Henderson D. McGinnis
EPIDEMIOLOGY
![]() Injuries to the leg and foot account for about 13% of traumatic wounds evaluated in the ED, distributed roughly into a third each for the foot, calf, and knee and thigh regions.
Injuries to the leg and foot account for about 13% of traumatic wounds evaluated in the ED, distributed roughly into a third each for the foot, calf, and knee and thigh regions.
![]() The foot is commonly injured in sports.
The foot is commonly injured in sports.
![]() Many children sustain foot lacerations from broken glass while playing outside.
Many children sustain foot lacerations from broken glass while playing outside.
![]() Bicycle spoke injuries result in complex lacerations with marked surrounding abrasions and even tissue loss, usually occurring over the lateral malleolus and the base of the fifth metatarsal.
Bicycle spoke injuries result in complex lacerations with marked surrounding abrasions and even tissue loss, usually occurring over the lateral malleolus and the base of the fifth metatarsal.
![]() Lawn mower injuries are usually sustained from the blades of push mowers when being pulled backwards. These wounds are heavily contaminated with multiple organisms.
Lawn mower injuries are usually sustained from the blades of push mowers when being pulled backwards. These wounds are heavily contaminated with multiple organisms.
![]() Metal lawn and garden edging is associated with plantar and knee injuries.
Metal lawn and garden edging is associated with plantar and knee injuries.
![]() Hockey skates are associated with injury to the underlying tibialis anterior tendon, extensor hallucis tendon, and the dorsalis pedis artery and nerve.
Hockey skates are associated with injury to the underlying tibialis anterior tendon, extensor hallucis tendon, and the dorsalis pedis artery and nerve.
PATHOPHYSIOLOGY
![]() The mechanism of the injury determines the likelihood of disruption to underlying tissue, the risk of a retained foreign body, and the degree of potential contamination.
The mechanism of the injury determines the likelihood of disruption to underlying tissue, the risk of a retained foreign body, and the degree of potential contamination.
![]() The following circumstances are associated with specific pathogens: (1) farming accidents (Clostridium perfringens), (2) wading in a freshwater stream (Aeromonas hydrophila), and (3) high-pressure water systems used for cleaning surfaces (Acinetobacter calcoaceticus).
The following circumstances are associated with specific pathogens: (1) farming accidents (Clostridium perfringens), (2) wading in a freshwater stream (Aeromonas hydrophila), and (3) high-pressure water systems used for cleaning surfaces (Acinetobacter calcoaceticus).
![]() Blunt force wounds often have irregular edges and are more likely to be associated with an underlying fracture. These characteristics increase the likelihood of wound infection compared to wounds caused by a sharp object.
Blunt force wounds often have irregular edges and are more likely to be associated with an underlying fracture. These characteristics increase the likelihood of wound infection compared to wounds caused by a sharp object.
CLINICAL FEATURES
![]() Evaluation of wounds in general is discussed in Chapter 11. It is important to determine the position of the limb at the time of injury, which will help to uncover occult tendon injuries.
Evaluation of wounds in general is discussed in Chapter 11. It is important to determine the position of the limb at the time of injury, which will help to uncover occult tendon injuries.
![]() Assessment for associated nerve, vessel, or tendon injury is mandatory.
Assessment for associated nerve, vessel, or tendon injury is mandatory.
![]() Prior to the use of anesthetic, the limb should be inspected for position at rest, and sensory neurologic function should be evaluated using light touch and two-point discrimination testing. One side can be compared to the other.
Prior to the use of anesthetic, the limb should be inspected for position at rest, and sensory neurologic function should be evaluated using light touch and two-point discrimination testing. One side can be compared to the other.
DIAGNOSIS AND DIFFERENTIAL
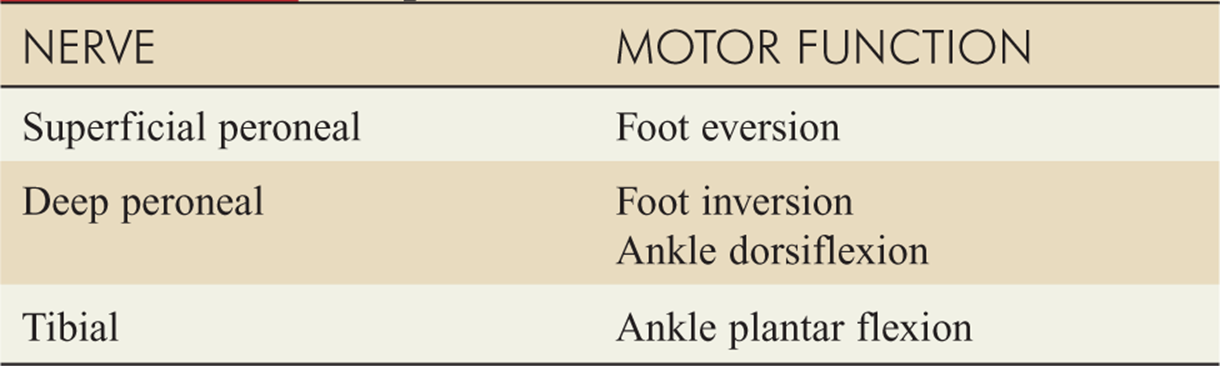
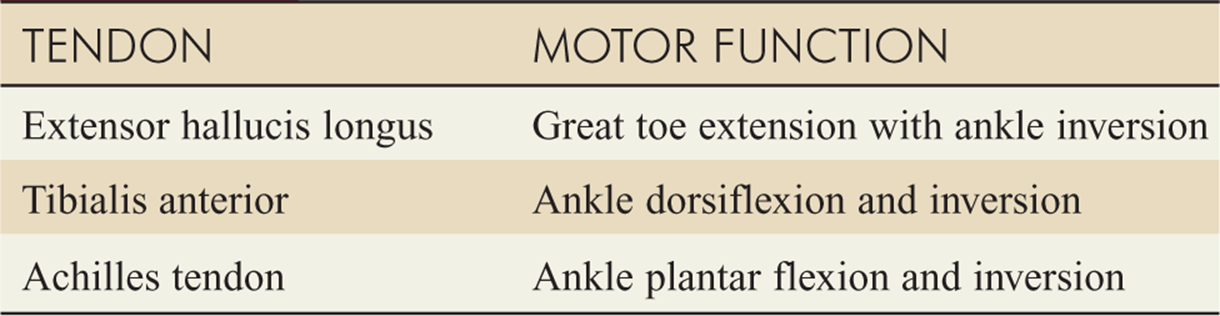
![]() Motor function may be better assessed after the wound is anesthetized (Tables 15-1 and 15-2). At this time, the wound can also be explored.
Motor function may be better assessed after the wound is anesthetized (Tables 15-1 and 15-2). At this time, the wound can also be explored.
![]() The limb should be moved through its full range of motion in order to exclude tendon injury.
The limb should be moved through its full range of motion in order to exclude tendon injury.
![]() Each tendon function should be tested individually, but the tendon should still be visibly inspected to rule out a partial laceration.
Each tendon function should be tested individually, but the tendon should still be visibly inspected to rule out a partial laceration.
![]() Laboratory studies are usually not indicated.
Laboratory studies are usually not indicated.
![]() Imaging is required if there is a possibility of fracture or radiopaque foreign body. X-ray all injuries caused by glass unless physical examination can reliably exclude a foreign body (see also Chapter 16). Also consider ultrasound or MRI in the evaluation of wounds for foreign bodies.
Imaging is required if there is a possibility of fracture or radiopaque foreign body. X-ray all injuries caused by glass unless physical examination can reliably exclude a foreign body (see also Chapter 16). Also consider ultrasound or MRI in the evaluation of wounds for foreign bodies.
TABLE 15-1 Motor Function of Lower Extremity Peripheral Nerves
EMERGENCY DEPARTMENT CARE AND DISPOSITION
GENERAL RECOMMENDATIONS
![]() See Chapter 11 for discussion of wound preparation; thorough irrigation of lower extremity wounds is essential.
See Chapter 11 for discussion of wound preparation; thorough irrigation of lower extremity wounds is essential.
![]() Wounds on the lower extremities are usually under greater tension than those on the upper limb. Consequently, a layered closure with 4–0 absorbable material to the fascia and interrupted 4–0 nonabsorb-able sutures to the skin is preferred. The foot is an exception to this guideline.
Wounds on the lower extremities are usually under greater tension than those on the upper limb. Consequently, a layered closure with 4–0 absorbable material to the fascia and interrupted 4–0 nonabsorb-able sutures to the skin is preferred. The foot is an exception to this guideline.
![]() Deep sutures should be avoided in diabetics and patients with stasis changes, because of the increased risk of infection.
Deep sutures should be avoided in diabetics and patients with stasis changes, because of the increased risk of infection.
![]() Tetanus immunization status should always be considered. The elderly are at particular risk for not being immunized.
Tetanus immunization status should always be considered. The elderly are at particular risk for not being immunized.
![]() Cyanoacrylate glue is usually not used on the lower extremities because of high wound tension.
Cyanoacrylate glue is usually not used on the lower extremities because of high wound tension.
![]() Lacerations involving the joint or tendons should be splinted in a position of function.
Lacerations involving the joint or tendons should be splinted in a position of function.
TABLE 15-2 Tendon Function of the Lower Extremities
KNEE INJURIES
![]() Wounds over the knee, as for all wounds over joints, should be examined throughout the range of movement.
Wounds over the knee, as for all wounds over joints, should be examined throughout the range of movement.
![]() Injuries over joints should also be evaluated for possible penetration of the joint capsule. Clinical evaluation alone is often insufficient. Radiography may reveal air in the joint.
Injuries over joints should also be evaluated for possible penetration of the joint capsule. Clinical evaluation alone is often insufficient. Radiography may reveal air in the joint.
![]() An alternative approach to diagnose joint penetration is to inject 60 mL of sterile saline, with or without a few drops of sterile fluorescein, into the joint using a standard joint aspiration technique at a site separate from the laceration. Leakage of the solution from the wound indicates disruption of the joint capsule injury. Consider the use of ultrasound in the evaluation of the injured knee.
An alternative approach to diagnose joint penetration is to inject 60 mL of sterile saline, with or without a few drops of sterile fluorescein, into the joint using a standard joint aspiration technique at a site separate from the laceration. Leakage of the solution from the wound indicates disruption of the joint capsule injury. Consider the use of ultrasound in the evaluation of the injured knee.
![]() The integrity of the popliteal artery, the popliteal nerve, and the tibial nerve should always be ascertained.
The integrity of the popliteal artery, the popliteal nerve, and the tibial nerve should always be ascertained.
![]() After closure, the knee should be splinted to prevent excessive tension on the wound edges.
After closure, the knee should be splinted to prevent excessive tension on the wound edges.
ANKLE INJURIES
![]() Lacerations to the ankle can easily damage underlying tendons. The joints should be moved through their full range with direct inspection of the wound to ensure there is no partial injury to the tendon. Particularly at risk are the Achilles tendon, the tibialis anterior, and the extensor hallucis longus.
Lacerations to the ankle can easily damage underlying tendons. The joints should be moved through their full range with direct inspection of the wound to ensure there is no partial injury to the tendon. Particularly at risk are the Achilles tendon, the tibialis anterior, and the extensor hallucis longus.
![]() Tendon injuries should be formally repaired.
Tendon injuries should be formally repaired.
![]() The Achilles tendon can rupture without a penetrating injury when a tensed gastrocnemius is suddenly contracted. This injury is most common in an athletic middle-aged male. Thompson’s test can be utilized to assess the Achilles tendon. While kneeling on a chair, the patient’s calf is gently squeezed at the midpoint. Absent plantar flexion of the foot indicates complete Achilles tendon laceration (a partial injury may still yield plantar flexion). Consider ultrasound imaging to evaluate the Achilles tendon.
The Achilles tendon can rupture without a penetrating injury when a tensed gastrocnemius is suddenly contracted. This injury is most common in an athletic middle-aged male. Thompson’s test can be utilized to assess the Achilles tendon. While kneeling on a chair, the patient’s calf is gently squeezed at the midpoint. Absent plantar flexion of the foot indicates complete Achilles tendon laceration (a partial injury may still yield plantar flexion). Consider ultrasound imaging to evaluate the Achilles tendon.
FOOT INJURIES
![]() Lacerations of the sole of the foot must be carefully explored to ensure not only the absence of tendon injury, but also the absence of foreign bodies. The patient lying prone with the foot supported on a pillow or overhanging the bed assists inspection.
Lacerations of the sole of the foot must be carefully explored to ensure not only the absence of tendon injury, but also the absence of foreign bodies. The patient lying prone with the foot supported on a pillow or overhanging the bed assists inspection.
![]() Regional anesthesia is often best for exploration and repair of lacerations in this area.
Regional anesthesia is often best for exploration and repair of lacerations in this area.
![]() Because of the high risk for infection, wounds older than 6 hours at presentation should probably not be repaired primarily.
Because of the high risk for infection, wounds older than 6 hours at presentation should probably not be repaired primarily.
![]() Large needles are required in order to adequately penetrate the thick dermis of the sole. Absorbable material is usually avoided in the foot. Nonabsorbable 3–0 or 4–0 material is used. Injuries to the dorsum of the foot can be repaired with 4–0 or 5–0 nonabsorbable sutures.
Large needles are required in order to adequately penetrate the thick dermis of the sole. Absorbable material is usually avoided in the foot. Nonabsorbable 3–0 or 4–0 material is used. Injuries to the dorsum of the foot can be repaired with 4–0 or 5–0 nonabsorbable sutures.
![]() Lacerations between the toes can be difficult to repair. An assistant can hold the toes apart. An interrupted mattress suture is often required to ensure adequate skin apposition.
Lacerations between the toes can be difficult to repair. An assistant can hold the toes apart. An interrupted mattress suture is often required to ensure adequate skin apposition.
![]() Crutches and a walking boot may be required after repair of any laceration on the foot.
Crutches and a walking boot may be required after repair of any laceration on the foot.
![]() Injuries to the foot caused by lawn mowers and by bicycle spokes may cause extensive soft tissue injury, along with underlying fractures and tendon lacerations. These injuries should be evaluated and treated by an orthopedic specialist.
Injuries to the foot caused by lawn mowers and by bicycle spokes may cause extensive soft tissue injury, along with underlying fractures and tendon lacerations. These injuries should be evaluated and treated by an orthopedic specialist.
![]() Infection occurs in 3% to 8% of lower extremity injuries, and up to 34% of foot lacerations. However, there is no evidence that prophylactic antibiotics reduce the frequency of postrepair wound infections. Therefore, the decision to use antibiotic prophylaxis is made using clinical judgment according to the degree of contamination, the presence of foreign debris, the presence of associated injuries, and host factors that predispose to infection.
Infection occurs in 3% to 8% of lower extremity injuries, and up to 34% of foot lacerations. However, there is no evidence that prophylactic antibiotics reduce the frequency of postrepair wound infections. Therefore, the decision to use antibiotic prophylaxis is made using clinical judgment according to the degree of contamination, the presence of foreign debris, the presence of associated injuries, and host factors that predispose to infection.
![]() Wounds sustained while wading in fresh water are prone to infection with Aeromonas hydrophila. Aeromonas hydrophila should be considered in any rapidly progressive case of cellulitis in the foot after an injury. Treat with fiuoroquinolone such as ciprofioxacin 500 milligrams twice daily. In children, trimethoprim-sulfamethoxazole, 5 mL of suspension per 10 kg up to 20 mL twice daily, is used.
Wounds sustained while wading in fresh water are prone to infection with Aeromonas hydrophila. Aeromonas hydrophila should be considered in any rapidly progressive case of cellulitis in the foot after an injury. Treat with fiuoroquinolone such as ciprofioxacin 500 milligrams twice daily. In children, trimethoprim-sulfamethoxazole, 5 mL of suspension per 10 kg up to 20 mL twice daily, is used.
HAIR-THREAD TOURNIQUET SYNDROME
![]() Hair-thread tourniquet syndrome is an unusual type of injury seen in infants. A strand or strands of hair wrap around one of the toes producing vascular compromise.
Hair-thread tourniquet syndrome is an unusual type of injury seen in infants. A strand or strands of hair wrap around one of the toes producing vascular compromise.
![]() The hair must be completely cut to avoid compromising the neurovascular bundle to the toe. This is best accomplished by making an incision on the extensor surface of the toe down to the extensor ligament.
The hair must be completely cut to avoid compromising the neurovascular bundle to the toe. This is best accomplished by making an incision on the extensor surface of the toe down to the extensor ligament.
DISPOSITION
![]() Patients should be instructed to keep wounds clean and dry.
Patients should be instructed to keep wounds clean and dry.
![]() Sutures should be removed in 10 to 14 days for the lower limb and in 14 days for lacerations over joints.
Sutures should be removed in 10 to 14 days for the lower limb and in 14 days for lacerations over joints.
![]() Patients should receive routine wound care instructions. Elevation of the affected limb will reduce edema and aid healing.
Patients should receive routine wound care instructions. Elevation of the affected limb will reduce edema and aid healing.
![]() Heavily contaminated wounds or those that require complex repair should be rechecked after 48 hours.
Heavily contaminated wounds or those that require complex repair should be rechecked after 48 hours.
![]() Use crutches 7 to 10 days as needed to prevent additional tension on the wound.
Use crutches 7 to 10 days as needed to prevent additional tension on the wound.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 48, “Lacerations of the Leg and Foot,” by Timothy F. Platts-Mills.