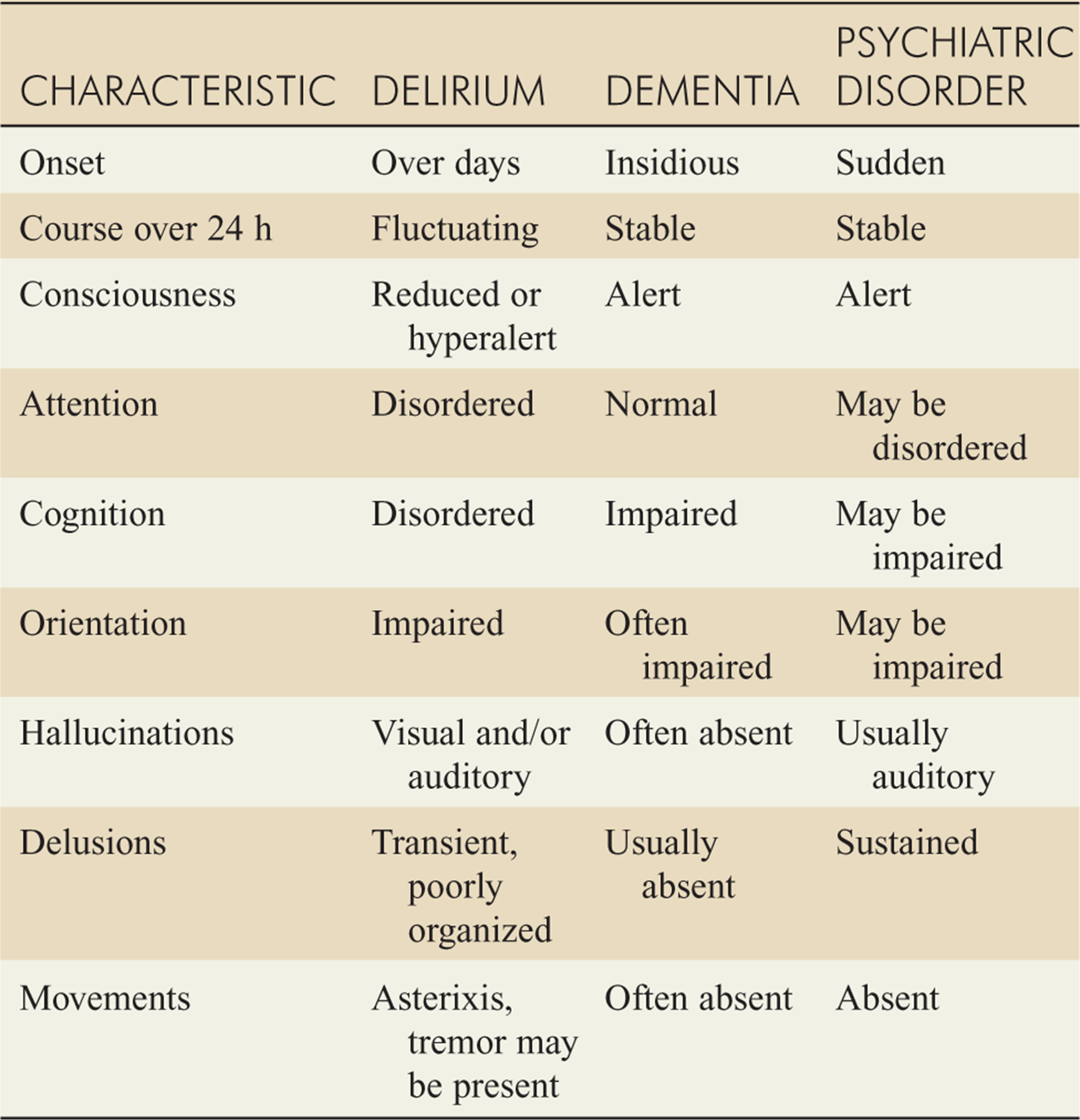
![]() Delirium generally develops over days, with fluctuating symptoms (Table 144-1).
Delirium generally develops over days, with fluctuating symptoms (Table 144-1).
TABLE 144-1 Features of Delirium, Dementia, and Psychiatric Disorder
![]() Attention, perception, thinking, and memory are altered.
Attention, perception, thinking, and memory are altered.
![]() Alertness is reduced, manifested by difficulty maintaining attention and concentration.
Alertness is reduced, manifested by difficulty maintaining attention and concentration.
![]() The patient may fluctuate rapidly between hypoactive and hyperactive states.
The patient may fluctuate rapidly between hypoactive and hyperactive states.
![]() The sleep-wake cycle may be disrupted, with somnolence by day and agitation at night.
The sleep-wake cycle may be disrupted, with somnolence by day and agitation at night.
![]() Tremor, asterixis, tachycardia, sweating, hypertension, and emotional outbursts may be present.
Tremor, asterixis, tachycardia, sweating, hypertension, and emotional outbursts may be present.
![]() Hallucinations tend to be visual, although auditory hallucinations can also occur.
Hallucinations tend to be visual, although auditory hallucinations can also occur.
DIAGNOSIS AND DIFFERENTIAL
![]() Both historical and physical examination findings are needed to confirm the diagnosis.
Both historical and physical examination findings are needed to confirm the diagnosis.
![]() The acute onset of attention deficits and cognitive abnormalities fluctuating in severity throughout the day and worsening at night (“sundowning”) is virtually diagnostic.
The acute onset of attention deficits and cognitive abnormalities fluctuating in severity throughout the day and worsening at night (“sundowning”) is virtually diagnostic.
![]() Diagnostic testing is directed at identifying an underlying process and should include serum electrolytes, hepatic and renal studies, urinalysis, CBC, and a chest radiograph.
Diagnostic testing is directed at identifying an underlying process and should include serum electrolytes, hepatic and renal studies, urinalysis, CBC, and a chest radiograph.
![]() A head CT scan should be performed if a mass lesion is suspected, followed by lumbar puncture if meningitis or subarachnoid hemorrhage is a consideration.
A head CT scan should be performed if a mass lesion is suspected, followed by lumbar puncture if meningitis or subarachnoid hemorrhage is a consideration.
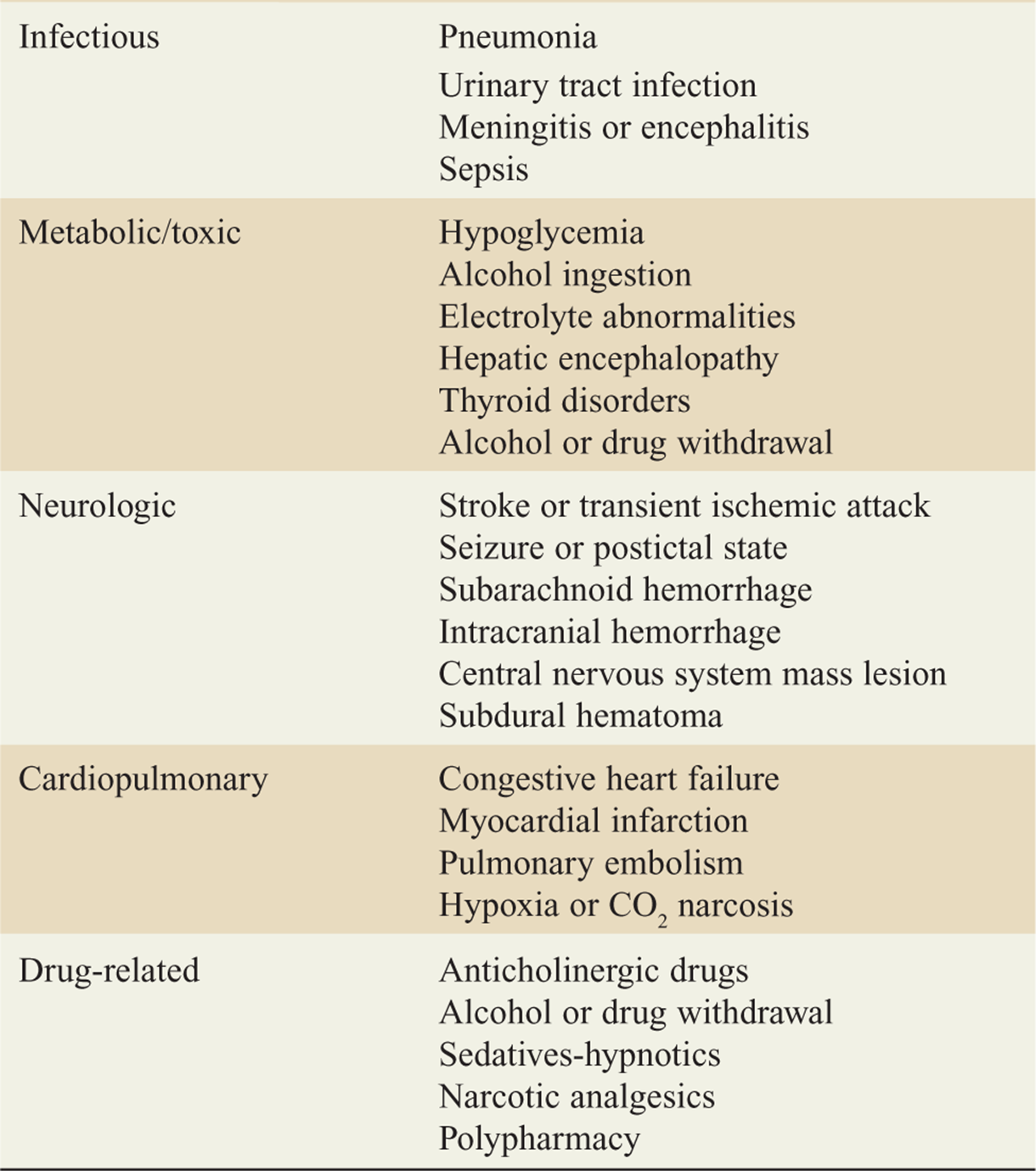
![]() The differential diagnosis of delirium in the elderly is listed in Table 144-2.
The differential diagnosis of delirium in the elderly is listed in Table 144-2.
TABLE 144-2 Important Medical Causes of Delirium in Elderly Patients
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treatment is directed at the underlying cause.
Treatment is directed at the underlying cause.
![]() Sedation is often necessary to relieve agitation. Haloperidol, 5 to 10 milligrams PO, IV, or IM, is a frequent first choice. The dose should be reduced to 1 to 2 milligrams in the elderly.
Sedation is often necessary to relieve agitation. Haloperidol, 5 to 10 milligrams PO, IV, or IM, is a frequent first choice. The dose should be reduced to 1 to 2 milligrams in the elderly.
![]() Lorazepam, 0.5 to 2 milligrams PO, IV, or IM, may be used in conjunction with haloperidol, with the dose dictated by the patient’s age and weight.
Lorazepam, 0.5 to 2 milligrams PO, IV, or IM, may be used in conjunction with haloperidol, with the dose dictated by the patient’s age and weight.
![]() Unless a readily reversible cause is identified and corrected and there is a return to baseline, most patients should be admitted for further evaluation and treatment.
Unless a readily reversible cause is identified and corrected and there is a return to baseline, most patients should be admitted for further evaluation and treatment.
DEMENTIA
PATHOPHYSIOLOGY
![]() Most cases in the United States are due to Alzheimer’s disease. The pathophysiology involves a reduction in neurons in the cerebral cortex, increased amyloid deposition, and the production of neurofibrillary tangles and plaques.
Most cases in the United States are due to Alzheimer’s disease. The pathophysiology involves a reduction in neurons in the cerebral cortex, increased amyloid deposition, and the production of neurofibrillary tangles and plaques.
![]() Vascular dementia accounts for the next largest number of cases and is a cerebrovascular disease with multiple infarctions.
Vascular dementia accounts for the next largest number of cases and is a cerebrovascular disease with multiple infarctions.
CLINICAL FEATURES
![]() Impairment of memory, particularly recent memory, is gradual and progressive. Remote memories are often preserved. Alzheimer’s disease is often associated with memory impairment and disorientation with preservation of motor and speech abilities.
Impairment of memory, particularly recent memory, is gradual and progressive. Remote memories are often preserved. Alzheimer’s disease is often associated with memory impairment and disorientation with preservation of motor and speech abilities.
![]() Symptoms are progressive and include problems naming objects, forgetting items, trouble reading, decreased performance in social situations, disorientation, difficulty with self-care tasks, personality changes, depression, anxiety, and speech difficulties.
Symptoms are progressive and include problems naming objects, forgetting items, trouble reading, decreased performance in social situations, disorientation, difficulty with self-care tasks, personality changes, depression, anxiety, and speech difficulties.
![]() Patients with vascular dementia often show similar symptoms, but may also have abnormalities of deep tendon reflexes, gait abnormalities, or weakness of an extremity.
Patients with vascular dementia often show similar symptoms, but may also have abnormalities of deep tendon reflexes, gait abnormalities, or weakness of an extremity.
DIAGNOSIS AND DIFFERENTIAL
![]() The history of memory problems in Alzheimer’s disease is usually one of slow onset and progression. If specific dates of worsening are noted, the possibility of vascular dementia increases.
The history of memory problems in Alzheimer’s disease is usually one of slow onset and progression. If specific dates of worsening are noted, the possibility of vascular dementia increases.
![]() Physical examination may be helpful in identifying associated causes and should include a detailed mental status examination.
Physical examination may be helpful in identifying associated causes and should include a detailed mental status examination.
![]() Diagnostic testing may include a CBC, metabolic profile, urinalysis, thyroid function tests, serum vitamin B12 level, and serologic testing for syphilis in patients at risk. Other tests may include an ESR, serum folate level, HIV testing, and chest radiograph.
Diagnostic testing may include a CBC, metabolic profile, urinalysis, thyroid function tests, serum vitamin B12 level, and serologic testing for syphilis in patients at risk. Other tests may include an ESR, serum folate level, HIV testing, and chest radiograph.
![]() Cranial CT or MRI should be considered at some point in the diagnostic evaluation.
Cranial CT or MRI should be considered at some point in the diagnostic evaluation.
![]() A lumbar puncture should be performed if the diagnosis is not readily apparent.
A lumbar puncture should be performed if the diagnosis is not readily apparent.
![]() The differential includes delirium, depression, infection, inflammatory processes, malignancy, toxins, trauma, metabolic disturbances, and normal-pressure hydrocephalus. Normal-pressure hydrocephalus should be considered in the setting of urinary incontinence and gait disturbance. Head CT will reveal excessively large ventricles.
The differential includes delirium, depression, infection, inflammatory processes, malignancy, toxins, trauma, metabolic disturbances, and normal-pressure hydrocephalus. Normal-pressure hydrocephalus should be considered in the setting of urinary incontinence and gait disturbance. Head CT will reveal excessively large ventricles.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() All types of dementia may be amenable to environmental or psychosocial interventions.
All types of dementia may be amenable to environmental or psychosocial interventions.
![]() Due to adverse effects, antipsychotic drugs should be reserved for patients with persistent psychotic features or those with extreme disruptive or dangerous behaviors.
Due to adverse effects, antipsychotic drugs should be reserved for patients with persistent psychotic features or those with extreme disruptive or dangerous behaviors.
![]() Treatment of vascular dementia is directed at risk factors, including hypertension.
Treatment of vascular dementia is directed at risk factors, including hypertension.
![]() If normal-pressure hydrocephalus is suspected, a trial of lumbar puncture with cerebrospinal fluid (CSF) drainage may be considered.
If normal-pressure hydrocephalus is suspected, a trial of lumbar puncture with cerebrospinal fluid (CSF) drainage may be considered.
![]() Most patients with a new diagnosis of dementia will require admission for further evaluation and management. However, patients with long-standing symptoms, consistent caregivers, and reliable follow-up may be discharged for outpatient evaluation after life-threatening conditions have been excluded.
Most patients with a new diagnosis of dementia will require admission for further evaluation and management. However, patients with long-standing symptoms, consistent caregivers, and reliable follow-up may be discharged for outpatient evaluation after life-threatening conditions have been excluded.
COMA
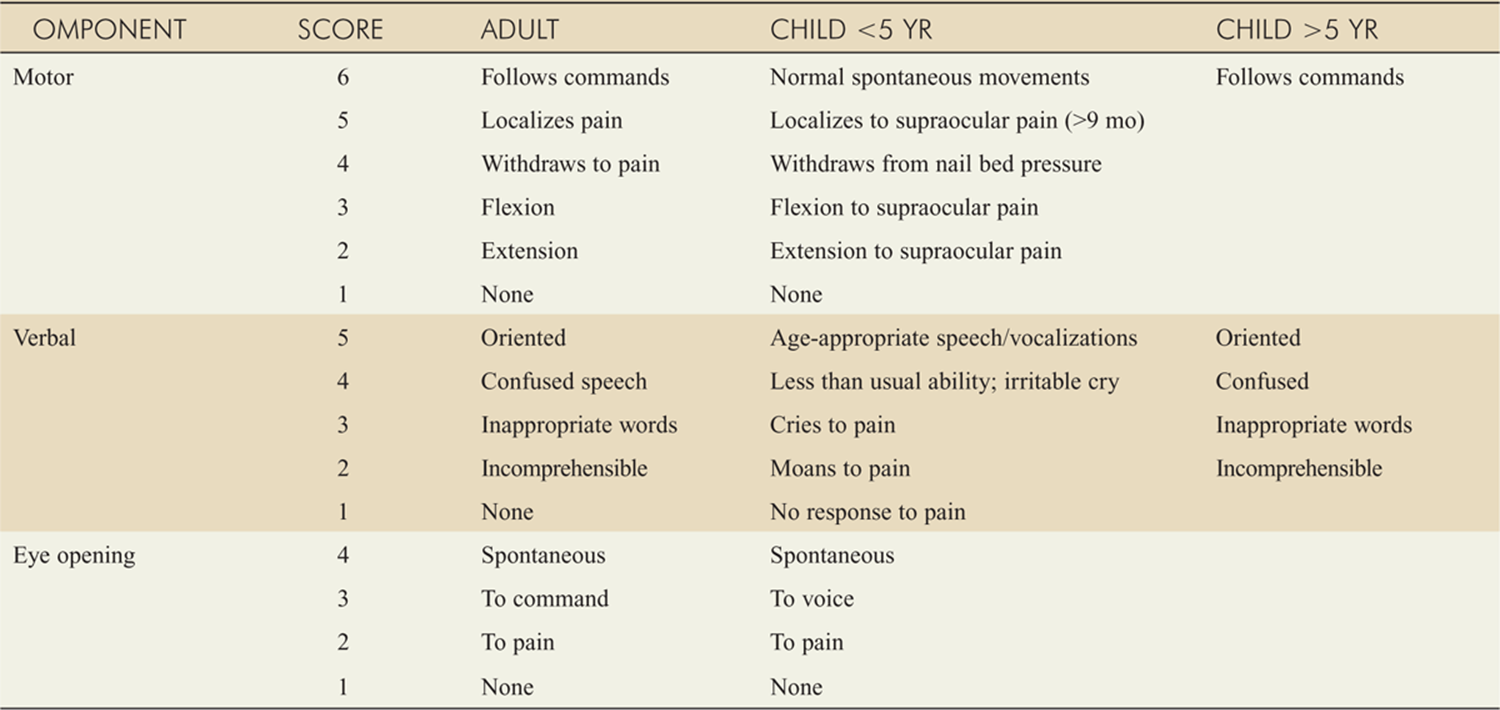
![]() Coma is a state of reduced alertness and responsiveness from which the patient cannot be aroused. The Glasgow Coma Scale is widely used as a scoring system in patients with altered mental status (Table 144-3).
Coma is a state of reduced alertness and responsiveness from which the patient cannot be aroused. The Glasgow Coma Scale is widely used as a scoring system in patients with altered mental status (Table 144-3).
TABLE 144-3 Glasgow Coma Scale
PATHOPHYSIOLOGY
![]() Coma may be due to a systemic disease that affects the CNS secondarily or a primary CNS process. Both cerebral hemispheres or the brain stem must be involved.
Coma may be due to a systemic disease that affects the CNS secondarily or a primary CNS process. Both cerebral hemispheres or the brain stem must be involved.
![]() Examples of systemic disease secondarily resulting in coma are hypoxia and hypoglycemia, in which substrates needed for neuronal function are lacking.
Examples of systemic disease secondarily resulting in coma are hypoxia and hypoglycemia, in which substrates needed for neuronal function are lacking.
![]() In primary CNS causes, coma may result from bilateral cortical dysfunction, localized brain stem pathology, or elevated intracranial pressure with decreased cerebral perfusion.
In primary CNS causes, coma may result from bilateral cortical dysfunction, localized brain stem pathology, or elevated intracranial pressure with decreased cerebral perfusion.
![]() Brain stem disorders include hemorrhage and herniation syndromes.
Brain stem disorders include hemorrhage and herniation syndromes.
![]() Uncal herniation results from an expanding mass that causes the medial temporal lobe to shift and compress the brain stem. The ipsilateral pupil will be fixed and dilated. Hemiparesis ipsilateral to the mass may develop from compression of descending motor tracts in the opposite cerebral peduncle.
Uncal herniation results from an expanding mass that causes the medial temporal lobe to shift and compress the brain stem. The ipsilateral pupil will be fixed and dilated. Hemiparesis ipsilateral to the mass may develop from compression of descending motor tracts in the opposite cerebral peduncle.
![]() Central herniation syndrome is characterized by progressive loss of consciousness, loss of brain stem reflexes, decorticate posturing, and irregular respirations.
Central herniation syndrome is characterized by progressive loss of consciousness, loss of brain stem reflexes, decorticate posturing, and irregular respirations.
CLINICAL FEATURES
![]() Clinical features vary with the depth of coma and the cause.
Clinical features vary with the depth of coma and the cause.
![]() Pupillary and other cranial nerve findings, hemiparesis, and response to stimulation can often assign the cause to diffuse CNS dysfunction (toxic-metabolic coma) or focal CNS dysfunction (structural coma).
Pupillary and other cranial nerve findings, hemiparesis, and response to stimulation can often assign the cause to diffuse CNS dysfunction (toxic-metabolic coma) or focal CNS dysfunction (structural coma).
![]() Diffuse CNS dysfunction can result from toxic and metabolic conditions. Physical findings do not point to a specific region of brain dysfunction. If present, movements and muscle stretch reflexes are symmetric. Pupillary response is generally preserved. The pupils are small but reactive, and extraocular movements, if present, are symmetric.
Diffuse CNS dysfunction can result from toxic and metabolic conditions. Physical findings do not point to a specific region of brain dysfunction. If present, movements and muscle stretch reflexes are symmetric. Pupillary response is generally preserved. The pupils are small but reactive, and extraocular movements, if present, are symmetric.
![]() Structural coma may be further subdivided into hemispheric (supratentorial) or posterior fossa (infratento-rial) coma.
Structural coma may be further subdivided into hemispheric (supratentorial) or posterior fossa (infratento-rial) coma.
![]() Coma from hemispheric lesions or supratentorial masses may present with progressive hemiparesis or asymmetric muscle tone and reflexes. Coma without lateralizing signs may result from decreased cerebral perfusion secondary to increased ICP. In severe cases, hypertension and bradycardia (the Cushing reflex) may develop.
Coma from hemispheric lesions or supratentorial masses may present with progressive hemiparesis or asymmetric muscle tone and reflexes. Coma without lateralizing signs may result from decreased cerebral perfusion secondary to increased ICP. In severe cases, hypertension and bradycardia (the Cushing reflex) may develop.
![]() Coma from infratentorial or posterior fossa lesions, such as an expanding cerebellar hemorrhage, may cause abrupt coma, abnormal extensor posturing, loss of pupillary reflexes, and loss of extraocular movements. Brain stem compression with loss of brain stem reflexes may develop rapidly. Another infratentorial cause of coma, pontine hemorrhage, may present with pinpoint-sized pupils.
Coma from infratentorial or posterior fossa lesions, such as an expanding cerebellar hemorrhage, may cause abrupt coma, abnormal extensor posturing, loss of pupillary reflexes, and loss of extraocular movements. Brain stem compression with loss of brain stem reflexes may develop rapidly. Another infratentorial cause of coma, pontine hemorrhage, may present with pinpoint-sized pupils.
![]() Pseudocoma or psychogenic coma may generally be distinguished from true coma by good history taking and observation of responses to stimulation. Pupillary responses, extraocular movements, muscle tone, and reflexes are intact. The patient may resist manual eye opening. The patient may consistently look away from the examiner, and nystagmus will be demonstrated with caloric vestibular testing.
Pseudocoma or psychogenic coma may generally be distinguished from true coma by good history taking and observation of responses to stimulation. Pupillary responses, extraocular movements, muscle tone, and reflexes are intact. The patient may resist manual eye opening. The patient may consistently look away from the examiner, and nystagmus will be demonstrated with caloric vestibular testing.
DIAGNOSIS AND DIFFERENTIAL
![]() Assessment is directed at rapidly determining if the CNS dysfunction is from diffuse impairment or from a local, and perhaps surgically treatable, lesion.
Assessment is directed at rapidly determining if the CNS dysfunction is from diffuse impairment or from a local, and perhaps surgically treatable, lesion.
![]() History, physical examination, lab tests, and neuroim-aging will usually identify the cause.
History, physical examination, lab tests, and neuroim-aging will usually identify the cause.
![]() Abrupt coma suggests an acute CNS process such as stroke or seizures, whereas gradual onset suggests a progressive CNS lesion or a metabolic process such as hyperglycemia.
Abrupt coma suggests an acute CNS process such as stroke or seizures, whereas gradual onset suggests a progressive CNS lesion or a metabolic process such as hyperglycemia.
![]() General examination may reveal signs of trauma or suggest other diagnostic possibilities, such as a toxidrome.
General examination may reveal signs of trauma or suggest other diagnostic possibilities, such as a toxidrome.
![]() Asymmetric muscle tone or reflexes, or asymmetric findings on examination of cranial nerves through papillary examination, assessment of corneal reflexes, and testing of oculovestibular reflexes suggest a focal lesion.
Asymmetric muscle tone or reflexes, or asymmetric findings on examination of cranial nerves through papillary examination, assessment of corneal reflexes, and testing of oculovestibular reflexes suggest a focal lesion.
![]() CT is the initial neuroimaging of choice.
CT is the initial neuroimaging of choice.
![]() Lumbar puncture should be considered if CT findings are unremarkable and CNS bleeding or infection is suspected.
Lumbar puncture should be considered if CT findings are unremarkable and CNS bleeding or infection is suspected.
![]() Basilar artery thrombosis should be suspected in a comatose patient with a “normal” head CT, in which the only finding may be a hyperdense basilar artery. MRI or cerebral angiography is needed to make the diagnosis.
Basilar artery thrombosis should be suspected in a comatose patient with a “normal” head CT, in which the only finding may be a hyperdense basilar artery. MRI or cerebral angiography is needed to make the diagnosis.
![]() If nonconvulsive status epilepticus or subtle status epilepticus is suspected, urgent electroencephalography should be performed and neurologic consultation sought.
If nonconvulsive status epilepticus or subtle status epilepticus is suspected, urgent electroencephalography should be performed and neurologic consultation sought.
![]() In the pediatric patient, toxic ingestions, infections, and child abuse have a greater frequency and should be actively investigated.
In the pediatric patient, toxic ingestions, infections, and child abuse have a greater frequency and should be actively investigated.
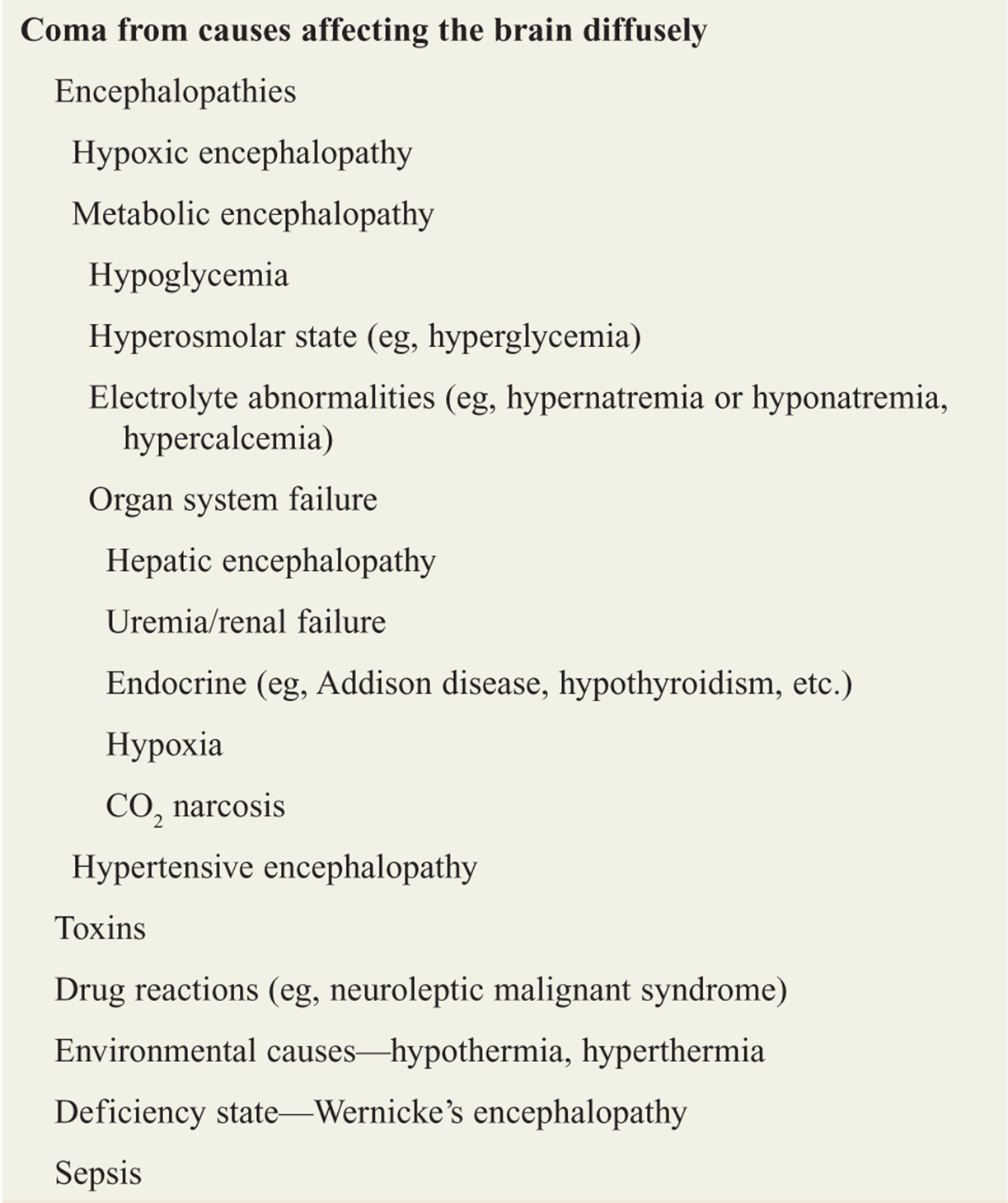
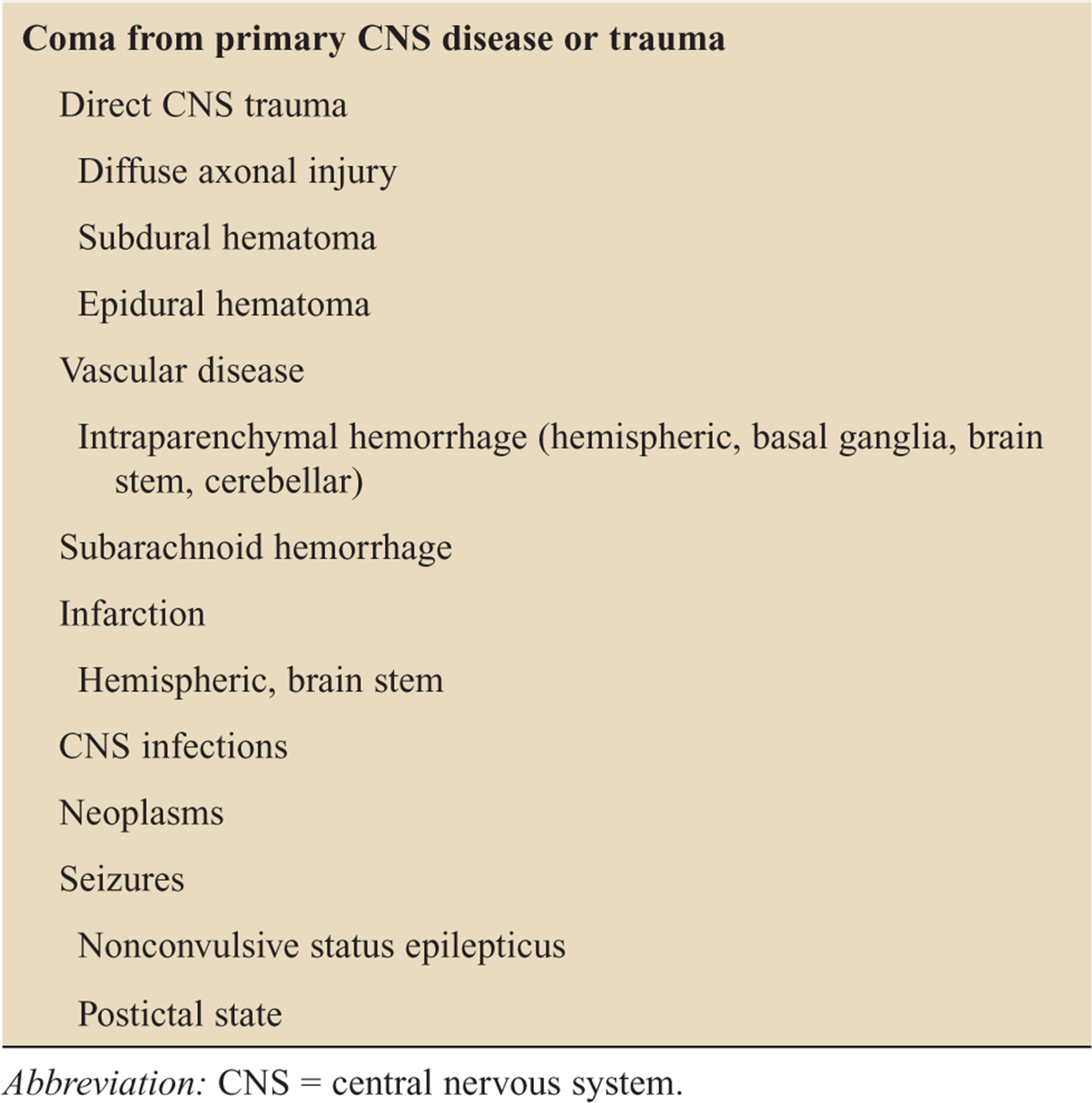
![]() The differential diagnosis includes generalized disease processes that also affect the brain, as well as primary CNS disorders (Table 144-4).
The differential diagnosis includes generalized disease processes that also affect the brain, as well as primary CNS disorders (Table 144-4).
TABLE 144-4 Differential Diagnosis of Coma
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treatment involves identification of the etiology and initiation of specific therapy.
Treatment involves identification of the etiology and initiation of specific therapy.
![]() Stabilization of airway, ventilation, and circulation is the top priority.
Stabilization of airway, ventilation, and circulation is the top priority.
![]() Readily reversible causes such as hypoglycemia, hypoxia, and opiate overdose should be sought. In the setting of hypoglycemia, thiamine should be administered before glucose in patients with a suspected history of alcohol abuse or malnutrition.
Readily reversible causes such as hypoglycemia, hypoxia, and opiate overdose should be sought. In the setting of hypoglycemia, thiamine should be administered before glucose in patients with a suspected history of alcohol abuse or malnutrition.
![]() Naloxone administration is prudent because signs of opiate overdose may be absent.
Naloxone administration is prudent because signs of opiate overdose may be absent.
![]() If increased ICP is suspected, steps should be taken to reduce it or minimize further rise.
If increased ICP is suspected, steps should be taken to reduce it or minimize further rise.
![]() In intubated patients, paralysis and sedation should be used to prevent the patient from “bucking” the ventilator.
In intubated patients, paralysis and sedation should be used to prevent the patient from “bucking” the ventilator.
![]() The head should be elevated 30 degrees and at mid-line to aid in venous drainage.
The head should be elevated 30 degrees and at mid-line to aid in venous drainage.
![]() Mannitol, 0.5 to 1.0 gram/kg IV, may transiently reduce ICP.
Mannitol, 0.5 to 1.0 gram/kg IV, may transiently reduce ICP.
![]() In cases of brain edema associated with tumor, dex-amethasone, 10 milligrams IV, reduces edema over several hours.
In cases of brain edema associated with tumor, dex-amethasone, 10 milligrams IV, reduces edema over several hours.
![]() Hyperventilation can reduce cerebral blood volume and transiently lower ICP. Current recommendations are to avoid excessive hyperventilation (partial pressure of arterial carbon dioxide ≤35 mm Hg) during the first 24 hours after brain injury.
Hyperventilation can reduce cerebral blood volume and transiently lower ICP. Current recommendations are to avoid excessive hyperventilation (partial pressure of arterial carbon dioxide ≤35 mm Hg) during the first 24 hours after brain injury.
![]() Patients with readily reversible causes of coma, such as insulin-induced hypoglycemia, may be discharged if treatment is initiated, the patient returns to baseline mental status, the cause of the episode is clear, and the patient has reliable home care and follow-up.
Patients with readily reversible causes of coma, such as insulin-induced hypoglycemia, may be discharged if treatment is initiated, the patient returns to baseline mental status, the cause of the episode is clear, and the patient has reliable home care and follow-up.
![]() In all other cases, admission is warranted for further evaluation and treatment.
In all other cases, admission is warranted for further evaluation and treatment.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 162, “Altered Mental Status and Coma,” by J. Stephen Huff.