C. Crawford Mechem
PATHOPHYSIOLOGY
![]() A seizure is an episode of abnormal neurologic function caused by inappropriate electrical discharge of brain neurons.
A seizure is an episode of abnormal neurologic function caused by inappropriate electrical discharge of brain neurons.
![]() Epilepsy is a clinical condition in which an individual is subject to recurrent seizures. The term is ordinarily not applied to seizures caused by reversible conditions.
Epilepsy is a clinical condition in which an individual is subject to recurrent seizures. The term is ordinarily not applied to seizures caused by reversible conditions.
![]() Primary or idiopathic seizures are those without a clear cause.
Primary or idiopathic seizures are those without a clear cause.
![]() Secondary or symptomatic seizures are the result of another identifiable condition.
Secondary or symptomatic seizures are the result of another identifiable condition.
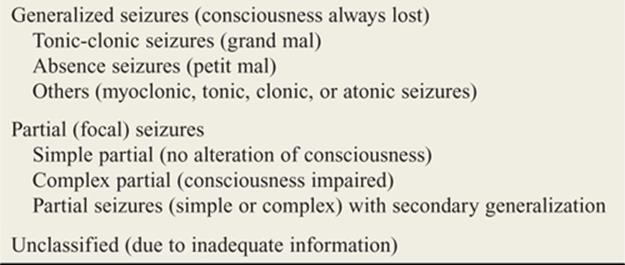
![]() Seizures may be classified in two major groups: generalized and partial (focal) (Table 147-1).
Seizures may be classified in two major groups: generalized and partial (focal) (Table 147-1).
![]() Generalized seizures are caused by simultaneous activation of the entire cerebral cortex.
Generalized seizures are caused by simultaneous activation of the entire cerebral cortex.
![]() Partial seizures are due to electrical discharges in a localized, structural lesion of the cerebral cortex. The discharges may remain localized or can generalize.
Partial seizures are due to electrical discharges in a localized, structural lesion of the cerebral cortex. The discharges may remain localized or can generalize.
![]() Complex partial seizures are often due to focal discharges in the temporal lobe.
Complex partial seizures are often due to focal discharges in the temporal lobe.
CLINICAL FEATURES
![]() Generalized seizures often begin with abrupt loss of consciousness without warning. The patient may then become rigid, with extension of the trunk and extremities, and fall to the ground. Apnea, cyanosis, urinary incontinence, and vomiting may be seen.
Generalized seizures often begin with abrupt loss of consciousness without warning. The patient may then become rigid, with extension of the trunk and extremities, and fall to the ground. Apnea, cyanosis, urinary incontinence, and vomiting may be seen.
![]() As the rigid (tonic) phase subsides, symmetric rhythmic (clonic) jerking of the trunk and extremities develops. After the attack, the patient is flaccid and unconscious.
As the rigid (tonic) phase subsides, symmetric rhythmic (clonic) jerking of the trunk and extremities develops. After the attack, the patient is flaccid and unconscious.
![]() A typical generalized seizure episode lasts from 60 to 90 seconds. Consciousness returns gradually, and postictal confusion and fatigue may persist for several hours.
A typical generalized seizure episode lasts from 60 to 90 seconds. Consciousness returns gradually, and postictal confusion and fatigue may persist for several hours.
TABLE 147-1 Classification of Seizures
![]() Absence seizures are brief, usually lasting only a few seconds. Patients appear confused or withdrawn and do not respond to voice or other stimulation. Postural tone is maintained, and patients usually remain continent. There is no postictal period.
Absence seizures are brief, usually lasting only a few seconds. Patients appear confused or withdrawn and do not respond to voice or other stimulation. Postural tone is maintained, and patients usually remain continent. There is no postictal period.
![]() Simple partial seizures remain localized and consciousness is not affected.
Simple partial seizures remain localized and consciousness is not affected.
![]() Unilateral tonic or clonic movements limited to one extremity suggest a focus in the motor cortex.
Unilateral tonic or clonic movements limited to one extremity suggest a focus in the motor cortex.
![]() Visual symptoms, such as flashing lights, often result from an occipital focus, while olfactory or gustatory hallucinations may arise from the medial temporal lobe.
Visual symptoms, such as flashing lights, often result from an occipital focus, while olfactory or gustatory hallucinations may arise from the medial temporal lobe.
![]() Symptoms of complex partial seizures may include automatisms, visceral symptoms, hallucinations, memory disturbances, distorted perception, and affective disorders.
Symptoms of complex partial seizures may include automatisms, visceral symptoms, hallucinations, memory disturbances, distorted perception, and affective disorders.
![]() Automatisms are typically simple, repetitive, purposeless movements such as lip smacking, fiddling with clothing or buttons, or repeating short phrases.
Automatisms are typically simple, repetitive, purposeless movements such as lip smacking, fiddling with clothing or buttons, or repeating short phrases.
![]() Visceral symptoms include sensation of butterflies rising up from the epigastrium.
Visceral symptoms include sensation of butterflies rising up from the epigastrium.
![]() Hallucinations may be olfactory, gustatory, visual, or auditory.
Hallucinations may be olfactory, gustatory, visual, or auditory.
![]() There may be complex distortions of visual perception, time, and memory.
There may be complex distortions of visual perception, time, and memory.
![]() Affective symptoms include fear, paranoia, depression, or elation.
Affective symptoms include fear, paranoia, depression, or elation.
![]() Eclampsia refers to the combination of seizures, hypertension, edema, and proteinuria in pregnant women beyond 20 weeks’ gestation or up to 3 weeks postpartum.
Eclampsia refers to the combination of seizures, hypertension, edema, and proteinuria in pregnant women beyond 20 weeks’ gestation or up to 3 weeks postpartum.
![]() Status epilepticus is continuous seizure activity for more than 5 minutes.
Status epilepticus is continuous seizure activity for more than 5 minutes.
![]() Nonconvulsive status epilepticus is characterized by coma, fluctuating mental status, or confusion with minimal or imperceptible convulsive activity. It is confirmed by EEG.
Nonconvulsive status epilepticus is characterized by coma, fluctuating mental status, or confusion with minimal or imperceptible convulsive activity. It is confirmed by EEG.
![]() Epilepsia partialis continua is focal tonic-clonic seizure activity with normal alertness and responsiveness. The distal leg and arm are most commonly affected.
Epilepsia partialis continua is focal tonic-clonic seizure activity with normal alertness and responsiveness. The distal leg and arm are most commonly affected.
DIAGNOSIS AND DIFFERENTIAL
![]() The first step in diagnosis is determining if the episode was indeed a true seizure. A careful history should be obtained from the patient and witnesses.
The first step in diagnosis is determining if the episode was indeed a true seizure. A careful history should be obtained from the patient and witnesses.
![]() Important historical information includes the rapidity of onset, presence of a preceding aura, progression of motor activity, whether the activity was local or generalized, and whether the patient became incontinent.
Important historical information includes the rapidity of onset, presence of a preceding aura, progression of motor activity, whether the activity was local or generalized, and whether the patient became incontinent.
![]() Determine the duration of the episode and postictal behavior.
Determine the duration of the episode and postictal behavior.
![]() If the patient has a known seizure disorder, investigate the regular pattern of seizures, medications taken, dosage changes, and the possibility of noncompliance.
If the patient has a known seizure disorder, investigate the regular pattern of seizures, medications taken, dosage changes, and the possibility of noncompliance.
![]() Investigate contributing factors such as sleep deprivation, alcohol or substance abuse or withdrawal, infection, or electrolyte disturbances.
Investigate contributing factors such as sleep deprivation, alcohol or substance abuse or withdrawal, infection, or electrolyte disturbances.
![]() In patients with first-time seizures, a more detailed history should include recent or remote head trauma or headaches, current pregnancy or recent delivery, systemic illness (especially cancer), coagulopathy or anticoagulation, or drug or alcohol ingestion or withdrawal. In patients who have traveled to, or who are natives of, developing world countries, neurocyst-icercosis, a central nervous system (CNS) infection with the larval stage of the tapeworm Taenia solium, should be considered.
In patients with first-time seizures, a more detailed history should include recent or remote head trauma or headaches, current pregnancy or recent delivery, systemic illness (especially cancer), coagulopathy or anticoagulation, or drug or alcohol ingestion or withdrawal. In patients who have traveled to, or who are natives of, developing world countries, neurocyst-icercosis, a central nervous system (CNS) infection with the larval stage of the tapeworm Taenia solium, should be considered.
![]() Common causes of secondary seizures are listed in Table 147-2.
Common causes of secondary seizures are listed in Table 147-2.
![]() The physical examination should include a search for any injuries or complications resulting from the seizure, such as posterior shoulder dislocation, oral trauma, and aspiration.
The physical examination should include a search for any injuries or complications resulting from the seizure, such as posterior shoulder dislocation, oral trauma, and aspiration.
TABLE 147-2 Common Causes of Secondary Seizures
|
Trauma (recent or remote) |
|
Intracranial hemorrhage (subdural, epidural, subarachnoid, intraparenchymal) |
|
Structural CNS abnormalities |
|
Vascular lesion (aneurysm, arteriovenous malformation) |
|
Mass lesions (primary or metastatic neoplasms) |
|
Degenerative neurologic diseases |
|
Congenital brain abnormalities |
|
Infection (meningitis, encephalitis, abscess) |
|
Metabolic disturbances |
|
Hypo- or hyperglycemia |
|
Hypo- or hypernatremia |
|
Hyperosmolar states |
|
Uremia |
|
Hepatic failure |
|
Hypocalcemia, hypomagnesemia (rare) |
|
Toxins and drugs (many) |
|
Cocaine, lidocaine |
|
Antidepressants |
|
Theophylline |
|
Alcohol withdrawal |
|
Drug withdrawal |
|
Eclampsia of pregnancy (may occur up to 8 weeks postpartum) |
|
Hypertensive encephalopathy |
|
Anoxic-ischemic injury (cardiac arrest, severe hypoxemia) |
![]() Perform a directed neurologic examination, including level of consciousness and mentation. A transient, focal deficit (usually unilateral) following a focal seizure is referred to as Todd paralysis and should resolve within 48 hours. If the symptoms cannot be attributed to a benign cause, further urgent evaluation is warranted.
Perform a directed neurologic examination, including level of consciousness and mentation. A transient, focal deficit (usually unilateral) following a focal seizure is referred to as Todd paralysis and should resolve within 48 hours. If the symptoms cannot be attributed to a benign cause, further urgent evaluation is warranted.
![]() In an adult with a first seizure or when the history is unclear, laboratory tests may include a bedside glucose, basic metabolic panel, calcium, magnesium, a pregnancy test, and toxicology studies.
In an adult with a first seizure or when the history is unclear, laboratory tests may include a bedside glucose, basic metabolic panel, calcium, magnesium, a pregnancy test, and toxicology studies.
![]() Obtain assays for anticonvulsant drug levels when applicable.
Obtain assays for anticonvulsant drug levels when applicable.
![]() In an adult with a history of seizures who presents after a typical, unremarkable seizure and has a normal physical examination, a bedside glucose level and an anticonvulsant drug level are usually all that are indicated.
In an adult with a history of seizures who presents after a typical, unremarkable seizure and has a normal physical examination, a bedside glucose level and an anticonvulsant drug level are usually all that are indicated.
![]() The blood prolactin level may be elevated for 15 to 60 minutes immediately after a seizure and may help distinguish a true seizure from a pseudoseizure.
The blood prolactin level may be elevated for 15 to 60 minutes immediately after a seizure and may help distinguish a true seizure from a pseudoseizure.
![]() Obtain a noncontrast head CT for patients with a first seizure or a change in established seizure pattern to identify an acute intracranial process.
Obtain a noncontrast head CT for patients with a first seizure or a change in established seizure pattern to identify an acute intracranial process.
![]() Because important processes, such as tumors or vascular anomalies, may not be evident on noncontrast studies, a follow-up contrast CT or MRI may be arranged, often in coordination with the consulting neurologist.
Because important processes, such as tumors or vascular anomalies, may not be evident on noncontrast studies, a follow-up contrast CT or MRI may be arranged, often in coordination with the consulting neurologist.
![]() Lumbar puncture is indicated if the patient is febrile or immunocompromised, or if subarachnoid hemorrhage is suspected in the presence of a normal non-contrast head CT.
Lumbar puncture is indicated if the patient is febrile or immunocompromised, or if subarachnoid hemorrhage is suspected in the presence of a normal non-contrast head CT.
![]() EEG can be considered to evaluate patients with persistent, unexplained altered mental status to exclude nonconvulsive status epilepticus or other processes or to detect ongoing status epilepticus after paralysis for endotracheal intubation and induction of general anesthesia.
EEG can be considered to evaluate patients with persistent, unexplained altered mental status to exclude nonconvulsive status epilepticus or other processes or to detect ongoing status epilepticus after paralysis for endotracheal intubation and induction of general anesthesia.
![]() The differential diagnosis of seizures includes syncope, pseudoseizures, migraine headache, hyper-ventilation syndrome, movement disorders, and nar-colepsy/cataplexy.
The differential diagnosis of seizures includes syncope, pseudoseizures, migraine headache, hyper-ventilation syndrome, movement disorders, and nar-colepsy/cataplexy.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Usually little is required during the course of a seizure other than to protect the patient from injury and prevent aspiration.
Usually little is required during the course of a seizure other than to protect the patient from injury and prevent aspiration.
![]() IV anticonvulsants are not indicated during the course of an uncomplicated seizure.
IV anticonvulsants are not indicated during the course of an uncomplicated seizure.
![]() Once the seizure subsides, a clear airway should be ensured. Suction and airway adjuncts should be readily available.
Once the seizure subsides, a clear airway should be ensured. Suction and airway adjuncts should be readily available.
![]() In a patient with a known seizure disorder, if anti-convulsant levels are low, supplemental doses may be administered and the regular regimen restarted or adjusted.
In a patient with a known seizure disorder, if anti-convulsant levels are low, supplemental doses may be administered and the regular regimen restarted or adjusted.
![]() Lorazepam (2-4 milligrams IV) is the initial agent of choice to control a seizure until more specific agents can be given. IV diazepam (5-10 milligrams IV) is an acceptable alternative.
Lorazepam (2-4 milligrams IV) is the initial agent of choice to control a seizure until more specific agents can be given. IV diazepam (5-10 milligrams IV) is an acceptable alternative.
![]() Oral loading of phenytoin (18 milligrams/kg PO as a single dose or divided into three doses given every 2 hours) will achieve therapeutic levels in 2 to 24 hours.
Oral loading of phenytoin (18 milligrams/kg PO as a single dose or divided into three doses given every 2 hours) will achieve therapeutic levels in 2 to 24 hours.
![]() IV phenytoin, 10 to 20 milligrams/kg at an IV rate of 25 milligrams/minute, achieves anticonvulsant effects in 1 to 2 hours.
IV phenytoin, 10 to 20 milligrams/kg at an IV rate of 25 milligrams/minute, achieves anticonvulsant effects in 1 to 2 hours.
![]() The dose of fosphenytoin is 10 to 20 milligrams phenytoin equivalent/kg at a maximum IV rate of 150 milligrams/min.
The dose of fosphenytoin is 10 to 20 milligrams phenytoin equivalent/kg at a maximum IV rate of 150 milligrams/min.
![]() In the known or suspected noncompliant patient, obtain a serum anticonvulsant level before administering a supplemental dose.
In the known or suspected noncompliant patient, obtain a serum anticonvulsant level before administering a supplemental dose.
![]() If anticonvulsant levels are adequate and the patient has had a single attack, specific treatment may not be needed if the pattern falls within the patient’s expected range.
If anticonvulsant levels are adequate and the patient has had a single attack, specific treatment may not be needed if the pattern falls within the patient’s expected range.
![]() Identify precipitants or conditions that have lowered the seizure threshold. If none is found, a change in or adjustment of medication may be needed. Make this decision in consultation with the patient’s primary physician or neurologist.
Identify precipitants or conditions that have lowered the seizure threshold. If none is found, a change in or adjustment of medication may be needed. Make this decision in consultation with the patient’s primary physician or neurologist.
![]() Treat patients with secondary seizures due to a neurologic condition due to the risk of recurrence.
Treat patients with secondary seizures due to a neurologic condition due to the risk of recurrence.
![]() There are no fixed guidelines regarding initiation of anticonvulsant therapy in the patient with a first seizure. The decision depends on the risk of recurrent seizures weighed against the risk-benefit ratio of anticonvulsant therapy.
There are no fixed guidelines regarding initiation of anticonvulsant therapy in the patient with a first seizure. The decision depends on the risk of recurrent seizures weighed against the risk-benefit ratio of anticonvulsant therapy.
![]() The goal of treatment for status epilepticus is seizure control within 30 minutes of onset (Fig. 147-1). Refractory status epilepticus is defined as persistent seizure activity despite the IV administration of adequate amounts of two antiepileptic agents, generally a benzodiazepine and phenytoin.
The goal of treatment for status epilepticus is seizure control within 30 minutes of onset (Fig. 147-1). Refractory status epilepticus is defined as persistent seizure activity despite the IV administration of adequate amounts of two antiepileptic agents, generally a benzodiazepine and phenytoin.
![]() Neuromuscular blocking agents, such as vecuronium, may be helpful. These drugs will abolish tonic-clonic movements and may facilitate ventilation, but they have no effect on abnormal neuronal activity. Therefore, EEG monitoring and other pharmacologic interventions are mandatory (Fig. 147-1).
Neuromuscular blocking agents, such as vecuronium, may be helpful. These drugs will abolish tonic-clonic movements and may facilitate ventilation, but they have no effect on abnormal neuronal activity. Therefore, EEG monitoring and other pharmacologic interventions are mandatory (Fig. 147-1).
![]() A large-bore IV line should be established and bedside glucose determination made. IV glucose should be given to hypoglycemie patients.
A large-bore IV line should be established and bedside glucose determination made. IV glucose should be given to hypoglycemie patients.
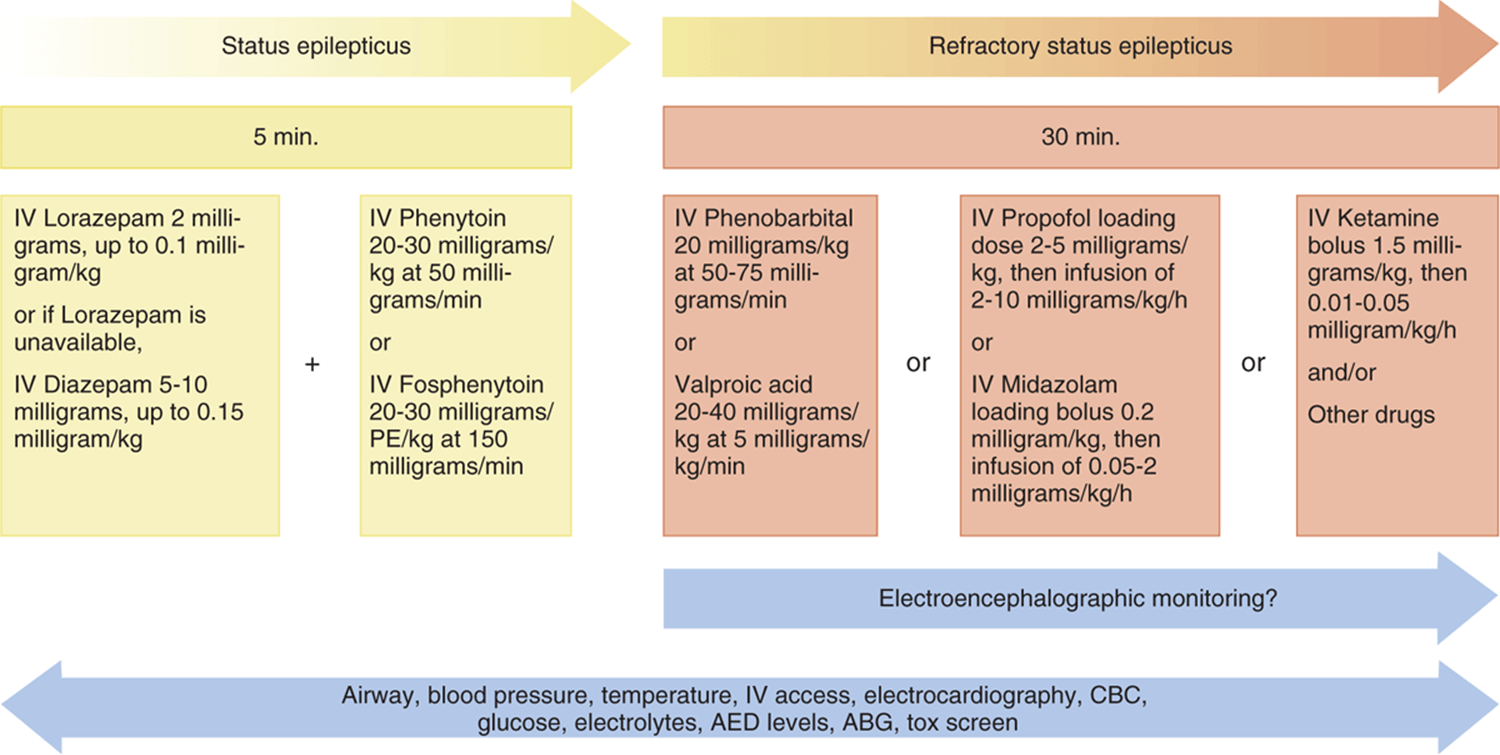
FIG. 147-1. Guidelines for management of status epilepticus. ABG = arterial blood gases; AED = antiepileptic drug; CBC = complete blood count; PE = phenytoin equivalent.
![]() If toxic ingestion is suspected, perform GI decontamination, if appropriate.
If toxic ingestion is suspected, perform GI decontamination, if appropriate.
![]() If bacterial meningitis is suspected, administer empiric antibiotic therapy.
If bacterial meningitis is suspected, administer empiric antibiotic therapy.
![]() Patients with a new-onset seizure may be discharged for further outpatient evaluation if they return to baseline and life-threatening conditions have been excluded. Disposition is ideally made in consultation with a neurologist or primary care physician.
Patients with a new-onset seizure may be discharged for further outpatient evaluation if they return to baseline and life-threatening conditions have been excluded. Disposition is ideally made in consultation with a neurologist or primary care physician.
![]() Instruct discharged patients to take precautions to minimize the risks for injury from further seizures. Driving is prohibited until cleared by the neurologist or primary care physician, and driving privileges should conform to state laws.
Instruct discharged patients to take precautions to minimize the risks for injury from further seizures. Driving is prohibited until cleared by the neurologist or primary care physician, and driving privileges should conform to state laws.
![]() Indications for admission following a new-onset seizure include persistent altered mental status, CNS infection or mass, eclampsia, underlying metabolic derangements not readily corrected in the ED, associated head trauma, absence of reliable caretakers at home, and inability to arrange a close follow-up appointment for further evaluation and therapy adjustment.
Indications for admission following a new-onset seizure include persistent altered mental status, CNS infection or mass, eclampsia, underlying metabolic derangements not readily corrected in the ED, associated head trauma, absence of reliable caretakers at home, and inability to arrange a close follow-up appointment for further evaluation and therapy adjustment.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 165, “Seizures and Status Epilepticus in Adults,” by Derrick D. Lung, Christina L. Catlett, and Judith E. Tintinalli.