Jeffrey L. Hackman
DIAGNOSIS OF KNEE AND HIP DISEASES AND SYNDROMES
![]() Most knee and hip diseases and syndromes are diag nosed or suggested by a focused history and physical examination (see Table 181-1).
Most knee and hip diseases and syndromes are diag nosed or suggested by a focused history and physical examination (see Table 181-1).
TABLE 181-1 Suggested Clues for the Differential Diagnosis of Hip and Knee Pain
Determine the location of the pain to narrow down the potential diagnosis.
Determine the activities that bring on the pain.
The knee “giving out” or “buckling” generally is due to pain and reflex muscle inhibition rather than an acute neurologic emergency. This complaint may also represent patellar subluxation or ligamentous injury and joint instability.
Poor conditioning or quadriceps weakness generally causes anterior knee pain of the patellofemoral syndrome; therapy should address this weakness.
Locking of the knee suggests a meniscal injury, which may be chronic.
A popping sensation or sound at the onset of pain is reliable for a ligamentous injury.
A recurrent effusion after activity suggests a meniscal injury.
Pain at the joint line suggests a meniscal injury.
REGIONAL NERVE ENTRAPMENT SYNDROMES
MERALGIA PARESTHETICA
![]() Compressive inflammation of the lateral femoral cutaneous nerve is the most common lower extremity nerve entrapment syndrome.
Compressive inflammation of the lateral femoral cutaneous nerve is the most common lower extremity nerve entrapment syndrome.
![]() Symptoms include pain in the hip, thigh, or groin, burning or tingling paresthesias, and hypersensitivity to light touch.
Symptoms include pain in the hip, thigh, or groin, burning or tingling paresthesias, and hypersensitivity to light touch.
![]() Tapping over the anterior superior iliac spine may reproduce the pain.
Tapping over the anterior superior iliac spine may reproduce the pain.
![]() Treatment involves removing the source of irritation (eg, obesity, pregnancy, tight pants belt) and NSAIDs.
Treatment involves removing the source of irritation (eg, obesity, pregnancy, tight pants belt) and NSAIDs.
OBTURATOR NERVE ENTRAPMENT
![]() The nerve is most commonly entrapped by pelvic fractures, causing pain in the groin and down the inner thigh.
The nerve is most commonly entrapped by pelvic fractures, causing pain in the groin and down the inner thigh.
![]() Other causes include fascial bands at the distal obturator canal in athletes, pelvic masses, and pelvic hematomas.
Other causes include fascial bands at the distal obturator canal in athletes, pelvic masses, and pelvic hematomas.
ILIOINGUINAL NERVE ENTRAPMENT
![]() Hypertrophy of the abdominal wall musculature or pregnancy may cause entrapment.
Hypertrophy of the abdominal wall musculature or pregnancy may cause entrapment.
![]() Pain and hypoesthesia may be exacerbated by hyper-extension of the hip.
Pain and hypoesthesia may be exacerbated by hyper-extension of the hip.
PIRIFORMIS SYNDROME
![]() Irritation of the sciatic nerve by the piriformis muscle causes pain in the buttocks and hamstring muscles.
Irritation of the sciatic nerve by the piriformis muscle causes pain in the buttocks and hamstring muscles.
![]() Pain is exacerbated by sitting, climbing stairs, or squatting.
Pain is exacerbated by sitting, climbing stairs, or squatting.
PSOAS ABSCESS
![]() Abscess of the psoas muscle may present with abdominal pain radiating to the hip or flank, fever, and limp.
Abscess of the psoas muscle may present with abdominal pain radiating to the hip or flank, fever, and limp.
![]() Staphylococcus aureus is the most common pathogen (80%).
Staphylococcus aureus is the most common pathogen (80%).
![]() The diagnosis is made by CT.
The diagnosis is made by CT.
![]() Treatment includes antibiotics and surgical drainage.
Treatment includes antibiotics and surgical drainage.
BURSAL SYNDROMES OF THE HIP AND KNEE
![]() Hip and knee bursae may cause localized pain due to inflammation, infection, rheumatologic disorders (psoriatic arthritis, rheumatoid arthritis, ankylosing spondylitis), or crystalline disease (gout, pseudogout).
Hip and knee bursae may cause localized pain due to inflammation, infection, rheumatologic disorders (psoriatic arthritis, rheumatoid arthritis, ankylosing spondylitis), or crystalline disease (gout, pseudogout).
![]() Infection may be difficult to distinguish from nonin-fectious inflammation.
Infection may be difficult to distinguish from nonin-fectious inflammation.
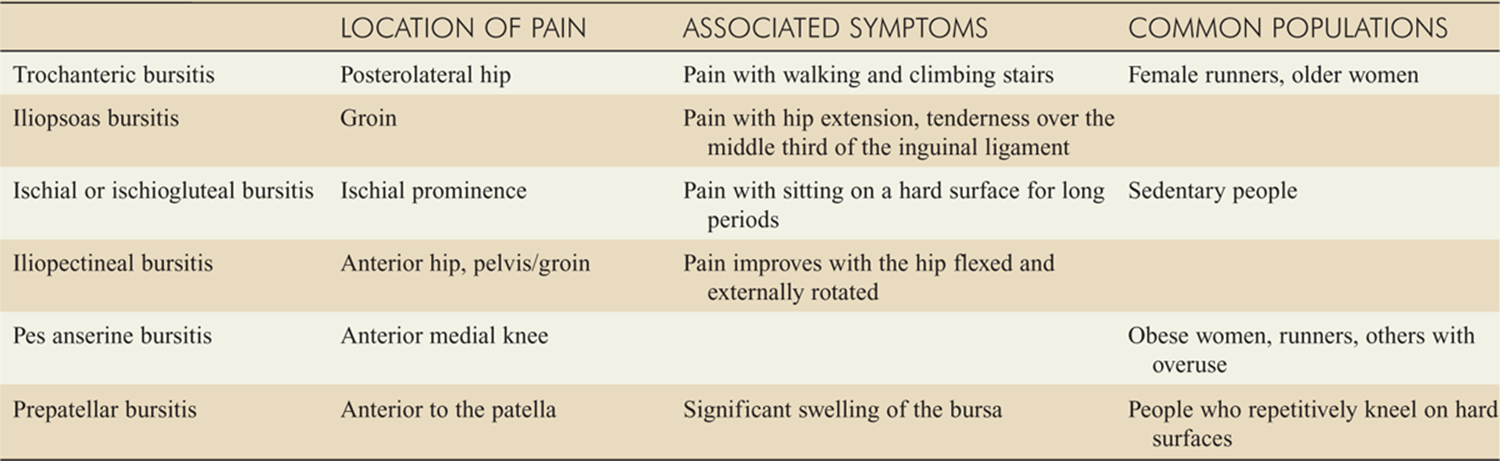
![]() Table 181-2 describes characteristics of the bursal syndromes.
Table 181-2 describes characteristics of the bursal syndromes.
TABLE 181-2 Characteristics of Bursal Syndromes of the Hip and Knee
![]() Figure 181-1 shows bursal swelling of the left knee.
Figure 181-1 shows bursal swelling of the left knee.

FIG. 181-1. Prepatellar bursitis of the left knee. (Reproduced with permission from Knoop K, Stack L, Storrow A, Thurman RJ: Atlas of Emergency Medicine, 3rd ed. © 2010, McGraw-Hill, New York.)
![]() Treatment is directed at the underlying cause.
Treatment is directed at the underlying cause.
![]() NSAIDs, rest, heat, and time are the basis of treatment for inflammatory conditions.
NSAIDs, rest, heat, and time are the basis of treatment for inflammatory conditions.
![]() Steroid injections into readily accessible bursa may be useful, but only if infection has been definitively excluded.
Steroid injections into readily accessible bursa may be useful, but only if infection has been definitively excluded.
![]() Care should be taken to avoid injecting steroids into tendons.
Care should be taken to avoid injecting steroids into tendons.
![]() Infections should be treated with antibiotics.
Infections should be treated with antibiotics.
![]() Immunocompromised patients with suspected infections should be admitted for IV antibiotics and orthopedic surgery consultation.
Immunocompromised patients with suspected infections should be admitted for IV antibiotics and orthopedic surgery consultation.
MYOFASCIAL SYNDROMES/OVERUSE SYNDROMES
![]() Overuse syndromes are caused by repetitive micro- trauma that outpaces the body’s ability to heal.
Overuse syndromes are caused by repetitive micro- trauma that outpaces the body’s ability to heal.
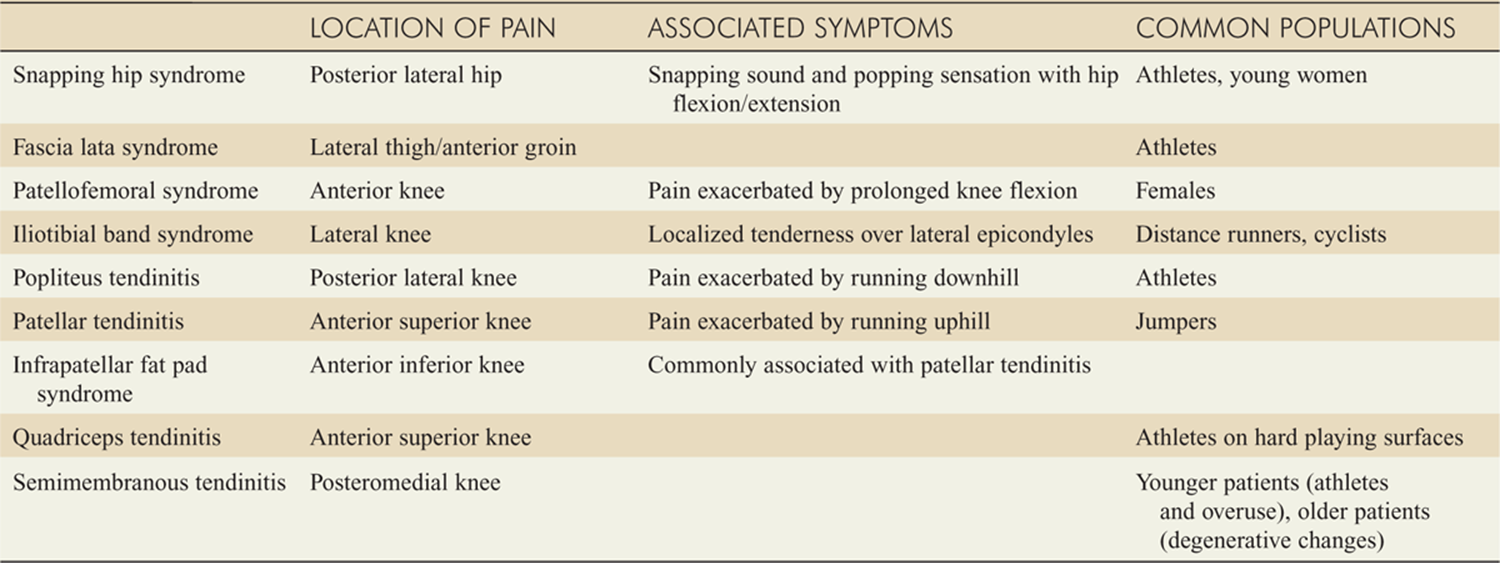
![]() Table 181-3 describes characteristics of various overuse syndromes.
Table 181-3 describes characteristics of various overuse syndromes.
![]() Treatment includes NSAIDs, heat, and rest, followed by gradual resumption of activities, physical therapy, and strengthening where appropriate.
Treatment includes NSAIDs, heat, and rest, followed by gradual resumption of activities, physical therapy, and strengthening where appropriate.
TABLE 181-3 Characteristics of Myofascial/Overuse Syndromes
BONE/ARTICULAR DERANGEMENTS
OSTEONECROSIS/AVASCULAR NECROSIS
![]() Bone infarction caused by a lack of blood supply may be an idiopathic or primary disorder, secondary to a systemic condition, or following trauma.
Bone infarction caused by a lack of blood supply may be an idiopathic or primary disorder, secondary to a systemic condition, or following trauma.
![]() Osteonecrosis may cause pain from the buttock to the knee.
Osteonecrosis may cause pain from the buttock to the knee.
![]() Plain radiographs may establish the diagnosis, but CT or MRI is more helpful early in the disease process.
Plain radiographs may establish the diagnosis, but CT or MRI is more helpful early in the disease process.
![]() Traumatic causes of avascular necrosis of the femoral head include femoral neck fracture, hip dislocation, and occult or minor trauma.
Traumatic causes of avascular necrosis of the femoral head include femoral neck fracture, hip dislocation, and occult or minor trauma.
![]() Nontraumatic necrosis may be idiopathic; other causes include sickle-cell disease, collagen vascular diseases, alcohol abuse, renal transplant, systemic lupus ery-thematosus, dysbarism, chronic pancreatitis, exogenous steroid administration, Cushing disease, caisson disease, Gaucher disease, and renal osteodystrophy
Nontraumatic necrosis may be idiopathic; other causes include sickle-cell disease, collagen vascular diseases, alcohol abuse, renal transplant, systemic lupus ery-thematosus, dysbarism, chronic pancreatitis, exogenous steroid administration, Cushing disease, caisson disease, Gaucher disease, and renal osteodystrophy
OSTEOMYELITIS
![]() Bony destruction is caused by bacterial or fungal infection.
Bony destruction is caused by bacterial or fungal infection.
![]() The infection comes from contiguous structures in about 80% of cases; hematogenous spread is responsible for the remainder of cases.
The infection comes from contiguous structures in about 80% of cases; hematogenous spread is responsible for the remainder of cases.
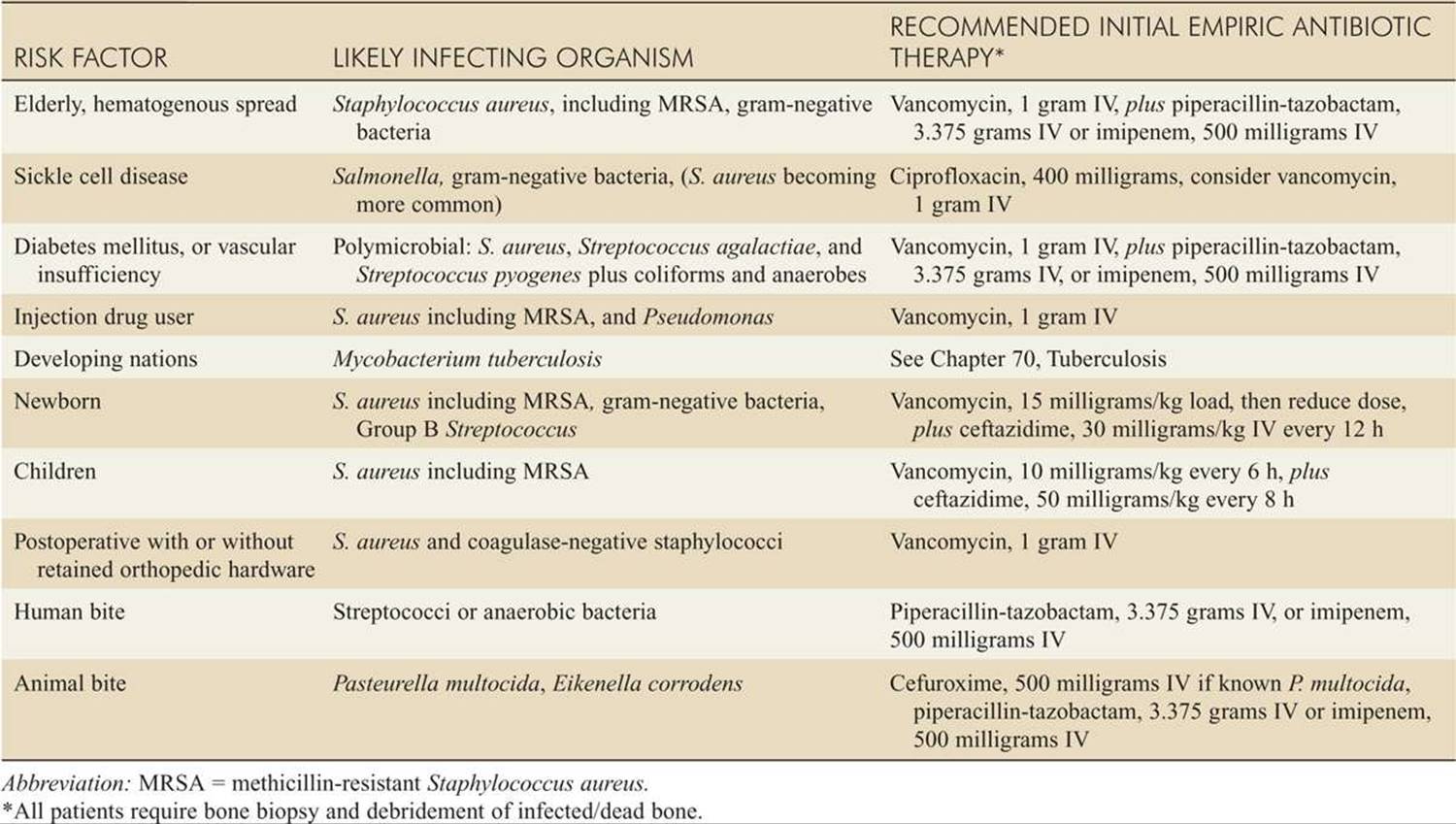
![]() See Table 181-4 for risk factors, likely organisms, and empiric treatments.
See Table 181-4 for risk factors, likely organisms, and empiric treatments.
PAGET DISEASE
![]() Paget disease, or osteitis deformans, is a familial disorder resulting in enlarged, deformed bones due to overactive breakdown and reformation.
Paget disease, or osteitis deformans, is a familial disorder resulting in enlarged, deformed bones due to overactive breakdown and reformation.
![]() The hip joint is affected in 50% of patients.
The hip joint is affected in 50% of patients.
![]() ED treatment is symptomatic.
ED treatment is symptomatic.
![]() Surgery may be required for complications.
Surgery may be required for complications.
![]() Long-term medications to reduce the rate of bone turnover (eg, calcitonin and alendronate) may help control the disease.
Long-term medications to reduce the rate of bone turnover (eg, calcitonin and alendronate) may help control the disease.
OSTEITIS PUBIS
![]() Osteitis pubis occurs following pregnancy, in athletes due to overuse of the adductors and gracilis muscles, and after bladder and prostate surgery.
Osteitis pubis occurs following pregnancy, in athletes due to overuse of the adductors and gracilis muscles, and after bladder and prostate surgery.
![]() Pain in the region of the pubis starts gradually and may become very severe, causing a characteristic “duck waddling gait.”
Pain in the region of the pubis starts gradually and may become very severe, causing a characteristic “duck waddling gait.”
![]() Symptoms may resolve over several months with rest and NSAIDs.
Symptoms may resolve over several months with rest and NSAIDs.
MYOSITIS OSSIFICANS
![]() Myositis ossificans or heterotopic calcification is the post-traumatic deposition of bone in abnormal sites.
Myositis ossificans or heterotopic calcification is the post-traumatic deposition of bone in abnormal sites.
![]() Symptoms include pain and a palpable mass, which may limit motion.
Symptoms include pain and a palpable mass, which may limit motion.
![]() Plain radiographs show an irregularly shaped mass near a joint or in a fascial plane.
Plain radiographs show an irregularly shaped mass near a joint or in a fascial plane.
TABLE 181-4 Risk Factors, Likely Infecting Organism, and Recommended Initial Empiric Antibiotic Therapy for Osteomyelitis
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 278, “Hip and Knee Pain,” by Kelly R O’Keefe and Tracy G. Sanson.