Principal Signs and Symptoms of Peripheral Nerve Disease
Disorders affecting mixed peripheral nerves cause various symptoms and signs corresponding, in anatomic distribution, to regions supplied by each nerve. To make a correct topographic diagnosis of peripheral nerve lesions, the clinician must thoroughly know the area of the sensory supply of each nerve, the muscles it innervates, and any muscle stretch reflex subserved by the nerve [377]. Certain nerves are purely motor, some are purely sensory, and others are mixed. The symptoms and signs of a peripheral nerve lesion include disturbances as detailed in the following text.
Sensory Disturbances
With the division of a sensory nerve, all modalities of cutaneous sensibility are lost only over the area exclusively supplied by that nerve (the autonomous zone). This zone is surrounded by an intermediate zone, which is the area of the nerve’s territory overlapped by the sensory supply areas of the adjacent nerves. The full extent (autonomous plus intermediate) of the nerve’s distribution constitutes the maximal zone. In clinical diagnosis, the autonomous zone of sensory loss for each nerve must be specifically sought to make an accurate topographic localization. In general, with peripheral nerve lesions, the area of light touch sensory loss is greater than the area of pinprick sensory loss.
Pain and paresthesias may also help in localizing a peripheral nerve lesion, but these subjective sensations frequently radiate beyond the distribution of the damaged nerve (e.g., proximal arm pain in the carpal tunnel syndrome). Some patients describe pain that is evoked by nonnoxious stimulation of the skin innervated by a damaged nerve (allodynia).
Motor Disturbances
Interruption of the motor fibers in a motor or mixed nerve leads to lower motor neuron paresis or paralysis of the muscles innervated by that nerve. Atrophy of specific muscle groups and characteristic deformities follow. The muscle or muscle groups involved may become flaccid (hypotonic), with decreased resistance to passive motion. This hypotonia may be the result of weakness preventing voluntary activity [382].
The actions of agonist muscles, which have the same or similar mechanical effects on a joint, and antagonist muscles, which have the opposite effect, should be considered in testing the strength of a particular muscle. The action of a powerful agonist may conceal weakness in a smaller muscle (e.g., the pectoralis may compensate for subscapular muscle weakness). Also, certain muscles may appear weak because their action requires the support of the paralyzed muscles (e.g., finger abduction by the dorsal interossei may seem weak when a radial nerve palsy prevents fixation of the wrist). A nerve often supplies several muscles with a similar action, and a lesion of that nerve results in weakness of the muscle group.
Disturbances of Muscle Stretch Reflexes
As a consequence of sensorimotor loss, the muscle stretch reflex subserved by each damaged nerve is decreased or absent.
Vasomotor, Sudomotor, and Trophic Disturbances
The skin subserved by the affected nerve may become thin and scaly. The nails may become curved, with retardation of nail and hair growth in the affected area. The affected area of the skin may become dry and inelastic and may cease to sweat. Because the analgesic cutaneous area is liable to injury, ulcers may develop.
Although ancillary procedures (e.g., electromyography and nerve stimulation studies, muscle and nerve biopsy, sweat tests) greatly aid in topographic diagnosis, the following discussion stresses only the bedside diagnosis and localization of individual peripheral nerve abnormalities.
Mononeuropathy Multiplex
Mononeuropathy multiplex (multifocal mononeuropathy) refers to the involvement of several isolated nerves. The nerves involved are often widely separated (e.g., right median and left femoral nerve). These multiple neuropathies result in sensory and motor disturbances that are confined to the affected individual nerves. Mononeuropathy multiplex is usually due to a disseminated vasculitis that affects individual nerves (e.g., vasculopathy in diabetes mellitus or polyarteritis nodosa).
Polyneuropathy
In polyneuropathy, the essential feature is the impairment of function of many peripheral nerves simultaneously, resulting in a symmetric, usually distal, loss of function. The characteristic features include muscle weakness with or without atrophy, sensory disturbances, autonomic and trophic changes, and hyporeflexia or areflexia. In general, the legs are affected before the arms. Polyneuropathy may be caused by different processes and may be mainly sensory (e.g., amyloidosis, paraneoplastic, leprosy), motor (e.g., Guillain–Barré syndrome, porphyria, lead intoxication), or both sensory and motor.
The loss of sensation in peripheral polyneuropathies may involve all modalities of sensation, but because nerve fibers of a specific caliber may be preferentially involved in the pathologic process, sensory impairment may be restricted to a certain form of sensation (dissociation of sensory loss). Preferential loss of pain and temperature perception may be seen in type I hereditary sensory neuropathy, amyloid neuropathy, Tangier disease, and in some cases of diabetic neuropathy. With these neuropathies, smaller-diameter nerve fibers conveying pain and temperature sensation are preferentially involved. A selective loss of touch pressure, two-point discrimination, and joint position sense (conveyed by larger myelinated fibers) with spared pain and temperature sensibility may occur with Friedreich’s ataxia, vitamin B12deficiency, and the Guillain–Barré syndrome.
The pattern of sensory and motor deficits in many polyneuropathies (e.g., diabetic polyneuropathy) develops according to axonal length, with sensory changes initially occurring at sites most distal from dorsal root ganglia cells [309]. When the sensory abnormality in the limbs extends proximally to 35 to 50 cm from the dorsal root ganglia, there is also a region of sensory loss over the anterior torso in accordance with the length of axons traversing the body wall. This sensory abnormality is wider in the lower abdomen and tends to be narrower in the thoracic region because of the longer, more oblique course of the sensory fibers to the lower abdomen and the shorter course of the nerves traveling along the ribs. When nerves <20 to 24 cm in length become involved, a “beanie cap” of sensory change over the scalp vertex occurs owing to the distal involvement of the ophthalmic branches of the trigeminal nerves. In extreme sensory neuropathies, only the shortest (<12 cm) nerve fibers are spared, so that there is sensory loss over the entire body except for a band of intact sensation over the posterior midline from the occiput to the sacral region [309].
The axonal length principle may also be applied to motor neuropathies where often the intrinsic foot muscles are initially affected, followed by the peroneal innervated muscles, and then by gastrocnemius-soleus involvement [309]. The anterior tibial compartment is affected before the posterior tibial compartment because the former’s nerve supply is longer than the latter by more than 10 cm. When all muscle groups below the knee are affected, intrinsic hand muscle involvement will develop. Patients with peripheral motor neuropathies often have greater motor weakness of ankle dorsiflexors than foot plantar flexors on a biomechanical as well as a physiologic basis [47]. In fact in patients with greater weakness of ankle plantar flexors than dorsiflexors, who are able to walk on their heels but not on their toes, intraspinal disease (e.g., conus-cauda equina tumor, spinal muscular atrophy, spinal stenosis, carcinomatous meningitis) rather than peripheral polyneuropathy should be suspected [47].
In some neuropathies (e.g., Tangier disease), the short axons are preferentially involved, and hence the sensory loss starts proximally and progresses distally, sometimes to the point where the entire body, except for the hands and regions below the knees, shows sensory impairment. Porphyric neuropathy may also start proximally, with paresis affecting the proximal arms, proximal legs, distal arms, and then distal legs (in that order). The muscle stretch reflexes in porphyria may be completely lost except for preserved ankle jerks, and the sensory loss may involve only the trunk, face, and proximal arms and thighs.
In some other neuropathies, the initial involvement and subsequent progression of clinical deficits may not be determined by the axonal length. For example, in lepromatous leprosy neuropathy, sensory loss occurs initially over the areas of the body having cooler surface temperatures (e.g., the tip of the nose, the malar areas of the cheeks) [308] because the proliferation of Mycobacterium leprae is greater in cooler tissues.
Lesions of Individual Nerves
Although peripheral nerves originate in plexuses (discussed in Chapter 3), it is easier to understand the course of peripheral nerves before reviewing the anatomy of the plexuses, than to understand the symptomatology of plexus lesions without the benefit of knowing peripheral innervation. For this reason, the authors have chosen to place this chapter first. Diagrams of the origin of each nerve in the plexus can be found in Chapter 3.
Nerve fibers do not randomly intertwine as they progress distally in nerve bundles. Evidence indicates that specific axons remain grouped together, particularly through their distal course, as they travel toward their destination [359]. Adjacent muscles and, similarly, adjacent sensory dermatomes are innervated by nerve fascicles that remain together within the nerve bundle. Therefore, ulnar neuropathies clinically “localized” to the wrist may actually be occurring at the elbow because of the preferential involvement of certain fascicles, whereas a proximal sciatic neuropathy sometimes masquerades as a peroneal neuropathy at the knee. These anatomic arrangements must always be taken into account when localizing pathologic processes [360].
Dorsal Scapular Nerve (C4–C5)
ANATOMY
The dorsal scapular nerve (a purely motor nerve) arises mainly from the C5 spinal nerve within the substance of the scalenus medius muscle. The nerve courses downward behind the brachial plexus deep to the levator scapulae muscle (which it supplies) and terminates by piercing the deep surfaces of the rhomboids (major and minor). The rhomboids normally elevate and adduct the medial border of the scapula (they are antagonists of the serratus anterior) and, along with the levator scapulae, rotate the scapula so that the inferior angle moves medially. The rhomboids are tested by having the patient press his or her elbow backward against resistance while the hand is on the hip [377].
NERVE LESIONS
Because the dorsal scapular nerve derives from the proximal plexus, affection of this nerve in an upper brachial plexopathy suggests a proximal lesion. The nerve may also be entrapped within the substance of the scalenus medius muscle. Isolated lesions of this nerve may occur in body builders [241]. A dorsal scapular nerve lesion results in the lateral displacement of the vertebral border of the scapula, which is rotated, with the inferior angle displaced laterally. Rhomboid atrophy is concealed by the overlying trapezius muscle. Rhomboid paresis is evident if the elbow can be pressed back only weakly against resistance (keeping the hand on the hip). Weakness is also evident when the patient attempts to push the palm backward against resistance with the arm folded behind the back.
Subclavian Nerve (C5–C6)
This purely motor nerve emerges from the upper trunk of the brachial plexus and descends in the posterior cervical triangle to innervate the subclavian muscle. This muscle depresses and medially draws the lateral end of the clavicle. Lesions of the subclavian nerve cause no important clinical disturbances.
Long Thoracic Nerve (C5–C7)
ANATOMY
This purely motor nerve (Fig. 2.1) arises from the C5–C7 roots shortly after they emerge from the intervertebral foramina. After passing through the scalenus muscle, the two upper roots are joined by a contribution from the C7 root. The nerve runs posterior to the brachial plexus and inferiorly behind the clavicle and then crosses the outer border of the first rib to reach the serratus anterior muscle. The nerve further descends along the lateral thoracic wall, sending individual filaments to the muscle slips of the serratus.
The serratus anterior muscle fixes and stabilizes the scapula against the chest wall and is tested by observing for scapular winging (the vertebral border of the scapula stands away from the thorax, forming a “wing”) while the patient pushes extended arms against a fixed object (e.g., a wall) [377].
NERVE LESIONS
The long thoracic nerve lies superficially in the supraclavicular region where it is subject to trauma [115]. Therefore, it is injured most frequently as a result of pressure on the shoulder (e.g., sudden trauma or carrying heavy objects on the shoulder—rucksack paralysis) [273]. Direct trauma to the shoulder or the lateral thoracic wall while playing football, or during a fall, or an auto accident may compress the nerve. Chiropractic manipulation of the cervical spine may also cause nerve injury [264]. Work-related or athletic activities, especially those involving repetitive stressful movements of the shoulder or those in which the arm is in an outstretched overhead position, may cause stretch or traction injury [319]. The overhead arm positioning may be a factor in the development of isolated long thoracic neuropathy during surgery with general anesthesia [179]. In a review of 197 cases of long thoracic neuropathy, 32 cases were iatrogenic owing to local invasive procedures such as first rib resections, mastectomies with axillary node dissection, thoracotomy, scalenectomies, infraclavicular plexus anesthesia, and chest tube insertion [179]. The nerve may be injured in up to 10% of patients undergoing radical mastectomies and in approximately 1% of patients undergoing simple mastectomies [96]. Isolated long thoracic nerve palsy may also occur as a manifestation of neuralgic amyotrophy (Parsonage–Turner syndrome) [101] or, rarely, after radiation therapy for breast cancer [286]. Also, familial long thoracic nerve palsy may be a major manifestation of familial brachial plexus neuropathy [275], and painful long thoracic neuropathy has been described as the sole manifestation of Lyme disease [245].

FIG. 2.1. The long thoracic nerve.
Nerve paralysis usually causes no deformity of the scapula when the arm is at rest. If, however, the patient is asked to push the arm forward against resistance or hold the arms up in front of the body, the scapula becomes winged (winged scapula or scapula alata), especially in its lower two-thirds region. The patient often complains of weakness of the shoulder and fatigue on raising the arm above the head. With injuries caused by excessive nerve stretch during physical activities, the sharp pain in the shoulder may radiate to the neck and upper arm.
Suprascapular Nerve (C5–C6)
ANATOMY
This purely motor nerve (Fig. 2.2) is a branch of the upper trunk of the brachial plexus. The nerve passes downward beneath the trapezius to the upper border of the scapula, where it passes through the suprascapular notch. This notch is bridged by the superior transverse scapular ligament, forming an osseofibrous foramen through which the nerve passes to enter the supraspinous area beneath the supraspinatus muscle. The nerve gives off branches to the supraspinatus and to the capsule of the shoulder joint and then courses around the free lateral border of the spine of the scapula to supply the infraspinatus muscle. Although the suprascapular nerve is said to have no cutaneous branches, rare cases have provided evidence for a cutaneous branch of the suprascapular nerve, as described in cadaveric studies [142].

FIG. 2.2. The suprascapular nerve.
The supraspinatus muscle normally abducts the humerus (mainly the first 15 degrees of abduction), whereas the infraspinatus muscle is mainly an external rotator of the upper arm.
NERVE LESIONS
The nerve may be injured in proximal upper brachial plexopathies and is also subject to damage in the supraclavicular region, especially with acute forceful depression of the shoulder and its dislocation. Fractures of the suprascapular notch or excessive callus formation after scapular fracture may compress the nerve. The nerve may also be injured after repair of rotator cuff tears [412]. Repetitive forced cross-body adductions of the arm or repetitive motions involving the scapulothoracic and shoulder joints may also injure the nerve. Suprascapular nerve injury has even been reported after driving for 2 hours speaking on a mobile telephone with the phone cradled between the ear and shoulder, probably by the nerve being compressed by the hard edge of the phone (mobile telephone user’s shoulder droop) [152]. Other etiologies of nerve injury include occupational overuse, sports-related injuries (especially sports involving overhead motions such as tennis, weight lifting, canoeing, and volleyball), direct nerve trauma, and ganglion cysts [187, 195].
Entrapment lesions (e.g., ganglia, spinoglenoid cyst, etc.) may occur in the suprascapular foramen [13,60,208,229,292,325]. This entrapment causes shoulder pain, which is aggravated by shoulder girdle movements, weakness, and eventual atrophy in the two spinati muscles. The pain is deep, located along the superior border of the scapula often extending toward the shoulder joint, occasionally radiating into the arm, and is made worse by movements that adduct the scapula or rotate the head away from the involved shoulder. Supraspinatus paresis results in weakness of arm abduction, whereas infraspinatus paresis results in impaired external rotations at the shoulder joint. Suprascapular involvement may also occur with neuralgic amyotrophy [101].
Harbaugh et al. described a patient with suprascapular nerve entrapment at the suprascapular notch presenting with right shoulder pain and atrophy with weakness of the right supra- and infraspinatus muscles [142]. The patient was noted to also have an area of numbness involving the right upper lateral shoulder. Although the suprascapular nerve is said to have no cutaneous branches, this case provides evidence for a cutaneous branch of the suprascapular nerve [142].
The branch of the infraspinatus muscle may be damaged in isolation by the entrapment of the suprascapular nerve at the spinoglenoid notch by a hypertrophied inferior transverse scapular ligament or a ganglion [7,191,208]. This results in shoulder pain, which is elicited by the external rotation of the shoulder joint, associated with weakness and wasting of the infraspinatus. Lesions at the suprascapular notch may also cause isolated infraspinatus weakness by involving only the portion of the nerve destined to innervate the infraspinatus muscle [41,191,351]. A lesion of the suprascapular nerve at the glenoid notch, causing isolated infraspinatus paresis and atrophy, may occur as a professional hazard in volleyball players [244]. Isolated infraspinatus paresis may also result from a nerve injury in body builders [44,241].
Subscapular Nerves (C5–C7)
ANATOMY
These purely motor nerves arise as branches of the posterior cord of the brachial plexus. The upper subscapular nerves supply the subscapularis, whereas the lower subscapular nerves supply the teres major.
NERVE LESIONS
Subscapular nerve palsies usually occur with posterior cord brachial plexus lesions. The arm is somewhat externally rotated, with some paresis of internal rotation, although the latissimus dorsi and pectoralis major muscles are usually able to compensate well for this paresis. The patient may complain of difficulty in scratching the lower back.
Thoracodorsal Nerve (C6–C8)
ANATOMY
This purely motor nerve, also known as the nerve to the latissimus dorsi, is a branch of the posterior cord of the brachial plexus and usually emerges from the plexus in a close association with the subscapular nerves. The nerve runs along the posterior axillary wall to reach and innervate the deep surface of the latissimus dorsi muscle. This muscle (along with the teres major) adducts and internally rotates the arm and depresses the raised arm. It is best tested by having the patient adduct the horizontally raised upper arm against resistance or by palpating the muscle bellies when the patient coughs [377].
NERVE LESIONS
Lesions of this nerve usually occur with damage to the posterior cord or proximal parts of the brachial plexus. Nerve lesions cause little deformity or atrophy, but proximal arm adduction is compromised. A combined movement comprising extension, adduction, and internal rotation, in which the dorsum of the hand is placed on the opposite buttock, readily reveals latissimus paresis. Isolated thoracodorsal nerve injury has been described in body builders [44,241].
Anterior Thoracic Nerves (C5–T1)
ANATOMY
The anterior thoracic nerves, purely motor nerves, (also called the pectoral nerves) are divided into the lateral anterior thoracic nerve (C5–C7), a branch from the anterior divisions of the upper and middle trunks of the brachial plexus, and the medial anterior thoracic nerve (C8–T1), a branch of the proximal section of the medial cord of the plexus. After these nerves descend posteriorly to the clavicle, the lateral nerve supplies the clavicular and upper sternocostal portions of the pectoralis major, and the medial division supplies the lower sternocostal portion of this muscle and the pectoralis minor.
The pectoralis major is an adductor and medial rotator of the humerus. It is tested by having the patient hold the arm in front of the body. The two portions can be seen and palpated when the patient resists attempts by the examiner to force the arm laterally [377].
NERVE LESIONS
Lesions of these nerves are of relatively little localizing importance except in corroborating brachial plexus damage. Adduction and medial rotation of the upper arm are weak, and the patient notices difficulty in using the arm in climbing. Isolated injury to the lateral anterior thoracic nerve as the result of a seat-belt injury may result in atrophy of the clavicular head of the pectoralis major [221]. Weight lifters may develop medial anterior thoracic nerve injury in isolation or in association with thoracodorsal nerve injury [44,241]. Bilateral medial anterior thoracic neuropathies in a weight lifter were thought to be due to concomitant pectoralis minor hypertrophy causing intramuscular entrapment of the nerves [302].
Gardetto et al. reported two cases of isolated damage to a muscle branch of the lateral pectoral nerve [117]. In both these patients, focal muscle atrophy developed gradually after the initiation of training schedules to increase the cross-section of the major pectoral muscle. The authors therefore assumed that compression injury to the nerve by repetitive muscle contractions may have been of pathogenic relevance. Anatomical studies of this region showed that the nerve branches of the lateral pectoral nerve, having to pierce through a connective tissue septum that is thicker by a few millimeters, may be subjected to an additional risk of compression [117].
Axillary Nerve (C5–C6)
ANATOMY
The axillary (circumflex) nerve (Fig. 2.3), a mixed nerve, arises as one of the terminal branches of the posterior cord of the brachial plexus from spinal segments C5 and C6. It lies first on the lateral side of the radial nerve, then courses laterally and backward to pass just below the shoulder joint. It then goes through the quadrilateral space, an anatomical compartment bounded inferiorly by the teres major muscle, medially by the long head of the triceps muscle, laterally by the surgical neck of the humerus, and superiorly by the teres minor muscle and subscapularis muscle. The nerve descends on the subscapularis muscle behind the axillary artery and then winds around the surgical head of the humerus, accompanied by the posterior circumflex humeral artery. It passes deep into the deltoid and teres minor muscles, supplying both. It sends sensory branches to the capsule of the shoulder joint (articular branch) and to the skin of the upper lateral aspect of the arm superficial to the deltoid muscle (lateral cutaneous nerve of the arm).
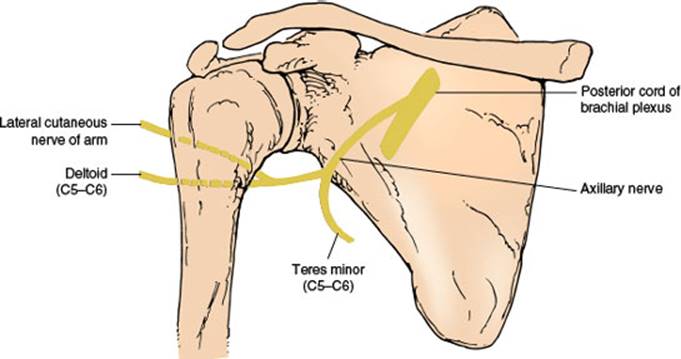
FIG. 2.3. The axillary nerve.
The teres minor muscle is a lateral rotator of the shoulder joint. The central part of the deltoid muscle is tested by having the patient abduct the upper arm against resistance (15–90 degrees), the anterior part by elevating the arm forward against resistance (up to 90 degrees), and the posterior part by having the patient retract the abducted upper arm against resistance.
NERVE LESIONS
Lesions of the posterior cord of the brachial plexus affect this nerve as well as the radial nerve (e.g., crutch paralysis). Trauma is the most common cause of axillary neuropathy. The axillary nerve is thought to be most vulnerable to traction injury of the brachial plexus because it is tethered to the deltoid muscle very close to the shoulder [39,153,267]. The nerve is most often injured as it winds around the lateral aspect of the humerus in a relatively exposed position (e.g., with fracture and dislocation of the humerus), when the shoulder joint is dislocated or when the scapula is fractured [15]. The axillary nerve may also be injured during reduction of a shoulder dislocation [398]. Axillary neuropathy may occur secondary to intramuscular injection high in the posterior aspect of the shoulder [170], after sleeping in a prone position with the arm raised above the head, following laparotomy (attributed to suspending the forearm from the anesthesia screen to gain better abdominal exposure), with neuralgic amyotrophy [101] or by direct nerve injury in athletes [267,271]. The nerve may be injured directly or entrapped by a fibrous band in the quadrilateral space [113,231]. Other etiologies of axillary injury in the quadrilateral space include trauma in athletes (especially volleyball players, baseball pitchers, and tennis players), the use of prosthetic devices for the upper arm using a “figure of eight” type of suspension, and hypertrophy of contiguous muscles [267]. As the posterior humeral circumflex artery also runs in the quadrilateral space, subclavian angiography in the quadrilateral syndrome may reveal occlusion of this vessel when the arm is abducted and externally rotated [59].
Nerve injuries usually cause a sensorimotor nerve palsy, but a purely motor nerve palsy is possible with nerve lesions at the humeral head. A purely sensory loss with no motor deficits is also possible [45]. For example, isolated damage to the sensory branch after arthroscopic surgery has been described [324]. In nerve lesions, the deltoid muscle becomes atrophic, causing a flattening or concavity of the shoulder contour. Teres minor paresis is usually not demonstrable on clinical examination because other muscles can perform its functions. Deltoid paralysis results in difficulty in abducting the arm, but other muscles of the shoulder girdle can compensate this function. An axillary cutaneous sensory defect is located on the outer aspect of the upper arm and is maximal on the patch of skin above the deltoid attachment.
Musculocutaneous Nerve (C5–C7)
ANATOMY
The musculocutaneous nerve, a mixed nerve (Fig. 2.4) arises from the lateral cord of the brachial plexus and proceeds obliquely downward between the axillary artery and the median nerve. The nerve pierces the coracobrachialis muscle and descends further between the biceps and brachialis muscles (it supplies all these three muscles). It may rarely innervate the pronator teres muscle (most often a median-innervated muscle). The nerve then continues distally as the lateral cutaneous nerve of the forearm after it pierces the deep fascia over the anterior elbow. The coracobrachialis muscle is a forward elevator of the arm, the brachialis (which occasionally also receives innervation from the radial nerve) is an elbow flexor, and the biceps is an elbow flexor and forearm supinator (especially when the elbow is flexed at 90 degrees). The biceps is tested by having the patient flex the supinated arm against resistance [377]. The biceps reflex is subserved by the musculocutaneous nerve.
The autonomous zone of the lateral cutaneous nerve of the forearm (a narrow band along the radial forearm) shows sensory loss with musculocutaneous nerve lesions. This zone of cutaneous sensory loss may extend from the elbow to the wrist and cover the entire lateral forearm from the dorsal to the ventral midline.
NERVE LESIONS
Nerve damage may result from lesions of the lateral cord of the brachial plexus. Proximal humeral lesions (e.g., fractures, osteochondroma) or shoulder dislocations may injure or compress the nerve [172]. Because the nerve is deep and is protected between the entry site into the coracobrachialis and the elbow, lesions are relatively uncommon here. A predominantly motor musculocutaneous neuropathy may develop after strenuous exercise of the upper extremity, probably due to nerve entrapment or stretch of the nerve where it passes through the coracobrachialis muscle in the upper arm [225]. Motor and sensory neuropathy may develop in this location after weight lifting, strenuous physical activity, rowing, football throwing, general anesthesia, or sleep [48,159,189,315] and has been described to occur with repetitive carrying of a heavy, rolled object by the shoulder with the object held in place by the arm curled around the object (carpet carrier’s palsy) [315]. Isolated biceps weakness may occur with distal motor nerve injury [44]. A purely sensory syndrome may result when the lateral cutaneous nerve of the forearm is damaged in the cubital fossa or forearm. This sensory branch may be injured by compression [258], venipuncture [40], or cutdown procedures because it lies directly under the median cubital vein in the center of the cubital fossa. Typically, patients notice pain in the proximal forearm, often aggravated by elbow extension, and paresthesias along the radial aspect of the forearm. A pure sensory neuropathy has also been observed in windsurfers who flex the upper extremity slightly at the elbow with the hand gripped over the boom [163]; this has also been observed with nerve compression from a handbag (handbag paresthesia) [140] and with nerve compression by the biceps aponeurosis [80].

FIG. 2.4. The musculocutaneous nerve.
With lesions of the musculocutaneous nerve, atrophy of the biceps and brachialis results in wasting of the ventral aspect of the upper arm. Loss of coracobrachialis function is difficult to detect clinically. With biceps weakness, flexion of the elbow is weak (especially when the forearm is supine), and the biceps reflex is lost.
Median Nerve (C6–T1)
ANATOMY
The mixed median nerve (Fig. 2.5) is formed in the axilla by the joining of the lateral cord of the brachial plexus (spinal segments C6–C7) with the medial cord (spinal segments C8–T1). The nerve then descends down the medial side of the arm in a close association with the brachial artery to the cubital fossa. From there, the median nerve enters the forearm between the two heads of the pronator teres muscle and gives off the anterior interosseous nerve, after which it dips under the sublimis bridge. It then courses deep to the flexor retinaculum at the wrist (carpal tunnel) to reach the hand. At a variable distance above the flexor retinaculum, the median nerve provides a palmar cutaneous branch, which crosses the flexor retinaculum either subcutaneously or through the superficial ligament fibers to supply the skin over the thenar eminence and proximal palm on the radial aspect of the hand. The median nerve passes through the carpal tunnel accompanied by the flexor tendons of the digits and emerges to divide into its terminal branches. These terminal branches include branches to the thenar muscles and the palmar digital nerves, which innervate the skin of the palmar aspect of the thumb, the second, third, and half of the fourth finger; the palm overlying the corresponding metacarpophalangeal joints; and the posterior middle and distal phalanges of the second, third, and half of the fourth finger.

FIG. 2.5. The median nerve.
The median nerve gives off no muscular branches until it reaches the elbow. As it passes between the heads of the pronator teres muscle, it supplies the following muscles:
1. Pronator teres (C6–C7), a forearm pronator. It is tested by having the patient pronate the forearm against resistance. This muscle may rarely be innervated by the musculocutaneous nerve.
2. Flexor carpi radialis (C6–C7), a radial flexor of the hand. This is tested by having the patient flex and abduct the hand at the wrist against resistance.
3. Palmaris longus (C7–T1), a flexor of the wrist.
4. Flexor digitorum superficialis (C7–T1), a flexor of the middle phalanges of the second, third, fourth, and fifth fingers. It is tested by having the patient flex the finger at the interphalangeal joint against resistance, with the proximal phalanx fixed.
After it passes between the two heads of the pronator teres, the median nerve gives off the purely motor anterior interosseus nerve, which innervates the following muscles:
1. Flexor pollicis longus (C7–C8), a flexor of the terminal phalanx of the thumb, it is tested by having the patient flex the distal phalanx of the thumb against resistance, while the proximal phalanx is fixed.
2. Flexor digitorum profundus I and II (C7–C8), a flexor of the terminal phalanges of the second and third fingers. It is tested by having the patient flex the distal phalanx of the second and third fingers against resistance, with the middle phalanx fixed.
3. Pronator quadratus (C7–C8), a forearm pronator.
At the distal end of the carpal tunnel, the median nerve divides into its terminal branches. The motor branches innervate the first and second lumbricals and the thenar muscles, which include the following:
1. Abductor pollicis brevis (C8–T1), an abductor of the metacarpal of the thumb. It is tested by having the patient abduct the thumb at right angles to the palm against resistance.
2. Opponens pollicis (C8–T1), a muscle that brings the metacarpal of the thumb into opposition. It is tested by having the patient touch the base of the little finger with the thumb against resistance.
3. Superficial head of the flexor pollicis brevis (C8–T1), a flexor of the proximal phalanx of the thumb.
4. Lumbricals I and II (C8–T1), flexors of the proximal and extensors of the two distal phalanges of the second and third fingers. They are tested by having the patient extend the finger at the proximal interphalangeal joint against resistance, with the metacarpophalangeal joint fixed and hyperextended.
The finger flexor reflex (C8–T1) is in part innervated by the median nerve.
It is important to be aware of potential variations in the innervation of the intrinsic hand muscles. Anomalous communications in the hand are sometimes referred to as Riche-Cannieu anastomoses [136] and are thought to involve communications between the motor branch of the median nerve and the deep ulnar nerve branch in the radial aspect of the hand. For example, the adductor pollicis and first dorsal interosseous muscles may be exclusively supplied by the median nerve (in 2% and 1% of individuals, respectively) and are therefore involved in median nerve lesions and spared in ulnar lesions. Also, the abductor pollicis brevis and the flexor pollicis brevis may be exclusively supplied by the ulnar nerve in 2% of individuals.
NERVE LESIONS
Lesions in the Axilla and Upper Arm. Median neuropathies in the axilla are often associated with damage to the ulnar and radial nerves (triad neuropathy) or brachial plexus. Etiologies include crutch compression, sleep paralysis, penetrating trauma, shoulder dislocation, vascular malformations, and sheath hemorrhage [303]. In the upper arm, the nerve may be damaged by penetrating trauma, humerus fractures, sleep paralysis, and arteriovenous fistulas [383]. The median nerve may be compressed in the upper arm by an anomalous course of the brachialis muscle [246]. Median lesions in the axilla or upper arm result in paresis or paralysis of all the muscles innervated by the median nerve, with a sensory loss in the distribution of both the palmar cutaneous and palmar digital branches. There is atrophy of the thenar eminence, affecting especially the abductor pollicis brevis and the opponens pollicis. Because of this atrophy, with recession of the metacarpal bones of the thumb to the plane of the other metacarpal bones, the hand takes on an abnormal appearance called simian hand or ape hand. This appearance results from the unopposed action of the extensor pollicis longus (radial nerve) and the adductor pollicis (ulnar nerve). Because the second finger cannot be flexed and the third finger can be flexed only partially, when the person attempts to make a fist, these fingers remain extended. The hand then takes on the appearance of that of a clergyman offering benediction (benediction hand). Because all the median muscles are affected, there are pareses of forearm pronation, radial wrist flexion, distal flexion of the thumb, palmar abduction, and opposition of the thumb and flexion of the second and, to a lesser extent, the third fingers.
Lesions at the Elbow. Median nerve compression at the elbow may be due to tumors and other masses, Struthers’ ligament or other anomalous ligaments, supracondylar spurs, entrapment within the two heads of the pronator teres muscle, a large brachialis muscle, the overlying bicipital aponeurosis, venous varix, and bone or ligament injuries (e.g., elbow fracture or dislocation) [75,78,413]. Vascular causes include catheterization, thrombosis, anomalies such as a persistent median artery, an anomalously enlarged ulnar artery, or a false aneurysm of the brachial artery [141,143,284,299,413]. Motor and sensory signs and symptoms are as described earlier in Lesions in the Axilla and Upper Arm but elbow lesions may also cause an anterior interosseous or pseudoanterior interosseous syndrome (see subsequent text).
Lesions at the Ligament of Struthers. In approximately 1% of the population, an anomalous spur of the bone occurs 3 to 5 cm above the medial epicondyle on the anteromedial humerus. A fibrous tunnel may be formed by a ligament (ligament of Struthers) that connects this spur to the medial epicondyle. The median nerve may be compressed here by this ligament, causing motor and sensory signs and symptoms as described earlier in Lesions in the Axilla and Upper Arm [18,42]. The ligament may also compress the brachial artery or, rarely, the ulnar nerve [240].
The Pronator Syndrome. The median nerve may be entrapped or constricted where it passes between the two heads of the pronator teres muscle and under the fibrous arch of the flexor digitorum superficialis (pronator syndrome) [134,247]. Nerve injury is especially likely to occur if the nerve passes deep to a hypertrophied pronator teres. This syndrome has the following characteristics:
1. Pain may be present in the proximal forearm, especially on resistance to pronation of the forearm and flexion at the wrist.
2. Tenderness is observed over the pronator teres muscle on the application of deep pressure.
3. Frequently, there is a lack of involvement of the pronator teres, flexor carpi radialis, palmaris longus, and flexor digitorum muscles because nerve branches to these muscles often depart from the median nerve proper before the site of nerve compression.
4. There is sparing of the muscles innervated by the anterior interosseous nerve if this nerve takes a high origin from the median trunk.
5. Paresthesias and sensory loss are observed in the median field of innervation (both palmar and digital cutaneous areas).
6. Atrophy and paresis of the median thenar musculature occur.
7. Tinel’s sign may be present.
The Anterior Interosseous Nerve Syndrome (Kiloh-Nevin Syndrome). Isolated lesions of this nerve [131,134,392] are not uncommon and may be due to strenuous exercise, trauma, a fibrous band constricting the nerve, or an accessory head of the flexor pollicis longus (Gantzer’s muscle) entrapping the nerve [304]. Injury to the nerve may follow cutdown procedure (for catheterization) [109,180,327,393] or venipuncture [312] in the antecubital fossa or supracondylar fractures [75]. The nerve may also be involved as part of the Parsonage–Turner syndrome (neuralgic amyotrophy) [101,293], injured while the patient is in the prone position for spinal surgery [8], affected by vascular anomalies [284], or compressed by bronchogenic carcinoma metastatic to the forearm [272]. Bilateral anterior interosseous nerve syndromes due to cytomegalovirus infection have been described [97]. This purely motor syndrome has several characteristics:
1. Pain is present in the proximal forearm or arm lasting hours to days.
2. Mild paresis of forearm pronation (due to pronator quadratus weakness) is observed. The anterior interosseous nerve may rarely give rise to the nerve of the pronator teres muscle and, therefore, the syndrome may rarely present with weakness of the pronator teres [16].
3. Paresis of flexion of the terminal phalanges of the second and third fingers (due to paresis of the flexor digitorum profundus I and II) is observed.
4. Paresis of flexion of the terminal phalanx of the thumb (due to paresis of the flexor pollicis longus) is observed.
5. There is a characteristic pinch attitude of the hand while attempting to make a full circle by applying the pulp of the thumb to that of the index finger with firm pressure. This results from weakness of the flexor pollicis longus and the flexor digitorum profundus. There is hyperextension of the interphalangeal joint of the thumb, inability to flex the distal phalanges of the thumb and index finger, and proximal approximation of the thumb on the index finger.
6. Normal sensation is observed.
Because the anterior interosseous nerve has no cutaneous representation, this syndrome is often considered a purely motor syndrome. However, sensory fibers of the wrist radiocarpal, radioulnar, intercarpal, and carpometacarpal joints travel in the anterior interosseous nerve [88,392]. Injury to the terminal branch of the anterior interosseous nerve can cause persistent, dull, aching volar wrist pain [88].
A pseudoanterior interosseous nerve syndrome has been described [393], with partial median nerve compromise at the antecubital level. The nerve bundles that form the anterior interosseous nerve are primarily involved, and the motor findings are those described with the anterior interosseous nerve syndrome. The anterior interosseous nerve fascicle within the median lies posteriorly at the elbow and is, therefore, most prone to injury by fractures at this site [359]. Other median-innervated muscles are spared, and the only clinical finding betraying a more proximal median nerve lesion is some median distribution sensory change, as the sensory fibers from the index finger and thumb also lie posteriorly [359]. This syndrome has been noted with supracondylar fracture of the humerus, proximal radial fracture, venipuncture or arterial catheterization, and neuroma.
Median nerve entrapment may occur in the forearm because of an accessory bicipital aponeurosis [350] or because of enlarged communicating veins directly compressing the median nerve [54]. Other etiologies include arteriovenous fistulas in patients on chronic renal dialysis, fractures of the ulna or radius, and tumors [397]. This syndrome is characterized by paresis or paralysis of muscles innervated by the anterior interosseous nerve as well as more proximal median-innervated muscles (e.g., pronator teres and flexor carpi radialis). Sensation is intact. Median nerve damage proximal to the carpal tunnel may occur in wheelchair athletes [58].
The Carpal Tunnel Syndrome. The median nerve is particularly vulnerable to compression as it passes into the hand between the carpal bones and the transverse carpal ligament (carpal tunnel) [81,266,301,356]. The incidence of carpal tunnel syndrome is increased among electronic-parts assemblers, frozen-food processors, musicians, cyclists, wheelchair athletes, and dental hygienists; repetitive wrist movements, vibrating tools, awkward wrist positions, and great force seem to correlate with this disorder [81]. Women are more commonly affected than men. The increased pressure within the carpal tunnel is usually caused by a nonspecific flexor tenosynovitis, but certain conditions such as diabetes mellitus, rheumatoid arthritis, pregnancy [386], amyloidosis, hypothyroidism, acromegaly, renal dialysis, and congenital narrowing of the carpal canal, may predispose to this syndrome. The frequency of carpal tunnel syndrome in computer users is surprisingly similar to that in the general population [357]. A carpal tunnel-like syndrome may also occur with compression of the median nerve in the distal forearm, proximal to the carpal tunnel (e.g., due to a thrombosed aneurysm of the epineural vessels) [52,114]. The carpal tunnel syndrome usually consists of four main symptoms:
1. Bouts of pain or paresthesias in the wrist and hand are observed that are often most severe and troublesome during the hours of sleep and that are relieved by shaking or rubbing the involved hand. Although these symptoms are usually localized to the wrist or median-innervated fingers, they may spread upward into the forearm [135,356]. For example, paresthesias and pain occurred proximal to the wrist in 36.5% of 255 patients in one study [356]. Patients may also report sensory symptoms in the hand outside the median distribution (e.g., in the whole hand, in an ulnar distribution, or in a radial distribution), but sensory signs do not extend beyond the median nerve distribution [135]. The symptoms are bilateral in over half the cases but usually appear first and are more severe in the dominant hand.
2. Paresis and atrophy of the abductor pollicis brevis and opponens pollicis muscles are present. Because the opponens pollicis is occasionally anomalously supplied by the ulnar nerve, this muscle may be spared. In the carpal tunnel syndrome, the lumbricals are often normal because, in the carpal tunnel, fibers that innervate the lumbricals lie more posteriorly than those to the thenar muscles, protecting the lumbrical motor fibers from compression [211].
3. Sensory loss on the radial palm, the palmar aspect of the first three-and-a-half fingers, and the dorsal aspect of the terminal phalanges of the second, third, and half of the fourth fingers is noted. This sensory loss is usually most prominent in the appropriate fingertips. (Because the palmar cutaneous nerve takes its origin proximal to the wrist joint, the sensation on the thenar eminence and proximoradial palm is spared. Therefore, if this area shows a sensory loss, the lesion is proximal to the wrist joint.) Because of the fascicular arrangement of median sensory fibers in the wrist, sensory abnormalities may be limited to one side of a digit or to a web space between two digits, falsely suggesting more distal median sensory branch impairment [359].
4. Increased sensitivity of the damaged nerve fibers to mechanical deformation is observed. Because of this, various clinical tests may help detect a lesion at the carpal tunnel. Light percussion over the median nerve at the volar surface of the wrist may elicit a tingling sensation radiating into the hand in the median distribution (Tinel’s sign). When a blood pressure cuff is applied to the arm and compression is above systolic pressure, median paresthesias and pain may be aggravated (cuff compression test of Gilliatt and Wilson). Flexion of the wrist to 90 degrees for 30 to 60 seconds may aggravate paresthesias and pain (Phalen’s sign) as may hyperextension of the wrist.
Lesions of the Palmar Cutaneous Branch of the Median Nerve. The palmar cutaneous branch arises about 5 cm above the wrist and courses distally on the radial side of the palmaris longus tendon. It passes subcutaneously or through a canal of its own within the transverse carpal ligament and then divides into branches supplying the skin over the thenar eminence. The nerve may be damaged by accidental lacerations and during carpal tunnel surgery. Other causes of neuropathy include compression by an abnormal palmaris longus muscle or by a ganglia and entrapment by scars or fascial bands [10,57,121,334,355]. Damage to the nerve produces pain, paresthesias, and numbness over the thenar eminence. Median nerve compression at the wrist may occur with handcuff compression [130].
Lesions within the Hand. Median nerve entrapment in the palm by the head of the left first metacarpal bone while holding golf clubs may cause a sensory neuropathy with hypesthesia in a median distribution [155]. Injury to the deep palmar branches of the median nerve in the distal carpal canal (e.g., by a palmar ganglion [178]) or at the thenar eminence produces a purely motor syndrome with weakness and wasting of the thenar muscles (abductor pollicis brevis, opponens pollicis, and superficial head of the flexor pollicis brevis) with no sensory abnormalities. Selective acute demyelination of the recurrent thenar motor branch of the median nerve owing to vibrations from a sander (vibration-induced median neuropathy) may cause weakness in the abductor pollicis brevis without sensory loss [176].
Lesions of the Palmar Digital Branches of the Median Nerve. The palmar digital nerves are the terminal branches of the median and ulnar nerves (Fig. 2.6). The median nerve divides into a number of branches after it emerges from the distal end of the carpal tunnel. Usually, it divides into two major branches, each of which then divides into the common digital nerves, which in turn divides into two proper digital branches. The two palmar digital branches to the thumb and to the lateral side of the second digit usually arise from the lateral terminal division of the median nerve. The other digital branches from the median nerve arise from the medial division and supply digital branches to the lateral three-and-a-half digits, but the entire fourth digit may be innervated by the median or ulnar nerve.
Lesions of a common palmar digital nerve in the hand cause sensory symptoms and loss usually involving the adjacent sides of two fingers, depending on the nerve distribution. Damage to a proper digital branch produces sensory loss and paresthesias restricted to the side of the finger. Etiologies include trauma (e.g., lacerations, finger dislocations, and fractures), compression from musical instruments (e.g., flutist’s neuropathy), tendon sheath cysts and tumors, tenosynovitis, nerve ischemia (e.g., in diabetes), and nerve tumors [26,79,296].
Digital neuropathy is a pure sensory neuropathy of a digital nerve. It may be caused by acute or chronic local trauma or pressure, or accompany systemic illnesses such as rheumatoid disease, leprosy, Raynaud disease, dysproteinemia, or diabetes mellitus [137]. Digital neuropathy of the median and ulnar nerves may be caused by Dupuytren contracture [137]. Dupuytren tissue usually affects the palmar fascia, superficial to the digital nerves, and it may rarely affect the spiral cord in the digits. A spiral cord may cause sensory loss due to impingement of digital nerves or Dupuytren tissue may compress the palmar digital nerves against the relatively inelastic deep transverse metacarpal ligament.

FIG. 2.6. Palmar view of the right hand showing the course of palmar digital branches of the median and ulnar nerves.
Bowler’s thumb is a digital neuropathy of the palmar digital branch that supplies the medial side of the thumb due to chronic compression from a bowling ball [92,263]. This compression is usually due to perineural fibrosis but, infrequently, a bowler’s thumb lesion is a traumatic neuroma caused by the proliferation of fibrous tissues, both around and within the digital nerve [263]. These phenomena are the result of adaptive changes in the thumb in response to frequent insertion and compression in the holes of the bowling ball. The clinical presentation of this condition may include paresthesias, hypesthesia, changes in two-point discrimination sense, or a positive Tinel’s sign in the distribution of the involved digital nerve, which may be thick and firm to palpation. This condition is most commonly described in bowling enthusiasts, although similar involvement can be caused by other sporting activities such as baseball, by repetitive use injuries, and following finger surgery [263].
Ulnar Nerve (C7–T1)
ANATOMY
The ulnar nerve, a mixed nerve, (Fig. 2.7) is the main branch of the medial cord of the brachial plexus and derives from the seventh and eighth cervical and first thoracic spinal roots. It crosses the axilla beneath the pectoralis minor muscle and continues to the upper arm, where it lies medial to the brachial artery. In the distal arm it enters a groove between the medial humeral epicondyle and the olecranon process. The aponeurosis between the olecranon and medial epicondyle forms the roof of an osseofibrous canal (the cubital tunnel), the floor of which is formed by the medial ligament of the elbow joint. It then passes between the humeral and ulnar heads of the flexor carpi ulnaris to rest on the flexor digitorum profundus. Immediately distal to the elbow joint the nerve gives off its first two muscular branches, to the flexor carpi ulnaris and the flexor digitorum profundus III and IV, respectively.

FIG. 2.7. The ulnar nerve.
1. Flexor Carpi Ulnaris (C7–T1). An ulnar flexor of the wrist. It is tested by having the patient flex and adduct the hand at the wrist against resistance.
2. Flexor Digitorum Profundus III and IV (C7–C8). A flexor of the terminal phalanges of the fourth and fifth fingers. It is tested by having the patient flex the distal phalanx against resistance while fixing the third phalanx.
The ulnar nerve then descends beneath the flexor carpi ulnaris and, in the distal forearm, gives off the palmar cutaneous branch, which supplies the skin over the hypothenar eminence. It then gives off a dorsal cutaneous branch, which supplies the dorsal ulnar aspect of the hand and the dorsal aspect of the fifth finger and half of the fourth finger. The ulnar nerve proper then enters the wrist lateral to the tendon of the flexor carpi ulnaris muscle. In the hand it gives off the superficial terminal branch, which is a sensory branch to the skin of the distal part of the ulnar aspect of the palm and the palmar aspect of the fifth and half of the fourth finger, and then passes between the pisiform carpal bone medially and the hook of the hamate carpal bone laterally (ulnar tunnel or canal of Guyon) as the deep muscular branch. This deep branch supplies several muscles:
1. Palmaris brevis (C8–T1). A cutaneous muscle at the proximal border of the ulnar aspect of the hand.
2. Abductor digiti minimi (C8–Tl). An abductor of the fifth finger. It is tested by having the patient abduct the fifth finger against resistance while the volar aspect of the hand is on a flat surface.
3. Opponens digiti minimi (C8–T1). An opposer of the fifth finger.
4. Flexor digiti minimi (C8–T1). A flexor of the fifth finger. It is tested by having the patient flex the fifth finger at the metacarpophalangeal joint against resistance.
5. Lumbricals III and IV (C8–T1). Flexors of the metacarpophalangeal joints and extensors of the proximal interphalangeal joints of the fifth and fourth fingers. They are tested by having the patient extend the proximal interphalangeal joint against resistance, with the metacarpophalangeal joint hyperflexed and fixed.
6. Interosseous muscles (C8–Tl). Flexors of the metacarpophalangeal joints and extensors of the proximal interphalangeal joints. The four dorsal interossei are finger abductors, whereas the three palmar interossei are finger adductors. They are tested by spreading or abducting the fingers against resistance. The median nerve innervates the first dorsal interosseous muscles in 1% of individuals. Rarely, the first dorsal interosseous muscle is innervated by the radial nerve (Froment–Rauber nerve). Rarely, all thenar muscles, including the opponens, may be innervated by the ulnar nerve (all-ulnar motor hand) [116,310].
7. Adductor pollicis (C8–T1). An adductor of the metacarpal of the thumb. It is tested by having the patient adduct the thumb at right angles to the palm against resistance. The median nerve innervates this muscle in 2% of individuals.
8. Deep head of the flexor pollicis brevis (C8–Tl). A flexor of the first phalanx of the thumb.
NERVE LESIONS
Lesions above the Elbow. Processes causing damage to the ulnar nerve in the axilla or upper arm may also damage the median and radial nerves (triad neuropathy). Nerve compression may be caused by sleeping with the arm hanging over a sharp edge or the head of a sleeping partner compressing the nerve against the humerus, crutches or tourniquets, arteriovenous fistulas in dialysis patients, aneurysms, hematomas, nerve tumors, and other masses [277, 367]. Supracondylar fractures of the humerus may also cause nerve injury [78,158]. Ulnar entrapment neuropathy in the midarm, proximal to the medial epicondyle, may be due to nerve compression by the medial intermuscular septum [253].
Lesions of the ulnar nerve above the elbow (e.g., a lesion of the medial cord of the brachial plexus) produce the following signs:
1. Abnormal appearance of the hand. The hypothenar eminence and interossei are atrophied and flattened. There is often a “claw-hand” deformity (main en griffe), in which the fifth, fourth, and, to a lesser extent, the third fingers are hyperextended at the metacarpophalangeal joints and flexed at the interphalangeal joints. The hyperextension at the metacarpophalangeal joints is due to paralysis of the interossei and ulnar lumbricals, which results in unopposed action of the long finger extensors (extensor digitorum); the flexion at the interphalangeal joints is due to the pull exerted by the long flexor tendons. Rarely, ulnar neuropathy may initiate or sustain a specific dystonia that is manifest by the flexion of the fourth and fifth digits [70].
2. Paresis or paralysis of the ulnar flexion. This applies to the ulnar flexion of the wrist and of the terminal phalanges of the fourth and fifth fingers, and at the metacarpophalangeal joints of the second to fifth fingers. Ulnar paresis also affects extension at the interphalangeal joints of the second to fifth fingers, adduction and abduction of the second to fifth fingers, and abduction and opposition of the fifth finger. As a result of adductor pollicis affection, Froment’s prehensile thumb sign (signe du journal) may be present (when a sheet of paper is grasped between the thumb and index finger and pulled, the proximal phalanx of the thumb is extended and the distal phalanx is flexed if an ulnar nerve lesion is present).
3. In 15% to 31% of subjects, a median-ulnar communication exists (Martin-Gruber anastomosis) [136,206] in which axons descending in the median or anterior interosseous nerve cross through the forearm to join the ulnar nerve at the wrist. The median fibers ultimately innervate the intrinsic hand muscles, especially the first dorsal interosseous, adductor pollicis, and hypothenar muscles. Therefore, if a patient has an ulnar neuropathy above the forearm, these muscles may be spared or minimally involved if a median-ulnar communication is present. The entry point of the crossing fibers from the median to the ulnar nerve usually occurs 3 to 10 cm distal to the medial humeral epicondyle [381]. Ulnar-to-median communications in the forearm [363] and those of only sensory fibers [151] may rarely occur. The overall incidence of Martin-Gruber anastomoses is approximately 17% [206]. Four types of connections exist: type 1 (60%) send motor branches from the median to the ulnar nerve to innervate “median” muscles; type II (35%) send motor branches from median to ulnar nerves to innervate “ulnar” muscles; type III (3%) send motor fibers from the ulnar to the median nerve to innervate median muscles; and type IV (1%) send motor fibers from the ulnar to the median nerve to innervate ulnar muscles.
4. Sensory findings. Because all three sensory branches of the ulnar nerve are affected (palmar, dorsal, and superficial terminal cutaneous branches), paresthesias and sensory loss occur on the dorsal and palmar surfaces of the fifth and ulnar half of the fourth finger and the ulnar portion of the hand to the wrist.
Lesions at the Elbow (Cubital Tunnel Syndrome). The ulnar nerve is most commonly compressed at the elbow in the cubital tunnel [29,30,53,81,238,239] because this tunnel narrows during movement, especially elbow flexion. Nerve entrapment is due to the thickening of the aponeurotic arch (the humero-ulnar aponeurotic arcade) between the two heads of the flexor carpi ulnaris or bulging of the medial collateral ligament of the elbow joint (floor of the cubital tunnel) [63]. The nerve may also be entrapped by a ganglion cyst or other mass of the elbow (e.g., intraneural perineuroma), by dense fibrous bands bridged directly between the medial epicondyle and the olecranon proximal to the cubital tunnel proper, by an accessory anconeus epitrochlearis muscle, by supracondylar spurs, or at its point of exit from the flexor carpi ulnaris muscle distally by a thickened muscular septum between the flexor carpi ulnaris and the flexor digitorum profundus [28,63,64]. Patients with end-stage renal disease receiving hemodialysis may be especially predisposed to ulnar neuropathy by factors such as arm positioning during hemodialysis, underlying polyneuropathy, and upper extremity vascular access [256].
The ulnar nerve at the elbow is also subject to external trauma, especially during coma or general anesthesia [148,205] and may be severed by missile injury [414]. Deformity from previous elbow injuries may lead to a nerve stretch, eventually producing signs and symptoms long after the original injury (tardy ulnar nerve palsy). The syndrome produced by these lesions is the same as that described previously in the section Lesions above the Elbow. A reliable sign of ulnar entrapment by the flexor carpi ulnaris muscle is the ulnar flexion maneuver [108], in which increased paresthesias in the fourth and fifth digits follow 3 minutes of elbow and wrist flexion in ulnar deviation.
The main clinical features of the cubital tunnel syndrome, which differentiate it from tardy ulnar nerve palsy, are [238]:
1. No evidence of joint deformity or prior trauma
2. Frequent occurrence of bilateral symptoms and signs of ulnar neuropathy
3. A taut, palpably enlarged nerve in the ulnar groove
4. Electrophysiologic (electromyographic) localization to the cubital tunnel
5. Operative findings of a swollen, taut, hyperemic nerve, distally limited by the proximal border of the aponeurosis joining the two heads of the flexor carpi ulnaris muscle.
Ulnar neuropathy at the elbow often spares the flexor carpi ulnaris muscle. This was thought to occur because the nerve branches to the flexor carpi ulnaris may arise at or proximal to the medial epicondyle (in 10% of individuals), but the involvement of flexor carpi ulnaris more often correlates with the severity of the neuropathy and with whether compression is retroepicondylic or at the humero-ulnar aponeurotic arcade [62]. Sparing of the flexor carpi ulnaris with ulnar neuropathy at the elbow is unrelated to the level of origin of its innervating branch but rather related to the internal topography of the nerve, the severity of compression, and the level of compression [62,359]. Ulnar neuropathy at the elbow may preferentially compress the nerve fascicle to distal hand muscles while sparing the sensory branches as well as the motor fascicle to the more proximal flexor carpi ulnaris and flexor digitorum profundus, thereby mimicking a Guyon’s canal ulnar neuropathy when the lesion is, in fact, at the elbow [359].
Lesions in the Forearm. Etiologies of ulnar nerve compression in the forearm include a hypertrophied flexor carpi ulnaris muscle, fibrous and fibrovascular bands, hematomas, and handcuffs [61,62,150,322]. Ulnar nerve entrapment at the forearm or wrist may occur in wheelchair athletes [58]. Damage may also occur with fractures of forearm bones (e.g., Colles’ fracture) [304,379]. Ischemic neuropathy may occur in patients with arteriovenous shunts for dialysis [397]. The clinical features are as explained earlier for the section Lesions above the Elbow except that the flexor carpi ulnaris and the flexor digitorum profundus I and II muscles are often spared. In a patient with surgical section of the distal ulnar nerve in the forearm, ulnar sensation in the dorsal hand was spared in relation to the superficial radial sensory innervation of the ulnar hand dorsum (“paradoxical” preservation of ulnar sensory function) [230].
Lesions at the Wrist and in the Hand. An ulnar lesion at the wrist [330] causes the same motor findings as a lesion at a more proximal level, except that the flexor carpi ulnaris and the flexor digitorum profundus III and IV are spared. The sensory findings depend on the location of the nerve lesion with respect to the sites of origin of the palmar and dorsal cutaneous branches. If the lesion is distal to these two branches, the sensory loss is restricted to the distal palm and the palmar surfaces of the fifth finger and the medial fourth finger (the area of supply of the superficial terminal cutaneous branch). The proximal palmar area and the entire dorsum of the hand are then spared.
Ebeling, Gilliatt, and Thomas have divided lesions of the ulnar nerve in the hand into three groups [98]:
1. Compression of the nerve as it enters the hand. All of the ulnar-innervated muscles of the hand are affected, and because the lesion is proximal to the superficial terminal cutaneous nerve, there is sensory loss on the distal palm and the palmar surfaces of the fifth finger and the medial half of the fourth finger.
2. Compression of the proximal part of the terminal motor branch (usually due to nerve compression within the canal of Guyon or pisohamate tunnel) [289]. In these purely motor lesions, all the hand muscles innervated by the ulnar nerve are affected. Because the lesion is distal to the superficial terminal cutaneous branch, there is no sensory loss.
3. Distal compression of the terminal motor branch of the ulnar nerve. This purely motor lesion is distal to the site of origin of the motor fibers of the hypothenar muscles and is also distal to all sensory branches [165]. It therefore results in paresis and atrophy of the interossei, the medial two lumbricals, the deep head of the flexor pollicis brevis, and the adductor pollicis muscles only.
Others have divided ulnar lesions at the wrist and hand into four groups [65]:
Type 1. Weakness of all ulnar intrinsic hand muscles and ulnar sensory impairment (dorsal ulnar sensory branch distribution not involved) caused by compression (e.g., by a carpal ganglion [124]) just proximal to or within the Guyon’s canal (both superficial and deep branches affected).
Type 2. Weakness of muscles innervated by a deep ulnar branch (including hypothenar) owing to its compression at its origin, but normal sensation.
Type 3. Weakness of muscles innervated by a deep ulnar branch with sparing of hypothenar muscles owing to its compression distal to branches innervating the hypothenar muscles [165].
Type 4. Compression at the distal end of the Guyon’s canal, resulting in the sensory branch alone being affected.
Ulnar nerve compression at the wrist or hand is most frequently caused by a ganglion from one of the carpal joints followed by occupational neuropathy, laceration, ulnar artery disease (e.g., aneurysm), or carpal bone fracture [124,165,330]. Other causes include lipoma, external pressure, nerve tumor, and rheumatoid cyst [84,112,289,411]. These patients present with obvious atrophy of the first dorsal interosseous and adductor muscles without sensory changes. In patients who developed an ulnar neuropathy after kidney transplant surgery, the presence of an arteriovenous shunt in the hand may have played a role [415]. A rare cause of ulnar compression in the Guyon’s canal is calcinosis in scleroderma [375]. The motor branch of the ulnar nerve may be compressed by the arch of origin of the adductor pollicis muscle at the point where the nerve crosses the third metacarpal or where the nerve penetrates the adductor muscle [306].
Palmaris brevis spasm syndrome has been described to occur following the prolonged use of a computer mouse and keyboard [207]. Electrophysiologic studies suggest a distal ulnar motor branch lesion.
Lesions of the Dorsal Cutaneous Branch of the Ulnar Nerve. The dorsal cutaneous branch arises above the wrist and winds medially around the ulna, deep to the tendon of the flexor carpi ulnaris muscle. It supplies the skin of the dorsum of the hand and the fifth finger. Damage to this branch may occur with blunt trauma, lacerations, handcuffs (handcuff neuropathy), wrist surgery, vein injection in addicts, and repetitive wrist movements in a person using a code-sensing machine at a checkout counter (pricer palsy) [130,144,331,332,391]. Nerve entrapment may occur where the nerve passes under the flexor carpi ulnaris tendon [120]. Pain and other sensory disturbances occur in the distribution of the nerve.
Lesions of the Palmar and Dorsal Digital Branches of the Ulnar Nerve. As noted above, the palmar digital nerves are the terminal branches of the median and ulnar nerves (Fig. 2.6). The superficial terminal branch of the ulnar nerve arises within the Guyon’s canal, passes into the hand, and divides into three palmar digital branches that supply the fifth digit and the ulnar half of the fourth digit (Fig. 2.6). Sensory loss and symptoms may affect the medial and lateral palmar aspects of the fifth digit and the ulnar half of the fourth digit, the ulnar aspect of the fourth digit and the medial half of the fifth digit, or the ulnar half of the fourth digit, the medial half of the fifth digit, or the ulnar half of the fifth digit in isolation, depending on the location of the nerve injury. The dorsal digital nerves are formed from the branches of the superficial radial and dorsal ulnar cutaneous nerves. The dorsal ulnar cutaneous nerve sends dorsal digital branches to the dorsum of the ulnar half of the fourth digit and the medial and lateral halves of the dorsum of the fifth digit (Fig. 2.8). Etiologies of palmar and dorsal digital neuropathies are as discussed under the section Lesions of the Palmar Digital Branches of the Median Nerve.
Pseudoulnar Nerve Palsy. Pseudoulnar nerve palsy refers to isolated hand weakness apparently in an ulnar distribution that is due to contralateral cerebral infarction in the white matter of the angular gyrus of the inferior parietal lobe [376]. Patients with this condition are found to have contralateral carotid artery stenosis. Isolated “ulnar” sensory loss and hand weakness may also occur with infarction, affecting the contralateral precentral gyrus and anterior aspect of the postcentral gyrus [274], and pseudoulnar sensory loss may occur with small cortical infarction of the midportion of the postcentral gyrus [66].
Radial Nerve (C5–C8)
ANATOMY
The radial nerve, a mixed nerve, (Fig. 2.9) derives from the posterior cord of the brachial plexus and comprises fibers from the spinal levels C5–C8. After descending posterior to the axillary artery, between the long and medial heads of the triceps, it then continues distally in the spiral groove of the humerus (in contact with the bone or separated from it by some fibers of the medial head of the triceps).
In the axilla, the nerve gives rise to the posterior cutaneous nerve of the arm, which supplies the skin over the posterior aspect of the arm as far down as the olecranon. A secondary sensory branch, the posterior cutaneous nerve of the forearm, arises either within or proximal to the spiral groove and innervates the skin on the distal extensor aspect of the arm and that of the forearm up to the wrist. Within or proximal to the spiral groove, two motor branches are given off. They supply the following two muscles:
1. Triceps (C6–C8), a forearm extensor subserving the triceps reflex. This muscle is tested by having the patient extend the forearm at the elbow against resistance.
2. Anconeus (C6–C8), a forearm extensor.

FIG. 2.9. The radial nerve.
After its course in the spiral groove, the radial nerve reaches the lateral aspect of the humerus and pierces the lateral intermuscular septum to occupy a position in front of the lateral condyle of the humerus between the brachialis and brachioradialis muscles. Here it supplies the following muscles:
1. Brachialis (C5–C6), an elbow flexor. It is also innervated by the musculocutaneous nerve.
2. Brachioradialis (C5–C6), a forearm flexor. It is tested by having the patient flex the forearm against resistance, with the forearm midway between pronation and supination. This muscle subserves the radial reflex.
3. Extensor carpi radialis longus (C5–C6), a radial extensor of the hand. It is tested by having the patient extend and abduct the hand against resistance.
The radial trunk then bifurcates into a superficial branch and a deep branch. The superficial branch passes over the origin of the extensor carpi radialis brevis and down the forearm under the brachioradialis. It emerges in the distal forearm, as the dorsal digital nerve, and supplies the skin on the medial aspect of the back of the hand and the dorsum of the first four fingers (the autonomous zone of supply is the skin over the first interosseous space).
The deep branch passes through the fibrous edge of the extensor carpi radialis by means of a slit in the supinator muscle (arcade of Frohse) to the posterior forearm. In the forearm, it is in contact with the interosseous membrane and is referred to as the posterior interosseous nerve. This purely motor nerve innervates the following muscles:
1. Supinator (C6–C7), a forearm supinator that is tested by having the patient supinate the forearm against resistance.
2. Extensor carpi radialis brevis (C5–C7), a radial extensor of the hand.
3. Extensor digitorum (C7–C8), an extensor of the metacarpophalangeal joints of the second through the fifth fingers. It is tested by having the patient extend the metacarpophalangeal joints against resistance.
4. Extensor digiti minimi (C7–C8), an extensor of the metacarpophalangeal joint of the fifth finger.
5. Extensor carpi ulnaris (C7–C8), an ulnar extensor of the hand that is tested by having the patient extend and adduct the hand at the wrist against resistance.
6. Abductor pollicis longus (C7–C8), an abductor of the metacarpal of the thumb. It is tested by having the patient abduct the carpometacarpal joint in a plane at right angles to the palm.
7. Extensor pollicis longus (C7–C8), an extensor of the thumb. It is tested by extending the thumb at the interphalangeal joint in a plane at right angles to the palm.
8. Extensor pollicis brevis (C7–C8), an extensor of the thumb that is tested by having the patient extend the thumb at the metacarpophalangeal joint against resistance.
9. Extensor indicis (C7–C8), an extensor of the second finger.
NERVE LESIONS
Lesions in the Axilla. Lesions of the posterior cord of the brachial plexus or high axillary lesions (e.g., due to crutches, shoulder dislocation, missile injuries) affect all the sensory and motor branches of the radial nerve. Lesions of the radial nerve at this location have been described as being due to nerve injury from the “windmill” pitching motion of competitive softball (windmill pitcher’s radial neuropathy) [338]. The following symptoms are observed:
Abnormal appearance of the hand. Characteristically, the hand hangs in flexion (wrist drop). There is wasting of the dorsal arm (triceps) and muscle mass on the posterior surface of the forearm.
Motor loss. There is paresis or paralysis of extension of the elbow, extension of the wrist, supination of the forearm, extension of all five metacarpophalangeal joints, and extension and abduction of the interphalangeal joint of the thumb. Elbow flexion tends to be weak. Abduction of the fingers is weak because the dorsal interossei require wrist flexion for their proper action. Ulnar involvement might be mistakenly assumed from this finding.
Reflexes signs. There is hyporeflexia or areflexia of the triceps (C6–C8) and radial (C5–C6) reflexes.
Sensory loss. There are paresthesias and sensory loss on the entire extensor surface of the arm and forearm and on the back of the hand and dorsum of the first four fingers.
Lesions of the Posterior Cutaneous Nerve of the Arm and Forearm. Entrapment of the posterior cutaneous nerve of the arm resulting in burning and tingling over the lower posterior arm may occur when the arm is drawn across the front of the body and the elbow is vigorously extended [218]. This purely sensory syndrome is likely due to the nerve stretch by tension from the long head of the triceps with extension during the above maneuvers, but it could also be due to posterior cutaneous nerve entrapment by the lateral head of the triceps. Isolated injury of the posterior cutaneous nerve of the arm or forearm may also be caused by injection, tourniquet application, arm injuries, and surgical procedures [67,69,94].
Lesions within the Spiral Groove of the Humerus. Lesions at this location are usually due to humeral fractures [111] or compressive lesions [55] (Saturday night palsy). The most common presentation of acute retrohumeral compression is one in which the subject wakens, often from a deep sleep (made deeper and perhaps more protracted by alcohol or sedatives), to find that he or she is unable to extend the wrist [55]. Tourniquet paralysis of the radial nerve may also occur. Newborns may have radial neuropathies related to fractures, lacerations, compression, or entrapment [103]. The radial nerve may also be entrapped by a musculotendinous arch of the lateral head of the triceps muscle [254] or damaged after repetitive arm exercise when a sudden forceful contraction and stretch of the arm muscles results in a delayed upper arm radial nerve palsy [362]. Soldiers may develop radial nerve palsies at the lateral border of the humerus after military shooting training owing to the persistent kneeling shooting posture [336]. The windmill pitching motion of competitive softball may also injure the nerve in the spiral groove (another form of windmill pitcher’s radial neuropathy) [338]. These patients have the same symptoms as those described previously for Lesions in the Axilla, except for the following modifications:
1. Sensibility on the extensor aspect of the arm is spared because this nerve usually arises high in the axilla.
2. Sensibility on the extensor aspect of the forearm may or may not be spared, depending on the site of origin of this nerve from the radial nerve proper.
3. The triceps muscle (and therefore the triceps reflex) is spared because the branches to the muscle have a proximal origin. The anconeus muscle is the most distal muscle spared in radial spiral groove lesions.
Differential involvement of the radial nerve fascicles along the spiral groove in “Saturday night palsy” might explain the variable presence of brachialis weakness or sensory impairment, either of which may be absent [359].
Lesions distal to the spiral groove and to the site of origin of the brachioradialis and extensor carpi radialis longus (prior to the bifurcation of the nerve) have symptoms that are similar to those seen with a spiral groove lesion, with the following exceptions:
1. The brachioradialis and extensor carpi radialis longus muscles are spared.
2. The radial reflex is spared.
3. Sensibility on the extensor surface of the forearm (posterior cutaneous nerve of the forearm) is more likely to be spared.
Progressive, severe, painless radial neuropathy may occur as a delayed complication of chronic intramuscular injection [236]. In patients with these symptoms, an exploration of the radial nerve revealed multifocal entrapment within the densely fibrotic triceps muscle at sites between the spiral groove and the distal course of the radial nerve near the elbow (chronic injection-induced triceps fibrosis). Isolated bilateral radial neuropathies distal to the radial groove at the posterolateral humerus have been described in a newborn [214]. The postulated mechanism included fetal activity for reasons including reduced amniotic fluid volume.
Lesions at the Elbow. The posterior interosseous nerve (deep motor branch of the radial nerve) may be injured or entrapped at the elbow [76,106]. Entrapment may be caused by the following:
1. A constricting band at the radiohumeral joint capsule
2. The sharp edge of the extensor carpi radialis brevis muscle
3. A fibrotendinous arch where the nerve enters the supinator muscle (arcade of Frohse) [56,348]
4. Its occurrence within the substance of the supinator muscle (supinator channel syndrome)
5. Other etiologies [76], such as lacerations and gunshot wounds; closed injuries due to fractures of the proximal radius or both radius and ulna; chronic repeated trauma related to stressful supination and pronation in swimmers, frisbee players, tennis players, violinists, and orchestra conductors [106,204,216]; nerve compression by the repetitive movements of the forearm (upholsterer’s posterior interosseous neuropathy) [402]; carrying a knapsack supported by a hyperpronated and extended wrist with the elbow in a flexed position (knapsack paralysis) [282]; the use of a Canadian (Lofstrand) crutch [118]; brachiocephalic arteriovenous fistula constriction (due to severe compression from a hypertrophied venous limb of the arteriovenous fistula) [317], iatrogenic due to radial head resection and injury secondary to tumor removal; rheumatoid arthritis [278]; local mass (e.g., lipoma, fibroma, ganglia, traumatic aneurysm of the posterior interosseous artery, chondroma, neurofibroma, schwannoma) [106,404]; and amyloid neuropathy with multiple myeloma [307]
When the posterior interosseous nerve is damaged at these locations, the supinator muscle and the superficial sensory branch of the radial nerve are often spared. Patients with this condition have atrophy and paresis of the extensor carpi ulnaris, extensor digitorum, extensor digiti minimi, abductor pollicis longus and brevis, and extensor indicis. Because the extensor carpi radialis is unaffected while the extensor carpi ulnaris is paretic, the wrist deviates radially, especially when the patient attempts to make a fist. The patient has difficulty in extending the metacarpophalangeal joints of all five fingers (drop-finger deformity), extending the wrist in an ulnar direction, extending the interphalangeal joint of the thumb, and abducting the thumb. Occasionally, an isolated paralysis of the descending motor branch of the posterior interosseous nerve may occur (e.g., due to constriction in the distal portion of the supinator muscle), resulting in a “drop-thumb” deformity owing to paresis of the extensor pollicis longus and brevis and abductor pollicis longus (the extensor indicis may also be involved) [146].
Some patients with radial or posterior inter-osseous nerve palsy demonstrate apparent weakness of ulnar-innervated muscles, such as the dorsal and palmar interossei and the abductor digiti minimi muscles [311]. These muscles insert on the extensor expansions, and their activation is associated with concomitant contraction of finger flexors and extensors. This apparent weakness may be due to their unopposed traction on the extensor expansion by the paralyzed extensor digitorum [311].
A focal myopathy that causes weakness of extension of the right index, middle, and fourth fingers at the metacarpal–phalangeal joints with no sensory deficit, thereby mimicking a posterior interosseous nerve syndrome, has been described [102].
Lesions of the Superficial Branch of the Radial Nerve (Cheiralgia Paresthetica). The superficial cutaneous branch of the radial nerve may be injured anywhere along its location in the forearm, resulting in a pure sensory syndrome (paresthesias and sensory loss) that affects the radial part of the dorsum of the hand and the dorsal aspect of the first three-and-a-half fingers. This neuropathy is sometimes called Wartenberg’s syndrome or cheiralgia paresthetica. (The autonomous zone of sensory loss occurs on the area of skin covering the first interosseous space.) Radial sensory entrapment [87] usually occurs with crush or twisting injuries to the wrist or forearm or may follow repetitive pronation– supination movements required in certain occupations. Pain or burning over the dorsomedial wrist with this entrapment is aggravated by pinching and gripping activities, and a positive Tinel’s sign may occur with percussion over the radial sensory nerve, especially where it exits from the deep fascia. The hyperpronation provocative test (pronation of the forearm with the ulnar flexion of the wrist) is often positive. The superficial cutaneous branch may also be entrapped in the forearm between the tendons of the brachioradialis and extensor carpi radialis muscles (here the nerve transits from the deep to the superficial branch) [86,347]. The nerve may be injured by handcuffs compressing the nerve against the distal radius (a type of handcuff neuropathy) [130,224,361]; by compression from wristwatch bands, bracelets, roped hands, or a cast; by direct nerve trauma or forearm lacerations; by nerve tumors; or as a complication of de Quervain’s tenosynovectomy.
Lesions of the Dorsal Digital Nerves. As noted in the preceding text, the dorsal digital nerves are formed from the superficial radial nerve and the dorsal cutaneous branch of the ulnar nerve (Fig. 2.8). The dorsal digital nerves that arise from four or five terminal branches of the superficial branch of the radial nerve supply the dorsal aspect of the thumb (through two branches) and the dorsal aspects of the second and third digits and the medial fourth digit. Sensory signs and symptoms occur in the distribution of the involved branches. For example, paresthesias and sensory loss confined to the radial side of the thumb may occur with a lesion of the distal dorsal digital nerve (in the thumb) [229]. Etiologies of dorsal digital neuropathies are as described earlier under Lesions of the Palmar Digital Branches of the Median Nerve.
Pseudoradial Nerve Palsy. Isolated flaccid weakness of the hand, predominantly affecting the wrist extensors and causing wrist drop, may rarely be due to a cerebral cortical infarct located in the precentral “hand knob” area [19].

FIG. 2.8. Dorsal view of the right hand, showing the dorsal digital nerves formed from the superficial radial and dorsal ulnar cutaneous nerves.
Medial Cutaneous Nerves of the Arm and Forearm (C8–T1)
ANATOMY
These two purely sensory branches arise from the medial cord of the brachial plexus. The medial cutaneous nerve of the arm supplies the skin of the axilla and the medial part of the arm. The medial cutaneous nerve of the forearm divides above the elbow into anterior and posterior divisions that supply the skin of the anteromedial and posteromedial forearms, respectively, down to the wrist.
NERVE LESIONS
Injuries to the medial cutaneous nerve of the arm and forearm nerves may occur in the axilla, affecting the medial cord of the brachial plexus. A sensory loss occurs in the distribution of the individual nerve branches. The medial cutaneous nerve of the forearm may be affected in isolation by a stretch injury or by injury due to the placement of an arterial graft [68]. The nerve may also be damaged as a complication of an ulnar nerve surgery at the elbow [85].
Intercostobrachial Nerve (T2)
The intercostobrachial nerve arises as the lateral cutaneous branch of the second intercostal nerve. It crosses the axilla and the medial side of the arm within the subcutaneous tissue supplying the skin of these regions. The axilla is part of the T-1 and T-2, and perhaps T-3 dermatomes. The intercostobrachial nerve is formed by predominantly T-2 fibers. Nerve injury results in pain and dysesthesia in the axilla and medial arm. Similar axillary sensory impairment can be caused by radiculopathies involving the upper thoracic roots, C-8 and T-1 root avulsions, and lower trunk brachial plexopathies, but the sensory disturbance with these lesions will involve surrounding areas in the corresponding dermatome and also are frequently accompanied by pain, weakness, and sometimes involvement of sympathetic fibers.
The intercostal brachial nerve is possibly the largest sensory nerve in the body and damage to the nerve may occur often following surgeries for breast cancer and axillary lymphadenectomy [51,217,370,372]. Less frequently it can be injured from anesthesia for procedures in the arm, compression by a tourniquet or mechanical pressure therapy devices, entrapment, nerve traction, neoplastic compression or invasion, and radiotherapy [23,167,199,217,220,370,403]. A case of intercostobrachial mononeuropathy has been described caused by compression of the nerve in the axilla induced by pulling an unconscious woman by the axilla [220].
Iliohypogastric (T12–L1), Ilioinguinal (L1), and Genitofemoral (L1–L2) Nerves
ANATOMY AND NERVE LESIONS
The mixed iliohypogastric nerve arises from the anterior rami of spinal root segments T12 and L1. The nerve runs across the psoas muscle and then behind the kidney, crossing the quadratus lumborum muscle and reaching the iliac crest. It then pierces the internal oblique and transversus abdominis muscles, both of which it supplies. It terminates in the lateral cutaneous branch a sensory nerve that supplies the skin over the outer buttock and hip, and the anterior cutaneous branch a sensory branch that supplies the anterior abdominal wall above the pubis.
This nerve may be injured in the lumbar plexus, at the posterior or anterior abdominal wall, or distally near the inguinal ring. Lesions of this nerve result in little motor deficit but lead to pain or sensory loss in the area of the cutaneous supply of the nerve. Painful iliohypogastric neuropathies are not uncommon after lower abdominal surgery [365].
The mixed ilioinguinal nerve arises from the anterior ramus of the first lumbar spinal segment within the psoas muscle. It runs laterally and downward, parallel with the iliohypogastric nerve, to reach the iliac crest. This nerve, such as the iliohypogastric, supplies the internal oblique and transversus abdominis muscles. After piercing these two muscles, it enters the inguinal canal and passes to the superficial inguinal ring, from which its sensory fibers emerge. These fibers are distributed to the skin of the medial thigh below the inguinal ligament as well as to the skin of the symphysis pubis and the external genitalia.
This nerve may be injured in the lumbar plexus, at the posterior abdominal wall, at the anterior abdominal wall, or within the inguinal canal. Painful ilioinguinal neuropathies are not uncommon after lower abdominal surgery (e.g., herniorrhaphy or appendectomy) [82,354,365], and entrapment of the nerve as it passes through the muscles of the abdominal wall, medial to the anterior superior iliac spine, has been described [198]. Neuropathy may occur after pregnancy, likely due to the stretching of the nerve [36,339]. Lower abdominal and inguinal pain and paresthesias in professional ice hockey players were found to be due to multiple tears of the external oblique muscle and aponeurosis causing ilioinguinal nerve entrapment [202]. Lesions of this nerve cause the ilioinguinal syndrome, which consists of pain and sensory loss in the inguinal region. Motor findings are negligible.
Although the ilioinguinal and iliohypogastric nerves typically lie outside the gynecologic field of operation, they may become susceptible to injury when the Pfannenstiel incision is extended beyond the lateral border of the rectus abdominis muscle, into the substance of the internal oblique muscle [160]. The symptoms are attributed to suture incorporation of the nerve during fascial repair, direct nerve trauma with subsequent neuroma formation, or neural constriction as a result of the normal scarring and healing processes. The diagnostic triad for ilioinguinal/iliohypogastric nerve postsurgical entrapment syndrome consists of the following [160]:
1. Sharp, burning pain emanating from the incision site and radiating to the suprapubic, labial, or thigh areas
2. Paresthesia over the appropriate nerve distribution
3. Pain relief after infiltration with a local anesthetic
The onset of symptoms may be immediate or may occur months to years after the offending surgical procedure. The symptoms are exacerbated as a result of stretching, coughing, sneezing, and valsalva and can be relieved with hip flexion or by adopting a stooped posture when ambulating [160].
In a study of 33 patients with ilioinguinal and iliohypogastric neuralgias, 29 (88%) of them had injuries from iatrogenic causes, and four (12%) had injuries caused by blunt trauma [186]. In the 23 isolated ilioinguinal neuralgias, operation associated with neuralgias in 13 (57%) was a herniorrhaphy followed by four (17%) after an appendectomy and three (13%) after a hysterectomy. Three (13%) patients had neuralgias resulting from blunt trauma. Nine (90%) of 10 ilioinguinal-iliohypogastric lesions were caused by iatrogenic causes, and 1 (10%) neuralgia resulted from blunt trauma [186]. In another study of 264 cases of neuralgia of the pelvic plexus and nerves treated surgically, 25 were cases of solely ilioinguinal neuralgia and 24 were cases of combined ilioinguinal neuralgias [384]. Of these, iatrogenic injury was the most common etiology.
The genitofemoral nerve, a predominantly sensory nerve, arises from the first and second lumbar segments within the substance of the psoas muscle. It traverses the psoas muscle and, near the inguinal ligament, divides into two branches: external spermatic (genital branch) and lumboinguinal (femoral branch). The external spermatic (genital) branch (mainly L1) enters the deep inguinal ring, traverses the inguinal canal, and ends in the cremaster muscle and skin of the scrotum (or labia majoris) and adjacent medial thigh. The lumboinguinal (femoral) branch (mainly L2) passes behind the inguinal ligament lateral to the femoral artery and supplies the skin of the upper thigh over the femoral triangle.
Injury to this nerve may occur in the lumbar plexus, within the abdomen, or in the femoral or inguinal region [82,251,354] (e.g., after inguinal herniorrhaphy, appendectomy, cesarean section, hysterectomy, vasectomy, blunt abdominal trauma, and even due to wearing tight jeans [259]). Among 30 patients undergoing herniorrhaphy, 14 (47%) showed motor involvement of the genitofemoral nerve on electrophysiologic studies, whereas 6 of 26 (23%) patients not treated surgically had involvement of this nerve [20]. These findings indicate that subclinical motor involvement of the genitofemoral nerve is common after inguinal herniorrhaphy, but the herniated mass itself may also be responsible for motor involvement of this nerve in some patients before surgery. Postoperative injury to this nerve is most likely to occur during the removal of a large pelvic mass adherent to the sidewall or when biopsy or removal of the external iliac lymph nodes is performed [160]. Injury causes pain (genitofemoral neuralgia) and sensory loss in the area of the cutaneous supply of the nerve. The cremasteric reflex, which is subserved by this nerve, may be lost on the side of the nerve lesion.
Femoral Nerve (L2–L4)
ANATOMY
The femoral nerve, a mixed nerve, (Fig. 2.10) arises within the substance of the psoas muscle from the posterior rami of the second, third, and fourth lumbar segments. The nerve runs in the groove between the psoas and iliacus muscles (flexors of the thigh, both of which it supplies) and descends beneath the inguinal ligament (lateral to the femoral artery) to enter the thigh. Just distal to the inguinal ligament within the femoral triangle, it separates into the anterior and posterior divisions. The anterior division divides almost immediately into a muscular branch (to the sartorius muscle, a flexor, and evertor of the thigh) and a sensory branch, the anterior femoral cutaneous nerve that supplies the skin of the anterior and medial aspects of the thigh. The anterior cutaneous branch further divides into the intermediate femoral cutaneous nerve and the medial femoral cutaneous nerve. The medial femoral cutaneous nerve has an anterior branch that innervates the anteromedial thigh and a posterior branch that innervates the medial aspect of the leg just below the knee. The posterior division of the femoral nerve immediately divides into the sensory saphenous nerve and muscular branches. The muscular branches of the posterior division of the femoral nerve supply the following muscles:
1. Pectineus muscle (L2–L3), an adductor, flexor, and evertor of the thigh.
2. Quadriceps femoris muscle (L2–L4), an extensor of the leg. It is tested by having the patient extend the leg against resistance with the extremity flexed at the hip and knee. This muscle is also, particularly through the rectus femoris, an extensor of the thigh. The tendon of this muscle subserves the patellar reflex.
The saphenous nerve descends to the knee in the adductor (Hunter’s) canal, accompanied by the femoral artery, and becomes cutaneous between the tendons of the sartorius and gracilis muscles. It then joins the great saphenous vein and proceeds to the medial aspect of the leg. It supplies the skin over the medial aspect of the lower leg as far as the medial malleolus.
NERVE LESIONS
The most common cause of femoral neuropathy is trauma, usually iatrogenic [184,200]. Common iatrogenic causes include inguinal herniorrhaphy, total hip replacement, intraabdominal vascular or gynecologic operations, and, less commonly, appendectomy, lumbar sympathectomy, laparoscopic procedures and inadvertent suturing of the nerve during abdominal hysterectomy [160,184,200,320]. A proximal femoral neuropathy may occur with pelvic surgery (e.g., hysterectomy) owing to the direct pressure exerted by the retractor blades or by an indirect compression of the nerve by compression of the adjacent psoas muscle by the tip of a retractor blade; the neuropathy may be bilateral [201]. In one study, improper placement of self-retaining or fixed retractors was the most common cause of femoral nerve injury arising in association with abdominal surgical procedures [160]. Unilateral or bilateral femoral neuropathy may also occur after surgery or childbirth in the lithotomy position, likely due to the compression of the nerve against the inguinal ligament or the excessive stretch of the nerve by abduction and external rotation of the thighs [9]. Other causes of femoral neuropathy while the patient is in the lithotomy position (e.g., for normal delivery, vaginal hysterectomy, or laparoscopy) include an iliopsoas or retroperitoneal hematoma, especially in patients with a bleeding diathesis [407]; compression by the fetal head, especially after a difficult delivery or the use of forceps [93]; or ischemia, especially with a history of intraoperative hypotension [5]. In patients undergoing vaginal surgery, maximal compression of the femoral nerve and subsequent traction-induced femoral neuropathy occur when patients are positioned in lithotomy with excessive hip flexion, hip abduction, and external hip rotation, resulting in an 80- to 90-degree extreme angulation of the femoral nerve beneath the unyielding inguinal ligament and subsequent compression injury [160]. Awareness of what constitutes proper lithotomy positioning preoperatively, and assurance that patients are appropriately positioned before initiating the procedure, will serve to significantly reduce the risk of both sciatic nerve injury (see subsequent text) and femoral nerve injury intraoperatively [160]. In a study of 264 cases of neuralgia of the pelvic plexus and nerves treated surgically, 119 patients underwent surgical exploration for femoral nerve injury [384]. Seventy-five percent of these patients had femoral nerve injuries attributable to trauma (iatrogenic versus penetrating injuries), and the remaining 25% of patients had cystic masses or tumors.

FIG. 2.10. The femoral nerve.
Femoral neuropathy may also follow renal transplantation with possible pathophysiology including direct nerve compression and nerve ischemia [329]. A pseudoaneurysm of the profunda femoral artery, formed after cardiac catheterization or percutaneous transluminal coronary angioplasty, may cause femoral nerve compression [166]. Femoral nerve damage may also occur in the course of renal transplantation owing to hematoma at the operative site [340]. Iliopsoas hemorrhage due to anticoagulation or hemophilia may damage the femoral nerve and is associated with deep loin, back, and groin pain as well as neuralgic pain in a femoral cutaneous distribution [200]. Delayed femoral neuropathy may also occur after inguinal radiation (usually developing 12–16 months after treatment) and is associated with a palpable mass of dense scar in the groin [203]. In intravenous drug abusers, iliopsoas infarction and acute femoral neuropathy may occur; this femoral involvement may be due to ischemia, inflammation, or compression of the nerve along its course through the iliopsoas muscle [173].
Femoral nerve injury may also be due to penetrating gunshot and stab wounds, blunt injuries, lacerations, femoral artery cannulation, and stretch or contusion injuries associated with pelvic fractures [184,200]. Acute stretch injuries may occur in gymnasts or dancers performing hyperextension hip exercises [237]. Tumors, including neurofibromas, schwannomas, sarcomas, ganglion cysts, leiomyosarcoma, metastases, and abscesses may also injure the nerve [184]. A large synovial cyst of the underlying hip joint in the extrapelvic part of the iliopsoas and external obturator muscles resulted in combined femoral and obturator nerve compression in one patient [366]. Ischemic neuropathy of the femoral nerve may occur in patients with diabetes. A localized hypertrophic mononeuropathy of the femoral nerve with progressive weakness and atrophy of the thigh has also been described [369].
Severe, combined, bilateral femoral and sciatic neuropathies have been described in the context of alcohol intoxication (hanging leg syndrome) [318]. The findings were consistent with severe bilateral femoral neuropathies localizing to the inguinal ligaments combined with severe bilateral proximal sciatic neuropathies corresponding to the sites of compression near the gluteal sulci. The suspected mechanism of femoral nerve injury is traction and compression of the inguinal nerve segment as it passes over the fulcrum of the superior pubic ramus.
A proximal lesion of the femoral nerve (e.g., at the lumbar plexus or within the pelvis) results in the following signs:
1. Atrophy. There is wasting of the musculature of the anterior part of the thigh.
2. Motor signs. There is weakness or paralysis of hip flexion (iliacus, psoas, and rectus femoris muscles) and an inability to extend the leg (quadriceps femoris). With paralysis of the sartorius muscle, lateral thigh rotation may be impaired.
3. Sensory symptoms and signs. Sensory loss, paresthesias, and, occasionally, pain occur on the anteromedial thigh and inner leg as far as the ankle.
4. Reflex signs. The patellar reflex is depressed or absent.
Lesions at the inguinal ligament result in similar findings, but thigh flexion is spared because of the more proximal origin of the femoral nerve branches to the iliacus and psoas muscles. A purely motor syndrome (quadriceps atrophy and paresis) may result from lesions within the femoral triangle that affect the posterior division of the femoral nerve distal to the origin of the saphenous branch. For example, isolated quadriceps paresis and atrophy may be due to localized nerve injury in weight lifters [44], selective atrophy of the distal portion of the vastus lateralis muscle followed by distal branch neuropathy due to stretching and compression of the nerve during strenuous exercise [265], and a muscle biopsy caused distal wasting of the vastus lateralis by injuring the distal femoral nerve [337]. Unilateral or bilateral anterior femoral cutaneous nerve injury, clinically sparing femoral branches to the saphenous nerve and quadriceps muscles, may occur following surgical dissection in the femoral triangles with femoral artery reconstructive surgery [32]. This purely sensory syndrome manifests by anterior-medial thigh pain and numbness and may occur after aortofemoral bypass graft surgery and other types of femoral artery reconstructive surgery. Isolated medial femoral cutaneous neuropathy, resulting in paresthesias and dysesthesias over the anteromedial thigh, after penetrating injury to the anteromedial aspect of the thigh has been described [209].
A purely sensory syndrome (pain, paresthesias, and sensory loss) may result when the saphenous nerve alone is damaged. The nerve may be entrapped proximally in the thigh by fibrous bands or branches of femoral vessels [250]. Isolated saphenous involvement may occur with femoral thrombectomy and femoral-popliteal bypass surgery [4] and after popliteal vein aneurysm resection with saphenous vein interposition [333]. Schwannomas of the nerve may develop in the thigh [99]. Spontaneous saphenous neuralgia [213] may result from nerve compromise in the subsartorial canal where the nerve crosses the femoral artery superficially and penetrates the roof of the canal. Medial knee and leg pain result, and tenderness over the subsartorial canal is present. The saphenous nerve may be damaged at the knee after medial arthrotomy or arthroscopy, in association with coronary artery bypass graft surgery, and by lacerations [205]. This nerve is most susceptible to injury where it pierces the aponeurotic roof of the adductor canal above the knee. Surfers who sit astride their boards and grip the boards between their knees may develop nerve compression (surfer’s neuropathy) [105]. A meniscal cyst can compress the nerve at the knee [394]. In all these syndromes, the only sign is a sensory disturbance that affects the medial side of the lower leg.
Damage to the infrapatellar branch of the saphenous nerve results in numbness and paresthesias in the skin over the patella (gonyalgia paresthetica) [223]. When bending the knee, occasional pins-and-needles sensations are produced. Gonyalgia paresthetica usually develops insidiously without acute trauma and is often accompanied by sharp pain below and lateral to the knee. The infrapatellar branch may be injured during arthroscopy or other knee operations, by accidental trauma, or by nerve compression [154].
Obturator Nerve (L2–L4)
ANATOMY
The obturator nerve, a mixed nerve, (Fig. 2.11) arises from the anterior primary rami of the second, third, and fourth lumbar segments within the substance of the psoas muscle. The nerve courses along the pelvis and enters the obturator canal. Within the obturator canal, it supplies the obturator externus muscle and then divides into two branches, the anterior and posterior branches, which descend into the medial thigh. The mixed anterior division supplies the pectineus, adductor longus, and adductor brevis (adductors of the thigh), and the gracilis (an internal rotator of the thigh and flexor of the knee) and ends in a sensory terminal branch that supplies the skin over the medial thigh. The motor posterior division supplies the obturator externus, adductor magnus, and adductor brevis muscles (adductors of the thigh). The adductor magnus may also be innervated by the sciatic nerve. Motor function subserved by the obturator nerve is evaluated by having the patient adduct the extended leg against resistance.

FIG. 2.11. The obturator nerve and the lateral femoral cutaneous nerve.
NERVE LESIONS
The obturator nerve may be damaged within the lumbar plexus, near the sacroiliac joint, on the lateral pelvic wall, or within the obturator canal. Obturator neuropathy may result from orthopedic, gynecological, or urological procedures or injuries [192]. Nerve damage may occur with obturator hernia, after cancer surgery in the pelvis, secondary to iliopsoas hemorrhage, with pelvic fractures, with pelvic trauma, after pelvic surgery, after femoral artery procedures, after bilateral total knee arthroplasty with prolonged tourniquet use, and after hip surgery (e.g., due to nerve traction or encasement of the nerve by a spur of methylmethacrylate cement) [233,344]. From a gynecologic standpoint, the obturator nerve is most frequently injured during retroperitoneal surgery for gynecologic malignancies or endometriosis [160]. The node-bearing tissues of the obturator space obscure the location of the obturator nerve and predispose it to injury. Obturator nerve injury can also occur at the time of paravaginal defect repair, performed to address symptomatic lateral displacement cystocele [160]. Bilateral obturator nerve injuries may occur during urologic surgery owing to prolonged hip flexion, resulting in the stretching of each nerve at the bony obturator foramen [270]. Prolonged or difficult labor may cause neuropathy by the compression of the nerve between the fetal head and the bony pelvic wall [389]. Other etiologies of neuropathy include endometriosis, obturator hernias, lipomatosis of the nerve, nerve sheath tumors, obturator nerve ganglion, metastasis to the obturator canal, myositis ossificans, and nerve entrapment by thickened fascia overlying the adductor brevis muscle described in athletes [49,50,242,257,290,321,323,344]. A large synovial cyst of the underlying hip joint in the extrapelvic part of the iliopsoas and external obturator muscles resulted in combined femoral and obturator nerve compression in one patient [366].
Obturator mononeuropathy in cancer patients is rare, but it may be the sole presenting sign of new or recurrent pelvic tumor or may occur as a complication of tumor surgery [169,298,316]. Tumor sites on pelvic computed tomography scan that correlate with obturator nerve compression or infiltration include the posterolateral wall of the upper pelvis or midpelvis, the anterior wall of the lower pelvis, and the external obturator and pectineus muscles extrinsic to the bony pelvis [298].
Patients with obturator neuropathy complain leg weakness and cannot stabilize the hip joint. Nerve lesions result in wasting of the musculature of the inner aspect of the thigh, paresis of adduction of the thigh, and a sensory disturbance affecting the medial aspect of the thigh.
Obturator neuralgia, consisting of pain radiating from the obturator nerve territory to the inner thigh, may occur from compression of the obturator nerve in the obturator canal [295]. The pain is characterized by its localization in the inguinal region and anterointernal side of the thigh, going down to the internal side of the knee. It is worse when standing or in a monopodal stance and walking may cause the pain and a limp.
Lateral Femoral Cutaneous Nerve (L2–L3)
ANATOMY
The lateral femoral cutaneous nerve, a purely sensory nerve, (Fig. 2.11) derives from the primary rami of the second and third lumbar segments within the substance of the psoas muscle. It penetrates the psoas and crosses the iliacus muscle to the anterior superior iliac spine. It then passes medially to the spine beneath the inguinal ligament and enters the thigh beneath the fascia lata. The nerve runs downward and divides into two branches: the anterior division, which supplies the skin of the anterior thigh to the knee, and the posterior division, which supplies the skin of the upper half of the lateral aspect of the thigh.
NERVE LESIONS
The nerve is often damaged within the abdomen (e.g., by iliopsoas hemorrhage) or in the inguinal region [168]. Prolonged sitting in the lotus position may cause a lateral femoral cutaneous neuropathy (a form of lotus neuropathy) [227]. Compression or angulation of the nerve by the inguinal ligament near the anterior superior iliac spine may result in acute or subacute pain and paresthesias along an oval area on the lateral or anterolateral aspect of the thigh. These paresthesias are associated with sensory loss in the cutaneous distribution of the lateral femoral cutaneous nerve (meralgia [meros, thigh; algos, pain] paresthetica or Bernhardt-Roth syndrome) [252,390,400]. This sensory syndrome occurs especially in obese individuals who wear constricting garments (e.g., corsets, carpenters’ belts) and may be bilateral. Tight-fitting pants (e.g., hip-huggers) may be a precipitating factor for meralgia paresthetica, especially in thin persons with an aberrant pathway of the lateral femoral cutaneous nerve [268]. Meralgia paresthetica has also been reported from seat-belt trauma; after long-distance walking or cycling, iliac bone procurement for grafting, after abdominal surgery including abdominal hysterectomy by a suprapubic approach (thought to be due to prolonged postprocedure hip flexion to relieve the abdominal incisional pain); as a complication of a groin flap or renal surgery; after trauma; after total hip arthroplasty; or with malignant tumor of the psoas muscle [12,25,35,37,164,182,384]. Nerve injury at the time of pelvic surgery may result from the inappropriate placement of lateral retractor blades associated with self-retaining or fixed retractors [160].
Seror and Seror reported the clinical and electrophysiological examinations in 131 cases of meralgia paresthetica among 120 unselected patients, 69 men and 51 women, aged 15 to 81 years [328]. All patients experienced permanent or intermittent pain and all but one had permanent sensory impairment of the thigh. The lateral aspect of the thigh was solely involved in 88 cases and the anterior aspect was also or exclusively involved in 32 cases. The right thigh was involved 62 times and the left 58 times. Symptom duration varied from 2 weeks to 20 years. Two cases had undergone previous spine surgery for presumed disk herniation with no benefit. A precise cause could explain the lateral femoral cutaneous nerve lesion in 46 cases, the other 74 cases being considered idiopathic (25% of patients were obese) [328].
Gluteal Nerves (L4–S2)
ANATOMY AND NERVE LESIONS
The gluteal nerves, purely motor nerves (Fig. 2.12) include the superior gluteal (from rami L4–S1) and inferior gluteal (from rami L5–S2) nerves, which supply the musculature of the buttocks. The superior gluteal nerve leaves the pelvis by way of the greater sciatic notch above the piriformis muscle (suprapiriform foramen) to supply the gluteus medius (L4–Sl), gluteus minimus (L4–Sl), and tensor fasciae latae (L4–Sl) muscles, which are abductors and internal rotators of the thigh. These muscles are especially important in maintaining the horizontal plane of the pelvis during walking.
Lesions of the superior gluteal nerve may occur within the lumbosacral plexus, pelvis, greater sciatic foramen, or buttock. Etiologies of superior gluteal neuropathy include hip surgery, pelvic or hip trauma, hip fracture or dislocation, iliac artery aneurysm, fall on the buttock, injection, and entrapment of the nerve between the tendinous edge of the piriformis muscle and the ilium [2,132,287,288,373,401]. On walking, the pelvis tilts toward the side of the unaffected raised leg (Trendelenburg’s sign). There is paresis or paralysis of thigh abduction and medial rotation. Isolated complete paralysis of the tensor fasciae latae may develop secondary to intramuscular injection [249].
The inferior gluteal nerve leaves the pelvis by way of the greater sciatic notch below the piriformis muscle (infrapiriform foramen), at which point it is near the sciatic nerve and the posterior cutaneous nerve of the thigh. This nerve sends its branches to the gluteus maximus muscle (L5–S2), the main hip extensor, which is tested by having the patient extend the thigh against resistance.
The inferior gluteal nerve may be injured within the lumbosacral plexus, pelvis, greater sciatic foramen, or buttock. Nerve palsy results in paresis or paralysis of hip extension, which is most noticeable when the patient attempts to climb stairs.
Mononeuropathies of inferior and superior gluteal nerves due to hypertrophy of piriformis muscle have been described in a basketball player [243].
Posterior Femoral Cutaneous Nerve (S1–S3)
ANATOMY AND NERVE LESIONS
The posterior femoral cutaneous nerve, a purely sensory nerve arises from the anterior primary rami of the first through the third sacral segments. It leaves the pelvis through the greater sciatic notch and descends into the buttock deep into the gluteus muscle. It supplies the skin of the posterior thigh and popliteal fossa.
Damage to this nerve (which may occur in the sacral plexus, greater sciatic foramen, or buttock) results in a sensory disturbance in the cutaneous area of supply of the nerve. Neuropathy may be due to injections, lacerations, falls onto the buttocks, presacral tumors, and prolonged bicycle riding [14,162,188]. Posterior femoral cutaneous neuralgia due to a venous malformation consists of attacks of pain in the lateral scrotum, posterolateral perineum, and posterior thigh to the popliteal fossa [72].
Pudendal Nerve (S1–S4)
ANATOMY AND NERVE LESIONS
The pudendal nerve originates from the anterior rami of the first through the fourth sacral segments. It leaves the pelvis through the greater sciatic notch below the piriformis muscle (infrapiriform foramen) and reaches the perineum. This mixed nerve supplies motor branches to the perineal muscles and external anal sphincter, as well as sensory branches to the skin of the perineum, penis (or clitoris), scrotum (or labia majus), and anus.

FIG. 2.12. The sciatic nerve proper, superior gluteal nerve, and inferior gluteal nerve.
The pudendal nerve may be injured by buttock injections, pelvic fractures, hip surgery, and prolonged bicycle riding (pedaller’s penis) [128,145,234]. Nerve compression by pelvic varices has also been described [248]. Lesions of this nerve produce a sensory disturbance in the cutaneous area of supply of these nerves, erectile impotence, and difficulty with bladder and bowel control. Injury to the pudendal nerve at the time of vaginal surgery usually occurs in association with sacrospinous ligament fixation for vaginal vault prolapse [160]. As the pudendal nerve exits the pelvis via the greater sciatic foramen, it runs directly behind the lateral one-third of the sacrospinous ligament before turning to reenter the pelvis through the lesser sciatic foramen. It is at this point that the surgeon can unknowingly entrap the pudendal nerve within the suture used to secure the apex of the vagina to the ipsilateral sacrospinous ligament. Incorporation of the pudendal nerve within this suture will result in immediate or delayed postoperative gluteal pain and associated perineal anesthesia or paresthesia [160]. Motor abnormalities are usually absent.
Sciatic Nerve (L4–S3) and Its Branches
SCIATIC NERVE PROPER
The sciatic nerve, a mixed nerve (Fig. 2.12), the largest in the body, derives from the fourth and fifth lumbar and the first and second sacral spinal segments. It emerges from the sacral plexus and leaves the pelvis through the greater sciatic foramen below the piriformis muscle (infrapiriform foramen). The nerve then curves laterally and downward beneath the gluteus maximus muscle; in the posterior aspect of the thigh, it innervates the semitendinosus (L4–S2), semimembranosus (L4–S2), and biceps femoris (L4–S2) muscles (i.e., the hamstring muscles, which are flexors of the knee joint) and the adductor magnus (L2–L4) muscle, an adductor of the thigh (which is also supplied by the obturator nerve). The nerve proceeds downward in the thigh, and at the apex of the popliteal fossa, it divides into its two terminal branches, the tibial (medial popliteal) nerve (L4–S3) and the common peroneal (lateral popliteal) nerve (L4–S2).
TIBIAL NERVE
The tibial nerve (Fig. 2.13) crosses the middle of the popliteal space and courses down the back of the leg. In the popliteal fossa, it gives off the medial sural cutaneous nerve. This branch supplies the skin on the calf and then joins the lateral sural cutaneous nerve (a branch of the common peroneal) at the level of the Achilles tendon, forming the sural nerve. The sural nerve supplies the skin on the lateral heel and lateral aspect of the foot and small toe.
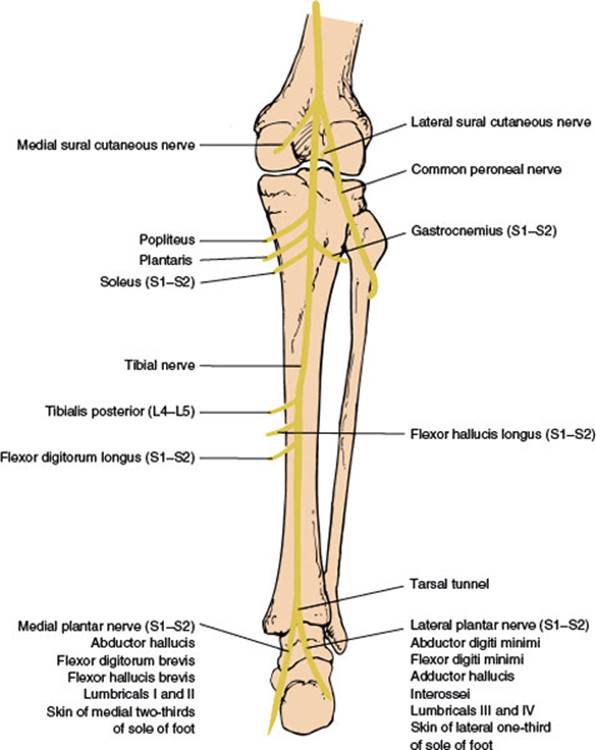
FIG. 2.13. The tibial nerve.
In the distal popliteal fossa, the tibial nerve sends branches to the gastrocnemius (S1–S2) and soleus (S1–S2) muscles, which are the main plantar flexors of the foot, and to the popliteus and plantaris muscles. The nerve then descends in a plane between the gastrocnemius and soleus muscles posteriorly and the tibialis posterior anteriorly. Here it gives off branches to the following three muscles:
1. Tibialis posterior (L4–L5), a plantar flexor and invertor of the foot. It is tested by having the patient invert the foot against resistance or walk on the toes. Inversion should be tested with the foot in complete plantar flexion, thereby eliminating the action of the tibialis anterior.
2. Flexor digitorum longus (L5–S2), a plantar flexor of the foot and of all the toes except the large toe. It is tested by having the patient flex the toes against resistance.
3. Flexor hallucis longus (S1–S2), a plantar flexor of the foot and that of the terminal phalanx of the great toe. It is tested by having the patient plantar flex the great toe against resistance.
The tibial nerve then passes inferior to the medial malleolus along with the tendons of the tibialis posterior, flexor hallucis longus, and flexor digitorum longus muscles and the posterior tibial artery and vein. At this location, the lancinate ligament roofs over these structures to form a fibroosseous tunnel (the tarsal tunnel). Within the tunnel the nerve divides into the medial plantar, the lateral plantar, and the medial calcaneal nerves [269]. The medial plantar nerve (S1–S2) supplies the skin of the medial two-thirds of the sole of the foot and innervates the abductor hallucis, flexor digitorum brevis, flexor hallucis, and the first two lumbricals of the foot. The lateral plantar nerve (S1–S2) carries sensation to the lateral third of the foot and innervates the abductor digiti minimi pedis, flexor digiti minimi, adductor hallucis, interossei, and the third and fourth lumbricals of the foot. The medial calcaneal branch supplies the skin of the medial aspect of the heel.
COMMON PERONEAL NERVE
The common peroneal nerve (Fig. 2.14) gives off the lateral sural cutaneous nerve in the popliteal fossa. This branch joins the medial sural cutaneous nerve (from the tibial nerve) to form the sural nerve. In the popliteal fossa, the common peroneal also gives off the lateral cutaneous nerve of the calf, which descends along the lateral head of the gastrocnemius muscle to supply the skin on the lateral aspect of the leg below the knee. The common peroneal nerve then rounds the head of the fibula and enters the substance of the peroneus longus muscle, where it divides into two branches: the deep peroneal (anterior tibial) nerve and the superficial peroneal nerve. The deep peroneal nerve gives motor branches to the following four muscles:
1. Tibialis anterior (L4–L5), a dorsiflexor and invertor of the foot. It is tested by having the patient dorsiflex the foot against resistance or walk on the heels.
2. Extensor hallucis longus (L5–Sl), an extensor of the great toe and dorsiflexor of the foot. It is tested by having the patient dorsiflex the distal phalanx of the big toe against resistance.
3. Extensor digitorum longus (L5–Sl), an extensor of the four lateral toes and dorsiflexor of the foot. It is tested by having the patient dorsiflex the toes against resistance.
4. Extensor digitorum brevis (L5–Sl), an extensor of the large toe and three medial toes. It is tested by having the patient dorsiflex the proximal phalanges of the toes against resistance.
The terminal branch of the deep peroneal nerve passes under the tendon of the extensor hallucis longus on the dorsum of the foot and, after supplying the extensor digitorum brevis, innervates the skin on the first interosseous space and the adjacent skin of the sides of the first and second toes.
The superficial peroneal nerve supplies the peroneus longus and brevis muscles (L5–S1), which are plantar flexors and evertors of the foot. These are tested by having the patient evert the foot against resistance. The nerve terminates as a sensory terminal branch, which innervates the skin of the lateral distal portion of the lower leg and the dorsum of the foot and toes (except the first interosseous space).
In 20% to 28% of individuals, the lateral part of the extensor digitorum brevis (which extends to the fourth and fifth digits) is supplied by an accessory deep peroneal nerve [90,136,353], which is a branch of the superficial peroneal nerve. This branch reaches the extensor digitorum brevis by winding around the lateral malleolus.
An anomaly of innervation involving the proximal tibial nerve, common peroneal nerve, and sural nerve has been described [136,276]. Nerve fibers from the tibial nerve crossed over to join the common peroneal nerve in the popliteal fossa. In this case, the sural nerve was found to arise totally from the common peroneal nerve. The patient (who had suffered injury to the common peroneal nerve at the knee) had evidence of some activity (on electrophysiologic testing) in the peroneus longus muscle with otherwise complete paralysis of all common peroneal innervated muscles [136,276]. Also, an all tibial foot has been described in which the tibial nerve innervated the tibialis anterior muscle along with the peroneal nerve, innervated the extensor digitorum brevis muscle, and coinnervated the skin between the first and second toes with the deep peroneal nerve [405].

FIG. 2.14. The peroneal nerve.
NERVE LESIONS
Lesions of the Sciatic Nerve Proper. The sciatic nerve is frequently damaged in the sacral plexus, the pelvis, the gluteal region, or at the sciatic notch. Nerve injury may occur with fracture dislocation of the hip [107], with apophyseal avulsion fracture [349], after penetrating injury [297], after pelvic cancer or hip joint surgery (because of traction or a projecting spur of methylmethacrylate [46,100,125,409], with compression by a heterotopic ossification [1], with infections (e.g., herpes simplex or zoster), after radiation therapy [280], with gluteal hemorrhage, or after intramuscular injection [193]. With injection, motor fibers are more susceptible than sensory fibers, and the peroneal division of the sciatic nerve is more severely injured because of its lateral position. Injury to the sciatic nerve may rarely occur at the time of laparotomy and generally results from sudden and unexpected pelvic hemorrhage requiring the placement of large mattress sutures deep within the lateral pelvis to control the bleeding [160]. Such an injury has also been reported in association with the laterally extended endopelvic resection technique, which is required at the time of exenterative pelvic surgery. In patients undergoing vaginal surgery, maximal tension on the sciatic nerve and subsequent traction-induced sciatic neuropathy occur when patients are positioned in lithotomy with hip flexion and knee extension or with external hip rotation and knee flexion [160]. In a study of 196 patients with iatrogenic sciatic nerve injuries at the buttock and thigh levels, 164 patients had injuries caused by injections at the buttock level, 15 sustained sciatic nerve injuries after a total hip arthroplasty, and 17 had iatrogenic damage at the thigh level [406]. As noted above, severe, combined, bilateral femoral and sciatic neuropathies have been described in the context of alcohol intoxication (hanging leg syndrome) [318].
In general, sciatic lesions tend to affect the peroneal division more than the tibial division in about 75% of cases [409]. Nerve tumors and compression by aneurysms of the iliac artery [378] may also cause neuropathy. Complete sciatic neuropathy was due to rhabdomyolysis causing a gluteal compartment syndrome in a patient using intravenous heroin [194]. Cyclic sciatic pain and sensorimotor changes may occur with sciatic endometriosis (catamenial sciatica) [43,294,313,410]. Sciatic neuropathy at the time of cardiac surgery is often due to lower-limb ischemia; patients with symptomatic peripheral vascular disease who have a balloon pump inserted into the femoral artery or who develop femoral artery occlusion are at greatest risk for this complication [232]. The nerve may be compressed by varicotic gluteal vessels [34,219]. Lymphoma may invade the nerve [174] and primary sciatic nerve lymphoma may also occur [89].
The piriformis syndrome is an entrapment syndrome of the sciatic nerve as it passes through the greater sciatic notch [3]. Buttock tenderness, leg pain aggravated by internal rotation of the flexed limb, a limp, and sciatica reproduced on deep digital palpation are the main features of this clinical syndrome, which is commonly caused by pelvic or buttock trauma, pelvic surgery, mass lesions, fibrous bands, and piriformis muscle anomalies. Other etiologies include pressure by a wallet (credit-card–wallet sciatica) [215] or by coins in a back pocket (car toll neuropathy) [38]. The sciatic nerve may also be compressed in the thigh as a consequence of yoga (lotus foot drop) [385], injured by compression against an underlying prominent lesser trochanter [77], or even damaged because of toilet seat entrapment (toilet seat sciatic neuropathy) [149,371,380]. A woman with profound bilateral lower extremity weakness and sensory abnormality after falling asleep in the head-to-knees yoga position (also called Paschimottanasana) has also been described (another form of yoga neuropathy) [387]. Similar cases have occurred with sciatic compression while in a drunken stupor or as a complication of hip surgery [387]. The pathophysiology of the lesion could be related to a stretch injury, a proximal compression/infarct of the nerve in the gluteal region (distal to the sciatic notch), or a combination of both.
High sciatic lesions result in the following signs (high thigh lesions may selectively involve peroneal fibers):
1. Deformity. A flail foot is present because of paralysis of the dorsiflexors and plantar flexors of the foot. When the leg is passively lifted, the foot is plantar flexed and inverted (foot drop), but it also dorsiflexes loosely when the foot is passively moved back and forth.
2. Atrophy. There is wasting of the hamstrings and all the muscles below the knee.
3. Motor signs. There is paresis or paralysis of knee flexion (hamstrings), foot eversion (peronei), foot inversion (tibialis anterior), foot dorsiflexion (tibialis anterior and anterior leg musculature), foot plantar flexion (gastrocnemius and soleus), toe dorsiflexion (extensors of the toes), and toe plantar flexion (plantar flexors of the toes).
4. Reflex signs. There is a decrease or absence of the Achilles reflex (S1–S2), which is subserved by the tibial nerve.
5. Sensory signs. There are sensory changes (paresthesias and sensory loss) on the outer aspect of the leg and the dorsum of the foot (common peroneal distribution) and on the sole and the inner aspect of the foot (tibial nerve). The skin of the medial leg as far as the medial malleolus is spared because it is innervated by the saphenous nerve (a branch of the femoral nerve). The patient often complains pain in the sensory distribution and may have tenderness along the course of the nerve, especially paravertebrally, or in the buttock and posterior thigh. Tests that stretch the sciatic nerve (e.g., Lasegue’s test, Gower’s test) accentuate this pain.
6. Trophic changes. Loss of hair and changes in the toenails and skin texture may occur in the distal leg below the knee.
As the sciatic nerve is composed of two nerve trunks, medial and lateral, which become the tibial and peroneal nerves, respectively, partial sciatic lesions may differentially involve these trunks and thereby cause misleading localization deficits. Sciatic neuropathies can therefore be mistaken clinically for more distal neuropathies, especially common peroneal neuropathies or, less often, tibial neuropathies [359].
The sciatic nerve in the thigh may be injured by gunshot wounds, femur fractures, lacerations, and contusions [193]. Nerve compression in the thigh may be due to fibrous bands and aneurysms; nerve tumors may also occur in this location [285,343]. The sciatic nerve proper may also be damaged just above the apex of the popliteal space (e.g., owing to popliteal fossa aneurysm) [27]. The findings are the same as those seen with a more proximal sciatic lesion, except that the hamstring muscles are spared.
Lesions of the Tibial Nerve. The tibial nerve is most often damaged in the popliteal space, within the tarsal tunnel, or within the foot (abductor hallucis syndrome).
1. Lesions at the popliteal fossa. Lesions of the tibial nerve at this location result in paresis or paralysis of plantar flexion and inversion of the foot, plantar flexion of the toes, and movements of the intrinsic muscles of the foot. Sensory impairment is located on the sole and the lateral border of the foot. Etiologies of proximal tibial neuropathy include Baker’s cysts, trauma (especially if associated with popliteal fossa hemorrhage), nerve tumors, and entrapment by the tendinous arch of the origin of the soleus muscle or a hypertrophic popliteus muscle [74,91,122,156,210,226,374]. Tibial nerve entrapment by the arch of origin of the soleus muscle can be distinguished from tibial nerve compression at the ankle and S1 radiculopathy by the presence of severe pain and tenderness and a positive Tinel’s sign in the popliteal fossa [226]. In a retrospective study of 52 patients with main trunk tibial neuropathy, trauma and ischemia were the most frequent causes, followed by tumors [95].
2. Lesions within the tarsal tunnel. At the proximal end of the tarsal tunnel, the trunk of the tibial nerve may be compressed by any process that causes narrowing of the tunnel [83,127,262]. Rarely, the first symptoms of the tarsal tunnel syndrome emerge after an acute event (ischemic or traumatic) proximal to but not affecting the ankle (“decompensation” of a preexisting asymptomatic tarsal tunnel syndrome) [17]. Because the medial plantar, lateral plantar, and medial calcaneal nerves branch distal to this location, there are burning paresthesias in the sole of the foot and sensory loss affecting the skin of the sole and medial heel. Occasionally, the plantar nerves may be compressed individually within the tarsal tunnel (e.g., leading to medial plantar nerve symptoms and signs only). Etiologies of the tarsal tunnel syndrome include trauma to the ankle (e.g., fracture and dislocation), ill-fitting footwear, casts, posttraumatic fibrosis, ganglia or cysts, nerve tumors, abnormal muscles (e.g., abductor hallucis or accessory flexor digitorum longus), and compression by the adjacent flexor retinaculum and arteriovenous complex of the posterior tibial artery and veins [21,147,196,314,342,368,388,399].
Sensory symptoms are usually precipitated by standing or walking or by pressure applied at the ankle behind and below the medial malleolus (Tinel’s sign). Nocturnal pain is also quite common (analogous to carpal tunnel syndrome), and patients often attain relief by hanging the involved leg out of bed. Motor deficits are minimal, but atrophy and paresis are present on examination of the intrinsic muscles of the foot.
3. Lesions within the foot. The medial or lateral plantar nerves may be damaged within the foot. This damage results in pain, paresthesias, and sensory loss in the distribution area of the individual nerve (e.g., the medial two-thirds of the sole of the foot in medial plantar nerve lesions). There may be localized tenderness over the individual nerve and some intrinsic muscle atrophy and paresis. The medial plantar nerve may be compressed by the calcaneonavicular ligament, where the nerve pierces the abductor hallucis muscle, by a hypertrophic or fibrous abductor hallucis muscle, or by tendon sheath cysts [261,358]. The medial plantar nerve may also be injured by trauma (e.g., foot fractures) or schwannomas. Distal medial plantar neuropathy has been noted to occur frequently in infantry soldiers probably due to repeated mechanical injury causing nerve compression. [157]. Two patients have been described with neuropathic medial plantar foot pain and tingling due to sciatic nerve schwannoma in the mid-thigh [126]. Lateral plantar neuropathy may be caused by ankle injury, surgical scarring, or schwannoma [31,138,260]. The most common site of lateral plantar nerve injury is at the passage of the nerve through the abductor tunnel at the instep of the foot [260]. Rarely, isolated medial calcaneal nerve compression (e.g., by ganglia or fascial entrapment) may occur, resulting in heel pain [269].
A plantar digital nerve may be compressed where it courses distally between the heads of the adjacent metatarsal bones, or stretched where it crosses the deep metatarsal ligament. Pain, usually in the third metatarsal space, is the result. This pain is referred to as Morton’s metatarsalgia. The digital nerve on the side of the large toe may be compressed by ill-fitting shoes or by scars following bunion surgery (Joplin’s neuroma) [11,73,235].
Lesions of the Common Peroneal Nerve
1. Lesions at the fibular head. The majority of peroneal palsies occur at the level of the fibular head, where the nerve is quite superficial and susceptible to injury [171]. Although the nerve may be damaged by nerve infarct, casts, ganglion, Baker cyst, cysts of the tibiofibular joint, hematoma, tumor, or leprosy, most lesions are traumatic (laceration, traction, or compression) [22,161,171,177,185,297,395]. In one study of 318 knee-level common peroneal nerve lesions, there were 141 stretch/contusions without fracture/dislocations (44%), 39 lacerations (12%), 40 tumors (13%), 30 entrapments (9%), 22 stretch/contusions with fracture/dislocations (7%), 21 compressions (7%), 13 iatrogenic injuries (4%), and 12 gunshot wounds (4%) [183]. Stretch-induced peroneal neuropathy at the fibular head may be due to forceful inversion and plantar flexion of the ankle while kicking a football (punter’s palsy) [212]. Postoperative peroneal palsies occur especially after operations performed in the lateral decubitus position or when the outer aspect of the upper leg rests against a leg strap or metal brace. The nerve may also be stretched by flexion of the hip and knee while the patient is in the lithotomy position (e.g., postpartum foot drop) and is especially liable to injury after total knee arthroplasty [300]. Compressive lesions of the common peroneal nerve are usually unilateral, but bilateral (often asymmetric) lesions may develop in patients who are habitual leg crossers, especially those who have just lost considerable weight, are emaciated (e.g., anorexia nervosa) or bedridden, or have sustained nerve infarcts secondary to vasculitis [171,395]. Compression may also occur with chronic squatting and with protracted sitting in the cross-legged position (e.g., strawberry pickers’ foot drop) [197,326] or during yoga (yoga foot drop) [71,222]. Bilateral peroneal palsy may occur during natural childbirth owing to prolonged pressure exerted by the patient’s palms directly over the upper lateral aspect of the shins while strongly drawing the knees toward her (pushing palsy) [6]. Drop foot, caused by peroneal neuropathy, may also occur during weight reduction (slimmer’s paralysis) [345]. Entrapment of the peroneal nerve in the fibular tunnel (fibular tunnel syndrome) may occur with a band at the origin of the peroneus longus muscle [228].
Intraneural ganglia are an underappreciated but treatable cause of common peroneal neuropathy [408]. Intraneural ganglia of the peroneal nerve develop from the superior tibio-fibular joint when disruption of the capsule allows dissection of synovial fluid along the articular branch of the peroneal nerve. In a study of 22 cases of intraneural ganglia causing common peroneal neuropathy compared in a case–control study to 11 cases of common peroneal neuropathy with imaging negative for intraneural ganglia, the intraneural ganglia group had a greater body mass index, more pain at the knee or in the peroneal distribution, more frequent fluctuating weakness with weight bearing, or a palpable mass at the fibular head [408]. The intraneural ganglia group was less likely to present with a history of weight loss, immobility, or leg crossing.
With lesions at the fibular head, the deep branch of the nerve is affected more commonly than the whole nerve [346,359], although the superficial branch alone may also be affected. With common peroneal neuropathies, weakness is usually more prominent in muscles supplied by the deep peroneal nerve than in muscles supplied by the superficial peroneal nerve, likely because of differing degrees of damage to individual fascicles within the common peroneal nerve [175,346,359]. When both branches (deep and superficial) are affected, there is paresis or paralysis of toe and foot dorsiflexion and of foot eversion. A variable sensory disturbance affects the entire dorsum of the foot and toes and the lateral distal portion of the lower leg. When only the deep branch of the peroneal nerve is affected, a deep peroneal nerve syndrome occurs (see subsequent section).
In some patients with common peroneal neuropathy, the extensor hallucis longus is the most severely affected muscle, producing big toe drop rather than foot drop [364]. This is presumably due to selective damage of the fascicle within the common peroneal nerve that contains the motor fibers that supply the extensor hallucis muscle [359].
Rupture of the tibialis anterior tendon (TAT) is an uncommon musculoskeletal condition that presents as foot drop but is rarely encountered by neurologists [181]. Most cases are caused by direct or indirect foot trauma. Diabetes, systemic lupus erythematosus, hyperparathyroidism, psoriasis, and gout may produce tenosynovitis and are other associated etiologies. Spontaneous TAT rupture is rare and may be the most difficult form to distinguish from a neurogenic etiology of foot drop. The most prominent clinical feature of TAT rupture is weakness of foot dorsiflexion. However, increased compensatory action of the extensor hallucis longus and extensor digitorum longus may minimize the degree of weakness and make identification more difficult. The absence of toe extensor, foot eversion, and hip abduction weakness helps to distinguish TAT rupture from other neuromuscular causes of foot drop, such as peroneal neuropathy, lumbosacral plexopathy, or L5 radiculopathy. The pathognomonic sign of TAT rupture is the presence of the retracted tendon, which produces a palpable defect or swelling along the dorsum of the ankle. Normal findings on needle EMG of the tibialis anterior muscle are useful to distinguish TAT rupture from neuromuscular causes of foot drop where reduction in the recruitment of motor units would be seen. MRI of the ankle may confirm TAT rupture by identifying partial or complete ruptures of the tendon.
2. The anterior tibial (deep peroneal) nerve syndrome. This nerve may be injured in isolation at the fibular head or more distally in the leg. Nerve injury results in a motor deficit (paresis or paralysis of toe and foot dorsiflexion); sensory deficit is limited to the web of skin located between the first and second toes. If an accessory (anomalous) deep peroneal nerve is present, the extensor digitorum brevis muscle, or at least the lateral portion of this muscle, is spared [90]. Etiologies of proximal nerve injury include compressive masses (e.g., ganglia, osteochondromas, aneurysms), direct trauma (e.g., fibular fractures or surgery), thrombosis of crural veins [33], and occlusion of the anterior tibial artery.
Isolated deep peroneal nerve injury may complicate arthroscopic knee surgery [104]. At the level of the knee joint, the deep and superficial peroneal nerves are usually joined as the common peroneal nerve. Because of the fascicular structure, however, a partial nerve injury can result in an isolated injury to deep peroneal fibers [104].
The deep peroneal nerve may also be compressed at the ankle (anterior tarsal tunnel syndrome) [396]. The anterior tarsal tunnel syndrome is caused by ankle fractures, dislocations, sprains, ill-fitting shoes, or extreme ankle inversion and is due to distal deep peroneal compression beneath the crural cruciate ligament [396]. This compression results in paresis and atrophy of the extensor digitorum brevis muscle alone. The terminal sensory branch to the skin web between the first and second toes may be affected by lesions at this location. Iatrogenic, isolated weakness or paralysis of the extensor hallucis longus muscle is a common complication of proximal tibial and fibular osteotomy; the nerve supply to the extensor hallucis longus is at high risk for injury during tibial osteotomy because of the proximity of the bone to the motor branches [190]. A distal peroneal neuropathy may occur because of nerve injury during needle aspiration of the ankle joint. The deep peroneal sensory branch may be entrapped in the foot distal to the inferior extensor retinaculum as the nerve passes under the tendon of the extensor hallucis brevis muscle; a Tinel’s sign can be elicited by percussion of the tendon, and numbness and tingling occur over the first web space of the foot [279].
3. The superficial peroneal nerve syndrome. The superficial peroneal nerve may be affected in isolation by lesions at the fibular head or by lesions more distally in the leg. Paresis and atrophy of the peronei (foot eversion) and a sensory disturbance affecting the skin of the lateral distal portion of the lower leg and dorsum of the foot are present. The web of skin between the first and second toes is spared (this is the area of supply of the deep peroneal nerve). If an accessory deep peroneal nerve is present, the lateral part of the extensor digitorum brevis muscle is paretic and atrophic [90]. The sensory portion of the superficial peroneal nerve may be affected in isolation (e.g., where it emerges from the fascia) owing to inversion injury or compression (e.g., by wearing high lace-up boots or skates) [24], causing a purely sensory syndrome. Symptoms may be accompanied by tenderness at the point of fascial perforation [352]. Iatrogenic needle-induced neuropathy of the dorsal medial interosseous branch of the peroneal nerve (during venography with the needle in the dorsum of the foot) has been documented [281]. Finally, an accessory deep peroneal neuropathy may occur in isolation (e.g., by trauma or entrapment by a fascial band), resulting in isolated atrophy and paresis of the extensor digitorum brevis [90,305].
4. Lesions of the lateral cutaneous nerve of the calf. The lateral cutaneous nerve of the calf is a cutaneous branch of the common peroneal nerve. Nerve injury may cause numbness, pain, and sensory loss over the posterolateral aspect of the leg, extending from the knee to the lower third of the leg. Mononeuritis of this nerve is rare. One case of congenital entrapment mononeuropathy of this nerve by the tendon of the femoral biceps has been reported in the literature [139], as well as two cases of mononeuritis in diabetics, in whom the nerve is susceptible to compression where it passes through the deep fascia into the subcutaneous space [110,119]. Lateral cutaneous nerve of calf neuropathy has also been described due to peri-popliteal cystic bursitis [123].
Lesions of the Sural Nerve. Sural neuropathies present with pain or paresthesias over the lateral ankle and border of the foot. The nerve may be damaged in the popliteal fossa, the calf, the ankle, or the foot. Most sural neuropathies are due to lacerations, trauma associated with fractures, Achilles tendon reconstructive surgery, arthroscopy, and stretch injuries due to sprains [129,133,283,291]. The nerve may be entrapped by tendon sheath cysts, ganglia, Baker’s cysts, and scar tissue [255,283,341]. Damage to the sural nerve owing to external compression (e.g., the upper edge of a ski boot or tight elastic stockings) has been infrequently reported [133,291,335]. In a study of 36 patients with isolated sural neuropathy, 16 had various forms of ankle trauma, in three of whom the associated sural neuropathies developed following medical intervention [360]. In this study, three patients developed sural neuropathy associated with vasculitis, and there were single patients with schwannoma and ganglionic cyst.
TABLE 2.1 Main Entrapment Neuropathies of the Upper Limbs

The main entrapment neuropathies of the upper and lower limbs are summarized in Tables 2.1 and 2.2, respectively.
TABLE 2.2 Main Entrapment Neuropathies of the Lower Limbs
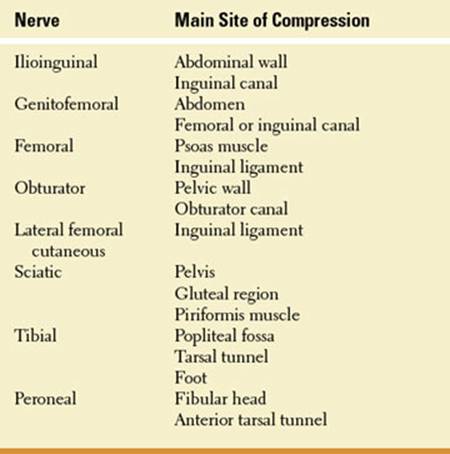
References
1. Abayev B, Ha E, Cruise C. A sciatic nerve lesion secondary to compression by a heterotopic ossification in the hip and thigh region—an electrodiagnostic approach: a review and case study. Neurologist2005;11:184–186.
2. Abitbol JJ, Gendron D, Laurin CA, et al. Gluteal nerve damage following total hip arthroplasty: a prospective analysis. J Arthroplasty 1990;5:319–322.
3. Adams JA. The pyriformis syndrome—report of four cases and review of the literature. S Afr J Surg 1980;18:13–18.
4. Adar R, Meyer E, Zweig A. Saphenous neuralgia: a complication of vascular reconstructions below the inguinal ligament. Ann Surg 1979;190:609–613.
5. Adelman JU, Goldberg GS, Puckett JD. Postpartum bilateral femoral neuropathy. Obstet Gynec 1973;42: 845–850.
6. Adornato BT, Carlini WG. “Pushing palsy”: a case of self-induced bilateral peroneal palsy during natural childbirth. Neurology 1992;42:936–938.
7. Aiello I, Serra G, Gilli P. Entrapment of the suprascapular nerve at the spinoglenoid notch. Ann Neurol 1982;12:314–316.
8. Albanese S, Butterbaugh G, Palmer AK, et al. Incomplete anterior interosseous nerve palsy following spinal surgery. Spine 1986;11:1037–1038.
9. Al-Hakim M, Katirji MB. Femoral mononeuropathy induced by the lithotomy position: a report of 5 cases with a review of literature. Muscle Nerve 1993;16: 891–895.
10. Al-Qattan MM. Anatomical classification of sites of compression of the palmar cutaneous branch of the median nerve. J Hand Surg 1977;22:48–49.
11. Ames PA, Lenet MD, Sherman M. Joplin’s neuroma. J Am Podiatry Assoc 1980;70:99–101.
12. Amoiridis G, Wohrie J, Grunwald I, et al. Malignant tumour of the psoas: another cause of meralgia paresthetica. Electromyogr Clin Neurophysiol 1993;33: 109–112.
13. Antoniadis G, Richter H-P, Rath S, et al. Suprascapular nerve entrapment: experience with 28 cases. J Neurosurg 1996;85:1020–1025.
14. Arnoldussen WJ, Korten JJ. Pressure neuropathy of the posterior femoral cutaneous nerve. Clin Neurol Neurosurg 1980;82:57–60.
15. Artico M, Salvati M, D’Andrea V, et al. Isolated lesions of the axillary nerve: surgical treatment and outcome in 12 cases. Neurosurgery 1991;29:697–700.
16. Ashworth NL, Marshall SC, Classen DA. Anterior interosseous nerve syndrome presenting with pronator teres weakness: a case report. Muscle Nerve 1997;20: 1591–1594.
17. Augustijn P, Vanneste J. The tarsal tunnel syndrome after a proximal lesion. J Neurol Neurosurg Psychiatry 1992;55:65–67.
18. Aydinlioglu A, Cirak B, Akpinar F, et al. Bilateral median nerve compression at the level of Struthers’ ligament. Case report. J Neurosurg 2000;92:693–696.
19. Back T, Mrowka M. Infarction of the “hand knob” area. Neurology 2001;57:1143.
20. Bademkiran F, Tataroglu C, Ozdedeli K, et al. Electrophysiological evaluation of the genitofemoral nerve in patients with inguinal hernia. Muscle Nerve 2005; 32:600–604.
21. Bailie DS, Kelikian AS. Tarsal tunnel syndrome: diagnosis, surgical technique, and functional outcome. Foot Ankle Int 1998;19:65–72.
22. Bakshi N, Chan KM, and Wirganowicz PZ. Peroneal intraneural ganglion. Neurology 2995;65:1753.
23. Balzarini A, Pirovano C, Diazzi G, et al. Ultrasound therapy of chronic arm lymphedema after surgical treatment of breast cancer. Lymphology 1993;26: 128–134.
24. Banerjee T, Koons DD. Superficial peroneal nerve entrapment. J Neurosurg 1981;55:991–992.
25. Banwart JC, Asher MA, Hassanein RS. Iliac crest bone graft harvest donor site morbidity: a statistical evaluation. Spine 1995;20:1055–1060.
26. Basheer H, Rabia F, El-Helw K. Neurofibromas of digital nerves. J Hand Surg 1997;22:61–63.
27. Beaudry Y, Stewart JD, Errett L. Distal sciatic nerve compression by a popliteal aneurysm. Can J Neurol Sci 1989;16:352–353.
28. Beekman R, Slooff W-BM, Van Oosterhout MFM, et al. Bilateral intraneural perineuroma presenting as ulnar neuropathy at the elbow. Muscle Nerve 2004;30: 239–243.
29. Beekman R, Van Der Plas JPL, Uitdehaag BMJ, et al. Clinical, electrodiagnostic, and sonographic studies in ulnar neuropathy at the elbow. Muscle Nerve 2004;30:202–208.
30. Beekman R, Wokke JHJ, Schoemaker MC, et al. Ulnar neuropathy at the elbow: follow-up and prognostic factors determining outcome. Neurology 2004;63: 1675–1680.
31. Belding RH. Neurilemoma of the lateral plantar nerve producing tarsal tunnel syndrome: a case report. Foot Ankle 1993;14:289–291.
32. Belsh JM. Anterior femoral cutaneous nerve injury following femoral artery reconstructive surgery. Arch Neurol 1991;48:230–232.
33. Bendszus M, Reiners K, Perez J, et al. Peroneal nerve palsy caused by thrombosis of crural veins. Neurology 2002;58:1675–1677.
34. Bendszus M, Rieckmann P, Perez J, et al. Painful vascular compression syndrome of the sciatic nerve caused by gluteal varicosities. Neurology 2003;61: 985–987.
35. Benezis I, Boutaud B, Leclerc J, et al. Lateral femoral cutaneous neuropathy and its surgical treatment: a report of 167 cases. Muscle Nerve 2007;36: 659–663.
36. Benini A. Ilio-inguinal and genito-femoral neuralgia: causes, clinical aspects, therapy. Schweiz Rundsch Med Prax 1992;81:1114–1120.
37. Beresford HR. Meralgia paresthetica after seat-belt trauma. J Trauma 1971;11:629–630.
38. Berlit P. Car toll neuropathy. J Neurol Neurosurg Psychiatry 1993;56:1329.
39. Berry H, Bril V. Axillary nerve palsy following blunt trauma to the shoulder region: a clinical and electrophysiological review. J Neurosurg 1982;45:1027–1032.
40. Berry PR, Wallis WE. Venipuncture nerve injuries. Lancet 1977;1:1236–1237.
41. Biedert RM. Atrophy of the infraspinatus muscle caused by a suprascapular ganglion. J Sports Med 1996;6:262–263.
42. Bilge T, Yalaman O, Bilge S, et al. Entrapment neuropathy of the median nerve at the level of ligament of Struthers. Neurosurgery 1990;27:787–789.
43. Binkovitz LA, King BF, Ehman RL. Sciatic endometriosis: MR appearance. J Comput Assist Tomogr 1991;15:508–510.
44. Bird SJ, Brown MJ. Acute focal neuropathy in male weight lifters. Muscle Nerve 1996;19:897–899.
45. Blom S, Dahlback LO. Nerve injuries in dislocations of the shoulder joint and fractures of the neck of the humerus. A clinical and electromyographical study. Acta Chir Scand 1970;136:461–466.
46. Bonney G. Iatrogenic injuries of nerves. J Bone Joint Surg Br 1986;68:9–13.
47. Bourque PR, Dyck PJ. Selective calf weakness suggests intraspinal pathology, not peripheral neuropathy. Arch Neurol 1990;47:79–80.
48. Braddom RL, Wolfe C. Musculocutaneous nerve injury after heavy exercise. Arch Phys Med Rehabil 1978;59:290–293.
49. Bradshaw C, McCory P. Obturator nerve entrapment. Clin J Sport Med 1997;7:217–219.
50. Bradshaw C, McCory P, Bell S, et al. Obturator nerve entrapment: a cause of groin pain in athletes. Am J Sports Med 1997;25:402–408.
51. Bratschi HU, Haller U. Significance of the intercostobrachial nerve in axillary lymph node excision. Geburtshilfe Frauenheilkd 1990;50:689–693.
52. Braun RM, Spinner RJ. Spontaneous bilateral median nerve compressions in the distal arm. J Hand Surg 1991;16:244–247.
53. Britz GW, Haynor DR, Kuntz C, et al. Ulnar nerve entrapment at the elbow: correlation of magnetic resonance imaging, clinical, electrodiagnostic, and intraoperative findings. Neurosurgery1996;38:458–465.
54. Brooks DM. Nerve compression by simple ganglia: a review of thirteen collected cases. J Bone Joint Surg 1952;34:391–396.
55. Brown WF, Watson BV. AAEM case report #27: acute retrohumeral radial neuropathies. Muscle Nerve 1993;16:706–711.
56. Bryan FS, Miller LS, Panjaganond P. Spontaneous paralysis of the posterior interosseus nerve: a case report and review of the literature. Clin Orthop 1971;80:9–12.
57. Buckmiller JF, Rickard TA. Isolated compression neuropathy of the palmar cutaneous branch of the median nerve. J Hand Surg 1987;12:97–99.
58. Burnham RS, Steadward RD. Upper extremity nerve entrapments among wheelchair athletes: prevalence, location, and risk factors. Arch Phys Med Rehabil 1994;75:519–524.
59. Cahill BR, Palmer RE. Quadrilateral space syndrome. J Hand Surg 1983;8:65–69.
60. Callahan JD, Scully TB, Shapiro SA, et al. Suprascapular nerve entrapment. A series of 27 cases. J Neurosurg 1991;74:893–896.
61. Campbell WW. Ulnar neuropathy in the distal forearm. Muscle Nerve 1989;12:347–352.
62. Campbell WW, Pridgeon RM, Riaz G, et al. Sparing of the flexor carpi ulnaris in ulnar neuropathy at the elbow. Muscle Nerve 1989;12:965–967.
63. Campbell WW, Pridgeon RM, Riaz G, et al. Variations in anatomy of the ulnar nerve at the cubital tunnel: pitfalls in the diagnosis of ulnar neuropathy at the elbow. Muscle Nerve 1991;14:733–738.
64. Campbell WW, Pridgeon RM, Sahni SK. Entrapment of the ulnar nerve at its point of exit from the flexor carpi ulnaris muscle. Muscle Nerve 1988;11: 467–470.
65. Cavallo M, Poppi M, Martinelli P, et al. Distal ulnar neuropathy from carpal ganglion: a clinical and electrophysiologic study. Neurosurgery 1988;22:902–905.
66. Cerrato P, Lentini A, Baima C, et al. Pseudo-ulnar sensory loss in a patient from a small cortical infarct of the postcentral knob. Neurology 2005;64:1981–1982.
67. Chang CW, Cho HK, Oh SJ. Posterior antebrachial cutaneous neuropathy: case report. Electromyogr Clin Neurophysiol 1989;29:109–111.
68. Chang CW, Oh SJ. Medial antebrachial cutaneous neuropathy: case report. Electromyogr Clin Neurophysiol 1988;28:3–5.
69. Chang CW, Oh SJ. Posterior antebrachial cutaneous neuropathy: case report. Electromyogr Clin Neurophysiol 1990;30:3–5.
70. Charness ME, Ross MH, Shefner JM. Ulnar neuropathy and dystonic flexion of the fourth and fifth digits: clinical correlation in musicians. Muscle Nerve 1996;19:431–437.
71. Chusid J. Yoga foot drop. JAMA 1971;217:827–828.
72. Chutkow JG. Posterior femoral cutaneous neuralgia. Muscle Nerve 1988;11:1146–1148.
73. Cichy SW, Claussen GC, Oh SJ. Electrophysiological studies in Joplin’s neuroma. Muscle Nerve 1995; 18:671–672.
74. Costigan D, Tindall S, Lexow S. Tibial nerve entrapment by the tendinous arch of origin of the soleus muscle: diagnostic difficulties. Muscle Nerve 1991; 14:880.
75. Cramer KE, Green NE, Devito DP. Incidence of anterior interosseous nerve palsy in supracondylar fractures in children. J Pediatr Orthop 1993;13:502–505.
76. Cravens G, Kline DG. Posterior interosseous nerve palsies. Neurosurgery 1990;27:397–402.
77. Crisci C, Baker MK, Wood MB, et al. Trochanteric sciatic neuropathy. Neurology 1989;39:1539–1541.
78. Culp RW, Osterman AL, Davidson RS, et al. Neural injuries associated with supracondylar fractures of the humerus in children. J Bone Joint Surg Am 1990;72: 1211–1215.
79. Cynamon KB. Flutist’s neuropathy. N Engl J Med 1981;305:961.
80. Davidson JJ, Bassett FH III, Nunley JA Jr. Musculocutaneous nerve entrapment revisited. J Shoulder Elbow Surg 1998;7:250–255.
81. Dawson DM. Entrapment neuropathies of the upper extremities. N Engl J Med 1993;329:2013–2018.
82. Dawson DM, Krarup C. Perioperative nerve lesions. Arch Neurol 1989;46:1355–1360.
83. DeLisa J, Saeed MA. The tarsal tunnel syndrome. Muscle Nerve 1983;6:664–670.
84. Dell PC. Compression of the ulnar nerve at the wrist secondary to a rheumatoid synovial cyst: case report and review of the literature. J Hand Surg 1979;4: 468–473.
85. Dellon AL, MacKinnon SE. Injury to the medial antebrachial cutaneous nerve during cubital tunnel surgery. J Hand Surg 1985;10:33–36.
86. Dellon AL, MacKinnon SE. Entrapment of the radial sensory nerve in the forearm. J Hand Surg 1986a;11:199–205.
87. Dellon AL, MacKinnon SE. Radial sensory nerve entrapment. Arch Neurol 1986;43:833–835.
88. Dellon AL, MacKinnon SE, Danshvar A. Terminal branch of anterior interosseous nerve as source of wrist pain. J Hand Surg 1984;9:316–322.
89. Descamps MJL, Barrett L, Groves M, et al. Primary sciatic nerve lymphoma: a case report and review of the literature. J Neurology Neurosurg Psychiatry. 2006; 77:1087–1089.
90. Dessi F, Durand G, Hoffmann JJ. The accessory deep peroneal nerve: a pitfall for the electromyographer. J Neurol Neurosurg Psychiatry 1992;55: 214–215.
91. DeRisio D, Lazaro R, Popp AJ. Nerve entrapment and calf atrophy caused by a Baker’s cyst: case report. Neurosurgery 1994;35:333–334.
92. Dobyns JH. Bowler’s thumb: diagnosis and treatment. J Bone Joint Surg Am 1972;54:751–755.
93. Donaldson JO, Wirz D, Mashman J. Bilateral postpartum femoral neuropathy. Conn Med 1985;49: 496–498.
94. Doyle JJ, David WS. Posterior antebrachial cutaneous neuropathy associated with lateral elbow pain. Muscle Nerve 1993;16:1417–1418.
95. Drees C, Wilbourn AJ, Stevens GHJ. Main trunk tibial neuropathies. Neurology 2002;59:1082–1084.
96. Duncan M, Lotze M, Gerber L, et al. Incidence, recovery, and management of serratus anterior muscle palsy after axillary dissection. Surg Clin North Am 1983;63:1243–1247.
97. Dunne JW, Prentice DA, Stewart-Wynne EG. Bilateral anterior interosseous nerve syndromes associated with cytomegalovirus infection. Muscle Nerve 1987; 10:446–448.
98. Ebeling P, Gilliatt RW, Thomas PK. A clinical and electrical study of ulnar nerve lesions of the hand. J Neurol Neurosurg Psychiatry 1960;23:1–9.
99. Edwards JC, Green CT, Riefel E. Neurilemoma of the saphenous nerve presenting as pain in the knee. J Bone Joint Surg Am 1989;71:1410–1411.
100. Edwards MS, Barbaro NM, Asher SW, et al. Delayed sciatic palsy after total hip replacement: case report. Neurosurgery 1981;9:61–63.
101. England JD, Sumner AJ. Neuralgic amyotrophy: an increasingly diverse entity. Muscle Nerve 1987;10: 60–68.
102. Erdem S, Demirci M, Tan E. Focal myopathy mimicking posterior interosseous nerve syndrome. Muscle Nerve 2001;24:969–972.
103. Escolar DM, Jones HR Jr. Pediatric radial mononeuropathies: a clinical and electromyographic study of sixteen children with review of the literature. Muscle Nerve 1996;19:876–883.
104. Esselman PC, Tomski MA, Robinson LR, et al. Selective deep peroneal nerve injury associated with arthroscopic knee surgery. Muscle Nerve 1993;16: 1188–1192.
105. Fabian RH, Norcross KA, Hancock MB. Surfer’s neuropathy. N Engl J Med 1987;316:555.
106. Fardin P, Negrin P, Sparta S, et al. Posterior interosseous nerve neuropathy. Clinical and electromyographical aspects. Electromyogr Clin Neurophysiol 1992;32:229–234.
107. Fassler PR, Swiontkowski MF, Kilroy AW, et al. Injury of the sciatic nerve associated with ace-tabular fracture. J Bone Joint Surg 1993;75:1157–1166.
108. Fine EJ, Wongjirad C. The ulnar flexion maneuver. Muscle Nerve 1985;8:612.
109. Finelli PF. Anterior interosseous nerve syndrome following cutdown catheterization. Ann Neurol 1977;1: 205–206.
110. Finelli PF, Dibenedetto M. Bilateral involvement of the lateral cutaneous nerve of the calf in a diabetic. Ann Neurol 1978;4:480–481.
111. Foster RJ, Swiontkowski MF, Bach AW, et al. Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg 1993;18:121–124.
112. Foucher G, Berard V, Snider G, et al. Distal ulnar entrapment due to a tumor of Guyon’s canal: a series of ten cases. Handchir Mikrochir Plast Chir 1993;25: 61–65.
113. Francel TJ, Dellon AL, Campbell JN. Quadrilateral space syndrome: diagnosis and operative decompression technique. Plast Reconstr Surg 1991;87:911–916.
114. Fricker R, Fuhr P, Pippert H, et al. Acute median nerve compression at the distal forearm caused by a thrombosed aneurysm of an epineural vessel: case report. Neurosurgery 1996;38:194.
115. Friedenberg SM, Zimprich T, Harper CM. The natural history of long thoracic and spinal accessory neuropathies. Muscle and Nerve 2002;25:535–539.
116. Ganes T. Complete ulnar innervation of the thenar muscles combined with normal sensory fibres in a subject with no peripheral nerve lesion. Electromyogr Clin Neurophysiol 1992;32:559–563.
117. Gardetto A, Thaler C, Kiechl S, et al. Isolated compression of the pectoral nerve resulting in atrophy of the major pectoral muscle. Muscle Nerve 2003;28: 760–763.
118. Genç H, Leventolu A, Güney F, et al. Posterior interosseous nerve syndrome caused by the use of a Canadian crutch. Muscle Nerve 2003;28:386–387.
119. Gessini L, Jandolo B, Pascucci P, et al. Diabetic neuropathy of the lateral cutaneous nerve of the calf. A case report. Ital J Neurol Sci 1985;6:107–108.
120. Gessini L, Jandolo B, Pietrangeli A. Entrapment neuropathy of the dorsal cutaneous of the hand. J Neurosurg Sci 1982;26:185–186.
121. Gessini L, Jandolo B, Pietrangeli A, et al. Compression of the palmar cutaneous nerve by ganglions of the wrist. J Neurosurg Sci 1983;27:241–243.
122. Ghaly RF. A posterior tibial nerve neurilemoma unrecognized for 10 years: case report. Neurosurgery 2001;48:668–672.
123. Ginanneschi F, Rossi A. Lateral cutaneous nerve of calf neuropathy due to peri-popliteal cystic bursitis. Muscle Nerve 2006;34:503–504.
124. Giuliani G, Poppi M, Pozzati E, et al. Ulnar neuropathy due to a carpal ganglion: the diagnostic contribution of CT. Neurology 1990;40:1001–1002.
125. Goldberg G, Goldstein H. AAEM case report 32: nerve injury associated with hip arthroplasty. Muscle Nerve 1998;21:519–527.
126. Gominak SC, Ochoa JL. Sciatic schwannoma of the thigh causing foot pain mimicking plantar neuropathy. Muscle Nerve 1998;21:528–530.
127. Goodgold J, Kopell HP, Spielholz NI. The tarsal tunnel syndrome. N Engl J Med 1965;273:742–745.
128. Goodson JD. Pudendal neuritis from biking. N Engl J Med 1981;304:365.
129. Gould N, Trevino S. Sural nerve entrapment by avulsion fracture of the base of the fifth metatarsal bone. Foot Ankle 1981;2:153–155.
130. Grant AC, Cook AA. A prospective study of handcuff neuropathies. Muscle Nerve 2000;23:933–938.
131. Greenen EK, Bunker T. Anterior interosseous nerve syndrome. Br J Hosp Med 1985;34:235.
132. Grisold W, Karnel F, Kumpan W, et al. Iliac artery aneurysm causing isolated superior gluteal nerve lesion. Muscle Nerve 1999;22:1717–1720.
133. Gross JA, Hamilton WJ, Swift TR. Isolated mechanical lesions of the sural nerve. Muscle Nerve 1980; 3:248–249.
134. Gross PT, Royden-Jones HR. Proximal median neuropathies: electromyographic and clinical correlation. Muscle Nerve 1992;15:390–395.
135. Gupta SK, Benstead TJ. Symptoms experienced by patients with carpal tunnel syndrome. Can J Neurol Sci 1997;24:338–342.
136. Gutmann L. AAEM minimonograph #2: important anomalous innervation of the extremities. Muscle Nerve 1993;16:339–347.
137. Guney F, Yuruten B, Karalezli N. Digital neuropathy of the median and ulnar nerves caused by Dupuytren’s contracture: case report. Neurologist. 2009;15:217– 219.
138. Hah JS, Kim DE, Oh SJ. Lateral plantar neuropathy: a heretofore unrecognized neuropathy. Muscle Nerve 1992;15:1175.
139. Hackam DG, Zwimpfer TJ. Congenital entrapment of the lateral cutaneous nerve of the calf presenting as a peroneal sensory neuropathy. Can J Neurol Sci 1998;25:168–170.
140. Hale BR. Handbag paresthesia. Lancet 1976;2:470.
141. Hankey GJ. Median nerve compression in the palm of the hand by an anomalously enlarged ulnar artery. Aust NZ J Surg 1988;58:511–513.
142. Harbaugh KS, Swenson R, Saunders RL. Shoulder numbness in a patient with suprascapular nerve entrapment syndrome: cutaneous branch of the suprascapular nerve: case report. Neurosurgery2000;47:1452– 1456.
143. Heberman ET, Cabot WD. Median nerve compression secondary to false aneurysm of the brachial artery. Bull Hosp Joint Dis 1974;35:58–161.
144. Henderson M, Robinson LR. Dorsal ulnar cutaneous handcuff neuropathy. Muscle Nerve 1991;14: 905–906.
145. Hershfield HB. Pedaller’s penis. Can Med Assoc J 1983;128:366–367.
146. Hirayama T, Takemitsu Y. Isolated paralysis of the descending branch of the posterior interosseous nerve. J Bone Joint Surg 1988;70A:1402–1403.
147. Ho VW, Peterfy C, Helms CA. Tarsal tunnel syndrome caused by strain of an anomalous muscle: an MRI-specific diagnosis. J Comput Assist Tomogr 1993;17: 822– 823.
148. Holekamp NM, Meredith TA, Landers MB, et al. Ulnar neuropathy as a complication of macular hole surgery. Arch Ophthalmol 1999;117:1607–1610.
149. Holland NR, Schwartz-Williams LA, Blotzer JW. “Toilet seat” sciatic neuropathy. Arch Neurol 1999; 56:116.
150. Holtzman RNN, Mark MH, Patel MR. Ulnar nerve entrapment neuropathy in the forearm. J Hand Surg 1974;9:576–578.
151. Hopf HC. Forearm ulnar-to-median nerve anastomosis of sensory axons. Muscle Nerve 1990;13:654–656.
152. Hopkins A. A novel cause of a pressure palsy: mobile telephone user’s shoulder droop. J Neurol Neurosurg Psychiatry 1996;61:349.
153. Hopkins GO, Ward AB, Garnett RA. Lone axillary nerve lesion due to closed non-dislocating injury of the shoulder. Injury 1985;16:305–306.
154. House JH, Ahmed K. Entrapment neuropathy of the infrapatellar branch of the saphenous nerve: a new peripheral nerve entrapment syndrome. Am J Sports Med 1977;5:106–115.
155. Hsu W-C, Chen W-H, Oware A, et al. An unusual entrapment neuropathy in a golf player. Neurology 2002;59:646–647.
156. Iada T, Kobayashi M. Tibial nerve entrapment by the tendinous arch of the soleus: a case report. Clin Orthop 1997;334:265–269.
157. Ifergane G, Zlotnik Y, Harari I, et al. Distal medial plantar neuropathy in infantry soldiers. Neurology 2006;67:916.
158. Ikram MA. Ulnar nerve palsy: a complication following percutaneous fixation of supracondylar fractures of the humerus in children. Injury 1996;27:303–305.
159. Inaba A, Takanori Y. Isolated musculocutaneous nerve palsy during sleep. Muscle Nerve 2003;28: 773–774.
160. Irvin W, Andersen W, Taylor P, et al. Minimizing the risk of neurologic injury in gynecologic surgery. Obstet Gynecol 2004;103:374–382.
161. Iverson DJ. MRI detection of cysts of the knee causing common peroneal neuropathy. Neurology 2005;65: 1829–1831.
162. Iyer VG, Shields CB. Isolated injection injury to the posterior femoral cutaneous nerve. Neurosurgery 1989;25:835–838.
163. Jablecki CK. Lateral antebrachial cutaneous neuropathy in a windsurfer. Muscle Nerve 1999;22: 944–945.
164. Jablecki CK. Postoperative lateral femoral cutaneous neuropathy. Muscle Nerve 1999;22:1129–1131.
165. Jacob A, Moorthy TK, Thomas SV, et al. Compression of the deep motor branch of the ulnar nerve: an unusual cause of pure motor neuropathy and hand wasting. Arch Neurol 2005;62:826–827.
166. Jacobs MJHM, Gregoric ID, Reul GJ. Profunda femoral artery pseudoaneurysm after percutaneous transluminal procedures manifested by neuropathy. J Cardiovasc Surg 1992;33:729–731.
167. Jankowski CJ, Keegan MT, Bolton CF, et al. Neuropathy following axillary brachial plexus block: is it the tourniquet? Anesthesiology 2003;99:1230–1232.
168. Jefferson D, Eames RA. Subclinical entrapment of the lateral femoral cutaneous nerve: an autopsy study. Muscle Nerve 1979;2:145–154.
169. Jitpraphai P, Molinares M, Wise GJ. Sarcoma of the prostate. Presentation as obturator nerve paralysis. J Med Assoc Thai 1972;55:186–194.
170. Johnson EW. Axillary nerve injury. Arch Neurol 1984;41:102–1028.
171. Jones HR, Felice KJ, Gross PT. Pediatric peroneal mononeuropathy: a clinical and electromyographic study. Muscle Nerve 1993;16:1167–1173.
172. Juel VC, Kiely JM, Leone KV, et al. Isolated musculocutaneous neuropathy caused by a proximal humeral exostosis. Neurology 2000;54:494–496.
173. Kaku DA, So YT. Acute femoral neuropathy and iliopsoas infarction in intravenous drug abusers. Neurology 1990;40:1317–1318.
174. Kanamori M, Matsui H, Yudoh K. Solitary T-cell lymphoma of the sciatic nerve: case report. Neurosurgery 1995;36:1203–1205.
175. Kang PB, Preston DC, Raynor EM. Involvement of superficial peroneal sensory nerve in common peroneal neuropathy. Muscle Nerve 2005;31:725–729.
176. Katirji MB, Preston DC. Vibration-induced median neuropathy. Neurology 2003;61:1011.
177. Katirji MB, Wilbourn AJ. Common peroneal mononeuropathy: a clinical and electrophysiologic study of 116 lesions. Neurology 1988;38:1723–1728.
178. Kato H, Ogino T, Nanbu T, et al. Compression neuropathy of the motor branch of the median nerve caused by palmar ganglion. J Hand Surg 1991;16: 751–752.
179. Kauppila LI, Vastamaki M. Iatrogenic serratus anterior palsy: long-term outcome in 26 patients. Chest 1996;109:31–34.
180. Kennedy AM, Grocott M, Schwartz MS, et al. Median nerve injury: an underrecognised complication of brachial artery cardiac catheterization? J Neurol Neurosurg Psychiatry 1997;63:542–546.
181. Kennelly KD, Shapiro SA, Kumar N, et al. Spontaneous tibialis anterior tendon rupture: a rare cause of foot drop. Neurology 2007;68:1949–1951.
182. Kho KH, Blijham PJ, Zwarts MJ. Meralgia paresthetica after strenuous exercise. Muscle Nerve 2005;31: 761–763.
183. Kim D, Murovic J, Tiel R, et al. Management and outcomes in 318 operative common peroneal nerve lesions at the Louisiana State University Health Sciences Center. Neurosurgery 2004;54:1421–1429.
184. Kim DH, Kline DG. Surgical outcome for intra- and extrapelvic femoral nerve lesions. J Neurosurg 1995; 83:783–790.
185. Kim DH, Kline DG. Management and results of peroneal nerve lesions. Neurosurgery 1996;39:312–320.
186. Kim DH, Murovic JA, Tiel RL, et al. Surgical management of 33 ilioinguinal and iliohypogastric neuralgias at Louisiana State University Health Sciences Center. Neurosurgery 2005;56:1013–1020.
187. Kim DH, Murovic JA, Tiel RL, et al. Management and outcomes of 42 surgical suprascapular nerve injuries and entrapments. Neurosurgery 2005;57:120– 127.
188. Kim J-E, Kang J-H, Choi JC, et al. Isolated posterior femoral cutaneous neuropathy following intragluteal injection. Muscle Nerve 2009;40:864–866.
189. Kim SM, Goodrich JA. Isolated musculocutaneous nerve palsy: a case report. Arch Phys Med Rehabil 1984;65:735–736.
190. Kirgis A, Albrecht S. Palsy of the deep peroneal nerve after proximal tibial osteotomy. J Bone Joint Surg 1992;74A:1180–1185.
191. Kiss G, Kòmàr J. Supraclavicular nerve compression at the spinoglenoid notch. Muscle Nerve 1990;13: 556–557.
192. Kitagawa R, Kim D, Reid N, et al. Surgical management of obturator nerve lesions. Neurosurgery 2009;65:(Supplement):A24–A28.
193. Kline DG, Kim D, Midha R, et al. Management and results of sciatic nerve injuries: a 24-year experience. J Neurosurg 1998;89:13–23.
194. Klockgether T, Weller M, Haarmeier T, et al. Gluteal compartment syndrome due to rhabdomyolysis after heroin abuse. Neurology 1997;48:275–276.
195. Knossalla F, Nicolas V, Tegenthoff M. Suprascapular nerve entrapment in a canoeist. Arch Neurol 2006;63: 781.
196. Kohno M, Takahashi H, Segawa H, et al. Neurovascular decompression for idiopathic tarsal tunnel syndrome: technical note. J Neurol Neurosurg Psychiatry 2000;69:87–90.
197. Koller RL, Blank NK. Strawberry pickers’ palsy. Arch Neurol 1980;37:320.
198. Kopell HP, Thompson WAL, Postel AH. Entrapment neuropathy of the ilioinguinal nerve. N Engl J Med 1962;266:16–19.
199. Krishnan KG, Pinzer T, Schackert G. The transaxillary approach in the treatment of thoracic outlet syndrome: a neurosurgical appraisal. Zentralbl Neurochir 2005;66:180–189.
200. Kuntzer T, van Melle G, Regli F. Clinical and prognostic features in unilateral femoral neuropathies. Muscle Nerve 1997;20:205–211.
201. Kvist-Poulsen H, Borel J. Iatrogenic femoral neuropathy subsequent to abdominal hysterectomy: incidence and prevention. Obstet Gynecol 1982;60:516–520.
202. Lacroix VJ, Kinnear DG, Mulder DS, et al. Lower abdominal pain syndrome in national hockey league players: a report of 11 cases. Clin J Sport Med 1998; 8:5–9.
203. Laurent LE. Femoral nerve compression syndrome with paresis of the quadriceps muscle caused by radiotherapy of malignant tumors. A report of four cases. Acta Orthop Scand 1975;46:804–808.
204. Lederman RJ. Peripheral nerve disorders in instrumentalists. Ann Neurol 1989;26:640–646.
205. Lederman RJ, Breuer AC, Hanson MR, et al. Peripheral nervous system complications of coronary artery bypass graft surgery. Ann Neural 1982;12: 297–301.
206. Leibovic SJ, Hastings H. Martin-Gruber revisited. J Hand Surg 1992;17:47–53.
207. Liguori R, Donadio V, Di Stasi V, et al. Palmaris brevis spasm: an occupational syndrome. Neurology 2003;60:1705–1707.
208. Liveson JA, Bronson MJ, Pollack MA. Suprascapular nerve lesions at the spinoglenoid notch: report of three cases and review of the literature. J Neurol Neurosurg Psychiatry 1991;54:241–243.
209. Lo YL, Lee KT, Rikhraj IS. Isolated medial femoral cutaneous neuropathy. Muscle Nerve 2004;30:812– 813.
210. Logigian EL, Berger AR, Shahani BT. Injury to the tibial and peroneal nerves due to hemorrhage in the popliteal fossa: two case reports. J Bone Joint Surg Am 1989;71:768–770.
211. Logigian EL, Busis NA, Berger AR, et al. Lumbrical sparing in carpal tunnel syndrome: anatomic, physiologic, and diagnostic implications. Neurology 1987; 37:1499–1505.
212. Lorei MP, Hershman EB. Peripheral nerve injuries in athletes. Treatment and prevention. Sports Med 1993;16:130–147.
213. Luerssen TG, Campbell RL, Defalque RJ, et al. Spontaneous saphenous neuralgia. Neurosurgery 1983; 13:238–241.
214. Lundy CT, Goyal S, Lee S, et al. Bilateral radial nerve palsy in a newborn. Neurology 2009;72:576.
215. Lutz EG. Credit-card-wallet sciatica. JAMA 1978; 240:738.
216. Maffulli N, Maffulli F. Transient entrapment of the posterior interosseous nerve in violin players. J Neurol Neurosurg Psychiatry 1991;54:65–67.
217. Magalhaes JE, Januario AMS, Lins OG. Intercostobrachial neuropathy due to axillary compression. Muscle Nerve 2009:39:411–412.
218. Makin GJV, Brown WF. Entrapment of the posterior cutaneous nerve of the arm. Neurology 1985;35: 1677–1678.
219. Maniker AH, Thurmond J, Padberg FT Jr, et al. Traumatic venous varix causing sciatic neuropathy: case Report. Neurosurgery 2004;55:E1236–E1239.
220. Marangoni C, Lacerenza M, Formaglio F, et al. Sensory disorder of the chest as presenting symptom of lung cancer. J Neurol Neurosurg Psychiatry 1993;56: 1033–1034.
221. Marrero JL, Goldfine LJ. Isolated lateral pectoral nerve injury: trauma from a seat belt. Arch Phys Med Rehabil 1989;70:239–240.
222. Marwah V. Compression of the lateral popliteal (common peroneal) nerve. Lancet 1964;2:1367– 1369.
223. Massey EW. Gonyalgia paresthetica. Muscle Nerve 1981;4:80–81.
224. Massey EW, Pleet AB. Handcuffs and cheiralgia paresthetica. Neurology 1978;28:1312–1313.
225. Mastaglia FL. Musculocutaneous neuropathy after strenuous physical activity. Med J Aust 1986;145: 153–154.
226. Mastaglia FL. Tibial nerve entrapment in the popliteal fossa. Muscle Nerve 2000;23:1883–1886.
227. Mattio TG, Nishida T, Minieka MM. Lotus neuropathy: report of a case. Neurology 1992;42:1636.
228. Maudsley RH. Fibular tunnel syndrome. J Bone Joint Surg Br 1967;49:384.
229. McCluskey L, Feinberg D, Dolinskas C. Suprascapular neuropathy related to a glenohumeral joint cyst. Muscle Nerve 1999;22:772–777.
230. McKlusky LF. Anomalous superficial radial sensory innervation of the dorsum of the hand: a cause of “paradoxical” preservation of ulnar sensory function. Muscle Nerve 1996;19:923–925.
231. McKowen HC, Voorhies RM. Axillary nerve entrapment in the quadrilateral space—case report. J Neurosurg 1987;66:932–934.
232. McManis PG. Sciatic nerve lesions during cardiac surgery. Neurology 1994;44:684–687.
233. Melamed NB, Satya-Murti S. Obturator neuropathy after total hip replacement. Ann Neurol 1983;13: 578–579.
234. Mellion MB. Common cycling injuries. Management and prevention. Sports Med 1991;11:52–70.
235. Merritt GN, Subotnick SI. Medial plantar digital proper nerve syndrome (Joplin’s neuroma)—typical presentation. J Foot Surg 1982;21:166–169.
236. Midroni G, Moulton R. Radial entrapment neuropathy due to chronic injection-induced triceps fibrosis. Muscle Nerve 2001;24:134–137.
237. Miller EH, Benedict FE. Stretch of the femoral nerve in a dancer: a case report. J Bone Joint Surg Am 1985;67:315–317.
238. Miller RG. The cubital tunnel syndrome: diagnosis and precise localization. Ann Neurol 1979;6:56–59.
239. Miller RG. AAEM Case Report #1: ulnar neuropathy at the elbow. Muscle Nerve 1991;14:97–101.
240. Mittal RL, Gupta BR. Median and ulnar nerve palsy: an unusual presentation of the supracondylar process. J Bone Joint Surg 1978;60:557–558.
241. Mondelli M, Cioni R, Federico A. Rare mononeuropathies of the upper limb in bodybuilders. Muscle Nerve 1998;21:809–812.
242. Mondelli M, Giannini F, Guazzi G, et al. Obturator neuropathy due to obturator hernia. Muscle Nerve 2002;26:291–292.
243. Mondelli M, Martell G, Greco G. Mononeuropathies of inferior and superior gluteal nerves due to hypertrophy of piriformis muscle in a basketball player. Muscle Nerve 2008;38:1660–1662.
244. Montagna P, Colonna S. Suprascapular neuropathy restricted to the infraspinatus muscle in volleyball players. Acta Neurol Scand 1993;87:248–250.
245. Monteyne P, Dupuis MJ, Sindic CJ. Neuritis of the serratus anterior muscle associated with Borrelia burgdorferi infection. Rev Neurol (Paris) 1994;150: 75–77.
246. Morini A, Viola L, Orrico D, et al. Proximal median mononeuropathy associated with an anomalous deep course through the brachialis muscle. J Neurol Neurosurg Psychiatry 2000;69:698–699.
247. Morris HH, Peters BH. Pronator syndrome: clinical and electrophysiological features in seven cases. J Neurol Neurosurg Psychiatry 1976;39:461–464.
248. Moser T, Scheiber-Nogueira M-C, Nogueira TS, et al. Pudendal nerve compression by pelvic varices: successful treatment with transcatheter ovarian vein embolisation. J Neurol Neurosurg Psychiatry2006;77:88.
249. Muller-Vahl H. Isolated complete paralysis of the tensor fasciae latae muscle. Eur Neurol 1985;24:289–291.
250. Murayama K, Takeuchi T, Yuyama T. Entrapment of the saphenous nerve by branches of the femoral vessels. A report of two cases. J Bone Joint Surg 1991; 73A1:770–772.
251. Murovic JA, Kim DH, Tiel RL, et al. Surgical management of 10 genitofemoral neuralgias at the Louisiana State University Health Sciences Center. Neurosurgery 2005;56:298–303.
252. Nahabedian MY, Dellon AL. Meralgia paresthetica: etiology, diagnosis, and outcome of surgical decompression. Ann Plast Surg 1995;35:590–594.
253. Nakajima M, Ono N, Kojima T, et al. Ulnar entrapment neuropathy along the medial intermuscular septum in the midarm. Muscle Nerve 2009;39:707–710.
254. Nakamichi K, Tachibana S. Radial nerve entrapment by the lateral head of the triceps. J Hand Surg 1991; 16:748–750.
255. Nakano KK. Entrapment neuropathy from Baker’s cyst. JAMA 1978;239:135.
256. Nardin R, Chapman K, Raynor E. Prevalence of ulnar neuropathy in patients receiving hemodialysis. Arch Neuro 2005;62:271–275.
257. Nardone R, Venturi A, Ladurner G, et al. Obturator mononeuropathy caused by lipomatosis of the nerve: a case report. Muscle Nerve 2008;38:1046–1048.
258. Nunley JA, Bassett FH. Compression of the musculocutaneous nerve at the elbow. J Bone Joint Surg 1982;64:1050–1052.
259. O’Brien MD. Genitofemoral neuropathy. Br Med J 1979;1:1052.
260. Oh SJ, Kwon KH, Hah JS, et al. Lateral plantar neuropathy. Muscle Nerve 1999;22:1234–1238.
261. Oh SJ, Lee KW. Medial plantar neuropathy. Neurology 1987;37:1408–1410.
262. Oh SJ, Sarala PK, Kuba T. Tarsal tunnel syndrome: electrophysiological study. Ann Neurol 1979;5:327–330.
263. Ostrovskiy D, Wilbourn A. Acute bowler’s thumb. Neurology 2004;63:938.
264. Oware A, Herskovitz S, Berger AR. Long thoracic nerve palsy following cervical chiropractic manipulation. Muscle Nerve 1995;18:1351.
265. Padua L, DeAloya E, LoMonaco M, et al. Mononeuropathy of a distal branch of the femoral nerve in a body building champion. J Neurol Neurosurg Psychiatry 1997;63:669–671.
266. Padua L, Padua R, Lo Monaco M, et al. Multiperspective assessment of carpal tunnel syndrome. A multicenter study. Neurology 1999;53:1654–1659.
267. Paladini D, Dellantonio R, Cinti A, et al. Axillary neuropathy in volleyball players: report of two cases and literature review. J Neurol Neurosurg Psychiatry 1996;60:345–347.
268. Park JW, Kim DH, Hwang M, et al. Meralgia paresthetica caused by hip-huggers in a patient with aberrant course of the lateral femoral cutaneous nerve. Muscle Nerve 2007;35:678–680.
269. Park TA, Del Toro DR. The medial calcaneal nerve: anatomy and nerve conduction technique. Muscle Nerve 1995;18:32–38.
270. Pellegrino MJ, Johnson EW. Bilateral obturator nerve injuries during urologic surgery. Arch Phys Med Rehabil 1988;69:46–47.
271. Perlmutter GS, Leffert RD, Zarins B. Direct injury to the axillary nerve in athletes playing contact sports. Am J Sports Med 1997;25:65–68.
272. Peters WJ, Todd TRJ. Anterior interosseous nerve compression: from metastatic bronchogenic carcinoma to the forearm. Plast Reconstr Surg 1983;72: 706–707.
273. Petrera JE, Trojaborg W. Conduction studies of the long thoracic nerve in serratus anterior palsy of different etiology. Neurology 1984;34:1033–1037.
274. Phan TG, Evans BA, Huston J. Pseudoulnar palsy from a small infarct of the precentral knob. Neurology 2000;54:2185.
275. Phillips LH. Familial long thoracic nerve palsy: a manifestation of brachial plexus neuropathy. Neurology 1986;36:1251–1253.
276. Phillips LH, Morgan RF. Anomalous origin of the sural nerve in a patient with tibial-common peroneal nerve anastomosis. Muscle Nerve 1993;16:414–417.
277. Phillips LH, Persing JA, Vandenberg SR. Electrophysiological findings in localized hypertrophic mononeuropathy. Muscle Nerve 1991;14:335–341.
278. Popelka S, Vainio K. Entrapment of the posterior interosseous branch of the radial nerve in rheumatoid arthritis. Acta Orthop Scand 1975;45:370–372.
279. Posas HN, Rivner MH. Deep peroneal sensory neuropathy. Muscle Nerve 1992;15:745–746.
280. Pradat P-F, Bouche P, Delanian S. Sciatic nerve moneuropathy: an unusual late effect of radiotherapy. Muscle Nerve 2009;40:872–874.
281. Preston D, Logigian E. Iatrogenic needle-induced peroneal neuropathy in the foot. Ann Intern Med 1988;109:921–922.
282. Pringle CE, Guberman AH, Jacob P. Another kind of knapsack palsy. Neurology 1996;46:585.
283. Pringle RM, Protheroe K, Mukherjee SK. Entrapment neuropathy of the sural nerve. J Bone Joint Surg 1974;56B:465–468.
284. Proudman TW, Menz PJ. An anomaly of the median artery associated with anterior interosseous nerve syndrome. J Hand Surg (Br) 1992;17:507–509.
285. Prusick VR, Herkowitz HN, Davidson DD, et al. Sciatica from a sciatic neurilemoma. J Bone Joint Surg Am 1986;68:1456–1457.
286. Pugliese GN, Green RF, Antonacci A. Radiation-induced long thoracic nerve palsy. Cancer 1987;60: 1247–1248.
287. Ramesh M, O’Bryne JM, McCarthy N, et al. Damage to the superior gluteal nerve after Hardinge approach to the hip. J Bone Joint Surg Br 1996;78: 903–906.
288. Rask MR. Superior gluteal nerve entrapment syndrome. Muscle Nerve 1980;3:304–307.
289. Rafecas JC, Daube JR, Ehman RL. Deep branch ulnar neuropathy due to giant cell tumor: report of a case. Neurology 1988;38:327–329.
290. Redwine DB, Sharpe DR. Endometriosis of the obturator nerve: a case report. J Reprod Med 1990;35: 434–435.
291. Reisin R, Pardal A, Ruggieri V, et al. Sural neuropathy due to external pressure: report of three cases. Neurology 1994;44:2408–2409.
292. Rengachary SS, Neff JP, Singer PA. Suprascapular entrapment neuropathy: a clinical, anatomical, and comparative study. Neurosurgery 1979;5:441–446.
293. Rennels GD, Ochoa J. Neuralgic amyotrophy manifesting as anterior interosseous nerve palsy. Muscle Nerve 1980;3:160–164.
294. Richards BJ, Gillett WR, Pollock M. Reversal of foot drop in sciatic nerve endometriosis. J Neurol Neurosurg Psychiatry 1991;54:935–936.
295. Rigaud J, Labat J-J, Riant T, et al. Obturator nerve entrapment: diagnosis and laparoscopic treatment. Technical case report. Neurosurgery 2007;61:E175.
296. Roberts AP, Allan DB. Digital nerve injuries in orthopaedic surgeons. Injury 1988;19:233–234.
297. Roganovic Z. Missile-caused complete lesions of the peroneal nerve and peroneal division of the sciatic nerve: results of 157 repairs. Neurosurgery 2005;57: 1201–1212.
298. Rogers LR, Borkowski GP, Albers JW, et al. Obturator mononeuropathy caused by pelvic cancer: six cases. Neurology 1993;43:1489–1492.
299. Rose RC. Acute carpal tunnel syndrome secondary to thrombosis of a persistent median artery. West Indian Med J 1995;44:32–33.
300. Rose HA, Hood RW, Otis JC. Peroneal-nerve palsy following total knee arthroplasty. a review of the hospital for special surgery experience. J Bone Joint Surg 1982;64A:347–351.
301. Ross MA, Kimura J. AAEM report #2: the carpal tunnel syndrome. Muscle Nerve 1995;18:567–573.
302. Rossi F, Triggs WJ, Gonzalez R, et al. Bilateral medial pectoral neuropathy in a weight lifter. Muscle Nerve 1999;22:1597–1599.
303. Roth G, Ludy JP, Egloff-Baer S. Isolated proximal median neuropathy. Muscle Nerve 1982;5:247–249.
304. Rubin M, Heise CW. Proximal neuropathy in Colles’ fracture. Can J Neurol Sci 1997;24:77–78.
305. Rubin M, Menche D, Pitman M. Entrapment of an accessory superficial peroneal sensory nerve. Can J Neurol Sci 1991;18:342–343.
306. Ruder JR, Wood VE. Ulnar nerve compression at the arch of origin of the adductor pollicis muscle. J Hand Surg 1993;18:893–895.
307. Ryan GM, Conners S. Posterior interosseous nerve paralysis and amyloid neuropathy of multiple myeloma. Clin Orthop 1982;171:202.
308. Sabin TD. Temperature-linked sensory loss: a unique pattern in leprosy. Arch Neurol 1969;20:257–262.
309. Sabin TD. Classification of peripheral neuropathy: the long and the short of it. Muscle Nerve 1986;9: 711–719.
310. Sachs GM, Raynor EM, Shefner JM. The all-ulnar motor hand without forearm anastomosis. Muscle Nerve 1995;18:309–313.
311. Sadeh M, Gilad R, Dabby R, et al. Apparent weakness of ulnar-innervated muscles in radial palsy. Neurology 2004;62:1424–1425.
312. Saeed MA, Gatens PF. Anterior interosseous nerve syndrome: unusual etiologies. Arch Phys Med Rehabil 1983;64:182.
313. Salazar-Grueso E, Roos R. Sciatic endometriosis: a treatable sensorimotor mononeuropathy. Neurology 1986;36:1360–1363.
314. Sammarco GJ, Conti SF. Tarsal tunnel syndrome caused by an anomalous muscle. J Bone Joint Surg Am 1994;76:1308–1314.
315. Sander HW, Quinto CM, Elinzano H, et al. Carpet carrier’s palsy: musculocutaneous neuropathy. Neurology 1997;48:1731–1732.
316. Saphner T, Gallion HH, Van Nagell JR, et al. Neurologic complications of cervical cancer: a review of 2261 cases. Cancer 1989;64:1147–1151.
317. Sawin PD, Loftus CM. Posterior interosseous nerve palsy after brachiocephalic arteriovenous fistula construction: report of two cases. Neurosurgery 1995;37: 537–539.
318. Scherer K, Skeen M, Strine S, et al. Hanging leg syndrome: combined bilateral femoral and sciatic neuropathies. Neurology 2006:66:1124–1125.
319. Schultz JS, Leonard JA. Long thoracic neuropathy from athletic activity. Arch Phys Med Rehabil 1992; 73:87–90.
320. Schottland JR. Femoral neuropathy from inadvertent suturing of the femoral nerve. Neurology 1996;47: 644–845.
321. Schwabegger AH, Shafighi M, Gurunluoglu R. An unusual case of thigh adductor weakness: obturator nerve ganglion. J Neurol Neurosurg Psychiatry 2004; 75:775.
322. Scott TF, Yager JG, Gross JA. Handcuff neuropathy revisited. Muscle Nerve 1989;12:219–220.
323. Scotto V, Rosica G, Valeri B, et al. Benign schwannoma of the obturator nerve: a case report. Am J Obstet Gynecol 1998;179:816–817.
324. Segmuller HE, Alfred SP, Zilio G, et al. Cutaneous nerve lesions of the shoulder and arm after arthroscopic surgery. J Shoulder Elbow Surg 1995;4:254– 258.
325. Semmler A, von Falkenhausen M, Schroder R. Suprascapular nerve entrapment by a spinoglenoid cyst. Neurology 2008;70:890.
326. Seppalainen AM, Aho K, Uusitupa M. Strawberry pickers’ foot drop. Br Med J 1977;2:767.
327. Seror P. Anterior interosseus nerve lesions: clinical and electrophysiological features. J Bone Joint Surg 1996;78B:238–241.
328. Seror P, Seror R. Meralgia paresthetica: clinical and electrophysiological diagnosis in 120 cases. Muscle Nerve 2006;29:650–654.
329. Sharma KR, Cross J, Santiago F, et al. Incidence of acute femoral neuropathy following renal transplantation. Arch Neurol 2002;59:541–545.
330. Shea JD, McClain EJ. Ulnar nerve compression syndromes at and below the wrist. J Bone Joint Surg 1969;51:1095–1103.
331. Sheean G, Morris JG. Handcuff neuropathy involving the dorsal ulnar cutaneous nerve. Muscle Nerve 1993;16:325.
332. Sheehan TP, Jabre JF. Dorsal ulnar sensory neuropathy in a heroin abuser. Muscle Nerve 1995;18:559.
333. Shenoy AM, Wiesman J. Saphenous mononeuropathy after popliteal vein aneurysm repair. Neurologist 2010:16:47–49.
334. Shimizu K, Iwasaki R, Hoshikawa H, et al. Entrapment neuropathy of the palmar cutaneous branch of the median nerve by fascia of flexor digitorum superficialis. J Hand Surg 1988;13:581–583.
335. Shaffrey ME, Jane JA, Persing JA, et al. Surgeon’s foot: a report of sural nerve palsy. Neurosurgery 1992; 30:927–930.
336. Shyu W-C, Lin J-C, Chang M-K, et al. Compressive radial nerve palsy induced by military shooting training: clinical and electrophysiologic study. J Neurol Neurosurg Psychiatry 1993;56:890–893.
337. Silbert PI, Moore R, Dawson B. Traumatic distal femoral neuropathy. J Neurol Neurosurg Psychiatry 1998;65:614.
338. Sinson G, Zager EL, Kline DG. Windmill pitcher’s radial neuropathy. Neurosurgery 1994;34:1087–1089.
339. Sippo WC, Gomez AC. Nerve entrapment syndromes from abdominal surgery. J Fam Pract 1987;25: 585–587.
340. Sisto D, Chiu WS, Geelhoed GW. Femoral neuropathy after renal transplant. South Med J 1980;73: 1464–1466.
341. Smith BE, Litchy WJ. Sural mononeuropathy: a clinical and electrophysiological study. Neurology 1989; 39:296.
342. Smith W, Amis JA. Neurilemoma of the tibial nerve: a case report. J Bone Joint Surg Am 1992;74:443–444.
343. Sogaard I. Sciatic nerve entrapment. J Neurosurg 1983;58:275–276.
344. Sorenson EJ, Chen JJ, Daube JR. Obturator neuropathy: causes and outcome. Muscle Nerve 2002; 25:605–607.
345. Sotaniemi KA. Slimmer’s paralysis—peroneal neuropathy during weight reduction. J Neurol Neurosurg Psychiatry 1984;47:564–566.
346. Sourkes M, Stewart JD. Common peroneal neuropathy: a study of selective motor and sensory involvement. Neurology 1991;41:1029–1033.
347. Spindler HA, Dellon AL. Nerve conduction studies in the superficial radial nerve entrapment syndrome. Muscle Nerve 1990;13:1–5.
348. Spinner M. The arcade of Frohse and its relationship to posterior interosseous nerve paralysis. J Bone Joint Surg 1968;5011:809–812.
349. Spinner RJ, Atkinson JLD, Wenger DE, et al. Tardy sciatic nerve palsy following apophyseal avulsion fracture of the ischial tuberosity. Case report. J Neurosurg 1998;89:819–821.
350. Spinner RJ, Carmichael SW, Spinner M. Partial median nerve entrapment in the distal arm because of an accessory bicipital aponeurosis. J Hand Surg 1991; 16A:236–244.
351. Spinner RJ, Tiel RL, Kline DG. Predominant infraspinatus muscle weakness in suprascapular nerve compression. Case illustration. J Neurosurg 2000;93:516.
352. Sridhara CR, Izzo KL. Terminal sensory branches of the superficial peroneal nerve: an entrapment syndrome. Arch Phys Med Rehabil 1985;66:789–791.
353. Stamboulis E. Accessory deep peroneal nerve. Electromyogr Clin Neurophysiol 1987;27:289–292.
354. Starling JR, Harms BA, Schroeder ME, et al. Diagnosis and treatment of genitofemoral and ilioinguinal entrapment neuralgia. Surgery 1987;102:581–586.
355. Stellbrink G. Compression of the palmar branch of the median nerve by atypical palmaris longus muscle. Handchirurgie 1972;4:155–157.
356. Stevens JC, Smith BE, Weaver AL, et al. Symptoms of 100 patients with electromyographically verified carpal tunnel syndrome. Muscle Nerve 1999;22:48–1456.
357. Stevens JC, Witt JC, Smith BE, et al. The frequency of carpal tunnel syndrome in computer users at a medical facility. Neurology 2001;56:1568–1570.
358. Stewart JD. Medial plantar neuropathy. Neurology 1981;31:149.
359. Stewart JD. Peripheral nerve fascicles: anatomy and clinical relevance. Muscle Nerve 2003;28:525–541.
360. Stickler DE, Morley KN, Massey EW. Sural neuropathy: etiologies and predisposing factors. Muscle Nerve 2006;34:482–484.
361. Stone DA, Laureno R. Handcuff neuropathies. Neurology 1991;41:145.
362. Streib E. Upper arm radial nerve palsy after muscular effort: report of three cases. Neurology 1992;42:1632– 1634.
363. Streib EW. Ulnar-to-median anastomosis in the forearm: electromyographic studies. Neurology 1979;29: 1534–1537.
364. Streib EW, Sun SF, Pfeiffer RF. Toe extensor weakness resulting from trivial athletic trauma. Am J Sports Med 1982;10:311–313.
365. Stulz P, Pfeiffer KM. Peripheral nerve injuries resulting from common surgical procedures in the lower portion of the abdomen. Arch Surg 1982;117:324–327.
366. Stuplich M, Hottinger AF, Stoupis C, et al. Combined femoral and obturator neuropathy caused by synovial cyst of the hip. Muscle Nerve 2005;32:552–554.
367. Subramony SH. Electrophysiological findings in crutch palsy. Electromyogr Clin Neurophysiol 1989; 29:281–285.
368. Takahura Y, Kitada C, Sugimoto K, et al. Tarsal tunnel syndrome. Causes and results of operative treatment. J Bone Joint Surg Br 1991;73:125–128.
369. Takao M, Fukuuchi Y, Koto A, et al. Localized hypertrophic mononeuropathy involving the femoral nerve. Neurology 1999;52:389–392.
370. Tasmuth T, von Smitten K, Hietanen P, et al. Pain and other symptoms after different treatment modalities of breast cancer. Ann Oncol 1995;6:453–459.
371. Taxay EP. Toilet-seat neuropathy. N Engl J Med 1969; 280:1484.
372. Taylor KO. Morbidity associated with axillary surgery for breast cancer. Austral NZ J Surg 2004;74:314–317.
373. Tesio L, Bassi L, Galardi G. Transient palsy of hip abductors after a fall on the buttocks. Arch Orthop Trauma Surg 1990;109:164–165.
374. Thiebot J, Laissy JP, Delangre T, et al. Benign solitary neurinomas of the sciatic popliteal nerves. CT study. Neuroradiology 1991;33:186–188.
375. Thurman RT, Jindal P, Wolff TW. Ulnar nerve compression in Guyon’s canal caused by calcinosis in scleroderma. J Hand Surg 1991;16:739–741.
376. Timsit S, Logak M, Manaï R, et al. Evolving isolated hand palsy: a parietal lobe syndrome associated with carotid artery disease. Brain 1997;120:2251–2257.
377. Tindall B. Aids to the examination of the peripheral nervous system. London, UK: WB Saunders, 1986: 1–61.
378. Tison F, Boulan P. An unusual sciatic neuropathy. J Neurol Neurosurg Psychiatry 1995;59:16.
379. Torpey BM, Pess GM, Kircher MT, et al. Ulnar nerve laceration in a closed bone forearm fracture. J Orthop Trauma 1996;10:131–134.
380. Tyrell PJ, Feher MD, Rossor MN. Sciatic nerve damage due to toilet seat entrapment: another Saturday night palsy. J Neurol Neurosurg Psychiatry 1989;52: 1113–1115.
381. Uchida Y, Sugioka Y. Electrodiagnosis of Martin-Gruber connection and its clinical importance in peripheral nerve surgery. J Hand Surg 1992;17:54–59.
382. Van Der Meché FGA, Van Gijn J. Hypotonia: an erroneous clinical concept? Brain 1986;109:1169–1178.
383. Veilleux M, Richardson P. Proximal median neuropathy secondary to humeral neck fracture. Muscle Nerve 2000;23:426–429.
384. Viswanathan A, Kim DH, Reid N, et al. Surgical management of the pelvic plexus and lower abdominal nerves. Neurosurgery 2009;65:(Supplement):A44–A51.
385. Vogel CM, Albin R, Albers JW. Lotus foot drop: sciatic neuropathy in the thigh. Neurology 1991;41: 605–606.
386. Voitk AJ, Mueller JC, Farlingen DE, et al. Carpal tunnel syndrome in pregnancy. Can Med Assoc J 1983;128:277.
387. Walker M, Meekins G, Hu S-C. Yoga neuropathy: a snoozer. Neurologist 2005;11(3):176–178.
388. Ward PJ, Porter ML. Tarsal tunnel syndrome: a study of the clinical and neurophysiological results of decompression. J R Coll Surg Edinb 1998;43:35–36.
389. Warfield CA. Obturator neuropathy after forceps delivery. Obstet Gynecol 1984;64:47S–48S.
390. Weizer MJ, Franssen H, Rinkel GJ, et al. Meralgia paresthetica: differential diagnosis and follow-up. Muscle Nerve 1996;19:522–524.
391. Wertsch JJ. Pricer palsy. N Engl J Med 1985;312: 1645.
392. Wertsch JJ. AAEM case report #25: anterior interosseous nerve syndrome. Muscle Nerve 1992;15:977–983.
393. Wertsch JJ, Sanger JR, Matloub HJ. Pseudo-anterior interosseous syndrome. Muscle Nerve 1985;8:68–70.
394. Widmer F, Gerster JC. Medial meniscal cyst imitating a tumor, with compression of the saphenous nerve. Rev Reum 1998;65:149–152.
395. Wilbourn AJ. AAEE case report #12: common peroneal mononeuropathy at the fibular head. Muscle Nerve 1986;9:825–836.
396. Wilbourn AJ. The anterior tarsal tunnel syndrome revisited. Muscle Nerve 1992;15:1175.
397. Wilbourn AJ, Furlan AJ, Hulley W. Ischemic monomelic neuropathy. Neurology 1983;33:447–451.
398. Wilbourn A, Lederman R, Sweeney P. Brachial plexopathy: a complication of closed repair of shoulder dislocation. Can J Neurol Sci 1992;19:300.
399. Wilemon WK. Tarsal tunnel syndrome: a 50 year survey of the world literature and a report of two cases. Orthop Rev 1979;8:111–117.
400. Williams PH, Trzil KP. Management of meralgia paresthetica. Neurosurgery 1991;74:76–80.
401. Willick SE, Margherita AJ, Carter GT. Isolated superior gluteal nerve injury: two case reports. Muscle Nerve 1998;21:951–953.
402. Wilson SM, Devarj V, Gardner-Thorpe C. Upholsterer’s PIN. J Neurol Neurosurg Psychiatry 2001; 70:706–707.
403. Wood KM. Intercostobrachial nerve entrapment syndrome. Southern Med J 1978;71:662–663.
404. Wu KT, Jordan RR, Eckert C. Lipoma, a cause of paralysis of deep radial (posterior interosseous) nerve: report of a case and review of the literature. Surgery 1974;75:790–795.
405. Yamashita M, Mezaki T, Yamamoto T. “All tibial foot” with sensory crossover innervation between the tibial and deep peroneal nerves. J Neurol Neurosurg Psychiatry 1998;65:798–799.
406. Yeremeyeva E, Kline DG, Kim D. Iatrogenic sciatic nerve injuries at buttock and thigh levels: The Louisiana State University experience review. Neurosurgery 2009;65 (Supplement):A63–A66.
407. Young MR, Norris JW. Femoral neuropathy during anticoagulant therapy. Neurology 1976;26:1173– 1175.
408. Young NP, Sorenson EJ, Spinner RJ, et al. Clinical and electrodiagnostic correlates of peroneal intraneural ganglia. Neurology 2009;72:447–452.
409. Yuen EC, Olney RK, So YT. Sciatic neuropathy: clinical and prognostic features in 73 patients. Neurology 1994;44:1669–1674.
410. Zager EL, Pfeifer S, Brown MJ, et al. Catamenial mononeuropathy and radiculopathy: a treatable neuropathic disorder. J Neurosurgery 1998;88:827–830.
411. Zahrawi F. Acute compression ulnar neuropathy at Guyon’s canal resulting from lipoma. J Hand Surg 1984;9:238–240.
412. Zanotti RM, Carpenter JE, Blasier RB, et al. The low incidence of suprascapular nerve injury after primary repair of massive rotator cuff tears. J Shoulder Elbow Surg 1997;6:258–264.
413. Zikel OM, Davis DH, Auger RG, et al. Venous varix causing median neuropathy. Case illustration. J Neurosurg 1997;87:130.
414. Zoran R. Missile-caused ulnar nerve injuries: outcomes of 128 repairs. Neurosurgery 2004;55:1120– 1129.
415. Zylicz Z, Nuyten FJ, Notermans SL, et al. Postoperative ulnar neuropathy after kidney transplantation. Anesthesia 1984;39:1117–1120.