Mark X. Cicero
PATHOPHYSIOLOGY
![]() The long bones of children are generally less dense and more porous than the long bones of adults. The resulting increased compliance contributes to the tendency of children’s long bones to respond to mechanical stress by bowing and buckling, rather than fracturing through and through.
The long bones of children are generally less dense and more porous than the long bones of adults. The resulting increased compliance contributes to the tendency of children’s long bones to respond to mechanical stress by bowing and buckling, rather than fracturing through and through.
![]() The periosteum of the diaphysis and the metaphysis is thicker in children and is continuous from the metaphysis to the epiphysis, surrounding and protecting the mechanically weaker physis.
The periosteum of the diaphysis and the metaphysis is thicker in children and is continuous from the metaphysis to the epiphysis, surrounding and protecting the mechanically weaker physis.
![]() The blood supply to the physis arises from the epiphysis, so separation of the physis from the epiphysis may be disastrous for future growth.
The blood supply to the physis arises from the epiphysis, so separation of the physis from the epiphysis may be disastrous for future growth.
![]() The ligaments of children are stronger and more compliant than those of adults, and sprains are less common than fractures in young children.
The ligaments of children are stronger and more compliant than those of adults, and sprains are less common than fractures in young children.
CHILDHOOD PATTERNS OF INJURY
![]() The growth plate (physis) is the weakest point in children’s long bones and the frequent site of fractures. The ligaments and periosteum are stronger than the physis, tolerating mechanical forces at the expense of physeal injury.
The growth plate (physis) is the weakest point in children’s long bones and the frequent site of fractures. The ligaments and periosteum are stronger than the physis, tolerating mechanical forces at the expense of physeal injury.
![]() The Salter–Harris classification is widely used to describe fractures involving the growth plate.
The Salter–Harris classification is widely used to describe fractures involving the growth plate.
TYPE I PHYSEAL FRACTURE
![]() Type I physeal fractures involve injury through the growth plate alone: the epiphysis separates from the metaphysis. The reproductive cells of the physis stay with the epiphysis. There are no bony fragments. Bone growth is undisturbed.
Type I physeal fractures involve injury through the growth plate alone: the epiphysis separates from the metaphysis. The reproductive cells of the physis stay with the epiphysis. There are no bony fragments. Bone growth is undisturbed.
![]() Diagnosis of this injury is suspected clinically in children with point tenderness over a growth plate. On radiograph, the only abnormality may be an associated joint effusion. There may be epiphyseal displacement from the metaphysis.
Diagnosis of this injury is suspected clinically in children with point tenderness over a growth plate. On radiograph, the only abnormality may be an associated joint effusion. There may be epiphyseal displacement from the metaphysis.
![]() Treatment consists of splint immobilization, ice, and elevation. Type I fractures of the distal fibula and radius are common, benign, and do not require orthopedic referral.
Treatment consists of splint immobilization, ice, and elevation. Type I fractures of the distal fibula and radius are common, benign, and do not require orthopedic referral.
TYPE II PHYSEAL FRACTURE
![]() Type II physeal fracture is the most common (75%) physeal fracture.
Type II physeal fracture is the most common (75%) physeal fracture.
![]() The fracture extends through the physis and metaphysis (Fig. 84-1). The periosteum remains intact over the metaphyseal fragment, but is torn on the opposite side. Growth is preserved since the physis remains with the epiphysis.
The fracture extends through the physis and metaphysis (Fig. 84-1). The periosteum remains intact over the metaphyseal fragment, but is torn on the opposite side. Growth is preserved since the physis remains with the epiphysis.
![]() Treatment is closed reduction with analgesia and sedation followed by cast immobilization.
Treatment is closed reduction with analgesia and sedation followed by cast immobilization.

FIG. 84-1. Salter–Harris type II fracture of distal tibia. CT image illustrating fracture extending through physeal growth plate and metaphysis (arrow). (Courtesy of Wake Medical Center, Raleigh, NC)
TYPE III PHYSEAL FRACTURE
![]() The hallmark of type III physeal fracture is an intraarticular fracture of the epiphysis with the cleavage plane continuing along the physis. This injury usually involves the proximal or distal tibia (Fig. 84-2).
The hallmark of type III physeal fracture is an intraarticular fracture of the epiphysis with the cleavage plane continuing along the physis. This injury usually involves the proximal or distal tibia (Fig. 84-2).
![]() The prognosis for bone growth depends on the circulation to the epiphyseal bone fragment and is usually favorable.
The prognosis for bone growth depends on the circulation to the epiphyseal bone fragment and is usually favorable.
![]() Reduction of the unstable fragment with anatomic alignment of the articular surface is critical. Open reduction is often required.
Reduction of the unstable fragment with anatomic alignment of the articular surface is critical. Open reduction is often required.
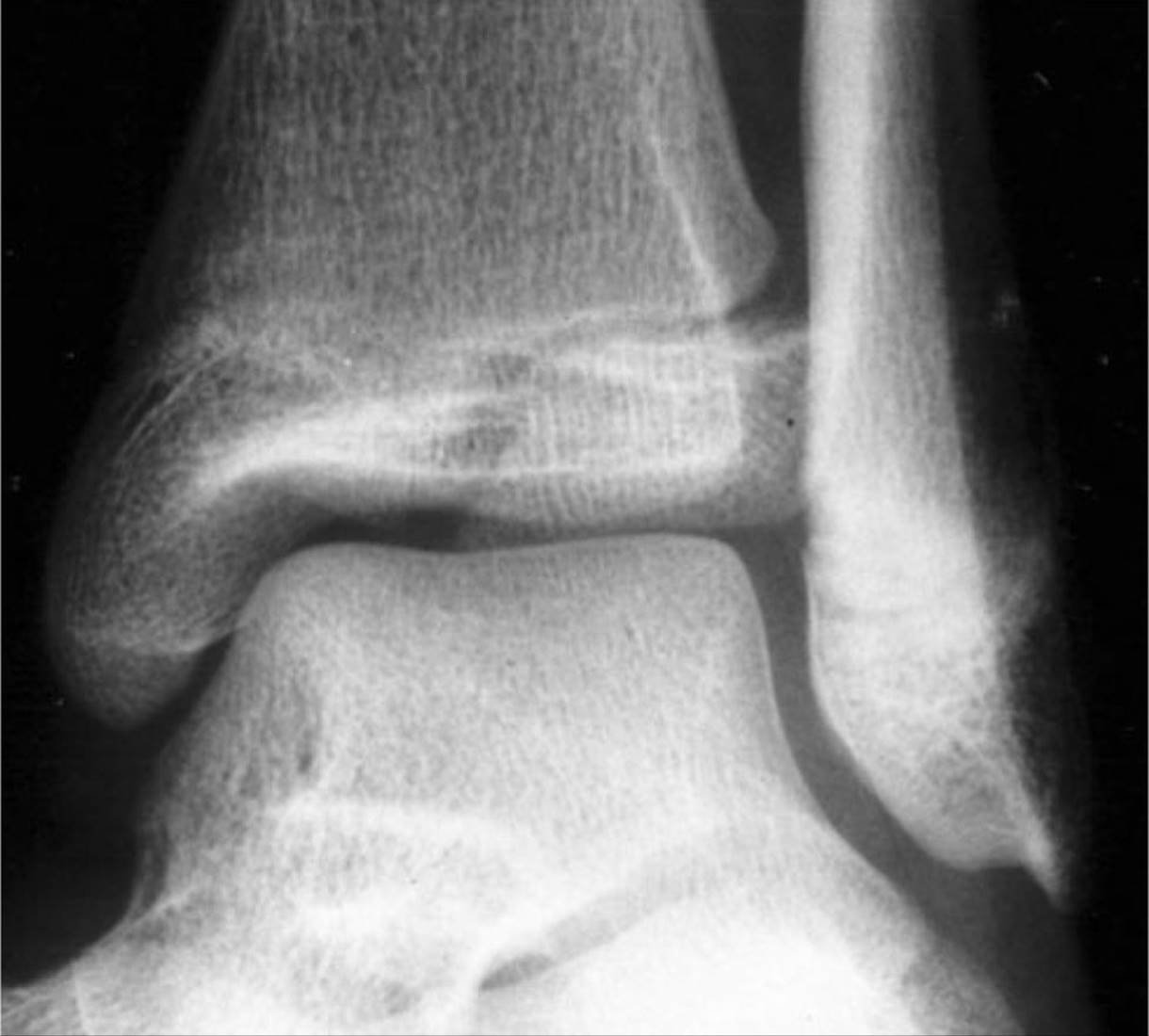
FIG. 84-2. A radiograph of a Salter–Harris type III fracture of the lateral portion of the distal tibia. Note the intra-articular component extending through the growth plate and the medial epiphysis of the tibia. (Reproduced with permission from Shah BR, Lucchesi M: Atlas of Pediatric Emergency Medicine, © 2006, McGraw-Hill, New York.)
TYPE IV PHYSEAL FRACTURE
![]() The fracture line of type IV physeal fractures begins at the articular surface and extends through the epiphysis, physis, and metaphysis (Fig. 84-3).
The fracture line of type IV physeal fractures begins at the articular surface and extends through the epiphysis, physis, and metaphysis (Fig. 84-3).
![]() This most often involves the distal humerus.
This most often involves the distal humerus.
![]() Open reduction is required to reduce the risk of premature bone growth arrest.
Open reduction is required to reduce the risk of premature bone growth arrest.

FIG. 84-3. Radiograph of a Salter–Harris type IV fracture of the medial malleolus. (Reproduced with permission from Shah BR, Lucchesi M: Atlas of Pediatric Emergency Medicine, © 2006, McGraw-Hill, New York.)
TYPE V PHYSEAL FRACTURE
![]() Type V physeal fracture is rare and usually involves the knee or ankle. The physis is crushed by severe compressive forces. There is no epiphyseal displacement.
Type V physeal fracture is rare and usually involves the knee or ankle. The physis is crushed by severe compressive forces. There is no epiphyseal displacement.
![]() The diagnosis is often difficult: initial diagnosis of sprain or type I injury may prove incorrect when later growth arrest occurs. Radiographs may look normal or demonstrate focal narrowing of the epiphyseal plate. There is usually an associated joint effusion.
The diagnosis is often difficult: initial diagnosis of sprain or type I injury may prove incorrect when later growth arrest occurs. Radiographs may look normal or demonstrate focal narrowing of the epiphyseal plate. There is usually an associated joint effusion.
![]() Treatment consists of cast immobilization, non-weight bearing, and close orthopedic follow-up in anticipation of focal bone growth arrest.
Treatment consists of cast immobilization, non-weight bearing, and close orthopedic follow-up in anticipation of focal bone growth arrest.
TORUS FRACTURES
![]() Children’s long bones are more compliant than those of adults and tend to bow and bend under forces where an adult’s might fracture. Torus (also called cortical or buckle) fractures involve a bulging or buckling of the bony cortex, usually at the metaphysis.
Children’s long bones are more compliant than those of adults and tend to bow and bend under forces where an adult’s might fracture. Torus (also called cortical or buckle) fractures involve a bulging or buckling of the bony cortex, usually at the metaphysis.
![]() Patients have soft tissue swelling and point tenderness over the fracture site. Radiographs may be subtle but show cortical disruption.
Patients have soft tissue swelling and point tenderness over the fracture site. Radiographs may be subtle but show cortical disruption.
![]() Torus fractures are not typically angulated, rotated, or displaced, so reduction is rarely necessary. Splinting or casting in a position of function for 3 to 4 weeks with orthopedic follow-up is recommended.
Torus fractures are not typically angulated, rotated, or displaced, so reduction is rarely necessary. Splinting or casting in a position of function for 3 to 4 weeks with orthopedic follow-up is recommended.
GREENSTICK FRACTURES
![]() In greenstick fracture, the cortex and periosteum are disrupted on one side of the bone, but intact on the other.
In greenstick fracture, the cortex and periosteum are disrupted on one side of the bone, but intact on the other.
![]() Treatment is closed reduction and immobilization.
Treatment is closed reduction and immobilization.
PLASTIC DEFORMITIES
![]() Plastic deformities are seen in the forearm and lower leg in combination with a completed fracture in the companion bone. The diaphyseal cortex is deformed, but the periosteum is intact.
Plastic deformities are seen in the forearm and lower leg in combination with a completed fracture in the companion bone. The diaphyseal cortex is deformed, but the periosteum is intact.
![]() Prompt orthopedic consultation is required for any plastic deformities, as proper reduction and realignment is essential.
Prompt orthopedic consultation is required for any plastic deformities, as proper reduction and realignment is essential.
FRACTURES ASSOCIATED WITH CHILD ABUSE
See Chapter 189, “Child and Elder Abuse.”
SELECTED PEDIATRIC INJURIES
CLAVICLE FRACTURE
![]() A clavicle fracture is the most common fracture in children.
A clavicle fracture is the most common fracture in children.
![]() Fractures may occur in the newborn during a difficult delivery. Neonates may demonstrate nonuse of the arm. If the fracture was not initially appreciated, parents may notice a bony callus at 2 to 3 weeks of age.
Fractures may occur in the newborn during a difficult delivery. Neonates may demonstrate nonuse of the arm. If the fracture was not initially appreciated, parents may notice a bony callus at 2 to 3 weeks of age.
![]() In older infants and children, the usual mechanism is a fall onto the outstretched arm or shoulder.
In older infants and children, the usual mechanism is a fall onto the outstretched arm or shoulder.
![]() Care of the patient with a clavicle fracture is directed toward pain control. Even if anatomic alignment is not achieved in the emergency department (ED), displaced fractures usually heal well, although there may be a residual bump at the fracture site.
Care of the patient with a clavicle fracture is directed toward pain control. Even if anatomic alignment is not achieved in the emergency department (ED), displaced fractures usually heal well, although there may be a residual bump at the fracture site.
![]() Figure-of-eight shoulder abduction restraints have been the traditional treatment, but many patients have more pain with this device. A simple sling or shoulder immobilizer are equally effective and less painful. Orthopedic follow-up can be arranged in the next week.
Figure-of-eight shoulder abduction restraints have been the traditional treatment, but many patients have more pain with this device. A simple sling or shoulder immobilizer are equally effective and less painful. Orthopedic follow-up can be arranged in the next week.
![]() Orthopedic consultation in the ED is required for an open fracture (which also requires antibiotics), anterior or posterior displacement of the medial clavicle, or a skin-tenting fracture fragment that has the potential to convert to an open fracture.
Orthopedic consultation in the ED is required for an open fracture (which also requires antibiotics), anterior or posterior displacement of the medial clavicle, or a skin-tenting fracture fragment that has the potential to convert to an open fracture.
SUPRACONDYLAR FRACTURES
![]() The most common elbow fracture in children is a supracondylar fracture of the distal humerus. The usual mechanism is a fall on an outstretched arm.
The most common elbow fracture in children is a supracondylar fracture of the distal humerus. The usual mechanism is a fall on an outstretched arm.
![]() The close proximity of the brachial artery to the fracture predisposes the arterial injury. Subsequent arterial spasm or compression by casts may further compromise distal circulation. Forearm compartment syndrome, known as Volkmann’s ischemic contracture, may occur.
The close proximity of the brachial artery to the fracture predisposes the arterial injury. Subsequent arterial spasm or compression by casts may further compromise distal circulation. Forearm compartment syndrome, known as Volkmann’s ischemic contracture, may occur.
![]() Symptoms include pain in the proximal forearm upon passive finger extension, stocking-glove anesthesia of the hand, and hard forearm swelling. Children complain of pain on passive elbow flexion and maintain the forearm pronated.
Symptoms include pain in the proximal forearm upon passive finger extension, stocking-glove anesthesia of the hand, and hard forearm swelling. Children complain of pain on passive elbow flexion and maintain the forearm pronated.
![]() Pulses may remain palpable at the wrist despite serious vascular impairment.
Pulses may remain palpable at the wrist despite serious vascular impairment.
![]() Injuries to the ulnar, median, and radial nerves are common too, occurring in 5% to 10% of all supracondylar fractures.
Injuries to the ulnar, median, and radial nerves are common too, occurring in 5% to 10% of all supracondylar fractures.
![]() Radiographs show the injury, but the findings may be subtle. A posterior fat pad sign is indicative of intra-articular effusion and thus fracture. The anterior humeral line should be assessed (Fig. 84-4). In subtle supracondylar fractures, the line often lies more anteriorly.
Radiographs show the injury, but the findings may be subtle. A posterior fat pad sign is indicative of intra-articular effusion and thus fracture. The anterior humeral line should be assessed (Fig. 84-4). In subtle supracondylar fractures, the line often lies more anteriorly.
![]() Supracondylar fractures are often classified as types I-III: type I fractures are subtle and may only be detected on radiograph through a fat-pad sign (Fig. 84-5); type II fractures reveal angulation but the posterior cortex is usually displaced; type III fractures disrupt both cortices with displacement of the distal fracture fragment.
Supracondylar fractures are often classified as types I-III: type I fractures are subtle and may only be detected on radiograph through a fat-pad sign (Fig. 84-5); type II fractures reveal angulation but the posterior cortex is usually displaced; type III fractures disrupt both cortices with displacement of the distal fracture fragment.
![]() In cases of neurovascular compromise, immediate fracture reduction is indicated. If an ischemic forearm compartment is suspected after reduction, surgical decompression or arterial exploration may be indicated.
In cases of neurovascular compromise, immediate fracture reduction is indicated. If an ischemic forearm compartment is suspected after reduction, surgical decompression or arterial exploration may be indicated.
![]() Type I supracondylar fractures can usually be splinted (posterior long-arm splint with the elbow at 90 degrees flexion and the wrist in neutral position, or a double sugar-tong splint) and referred for outpatient follow-up.
Type I supracondylar fractures can usually be splinted (posterior long-arm splint with the elbow at 90 degrees flexion and the wrist in neutral position, or a double sugar-tong splint) and referred for outpatient follow-up.
![]() Types II and III supracondylar fractures typically require surgical pinning.
Types II and III supracondylar fractures typically require surgical pinning.
![]() Admission is recommended for patients with displaced fractures or significant soft tissue swelling. Open reduction is often required.
Admission is recommended for patients with displaced fractures or significant soft tissue swelling. Open reduction is often required.
![]() Lateral and medial condylar fractures and intercondylar and transcondylar fractures carry risks of neurovascular compromise, especially to the ulnar nerve. These patients have soft tissue swelling and tenderness, maintaining the arm in flexion. Most patients require open reduction.
Lateral and medial condylar fractures and intercondylar and transcondylar fractures carry risks of neurovascular compromise, especially to the ulnar nerve. These patients have soft tissue swelling and tenderness, maintaining the arm in flexion. Most patients require open reduction.

FIG. 84-4. Anterior humeral line. A line drawn along the anterior cortex of the humeral shaft normally intersects the middle third of the capitellum. A normal radiographic teardrop is seen where the cortices of the olecranon and coronoid fossae come together (black arrow). A small normal anterior fat pad is visible (arrowhead). (Reproduced with permission from Schwartz D: Emergency Radiology Case Studies, ©2008, McGraw-Hill, New York.)

FIG. 84-5. Type I supracondylar fracture: Note the anterior and posterior fat pad signs suggestive of fracture without displacement of the distal fragment.
RADIAL HEAD SUBLUXATION (“NURSEMAID’S ELBOW”)
![]() Radial head subluxation is a very common injury that is seen most often in children between the ages of 1 and 4 years. The typical history is that the child was lifted up by an adult pulling on the hand or wrist. Sometimes there is a history of trauma, and sometimes there is no memorable event at all, but the child refuses to use the arm.
Radial head subluxation is a very common injury that is seen most often in children between the ages of 1 and 4 years. The typical history is that the child was lifted up by an adult pulling on the hand or wrist. Sometimes there is a history of trauma, and sometimes there is no memorable event at all, but the child refuses to use the arm.
![]() The arm is held close to the body, flexed at the elbow with the forearm pronated. Gentle examination reveals no tenderness to direct palpation, but any attempts to supinate the forearm or move the elbow cause pain.
The arm is held close to the body, flexed at the elbow with the forearm pronated. Gentle examination reveals no tenderness to direct palpation, but any attempts to supinate the forearm or move the elbow cause pain.
![]() If the history and examination are classic, radiographs are not needed, but if the history is atypical or there is point tenderness or signs of trauma, radiographs should be obtained.
If the history and examination are classic, radiographs are not needed, but if the history is atypical or there is point tenderness or signs of trauma, radiographs should be obtained.
![]() There are two maneuvers for reduction. The supination-flexion technique (Fig. 84-6) is performed by holding the patient’s elbow at 90 degrees with one hand, then firmly supinating the wrist and simultaneously flexing the elbow so the wrist is directed to the ipsilateral shoulder. There may be a “click” with reduction and the child may transiently cry and resist.
There are two maneuvers for reduction. The supination-flexion technique (Fig. 84-6) is performed by holding the patient’s elbow at 90 degrees with one hand, then firmly supinating the wrist and simultaneously flexing the elbow so the wrist is directed to the ipsilateral shoulder. There may be a “click” with reduction and the child may transiently cry and resist.
![]() The hyperpronation technique (Fig. 84-7) is reported to be more successful, less painful, and can be used primarily, or as a back-up if supination fails. The hyperpronation technique is performed by holding the child’s elbow at 90 degrees or in full extension in one hand, then firmly pronating the wrist. Usually the child will resume normal activity in 15 to 30 minutes if reduction is achieved. If the child is not better after a second reduction attempt, alternate diagnoses and radiographs should be considered. No specific therapy is needed after successful reduction. Parents should be reminded to avoid linear traction on the arm, as there is an increased risk of recurrence.
The hyperpronation technique (Fig. 84-7) is reported to be more successful, less painful, and can be used primarily, or as a back-up if supination fails. The hyperpronation technique is performed by holding the child’s elbow at 90 degrees or in full extension in one hand, then firmly pronating the wrist. Usually the child will resume normal activity in 15 to 30 minutes if reduction is achieved. If the child is not better after a second reduction attempt, alternate diagnoses and radiographs should be considered. No specific therapy is needed after successful reduction. Parents should be reminded to avoid linear traction on the arm, as there is an increased risk of recurrence.
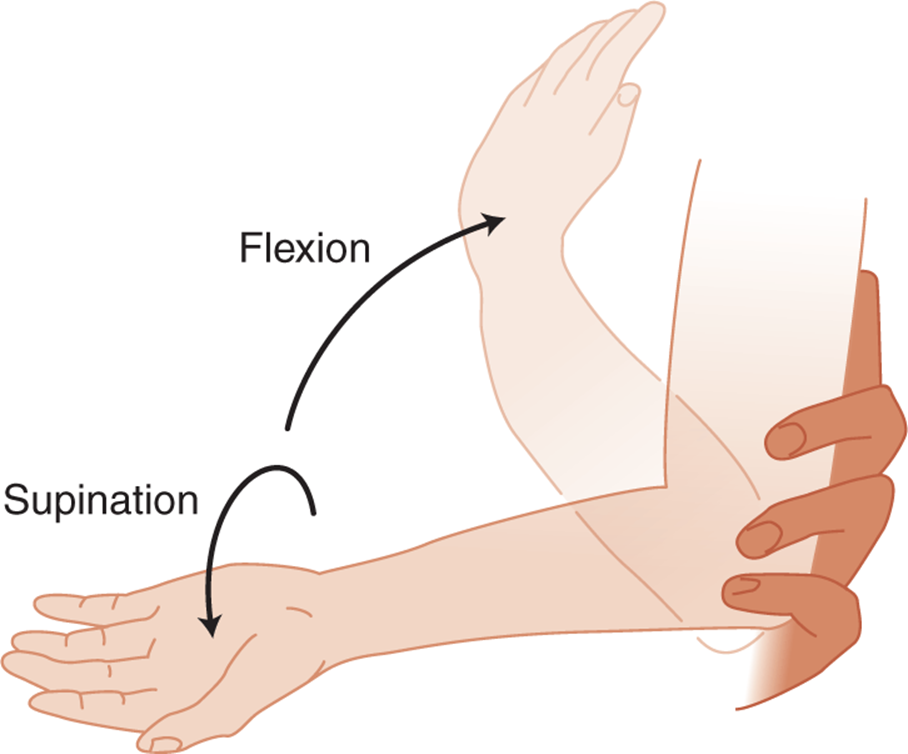
FIG. 84-6. Supination-flexion technique. Hold the elbow at 90 degrees; then firmly supinate the wrist and the forearm toward the ipsilateral shoulder.
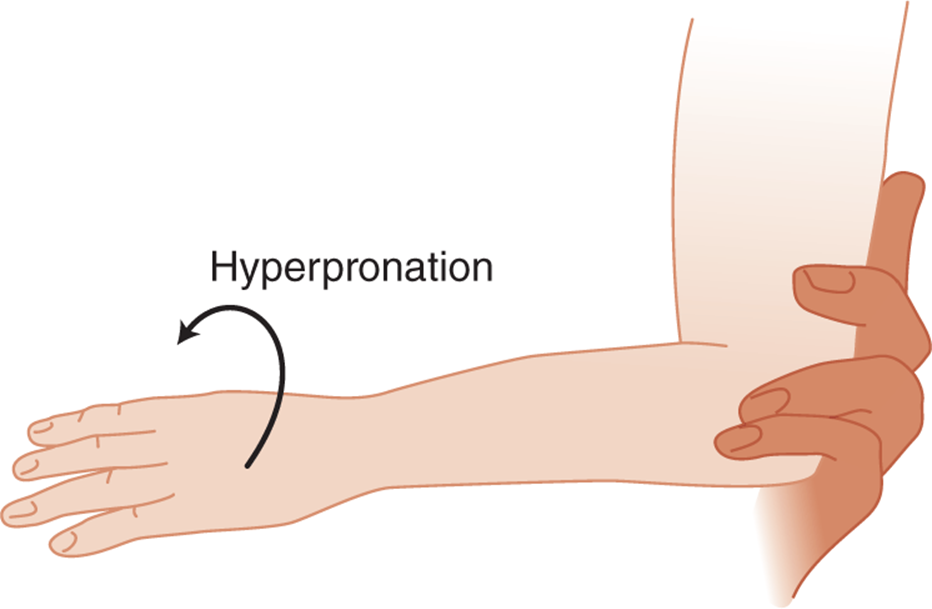
FIG. 84-7. Hyperpronation. Hold the elbow at 90 degrees; then firmly pronate the wrist.
SLIPPED CAPITAL FEMORAL EPIPHYSIS
![]() Slipped capital femoral epiphysis (SCFE) is more common in boys, with peak incidence between ages 12 and 15 years, and in girls between ages 10 and 13 years.
Slipped capital femoral epiphysis (SCFE) is more common in boys, with peak incidence between ages 12 and 15 years, and in girls between ages 10 and 13 years.
![]() With a chronic SCFE, children complain of dull pain in the groin, anteromedial thigh, or knee, which becomes worse with activity. With walking, the leg is externally rotated and the gait is antalgic. Hip flexion and rotation are restricted and painful.
With a chronic SCFE, children complain of dull pain in the groin, anteromedial thigh, or knee, which becomes worse with activity. With walking, the leg is externally rotated and the gait is antalgic. Hip flexion and rotation are restricted and painful.
![]() Acute presentation of SCFE is usually due to trauma or may occur in a patient with preexisting chronic SCFE. Patients present in great pain, with marked external rotation of the thigh and leg shortening. The hip should not be forced through full range of motion, as this may displace the epiphysis further.
Acute presentation of SCFE is usually due to trauma or may occur in a patient with preexisting chronic SCFE. Patients present in great pain, with marked external rotation of the thigh and leg shortening. The hip should not be forced through full range of motion, as this may displace the epiphysis further.
![]() The differential includes septic arthritis, toxic synovitis, Legg–Calvé–Perthes’ disease, and other hip fractures.
The differential includes septic arthritis, toxic synovitis, Legg–Calvé–Perthes’ disease, and other hip fractures.
![]() Children with SCFE are not febrile or toxic and have normal white blood cell counts (WBCs) and erythrocyte sedimentation rates (ESRs) which are not needed unless the patient is febrile.
Children with SCFE are not febrile or toxic and have normal white blood cell counts (WBCs) and erythrocyte sedimentation rates (ESRs) which are not needed unless the patient is febrile.
![]() On radiograph, medial displacement of the femoral epiphysis will be seen on anteroposterior (AP) views, while frog-leg views detect posterior displacement. In the AP view, a line along the superior femoral neck should transect the lateral quarter of the femoral epiphysis in normal children.
On radiograph, medial displacement of the femoral epiphysis will be seen on anteroposterior (AP) views, while frog-leg views detect posterior displacement. In the AP view, a line along the superior femoral neck should transect the lateral quarter of the femoral epiphysis in normal children.
![]() Management of SCFE is operative. Patients should be made non-weight bearing and NPO and admitted to the hospital. The main long-term complication is avascular necrosis of the femoral head.
Management of SCFE is operative. Patients should be made non-weight bearing and NPO and admitted to the hospital. The main long-term complication is avascular necrosis of the femoral head.
SELECTED NONTRAUMATIC MUSCULOSKELETAL DISORDERS OF CHILDHOOD
![]() Kawasaki’s disease is discussed in Chapter 84.
Kawasaki’s disease is discussed in Chapter 84.
![]() Acute supperative arthritis is discussed in Chapter 180.
Acute supperative arthritis is discussed in Chapter 180.
JUVENILE IMMUNE ARTHRITIS
![]() The group of diseases comprising juvenile immune arthritis (JIA; formerly juvenile rheumatoid arthritis) share the findings of chronic noninfectious synovitis and arthritis, with varying systemic manifestations.
The group of diseases comprising juvenile immune arthritis (JIA; formerly juvenile rheumatoid arthritis) share the findings of chronic noninfectious synovitis and arthritis, with varying systemic manifestations.
![]() Pauciarticular disease is the most common form, usually involving a single large joint such as the knee. Permanent joint damage occurs infrequently.
Pauciarticular disease is the most common form, usually involving a single large joint such as the knee. Permanent joint damage occurs infrequently.
![]() Polyarticular disease occurs in one-third of cases; both large and small joints are affected, and there may be progressive joint damage.
Polyarticular disease occurs in one-third of cases; both large and small joints are affected, and there may be progressive joint damage.
![]() Systemic JIA occurs in 20% of patients. This form is associated with high fevers and chills. Extraarticular manifestations are common, including a red macular coalescent rash, hepatosplenomegaly, and serositis.
Systemic JIA occurs in 20% of patients. This form is associated with high fevers and chills. Extraarticular manifestations are common, including a red macular coalescent rash, hepatosplenomegaly, and serositis.
![]() The diagnosis of JIA will likely not be made in the ED, as it requires 6 weeks of persistent joint swelling. Lab tests focus mostly on excluding other diagnoses. Complete blood count (CBC), ESR, and C-reactive protein (CRP) may be normal. Arthrocentesis may be necessary to exclude septic arthritis, particularly in pauciarticular disease.
The diagnosis of JIA will likely not be made in the ED, as it requires 6 weeks of persistent joint swelling. Lab tests focus mostly on excluding other diagnoses. Complete blood count (CBC), ESR, and C-reactive protein (CRP) may be normal. Arthrocentesis may be necessary to exclude septic arthritis, particularly in pauciarticular disease.
![]() Radiographs initially show joint effusions but are nonspecific.
Radiographs initially show joint effusions but are nonspecific.
![]() Initial therapy for patients with an established diagnosis includes nonsteroidal anti-inflammatory drugs (NSAIDs). Glucocorticoids are occasionally used, for example, for unresponsive uveitis or decompensated pericarditis or myocarditis. Systemic immunosuppressents are often prescribed by rheumatologists for severe disease.
Initial therapy for patients with an established diagnosis includes nonsteroidal anti-inflammatory drugs (NSAIDs). Glucocorticoids are occasionally used, for example, for unresponsive uveitis or decompensated pericarditis or myocarditis. Systemic immunosuppressents are often prescribed by rheumatologists for severe disease.
LEGG-CALVÉ-PERTHES’ DISEASE
![]() Legg-Calvé-Perthes’ disease is avascular necrosis of the femoral head with subchondral stress fracture. Collapse and flattening of the femoral head ensues, with potential subluxation.
Legg-Calvé-Perthes’ disease is avascular necrosis of the femoral head with subchondral stress fracture. Collapse and flattening of the femoral head ensues, with potential subluxation.
![]() The hip is painful with limited range of motion, muscle spasm, and soft tissue contractures. Onset of symptoms occurs between 4 and 9 years of age, with boys outnumbering girls 4:1. The disease is bilateral in 10% of patients. Children present with limp and chronic dull pain in the groin, thigh, or knee, which becomes worse with activity. Systemic symptoms are absent.
The hip is painful with limited range of motion, muscle spasm, and soft tissue contractures. Onset of symptoms occurs between 4 and 9 years of age, with boys outnumbering girls 4:1. The disease is bilateral in 10% of patients. Children present with limp and chronic dull pain in the groin, thigh, or knee, which becomes worse with activity. Systemic symptoms are absent.
![]() Hip motion is restricted; there may be a flexion-abduction contracture and thigh muscle atrophy.
Hip motion is restricted; there may be a flexion-abduction contracture and thigh muscle atrophy.
![]() Initial radiographs (in the first 1–3 months) show widening of the cartilage space in the affected hip and diminished ossific nucleus of the femoral head. The second sign is subchondral stress fracture of the femoral head. The third finding is increased femoral head opacification. Finally, deformity of the femoral head occurs, with subluxation and protrusion of the femoral head from the acetabulum.
Initial radiographs (in the first 1–3 months) show widening of the cartilage space in the affected hip and diminished ossific nucleus of the femoral head. The second sign is subchondral stress fracture of the femoral head. The third finding is increased femoral head opacification. Finally, deformity of the femoral head occurs, with subluxation and protrusion of the femoral head from the acetabulum.
![]() Bone scan and magnetic resonance imaging are helpful in making this diagnosis, showing bone abnormalities well before plain films.
Bone scan and magnetic resonance imaging are helpful in making this diagnosis, showing bone abnormalities well before plain films.
![]() The differential diagnosis includes toxic tenosynovitis, tuberculous arthritis, tumors, and bone dyscrasias.
The differential diagnosis includes toxic tenosynovitis, tuberculous arthritis, tumors, and bone dyscrasias.
![]() In the ED, the most important thing is to consider this chronic but potentially crippling condition. Nearly all children are hospitalized initially for traction.
In the ED, the most important thing is to consider this chronic but potentially crippling condition. Nearly all children are hospitalized initially for traction.
OSGOOD-SCHLATTER DISEASE
![]() Osgood-Schlatter disease is a common apophysitis that affects preteen boys more than girls. Repetitive stress on the tibial tuberosity by the quadriceps muscle initiates inflammation of the tibial tuberosity, without necrosis.
Osgood-Schlatter disease is a common apophysitis that affects preteen boys more than girls. Repetitive stress on the tibial tuberosity by the quadriceps muscle initiates inflammation of the tibial tuberosity, without necrosis.
![]() Children present with pain and tenderness over the anterior knee, which becomes worse with flexion and better with rest.
Children present with pain and tenderness over the anterior knee, which becomes worse with flexion and better with rest.
![]() The patellar tendon is thick and tender, with the tibial tuberosity enlarged and inflammed.
The patellar tendon is thick and tender, with the tibial tuberosity enlarged and inflammed.
![]() Radiographs show soft-tissue swelling over the tuberosity and patellar tendon thickening without knee effusion. Normally, the ossification site at the tubercle at this age will be irregular, but the prominence of the tubercle is characteristic of Osgood-Schlatter disease.
Radiographs show soft-tissue swelling over the tuberosity and patellar tendon thickening without knee effusion. Normally, the ossification site at the tubercle at this age will be irregular, but the prominence of the tubercle is characteristic of Osgood-Schlatter disease.
![]() The disorder is self-limited. Acute symptoms improve after restriction of physical activities, ice, and NSAIDs. Crutches may be necessary, although a knee immobilizer or cylinder cast are rarely needed. Exercises to stretch taut and hypertrophicd quadriceps muscles are also helpful.
The disorder is self-limited. Acute symptoms improve after restriction of physical activities, ice, and NSAIDs. Crutches may be necessary, although a knee immobilizer or cylinder cast are rarely needed. Exercises to stretch taut and hypertrophicd quadriceps muscles are also helpful.
POST-STREPTOCOCCAL REACTIVE ARTHRITIS
![]() Because of increased group A β-hemolytic streptococcal infections, the incidence of post-streptococcal reactive arthritis (PSRA) is also increasing. PSRA is a sterile, inflammatory, nonmigratory mono- or oligoarthritis occurring in the setting of antecedent infection at a distant site with β-hemolytic streptococci and also Staphylococcus and Salmonella species.
Because of increased group A β-hemolytic streptococcal infections, the incidence of post-streptococcal reactive arthritis (PSRA) is also increasing. PSRA is a sterile, inflammatory, nonmigratory mono- or oligoarthritis occurring in the setting of antecedent infection at a distant site with β-hemolytic streptococci and also Staphylococcus and Salmonella species.
![]() Unlike acute rheumatic fever, PSRA is not associated with carditis, and in general is a milder illness. However, the arthritis in PSRA is more severe and prolonged compared to acute rheumatic fever, and may be resistant to NSAIDs.
Unlike acute rheumatic fever, PSRA is not associated with carditis, and in general is a milder illness. However, the arthritis in PSRA is more severe and prolonged compared to acute rheumatic fever, and may be resistant to NSAIDs.
![]() To establish the diagnosis of PSRA, antecedent infection with group A streptococci must be established, either with throat culture or a fourfold rise in antistreptolysin O (ASO) or anti-DNase B titer.
To establish the diagnosis of PSRA, antecedent infection with group A streptococci must be established, either with throat culture or a fourfold rise in antistreptolysin O (ASO) or anti-DNase B titer.
![]() PSRA is responsive to NSAIDs. The issue of penicillin prophylaxis, a mainstay of therapy in acute rheumatic fever, is controversial in PSRA. However, if group A Streptococcus is recovered from the throat, an acute course of treatment with penicillin or erythromycin should be instituted.
PSRA is responsive to NSAIDs. The issue of penicillin prophylaxis, a mainstay of therapy in acute rheumatic fever, is controversial in PSRA. However, if group A Streptococcus is recovered from the throat, an acute course of treatment with penicillin or erythromycin should be instituted.
ACUTE RHEUMATIC FEVER
![]() Acute rheumatic fever (ARF) is an acute inflammatory multisystem illness affecting primarily school-age children. It is not common in the United States, although occasional epidemics have been described and sporadic cases occur.
Acute rheumatic fever (ARF) is an acute inflammatory multisystem illness affecting primarily school-age children. It is not common in the United States, although occasional epidemics have been described and sporadic cases occur.
![]() ARF follows infection with certain strains of group A β-hemolytic Streptococcus, which stimulates antibody production that cross-react with host tissues. Children develop ARF 2 to 6 weeks after symptomatic or asymptomatic streptococcal pharyngitis.
ARF follows infection with certain strains of group A β-hemolytic Streptococcus, which stimulates antibody production that cross-react with host tissues. Children develop ARF 2 to 6 weeks after symptomatic or asymptomatic streptococcal pharyngitis.
![]() Arthritis, which occurs in most initial attacks, is migratory and polyarticular, primarily affecting large joints.
Arthritis, which occurs in most initial attacks, is migratory and polyarticular, primarily affecting large joints.
![]() Carditis occurs in one-third of patients, and can affect valves, muscle, and pericardium. Carditis confers greatest mortality and morbidity.
Carditis occurs in one-third of patients, and can affect valves, muscle, and pericardium. Carditis confers greatest mortality and morbidity.
![]() Sydenham’s chorea occurs in 10% of patients and may occur months after the initial infection. Manifestations include sudden, aimless, irregular movements and muscle weakness, and may be the sole clinical manifestation of ARF.
Sydenham’s chorea occurs in 10% of patients and may occur months after the initial infection. Manifestations include sudden, aimless, irregular movements and muscle weakness, and may be the sole clinical manifestation of ARF.
![]() The classic rash of ARF, erythema marginatum, is fleeting, faint, and serpiginous, usually accompanying carditis. Subcutaneous nodules, found on the extensor surfaces of extremities, are quite rare.
The classic rash of ARF, erythema marginatum, is fleeting, faint, and serpiginous, usually accompanying carditis. Subcutaneous nodules, found on the extensor surfaces of extremities, are quite rare.
![]() Laboratory tests are used to confirm prior streptococcal infection (throat culture and streptococcal serology) or to assess carditis (electrocardiogram, chest radiograph, and echocardiogram).
Laboratory tests are used to confirm prior streptococcal infection (throat culture and streptococcal serology) or to assess carditis (electrocardiogram, chest radiograph, and echocardiogram).
![]() The differential diagnosis includes JIA, septic arthritis, Kawasaki’s disease, leukemia, and other cardiomyopathies and vasculitides.
The differential diagnosis includes JIA, septic arthritis, Kawasaki’s disease, leukemia, and other cardiomyopathies and vasculitides.
![]() Significant carditis is managed with prednisone 1 to 2 milligrams/kg/dose given daily. Arthritis is initially treated with high-dose aspirin (75–100 milligrams/kg/d).
Significant carditis is managed with prednisone 1 to 2 milligrams/kg/dose given daily. Arthritis is initially treated with high-dose aspirin (75–100 milligrams/kg/d).
![]() All children with ARF are treated with penicillin (PCN): benzathine PCN 1.2 million U intramuscularly, procaine PCN G 600,000 U intramuscularly daily for 10 days, or oral PCN VK 6.25 to 12.5 milligrams/kg/dose four times a day for 10 days. Use erythromycin if the patient is PCN allergic.
All children with ARF are treated with penicillin (PCN): benzathine PCN 1.2 million U intramuscularly, procaine PCN G 600,000 U intramuscularly daily for 10 days, or oral PCN VK 6.25 to 12.5 milligrams/kg/dose four times a day for 10 days. Use erythromycin if the patient is PCN allergic.
![]() Long-term prophylaxis is indicated for patients with ARF, and lifelong prophylaxis is recommended for patients with carditis.
Long-term prophylaxis is indicated for patients with ARF, and lifelong prophylaxis is recommended for patients with carditis.
TRANSIENT TENOSYNOVITIS OF THE HIP
![]() Transient tenosynovitis is the most common cause of hip pain in children less than age 10 years of age. The peak age is 3 to 6 years, and boys are affected more than girls. The cause is unknown.
Transient tenosynovitis is the most common cause of hip pain in children less than age 10 years of age. The peak age is 3 to 6 years, and boys are affected more than girls. The cause is unknown.
![]() Symptoms may be acute or gradual: patients have pain in the hip, thigh, or knee, and an antalgic gait (or refusal to bear weight). Pain limits the hip’s range of motion. There may be a low-grade fever or history of recent upper respiratory infection, although patients do not appear toxic.
Symptoms may be acute or gradual: patients have pain in the hip, thigh, or knee, and an antalgic gait (or refusal to bear weight). Pain limits the hip’s range of motion. There may be a low-grade fever or history of recent upper respiratory infection, although patients do not appear toxic.
![]() The WBC and ESR are usually normal. Radiographs of the hip are normal or show a mild-to-moderate effusion. The main ED task is differentiation from septic arthritis, particularly if the patient is febrile, with elevation of WBC or ESR and effusion.
The WBC and ESR are usually normal. Radiographs of the hip are normal or show a mild-to-moderate effusion. The main ED task is differentiation from septic arthritis, particularly if the patient is febrile, with elevation of WBC or ESR and effusion.
![]() Diagnostic arthrocentesis is required, either with fluoroscopic or ultrasound guidance or in the operating room, in ambiguous cases. The fluid in transient tenosynovitis is a sterile clear transudate.
Diagnostic arthrocentesis is required, either with fluoroscopic or ultrasound guidance or in the operating room, in ambiguous cases. The fluid in transient tenosynovitis is a sterile clear transudate.
![]() Once septic arthritis and hip fracture have been ruled out, patients can be treated with anti-inflammatory agents such as ibuprofen 10 milligrams/kg, and close follow-up.
Once septic arthritis and hip fracture have been ruled out, patients can be treated with anti-inflammatory agents such as ibuprofen 10 milligrams/kg, and close follow-up.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 133, “Musculoskeletal Disorders in Children,” by Courney Hopkins-Mann, Damilola Ogunnaike-Joseph, and Donna Moro-Sutherland.